Back to Journals » Infection and Drug Resistance » Volume 13
Prevalence, Associated Risk Factors and Rifampicin Resistance Pattern of Pulmonary Tuberculosis Among Children at Debre Markos Referral Hospital, Northwest, Ethiopia
Authors Liyew Ayalew M, Birhan Yigzaw W, Tigabu A ![]() , Gelaw Tarekegn B
, Gelaw Tarekegn B
Received 21 August 2020
Accepted for publication 14 October 2020
Published 29 October 2020 Volume 2020:13 Pages 3863—3872
DOI https://doi.org/10.2147/IDR.S277222
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Mulusew Liyew Ayalew,1 Wubet Birhan Yigzaw,2 Abiye Tigabu,1 Baye Gelaw Tarekegn1
1Department of Medical Microbiology, School of Biomedical and Laboratory Sciences, College of Medicine and Health Sciences, University of Gondar (UOG), Gondar, Ethiopia; 2Department of Immunology and Molecular Biology, School of Biomedical and Laboratory Sciences, College of Medicine and Health Sciences, University of Gondar (UOG), Gondar, Ethiopia
Correspondence: Abiye Tigabu
Department of Medical Microbiology, School of Biomedical and Laboratory Sciences, College of Medicine and Health Sciences, University of Gondar (UOG), P.O. box 196, Gondar, Ethiopia
Tel +251-918-192721
Email [email protected]
Background: Tuberculosis presents a heightened threat to community health throughout the world but disproportionately afflicts low-income nations. In Ethiopia, TB is a significant health problem in children causing significant morbidity and mortality. Therefore, this study aimed to determine the prevalence, risk factors, and rifampicin resistance of pulmonary tuberculosis among children.
Methods: A hospital-based cross-sectional study was conducted on 384 children less than 15 years of age at Debre Markos Referral Hospital from February to May 2019. Sputum and gastric lavage samples were used to detect Mycobacterium tuberculosis and its rifampicin resistance pattern. MTB/RIF GeneXpert assay was used for the laboratory diagnosis.
Results: The prevalence of pulmonary tuberculosis and rifampicin resistance was 22 (5.73%) and 2 (0.52%), respectively. Educational status of the family (P = 0.02; AOR = 4.12; CI = 1.28– 13.15), residence (P = 0.04; AOR = 3.09; CI =1.05– 9.06), history of tuberculosis contact (P ≤ 0.001; AOR = 14.78; CI = 4.43– 49.26), HIV infection (P ≤ 0.001; AOR = 5.51; CI = 1.72– 17.7), malnourished status (P = 0.01; AOR = 4.11; CI = 1.33– 12.65), duration of cough greater than 3 weeks (P = 0.04; AOR = 3.2; CI = 11.05– 9.78), weight loss (P ≤ 0.001; AOR = 307.8; CI = 32– 2980), and children with mucoid sputum (P = 0.02; AOR = 3.76; CI = 1.2– 12.2) were significantly associated with tuberculosis infection.
Conclusion: This study showed a high prevalence of pulmonary tuberculosis infection among children. Residence, educational status of the family, contact history with tuberculosis cases, HIV, and malnutrition were risk factors for tuberculosis infection. Therefore, periodic surveillance of tuberculosis and assessing risk factors among children should be addressed. Moreover, a regular large scale survey should be conducted to assess the burden and intervene accordingly.
Keywords: tuberculosis, rifampicin resistance, children, Mycobacterium tuberculosis, MTB/RIF GeneXpert
Background
Tuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis. It primarily affects the lungs but can also affect the central nervous system, intestine, bone and joints, lymph glands, and other body tissues resulting in extra-pulmonary tuberculosis.1 TB can be transmitted by aerosol droplets generated by sputum positive patients with pulmonary tuberculosis.2,3 Children are among the chief victims of tuberculosis, suffering greater morbidity and mortality during early childhood than people at any other age in life.4–6 The World Health Organization (WHO) estimates that one-third of the world’s population is infected with TB and that 10 million new TB cases and 1.6 million deaths occurred in the world. Eighty percent of all cases were in 22 countries, mainly in Africa and Asia. Africa is the region with the highest burden of all forms of TB cases, and Ethiopia has a high rate of TB infection. The annual incidence of new TB cases was estimated to be 207/100,000, and the country is one of the 27 high multi-drug resistant tuberculosis (MDR-TB) countries with estimated 6200 MDR-TB patients each year.7,8
Pediatric tuberculosis represents the main public health concern worldwide.9,10 The World Health Organization reported that about 9 million people develop TB each year, and of whom about 1 million (11%) occur in children aged less than 15 years. Children contribute to 3–6% of the total TB caseload in developed countries and more than 25% of the burden of TB disease in developing countries. Nonetheless, pediatric TB has been relatively neglected for several years, mainly due to difficulties in Mycobacterium isolation in children.9 In 2017, an estimated 1 million children became ill with TB and 230,000 children died of TB (including children with Human Immunodeficiency Virus (HIV) associated TB).11 It is well known that childhood TB infection is facilitated by risk factors such as contact to the index case, HIV infection, malnutrition, young age, diabetes, indoor air pollution, alcohol, use of immunosuppressive drugs, tobacco smoke, behavioral and socioeconomic factors.12
Tuberculosis is among the top 10 causes of death among children worldwide, and millions of children are affected by TB.13 Childhood TB occurs in every part of the world, and the largest number of new childhood TB cases occurred in the South-East Asia and Western Pacific regions, with 62% of new TB cases, followed by the African region, with 25% of new TB cases. The African region has the largest number of children reported with tuberculosis infection, particularly from Sub-Saharan African countries. In 2017, 87% of new TB cases occurred in the 30 high TB burden countries. Eight countries; India, China, Indonesia, Philippines, Pakistan, Nigeria, Bangladesh, and South Africa accounted for two-thirds of the new TB cases.9 TB has always been highly prevalent in Ethiopia. According to the 2011 Ethiopian Ministry of Health (MOH) report, TB is the eighth leading cause of hospital admissions and the third leading cause of hospital deaths in Ethiopia, which presents Ethiopia as the seventh-highest TB burden country globally and ranks third in Africa.14
Tuberculosis is neglected in children by international and national policies and reports. This negligence leads to the lack of information regarding the epidemiology of pediatrics tuberculosis, drug resistance profile, and risk factors. However, pediatrics tuberculosis may be the hidden fire for future epidemics of tuberculosis since the bacteria can live for a longer time and until the child turned into an adult and able to produce productive sputum, which may play a role in the transmission of tuberculosis and also a scarcity of information on the epidemiology of pediatrics tuberculosis at a global and national level in general and in Debremarkos in particular. Hence, this study aimed to determine the prevalence, risk factors, and rifampicin resistance pulmonary TB among children at Debre Markos referral hospital.
