Back to Journals » Infection and Drug Resistance » Volume 14
Prevalence of Aminoglycoside Resistance and Aminoglycoside Modifying Enzymes in Acinetobacter baumannii Among Intensive Care Unit Patients, Ismailia, Egypt
Authors Kishk R ![]() , Soliman N, Nemr N, Eldesouki R
, Soliman N, Nemr N, Eldesouki R ![]() , Mahrous N
, Mahrous N ![]() , Gobouri A, Azab E
, Gobouri A, Azab E ![]() , Anani M
, Anani M ![]()
Received 14 November 2020
Accepted for publication 18 December 2020
Published 19 January 2021 Volume 2021:14 Pages 143—150
DOI https://doi.org/10.2147/IDR.S290584
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Rania Kishk,1 Nourhan Soliman,2 Nader Nemr,3 Raghda Eldesouki,4 Nageh Mahrous,3 Adil Gobouri,5 Ehab Azab,6 Maha Anani2
1Microbiology and Immunology Department, Faculty of Medicine, Suez Canal University, Ismailia, Egypt; 2Clinical Pathology Department, Faculty of Medicine, Suez Canal University, Ismailia, Egypt; 3Endemic and Infectious Diseases Department, Faculty of Medicine, Suez Canal University, Ismailia, Egypt; 4Genetics Unit, Histology Department, Faculty of Medicine, Suez Canal University, Ismailia, Egypt; 5Department of Chemistry, College of Science, Taif University, Taif 21944, Saudi Arabia; 6Department of Biotechnology, College of Science, Taif University, Taif 21944, Saudi Arabia
Correspondence: Rania Kishk
Faculty of Medicine, Suez Canal University, Ismailia, Egypt
Tel +201025099921
Email [email protected]
Background: Acinetobacter baumannii is an opportunistic pathogen that rapidly develops antibiotic resistance against commonly prescribed antimicrobial agents in hospitalized patients worldwide. Aminoglycosides are commonly used in the treatment of A. baumannii health care-associated infections (HAIs). Aminoglycosides resistance mechanisms are varied and commonly involve production of aminoglycoside-modifying enzymes (AME) and efflux systems.
Aim: This study aimed to provide an insight into the frequency of genes encoding AME in A. baumannii strains isolated from different clinical specimens in intensive care units (ICU).
Methodology: A total of 52 multidrug-resistant (MDR) A. baumannii strains were isolated from ICU, Suez Canal University Hospitals. Species identification and antibiotics susceptibility testing were done by the automated system VITEK 2. The genes encoding AME were detected by PCR.
Results: Aminoglycosides resistance (amikacin, gentamicin and tobramycin) was observed in 35 isolates (67.3%). We found that aacC1 gene was the predominant AME resistance gene among A. baumannii isolates, detected in 14 isolates (40%), aphA6 in 11 isolates (31.4%) and addA1 in 5 isolates (14.2%). We found 5 isolates containing 2 AME genes, 3 of them with aacC1 and aphA6 and the remaining 2 with both aacC1 and aadA1 genes. Nearly, 5 isolates (14.2%) were negative for all AME resistance genes.
Conclusion: Our study indicated that AME encoding genes are predominant in A. baumannii strains in our region which stressed on the importance of preventive measures to control spreading of resistance genes.
Keywords: Acinetobacter baumannii, aminoglycoside-modifying enzymes; AME, aacC1, aphA6, aadA1, aadB
Introduction
A. baumannii can cause severe health care-associated infections (HAIs) of the skin and soft tissue, wound infections, urinary tract infections, pneumonia and secondary meningitis. The highest mortality rates, however, are seen in ventilator-associated pneumonia (VAP) and bloodstream infections especially in intensive care units (ICUs).1
Acinetobacter may develop antibiotic resistance very rapidly.2,3 A significant element of A. baumannii, empowering its endurance and spread inside the health care system, is its capacity to upregulate inherent as well as to gain outside components of antimicrobial resistance.4 They also had the ability to acquire a wide variety of antibiotic resistance genes and rapid development of multidrug-resistant (MDR), extensively drug-resistant (XDR) and even pan drug-resistant (PDR) strains. MDR A. baumannii strains are resistant to beta-lactams, aminoglycosides, carbapenems and fluoroquinolones.5 Decreased membrane permeability due to loss of porins, acquisition of extended-spectrum β - lactamase, and multidrug efflux systems are mechanisms claimed for A. baumannii multidrug resistance.6
The aminoglycoside antibiotic class is commonly used in the treatment of HAIs from gram-negative bacilli, including A. baumannii strains. The bactericidal activity of aminoglycosides depends on their concentration rather than on the exposure duration to inhibitory concentrations of them. Recently, different resistance mechanisms had been developed against these antimicrobial drugs.5
