Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Prevalence of Depression, Anxiety, and Post-Traumatic Stress Disorder and Their Associated Factors Among Internally Displaced Persons in Burao, Somaliland: Community-Based Cross-Sectional Study
Authors Nuh AY ![]()
Received 24 June 2025
Accepted for publication 4 November 2025
Published 8 November 2025 Volume 2025:21 Pages 2465—2478
DOI https://doi.org/10.2147/NDT.S549351
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Abdilaahi Yusuf Nuh1,2
1Department of Public Health, Faculty of Health Science, Alpha University, Burao, Somaliland; 2Department of Epidemiology, Faculty of Public Health, Jimma University, Jimma, Ethiopia
Correspondence: Abdilaahi Yusuf Nuh, Email [email protected]
Objective: This study assessed the prevalence of depression, anxiety, and post-traumatic stress disorder (PTSD) and examined their associated factors among internally displaced persons (IDPs) in Burao, Somaliland.
Methods: A community-based cross-sectional study was conducted from April 15 to May 30, 2025, among 372 IDPs aged ≥ 18 years selected through systematic random sampling from two settlements. Data were collected using structured interviewer-administered questionnaires incorporating internationally validated tools: The Patient Health Questionnaire-9 (PHQ-9), Generalized Anxiety Disorder-7 (GAD-7), and Primary Care PTSD Screen for DSM-5 (PC-PTSD-5). Descriptive statistics were computed, followed by univariable and multivariable logistic regression analyses to identify factors associated with each disorder. Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were reported, with p < 0.05 considered statistically significant.
Results: The prevalence of depression, anxiety, and PTSD was 63.4%, 53.0%, and 38.2%, respectively. For depression, participants displaced for 1– 5 years were less likely to report depressive symptoms (AOR = 0.14, 95% CI: 0.04– 0.47). For anxiety, married individuals had higher odds (AOR = 3.38, 95% CI: 1.38– 8.28), larger household size increased risk (AOR = 1.89, 95% CI: 1.11– 3.22), while secondary education was protective (AOR = 0.06, 95% CI: 0.01– 0.47). For PTSD, older age was a strong predictor (26– 35 years: AOR = 2.41, 95% CI: 1.10– 5.30; 36– 60 years: AOR = 3.58, 95% CI: 1.62– 7.89), and being single increased odds (AOR = 4.41, 95% CI: 1.24– 15.75).
Conclusion: Mental disorders are highly prevalent among IDPs in Burao, with depression being the most common. Each disorder demonstrated distinct risk profiles: demographic, educational, and displacement-related factors influenced the likelihood of depression, anxiety, and PTSD differently. Tailored psychosocial and community-based mental health interventions are urgently needed to address these specific risk factors and reduce the mental health burden among displaced populations.
Keywords: internally displaced persons, depression, anxiety, post-traumatic stress disorder, Somaliland, risk factors
Introduction
Internally displaced persons (IDPs) are individuals who have been forced to leave their original homes or places of residence but have resettled within the borders of their own country or territory.1 Displacement is a traumatic event that disrupts families and impacts physical and psychological health across all ages.2–4 In Africa, climate change and environmental stressors are projected to increase the risk of conflict, with one study estimating a 54% rise in conflicts by 2030.5 Each year, countless people worldwide are compelled to abandon their homes due to violence, warfare, and natural calamities, while others continue to live in displacement within their own countries.6 By the end of 2020, it was estimated that approximately 55 million people were internally displaced due to conflicts and environmental challenges, with around 40.5 million new displacements occurring in 2020 alone. This increase in displacement was linked to conflicts and natural disasters across 149 countries.7
In Somaliland, internal displacement represents a complex and recurring issue, driven by interrelated factors such as insecurity, drought, and other natural disasters.8 The drought of 2016–2017 alone resulted in the displacement of approximately 300,000 individuals across the region. Consistent with broader urbanization trends, both protracted and newly displaced internally displaced persons (IDPs) in Somaliland predominantly reside in urban centers, particularly Hargeisa and Burao, where they are either integrated into host communities or reside in dedicated settlements.9 Despite the growing concern, there is no published data on the prevalence of mental disorders in the general population of Somaliland, making it difficult to assess the additional burden faced by internally displaced persons.
Mental disorders are a significant public health problem, and 14% of the total burden of disease has been attributed to neuropsychiatric disorders including depression and other common mental disorders.10 Additionally, the proportion of global Disability Adjusted Life Years (DALYs) attributed to mental disorders increased to 4.9% (3.9–6.1) and Years lived with disability (YLDs) contributed to most of the mental disorder burden, with 125.3 million YLDs (95% UI 93.0–163.2; 14.6% [12.2–16.8] of global YLDs) in 2019.11 Exposure to repeated trauma and extreme violence such as torture is associated with an increased risk for a mental disorder.12–14
In numerous epidemiological surveys and studies concerning the psychopathology of conflict-affected, depression is identified as one of the most prevalent mental health disorders.15,16 Affecting approximately 121 million individuals globally, depression is among the leading causes of disability worldwide.17
A systematic review has indicated that approximately 31% of refugees and internally displaced populations fulfill the diagnostic criteria for post-traumatic stress disorder (PTSD). In comparison, around 32% meet the criteria for major depressive disorders.18 The prevalence of PTSD and depressive disorders is frequently examined in conflict settings, given the anticipated widespread psychological trauma among these populations. A study conducted on internally displaced persons (IDPs) in Ukraine reported a PTSD prevalence of 32%, with depression prevalence at 22%.19 In Colombia, research identified high levels of PTSD and depression among IDPs, with prevalence rates of 88% and 41%, respectively.16
Also, meta-analyses of several studies published between 1980 and 2017, where estimated the prevalence of PTSD (96/129; 74.4% of the studies), depression (70/129; 54.3% of the studies), and anxiety (38/129; 29.4% of the studies) identified a relationship between exposure to different types of disaster and conflict-related events and mental health disorders including anxiety, depression, and PTSD.20 The prevalence of mental health diseases was 21% (95% CI 18.8–25.7) at the point in time in the conflict-affected populations assessed.20
Lower educational level was significantly associated with PTSD and depression, whereas a higher educational level could be a protective factor for the development of PTSD.21 A study on the prevalence of PTSD among Syrian refugees in Turkey found that a family history of mental disorders is significantly associated with PTSD.22 Somalia has been in turmoil and political instability for the last three decades. The country has experienced fierce conflicts between rival groups and frequent terrorist attacks since the collapse of Siad Barre’s regime in 1991. The World Health Organization reports that one-in-three people are affected by mental disorders, with individuals suffering from mental illnesses being subjected to stigma and social isolation. For such individuals, the burden of care is largely left to their caregivers.23
Despite growing global evidence, there is limited research on the mental health of IDPs in Somaliland. To date, no published studies have specifically assessed the prevalence and associated factors of depression, anxiety, and PTSD among IDPs in Burao. Understanding the burden and risk factors in this population is crucial for developing targeted mental health interventions. Therefore, this study aimed to determine the prevalence of depression, anxiety, and Post-Traumatic Stress Disorder (PTSD) and identify the associated factors among internally displaced persons (IDPs) living in Burao, Somaliland.