Methods
Study Area
The study was conducted at Debre Markos referral hospital, East Gojjam, Amhara regional state, Northwest Ethiopia. The town serves as the capital city of the East Gojjam Administrative Zone. It is situated in the Northwest of the capital city of Ethiopia, Addis Ababa at a distance of 300 Km and located at 1020ʹN latitude and 3743ʹE longitude. The town has a total area of 6160 Km2 and its altitude ranges from 1302 to 17,000 m above sea level with an annual rainfall that falls from 1300 to 1380 mm. According to the Central Statical Agency of Ethiopia, Debremarkos town has an estimated population of 119,000 with a 97.07% Orthodox Christian by religion, while 1.7% of the populations are Muslims and 1.1% Protestant.15 The hospital provides health service to more than 3.5 million populations in its catchments, the hospital has 132 beds for inpatient and outpatient services.16
Study Design and Period
A cross-sectional study was conducted among children with less than 15 years of age of tuberculosis suspected patients at Debre Markos referral hospital from February to May 2019.
Source and Study Population
The source population for this study was all children less than 15 years of age seeking health services. The study population was all TB suspected children less than 15 years of age seeking health services at Debre Markos referral hospital during the study period. Study participants who were unable to give socio-demographic information and samples at the time of data collection were excluded.
Sample Size Determination and Sampling Technique
Single population proportion formula was used to calculate the sample size as follows: n = z2 p (1-p)/d2; where: n = the minimum required sample size; z = Standard normal distribution value at 95% CI, which is 1.96; P = the prevalence of childhood TB taken as 50%, since there is no previous report; d = the margin of error taken as 5%. n =  =
= = 384. The calculated sample size was 384. A convenience sampling technique was used and eligible participants during the study period were included in the study until the sample size 384 reached. The aims of the study and the benefits of participation were clearly explained to the participants before data collection. Participation was voluntarily and they have told them it is their right to withdraw from the study at any time during data collection. A questionnaire-based on known and possible factors was developed to explore the objectives of the study and pre-tested.
= 384. The calculated sample size was 384. A convenience sampling technique was used and eligible participants during the study period were included in the study until the sample size 384 reached. The aims of the study and the benefits of participation were clearly explained to the participants before data collection. Participation was voluntarily and they have told them it is their right to withdraw from the study at any time during data collection. A questionnaire-based on known and possible factors was developed to explore the objectives of the study and pre-tested.
Data Collection
The questionnaire was prepared in English then translated to the local language Amharic. Then, the socio-demographic characteristics, clinical information, and specimens were collected by face to face interview using a pretested structured questionnaire. HIV screening is done according to the Ethiopian national HIV test algorithm. An HIV test was done for each participant. For infants, HIV test was done by polymerase chain reaction (PCR) after collecting blood using a dry blood spot (DBS) method.
Assessment of Nutritional Status
The nutritional status of each child was determined by body mass index (BMI). The height and the weight of children were measured and the BMI determined by dividing weight to that of the height square. The nutritional status of the children was determined as underweight, normal weight, overweight or obese for a given height measurement using internationally recognized classifications published by the WHO (Underweight < 18.5; Normal range 18.5–24.99; Overweight 25–30; Obese > 30).17 Mid-upper arm circumference (MUAC) also used to determine nutritional status for children between 6 months and 5 years’ old who had malnutrition (wasting or thinness) by measuring the circumference of the left upper arm, measured at the mid-point between the tip of the shoulder and the tip of the elbow. If MUAC was <1.5 cm it is severe malnutrition, if it was between 11.5–12.4 cm it was moderate malnutrition if MUAC was >12.5 cm healthy.18
Sputum Collection
Sputum was obtained by expectoration method from children greater than 5 years of age who able to cooperate to provide purulent sputum by instructing the child to rinse his or her mouth with water before producing the specimen. Then, the child was told to take two deep breaths, holding the breath for a few seconds after each inhalation and then exhaling slowly. He or she was asked to breathe in the third time and then forcefully blow the air out by asking the child to breathe in again and then cough to produce purulent sputum from deep in the lungs. However, for children under 6 years of age and unable to provide purulent sputum, sputum induction was undertaken after a 2–3 h fast by a physician trained in this technique. Children were pretreated with 200 g salbutamol via a metered-dose inhaler with the attached spacer to prevent bronchoconstriction. A jet nebulizer that was attached to oxygen at a flow rate of 5 L per minute delivered 5 mL of 5% sterile saline for 15 minutes. Thereafter, chest percussion, vibration, or active breathing performed by a physician, and sample collection following spontaneous expectoration or suction of the naso-oropharynx.19
Gastric Lavage Collection
Gastric lavage was performed in the early morning after an overnight fast of at least 4 hours. A nasogastric tube was passed and normal saline 20 mL inserted, left for 3 minutes, and then aspirated. An additional 5–10 mL of normal saline was introduced and aspirated, until a minimum of 20 mL of aspirate was obtained. Then the gastric content was transferred into a sterile container, and the specimen container was wiped with alcohol to prevent cross-contamination, and transported to the laboratory as soon as possible within 4 hours.19
Sample Processing and Laboratory Detection
Specimens were decontaminated and processed using standardized protocols and quality assurance procedures provided by the manufacture. Following decontamination with N-acetyl-L-cysteine and sodium hydroxide, samples were then mixed with sample reagent for liquefaction and inactivation in a ratio of 2:1 before being transferred into a pre-labeled cartridge, which was then inserted into an Xpert MTB/Rif machine. The Xpert MTB/RIF purifies and concentrates Mycobacterium tuberculosis complex bacilli from sputum samples, isolates genomic material from the captured bacteria by sonication, and subsequently amplifies and detects the genomic DNA by PCR. Xpert MTB/Rif test was considered positive if MTB was detected. Repeat Xpert MTB/Rif tests were done for indeterminate results. Rifampicin resistance inducing mutations in the RNA polymerase beta (rpoB) gene in the Mycobacterium tuberculosis genome in a real-time format using fluorescent-labeled probes (molecular beacons).20,21
Data and Laboratory Quality Control
Data quality was maintained by pretesting the questionnaire as well as training of the data collector and research assistant. Data also checked for completeness, accuracy, consistency, and clarity. The MTB/RIF Genexpert assay was monitored by two internal quality control proper test controls. First, the sample processing control (SPC) ensures adequate processing and monitors the presence of inhibition. Second, the Probe check control (PCC) verifies that the steps of the tests (rehydration, filling of the cartridge, etc.) take place correctly. When there was an inadequate sample, the presence of inhibiter as well as error in sample processing, the Genexpert automatically reject the specimens.
