")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Prevalence of and Risk Factors for Skin Picking Disorder Symptoms Among Adults in an Arab Middle Eastern Population: A Cross-Sectional Study
Authors Khatib HA, Alghamdi WA, Subki AH , Butt NS , Alsallum MS , Alsulaimani AS, Alnajjar SF, Alzaidi FD, Alasmari AA, Alshamrani HM , Al-Zaben F, Koenig HG
Received 7 November 2021
Accepted for publication 23 August 2022
Published 2 December 2022 Volume 2022:15 Pages 2583—2591
DOI https://doi.org/10.2147/CCID.S348258
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Hazim Abdulkarim Khatib,1 Waleed Ahmed Alghamdi,2 Ahmed Hussein Subki,3 Nadeem Shafique Butt,4 Mohammed Saad Alsallum,5 Ahmed Salem Alsulaimani,6 Sara Faisal Alnajjar,7 Fahad Daifallah Alzaidi,8 Abdulrahman Ali Alasmari,9 Hussein Mesfer Alshamrani,10 Faten Al-Zaben,2 Harold G Koenig2,11,12
1Department of Internal Medicine, King Abdulaziz Hospital, Jeddah, Saudi Arabia; 2Department of Psychiatry, King Abdulaziz University, Jeddah, Saudi Arabia; 3Department of Internal Medicine, King Faisal Specialist Hospital & Research Centre, Jeddah, Saudi Arabia; 4Department of Community Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 5Department of Neurology, King Abdulaziz Medical City, Jeddah, Saudi Arabia; 6Department of Emergency Medicine, King Fahad Medical City, Riyadh, Saudi Arabia; 7Department of Diagnostic Radiology, King Abdulaziz University Hospital, Jeddah, Saudi Arabia; 8Department of Internal Medicine, King Abdulaziz University Hospital, Jeddah, Saudi Arabia; 9Department of Forensic Medicine, Forensic Medicine Center, Jeddah, Saudi Arabia; 10Department of Dermatology, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 11School of Public Health, Ningxia Medical University, Yinchuan, People’s Republic of China; 12Department of Psychiatry, Duke University Medical Center, Durham, NC, USA
Correspondence: Waleed Ahmed Alghamdi; Harold G Koenig, Email [email protected]; [email protected]
Introduction: Skin Picking Disorder (SPD) is a skin-related disease, also recognized as psychogenic excoriation, dermatillomania, or excoriation disorder. SPD is defined as a habitual picking of skin, which in turn harms skin tissue. Given the paucity of information on SPD symptoms, their prevalence, and risk factors in Saudi Arabia, the present study seeks to fill this gap by investigating these factors in a community sample from Jeddah.
Methods: This descriptive cross-sectional study was conducted in the city of Jeddah. The Skin Picking Scale-Revised (SPS-R) scale was administered to a convenience sample of 520 respondents. A partial least squares path model (PLS-PM) for “impairment” and “symptoms severity” subscales was assessed by evaluating the validity of measurement and structural models.
Results: Skin picking behavior was reported by 28.8% (n=150). A significant level of skin picking disorder symptoms was present in 1.2% (n=6). Skin picking visual effect, depressive symptoms, and being unmarried were the only positive independent predictors of the total SPS-R score.
Conclusion: SPD symptoms are relatively common among the adult population in Jeddah, but those with threshold symptoms indicative of SPD are relatively few. Such behavior is particularly common in vulnerable groups such as those with depressive symptoms and the unmarried. More attention to this condition by clinicians will improve the quality of life of those affected, and reduce the emotional and physical health consequences of this often unrecognized condition.
Keywords: skin picking disorder, dermatillomania, excoriation disorder, prevalence, risk factors, The Skin Picking Scale-Revised scale
Introduction
Skin Picking Disorder (SPD) is a skin-related disease, also recognized as psychogenic excoriation, dermatillomania, or excoriation disorder. SPD is defined as a habitual picking of the skin, which in turn harms skin tissue.1 The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) has formally classified SPD as a category of obsessive-compulsive (OCD) related disorder.2 SPD has been of particular interest to researchers because of the recent attention this disorder has received as well as its relatively high prevalence, morbidity, and comorbidity.3 Lochner, Roos & Stein report that the prevalence of SPD ranges from 1.4% to 5.4%.4 The disorder is particularly common during adolescence, often coinciding with the onset of puberty. Prochwicz et al have recently examined skin picking in persons from a range of different cultures.5 The results of that study indicated that the overall prevalence of SPD was 7.7%. In Turkey, the prevalence of skin picking among students has been estimated to be nearly 90%, although extreme symptoms are present in only 2%.6 Bohne et al conducted a study of skin picking in German students, also finding a prevalence of nearly 90%, although only 4.6% showed symptoms of clinical impairment and possible SPD.7 Skin picking symptoms in the latter study were driven by a range of triggers, conditions, and emotions. The study found that 85% pinched their skin and 77% clawed their skin; the location of the skin picking was on the face in 95% of cases or cuticles in 53% of cases. In 20%, the picked skin was actually eaten.