Method and Materials
Study Design, Period, and Setting
A community-based cross-sectional study was conducted with internally displaced persons aged 18 years and above between April 15 and May 30, 2025.
According to the United Nations Guiding Principles on Internal Displacement, internally displaced persons (IDPs) are defined as individuals or groups who have been compelled or forced to flee or leave their homes or usual places of residence. This displacement is often due to, or in anticipation of, the impacts of armed conflict, widespread violence, human rights violations, or natural or human-made disasters, and these individuals have not crossed an internationally recognized state border.24 In this study an IDP was considered aligning with the United Nations Guiding Principles on Internal Displacement.
Burao City is the second-largest city in Somaliland and the capital of the Togdheer region, located 260 km away from Hargeisa, the capital of Somaliland. Burao is one of the largest urban centers in Somaliland and hosts a significant population of internally displaced persons (IDPs) who have fled conflict, drought, or other humanitarian crises in surrounding regions. As of 2021, Burao hosted an estimated 37,578 displaced households, accounting for approximately 225,468 individuals.25
Within Burao city, there are a total of six recognized IDP settlements. For this study, data were collected from two of these settlements: Aden Saleban and Kur-Libah were purposively selected due to their large IDP populations and logistical accessibility.
Eligibility Criteria
Inclusion Criteria
Adults aged ≥18 years, residing in the selected settlements for at least six months, and willing to participate.
Exclusion Criteria
Individuals with severe illness preventing participation or communication at the time of the survey.
Sample Size Determination
The sample size for this study was determined using the single population proportion formula. A previous multi-center study conducted in Baidoa, Dolow, and Kismayo, Somalia, reported the prevalence of anxiety, depression, and PTSD as 35%, 32.1%, and 30%, respectively.26 Prevalence of anxiety from a previous Somali IDPs study, chosen as it gave the largest sample size compared to depression (32.1%) and PTSD (30%). With a 95% confidence interval and a margin of error (d) of 5%, and accounting for a 10% non-response rate, the minimum required sample size was calculated to be 385. This ensured a conservative estimate and minimized the risk of under sampling.
n=350
p=35%
d=5%
Where:
p= prevalence of anxiety among IDPs.
d= margin of error.
n= sample size.
 = A standard score of the confidence interval of 95%, ie 1.96.
= A standard score of the confidence interval of 95%, ie 1.96.
Sampling Technique
A proportional allocation was applied to each settlement based on the number of households. Within each settlement, systematic random sampling was used. A sampling interval (k) was determined by dividing the total number of households by the required sample size for that site. The first household was selected randomly, and subsequent households were chosen at regular intervals until the sample size was reached. If more than one eligible participant was found in a household, one was randomly selected using a lottery method.
Study Variables
Dependent Variables
In this study, symptoms of post-traumatic stress disorder (PTSD), depression, and anxiety, were considered as dependent variables.
Independent Variables
The sociodemographic variables included age, gender, marital status, educational attainment, monthly household income, and household size. Factors related to displacement encompass the duration since displacement and the absence of adequate shelter. Behavioral factors were centered on substance use, specifically the consumption of khat and tobacco. Health-related variables considered the presence of any chronic medical conditions. Also, psychosocial support was assessed.
Measurement of Variables
PTSD
Assessed using the Primary Care PTSD Screen for the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (PC-PTSD-5), a five-item instrument scored 0–5 (Yes/No format). A score ≥4 was considered positive for probable PTSD.27,28
Anxiety
Assessed using the Generalized Anxiety Disorder 7-item scale (GAD-7), scored 0–21. A cut-off score ≥10 indicated probable anxiety disorder.29–31
Depression
Measured with the Patient Health Questionnaire-9 (PHQ-9), scored 0–27. A cut-off score ≥10 indicated moderate-to-severe depression.17,32
Social Support
Measured using the OSS-3 (score 3–8 = poor, 9–11 = moderate, 12–14 = strong support).33
Household Income
Collected as a continuous value (USD/month), then categorized into low, medium, and high.
Psychosocial Support
Determined by asking whether participants had access to any individual or institutional emotional, financial, or social assistance during the past six months.33
Data Collection Instruments
The data were collected using an interviewer administered and structured questionnaire. It was collected ten nurses and regularly supervised by the first author. The questionnaire was designed in English and translated into Somali and back to English to maintain consistency. Data collectors were trained how to interview the participants and explain unclear questions and purpose of the study. Before administering the questionnaire, each respondent listened to the explanations about the aim of the study and terms of participation.