Data Entry, Analysis and Interpretation
Data was entered into Epidemiological Information (EPI-Info) version-7 to check data completeness and clearance, then transferred to SPSS version-20 for analysis. The characteristics of the study populations were summarized using frequencies, mean, and standard deviation. Bivariate and multivariate analysis used to determine the strength of the association between variables. The adjusted odds ratio computed using multivariate logistic regression for variables with p-value < 0.2 to control the effect of confounding variables. P-value < 0.05 was considered statistically significant at 95% confidence interval.
Results
Socio-Demographic and Clinical Characteristics of Children
In this study, a total of 384 children were included. Out of these, 51% (196/384) were males, and the mean age of the children was 8.56 years with SD of ± 3.91 with an age range of 0–15 years. Most of the children, 39.06% (150/384) belonged to 6–10 years of age while 34.11% (131/384) belonged to 11–15 years of age. The majority, 51.04% (196/384) children were from rural residents while the rest, 48.96% (188/384) from an urban area. Forty-nine percent of children attend education while the rest, 51% did not. Clinical characteristics of children showed that 236 (61.46%) had fever, 88 (22.92%) night sweat, 168 (43.75%) weight loss, 229 (59.64%) loss of appetite, and 384 (100%) had a cough for more than three weeks. In this study, 157 (40.9%) children delivered muco-salivary sputum, 124 (32.3%) gave mucoid sputum, and 103 (26.8%) gave gastric lavage sample (Table 1).
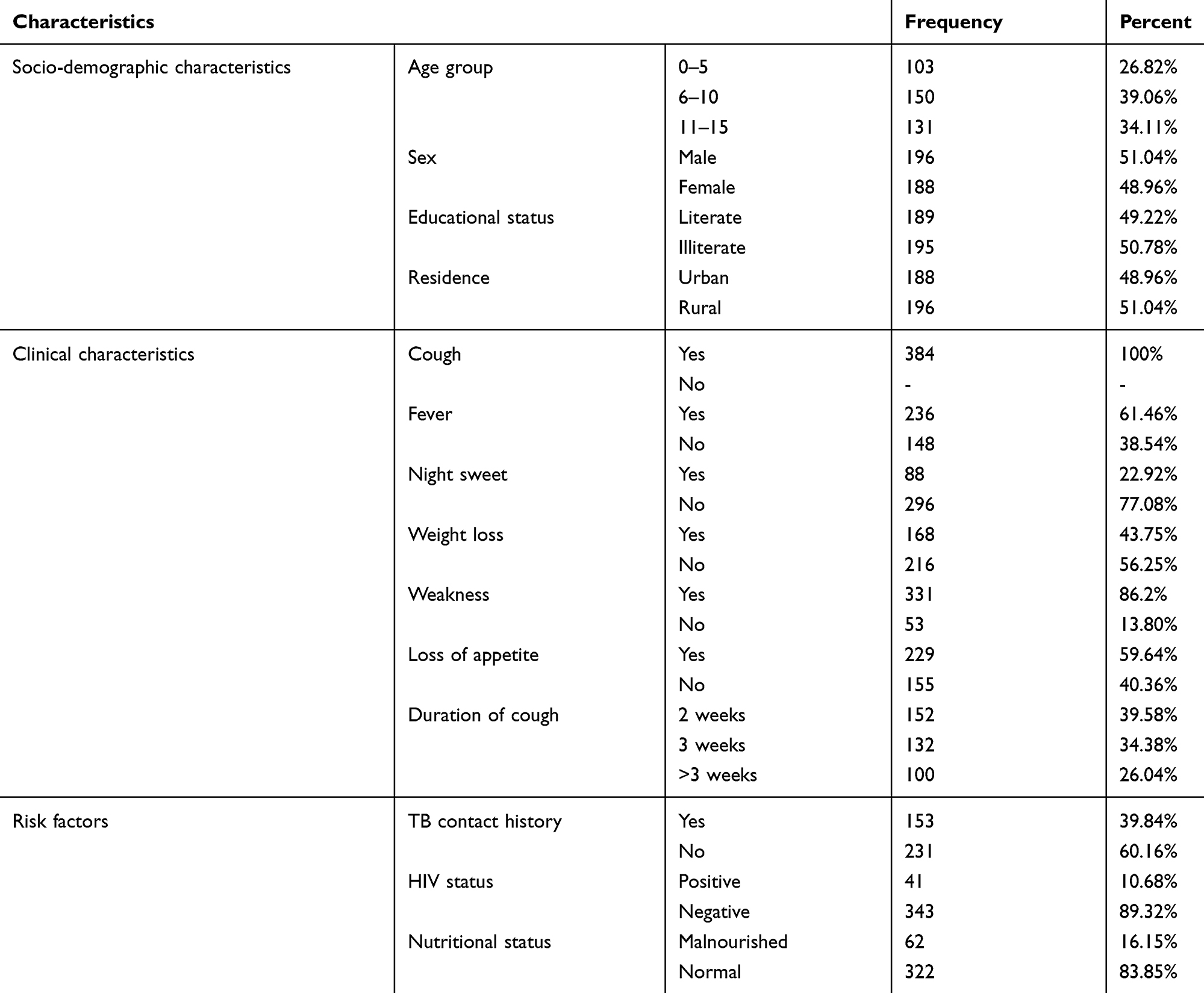 |
Table 1 Frequency of Socio-Demographic Characteristics, Clinical Characteristics, and Risk Factors of TB Suspected Children Under 15 Years of Age (N =384) at Debremarkos Referral Hospital, Northwest Ethiopia, February - May, 2019 |
Frequency of Risk Factors Among Children
Risk factor assessment showed that 153 (39.84%) children had history of contact with TB patients, 22 (5.73%) had history of anti-TB treatment, 41 (10.68%) were HIV positive, and 62 (16.15%) children were malnourished. In this study, being illiterate (P = 0.02; AOR = 4.12; CI = 1.28–13.15), being rural in residence (P = 0.04; AOR = 3.09; CI =1.05–9.06), history tuberculosis contact (P ≤ 0.001; AOR =14.78; CI = 4.43–49.26), HIV infection (P ≤ 0.001; AOR = 5.51; CI = 1.72–17.7), being malnourished (P = 0.01; AOR = 4.11; CI = 1.33–12.65) and duration of cough greater than 3 weeks (P = 0.04; AOR =3.2; CI =11.05–9.78) were a significant risk factors for childhood tuberculosis (Table 2). Moreover, children had fever (P ≤ 0.001; AOR = 12.19; CI = 3.05–48.7), night sweat (P ≤ 0.001; AOR =15.24; CI = 4.2–55.22), weight loss (P ≤ 0.001; AOR =307.8; CI = 32–2980), loss of appetite (P = 0.01; AOR = 10.32; CI = 2.5–42.2) and children with mucoid sputum (P = 0.02; AOR = 3.76; CI = 1.2–12.2) were also significantly associated with childhood tuberculosis (Table 3).
