Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Prevalence of Chronic Obstructive Pulmonary Disease and Chronic Bronchitis Among Predominantly Smoking Workers in the Seafood Industry in Greenland
Authors Frederiksen AL, Laustsen BH ![]() , Bælum J
, Bælum J ![]() , Pedersen ML, Bønløkke JH
, Pedersen ML, Bønløkke JH ![]()
Received 12 November 2021
Accepted for publication 28 March 2022
Published 20 May 2022 Volume 2022:17 Pages 1167—1177
DOI https://doi.org/10.2147/COPD.S349106
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Anja Lærke Frederiksen,1 Birgitte Hamann Laustsen,2,3 Jesper Bælum,4 Michael Lynge Pedersen,1,3 Jakob Hjort Bønløkke5
1Steno Diabetes Center Greenland, Nuuk, Greenland; 2Department of Clinical Medicine, Faculty of Medicine, Danish Ramazzini Centre, Aalborg University, Aalborg, Denmark; 3Greenland Center for Health Research, Institute of Nursing and Health Science, University of Greenland, Nuuk, Greenland; 4Research Unit for General Practice, Department of Public Health, University of Southern Denmark, Odense, Denmark; 5Department of Occupational and Environmental Medicine, Danish Ramazzini Centre, Aalborg University Hospital, Aalborg, Denmark
Correspondence: Jakob Hjort Bønløkke, Department of Occupational and Environmental Medicine, Danish Ramazzini Centre, Aalborg University Hospital, Havrevangen 1, Aalborg, 9000, Denmark, Tel + 45 97664109, Email [email protected]
Introduction: For decades, the prevalence of smoking has been high in Greenland. Even so, the prevalence of chronic obstructive pulmonary disease (COPD), a smoking-related disease, remains largely unexplored. This cross-sectional study aimed to estimate the prevalence of COPD and chronic bronchitis (CB) among Inuit workers in the seafood industry in Greenland.
Methods: A total of 355 participants, 254 males and 101 females, met the inclusion criteria. Participants had a mean age of 38 years (standard deviation 13.5; range 17– 68 years). COPD was diagnosed based on post-bronchodilator ratio between forced expiratory volume within one second and forced vital capacity (FEV1/FVC) below the lower limit of normal (LLN) according to the Global Lung Function Initiative. Participants completed a questionnaire aiming to diagnose CB.
Results: The overall prevalence was 9.9% for COPD; 7.4% for CB. Participants were predominantly smokers; 73.2% active smokers, 91.8% active or former smokers. The prevalence of COPD was high, especially among those under 40 years of age. Both COPD and CB were associated with smoking status.
Discussion: This study among Greenlandic seafood workers found that smoking was a risk factor for COPD and CB among Greenlanders of Inuit origin. The high prevalence of COPD and the high prevalence of smoking underlines the importance of further initiatives to reduce smoking in Greenland.
Keywords: chronic obstructive pulmonary disease, chronic bronchitis, Greenland, Inuit, smoking, lung function
Plain Language Summary
Despite high smoking rates in Greenland, little is known about how common smoking-related diseases such as chronic obstructive pulmonary disease (COPD) or chronic bronchitis (CB) are in the country; neither in the general population nor in the working population. Official statistics on these diseases may underestimate how common the diseases are. Therefore, we studied these diseases among 355 seafood industry workers of Inuit origin in Greenland. Smoking rates were high with 92% ever smokers, and 73% active smokers. Among participants under 40 years of age, COPD was observed in 10%. Both COPD and CB were associated with smoking status. Our study underlines that smoking is a risk factor for COPD and CB among Greenlanders of Inuit origin. The study observed better lung function in Inuit than predicted from normal values for Caucasians. The lack of Inuit lung function reference values may contribute to the underestimation of COPD in Greenland. The study underlines the importance of further initiatives to obtain Inuit lung function reference values and to reduce smoking in Greenland.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by persistent and usually progressive airflow limitation associated with inflammation in the lungs.1 Demonstration of persistent airflow limitation by spirometry is required to make the diagnosis. A post-bronchodilator ratio between forced expiratory volume within one second and forced vital capacity (FEV1/FVC) below 70% confirms persistent airflow limitation according to the widely used definition of the Global Initiative for Chronic Obstructive Lung Disease (GOLD).2 This criterion may falsely lead to the diagnosis of COPD in some healthy elderly individuals and in specific ethnic groups. On the other hand, the GOLD criterion leads to an underestimation of COPD in persons aged below 40 years.3 Instead, persistent airflow limitation may be defined as FEV1/FVC ratio below the lower limit of normal (LLN) as proposed by the Global Lung Function Initiative (GLI2012) thereby obtaining a more realistic age corrected cut-off between normal and obstructive airflow.3 COPD is a life-threatening disease, which can lead to reduced activity, impaired quality of life and premature death. The global prevalence of COPD among adults aged 40 years or above has been estimated to 9–10%, mainly based on studies from Europe and North America.4 Worldwide, it is the third leading cause of death.5 Even so, COPD is probably widely underdiagnosed.6 In the Western world, the main risk factor for developing COPD is smoking. In- and outdoor air pollution and occupational exposures are additional risk factors for developing COPD and chronic bronchitis (CB). Furthermore, smoking is a main risk factor for developing CB, characterized by chronic cough and sputum production.7 Globally, the prevalence of CB varies widely, from 2.6% to 16% in population surveys, and it affects approximately one-third of patients with COPD. Furthermore, the presence of CB among smoking young adults increases the risk of developing COPD.2,8
COPD may be underdiagnosed in Greenland. A recent study from Greenland reported that 7.5% of the population were users of medicine targeting obstructive lung disease. Yet, less than a third of those had been tested with spirometry over the past two years, indicating low diagnostic activity and limited monitoring of COPD in Greenland.9
Lung function has been reported to be higher among Greenlanders and other Inuit living in the circumpolar area10 than among Europeans of the same gender, age, and height.11,12 Consequently, predicted FEV1 and FVC among Inuit is likely underestimated when using Caucasian standard references. On the other hand, the FEV1/FVC ratio has been found to be lower among Greenlanders than among Danes of similar gender, age and height.12 Therefore, the prevalence and severity of COPD among Greenlanders and other Inuit may be difficult to estimate from existing equations from other populations.