The most common behavior in SPD is the near-constant rubbing, picking, or scratching of the skin, leading to skin discoloration, scarring, and infection. In its mildest form, SPD is a self-limited condition.8 Some individuals, however, experience an inability to control their picking leading to unconscious skin picking throughout the day, which not only influences their social and work life but also results in scars, skin ulcers, and even physical deformities.8,9 Keuthen et al have reported that about 1 to 2% of the general population meets the full SPD diagnostic criteria.10
Studies in community samples indicate that skin picking is common and often occurs in conjunction with other psychiatric disorders.10 Initially, its occurrence is focused and conscious, which after a certain time, becomes automatic and unconscious.11 This progression is similar to the features of grooming disorder and trichotillomania.12 In addition, SPD should be approached as a heterogenous spectrum in terms of presentation. Skin picking is usually triggered by stress, boredom, anxiety, or physical sensations (unevenness of the skin).13,14 Individuals with SPD often feel ashamed to come forward and seek help due to perceived social embarrassment and its stigma as a bad habit or untreatable disease, aggravating its severity.15 Difficulties with emotional regulation and reactivity have also been shown to escalate picking behavior to control anxiety, depression, and other disturbing emotions.16 Feeling that the skin is bumpy or uneven or looking blemished or discolored is recognized as worsening SPD.
Grant et al have found that SPD behavior can have a substantial detrimental impact on the tissues resulting in medical complications, eg, localized infections and even septicemia (reported in 38% of SPD cases).17 This study also indicated that the excoriating nature of this condition could lead to a need for blood transfusions or skin grafting (Grant et al, 2012).17 Given the seriousness of SPD and potential complications, it is surprising that this disorder is often unrecognized and untreated.
Commonly reported characteristics across cultures among those with SPD are fright, guilt, outrage, worry, and gloom, indicating that these may be common underlying personality traits. One major concern associated with SPD is the lack of studies on this disorder despite its relatively high prevalence across different cultures.6 Prochwiczet et al emphasized the need for future studies to gather insights on how to treat this disorder and reduce the impairment it causes.5 Given the paucity of information on SPD, its prevalence, and risk factors in Saudi Arabia, the present study sought to fill this gap by investigating these factors in a community sample from Jeddah. The rationale for a Saudi population is that, to our knowledge, there has been no published research on SPD in this country. Therefore, we examine here the prevalence of and risk factors for SPD symptoms in a general adult population in Jeddah.
Methodology
Study Design and Setting
A descriptive cross-sectional study was carried out in Jeddah, a port city in the western region of Saudi Arabia with a population of approximately 4 million people. The study was carried out from May 2017 to October 2017, complied with Declaration of Helsinki, and was approved by the Institutional Review Board (IRB) of King Abdulaziz University Hospital. Written informed consent was obtained from all participants.
Participants
The study included participants from across the city of Jeddah. Participants were a convenience sample of consenting adults aged 18 and above from four major shopping malls in the city. The shopping malls were geographically distributed equally across the city. A total of 553 adults were asked to complete the questionnaire, and 520 agreed to do so (94% response rate). The participants were approached politely and reassured that their privacy would be protected, hence the high response rate. The calculation of sample size was done using the following formula.18

A sample size of 532 achieves 90% power to detect a difference (P1-P0) of 7% using a two-sided exact test with a significance level (alpha) of 0.05.
Data Collection
Demographic information collected included nationality, sex, age, education, social situation, living dynamics, employment status, and monthly income. This information was collected using a demographic data form on iPads. For assessing the SPD symptom severity, the Skin Picking Scale-Revised (SPS-R) was used.16 This is an 8-item self-administrated symptom scale; not a diagnostic measure. The items on the SPS-R assess the frequency of skin picking, the time spent on skin picking, the intensity of skin picking behaviors, control over the behavior, avoidance of consequences, interference with daily activity, emotional distress from picking, and degree of skin damage due to the picking. Response options are on a 4-point Likert scale, ranging from 0 to 4, with the total score ranging from 0 to 32. Higher scores reflect a higher level of symptom severity. The first four questions form the “symptom severity” subscale and the remaining items make up the “impairment” subscale. Studies have demonstrated the validity and reliability of the SPS-R.16,19 The original English version of the SPS-R was translated into Arabic by two independent native Arabic-speaking physicians with excellent knowledge of English. This Arabic version was back-translated into English by two independent native English-speaking physicians with excellent knowledge of Arabic, and any discrepancies were resolved jointly.
Statistical Analysis
Categorical variables were presented as frequencies (n, %). Cronbach alpha coefficients were calculated for the overall SPS-R, the symptom severity subscale, and the impairment subscale. The alpha was evaluated using the guidelines suggested by George and Mallery (2016) where > 0.90 is excellent, > 0.80 good, > 0.70 acceptable, > 0.60 questionable, > 0.50 poor, and ≤ 0.50 is unacceptable.20
A partial least squares path modeling (PLS-PM) analysis was conducted to determine whether the latent variables – symptom severity and impairment – adequately described the data. Forward stepwise regression was used to identify significant factors related to SPS-R. Predictors significant at >0.05 (gender, age, education, job status, income, and OCD) were excluded from the model. Data were analyzed using IBM SPSS Statistics version 23 and The R Project for Statistical Computing.