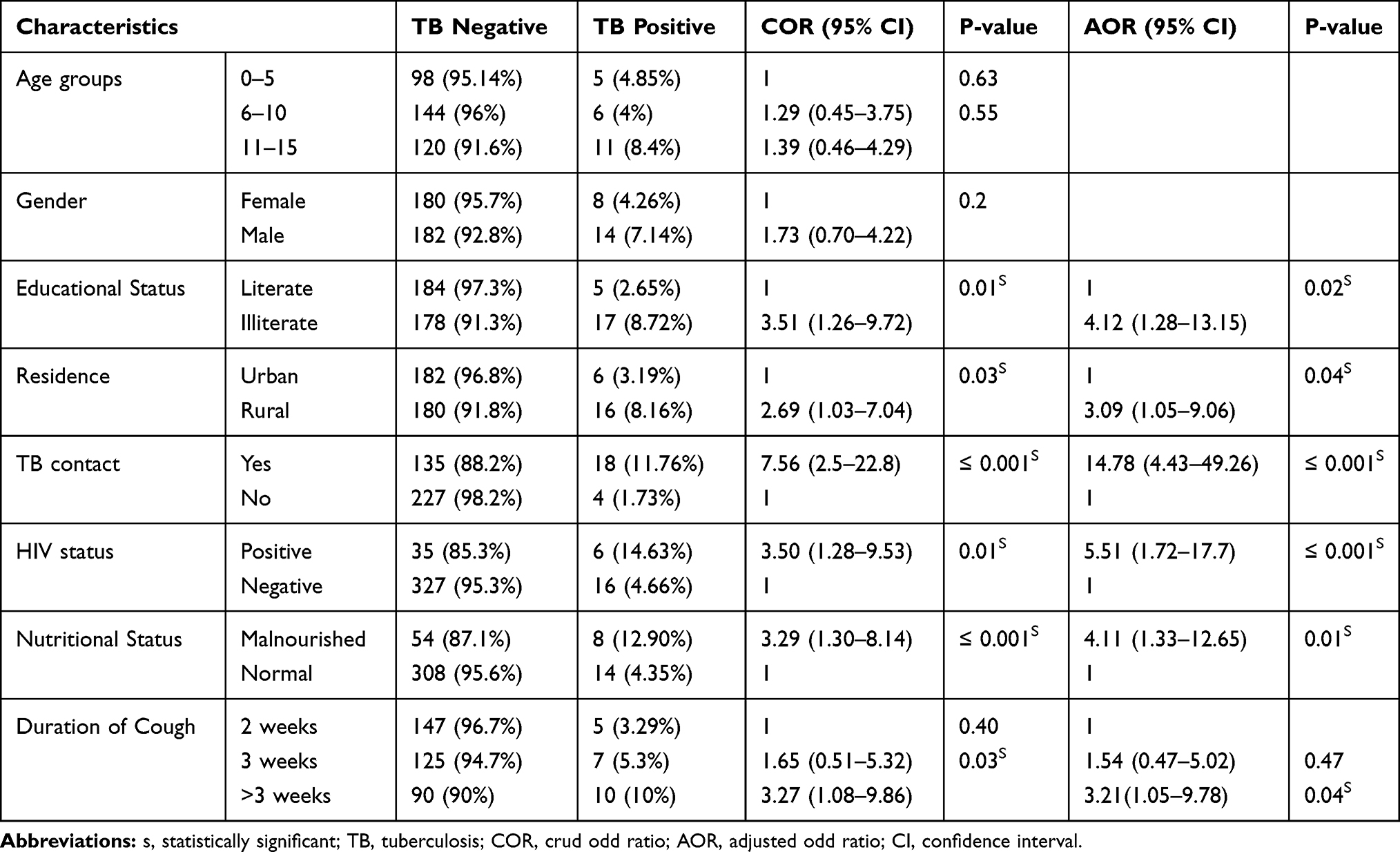 |
Table 2 Bivariate and Multivariate Analysis (N=384) That Shows the Relationship Between Risk Factors and Prevalence of Pulmonary Tuberculosis at Debremarkos Referral Hospital, Northwest Ethiopia, February – May, 2019 |
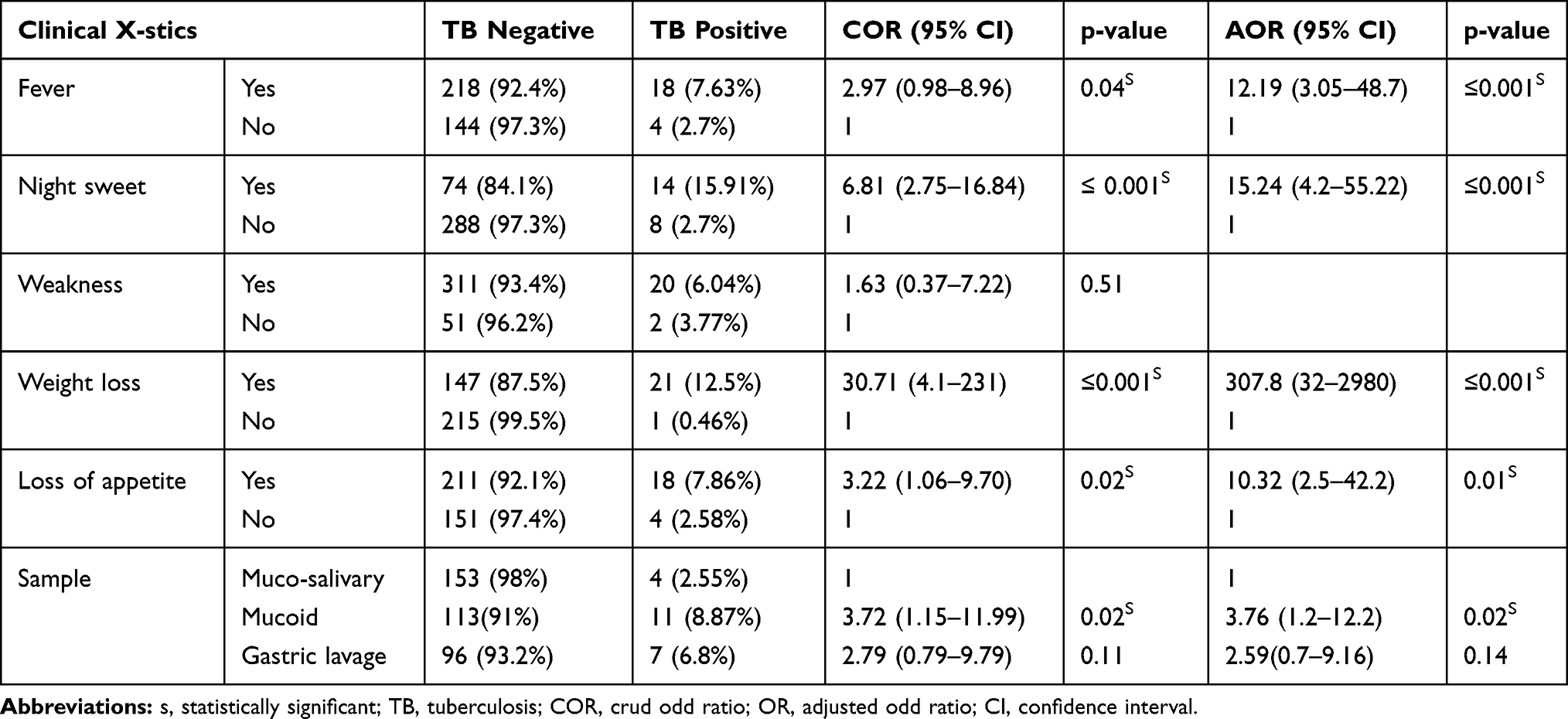 |
Table 3 Bivariate and Multivariate Analysis (N=384) That Shows the Relationship Between Clinical Characteristics and Prevalence of Pulmonary Tuberculosis at Debremarkos Referral Hospital, Northwest Ethiopia, February–May, 2019 |
Prevalence of Mycobacterium tuberculosis and Its Rifampicin Resistance
The prevalence of pulmonary tuberculosis among children was 22 (5.73%), and two (0.52%) of them were rifampicin-resistant. The prevalence of pulmonary tuberculosis among different age categories of children showed 5 (4.85%), 6 (4%), and 11 (8.4%) among the age groups 0–5, 6–10, and 11–15 years, respectively. The proportion of pulmonary tuberculosis among male children was 14 (7.14%), but 8 (4.26%) among females which shows that males are almost 2 times more likely to acquire pulmonary tuberculosis than females, but no statistically significant association between pulmonary tuberculosis with sex. The proportion of pulmonary tuberculosis among urban and rural children was 6 (3.19%) and 16 (8.16%), respectively. Data also showed a statistically significant association between pulmonary tuberculosis and residence [P = 0.04; AOR = 3.09 (95% CI).
The prevalence of pulmonary tuberculosis among children that attend education was 5 (2.65%), but 17 (8.72%) among children that did not attend [P = 0.01; AOR = 4.12, 95% CI: 1.28–13.15]. The prevalence of pulmonary tuberculosis among children that had a history of contact with TB patients was 18 (11.76%). Children that had a history of TB contact were almost 14.78 times at higher risk for pulmonary tuberculosis than those that had no TB contact history [P ≤ 0.001; AOR = 14.78, 95% CI: 4.43–49.26]. The prevalence of pulmonary tuberculosis among HIV positive children was 6 (14.63%), but 16 (4.66%) among HIV negatives. Moreover, data also showed a statistically significant association between pulmonary tuberculosis and HIV infection (P = 0.01). The odds of acquiring pulmonary tuberculosis among HIV positive children were 5.51 times higher than HIV negatives [AOR = 5.51, 95% CI: 1.72–17.7].