For decades, very high smoking rates among adults have been reported in Greenland; 68% in 1993 and 57% in 2014.13,14 A similar rate of 70% current smokers were found in our first analyses of workers employed in the Greenlandic seafood industry, the most important industry in Greenland employing around 15% of the workforce.15 Furthermore, in a school survey, 49% of teenagers at age 16 years reported being everyday smokers.16 Although a minor decrease has been observed in recent years, more than half (52%) of the adult population is currently everyday smokers.11 Thus, a high prevalence of smoking-related diseases, including COPD and CB, may potentially be expected among Greenlandic workers. Work in the seafood industry is known to increase the risk of asthma, whereas despite high levels of exposure to aerosols, COPD or CB has rarely been reported.17 However, the prevalence of COPD and CB in Greenland remains largely unexplored, and particularly so in subgroups of the population.
The aim of this study was to estimate the prevalence of COPD and CB among adult workers in the seafood industry.
Materials and Methods
Study Design
This was a cross-sectional study of Greenlandic workers in the seafood industry working in factories and trawlers in Nuuk, Ilulissat, Sisimiut and smaller settlements along the Western coastline of Greenland, described previously.15,18 Information was gathered from lung function tests and a health questionnaire offered as an interview in a study on the possible health risks of working in the fishing industry in Greenland conducted in 2016–2018 (see Supplementary Material). Bilingual Danish-Greenlandic medical students conducted the interviews. The study was approved by the Ethics Committee for Medical Research in Greenland (2015-11317), by the Regional Ethics Committee in the Central Denmark Region (1-16-02-475-16), and by the Danish Data Protection Agency. Written and oral, informed consent was obtained from each participant. The study was conducted in accordance with the Declaration of Helsinki. Participants with an abnormal lung function were encouraged to seek medical health care for further diagnosis and treatment.
Settings
Greenland is the largest island in the world covering around two million square kilometers. It is sparsely populated along the 4000 km coastline in 17 towns and approximately 60 settlements. The majority of the population is of Inuit origin.19 Greenlandic Inuit share a common ancestry with Inuit from Canada, Alaska and Russia.20 The population counts approximately 56,000 inhabitants. Among those, around 5700 were born outside of Greenland and later immigrated, mostly from Denmark.18,19
Since 1979, Greenland has had home-rule government, and since 2009 it has been self-ruled within the Danish Realm.21 In 1953, Greenland became a Danish county and a comprehensive strategy was initiated to develop the country towards a modern society and establish modern fishery in Greenland. Today, the seafood industry has grown enormously and is the primary source of export from Greenland.21
Study Population
The study included 355 Inuit workers from the seafood industry in Greenland (Figure 1), found in the working force of fishing, hunting and agriculture consisting of 4174 employees. Only workers reporting to be of Greenlandic ethnicity, thereby in this present study defined as Inuit, were included in this study. Workers from factories and trawlers were informed in oral form by the management prior to the visits and in this way invited to participate. Detailed information about the study and health examinations was given in oral and written form by researchers at the factories on the first day of the visits. All workers were encouraged to participate and attend while the research team was at the factories to disseminate information and conduct examinations. The researchers informed that participation was voluntary, invited to questions, and allowed for decisions on participation to be taken later, although for practical reason it had to be during the 1–5 day long visits to each facility. The management was not informed by the researchers about whether employees participated or not. All participants gave oral and written consent in Danish or Greenlandic based on the participants’ preference.
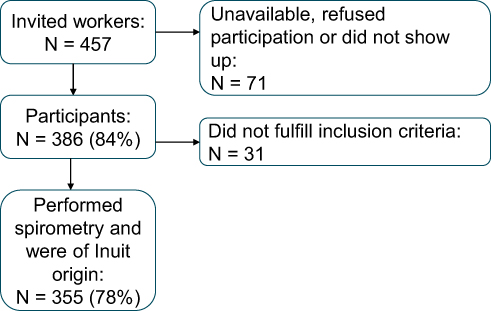 |
Figure 1 Flow diagram showing selection of the participants. |
The participants completed a questionnaire in either Greenlandic or Danish according to their preference, in which they stated their age, gender, ethnicity and history of smoking (see Supplementary Material). Furthermore, the questionnaire contained questions about airway symptoms including cough during the past 12 months, cough with mucus in the morning, cough with mucus production most mornings for at least three months in one year and, if affirmed, for how many years.
