")
Back to Journals » Clinical Ophthalmology » Volume 16
Prevalence of Cystoid Macular Edema After Cataract Surgery in Eyes with Previous Macular Surgery
Authors Padidam S, Skopis G, Lai MM
Received 24 August 2021
Accepted for publication 26 January 2022
Published 16 February 2022 Volume 2022:16 Pages 423—427
DOI https://doi.org/10.2147/OPTH.S333754
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sneha Padidam,1,2 George Skopis,2 Michael M Lai1,2
1The Retina Group of Washington, Chevy Chase, MD, USA; 2Department of Ophthalmology, Medstar Washington Hospital Center, Washington, DC, USA
Correspondence: Michael M Lai, Tel +301-656-8100, Email [email protected]
Objective: To determine the prevalence and risk factors for cystoid macular edema (CME) after cataract surgery in eyes that have previously undergone macular surgery.
Study Design and Methods: Retrospective consecutive interventional case series. Patient medical records and Spectral Domain Optical Coherence Tomography (SD-OCT) were reviewed for eyes that underwent vitrectomy for full thickness macular hole (FTMH), lamellar macular hole (LMH) or epiretinal membrane (ERM) and subsequent cataract surgery at a large private retina practice between 2016 and 2018.
Results: Around 9.1% of eyes (22/243) developed CME post cataract surgery. The mean time from macular surgery to cataract surgery was 273 days (range: 87– 797) in eyes with CME and 289 days (range: 22– 897) in eyes without CME (p = 0.67). There was no difference in final visual acuity between eyes with CME (20/40, logMAR 0.312) and without CME (20/30, logMAR 0.206) (p = 0.101). Compared with patients with FTMH or LMH, patients with epiretinal membrane were more likely to develop post cataract CME (OR = 2.97, p = 0.031, Chi square test).
Conclusion: In eyes with history of macular surgery, the prevalence of post cataract surgery CME was around 9.1%. The development of CME is not dependent on timing of cataract surgery but is more common in eyes with history of epiretinal membrane.
Keywords: cystoid macular edema, macular hole, epiretinal membrane, pseudophakic cystoid macular edema
Background and Objective
Macular hole (MH) and epiretinal membrane (ERM) are common forms of retinal pathology that can significantly affect vision. Based on population studies, the prevalence of epiretinal membrane (ERM) is 9.1%1 and the prevalence of macular hole is 0.02–0.09%.2–4 Formation of cataract after vitrectomy surgery, including vitrectomy surgery for macular hole or epiretinal membrane, is common with over 80% of eyes developing cataracts at six months and nearly 100% of eyes developing cataracts at two years post vitrectomy.5 Cystoid macular edema (CME) after cataract surgery is a common complication with a reported incidence of 0.1–2.35%.6 Presence of various factors that disrupt the blood retinal barrier such as diabetes mellitus, uveitis, retinal vein occlusion and epiretinal membranes have been shown to contribute to increased rates of CME.6
Despite the high rates of cataract extraction after macular hole or epiretinal membrane repair, few studies have examined the rates and risk factors associated with pseudophakic CME in eyes with previous macular surgery.7–9 Additionally, these studies used larger gauge vitrectomy and did not consistently utilize spectral domain optical coherence tomography to assess for cystoid macular edema. The present study was conducted to assess the rates of pseudophakic CME in eyes that have previously undergone small-gauge vitrectomy for macular hole or epiretinal membrane repair. In addition, potential risk factors associated with subsequent pseudophakic CME were examined.
Study Design/Patients and Methods
A retrospective review of all patients who underwent macular surgery for lamellar macular hole (LMH), MH or ERM by 21 surgeons at the Retina Group of Washington between January 1, 2016 and December 31, 2018 followed by cataract surgery was performed. Institutional review board approval was obtained through the MedStar Washington Hospital Center affiliated with MedStar Georgetown University Hospital. All data were de-identified and collected in accordance with the Health Insurance Portability and Accountability Act (HIPAA) and the Declaration of Helsinki.