While the PC-PTSD-5, GAD-7, and PHQ-9 are widely used in humanitarian and conflict-affected contexts, they have not yet been formally validated in Somaliland. Nevertheless, these instruments have been validated in similar low- and middle-income country (LMIC) settings, including South Africa, Kenya, and Ethiopia, where they demonstrated good psychometric properties.29–31 For this study, cultural adaptation procedures were undertaken, including translation into the local language, back-translation to ensure accuracy, and pre-testing on 5% of the sample in a non-study settlement to assess clarity and cultural relevance. Internal consistency reliability was assessed using Cronbach’s alpha, which yielded a value of 0.83, indicating good reliability in this setting.
Data Quality Assurance
To ensure data quality, a pre-test was conducted on 20 participants outside the study sites to assess the clarity and reliability of the questionnaire. Data collection was accompanied by daily supervision and random spot checks to monitor adherence to the study protocol. All data were entered twice by independent data clerks, and cross-checking was performed to identify and correct any discrepancies. Incomplete questionnaires were reviewed immediately to address missing information before final submission.
Statistical Analysis
Data analysis was conducted using STATA version 17. Descriptive statistics were done for all variables in the study and displayed as frequency, percentages, means, and standard deviations. We considered three main outcomes (dependent variables): PTSD, anxiety, and depression. The Chi-square was used to assess associations between the main outcomes and the independent variables.
Variables with p < 0.25 in bivariate analysis were considered candidates for the multivariable logistic regression models. Model fitness was assessed using the Hosmer–Lemeshow goodness-of-fit test (χ2 = 252.12, p = 0.0012). Multicollinearity was examined using variance inflation factors (VIF), with all variables below the conventional threshold of 5, indicating no significant multicollinearity.
Result
Sociodemographic Characteristics of Study Participants
The study included 372 participants, resulting in a response rate of 96.6%. Among these 372 respondents, the majority of internally displaced persons (IDPs) in Burao City were aged between 26 and 60 years, with 137 (37%) aged 26–35 and 156 (42%) aged 36–60. The sample was predominantly male, comprising 260 (70%) of the participants. Most respondents were married, with 285 (77%) reporting this status, while 39 (10%) were single. A significant proportion, 268 (72%), had no formal education, and household sizes typically ranged from 5 to 9 members for 254 (68%) respondents. Notably, 288 (77%) of the IDPs reported lacking shelter, indicating precarious living conditions. Regarding the duration of displacement, 237 (64%) had been displaced for over five years, suggesting a prolonged period of instability.
Substance use was prevalent among the population, with 288 (77%) chewing khat and 304 (82%) using tobacco. Chronic illness was reported by 197 (53%) of respondents, highlighting considerable health vulnerabilities. Despite these challenges, strong social support was reported by 299 (80%) of the IDPs, which may provide some resilience against the adverse impacts of displacement. Poor social support was reported by only 64 (17%) of respondents (Table 1).
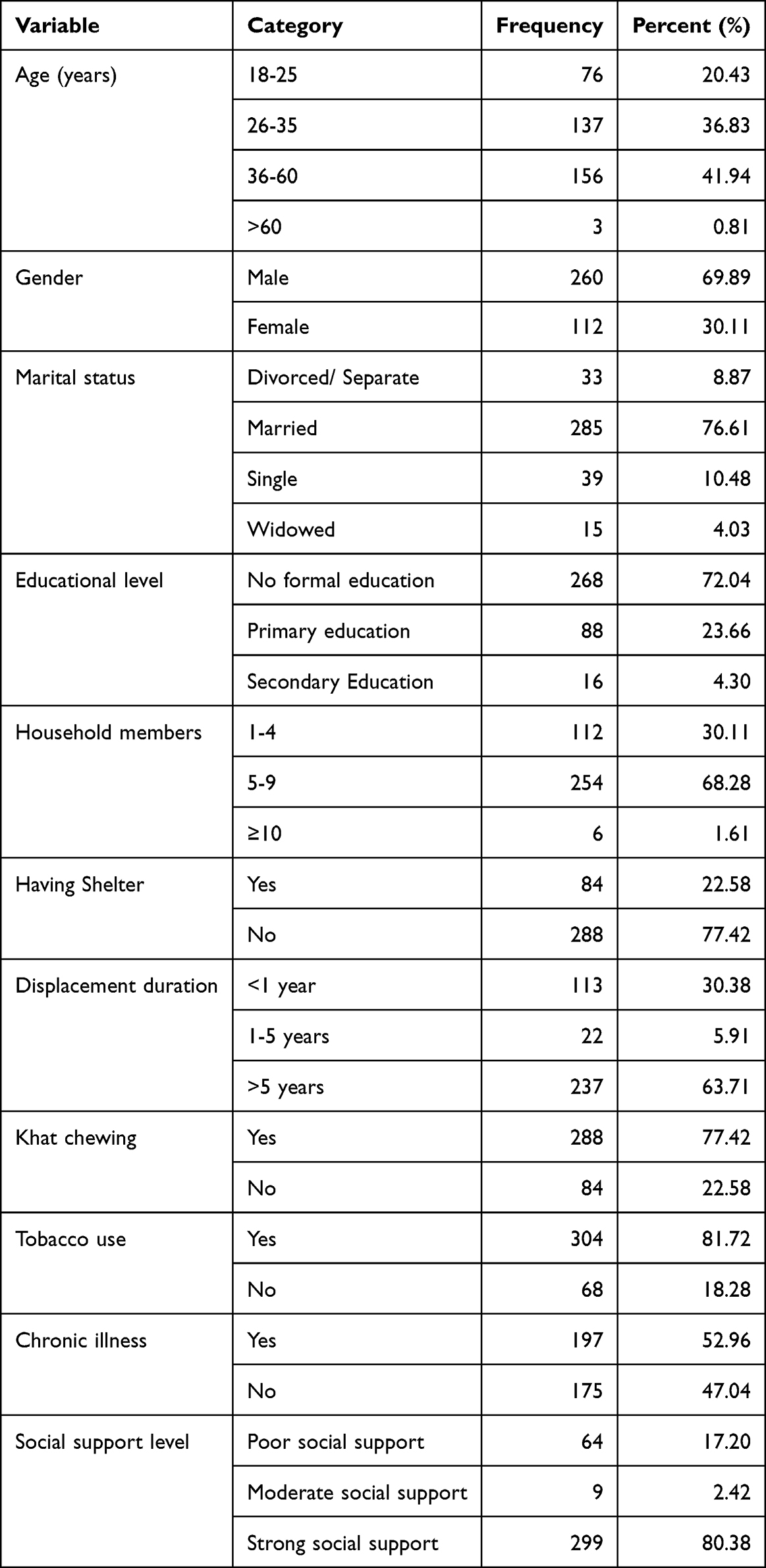 |
Table 1 Socio-Demographic Characteristics Among Internally Displaced Peoples in Burao City, Somaliland (n=372) |
Prevalence of Depression, Anxiety, and Post-Traumatic Stress Disorder
Among the 372 respondents, depression emerged as the most prevalent condition, reported by 236 individuals (63.4%). This was followed by anxiety, affecting 197 participants (53.0%), and post-traumatic stress disorder (PTSD), reported by 142 individuals (38.2%). These findings underscore a significant mental health burden among internally displaced persons in Burao, highlighting the necessity for targeted psychosocial support interventions (Figure 1).