Development of resistance to newer semisynthetic aminoglycosides such as tobramycin, isepamicin, amikacin and sisomicin are being described in many countries worldwide.7 The resistance mechanisms of A. baumannii to aminoglycoside agents are different and typically include aminoglycoside-modifying enzymes (AME) production, which might be classified into aminoglycoside phosphotransferases (APH) (3ʹ)-Via (aphA6), aminoglycoside acetyltransferases (AAC) (3)-Ia (aacC1), besides aminoglycoside nucleotidyltransferases (ANT) (2ʹ’)-Ia (aadB) and ANT(3”) -Ia (aadA1). The genes of those enzymes are carried on plasmids and transposons and are transferred easily among A. baumannii population.8 APH (3ʹ)-VI, AAC (3)-I and ANT(3”)-I synthesis were found to be predominant by many researches on A. baumannii isolates, but there are substantial regional differences in their genotypes.8
The main mechanism of aminoglycoside resistance is enzymatic alteration of amino-or hydroxyl-groups of aminoglycosides. Aminoglycoside enzymatic modification results in decreased binding to the ribosome of the aminoglycoside molecule. Previous studies suggested several mechanisms of aminoglycoside resistance in Acinetobacter spp.9 Enzymatic inactivation by AAC, ANT, and APH is the most prevalent resistance mechanism.10
Although aminoglycosides present nephrotoxicity risks and other side effects, they are considered to be important antimicrobial agents and are used to treat HAIs. The high rates of aminoglycoside resistance could cause a serious issue for combination therapy of aminoglycoside with broad-spectrum β-lactams including cephalosporins and carbapenems against A. baumannii infections. AME and efflux pumps are the most important sources of aminoglycoside resistance among A. baumannii isolates where their genes encoding these aminoglycoside resistance mechanisms can be distributed mobile elements.11
The overall prevalence of aminoglycoside resistance genes and the mechanisms of resistance among A. baumannii clinical isolates in ICU have not been well studied in our country. Therefore, the aim of the present study was to provide an insight into the frequency of gene encoding AME in A. baumannii strains isolated from different clinical specimens in ICU.
Materials and Methods
Study Design
This cross-sectional descriptive study was carried out during the period from January 2019 to December 2019. Samples were processed in microbiology laboratory, Faculty of Medicine, Suez Canal University. This study included only patients during ICU stay and developed HAIs. We excluded patients on antibiotic treatment, patients with A. baumannii as a colonization not infection. Non-duplicated MDR A. baumannii strains were isolated from patients with HAIs in Suez Canal University Hospitals. In case of duplicate isolates (>1 isolates from the same patient) the first isolate was selected for further analysis. Approval was obtained from the ethics committee of Suez Canal University Faculty of Medicine. The procedures used in this study adhere to the tenets of the Declaration of Helsinki. Written, informed consent was obtained from each patient included in this study.
Bacterial Isolation, Identification and Antibiotics Susceptibility
The collected samples (blood, urine, sputum, pus and endotracheal aspirate) were cultured on blood and Mac Conkey (Oxoid, UK) media. Bactec-Alert 3D (Becton Dickinson, Sparks, The United State of America) blood culture incubation system was used for the isolation of bacteria from the blood cultures.
Colonies were identified as A. baumannii by colony morphology, Gram stain and different biochemical reactions.12 A gram stain was performed to determine an organism’s gram reaction and morphology prior to selecting which identification card to inoculate Suspected isolates were oxidase negative, catalase positive, indole negative, citrate positive and non-motile. Finally, species identification and antibiotic susceptibility tests were performed by VITEK 2 Compact 5 (bioMérieux, Inc., Durham, NC, USA). MICs were interpreted as being in susceptible, intermediate, or resistant groups according to the breakpoints recommended by the CLSI standards.13 Testing was performed according to the manufacturer’s instructions. Vitek 2 testing was performed using software version 5.04 and AST-GN71 REF 413,402 cards, according to the manufacturer’s instructions.14,15 A. baumannii isolates that were resistant to more than three of the existing antibiotics determined were identified as MDRs. MDR is defined as non-susceptibility to at least one agent in three or more antimicrobial categories. XDR is defined as non-susceptibility to at least one agent in all but two or fewer antimicrobial categories (i.e., bacterial isolates remain susceptible to only one or two categories).16 Antibiotics used were ampicillin/sulbactam, cefazoline, ceftriaxone, cefepime, imipenem, meropenem, amikacin, gentamicin, tobramycin, ciprofloxacin, tigecycline and trimethoprim/sulphamethoxazole. The isolates were preserved at –80°C in glycerol 15% in brain heart infusion broth (BHIB, Oxoid, Basingstoke, UK) and then subcultured in brain heart infusion broth (BHIB) at 37°C for 24h.