Results
Most respondents were Saudi (n= 466,90%) and the majority were female (n= 287,55%). Two-thirds of participants had completed a bachelor’s degree from college (n= 334,64%). Around 50% were single (n= 267), and most lived with their families (n= 490,94%). The most frequent job category was employed (n= 217,42%), although almost half of the respondents reported a monthly income of < 5000 SR (n= 248,48%). Most respondents did not report having been diagnosed with depression (n= 486,93%) or OCD (n= 490,94%). Almost 29% reported skin-picking behavior (n= 150,28.8%). The threshold for significant skin-picking on the SPS-R was exceeded by only 1.2% of respondents (n=6). Frequencies and percentages are presented in Table 1.
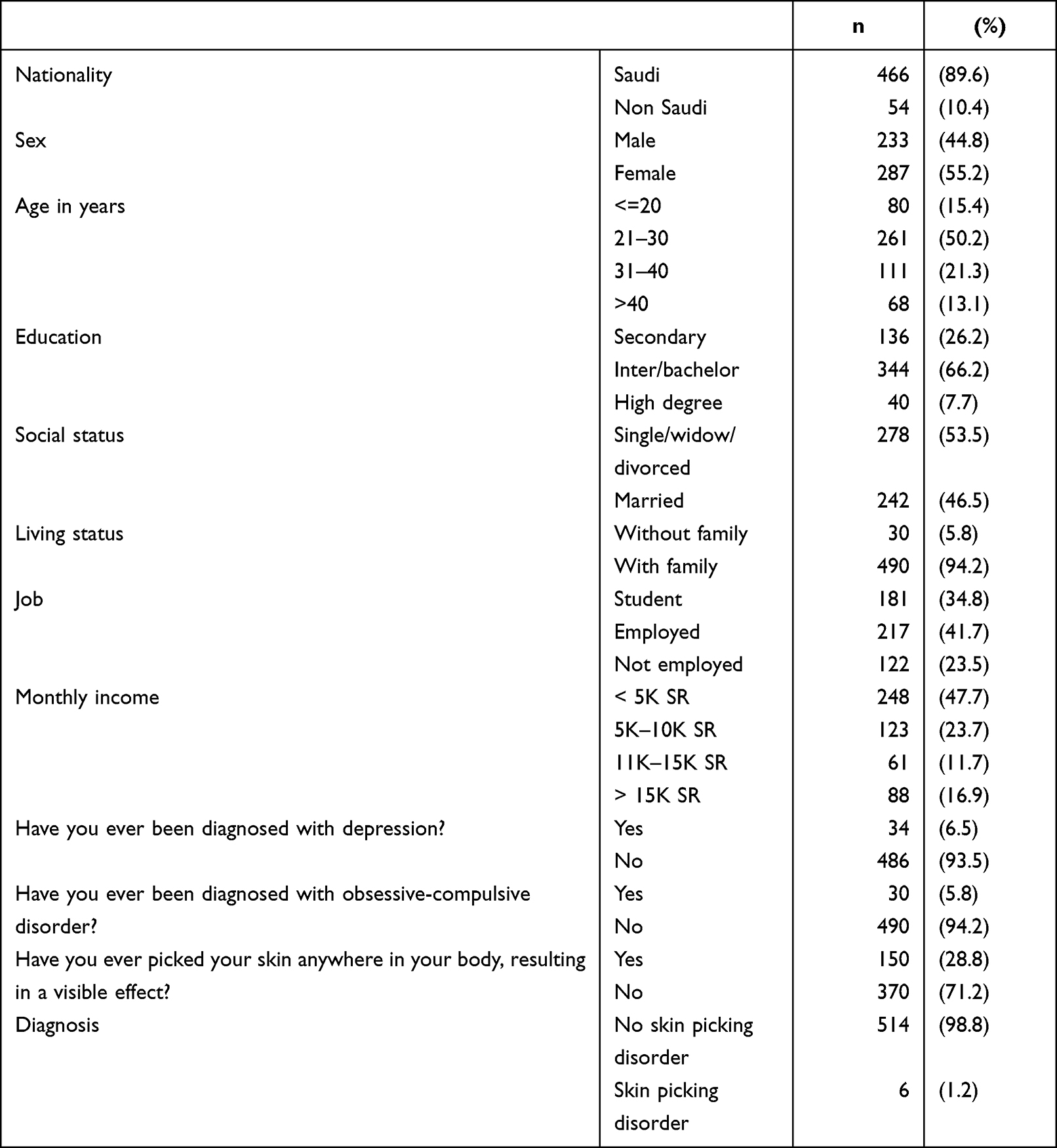 |
Table 1 Socio-Demographic Characteristics of Respondents |
Internal reliability alpha for the SPS-R overall was 0.87, for the symptom severity subscale was 0.82, and for the impairment subscale was 0.78; all indicating acceptable reliability (Table 2). The PLS-PM model was examined by evaluating the validity of the measurement and structural models. The measurement model was assessed by examining the unidimensional nature of indicators, the loadings and communalities for each indicator, and the cross-loadings. Bootstrapping was used to check the significance of each loading in the model. The node diagram for the measurement model is illustrated in Figure 1. The factor loadings and communality were examined to identify any indicators with weak loadings with regard to the latent variables. The variability in each indicator should explain at least 50% of its latent variable construct (|loading| ≥ 0.707; communality ≥ 0.50), and if not, the loading is considered weak. There were no indicators with weak loadings, suggesting that each indicator explained a significant portion of its latent construct. Table 3 presents the loadings and communalities for the measurement model of the PLS-PM. The cross-loadings were also examined to assess the validity of the model. A cross-loading occurs when an indicator has a higher absolute loading on a different latent variable compared to the specified latent variable for that indicator. There were no cross-loadings for variables in the model, indicating that the factor structure was appropriate for the data. Details are presented in Figure 1 and Table 3.