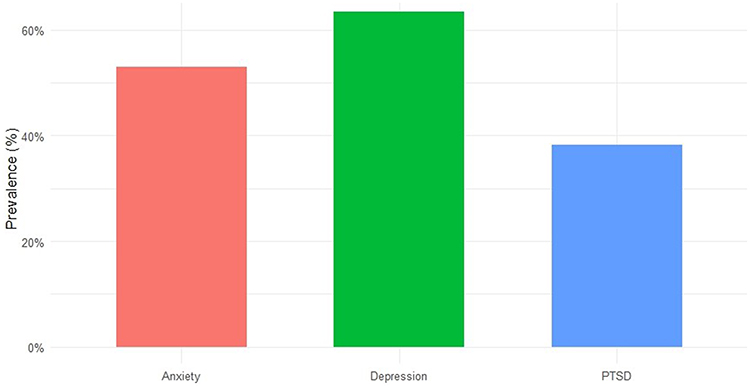 |
Figure 1 Prevalence of depression, anxiety, and post-traumatic stress disorder in IDPs Burao, Somaliland, 2025. |
Socio-Demographic Factors and Displacement Variables Associated with the Depression, Anxiety, and Post-Traumatic Stress Disorder
The bi-variate analysis revealed several sociodemographic and displacement-related factors significantly linked to depression, anxiety, and post-traumatic stress disorder (PTSD) among internally displaced persons (IDPs) in Burao, Somaliland. Gender showed a significant association with PTSD (p = 0.031). Among male participants, 170 (65.4%) screened positive for PTSD, while 90 (34.6%) did not. Conversely, among females, 60 (53.6%) did not have PTSD, whereas 52 (46.4%) did.
These findings suggest that male IDPs were more prone to PTSD than females, possibly due to greater exposure to traumatic events or differing coping mechanisms. Marital status was significantly associated with both depression (p = 0.040) and PTSD (p = 0.031). Among those who were divorced or separated, 21 (63.6%) reported symptoms of depression, compared to 12 (36.4%) who did not. Similarly, 23 (69.7%) of divorced/separated individuals screened positive for PTSD, versus 10 (30.3%) who did not. These results underscore a particularly vulnerable subgroup, as marital dissolution may lead to reduced social support, economic instability, and emotional distress, all contributing to poor mental health outcomes. Educational level was significantly associated with anxiety (p = 0.009). IDPs with no formal education had the highest prevalence of anxiety, with 147 (54.9%) screening positive and 121 (45.1%) screening negative. In contrast, individuals with secondary education exhibited markedly lower anxiety, with only 1 (7.7%) reporting anxiety symptoms and 12 (92.3%) without.
Duration of displacement was significantly associated with both depression (p = 0.018) and PTSD (p = 0.022). Among those displaced for less than one year, 77 (68.1%) experienced depression and 54 (46.2%) had PTSD. Conversely, among those displaced for more than five years, 151 (63.7%) had depression and 83 (35.0%) had PTSD. These findings imply that recent displacement is a critical period for mental health vulnerability, likely due to acute stressors such as loss of home, uncertainty, and lack of integration. Lastly, a significant association was found between chronic illness and depression (p = 0.003). Among individuals with chronic illness, 120 (60.9%) reported depression symptoms, compared to 116 (49.5%) among those without chronic illness (Table 2).