In addition, anthropometric measurements and a spirometry were performed. Weight and height were measured without shoes and wearing light indoor clothes. Spirometry was used to measure forced expiratory volume in the first second of expiration (FEV1) and forced vital capacity (FVC). If the ratio between FEV1 and FVC (FEV1/FVC) was 0.8 or lower, a post-bronchodilator test was performed by repeating spirometry 15 minutes after inhalation of 0.24 mg salbutamol. The test was deemed positive if FEV1 and/or FVC improved by 12% and at least 200 mL after inhalation of the β2-agonist. The calibration of the spirometer (Easy-One® NDD Medical Technologies, Zurich, Switzerland) was checked daily and set on processing measured values as Caucasian by GLI2012.3 The best FEV1 and the best FVC from each patient obtained either before or after inhalation of 0.24 mg salbutamol were included in the study.
Variables and Definition
Since no Inuit lung function reference is available, Caucasian reference values were used as recommended by Fenton et al.22 FEV1 and FVC as % of predicted reference values (FEV1%; FVC%) were calculated.
Participants were considered to have COPD if both the pre- and post-bronchodilator FEV1/FVC were lower than the reference LLN of FEV1/FVC using the GLI2012 standard. Participants with a positive post-bronchodilator test (ie, suggestive of asthma) were excluded from the COPD group in a sensitivity analysis. Similarly, a sensitivity test was performed with participants reporting asthma-like symptoms as defined in a previous publication.23 Participants were considered to have CB if they reported cough and sputum production for at least three months for a minimum of two consecutive years.24 Participants were categorized as active smokers if they reported current daily smoking, as former smokers if they reported having quit smoking and still did not smoke (no matter the length of abstinence), and non-smokers if they had never smoked daily.
Statistics
The prevalence of COPD, CB and the combined prevalence was calculated with 95% confidence intervals (95% CI) for males and females alike. Normally distributed variables were described using mean values and standard deviations. Check for normality was done by QQ-plot. Means were compared using the two-sided Student’s t-test for independent samples. Proportions were compared using Fisher’s exact test. Logistic regression was used to study the association between COPD or CB and smoking, age group and gender. Linear regression was used to study the association between FEV1% and age. Two-tailed tests were performed and a p-value below 0.05 was considered significant. Statistical analyses were performed using SPSS statistical software, version 25.0 (IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.).