DNA Extraction
DNA was extracted from aminoglycoside resistant strains using Spin ABT Kit (Applied Biotechnology Co. Ltd, Egypt) from fresh subculture on MacConkey agar plates according to manufacturer’s instructions. DNA concentration and the purity were assessed by a Nanodrop. A yield of more than 20 µg should be obtained and the A260/A280 ratio should be between 1.7–1.9. DNA was finally eluted in water and preserved at −20°C until use.
Detection of Aminoglycoside Resistance Genes
The genes encoding AME, including phosphotransferases APH (3ʹ)-Via (aphA6), acetyltransferases AAC (3)-Ia (aacC1), nucleotidyl transferases ANT (2ʹ’)-Ia (aadB) and ANT (3”) -Ia (aadA1), were detected by PCR in only aminoglycoside resistant isolates. The sequences of primers used in the PCR amplification5 are demonstrated in Table 1.
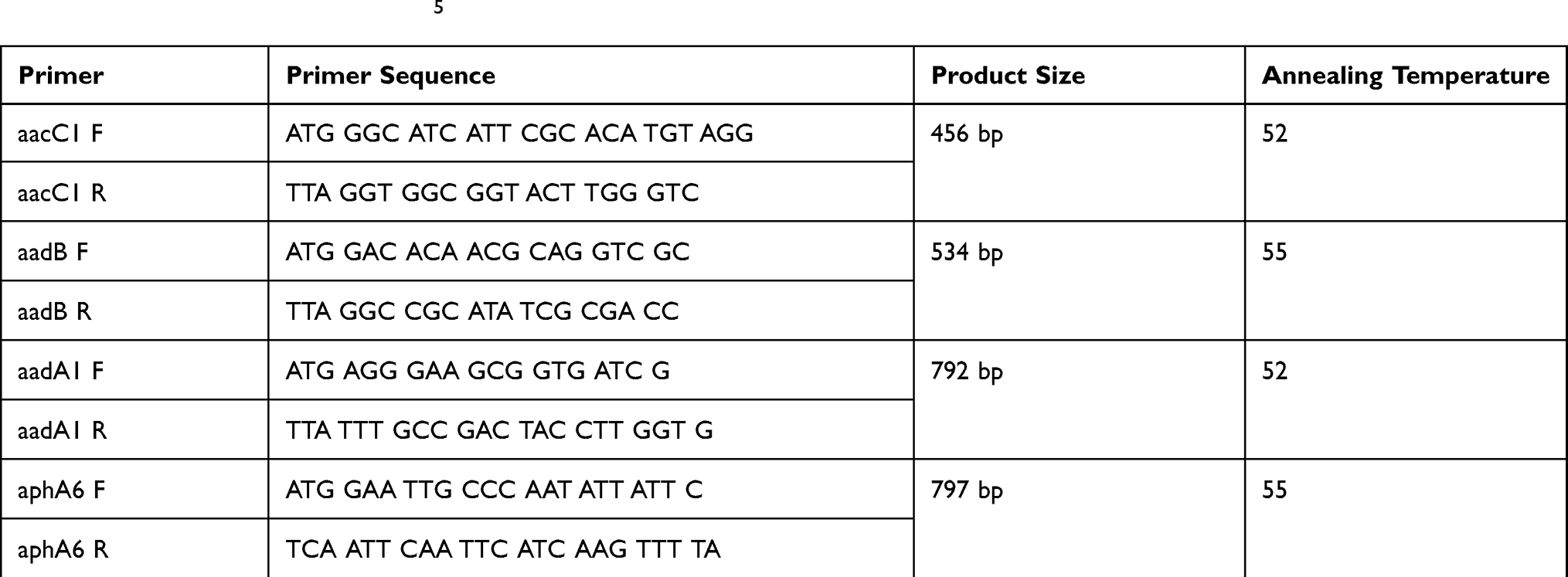 |
Table 1 Primers Used in This Study5 |
PCR reactions were performed in a final volume of 25 μL (24 μL PCR master mix plus 1 μL of template DNA). Reaction mixtures without a DNA template were used as negative control. PCR amplification was carried out in a thermal cycler (Peltier Thermal cycler, MJ Research, USA) with the following conditions: initial denaturation at 95°C for 3 minutes, followed by 35 cycles of 60 seconds, denaturation at 94°C for 60 seconds, then 60 seconds for annealing at primers annealing temperatures (Table 1) and 45 seconds for extension at 72°C with a final extension at 72°C for 5 minutes.
The amplicon size was analyzed by electrophoresis on 1.2% agarose gel in a tris-acetate-EDTA (TAE) buffer at 90 volts alongside a 1 Kb DNA ladder (Applied Biotechnology Co. Ltd, Egypt). Electrophoresis was performed for one hour and finally the gels were stained with ethidium bromide and visualized using the gel documentation system.