The electronic medical record of the Retina Group of Washington (Electronic Medical Assistant [EMA], Modernizing Medicine; Boca Raton, FL) was queried for patients who underwent pars plana vitrectomy for macular hole repair or epiretinal membrane repair in the designated time period. Patient medical records were reviewed to include only patients who underwent subsequent cataract extraction with intraocular lens implantation. Exclusion criteria were combined vitrectomy and cataract extraction, internal limiting membrane flap during macular hole surgery, and prior pathology including diabetic retinopathy, central retinal vein occlusion, branch retinal vein occlusion, uveitis, age-related macular degeneration, follow up of less than 3 months after cataract surgery, and history of retinal detachment repair. Either brilliant blue G stain or indocyanine green staining were used per physician preference during the macular surgery. Patients were referred to a cataract specialist when their cataract became visually significant as per patient symptoms and preference of the retina specialist. The cataract surgeries were completed by a fully trained cataract surgeon. The use of steroid eye drops and non-steroidal anti-inflammatory drops before and after cataract surgery was per the discretion of the cataract surgeon and these data were not included in the study.
All patient charts were reviewed for age, sex of the patients, gauge of vitrectomy surgery, visual acuity at time points prior to macular surgery, after macular surgery, prior to cataract surgery and after cataract surgery, days between vitrectomy surgery and cataract extraction and whether ILM was peeled at time of macular surgery. Optical coherence tomography (Zeiss Cirrus 5000, Carl Zeiss Meditec, Jena, Germany; Spectralis, Heidelberg Engineering, Heidelberg, Germany) images were reviewed at time points prior to macular surgery, prior to cataract surgery and after cataract surgery. The post macular surgery OCT was examined 2–3 months after macular surgery. The post cataract surgery OCT was examined 2–3 months after cataract when the patient returned to the retina office for follow-up.
CME was defined as cystic changes noted on spectral domain optical coherence tomography with an increase in central macular thickness (CMT) of at least 20 microns. Central macular thickness was measured from cross-sectional images using software to measure the distance between the inner and outer limiting boundaries of the retina.