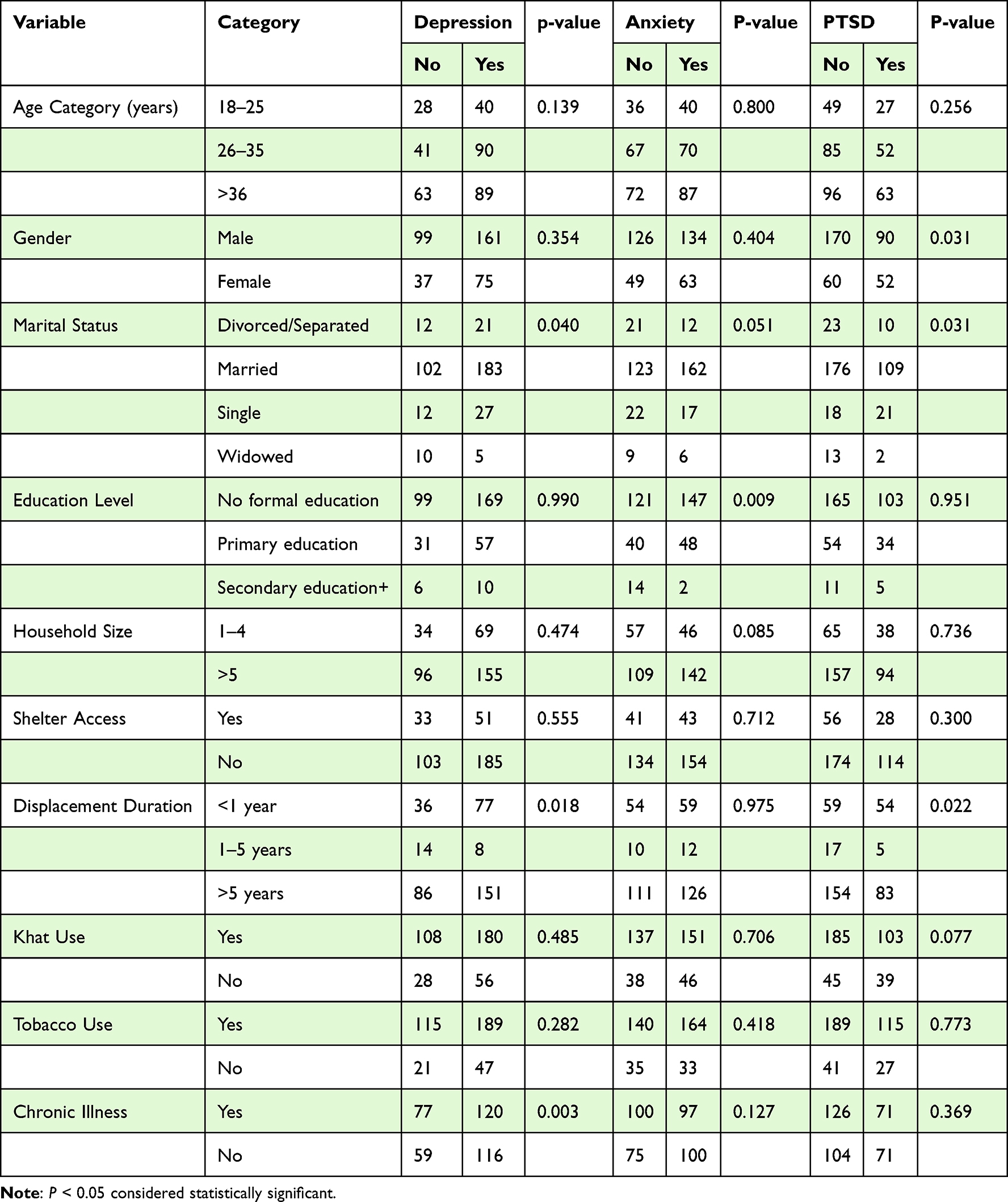 |
Table 2 Bi-Variate Analysis of Associated Factors of Depression, Anxiety, and PTSD IDPs in Burao, Somaliland 2025 |
Multi-Variable Analysis of Associated Variables of Depression, Anxiety, and Post-Traumatic Stress Disorder in IDPs in Burao, Somaliland
The multivariable logistic regression analysis revealed several statistically significant factors independently linked to depression, anxiety, and post-traumatic stress disorder (PTSD) among internally displaced persons (IDPs) in Burao, Somaliland. Age was notably associated with PTSD. Participants aged 26–35 had more than double the odds of developing PTSD compared to those aged 18–25 (OR = 2.41, SE = 0.97, 95% CI: 1.10–5.30, p = 0.029), while those aged 36–60 had over three times the odds (OR = 3.58, SE = 1.44, 95% CI: 1.62–7.89, p = 0.002).
Marital status was significantly associated with both anxiety and PTSD. Married individuals were more than three times as likely to report anxiety symptoms compared to those who were divorced or separated (OR = 3.38, SE = 1.55, 95% CI: 1.38–8.28, p = 0.008). Additionally, single participants had significantly higher odds of PTSD compared to the divorced/separated group (OR = 4.41, SE = 2.86, 95% CI: 1.24–15.75, p = 0.022), indicating that being unmarried may be a risk factor for PTSD, possibly due to reduced emotional or financial support systems. Education level was significantly protective against anxiety. Participants with secondary education had substantially lower odds of anxiety compared to those with no formal education (OR = 0.06, SE = 0.06, 95% CI: 0.01–0.47, p = 0.008).
Household size was also associated with anxiety. IDPs living in households with 5–9 members were nearly twice as likely to experience anxiety as those in smaller households of 1–4 members (OR = 1.89, SE = 0.51, 95% CI: 1.11–3.22, p = 0.019). Larger households may introduce additional stress due to overcrowding, limited resources, and caregiving burdens. The duration of displacement showed a protective effect against depression. Compared to those displaced for less than one year, individuals displaced for 1–5 years had significantly lower odds of depression (OR = 0.14, SE = 0.09, 95% CI: 0.04–0.47, p = 0.001) (Table 3).