Results
Among 457 invited workers, 386 participated in the study, 69 from trawlers and 317 from factories, yielding a participation rate of 84.5%. Among those, 355 (254 males and 101 females) met the Inuit criteria and had a spirometry done (Figure 1). Participants had a mean age of 38 years (SD 13.5; range 17–68 years). Basic characteristics are illustrated in Table 1. Males were taller, heavier, and had a higher FEV1 and FVC than females. However, the females had a higher BMI than the males. The mean age of smoking debut was approximately 15 years. More than two-thirds (73.2%) of the participants were active smokers and 91.2% (323/354) were active or former smokers with no difference observed between genders.
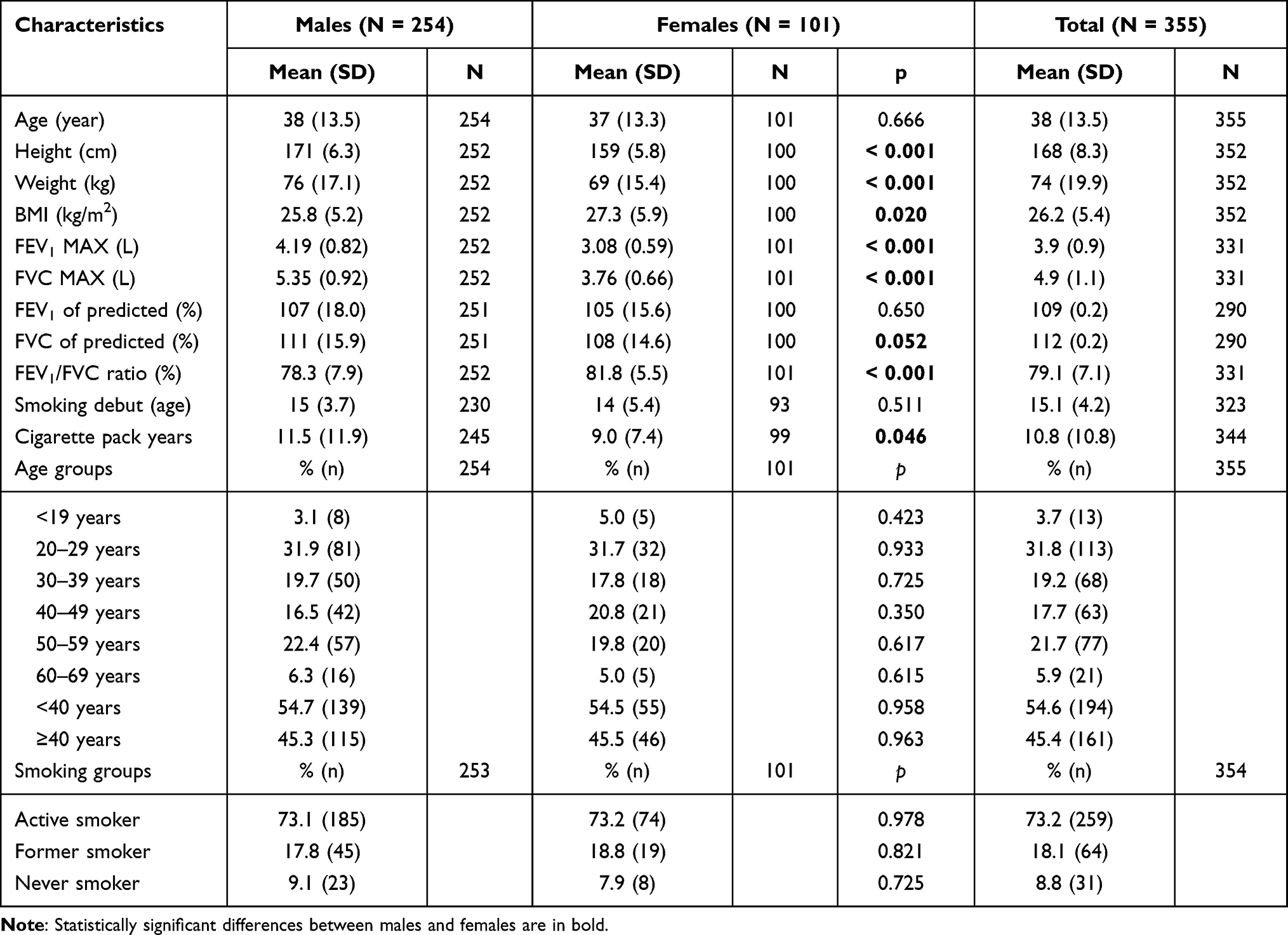 |
Table 1 Basic Characteristics of Greenlandic Workers from the Greenlandic Fishing Industry Included in the Study |
The mean FEV1% and FVC% were above average Caucasian reference values for both genders; 107% and 111% for males and 106% and 108% for females, respectively. The FEV1% was negatively associated with increasing age for both males (β = −0.032, p < 0.001) and females (β = −0.024, p < 0.001).
The prevalence of COPD was 9.9% (Table 2). The prevalence among males (11.9%) did not differ significantly from among females (5.0%) (p = 0.051). The prevalence of COPD among those <40 years (10.9%) was not significantly higher than among those >40 years (8.9%). The prevalence of CB was 7.4% with no gender difference observed; 8.4% among males and 5.5% among females (p = 0.368), whereas the prevalence was higher, 11.8% among those >40 years compared with 3.7% among those <40 years (p = 0.04).
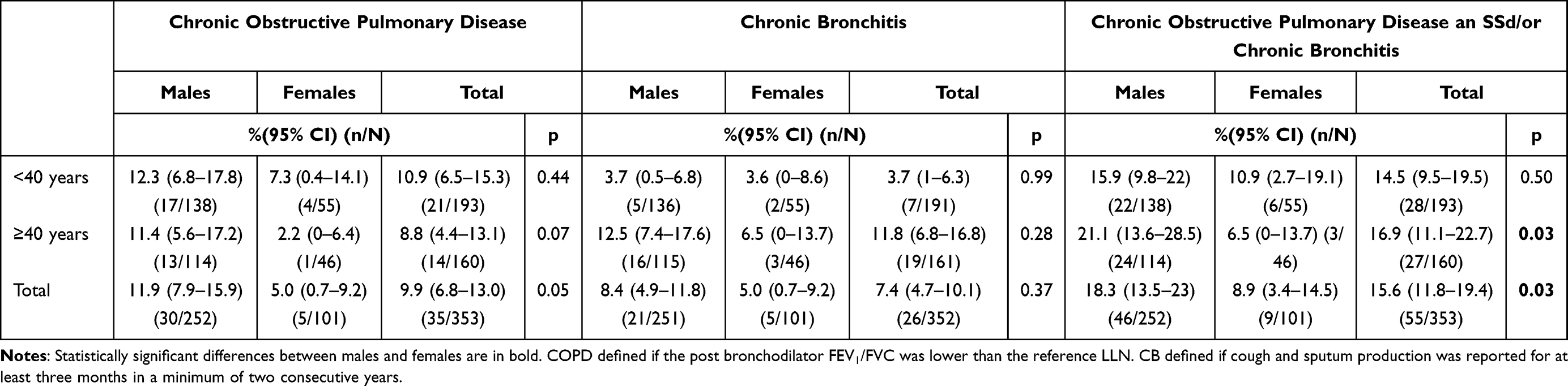 |
Table 2 Prevalence of Chronic Obstructive Pulmonary Disease and Chronic Bronchitis by Age and Gender Group Among Greenlandic Workers in the Greenlandic Fishing Industry |
Six participants were classified with both COPD and CB. Thus, among 34 participants with COPD 17.6% (6/34) also had CB. Among 26 participants with CB 23.1% also had COPD (6/26).
COPD was associated with ever smoking (odds ratio (OR) = 2.8 (95% CI: 1.1–7.2) p = 0.030) (Table 3). This association remained significant after adjusting for age and gender (OR = 2.8 (95% CI: 1.1–7.1) p = 0.031). Furthermore, CB was associated with ever smoking (OR = 2.9 (95% CI: 1.4–6.4) p = 0.006 compared with non-smokers) and increasing age (OR = 1.026 (95% CI: 1.004–1.049) p = 0.003). The association between CB and smoking remained significant after adjusting for age and gender (OR = 3.3 (95% CI: 1.5–7.3) p = 0.004).