Data of the current study also showed a prevalence of pulmonary tuberculosis among malnourished children is 8 (12.9%), but 14 (4.35%) among children with normal BMI. A statistically significant association between the prevalence of pulmonary tuberculosis with that of malnutrition status (P = 0.01) was observed. Malnourished children were almost four times at risk for pulmonary tuberculosis than children with normal BMI [AOR = 4.11, 95% CI: 1.33–12.65]. According to this study children who had fever had 12.19 times higher TB occurrence than those had no fever [AOR = 12.19; 95% CI: 3.05–48.7, p-value ≤ 0.001]. Based on data of this study, a child who had night sweat had 15.24 times the occurrence of TB than those had not [AOR = 15.24; 95% CI: 4.2–55.22, p-value ≤ 0.001]. The prevalence of tuberculosis in children who had weight loss is 307.8 times higher than those who did not loss their weight, [AOR = 307.8 (31.79–2979.89, p ≤ 0.001)].
Discussion
Childhood tuberculosis has been relatively neglected, mainly due to many challenges in diagnosis and lower priority given to childhood tuberculosis by TB control programs. It is particularly evident in developing countries with poor public health infrastructure.22 Mycobacterium tuberculosis causes much morbidity and mortality in children all over the world due to many predisposing risk factors that contribute to the transmission and development of the disease tuberculosis.23–27 Some of these risk factors are the presence of index cases, HIV infection, malnutrition, and others.28–30 Drug-resistant TB (DRTB) is also emerging, which causes higher morbidity and mortality in children than drug-susceptible TB. Rifampicin resistant TB is one of the DRTB that affects every part of the world.31–33
In this study, the prevalence of pulmonary tuberculosis among children is 5.73% (22/384), which is similar to the finding in Tanzania (5.2%).34 However, it is higher than the findings reported in Zambia (1.58%),35 Mozambique (1.65),36 South Africa (1.3%),37 and lower than reports from India (15%),38 Zimbabwe (8.7%),39 Greenland (8.5%),40 South Africa (13%),41 Uganda (10%),42 Ethiopia (13.6%),43 Bangladesh (32.97%)44 and Nigeria (32%).45 The reason for variation might be due to the difference in the prevalence of tuberculosis in the general population, methods of sputum sample collection and diagnosis. While we used only Xpert MTB/RIF assay, the other study applied microscopy and culture.