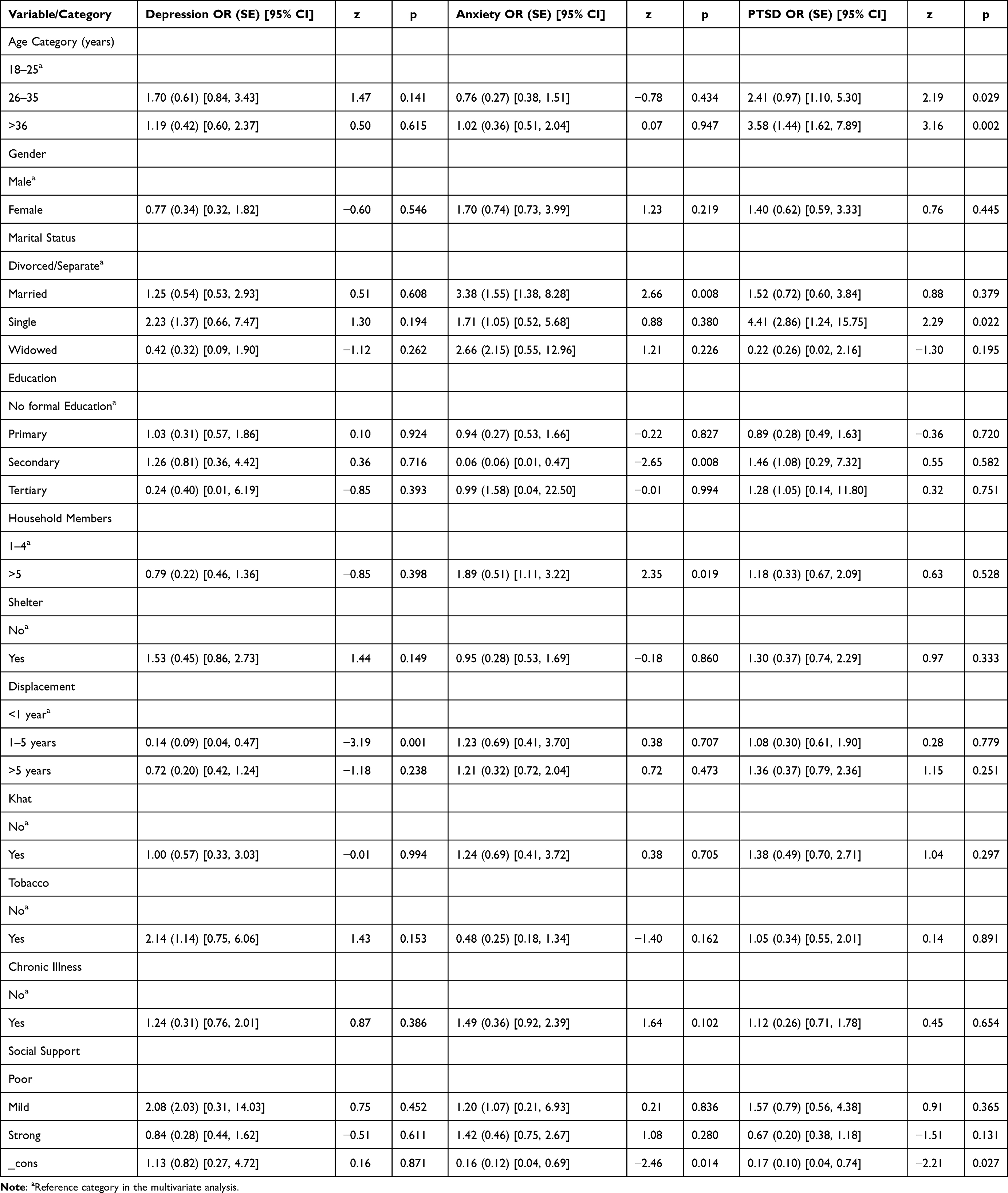 |
Table 3 Multivariable Analysis of Depression, Anxiety and PTSD and Associated Factors in IDPs Burao-Somaliland 2025 |
Discussion
This study revealed a substantial burden of Depression, Anxiety, and post-traumatic stress disorder (PTSD) among internally displaced persons (IDPs) in Burao, Somaliland, with prevalence rates for depression (63.4%), anxiety (53.0%), and post-traumatic stress disorder (PTSD) (38.2%) that surpass both global and regional averages for displaced and conflict-affected populations. Global WHO estimates suggest that approximately 22% of people living in conflict settings experience CMDs, with about 9% experiencing moderate to severe conditions.34 Our results are markedly higher, consistent with evidence from Somalia, Sudan, and Colombia, where protracted displacement, inadequate shelter, and poverty contribute to elevated CMD prevalence.30,35 These findings underscore the chronic and multifaceted stressors faced by IDPs in Somaliland, including prolonged insecurity, economic deprivation, and disrupted social networks.14,36
Age was a strong predictor of PTSD, with individuals aged 26–60 years having significantly higher odds compared to the youngest age group. This could be due to cumulative trauma exposure, repeated displacement, and increased caregiving and economic responsibilities over time.19 Studies from Georgia and South Sudan have similarly shown that middle-aged and older adults in IDP settings exhibit heightened PTSD risk due to both past trauma and ongoing socioeconomic stressors.36,37
Marital status was also a significant determinant, although the pattern differed from some previous findings. While prior studies in various conflict settings have found marriage to be protective against CMDs due to emotional and material support,13,38 our results indicate that married participants had higher odds of anxiety than those divorced/separated. This may reflect context-specific factors in Burao, where married individuals often face larger household sizes, more dependents, and heightened economic strain, all of which may exacerbate anxiety.39 Conversely, divorced/separated participants though possibly facing stigma may have fewer immediate caregiving burdens. Furthermore, single participants had higher odds of PTSD compared to divorced/separated individuals, likely due to the absence of partner-based emotional or financial support, which is critical for trauma coping in displacement contexts.13,39
Educational attainment showed a protective effect, with secondary education reducing anxiety odds by over 90%. Education can enhance coping capacity by improving problem-solving skills, health literacy, and access to information, as reported in other humanitarian settings.38 Larger household size (5–9 members) was linked to increased anxiety, possibly due to overcrowding, resource competition, and interpersonal tensions, which have been associated with poor mental health among displaced populations.13,17
Duration of displacement also played an important role. Those displaced for less than one year had higher odds of depression, consistent with the acute stress response model in the immediate aftermath of displacement.36 By contrast, displacement for 1–5 years was associated with lower depression odds, potentially reflecting partial adaptation through community integration and improved access to services.3,36 Chronic physical illness was positively associated with depression, consistent with literature showing strong bidirectional links between chronic disease and CMDs, especially in resource-limited humanitarian contexts.26
Limitations and Recommendations
This study acknowledges several limitations. The cross-sectional design restricts causal inference, thereby hindering the determination of the temporal relationship between displacement-related factors and Depression, Anxiety, and PTSD. The reliance on self-reported data introduces the potential for recall and social desirability biases. Although the screening tools employed (PC-PTSD-5, GAD-7, PHQ-9) have been extensively validated in similar low- and middle-income contexts, they have not undergone formal validation in Somaliland, which may impact diagnostic accuracy. Also, symptom overlap among the instruments could have resulted in an overestimation of comorbidity. Furthermore, the study was conducted exclusively in two IDP settlements in Burao, which may limit the generalizability of the findings to other displacement contexts within Somaliland.