Statistical Analysis
All statistical analyses were performed using Statistical Package for Social Science program (SPSS version 22 for windows). Continuous data were summarized by mean, standard deviation and range while qualitative data were summarized by frequencies. In analytical data, the chi-square test was used to detect the difference between qualitative data. Statistical significance was considered at p.value ≤ 0.05.
Results
Clinical Specimens and MDR A. baumannii
A total of 52 non duplicated MDR A. baumannii isolates were recovered from clinical specimens of hospitalized patients with HAIs that had been admitted to the ICUs in Suez Canal University Hospitals, Ismailia, Egypt. The isolates were obtained from invasive and non-invasive sites, including endotracheal aspirates (29/52, 55.8%), urine (11/52, 21.2%), sputum (5/52, 9.6%), blood (5/52, 9.6%) and pus from wound (2/52, 3.8%). The mean ± SD of age was 48 years± 1.334, with a range of 1 to 86 years.
Distribution of MDR A. baumannii According to Age
Most MDR A. baumannii isolates were observed in the age group, 60–<80 years old (33/52, 63.4%) (p=0.001) followed by 20–<40 years (8/52, 15.4%), 40–<60 (6/52, 11.5%), more than 80 years old (4/52, 7.7%) and only 1 strain was isolated from 0–<20 (1/52, 2%).
Antimicrobial Susceptibility of MDR A. baumannii Isolates
The highest resistance was against cefazoline (100%), ampicillin/sulbactam (80.8%) and cefepime (78.8%). On the other hand, all strains were susceptible to tigecycline (100%). Resistance to at least one aminoglycoside (amikacin, gentamicin and/or tobramycin) was observed in 35 isolates (67.3%). All isolates with amikacin and gentamicin resistance were Tobramycin resistant (Table 2).
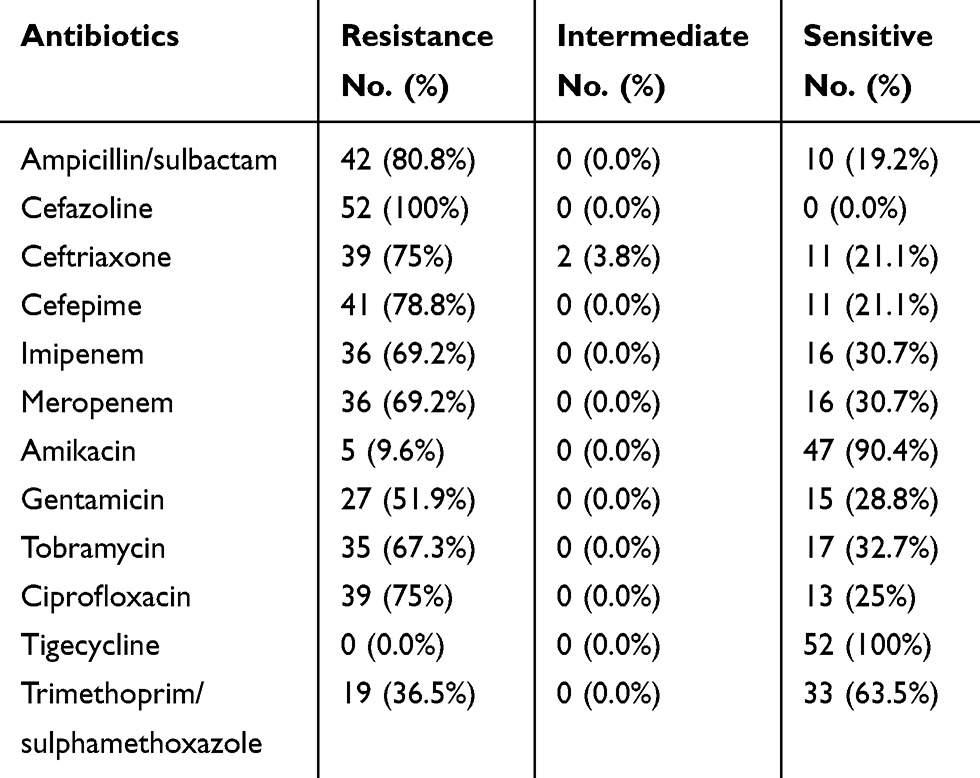 |
Table 2 Antimicrobial Resistance Pattern of A. baumannii Against Different Antibiotics (N=52) |
In relation to age, most aminoglycoside resistant isolates was observed in the age group, 60–<80 years old (27/35, 77.1%), only 6 isolates were equally distributed between the 2 age groups 20–<40 years and 40–<60 (3/35, 8.6% for each) and 2 isolates were more than 80 years old (2/35, 5.7%) (p=0.001).