Rifampicin resistant TB isolates found by gene Xpert were strong predictors of MDR-TB, and the existence of rifampicin-resistant TB is a serious health problem since children can acquire infection independently in the community. Therefore, molecular typing of isolates from pediatrics TB patients and their potential contacts is essential to determine the source of transmission. The prevalence of rifampicin-resistant pulmonary tuberculosis infection in this study is 0.52%, which is in line with the finding reported in India (0.66%).46 However, it is lower than the findings reported in Ethiopia (7.9%),43 South Africa (22.2%),47 and China (30%).48 The discrepancy might be due to variations like study populations, study setting, study design, and socio-cultural practice.
According to our study, being rural in residence was identified as an independent risk factor for tuberculosis, which shows a significant difference (P = 0.003) of tuberculosis prevalence among children living in rural (8.16%) and urban (3.19%). The odds of acquiring pulmonary tuberculosis was almost three times higher among children living in rural settings compared with that of the urban dwellers [AOR =3.09, 95% CI: 1.05–9.06]. This finding is in agreement with the report from a previous study in India,49 and it might be due to low socioeconomic status and high illiterate families in a rural setting. The prevalence of pulmonary tuberculosis among children with literates and illiterate’s families was 2.65%, 8.72%%, respectively [AOR = 3.51, 95% CI: 1.26–9.72], and the difference was statistically significant (P = 0.02). Children from illiterate’s families were 3.51 times more at risk of developing the disease tuberculosis. The high prevalence of childhood tuberculosis among children with illiterate families might be due to low awareness about TB transmission and risk factors that make the child at risk of acquiring TB. This finding also supported by reports from Bangladesh (RR = 3.12)50 and Brazil (OR = 3.7).51
In this study, the prevalence of pulmonary tuberculosis among children who had a history of contact with TB patients is 11.76% (AOR=14.78, 95% CI: 4.43–49.26), which is higher than those who had not a history of TB contact. HIV-infected children were 14.78 times more likely to have TB disease than uninfected ones. A study in South Africa,37 Ethiopia52, and India53 indicated that contact history with known TB-infected patients is a source of TB. The prevalence of pulmonary tuberculosis was higher among HIV-positive children (14.63%) compared with HIV negatives (4.66%) (AOR = 5.51, 95% CI: 1.72–17.7), and the difference was statistically significant (P = 0.00). The difference might be due to HIV infected children is very susceptible to develop active tuberculosis diseases due to waned immunity.
The prevalence of tuberculosis among malnourished and non-malnourished children was 12.90% and 4.35%, respectively with AOR = 4.11 (p = 0.01, 95% CI: 1.33–12.65). The prevalence of malnutrition (16.15%) among children in the current study is less than a study in Boston, USA (29%).54 Malnourished children were 4.11 times more at risk of acquiring the disease tuberculosis as compared with normal nutritional status. The difference due to the immunocompromization of malnourished children, which contributes to the conversion of latent tuberculosis to active tuberculosis cases. The prevalence of TB/HIV co-infection (14.63%) in this study almost comparable with a study conducted in Uganda.42 However, it is lower than a report in Mozambique (44%).36 Children living with human immunodeficiency virus were 5.51 times more at risk of acquiring the disease tuberculosis in comparison with those without HIV infection. TB/HIV co-infection variability among different studies might be due to variation in risk for HIV acquisition, method of diagnosis, study setting, or TB control practice.
Production of mucoid sputum, cough more than two weeks, loss of appetite, weight loss, night sweat, and fever are among the clinical signs and symptoms from patients who are presumptive pulmonary tuberculosis. In the present study, loss of appetite, weight loss, night sweat, fever, and production of mucoid sputum were significant clinical features of patients in the multivariate analysis. Weight loss symptoms are common in the general pediatric population, and it was significantly more common in children with newly diagnosed tuberculosis. Children who lost their weight had 307.8 times higher TB occurrence than those who did not lose weight. This study in agreement with a report in South Africa.37
Strength and Limitations of the Study
Studying neglected vulnerable children is the tough side of this study, which able to address the information gap on the prevalence of TB, rifampicin-resistant patterns, and risk factors among children. However, this study did not address extra-pulmonary TB, drug-resistant tests for anti-Mycobacterium drugs other than rifampicin.
Conclusions and Recommendations
Active tuberculosis and drug-resistant tuberculosis are prevalent in children. Risk factors such as TB contact history, HIV, and malnutrition are associated with pulmonary tuberculosis among children. Therefore, efforts must be undertaking to control and eliminate this fatal disease, and further studies should be studied to address the burden, risk factors, and drug-resistant pattern of tuberculosis in the study area.
Abbreviations
AOR, adjusted odds ratio; BMI, body mass index; CI, confidence interval; CSA, Central Statistical Agency; DBS, dry blood test; DNA, deoxyribonucleic acid; DR-TB, drug resistant tuberculosis; HIV, human immunodeficiency virus; MDR-TB, multi drug resistant; MOH, Ministry of Health; MTB, Mycobacterium tuberculosis; MUAC, mid upper arm circumference; PCC, probe check control; PCR, polymerase chain reaction; RR-TB, rifampicin resistant tuberculosis; RIF, rifampicin; RNA, ribonucleic acid; SPC, sample processing control; SPSS, Statistical Package for Social Science; TB, tuberculosis; WHO, World Health Organization.
Data Sharing Statement
All data generated or analyzed during this study were included in this manuscript. Data that support the findings of this study are also available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted by following the principles of the Declaration of Helsinki. Ethical clearance was obtained from the University of Gondar ethical review committee, and written permission was obtained from Debremarkos referral hospital administration. Before the enrolment of a patient in the study, written informed consent was obtained from parents or legal guardians. Additionally, the confidentiality of information was assured. Each confirmed TB case/positive findings were linked to TB OPD/healthy institutions to begin anti-TB treatment.
Consent for Publication
Not applicable
Acknowledgments
We would like to thank the University of Gondar and study participants for the support given to conduct this study. We were also very grateful to thank all the health professionals and laboratory technicians working at Debremarkos hospital for all the support they gave us during the data collection and laboratory investigations.