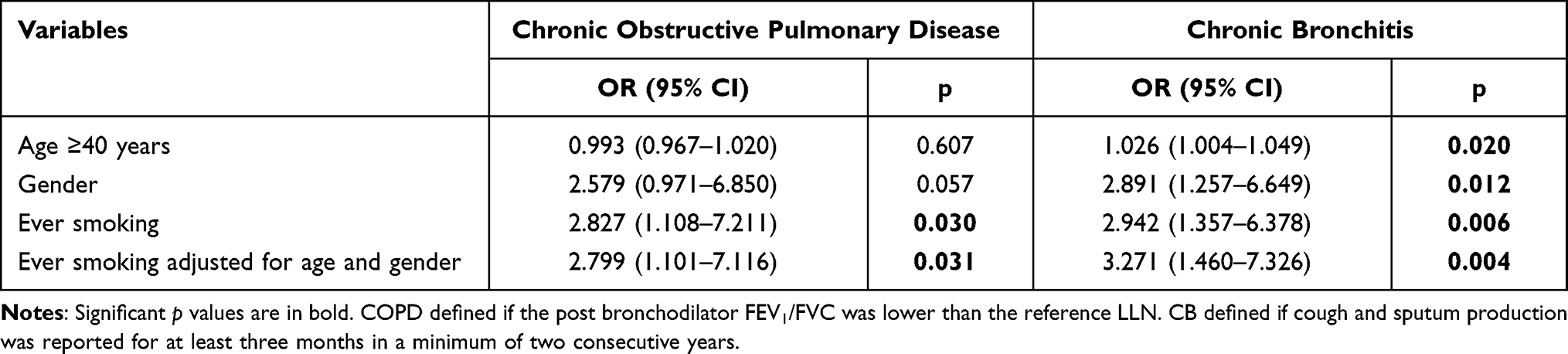 |
Table 3 Associations Between Ever Smoking, Age, Gender and Chronic Obstructive Pulmonary Disease or Chronic Bronchitis Among Greenlandic Workers in the Greenlandic Fishing Industry |
In sensitivity analyses, all participants with a positive bronchodilator test (N = 8) were excluded from the COPD group. Results were essentially similar, revealing that the association of COPD with smoking remained statistically significant and showing non-significant trends toward higher COPD prevalences among those <40 years and among males (data not shown). When excluding all participants who evoked symptoms suggestive of asthma from being diagnosed with COPD, the prevalence of COPD decreased to 6.3% (males: 8.3%; females 3.8%) still without statistically significant differences in prevalence related to sex or age group (data not shown). This caused the associations with smoking (Table 3) to become nonsignficant (p > 0.1). When applying the GOLD standard criteria for airflow limitation of a FEV1/FVC ratio of 0.7, the no. of participants defined as having COPD changed a little from N = 35 to N = 34.
Discussion
The overall prevalence was 9.9% for COPD and 7.4% for CB. Surprisingly, we found no increase in the prevalence of COPD related to age, whereas CB was markedly higher in the age group ≥40 years (11.8%) than in the group <40 years (3.7%). The participants were predominantly smokers, with 91.2% classified as either current smokers or former smokers and with 73.2% current smokers. Both COPD and CB were associated with smoking, also when adjusted for age and gender. This underlines that smoking is also a risk factor for COPD and CB among Greenlanders of Inuit origin.25
Strengths and Limitations
This is the first study to describe the prevalence of COPD based on post-bronchodilator spirometry in a working Greenlandic population and to document a high prevalence of COPD in Greenland. The participation rate was high as almost every worker present in the factories on the examination day was included in the study. Those who did not show up for examination may potentially be those with either the poorest health or social status or those who took the day off for other activities. Because of the high participation ratio, we do not believe that selection bias severely affects the results of the study regardless of the reason for not being at the factories on the examination day. Language barriers were minimized by letting Danish-Greenlandic medical students conduct the clinical interviews. The study population consisted of employed workers and was not a fully representative section of the Greenlandic population. Even so, 8.5% (355/4174) of the working force employed in the fishing, hunting and agriculture industry was represented in this study. In total, the study participants comprise 1.5% (355/23,217) of the total number of employed Greenlanders in 2017.21 The proportion of males in this study, 71.5%, was considerably higher than the 52.8% males in the general population.21 Furthermore, the percentage of smokers in this study was considerably higher than the percentage of smokers in the general population; 73.2% compared with 52% of everyday smokers nationwide.11 Considering how our population differed from the general population, including the high risk of a HWE, our results cannot be used to predict the prevalence of COPD and CB in the general population. However, the study gives an indication of a high prevalence of COPD among active Greenlandic smokers that has not previously been well described. Furthermore, the prevalence of CB should be interpreted with some caution since the diagnosis is based on self-reported symptoms. Yet, the diagnosis is based on symptoms and cannot be measured otherwise.