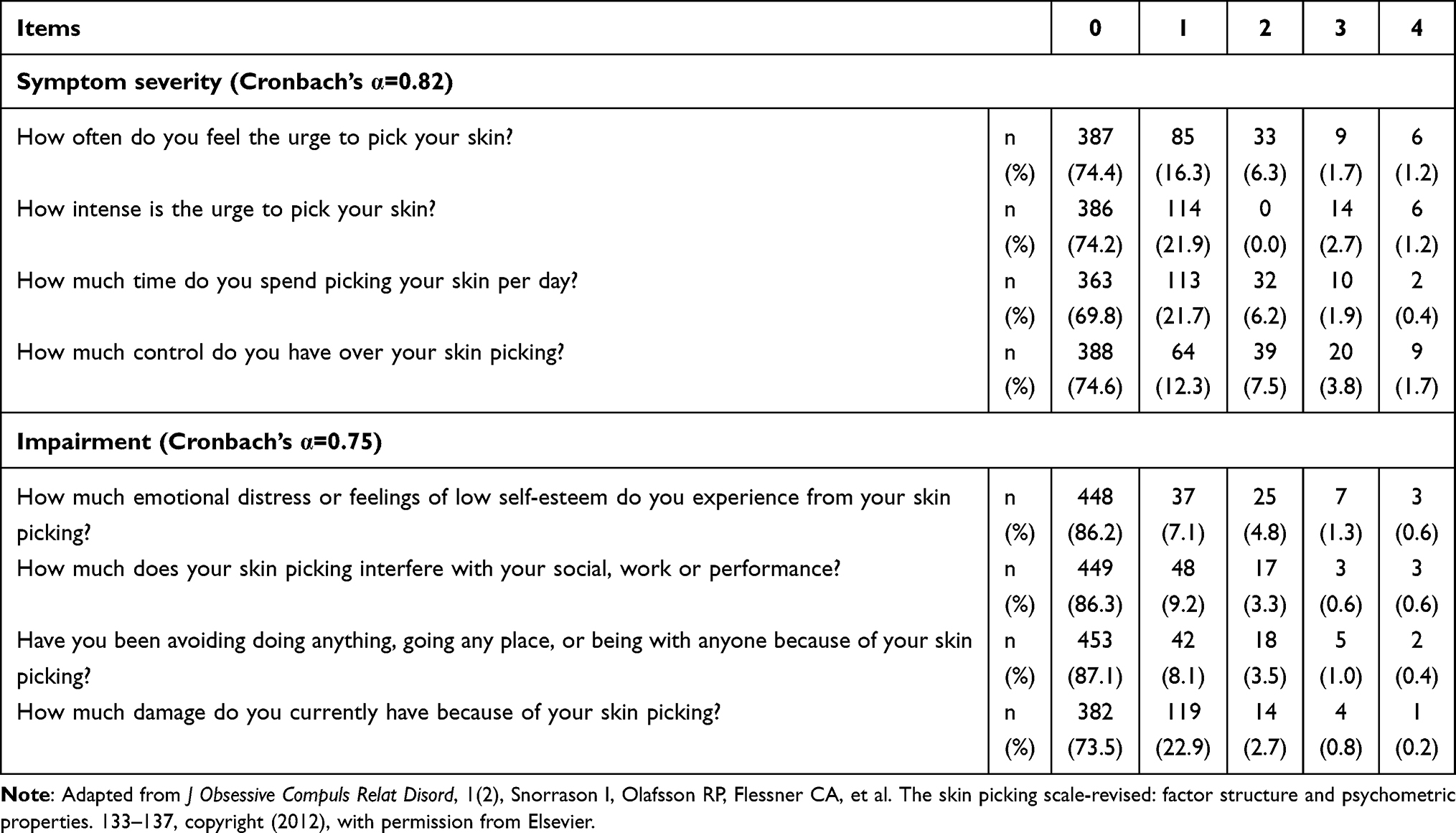 |
Table 2 Distribution and Reliability of SPS-R and Its Sub-Scales |
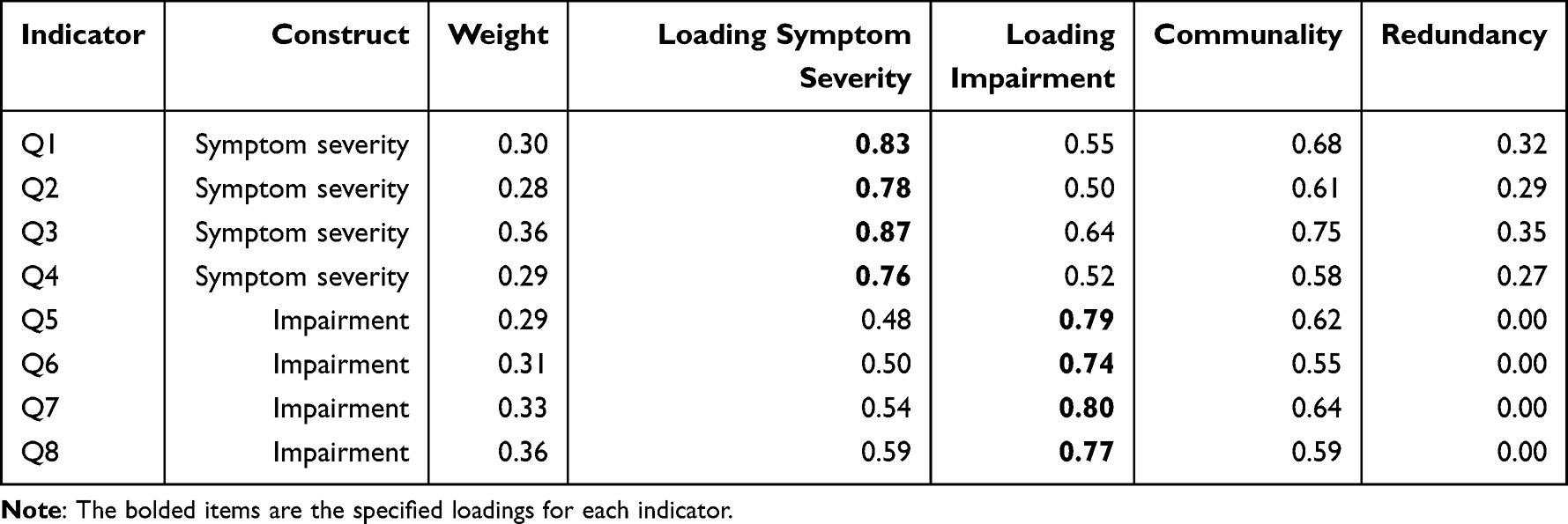 |
Table 3 Measurement Model Summary Table for the PLS-PM Model |
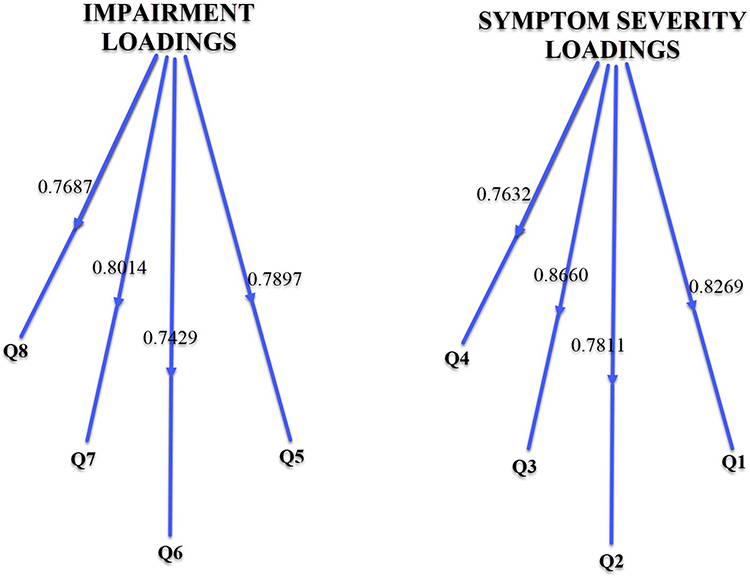 |
Figure 1 Node diagram for the measurement model of the PLS-PM model with loadings shown. |
The results from the linear regression model were significant (F[3516] = 52.2, p<0.001). The skin picking visual effect variable describes whether the respondents visually saw any effect on their skin from their picking. The skin picking visual effect variable was identified as the most significant factor (β = 3.77, t=10.79, p < 0.001). This indicates that those with skin picking visual effect had 3.77 higher skin picking scores on average compared to those whose skin picking did not result in any visual effect. A history of depression was also significantly related to SPS-R score (β = 2.32, t3.68, p <0.001). Those with a prior diagnosis of depression had 2.32 higher SPS-R scores. Marital status was also found to be a significant predictor for SPS-R score (β=0.74, t = 2.33, p = 0.02). Those who were single/divorced/widowed scored 0.74 higher on the SPS-R as compared to those who were currently married (Table 4).