Author Contributions
All authors contributed equally to the conception, drafting, study design, execution, acquisition, analysis, and interpretation of data, write up and critically reviewing of the manuscript; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Qazi SA, Khan S, Khan MA. Epidemiology of childhood tuberculosis in a hospital setting. J Pak Med Assoc. 2012;1:164–167.
2. Perez-Velez CM, Marais BJ. Tuberculosis in children. N Engl J Med. 2012;367(4):348–361. doi:10.1056/NEJMra1008049
3. Kumar NP, Anuradha R, Andrade BB, et al. Circulating biomarkers of pulmonary and extrapulmonary tuberculosis in children. Clin. Vaccine Immunol. 2013;20(5):704–711. doi:10.1128/CVI.00038-13
4. Blount RJ, Tran B, Jarlsberg LG, et al. Childhood tuberculosis in northern Viet Nam: a review of 103 cases. PLoS One. 2014;9(5):1–8. doi:10.1371/journal.pone.0097267
5. Bolursaz MR, Khalilzadeh S, Baghaie N, et al. and radiographic findings of pulmonary tuberculosis in infants. J Comprehensive Pediatrics. 2013;4(4):170–174. doi:10.17795/compreped-14337
6. Peter R. Donald: A Brief History of Childhood Tuberculosis. Vol. 1. Oxford University Press; 2015:1–5.
7. Bogale S, Diro E, Shiferaw AM, Yenit MK. Factors associated with the length of delay with tuberculosis diagnosis and treatment among adult tuberculosis patients attending at public health facilities in Gondar town, Northwest, Ethiopia. BMC Infect Dis. 2017;17(1):145. doi:10.1186/s12879-017-2240-0
8. WHO. World Health Organization Global Tuberculosis Report, 2015. Geneva, Switzerland; 2015. Available from: https://apps.who.int/iris/handle/10665/191102.
9. Berti E, Galli L, Venturini E, de Martini M, Chiappini E. Tuberculosis in childhood: a systematic review of national and international guidelines. BMC Infect Dis. 2014;14(1):S3. doi:10.1186/1471-2334-14-S1-S3
10. Swaminathan S, Rekha B. Pediatric tuberculosis: global overview and challenges. Clin Infect Dis. 2010;50(3):184–194. doi:10.1086/651490
11. Glaziou P, Sismanidis C, Floyd K, Raviglione M. Global epidemiology of tuberculosis. Cold Spring Harb Perspect Med. 2015;5(2):a017798. doi:10.1101/cshperspect.a017798
12. Narasimhan P, Wood J, MacIntyre CR, Mathai D. Risk factors for tuberculosis. Pulm Med. 2013;2013:1–11. doi:10.1155/2013/828939
13. Hamzaoui A, Yaalaoui S, Cherif FT, Saidi LS, Berraies A. Childhood tuberculosis: a concern of the modern world. Eur Respir Rev. 2014;23(133):278–291. doi:10.1183/09059180.00005314
14. Acosta CD, Rusovich V, Harries AD, Ahmedov S, van den Boom M, Dara M. A new roadmap for childhood tuberculosis. Lancet Global Health. 2014;2(1):15–17. doi:10.1016/S2214-109X(13)70153-0
15. Deress T, Hassen F, Adane K, Tsegaye A. Assessment of knowledge, attitude, and practice about biomedical waste management and associated factors among the healthcare professionals at Debre Markos Town healthcare facilities, Northwest Ethiopia. J Environ Public Health. 2018;2018.
16. Esmael A, Tsegaye G, Wubie M, Endris M. Tuberculosis and human immune deficiency virus co-infection in debre markos referral hospital in northwest ethiopia: a five years retrospective study. J AIDS Clin Res. 2013;4:263. doi:10.4172/2155-6113.1000263
17. Nuttall FQ; BMI. Body Mass Index. Nutr Today. 2015;50(3):117–128.
18. Saeed HA, Mogendi JB, Akparibo R, Kolsteren P. Reliability of mid-upper arm circumference measurements taken by community health nurses. Curr Res Nutri Food Sci J. 2015;3(1):26–35. doi:10.12944/CRNFSJ.3.1.04
19. Binod Lal B, Kedar Narsign KC. National childhood TB management guideline. Government of nepal ministry of health department of health service national tuberculosis centre. Nepal Med Coll J. 2012;13(2):58–61.
20. Dorman SE, Schumacher SG, Alland D, et al. Xpert MTB/RIF Ultra for detection of Mycobacterium tuberculosis and rifampicin resistance: a prospective multicentre diagnostic accuracy study. Lancet Infect Dis. 2018;18(1):76–84.