Genotypic Detection of AME Resistance Genes
Aminoglycoside resistant isolates (35 isolates) were screened for the presence of AME resistance genes by PCR. Nearly, 5 isolates (14.2%) were negative for all AME resistance genes. Interestingly, aacC1 gene was detected in 14 isolates (40%), aphA6 in 11 isolates (31.4%) and addA1 in 5 isolates (%). We did not detect aadB in any isolates. Surprisingly, we found 5 isolates containing 2 AME resistance genes, 3 of them with aacC1 and aphA6 and the remaining 2 were carrying both aacC1 and aadA1 resistance genes (Figures 1–3).
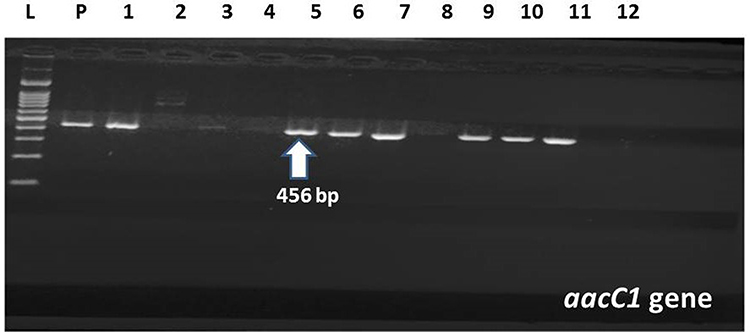 |
Figure 1 Amplification of aaaC1 gene in MDR A. baumannii by PCR; Lane (L) shows 100-bp molecular size ladder, lane (P) is the positive control, lanes 1,5,6,7,9,10,11 are the positive samples carrying aaaC1 gene (456 bp). Lanes 2,3,4,8 are negative samples. Lane (12) is the negative control. |
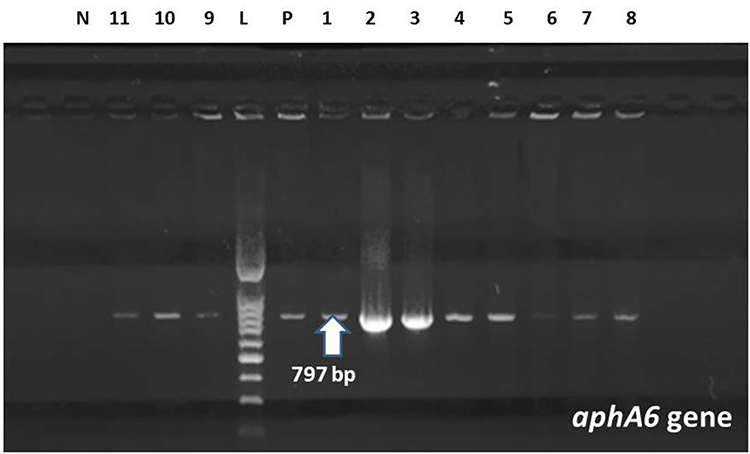 |
Figure 2 Amplification of aphA6 gene in MDR A. baumannii by PCR; Lane (L) shows 100-bp molecular size ladder, lane (P) is the positive control, lanes 1–11 are the positive samples carrying aphA6 gene (797 bp). Lane (N) is the negative control. |
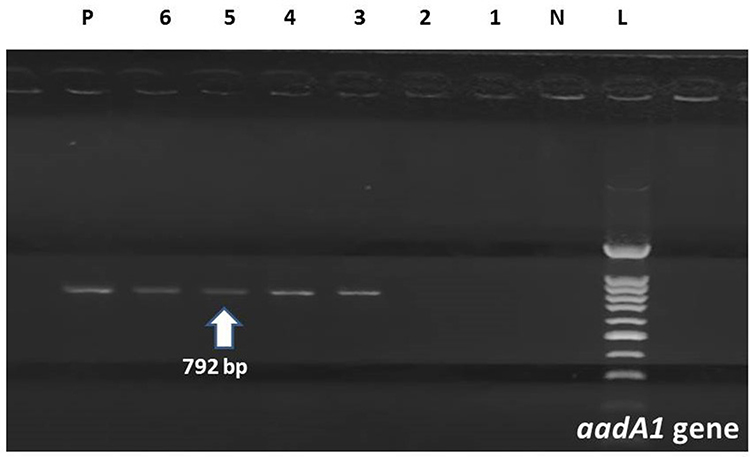 |
Figure 3 Amplification of aadA1 gene in MDR A. baumannii by PCR; Lane (L) shows 100-bp molecular size ladder. Lane (N) is the negative control. Lanes 3–6 are the positive samples carrying aadA1 gene (792 bp). Lanes 1.2 are negative samples. Lane (P) is the positive control. |
Distribution of AME Resistance Genes According to the Clinical Isolates
Among the MDR A. baumannii isolated from endotracheal aspirates (29 isolates), 22 isolates (75.8%) were aminoglycoside resistance phenotypically. One of them (4.5%) was negative by PCR for AME genes, 12 isolates (54.6%) were carrying aaccC1 gene, 8 isolates with aphA6 gene (36.4%) and only one isolate (4.5%) was carrying aadA1. Resistance genes were detected in only 4 urine samples distributed equally to aacC1 and aadA1 genes (2 isolates for each, 33.3%). On the other hand, we detect aphA6 and aaadA1 resistance genes in sputum (2 isolates for each, 50%) while only aphA6 gene was detected in blood samples (1 isolate). No AME resistance genes were detected in pus specimens (Table 3).