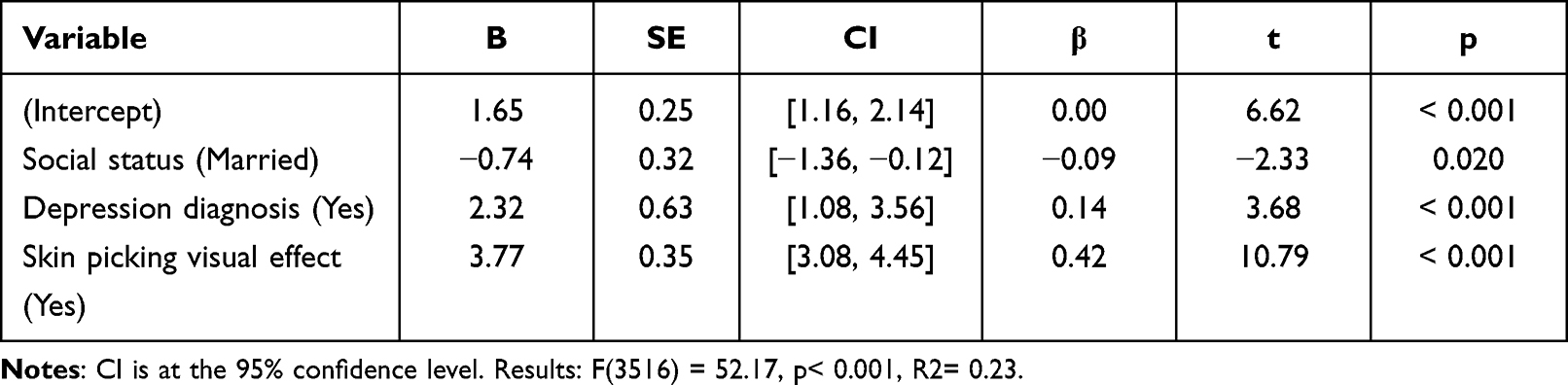 |
Table 4 Results for Linear Regression with Social Status, Depression Diagnosis, and Skin Picking |
Discussion
Skin picking behavior is relatively common among community-dwelling adults in Jeddah, with a prevalence of nearly 30%, ranging from simple skin picking to severe SPD symptoms. This prevalence is less than that reported by Prochwicz et al5 in their Polish population, where the prevalence of skin picking behavior was found to be 47% in the population, with SPD at 7.7% (vs 1.2% in the present sample). A 5.4% prevalence of SPD has been reported in Jewish populations.21 A higher prevalence of SPD has been reported in a medical student population in Karachi, Pakistan, at 9%.22 The differences between our study and other studies may be attributed to differences between the studied populations, such as geographic location, religion, income, sampling methods, and how SPD was identified in each study. The SPS-R questionnaire used in the present study allowed for investigation of variables that influenced symptom severity and impairment based on its subscales.16
While most participants reported only mild symptom severity, the relatively wide prevalence of such symptoms should stimulate further investigation on how skin picking affects quality of life and how to treat more severe cases. Perceptions of psychiatric illness in Saudi populations are plagued with superstition, where people often believe that these conditions are the result of supernatural causes, such as the evil eye or magical spells cast on a person.23 Individuals with SPD may feel overwhelmed with intense shame, guilt, and fear from being stigmatized by society, so they underreport symptoms or underestimate its severity to physicians,24 or worse, go to supernatural healers who promise false treatments that can do more harm than good.25
SPD may also serve as a coping mechanism or way to reduce tension when dealing with work or interpersonal stressors, anxiety, or depression, and has been classified by some as a behavioral addiction.26 The present study found that depression was significantly associated with skin picking behavior, similar to that reported by Nirmal et al27 who also found an increase in this behavior among individuals suffering from depression. Grant & Chamberlain explained this association as due to problems with impulsivity among those with depression.28 Neurobiologically similar to that of other addictions, SPD has also been reported to be more common in those with alcohol or nicotine dependence.29 Alternatively, SPD may also be the cause of anxiety and depression, due to the impairment and stress it can inflict, either emotionally through poor self-esteem and self-loathing, or physically through wounds that can disfigure and increase the risk of infection.5,30
Our study found no association between SPD and OCD. This is in contrast to several studies, such as that by Keuthen et al which showed high comorbidity between SPD and OCD in patients with Trichotillomania.31 One explanation for the different findings in the current study is the way participants were asked about a prior diagnosis of OCD, which may be affected by recall bias (and many may not have presented to a health care specialist for diagnostic evaluation).