21. Kebede A, Beyene D, Yenew B, et al. Monitoring quality indicators for the Xpert MTB/RIF molecular assay in Ethiopia. PLoS One. 2019;14(11):e0225205. doi:10.1371/journal.pone.0225205
22. Brent AJ. Childhood TB surveillance: bridging the knowledge gap to inform policy. J Trop Med. 2012;1:1–5. doi:10.1155/2012/865436
23. Tsai KS, Chang HL, Chien ST, et al. Childhood tuberculosis: epidemiology, diagnosis, treatment, and vaccination. Pediatr Neonatol. 2013;54(5):295–302. doi:10.1016/j.pedneo.2013.01.019
24. Jenkins HE. Global burden of childhood tuberculosis. Pneumonia. 2016;8(1):24. doi:10.1186/s41479-016-0018-6
25. Dangisso MH, Datiko DG, Lindtjørn B. Low case notification rates of childhood tuberculosis in southern Ethiopia. BMC Pediatr. 2015;15(1):142. doi:10.1186/s12887-015-0461-1
26. Marais BJ, Gupta A, Starke JR, El Sony A. Tuberculosis in women and children. The Lancet. 2010;375(9731):2057–2059. doi:10.1016/S0140-6736(10)60579-X
27. Jubulis J, Kinikar A, Ithape M, et al. Modifiable risk factors associated with tuberculosis disease in children in Pune, India. Int J Tuberculosis Lung Dis. 2014;18(2):198–200. doi:10.5588/ijtld.13.0314
28. Jaganath D, Mupere E. Childhood tuberculosis and malnutrition. J Infect Dis. 2012;206(12):1809–1815. doi:10.1093/infdis/jis608
29. Cruz AT, Starke JR. Pediatric tuberculosis. Pediatrics Rev. 2010;31(1):13. doi:10.1542/pir.31-1-13
30. Ettehad D, Schaaf HS, Seddon JA, Cooke GS, Ford N. Treatment outcomes for children with multidrug-resistant tuberculosis: a systematic review and meta-analysis. Lancet Infect Dis. 2012;12(6):449–456. doi:10.1016/S1473-3099(12)70033-6
31. Schaaf HS, Marais BJ. Management of multidrug-resistant tuberculosis in children: a survival guide for paediatricians. Paediatr Respir Rev. 2011;12(1):31–38. doi:10.1016/j.prrv.2010.09.010
32. Dodd PJ, Sismanidis C, Seddon JA. Global burden of drug-resistant tuberculosis in children: a mathematical modelling study. Lancet Infect Dis. 2016;16(10):1193–1201. doi:10.1016/S1473-3099(16)30132-3
33. Schnippel K, Shearer K, Evans D, Berhanu R, Ndjeka N. Predictors of mortality and treatment success during treatment for rifampicin-resistant tuberculosis within the South African National TB Programme, 2009 to 2011: a cohort analysis of the national case register. Int J Infect Dis. 2015;1(39):89–94. doi:10.1016/j.ijid.2015.09.002
34. Li N, Manji KP, Spiegelman D, et al. Incident tuberculosis and risk factors among HIV-infected children in Tanzania. AIDS. 2013;27(8):1273–1281. doi:10.1097/QAD.0b013e32835ecb24
35. Munthali T, Chabala C, Chama E, et al. Tuberculosis caseload in children with severe acute malnutrition related with high hospital based mortality in Lusaka, Zambia. BMC Res Notes. 2017;10(1):206. doi:10.1186/s13104-017-2529-5
36. López-Varela E, Augusto OJ, Gondo K, et al. Incidence of tuberculosis among young children in rural Mozambique. Pediatr Infect Dis J. 2015;34(7):686–692. doi:10.1097/INF.0000000000000710
37. Marais BJ, Obihara CC, Gie RP, et al. The prevalence of symptoms associated with pulmonary tuberculosis in randomly selected children from a high burden community. Arch Dis Child. 2005;90(11):1166–1170. doi:10.1136/adc.2004.060640
38. Shaikh N, Gupte A, Dharmshale S, et al. Novel interferon-gamma assays for diagnosing tuberculosis in young children in India. Int J Tuberc Lung Dis. 2017;21(4):412–419. doi:10.5588/ijtld.16.0428
39. Chipinduro M, Mateveke K, Makamure B, Ferrand RA, Gomo E. Stool Xpert® MTB/RIF test for the diagnosis of childhood pulmonary tuberculosis at primary clinics in Zimbabwe. Int J Tuberc Lung Dis. 2017;21(2):161–166. doi:10.5588/ijtld.16.0357
40. Seddon JA, Hesseling AC, Godfrey-Faussett P, Fielding K, Schaaf HS. Risk factors for infection and disease in child contacts of multidrug-resistant tuberculosis: a cross-sectional study. BMC Infect Dis. 2013;13(1):392.
41. Nicol MP, Workman L, Isaacs W, et al. Accuracy of the Xpert MTB/RIF test for the diagnosis of pulmonary tuberculosis in children admitted to hospital in Cape Town, South Africa: a descriptive study. Lancet Infect Dis. 2011;11(11):819–824. doi:10.1016/S1473-3099(11)70167-0
42. Jaganath D, Zalwango S, Okware B, et al. Contact investigation for active tuberculosis among child contacts in Uganda. Clin Infect Dis. 2013;57(12):1685–1692. doi:10.1093/cid/cit645
43. Arega B, Menbere F, Getachew Y. Prevalence of rifampicin resistant Mycobacterium tuberculosis among presumptive tuberculosis patients in selected governmental hospitals in Addis Ababa, Ethiopia. BMC Infect Dis. 2019;19(1):307.
44. Sultana AT, Gathia R, Huda MM, Begum JA, Amin MR. Pattern of childhood tuberculosis among the patients admitted in Dhaka Shishu (Children) Hospital. Northern Int Med Coll J. 2017;8(2):213–215. doi:10.3329/nimcj.v8i2.32552
45. Attah CJ, Oguche S, Egah D, Ishaya TN, Banwat M, Adgidzi AG. Risk factors associated with paediatric tuberculosis in an endemic setting. Alexandria J Med. 2018;1:1–6.
46. Hesseling AC, Kim S, Madhi S, et al. High prevalence of drug resistance amongst HIV-exposed and-infected children in a tuberculosis prevention trial. TInt J Tuberculosis Lung Dis. 2012;16(2):192–195. doi:10.5588/ijtld.10.0795
47. Dodd PJ, Gardiner E, Coghlan R, Seddon JA. Burden of childhood tuberculosis in 22 high-burden countries: a mathematical modelling study. Lancet Global Health. 2014;2(8):e453–9. doi:10.1016/S2214-109X(14)70245-1
48. Jiao W, Liu Z, Han R, et al. Prevalence of drug resistant Mycobacterium tuberculosis among children in China. Tuberculosis. 2015;95(3):315–320. doi:10.1016/j.tube.2015.02.041
49. Rao VG, Bhat J, Yadav R, et al. Prevalence of pulmonary tuberculosis - a baseline survey In Central India. PLoS One. 2012;7(8):1–6.
50. Karim MR, Rahman MA, Mamun SA, Alam MA, Akhter S. What cannot be measured cannot be done; risk factors for childhood tuberculosis: a case control study. Bangladesh Med Res Counc Bull. 2012;38(1):27–32. doi:10.3329/bmrcb.v38i1.10449
51. Stevens H, Ximenes RA, Dantas O, Rodrigues LC. Risk factors for tuberculosis in older children and adolescents: a matched case– control study in Recife. Braz Licensee BioMed Central. 2014;1:1–4.
52. Braitstein P, Nyandiko W, Vreeman R, et al. The clinical burden of tuberculosis among human immunodeficiency virus-infected children in Western Kenya and the impact of combination antiretroviral treatment. Pediatr Infect Dis J. 2009;28(7):626–632. doi:10.1097/INF.0b013e31819665c5
53. Singh M. Prevalence and risk factors for transmission of infection among children in household contact with adults having pulmonary tuberculosis. Arch Dis Child. 2005;90(6):624–628. doi:10.1136/adc.2003.044255
54. Drobac PC, Mukherjee JS, Joseph JK, et al. Community-based therapy for children with multidrug-resistant tuberculosis. Pediatrics. 2006;117(6):2022–2029. doi:10.1542/peds.2005-2235
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.