 |
Table 3 Distribution of AME Resistance Genes According to the Clinical Isolates |
Discussion
The present study aims to determine the prevalence of aminoglycosides genes of resistance among different clinical isolates of A. baumannii isolated from ICUs in Suez Canal University Hospitals, Ismailia, Egypt. We found that 71% (37/52) of our A. baumannii patients aged over 60 years old. In 2010, Sengstock and his colleagues studied MDR A. baumannii as an emerging pathogen among elderly in community hospitals and nursing homes. They found that 68% of the patients aged over 60 years.17 Aging was considered one of the risk factors of MDR A. baumannii infection as reported by a multi-centre study.18 Another research reported aging as a significantly associated factor with mortality in A. baumannii infection19 with worse outcomes than the young.20,21 This is due to impaired adaptive and innate immune systems in elderly which might influence the prevention and treatment of A. baumannii infection.22–24 So, preventing A. baumannii infection in the elderly would be an important public health issue.
In our study, aminoglycosides resistance was observed by MIC in 35 isolates (67.3%) [Amikacin (9.6%), gentamicin (51.9%) and tobramycin (67.3%)]. All isolates with amikacin and gentamicin resistance were Tobramycin resistance. In 2010, Akers et al, reported that the aminoglycoside antibiotics susceptibility were 96.6% to gentamicin and 77.5% to tobramycin.25 Previously, a high rate of resistance to aminoglycosides was reported by several investigators in Iran.5,26–28
Thirty-five aminoglycoside resistant isolates were investigated for the presence of AME resistance genes by PCR. We found that aacC1 gene was the predominant aminoglycoside-modifying gene among the A. baumannii isolates from ICU patients which detected in 14 isolates (40%), aphA6 in 11 isolates (31.4%) and addA1 in 5 isolates (14.2%).These findings were compatible with an Iranian study performed in 2014 reported that aacC1 gene in is the most prevalent one (65.11%), while aphA6, aadA1 was detected in (60.46%), (27.9%) of the isolates respectively.5
Nie et al proposed that increased aminoglycoside resistance in A. baumannii is related to acc (6ʹ).29 Another study reported the presence of acetyltransferase genes (aacC1) in 63.3% of Acinetobacter isolates and other genes including aphA6, aadA1 and aadB were detected in 65%, 41.7% and 3.3%, of the isolates, respectively.30 In our study the prevalence of aphA6 and aadA1 genes was less prevalent than reported previously.31,32 However, Farsiani et al reported a prevalence of aphA1 (75%) among A. baumannii isolates from HAIs in the north-east of Iran while aadA1 gene was not identified in the examined isolates.33 More recently in 2018, another study reported that aadA1 is the most frequent AMEs amongst nosocomial A. baumannii isolates from Iranian patients.34
We did not detect aadB in any isolates. This was incompatible with other studies reported high prevalence of aadB genes in their population.5,30 In a Korean study, the majority of AME genes detected by PCR were aacC1 (56%), aadB (48%), and aphA6 (71%).35
In Czech Republic, investigators assessed the variety of genes encoding AME and their relation to class 1 integrons in A. baumannii. They reported aminoglycoside resistance genes in 95% of isolates where the predominance was to aacC1 gene followed by aadA1, aphA6, and aadB.36 Previously, a high rate of resistance to aminoglycosides was reported by several investigators in Iran.5,26,28,31
Considering these differences, it appeared that the aminoglycoside resistance genes were distributed among various genotypically distinct groups of A. baumannii strains. Thus, these data could reflect a widespread occurrence and clonal variation in HAIs A. baumannii isolates in various regions.
Limitations of the Study
Our study was a single center, short study in our institution only with small number of isolates. So, it is lack in A. baumannii strain variety. Also, we cannot evaluate of the clonal relatedness of the 52 isolates. The correlation between the detected AMEs and the resistance patterns is unclear. Role of other mechanisms of aminoglycoside resistance was not studied (e.g., efflux pumps and 16S-ribosomal RNA methyltransferases).
Conclusion
Our study results showed a significant variety of genes encoding AME in our region. We also found that the genes related to AME are prevalent in the A. baumannii strains giving a special concern to the importance of prevention and control measures to prevent their spread.