In the present study, nearly 13% of participants reported that their social life was significantly affected by their skin picking behavior. Several other studies have found that SPD had a negative effect on quality of life, such as in the Polish study described earlier, which found that nearly 6% of those affected by skin picking sought to avoid social situations because of this behavior.5,32 Another study found that those with SPD experienced significant impairments in physical and psychological quality of life, although their social life was largely unaffected.3
We also found that marital status (being divorced or separated) was associated with a higher likelihood of skin picking behavior; however, it is worthy to note that the majority of our patients were < 30 years of age, which may have affected this finding. However, the association with marital status is consistent with those of Ribeiro, Ribeiro, and Von Doellinger,33 who reported that problems in close relationships may promote frustration, impulsivity, and aggression, which then manifests as skin picking behavior. Other authors have hypothesized that if language cannot be used to express emotions and regulate affect, then skin picking or other forms of self-mutation may be used as a substitute.34
Study Limitations
The generalizability and interpretation of findings from the present study are limited by the number of study limitations. First is the study sample, ie, Saudi adults living in the large metropolitan city of Jeddah, which requires caution when generalizing these findings to those in other areas of the country. Second, the cross-sectional design prevents any conclusions about the causal nature of the skin picking correlates identified here (such as depression). Third, the majority of our patients were less than 30 years old, which may limit these results to a younger population. Fourth, depression and OCD were not identified through a structured psychiatric interview or clinical assessment, but rather participants were simply asked to self-report a diagnosis of these disorders, which may be subject to recall bias or lack of presentation to a healthcare professional for diagnostic evaluation. Fifth, we did not ask questions about addiction, anxiety, or body dysmorphic disorder, which may have been related to SPD symptoms in various ways. Sixth, no pilot study was done beforehand to test the scale characteristics of the Arabic version of the SPS-R. Finally, the use of a self-reported measure for SPD symptoms, rather than a structured clinical interview administered by a trained interviewer, may have affected the accuracy of identifying those with a true disorder. On the other hand, the SPS-R is a reliable measure with strong face validity that provides information about the severity and impairment of skin picking symptoms, thus allowing at least the preliminary identification of psychological and social correlates of this behavior.
Conclusion
The present study found that skin picking disorder symptoms are not rare among the adult population of Jeddah, particularly in vulnerable groups such as those with depression and those who are widowed, divorced, separated, or single. A self-reported history of an OCD diagnosis was surprisingly not associated with SPD. More research, particularly longitudinal studies, is needed to further examine the causes and outcome of skin picking behavior. Education of mental health professionals and primary care medical providers about skin picking disorder is necessary to increase awareness so that identification and treatment may be instituted to reduce the impairment that severe skin picking causes. More attention to this condition by clinicians will improve the quality of life of those affected, and reduce the emotional and physical health consequences of this often unrecognized condition.
Acknowledgments
The authors would like to express thanks to all those who participated in this research. This study was not funded.
Disclosure
None of the authors have any conflicts of interest related to the subject of this research.
References
1. Hawatmeh A, Al-khateeb A. An unusual complication of dermatillomania. Quant Imaging Med Surg. 2017;7(1):166. doi:10.21037/qims.2016.12.02
2. Association AP. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). American Psychiatric Pub; 2013.
3. Machado MO, Köhler CA, Stubbs B, et al. Skin picking disorder: prevalence, correlates, and associations with quality of life in a large sample. CNS Spectr. 2018;23(5):311–320. doi:10.1017/S1092852918000871
4. Lochner C, Roos A, Stein D, Roos A, Stein DJ. Excoriation (skin-picking) disorder: a systematic review of treatment options. Neuropsychiatr Dis Treat. 2017;13:1867. doi:10.2147/NDT.S121138
5. Prochwicz K, Kałużna-Wielobób A, Kłosowska J. Skin picking in a non-clinical sample of young Polish adults. Prevalence and characteristics. Compr Psychiatry. 2016;71:77–85. doi:10.1016/j.comppsych.2016.08.013
6. Calikusu C, Kucukgoncu S, Tecer Ö, et al. Skin picking in Turkish students: prevalence, characteristics, and gender differences. Behav Modif. 2012;36(1):49–66. doi:10.1177/0145445511420282
7. Bohne A, Wilhelm S, Keuthen NJ, et al. Skin picking in German students: prevalence, phenomenology, and associated characteristics. Behav Modif. 2002;26(3):320–339. doi:10.1177/0145445502026003002
8. Alexandrov P, Tan WP, Elterman L. Genital Dermatillomania. Curr Urol. 2017;11(1):54–56. doi:10.1159/000447195
9. Hayes SL, Storch EA, Berlanga L. Skin picking behaviors: an examination of the prevalence and severity in a community sample. J Anxiety Disord. 2009;23(3):314–319. doi:10.1016/j.janxdis.2009.01.008
10. Keuthen NJ, Koran LM, Aboujaoude E, et al. The prevalence of pathologic skin picking in US adults. Compr Psychiatry. 2010;51(2):183–186. doi:10.1016/j.comppsych.2009.04.003
11. Torales J, Díaz NR, Barrios I, et al. Psychodermatology of skin picking (excoriation disorder): a comprehensive review. Dermatol Ther. 2020;33(4):e13661. doi:10.1111/dth.13661
12. Grant JE, Chamberlain SR. Trichotillomania and skin-picking disorder: different kinds of OCD. Focus. 2015;13(2):184–189. doi:10.1176/appi.focus.130212
13. Schumer MC, Bartley CA, Bloch MH. Systematic review of pharmacological and behavioral treatments for skin picking disorder. J Clin Psychopharmacol. 2016;36(2):147. doi:10.1097/JCP.0000000000000462
14. Neziroglu F, Rabinowitz D, Breytman A, et al. Skin picking phenomenology and severity comparison. Prim Care Companion J Clin Psychiatry. 2008;10(04):306. doi:10.4088/PCC.v10n0406
15. Roi C, Bazzano A. Improvement in excoriation (skin-picking) with use of risperidone in a patient with developmental disability. Pediatr Rep. 2017;9(1):6946. doi:10.4081/pr.2017.6946
16. Snorrason I, Olafsson RP, Flessner CA, et al. The skin picking scale-revised: factor structure and psychometric properties. J Obsessive Compuls Relat Disord. 2012;1(2):133–137. doi:10.1016/j.jocrd.2012.03.001
17. Grant JE, Stein DJ, Woods DW, et al. Trichotillomania, Skin Picking, and Other Body-Focused Repetitive Behaviors. American Psychiatric Pub; 2012.