Prevalence of COPD and CB
The prevalence of COPD among participants working in the seafood industry younger than 40 years was high (10.9%). This is much higher than the estimate from the European Community Respiratory Health Survey that 2.4% of the general European population aged 20–44 years were classified as having COPD.26 The prevalence of COPD among participants aged 40 years or more (8.8%) was slightly lower than among the younger participants. A global estimate of COPD for this age group of approximately 10% was published in a comprehensive systematic review from 2006.4 In any case, direct comparisons with general population studies may not be relevant because our study was conducted in a population of workers rather than in the general Greenlandic population. The LLN (GLI2012) definition of COPD yields more reliable estimates of COPD prevalence than does the fixed FEV1/FVC ratio of the GOLD definition of COPD that tends to underestimate prevalences in younger and overestimate prevalences in older age groups. However, use of the LLN definition requires the use of LLN values calculated from the ethnic group under study, which is impossible for Inuit for whom GLI reference values do not exist. The present study indicates that the COPD prevalence among active Greenlandic workers may be high compared with that of other countries given the age of our study participants.11,12 This is in line with a very high smoking prevalence both in young adults and in the main population in Greenland (52%) compared with 23% of the adult population in Denmark in 2018.27 The prevalence of heavy smoking is also higher among younger than older Greenlanders.11
Our results may be attenuated by a Healthy Worker Effect (HWE). Working in the seafood industry is physically demanding and it involves exposure to airway and skin irritants. In such jobs, a tendency exists for workers with symptoms and health problems to leave the industry and find less strenuous jobs causing the remaining workers at the workplace to have less disease and symptoms.28 Because the study had a cross-sectional design, we could not quantify to what extent a HWE caused the participating workers to be healthier than the general population. A HWE could explain the lack of an association between COPD prevalence and age if workers with poorer lung health left the industry before reaching a high age.
In our study, COPD was not significantly associated with male gender and age. However, a statistically higher prevalence of COPD among males may have been missed because of the small size of the study and the resulting high risk of type 2 error in the data. This runs contrary to other studies, such as the PLATINO study, which showed a consistent pattern of a higher prevalence of COPD among males than among females.29 This may, in part, be so because the LLN of FEV1/FVC reference is specific to gender and age. As to the lack of association with gender, this may also be a result of a higher smoking prevalence among females (73.2%) than seen among females in other parts of the world. In comparison, Mazurek et al found that 17.3% and 12.9% of American working females in the reproductive age in 2009–2013 were current and former cigarette smokers, respectively.30
The prevalence of CB among our participants was 7.4%, which is in the range of a globally estimated prevalence of 1.4–15.9% according to a comprehensive review.4 In line with our findings, older age and current smoking are factors associated with CB globally.7 CB among participants with COPD showed a prevalence of 21.6% (8/37) in accordance with a very wide range (7.4–53%) reported globally.7
The high prevalence of COPD and CB observed in the present study is in line with the increasing prevalence of other smoking-related diseases in Greenland.13,28,31 Thus, the incidence of lung cancer rose by 23% from 1973 to 1997, where the emergence of westernization, including assimilating of smoking appeared.32 Lung cancer is the most common cancer in Greenland and it is related to 34% of all cancer deaths in the 2000–2014 period.33
Lung Function Among Greenlanders
The mean FEV1 and FVC measured in the participants were above average Caucasian reference values for both genders; FEV1 109% and FVC 112%. At 0.79 the mean FEV1/FVC ratio was slightly lower than the predicted ratio based on equations for Caucasians of 0.82. This is in line with former studies suggesting that Inuit have a higher lung capacity, especially regarding FVC, than Caucasians of the same gender, height and age.11,12
A negative association between FEV1 as a percentage of the predicted value and age was observed, indicating an accelerated decline in lung function with age within the studied population. This can most likely be explained by the extremely high prevalence of smokers and former smokers. However, because reference values for lung function do not exist for this ethnic group, we cannot completely rule out that FEV1 declines more rapidly among Inuit than among Caucasians.
Smoking
We found a high prevalence of smokers. The participants had a smoking rate above the current smoking rate reported in a population survey from 2018, 73.2% versus 52%.11 On the other hand, an even higher smoking rate was seen among unemployed Greenlanders, 82%.34
Smoking cessation is the only intervention shown to slow the decline of lung function.6,35 Smoking cessation was recently found to improve FEV1% predicted by 7 percentage points.36 Several initiatives have been taken to reduce smoking in Greenland. In 2004, a much tighter smoking policy was introduced by law, including non-smoking in public buildings, means of transportation and institutions. In 2010,37 this legislation was further tightened, and in 2017, a blueprint for prevention of smoking was launched.38
Still, the prevalence of smokers in Greenland remains high11 and the high prevalence among young adults is particularly disturbing.16 The high prevalence of COPD and CB related to smoking underlines the importance of introducing further initiatives to reduce smoking in Greenland.
Conclusions
This study found that the prevalence of COPD and CB was high in a relatively young cohort of Greenlandic Inuit workers in the seafood industry. The high prevalence of these diseases was related to a high smoking prevalence. The high prevalence of COPD, CB and smoking underlines the importance of introducing further initiatives to reduce smoking in Greenland.
Despite the high prevalence of both smoking and COPD, the participants seemed to have high lung function values, confirming a higher FEV1 and FVC in Inuit than in Caucasians. On the other hand, an accelerated deterioration in FEV1 with age suggested a considerable sensitivity to smoking. Inuit lung function reference values should be developed to facilitate investigation of the prevalence of COPD and CB in the general Greenlandic population.
