Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
Prevalence and Risk Factors of Chronic Obstructive Pulmonary Disease Among Agriculturists in a Rural Community, Central Thailand
Authors Kitjakrancharoensin P ![]() , Yasan K, Hongyantarachai K, Ratanachokthorani K, Thammasarn J, Kuwuttiwai D, Ekanaprach T, Jittakarm R, Nuntapravechpun R, Hotarapavanon S, Kulrattanarak S, Tongkaew S
, Yasan K, Hongyantarachai K, Ratanachokthorani K, Thammasarn J, Kuwuttiwai D, Ekanaprach T, Jittakarm R, Nuntapravechpun R, Hotarapavanon S, Kulrattanarak S, Tongkaew S ![]() , Deemeechai S, Mungthin M, Rangsin R
, Deemeechai S, Mungthin M, Rangsin R ![]() , Wongsrichanalai V
, Wongsrichanalai V ![]() , Sakboonyarat B
, Sakboonyarat B
Received 16 May 2020
Accepted for publication 31 August 2020
Published 15 September 2020 Volume 2020:15 Pages 2189—2198
DOI https://doi.org/10.2147/COPD.S262050
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Peranut Kitjakrancharoensin,1 Kittipong Yasan,1 Kwanjira Hongyantarachai,1 Kanoot Ratanachokthorani,1 Jutinun Thammasarn,1 Dantham Kuwuttiwai,1 Thunpimol Ekanaprach,1 Rawisut Jittakarm,1 Rungroj Nuntapravechpun,1 Sirasih Hotarapavanon,1 Spain Kulrattanarak,1 Sarisa Tongkaew,1 Sirivimon Deemeechai,1 Mathirut Mungthin,2 Ram Rangsin,3 Virissorn Wongsrichanalai,4 Boonsub Sakboonyarat3
1Phramongkutklao College of Medicine, Bangkok, Thailand; 2Department of Pharmacology, Phramongkutklao College of Medicine, Bangkok, Thailand; 3Department of Military and Community Medicine, Phramongkutklao College of Medicine, Bangkok, Thailand; 4Department of Medicine, Phramongkutklao College of Medicine, Bangkok, Thailand
Correspondence: Boonsub Sakboonyarat
Department of Military and Community Medicine, Phramongkutklao College of Medicine, Bangkok 10400, Thailand
Tel +66 859545955
Email [email protected]
Purpose: The present study aimed to determine the prevalence and risk factors of chronic obstructive pulmonary disease (COPD) among agriculturists in a remote rural community in central Thailand.
Methods: A cross-sectional study was conducted in January 2020. Face-to-face interviews were conducted using standardized questionnaires to determine demographic characteristics and risk behaviors. COPD was defined by the spirometric criterion for airflow limitation constituting a postbronchodilator fixed ratio of FEV1/FVC < 0.70 following the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines 2019. Multivariable logistic regression analysis was used to determine the risk factors for COPD, and the magnitude of association was presented as adjusted odds ratio (AOR) with 95% confidence interval (95% CI).
Results: A total of 546 agriculturists were enrolled in the study. The overall prevalence of COPD was 5.5% (95% CI: 3.6– 7.4). The prevalence of COPD among males was 8.0% (95% CI: 4.7– 11.3), and 3.2% (95% CI: 1.1– 5.2) among females. The risk factors of COPD included age ≥ 60 years old (AOR 2.7, 95% CI: 1.1– 7.0), higher intensity of smoking (AOR 1.1, 95% CI: 1.0– 1.1), swine farm worker (AOR 4.1, 95% CI: 1.7– 10.3), cattle farm worker (AOR 3.3, 95% CI: 1.4– 8.2) and home cooking (AOR 2.7, 95% CI: 0.8– 9.7).
Conclusion: Our data emphasized that COPD was one of the significant health problems among agriculturists in a rural community. Agricultural jobs such as animal farmers and behavioral factors such as smoking were associated with COPD. Effective public health interventions, especially, modifying risk behaviors, should be promoted in remote rural areas to prevent the disease and reduce its morbidity and mortality.