18. Wang W. Clinical Epidemiology-Basic Principles and Practical Applications. WEI Wang, ed. Beijing: Higher Education Press Publication; Vol. 101, 2012.
19. Rabiei M, Kalantari M, Askari K, et al. Factor structure, validity and reliability of the skin picking scale revised version. Zahedan J Res Med Sci. 2014;16:40–44.
20. George D, Mallery P. IBM SPSS Statistics 23 Step by Step: A Simple Guide and Reference. Taylor & Francis; 2016.
21. Leibovici V, Koran LM, Murad S, et al. Excoriation (skin-picking) disorder in adults: a cross-cultural survey of Israeli Jewish and Arab samples. Compr Psychiatry. 2015;58:102–107. doi:10.1016/j.comppsych.2014.12.008
22. Siddiqui EU, Naeem SS, Naqvi H, et al. Prevalence of body-focused repetitive behaviors in three large medical colleges of Karachi: a cross-sectional study. BMC Res Notes. 2012;5(1):614. doi:10.1186/1756-0500-5-614
23. Wahass S, Kent G. A comparison of public attitudes in Britain and Saudi Arabia towards auditory hallucinations. Int J Soc Psychiatry. 1997;43(3):175–183. doi:10.1177/002076409704300303
24. Farooqi YN. Traditional healing practices sought by Muslim psychiatric patients in Lahore, Pakistan. Intl J Disabil Dev Educ. 2006;53(4):401–415. doi:10.1080/10349120601008530
25. Koenig H, Zaben F, Sehlo M, et al. Mental health care in Saudi Arabia: past, present and future. Open J Psychiatry. 2014;04(02):113–130. doi:10.4236/ojpsych.2014.42016
26. Chamberlain SR, Lochner C, Stein DJ, et al. Behavioural addiction—A rising tide? Eur Neuropsychopharmacol. 2016;26(5):841–855. doi:10.1016/j.euroneuro.2015.08.013
27. Nirmal B, Shenoi SD, Rai S, et al. ‘Look beyond skin’: psychogenic excoriation - a series of five cases. Indian J Dermatol. 2013;58(3):246. doi:10.4103/0019-5154.110885
28. Grant JE, Odlaug BL, Chamberlain SR, et al. Skin Picking Disorder. Am J Psychiatry. 2012;169(11):1143–1149. doi:10.1176/appi.ajp.2012.12040508
29. Flessner CA, Woods DW. Phenomenological Characteristics, Social Problems, and the Economic Impact Associated With Chronic Skin Picking. Behav Modif. 2006;30(6):944–963. doi:10.1177/0145445506294083
30. Snorrason Í, Smári J, Ólafsson RP. Emotion regulation in pathological skin picking: findings from a non-treatment seeking sample. J Behav Ther Exp Psychiatry. 2010;41(3):238–245. doi:10.1016/j.jbtep.2010.01.009
31. Keuthen NJ, Curley EE, Scharf JM, et al. Predictors of comorbid obsessive-compulsive disorder and skin-picking disorder in trichotillomania. Ann Clin Psychiatry. 2016;28(4):280–288.
32. Odlaug BL, Lust K, Schreiber LR, et al. Skin picking disorder in university students: health correlates and gender differences. Gen Hosp Psychiatry. 2013;35(2):168–173. doi:10.1016/j.genhosppsych.2012.08.006
33. Ribeiro Â, Ribeiro JP, von Doellinger O. A skin-picking disorder case report: a psychopathological explanation. J Bras Psiquiatr. 2015;64(2):177–180. doi:10.1590/0047-2085000000075
34. Suyemoto KL. The functions of self-mutilation. Clin Psychol Rev. 1998;18(5):531–554. doi:10.1016/S0272-7358(97)00105-0
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.