Abbreviations
CB, chronic bronchitis; CI, confidence interval; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume within one second; FVC, forced vital capacity; GLI, Global Lung Function Initiative; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HWE, healthy worker effect; LLN, lower limit of normal; OR, Odds ratio; QQ-plot, quantile–quantile plot.
Data Sharing Statement
The authors agree to share data upon reasonable request to the extent that this does not violate personal data protection rights.
Funding
The study was funded by the Greenlandic Occupational Health Award, the Occupational Health Service in Greenland, the Greenlandic Workers Union, the Greenlandic Employers Association, Royal Greenland, Polar Seafood, Bank of Greenland and the Danish Working Environment Research Fund and by grant NNF20SA0064190 from the Novo Nordisk Foundation. The sponsors had no role in the study design, data collection, analysis or interpretation of data, nor in the writing of the report or in the decision to submit the article for publication.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Vestbo J. COPD: Definition and Phenotypes. Clin Chest Med. 2014;35(1):1–6. doi:10.1016/j.ccm.2013.10.010
2. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2019 Report); 2018. Available from: https://goldcopd.org/wp-content/uploads/2018/11/GOLD-2019-v1.7-FINAL-14Nov2018-WMS.pdf.
3. Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: the global lung function 2012 equations. Eur Respir J. 2012;40(6):1324–1343. doi:10.1183/09031936.00080312
4. Halbert RJ, Natoli JL, Gano A, Badamgarav E, Buist AS, Mannino DM. Global burden of COPD: systematic review and meta-analysis. Eur Respir J. 2006;28(3):523–532. doi:10.1183/09031936.06.00124605
5. World Health Organization. Chronic obstructive pulmonary disease factsheet. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-%28copd%29.
6. Pauwels RA, Rabe KF. Burden and clinical features of chronic obstructive pulmonary disease (COPD). Lancet. 2004;364(9434):613–620. doi:10.1016/S0140-6736(04)16855-4
7. Mejza F, Gnatiuc L, Buist AS, et al. Prevalence and burden of chronic bronchitis symptoms: results from the BOLD study. Eur Respir J. 2017;50(5):1700621. doi:10.1183/13993003.00621-2017
8. Guerra S, Sherrill DL, Venker C, Ceccato CM, Halonen M, Martinez FD. Chronic bronchitis before age 50 years predicts incident airflow limitation and mortality risk. Thorax. 2009;64(10):894–900. doi:10.1136/thx.2008.110619
9. Lauridsen MV, Backe MB, Bonefeld-Jørgensen EC, Skovgaard N, Pedersen ML. Prevalence and quality of care among patients using medication targeting obstructive lung disease: a cross-sectional study in the five regions of Greenland. Int J Circumpolar Health. 2021;80(1). doi:10.1080/22423982.2021.1948244
10. Rode A, Shephard RJ. Pulmonary function of Canadian Eskimos. Scand J Respir Dis. 1973;54(4):191–205.
11. Larsen CVL, Hansen CB, Ingemann C, et al. Befolkningsundersøgelsen i Grønland 2018 - Levevilkår, Livsstil Og Helbred. [The Population Health Survey in Greenland 2018 - Living Conditions, Lifestyle and Health]. Statens Institut for Folkesundhed, SDU; 2019. [National Institute of Public Health, SDU; 2019] Danish.
12. Krause TG, Pedersen BV, Thomsen SF, et al. Lung function in Greenlandic and Danish children and adolescents. Respir Med. 2005;99(3):363–371. pm: 15733513. doi:10.1016/j.rmed.2004.07.016
13. Dahl-Pedersen IK, Larsen CVL, Nielsen NO, Jørgensen ME, Bjerregaard P. Befolkningsundersøgelsen i Grønland 2014 - Levevilkår, Livsstil og Helbred. Statens Institut for Folkesundhed; 2016. [Population Health Survey in Greenland 2014 - Living Conditions, Lifestyle and Health. National Institute of Public Health; 2016]. Danish.
14. Bjerregaard P, Curtis T, Senderovitz F, Christensen U, Pars T. Levevilkår, Livsstil og Helbred i Grønland; 1995. [Living Conditions, Lifestyle and Health in Greenland; 1995]. Available from: https://www.sdu.dk/sif/-/media/images/sif/udgivelser/2005/groenland/levevilkaar_livsstil_og_helbred_i_groenland.pdf.
15. Laustsen BH, Omland Ø, Würtz ET, et al. Rhino conjunctivitis and asthma among seafood processing workers in Greenland. A cross-sectional study. Front Allergy. 2021;2(October):1–12. doi:10.3389/falgy.2021.747011
16. Niclasen B. Trivsel og sundhed blandt folkeskoleelever i Grønland: resultater fra skolebørnsundersøgelsen HBSC Greenland i 2014; 2015. [Well-being and health among primary school pupils in Greenland: results from the HBSC (Health Behaviour in School-aged Children) survey in Greenland in 2014; 2015]. Available from: https://www.sdu.dk/sif/-/media/images/sif/udgivelser/2005/groenland/trivsel_og_sundhed_blamdt_folkeskolelever_i_groenland_2014.pdf.