Keywords: COPD, farmers, swine, cattle, smoking, Thailand
Introduction
Chronic obstructive pulmonary disease (COPD) is an under-recognized health problem and the leading cause of morbidity and mortality worldwide.1 Projections of global COPD mortality in 2030 involved approximately 7.4% of total deaths making it the fourth leading cause of death.2 A recent review demonstrated that the estimated prevalence of COPD was 12.2% overall, 15.7% among males and 9.9% among females.3 In Thailand, the national prevalence of COPD was 2.1% in 1999 and is projected to total 7.0% in 2010.4
COPD is a principle condition leading to several serious complications, ie, cor pulmonale, recurrent pneumonia, pneumothorax and respiratory failure.5–8 Although the pathogenic mechanisms of COPD remain unclear, various risk factors such as genetic constitution, bronchial hyper-responsiveness, perinatal factors, childhood asthma, air pollution and cigarette smoking were identified to cause the disease.6–8 In addition, COPD is considered a common occupational disease in particular populations including tunnel workers,9 coal miners10 and agricultural workers.11,12 Related studies have reported the prevalence of COPD among agricultural workers including cattle, swine and poultry breeders was relatively high compared with that among nonfarming workers.12 Agricultural workers can be exposed to biochemical, organic and inorganic substances which may contribute to COPD, for instance, dust, biomass smoke, ammonia, silica and endotoxins.8,11–18
Approximately one half of the Thai population live in rural areas where the characteristics of healthcare infrastructure and providers differ from those of urban settings especially in remote rural areas.19 According to Thai national health policies, some noncommunicable diseases including type 2 diabetes and hypertension, but not COPD have been actively surveyed at the community level. Thus, the current situation of COPD in rural communities remains limited. Most of the Thai population in rural communities works as agriculturists. However, the information of factors potentially responsible for COPD among agriculturists remains limited, which is essential to focus on preventing the disease. Attenuating the risk factors of COPD will also help to slow disease progression and reduce associated complications. The present study aimed to determine the prevalence and risk factors of COPD among agriculturists in a remote rural community in Chachoengsao Province, central Thailand.
Materials and Methods
Study Designs and Subjects
The study was conducted in a remote rural community in Thakradan Subdistrict, Sanam Chai Khet District, Chachoengsao Province located 160 km east of the Bangkok Metropolitan Area, Thailand. Thakradan rural community consists of five villages including Na-Yao, Na-Ngam, Na-Isan, Thungso-Hongsa and Thung-Hiang. These remote villages house approximately 4000 people, most of whom were agriculturists or herdsmen. This community might represent a typical Thai agriculture community. A longitudinal survey had been conducted in this community since Phramongkutklao College of Medicine established a teaching community. Recently, noncommunicable diseases including diabetes and hypertension have raised concerns in this community, leading to some intervention programs. However, the true situation for COPD including its actual magnitude and associated factors remains unknown. To date, no recent study could represent the real situation of COPD in a Thai rural community. This single-site study provided preliminary information regarding the COPD situation in such a population. A cross-sectional study was conducted in January 2020. The minimal calculated sample size of 351 was determined using Slovin’s20 according to a 95% confidence interval (CI) with a margin error of 0.05. The investigators expected that 20% of available individuals would be unable to participate; thus, we enrolled approximately 422 individuals to our study. Information on population was retrieved from the Ministry of Interior (Thailand), the National Population Registry to determine the sampling frame. The registered populations were selected from five villages using stratified sampling by village and then a random sample was drawn from each stratum.21 The subjects residing in the target areas at the period of study were included. Inclusion criteria comprised agriculturists or herders aged at least 18 years old. Agriculturists and herders were defined as those working as agriculturists or herders more than ten years. Subjects were excluded from the study, if they presented contraindications for spirometry including acute myocardial infarction within one week, no decompensated heart failure, cardiac arrhythmia, history of syncope related to forced expiration/cough, eye surgery within one week, brain surgery within four weeks, sinus surgery or middle ear surgery or infection within one week, presence of pneumothorax, thoracic surgery within four weeks, abdominal surgery within four weeks, late-term pregnancy and active or suspected transmissible respiratory or systemic infections such as tuberculosis.22
This study was reviewed and approved by the Royal Thai Army Medical Department Institutional Review Board. Written informed consent was obtained from the participants following the WMA Declaration of Helsinki–Ethics principles for medical research involving human subjects (Reference number: R156q/62).
Data Collection
The investigators provided the information sheets and informed subjects of the objectives and methods of the study. Informed consent was obtained before conducting the research. If participants could not read the information sheet, the investigators would read the information to them and then participants could use their fingerprint to confirm their agreement on the consent form. Participants did not receive any incentive for joining the study. Among the 648 enrolled individuals, 546 participants were included in the study. During the study, face-to-face interviews were conducted using standardized questionnaires to obtain essential information from participants within 30 minutes. The interviews were conducted by well-trained interviewers.