Data Sharing Statement
All authors claim that all data and materials as well as software application or custom code support our published claims and comply with field standards.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Acknowledgments
We thank Taif University researchers supporting project number TURSP-2020/13, Taif University, Taif, Saudi Arabia.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted * Dove Medical Press Ltd *; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Dijkshoorn L, Nemec A, Seifert H. An increasing threat in hospitals: multidrug-resistant Acinetobacter baumannii. Nat Rev Microbiol. 2007;5(12):939–951. doi:10.1038/nrmicro1789
2. Parte AC. LPSN - list of prokaryotic names with standing in nomenclature (bacterio.net), 20 years on. Int J Syst Evol Microbiol. 2018;68(6):1825–1829. doi:10.1099/ijsem.0.002786
3. Visca P, Seifert H, Towner KJ. Acinetobacter infection - an emerging threat to human health. IUBMB Life. 2011;63(12):1048–1054. doi:10.1002/iub.534
4. Pogue JM, Mann T, Barber KE, Kaye KS. Carbapenem-resistant Acinetobacter baumannii: epidemiology, surveillance and management. Expert Rev Anti Infect Ther. 2013;11(4):383–393. doi:10.1586/eri.13.14
5. Aliakbarzade K, Farajnia S, Karimi Nik A, Zarei F, Tanomand A. Prevalence of aminoglycoside resistance genes in Acinetobacter baumannii isolates. Jundishapur J Microbiol. 2014;7(10):e11924. doi:10.5812/jjm.11924
6. Kim YJ, Kim SI, Kim YR, et al. Carbapenem-resistant Acinetobacter baumannii: diversity of resistant mechanisms and risk factors for infection. Epidemiol Infect. 2012;140(1):137–145. doi:10.1017/S0950268811000744
7. Upadhyay S, Khyriem AB, Bhattacharya P, Bhattacharjee A, Joshi SR. High-level aminoglycoside resistance in Acinetobacter baumannii recovered from Intensive Care Unit patients in Northeastern India. Indian J Med Microbiol. 2018;36(1):43–48. doi:10.4103/ijmm.IJMM_17_225
8. Lin M-F, Liou M-L, Tu -C-C, Yeh H-W, Lan C-Y. Molecular epidemiology of integron-associated antimicrobial gene cassettes in the clinical isolates of Acinetobacter baumanniifrom Northern Taiwan. Ann Lab Med. 2013;33(4):242. doi:10.3343/alm.2013.33.4.242
9. The Aminoglycoside Resistance Study Groups. The most frequently occurring aminoglycoside resistance mechanisms–combined results of surveys in eight regions of the world. J Chemother (Florence, Italy). 1995;7(Suppl 2):17–30.
10. Shaw KJ, Rather PN, Hare RS, Miller GH. Molecular genetics of aminoglycoside resistance genes and familial relationships of the aminoglycoside-modifying enzymes. Microbiol Rev. 1993;57(1):138–163. doi:10.1128/MR.57.1.138-163.1993
11. Lee C-R, Lee JH, Park M, et al. Biology of Acinetobacter baumannii: pathogenesis, antibiotic resistance mechanisms, and prospective treatment options. Front Cell Infect Microbiol. 2017;7.
12. Forbes BA, Sahm DF, Weissfeld A. Bailey and Scott’s Diagnostic Microbiology.
13. CLSI. Performance Standards for Antimicrobial Susceptibility Testing.
14. biomerieuxdirect.com. AST-GN69 TEST KIT | VITEK 2 Suscept.test. 64 Wells Gram - | Vitek2 AST Cards 64 Wells | Automated: VITEK system | ID/AST Auto | Bacteriology | bioMerieux Clinical USA. n.d.