Given the observed high prevalence and multifactorial determinants of Depression, Anxiety, and PTSD, it is recommended that humanitarian and governmental actors integrate comprehensive mental health and psychosocial support (MHPSS) into existing IDP assistance programs. Particular attention should be directed towards older adults, married individuals with significant caregiving responsibilities, and those recently displaced. Expanding educational opportunities for IDPs is also advised, as these may serve both economic and mental health protective functions. Further longitudinal research is warranted to explore the causal pathways linking displacement dynamics to mental health and to evaluate the effectiveness of targeted interventions in this context.
Conclusion
This study underscores the significant mental health challenges encountered by internally displaced persons (IDPs) in Burao, Somaliland, where there is a high prevalence of depression, anxiety, and post-traumatic stress disorder (PTSD). Key factors linked to these mental health conditions include age, marital status, education level, household size, duration of displacement, gender, and chronic illness. These findings highlight the urgent need for targeted, context-specific mental health interventions that consider sociodemographic vulnerabilities and the dynamics of displacement. Central to humanitarian response strategies in displacement settings should be the enhancement of psychosocial support, improved access to education and healthcare, and addressing the needs of recently displaced populations.
Abbreviations
AOR, Adjusted Odds Ratio; CI, Confidence Interval; CMD, Common Mental Disorders; DALYs, Disability Adjusted Life Years; DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; GAD-7, Generalized Anxiety Disorder-7; HIV, Human Immunodeficiency Virus; IDPs, Internally Displaced Persons; LMICs, Low- and Middle-Income Countries; PHQ-9, Patient Health Questionnaire-9; PTSD, Post-Traumatic Stress Disorder; YLDs, Years Lived with Disability.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available due to participant confidentiality and ethical considerations, but are available from the corresponding author upon reasonable request.
Ethical Approval and Consent to Participate
The study was approved by the Ethical Review Board of Alpha University Burao (AUCH/IRB/124/25) and was conducted under the Declaration of Helsinki. In addition, all participants provided their written informed consent to participate in this study.
Acknowledgment
Alpha University Burao (AUB). A preprint of this manuscript is available on Research Square: https://www.researchsquare.com/article/rs-6858475/v1.
Author Contributions
A.Y conceptualized and designed the study, collected and analyzed the data, interpreted the findings, and drafted and revised the manuscript. The author approved the final version of the manuscript and is accountable for all aspects of the work.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Cohen R. The guiding principles on internal displacement: an innovation in international standard setting. Glob Gov. 2004;10(4):459–480. doi:10.1163/19426720-01004006
2. Internal Displacement Monitoring Centre (IDMC) and, (NRC) NRC. Global report on internal displacement 2018. Geneva, Switzerland; 2018.
3. Siriwardhana C, Stewart R. Forced migration and mental health: prolonged internal displacement, return migration and resilience. Int Health. 2013;5(1):19–23. doi:10.1093/inthealth/ihs014
4. Virgincar A, Doherty S, Siriwardhana C. The impact of forced migration on the mental health of the elderly: a scoping review. Int Psychogeriatr. 2016;28(6):889–896. doi:10.1017/S1041610216000193
5. Burke MB, Miguel E, Satyanath S, Dykema JA, Lobell DB. Warming increases the risk of civil war in Africa. Proc Natl Acad Sci. 2009;106(49):20670–20674. doi:10.1073/pnas.0907998106
6. UNHCR. Handbook for the protection of internally displaced persons [Internet]. 2010. Available from: https://www.unhcr.org/4c2355229.pdf.
7. (IDMC) IDMC. Internal displacement in a changing climate [Internet]. 2022. Available from: https://www.internal-displacement.org/sites/default/files/publications/documents/grid2021_idmc.pdf.
8. And I, NRC. Adopting Somaliland’s draft policy framework on internal displacement. 2015.
9. Glendinning D, (the Regional Durable Solutions Secretariat – ReDSS – and the Somaliland Durable Solutions Consortium: World Vision, TASCO, NRC, DRC and CW. Somaliland durable solutions analysis: review of existing data and assessments to identify gaps and opportunities to inform (Re)integration planning and programming for displacement affected communities [Internet]. 2018. Available from: https://www.regionaldss.org/wp-content/uploads/2024/02/REDSS-SOMALILAND-REPORT-online.pdf.
10. Rawal NM, Pradhan M, Manandhar P, Adhikari SP, Amatya R, Khadka B. Prevalence of post-traumatic stress disorder and its associated factors among nepali army service members and veterans: 15 years post insurgency. Nepal Med Coll J. 2021;23(4):281–289. doi:10.3126/nmcj.v23i4.42208
11. Collaborators GBD 2019 MD. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet Psychiatry. 2022;9(2):137–150. doi:10.1016/S2215-0366(21)00395-3
12. Blanchet K, Ramesh A, Frison S, et al. Evidence on public health interventions in humanitarian crises. Lancet. 2017;390(10109):2287–2296. doi:10.1016/S0140-6736(16)30768-1
13. Porter M, Haslam N. Predisplacement and postdisplacement factors associated with mental health of refugees and internally displaced persons: a meta-analysis. JAMA. 2005;294(5):602–612. doi:10.1001/jama.294.5.602
14. De Jong JTVM, Komproe IH, Van Ommeren M. Common mental disorders in postconflict settings. Lancet. 2003;361(9375):2128–2130. doi:10.1016/S0140-6736(03)13692-6
15. Mahmood HN, Ibrahim H, Goessmann K, Ismail AA, Neuner F. Post-traumatic stress disorder and depression among Syrian refugees residing in the Kurdistan region of Iraq. Confl Health. 2019;13:1–11.