17. Bonlokke JH, Bang B, Aasmoe L, et al. Exposures and health effects of bioaerosols in seafood processing workers - a position statement. J Agromedicine. 2019;24(4):441–448. doi:10.1080/1059924X.2019.1646685
18. Laustsen BH, Ebbehøj NE, Sigsgaard T, Rasmussen K, Bønløkke JH. Work environment, occupational diseases and accidents among seafood industry workers in Greenland. Dan Med J. 2022;69(2):A05210470.
19. Statistics Greenland. Greenland in figures 2018; 2018. Available from: https://stat.gl/publ/da/GF/2018/pdf/GreenlandinFigures2018.pdf.
20. Bjerregaard P, Young TK. The Circumpolar Inuit. Health of a Population in Transition. Munksgaard; 1998.
21. Statistics Greenland. Available from: http://www.stat.gl/default.asp?lang=en.
22. Fenton ME, Graham BL, Stanojevic S, Whitford L, Ironstand L. Interpretation of spirometry in Saskatchewan first nations adults. Ann Am Thorac Soc. 2018;15(10):1237–1239. doi:10.1513/AnnalsATS.201711-909RL
23. Laustsen BH, Omland Ø, Würtz ET, Jørgensen L, Bønløkke JH. Serum selenium levels and asthma among seafood processing workers in Greenland. Int J Circumpolar Health. 2021;80(1):1–9. doi:10.1080/22423982.2021.1972525
24. Medical Research Council. Definition and classification of chronic bronchitis for clinical and epidemiological purposes. Lancet. 1965;1(7389):775–779.
25. Lahousse L, Seys LJM, Joos GF, Franco OH, Stricker BH, Brusselle GG. Epidemiology and impact of chronic bronchitis in chronic obstructive pulmonary disease. Eur Respir J. 2017;50(2):1602470. doi:10.1183/13993003.02470-2016
26. de Marco R, Marcon A, Rossi A, et al. Asthma, COPD and overlap syndrome: a longitudinal study in young European adults. Eur Respir J. 2015;46(3):671–679. doi:10.1183/09031936.00008615
27. Danish Cancer Society. Voksnes rygevaner. [Smoking habits of adults]. Available from: https://www.cancer.dk/forebyg/undga-roeg-og-rygning/fakta-om-rygning/voksnes-rygevaner/.
28. Le Moual N, Kauffmann F, Eisen EA, Kennedy SM. The healthy worker effect in asthma: work may cause asthma, but asthma may also influence work. Am J Respir Crit Care Med. 2008;177(1):4–10. doi:10.1164/rccm.200703-415PP
29. Menezes AMB, Perez-Padilla R, Jardim JRB, et al. Chronic obstructive pulmonary disease in five Latin American cities (the PLATINO study): a prevalence study. Lancet. 2005;366(9500):1875–1881. doi:10.1016/S0140-6736(05)67632-5
30. Mazurek JM, England LJ. Cigarette smoking among working women of reproductive age - United States, 2009-2013. Nicotine Tob Res. 2016;18(5):894–899. doi:10.1093/ntr/ntv292
31. West R. Tobacco smoking: health impact, prevalence, correlates and interventions. Psychol Heal. 2017;32(8):1018–1036. doi:10.1080/08870446.2017.1325890
32. Friborg J, Koch A, Wohlfarht J, Storm H-H, Melbye M. Cancer in Greenlandic Inuit 1973-1997: a cohort study. Int J Cancer. 2003;107(6):1017–1022. doi:10.1002/ijc.11502
33. Yousaf U, Engholm G, Storm H, et al. Cancer incidence and mortality in Greenland 1983-2014 - including comparison with the other Nordic countries. EClinicalMedicine. 2018;2-3:37–49. doi:10.1016/j.eclinm.2018.08.003
34. Bjerregaard P, Larsen CVL. Three lifestyle-related issues of major significance for public health among the Inuit in contemporary Greenland: a review of adverse childhood conditions, obesity, and smoking in a period of social transition. Public Health Rev. 2018;39(1):5–12. doi:10.1186/s40985-018-0085-8
35. Vijayan VK. Chronic obstructive pulmonary disease. Indian J Med Res. 2013;137(2):251–269.
36. Pezzuto A, Carico E. Effectiveness of smoking cessation in smokers with COPD and nocturnal oxygen desaturation: Functional analysis. Clin Respir J. 2020;14(1):29–34. doi:10.1111/crj.13096
37. Lovafdelingen. Inatsisartutforordning nr. 6 af 26. maj 2010 om ændring af landstingsforordning om tobak og sikring af røgfrie miljøer samt mærkning af tobaksvarer; 2010. [Inatsisartutforordning no. 6 of 26 May 2010 amending the Greenlandic Parliament regulation on tobacco and securing smoke-free environments as well as labeling of tobacco products; 2010]. Available from: https://lovgivning.gl/lov?rid=%7B9E486BA8-3370-44F1-9561-A7064E1B2F9B%7D.
38. Government of Greenland. Handleplan for forebyggelse af rygning 2017–2019. 2017:1–14. [Action plan for smoking prevention 2017–2019. 2017: 1–14]. Available from: https://www.peqqik.gl/-/media/Files/Publikationer/Rapporter_og_redegoerelser/2017/HandleplanForebyggelseAfRygning20172019/Handleplan-for-forebyggelse-af-rygning-2017-2019-DA.pdf?la=da-DK.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.