The Department of Biostatistics at Georgetown University performed statistical analyses using SAS version 9.4 software (SAS Institute Inc., Cary, NC). Continuous variables were presented using mean and standard deviation, or using median and interquartile range (p25, p75) when variables are highly skewed. Comparison of mean of continuous variable between three groups is conducted using t test for variables with normal distribution and using Wilcoxon Rank sum test for non-normal variables. Comparison of proportions between groups is conducted using chi squared test. Logistic regression model is conducted for dichotomous outcome CME vs no CME.
Results
A total of 243 patients with a mean age of 65.5 met the inclusion and exclusion criteria for the study. 135 patients with epiretinal membrane (ERM), 96 patients with full thickness macular hole (FTMH) and 12 patients with lamellar macular hole (LMH) met criteria for inclusion. 241 of the 243 patients underwent 25 gauge PPV with the remaining 2 undergoing 23 gauge PPV. Baseline demographics of patients who developed CME and did not develop CME are shown in Table 1. The overall prevalence of patients with cystoid macular edema was 9.1% (n = 22). No macular hole reopening was observed. Two of the 22 patients with CME were treated with sub-tenon triamcinolone injections. Two patients with CME required intravitreal triamcinolone and intravitreal dexamethasone (Ozurdex, Allergan) injections. The other 18 patients with CME were treated with topical non-steroidal anti-inflammatory drops and corticosteroid drops.
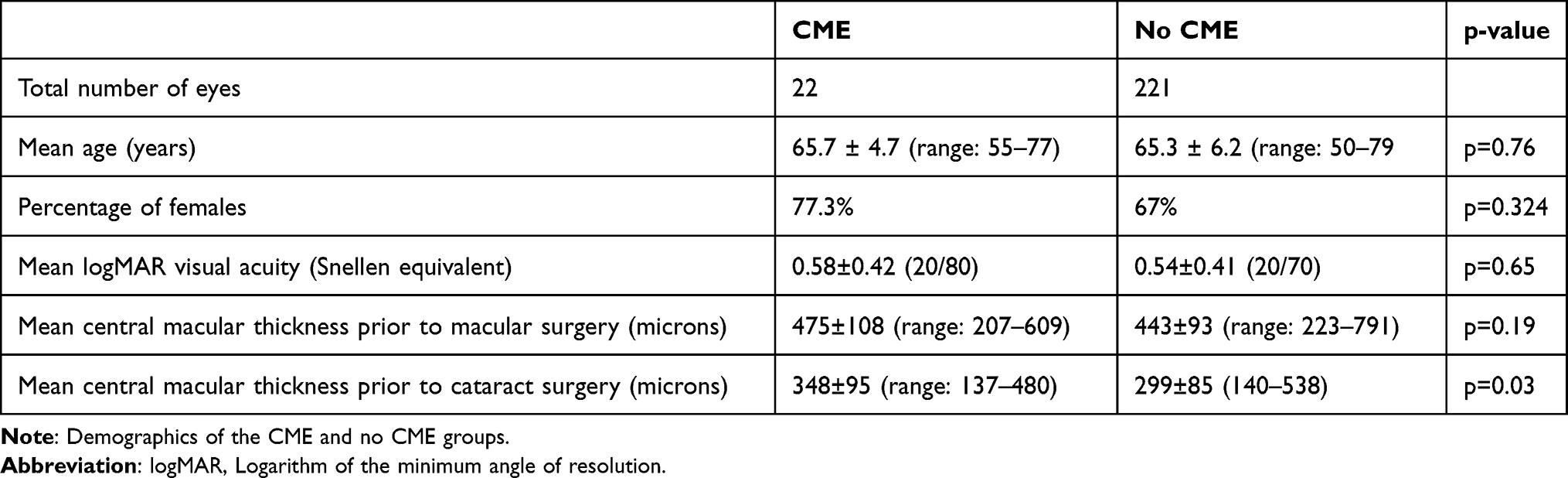 |
Table 1 Demographics |
The mean time from macular surgery was 273.1 ± 165 days (range: 87–797) in eyes with CME and 289.0 ± 158 days (range: 22–897) in eyes without CME (p = 0.67). The mean presenting central macular thickness (CMT) prior to macular surgery was 475±108 (range: 207–609) in patients with edema and 443±93 (range: 223–791) in patients without edema (p = 0.19). Mean CMT prior to cataract surgery in eyes with subsequent CME post cataract surgery was 348±93 (range: 137–480) microns compared with 299±85 (range: 140–538) microns in eyes without CME post cataract surgery (p = 0.03). The mean increase in CMT from prior to cataract surgery to after cataract surgery was 96 microns in eyes with CME and 4.0 microns in eyes without CME (p = 0.0001) (Table 2). Of note, the final visual acuity after cataract surgery, which was measured at most recent follow up after cataract surgery, was 20/40 (logarithm of the minimum angle of resolution (logMAR) 0.31±0.26) in eyes with CME and 20/30 (logMAR 0.20±0.23) in eyes without CME (p = 0.101).
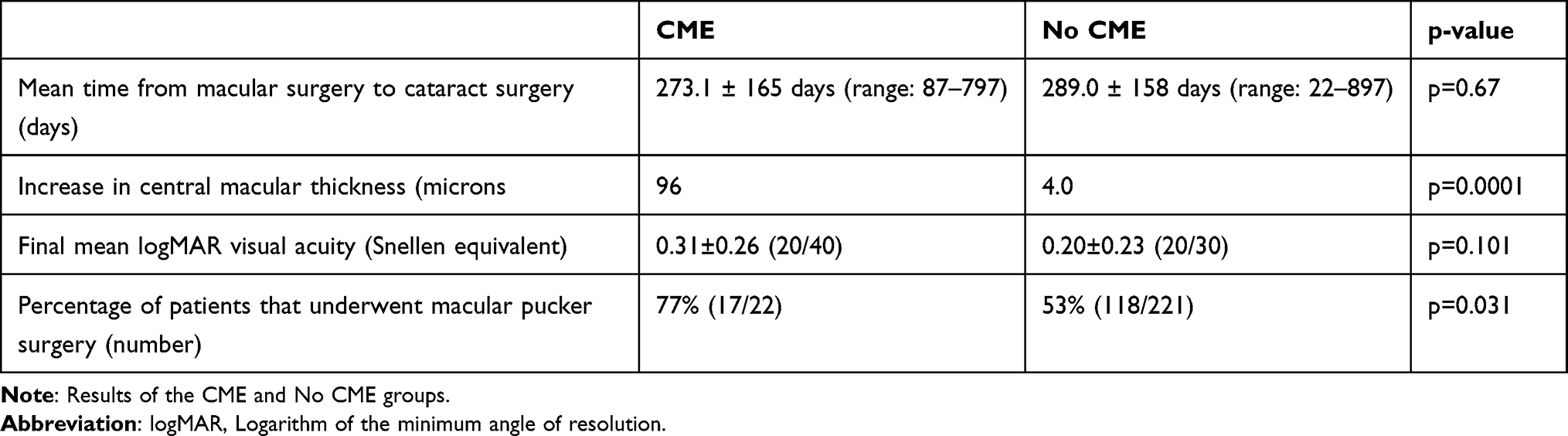 |
Table 2 Results |
Out of the 22 patients with CME, 17 patients (77%) had surgery for ERM and 5 had surgery for FTMH/LMH. Out of the 221 patients without CME, 118 had surgery for ERM (53%) and 103 had surgery for FTMH/LMH. Compared with patients with macular hole (FTMH or LMH), patients with ERM were more likely to develop post cataract surgery CME (odds ratio = 2.97, p = 0.031 (Chi square test)).