16. Richards A, Ospina-Duque J, Barrera-Valencia M, et al. Posttraumatic stress disorder, anxiety and depression symptoms, and psychosocial treatment needs in Colombians internally displaced by armed conflict: a mixed-method evaluation. Psychol Trauma Theory Res Pract Policy. 2011;3(4):384. doi:10.1037/a0022257
17. Steel JL, Dunlavy AC, Stillman J, Pape HC. Measuring depression and PTSD after trauma: common scales and checklists. Injury. 2011;42(3):288–300. doi:10.1016/j.injury.2010.11.045
18. Taha PH, Sijbrandij M. Gender differences in traumatic experiences, PTSD, and relevant symptoms among the iraqi internally displaced persons. Int J Environ Res Public Health. 2021;18(18):9779. doi:10.3390/ijerph18189779
19. Roberts B, Makhashvili N, Javakhishvili J, et al. Mental health care utilisation among internally displaced persons in Ukraine: results from a nation-wide survey. Epidemiol Psychiatr Sci. 2019;28(1):100–111. doi:10.1017/S2045796017000385
20. Charlson F, van Ommeren M, Flaxman A, Cornett J, Whiteford H, Saxena S. New WHO prevalence estimates of mental disorders in conflict settings: a systematic review and meta-analysis. Lancet. 2019;394(10194):240–248. doi:10.1016/S0140-6736(19)30934-1
21. Housen T, Lenglet A, Ariti C, et al. Prevalence of anxiety, depression and post-traumatic stress disorder in the Kashmir Valley. BMJ Glob Heal. 2017;2(4):e000419. doi:10.1136/bmjgh-2017-000419
22. Alpak G, Unal A, Bulbul F, et al. Post-traumatic stress disorder among Syrian refugees in Turkey: a cross-sectional study. Int J Psychiatry Clin Pract. 2015;19(1):45–50. doi:10.3109/13651501.2014.961930
23. World Health Organization. A situation analysis of mental health in Somalia. World Health Organization. 2010. Available from: http//applicationsemrowhoint/dsaf/EMROPUB_2010_EN_736pdf.
24. UNHCR. IDP definition. Emergency handbook. [Internet]. 2023. Available from: https://emergency.unhcr.org/search?search=IDPdefinition.
25. Agency ND and R. Multi-Sector IDPs needs assessment report [Internet]. 2021. Available from: https://ndra.govsomaliland.org/article/multisector-idps-needs-assessment?category=reports-8.
26. Salad AM, Malik SKMMR, Ndithia JM, Noor Z, Madeo M, Ibrahim M. Prevalence of mental disorders and psychological trauma among conflict-affected population in Somalia: a cross-sectional study. Front Public Health. 2023;11:1219992. doi:10.3389/fpubh.2023.1219992
27. Prins A, Bovin MJ, Smolenski DJ, et al. The primary care PTSD screen for DSM-5 (PC-PTSD-5): development and evaluation within a veteran primary care sample. J Gen Intern Med. 2016;31(10):1206–1211. doi:10.1007/s11606-016-3703-5
28. Bovin MJ, Kimerling R, Weathers FW, et al. Diagnostic accuracy and acceptability of the primary care posttraumatic stress disorder screen for the diagnostic and statistical manual of mental disorders among US veterans. JAMA Netw Open. 2021;4(2):e2036733–e2036733. doi:10.1001/jamanetworkopen.2020.36733
29. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
30. Plummer F, Manea L, Trepel D, McMillan D. Screening for anxiety disorders with the GAD-7 and GAD-2: a systematic review and diagnostic metaanalysis. Gen Hosp Psychiatry. 2016;39:24–31. doi:10.1016/j.genhosppsych.2015.11.005
31. Haas AD, Technau K, Pahad S, et al. Mental health, substance use and viral suppression in adolescents receiving ART at a paediatric HIV clinic in South Africa. J Int AIDS Soc. 2020;23(12):e25644. doi:10.1002/jia2.25644
32. Roehr B. American psychiatric association explains DSM-5. BMJ. 2013;346. doi:10.1136/bmj.f3591
33. Abiola T, Udofia O, Zakari M. Psychometric properties of the 3-item Oslo social support scale among clinical students of Bayero University Kano, Nigeria. Malaysian J Psychiatry. 2013;22(2):32–41.
34. Mohamed YA. Prevalence and correlates of common mental disorders among internally displaced adolescents and non-displaced adolescent students in Mogadishu, Somalia. 2019.
35. Neria Y, Nandi A, Galea S. Post-traumatic stress disorder following disasters: a systematic review. Psychol Med. 2008;38(4):467–480. doi:10.1017/S0033291707001353
36. Bogic M, Ajdukovic D, Bremner S, et al. Factors associated with mental disorders in long-settled war refugees: refugees from the former Yugoslavia in Germany, Italy and the UK. Br J Psychiatry. 2012;200(3):216–223. doi:10.1192/bjp.bp.110.084764
37. Roberts B, Damundu EY, Lomoro O, Sondorp E. Post-conflict mental health needs: a cross-sectional survey of trauma, depression and associated factors in Juba, Southern Sudan. BMC Psychiatry. 2009;9(1):1–10. doi:10.1186/1471-244X-9-7
38. Tol WA, Barbui C, Galappatti A, et al. Mental health and psychosocial support in humanitarian settings: linking practice and research. Lancet. 2011;378(9802):1581–1591. doi:10.1016/S0140-6736(11)61094-5
39. Miller KE, Rasmussen A. War exposure, daily stressors, and mental health in conflict and post-conflict settings: bridging the divide between trauma-focused and psychosocial frameworks. Soc Sci Med. 2010;70(1):7–16. doi:10.1016/j.socscimed.2009.09.029
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.