15. Humphries RM, Hindler JA, Goldstein EJC. Emerging resistance, new antimicrobial agents but no tests! The challenge of antimicrobial susceptibility testing in the current US regulatory landscape. Clin Infect Dis. 2016;63(1):83–88. doi:10.1093/cid/ciw201
16. Magiorakos A, Srinivasan A, Carey RB, et al. Multidrug‐resistant, extensively drug‐resistant and pandrug‐resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18:268–281. doi:10.1111/j.1469-0691.2011.03570.x
17. Sengstock DM, Thyagarajan R, Apalara J, Mira A, Chopra T, Kaye KS. Multidrug-resistant Acinetobacter baumannii: an emerging pathogen among older adults in community hospitals and nursing homes. Clin Infect Dis. 2010;50(12):1611–1616. doi:10.1086/652759
18. Huang H, Chen B, Liu G, et al. A multi-center study on the risk factors of infection caused by multi-drug resistant Acinetobacter baumannii. BMC Infect Dis. 2018;18(1). doi:10.1186/s12879-017-2932-5
19. Fournier PE, Richet H, Weinstein RA. The epidemiology and control of Acinetobacter baumannii in health care facilities. Clin Infect Dis. 2006;42(5):692–699. doi:10.1086/500202
20. Garnacho J, Sole-Violan J, Sa-Borges M, Diaz E, Rello J. Clinical impact of pneumonia caused by Acinetobacter baumannii in intubated patients: a matched cohort study. Crit Care Med. 2003;31(10):2478–2482. doi:10.1097/01.CCM.0000089936.09573.F3
21. Garnacho-Montero J, Ortiz-Leyba C, Fernández-Hinojosa E, et al. Acinetobacter baumannii ventilator-associated pneumonia: epidemiological and clinical findings. Intensive Care Med. 2005;31(5):649–655. doi:10.1007/s00134-005-2598-0
22. Mahbub SL, Brubaker A, Kovacs E. Aging of the innate immune system: an update. Curr Immunol Rev. 2011;7(1):104–115. doi:10.2174/157339511794474181
23. Allman D, Miller JP. B cell development and receptor diversity during aging. Curr Opin Immunol. 2005;17(5):463–467. doi:10.1016/j.coi.2005.07.002
24. Goronzy JJ, Weyand CM. T cell development and receptor diversity during aging. Curr Opin Immunol. 2005;17(5):468–475. doi:10.1016/j.coi.2005.07.020
25. Akers KS, Chaney C, Barsoumian A, et al. Aminoglycoside resistance and susceptibility testing errors in Acinetobacter baumannii-calcoaceticus complex. J Clin Microbiol. 2010;48(4):1132–1138. doi:10.1128/JCM.02006-09
26. Sheikhalizadeh V, Hasani A, Ahangarzadeh Rezaee M, et al. Comprehensive study to investigate the role of various aminoglycoside resistance mechanisms in clinical isolates of Acinetobacter baumannii. J Infect Chemother. 2017;23(2):74–79. doi:10.1016/j.jiac.2016.09.012
27. Japoni-Nejad A, Farshad S, van Belkum A, Ghaznavi-Rad E. Novel cassette array in a class 1 integron in clinical isolates of Acinetobacter baumannii from central Iran. Int J Med Microbiol. 2013;303(8):645–650. doi:10.1016/j.ijmm.2013.09.005
28. Sistanizad M, Kouchek M, Miri M, et al. Carbapenem restriction and its effect on bacterial resistance in an intensive care unit of a Teaching Hospital. Iran J Pharm Res. 2013;12(3):503–509.
29. Nie L, Lv Y, Yuan M, et al. Genetic basis of high-level aminoglycoside resistance in Acinetobacter baumannii from Beijing, China. Acta Pharm Sin B. 2014;4(4):295–300. doi:10.1016/j.apsb.2014.06.004
30. Moniri R, Farahani RK, Shajari G, Shirazi MN, Ghasemi A. Molecular epidemiology of aminoglycosides resistance in Acinetobacter Spp. with emergence of multidrug-resistant strains. Iran J Public Health. 2010;39(2):63–68.
31. Tahbaz SV, Azimi L, Lari AR. Characterization of aminoglycoside resistance mechanisms in Acinetobacter baumannii isolates from burn wound colonization. Ann Burns Fire Disasters. 2019;32(2):115–121.
32. Asadollahi K, Taherikalani M, Maleki A, et al. Diversity of aminoglycoside modifying enzyme genes among multidrug resistant Acinetobacter baumanniigenotypes isolated from nosocomial infections in Tehran hospitals and their association with class 1 integrons. Acta Microbiol Immunol Hung. 2011;58(4):359–370. doi:10.1556/AMicr.58.2011.4.11
33. Farsiani H, Mosavat A, Soleimanpour S, et al. Limited genetic diversity and extensive antimicrobial resistance in clinical isolates of Acinetobacter baumannii in north-east Iran. J Med Microbiol. 2015;64(7):767–773. doi:10.1099/jmm.0.000090
34. Salimizand H, Zomorodi AR, Mansury D, et al. Diversity of aminoglycoside modifying enzymes and 16S rRNA methylases in Acinetobacter baumannii and Acinetobacter nosocomialis species in Iran; wide distribution of aadA1 and armA. Infect Genet Evol. 2018;66:195–199. doi:10.1016/j.meegid.2018.09.028
35. Lee K, Yong D, Jeong SH, Chong Y. Multidrug-resistant Acinetobacter spp.: increasingly problematic nosocomial pathogens. Yonsei Med J. 2011;52(6):879–891. doi:10.3349/ymj.2011.52.6.879
36. Nemec A, Dolzani L, Brisse S, van den Broek P, Dijkshoorn L. Diversity of aminoglycoside-resistance genes and their association with class 1 integrons among strains of pan-European Acinetobacter baumannii clones. J Med Microbiol. 2004;53(Pt 12):1233–1240. doi:10.1099/jmm.0.45716-0
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.