Using multivariate analysis, it was examined whether age, sex, time interval between macular surgery and cataract surgery were associated with the development of edema. None of these variables were found to be associated with the development of pseudophakic CME.
Discussion
This study analyzes the rate of CME after cataract surgery in patients who had previously undergone pars plana vitrectomy and membrane peel for macular hole or epiretinal membrane. Post cataract surgery CME was defined as the presence of cystic changes on SD-OCT and increase of 20 microns in CMT on SD-OCT. Our overall prevalence of CME in eyes that underwent cataract surgery after previous vitrectomy and ILM peel for macular hole and previous vitrectomy and membrane peel/ILM peel for ERM was 9.1%. Among eyes affected by CME, the mean increase in central macular thickness was 96 microns.
A search of the medical literature shows few previous studies that also reported the rates of pseudophakic CME in eyes with previous macular surgery. Bhatnagar et al. found a CME rate of 9.3% in 86 eyes that underwent cataract extraction after macular hole repair (Bhatnagar). In their study, CME was diagnosed when clinically noted on biomicroscopy and OCT was not utilized as it was in our study. Passenard et al. noted a CME rate of 9.4% in eyes that had undergone cataract extraction after macular hole repair.10 Of note, the earliest study by Haritglou et al. noted a 3.8% rate of CME in 52 patients who underwent cataract extraction after macular hole repair, but did not utilize OCT consistently as we did in our study.9 Unlike our study, all three studies utilized 20-gauge instrumentation and did not consistently utilize SD-OCT. Therefore, it is possible that those studies may have underestimated the prevalence of CME.
As for pseudophakic CME rates after ERM surgery, Dugas et al. found one case of persistent pseudophakic CME out of 65 eyes (1.5%) that previously underwent pars plana vitrectomy, membrane peel and ILM peel for epiretinal membrane.8 In this study, the diagnostic OCT was completed at 1-year post cataract surgery, and thus only persistent CME was reported. Mylonas et al. completed a prospective study evaluating eyes which underwent 23 gauge PPV/ILM peel followed by cataract surgery.11 SD-OCT was used to evaluate for cystic changes and central macular thickness one month after cataract surgery. They found that 5 out of 19 patients (26%) developed an increase in CMT of over 35 microns and cystic changes one month after cataract surgery. The higher rate of CME in patients undergoing surgery for epiretinal membrane is consistent with our finding that patients undergoing surgery for ERM are more likely to have CME after cataract surgery compared with patients that undergo surgery for MH followed by cataract surgery. In the current study, we found that eyes with history of ERM were almost 3 times more likely to develop pseudophakic CME compared with eyes with history of MH.
In our study, no MH reopening was observed even when pseudophakic CME occurred which is consistent with more recent studies in which ILM peeling was completed at the time of macular hole surgery.10 The study by Batnagar et al. reported a MH reopening rate of 19.8%.7 A closer examination of the study showed that only 62.8% of the eyes had the ILM removed at the time of MH repair, considerably lower than all other studies, including our present study. Removing ILM confers added protection against late MH reopening by preventing re-proliferation of preretinal membranes.
In addition to analyzing the rates of pseudophakic CME, our study also addressed the question of timing of cataract extraction after macular surgery. We found that the time interval between macular surgery and cataract surgery had no significant impact on the risk of pseudophakic CME. It has been well established that cataract formation is a major cause of decreased visual acuity after PPV and our study supports the idea that there is little benefit to prolonged periods of time between the two surgeries.
We additionally found that increased central macular thickness prior to cataract surgery increases the risk of CME. This appears to be a novel risk factor not described by previous studies. Eyes with ERM tend to exhibit higher CMT compared with eyes with macular hole post vitrectomy; therefore, it is possible that this observation may be related to our finding that eyes with history of ERM are at higher risk of developing pseudophakic CME compared with eyes with history of macular hole.
Limitations of our study include its retrospective nature. The timings of the post cataract surgery evaluation were dependent on the patient’s follow up schedule with our retina practice. The patients underwent cataract surgery by surgeons at different institutions and their follow up with our practice was not standardized. As the study was completed at a retina only practice, we did not have information regarding grade and type of cataract prior to the cataract surgery, ultrasound energy use during the cataract surgery, length of the cataract surgery or level of expertise of the cataract surgeon, all of which can affect the prevalence of CME. Additionally, their post cataract surgery eyedrop regimen including type and length of topical non-steroidal anti-inflammatory usage was similarly not standardized and may affect the finding of pseudophakic CME and their outcomes.
In conclusion, the prevalence of patients with CME after cataract surgery in eyes that have undergone epiretinal membrane and macular hole report is 9.1%. Cystoid macular edema develops more frequently in eyes that have undergone epiretinal membrane surgery compared with macular hole surgery. In our study, development of CME is not dependent on the timing of cataract surgery. Lastly, there was no statistically significant difference in final visual outcomes in eyes with and without CME. We believe these findings can help surgeons counsel patients regarding timing and outcomes of cataract surgeries following vitrectomies for macular pathologies.
Presentations
American Society of Retina Specialists Paper on Demand presentation virtual meeting July 2020.
The Retina Society presentation virtual meeting August 2020.
Funding
There is no funding to report.
Disclosure
No conflicting relationship exists for any author.
References
1. Xiao W, Chen X, Yan W, Zhu Z, He M. Prevalence and risk factors of epiretinal membranes: a systematic review and meta-analysis of population-based studies. BMJ Open. 2017;7(9):e014644. doi:10.1136/bmjopen-2016-014644
2. Rahmani B, Tielsch JM, Katz J, et al. The cause-specific prevalence of visual impairment in an urban population: the Baltimore Eye Survey. Ophthalmology. 1996;103:1721–1726. doi:10.1016/S0161-6420(96)30435-1
3. Wang S, Xu L, Jonas JB. Prevalence of full-thickness macular holes in urban and rural adult Chinese: the Beijing Eye Study. Am J Ophthalmol. 2006;141:589–591. doi:10.1016/j.ajo.2005.10.021
4. Sen P, Bhargava A, Vijaya L, George R. Prevalence of idiopathic macular hole in adult rural and urban south Indian population. Clin Experiment Ophthalmol. 2008;36:257–260. doi:10.1111/j.1442-9071.2008.01715.x
5. Cheng L, Azen SP, El-Bradey MH, et al. Duration of vitrectomy and postoperative cataract in the vitrectomy for macular hole study. Am J Ophthalmol. 2001;132(6):881–887. doi:10.1016/S0002-9394(01)01263-6
6. Henderson BA, Kim JY, Ament CS, et al. Clinical pseudophakic cystoid macular edema. Risk factors for development and duration after treatment. J Cataract Refract Surg. 2007;33(9):1550–1558. doi:10.1016/j.jcrs.2007.05.013
7. Bhatnager P, Kaiser PK, Smith SD, Meisler DM, Lewis H, Sears JE. Reopening of previously closed macular holes after cataract extraction. Am J Ophthalmol. 2007;144:252–259. doi:10.1016/j.ajo.2007.04.041
8. Dugas B, Ouled-Moussa R, LaFontaine P, et al. Idiopathic epiretinal macular membrane and cataract extraction: combined versus consecutive surgery. Am J Ophthalmol. 2010;149:302–306. doi:10.1016/j.ajo.2009.09.011
9. Haritoglou C, Gass CA, Schaumberger M, Ehrt O, Gandorfer A, Kampik A. Macular changes after peeling of internal limiting membrane in macular hole surgery. Am J Ophthalmol. 2001;132:363–368. doi:10.1016/S0002-9394(01)01093-5
10. Passemard M, Yakoubi Y, Muselier A, et al. Long-term outcome of idiopathic macular hole surgery. Am J Ophthalmol. 2010;149(1):120–126. doi:10.1016/j.ajo.2009.08.003
11. Mylonas G, Sacu S, Deak G, et al. Macular edema following cataract surgery in eyes with previous 23-gauge vitrectomy and peeling of the internal limiting membrane. Am J Ophthalmol. 2013;155:253–259. doi:10.1016/j.ajo.2012.07.013
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.