The Thai version of the standardized questionnaires was adapted by following the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines 2019 and European Community Respiratory Health Survey II.23,24 The standardized questionnaire of the study was reviewed and approved by a pulmonologist, epidemiologist, and the institutional review board before using in an interview. The questionnaires covered information on demographic characteristics, occupational history and factors related to COPD within the previous 12 months. Data regarding agricultural history comprised two main specific groups including (1) plant cultivation (rice, cassava, rubber tree and corn) and (2) livestock (poultry, cattle and swine). To be classified in each group, subjects must have been employed in any type of cultivation or livestock breeding for more than ten years. Smoking status was categorized as never, ex-smoker and current smoker. Never smoked characterized participants who had never smoked, or who had smoked less than 100 cigarettes in his or her lifetime.25 Ex-smoker was defined as smoke-free for 12 months. Additionally, smokers were asked the age at which they started to smoke. Smoking history included the number of packaged or hand-rolled cigarettes daily and the number of smoking years. The number of pack-years was calculated using the number of packs of cigarettes smoked daily multiplied the number of years the patient had smoked (1 pack = 20 cigarettes).26 Home cooking history was defined by participants having a cooking process conducted in their home during the last 12 months. Exercise was defined by regular aerobic exercise for 30 minutes daily and at least 3 days/week. Bodyweight and height were measured using standardized balance scales (DETECTO, St. Webb City, MO, USA) (to the nearest 0.1 kg) and stadiometer (DETECTO) (to the nearest 0.1 cm), respectively. Body mass index (BMI) was calculated as body weight in kilograms divided by height in meters squared (kg)/height (m2). BMI level was classified according to the Asia-Pacific BMI classifications in five groups, ie, <18.5 kg/m2, 18.5 to 22.9 kg/m2, 23.0 to 24.9 kg/m2, 25.0 to 29.9 kg/m2 and ≥30 kg/m2.27
Spirometry Testing
Spirometry testing was performed using a pneumotachograph (MinispirTM Spirometer with SpO2, MIR, Rome, Italy) between 08.00 and 12:00 AM. The spirometer is used by medical technologists who have been trained in a specific program of a pulmonary function test. Standardization of spirometry testing was conducted following the official American Thoracic Society and European Respiratory Society technical statements (ATS/ERS).22 The participants were advised to avoid smoking within one hour before testing, performing vigorous exercise within one hour before testing, and wearing clothing that substantially restricted full chest and abdominal expansion. The medical technologists instructed and demonstrated the test before performing spirometry testing. The participants attached the nose clip, inserted the mouthpiece in the mouth, and closed their lips around the mouthpiece. The participants breathed normally; then inhaled completely and rapidly with a pause of ≤2 seconds at total lung capacity (TCL). Next, the participants exhaled with maximal effort until no more air could be expelled. After that, the participants inhaled with maximal effort until completely full. A minimum of three acceptable forced expiratory volumes in one second (FEV1) and three acceptable forced vital capacity (FVC) measurements were reported. The largest FEV1 and the largest FVC were calculated for FEV1/FVC. Bronchodilator responsiveness testing was performed when the FEV1/FVC ratio was <0.7. Bronchodilator responsiveness testing was performed by administering 400 μg of the short-acting β2-agonist salbutamol (Ventolin™) delivered as 2 Metered-Dose Inhaler (MDI) actuations of 200 μg. The participants gently and incompletely exhaled and actuated the salbutamol MDI at the beginning of a slow inhalation to TLC from the holding chamber. After that, the participants held their breath for five to ten seconds before exhaling. Two separate MDI actuations were delivered at 30-second intervals. Then, the post-bronchodilator maneuver was performed 15 minutes after administering the final MDI actuation. COPD was defined by the spirometric criterion for airflow limitation constituting a post-bronchodilator fixed ratio of FEV1/FVC < 0.70.23
Classification of airflow limitation severity in COPD (based on post-bronchodilator FEV1) in among subjects with FEV1/FVC < 0.70 were divided into 4 four levels including mild, moderate, severe, and very severe. GOLD 1 (mild) was defined by FEV1 ≥ 80% predicted. GOLD 2 (moderate) was defined by 50% ≤FEV1 ≤ 80% predicted. GOLD 3 (severe) was defined by 30% ≤FEV1 ≤ 50% predicted, and GOLD4 (very severe) was defined by FEV1<30%.23
The participants presenting COPD would receive standard care under their healthcare coverage scheme. The list of participants with COPD was registered in the health database at the Health Promoting Hospital Baan Na-Yao, the primary care unit in the rural area. Additionally, participants with COPD received long-term medical treatment such as bronchodilators, inhaled corticosteroids, and recommendations of life-style modification to alleviate COPD progression including smoking cessation.
Statistical Analysis
Data were analyzed using StataCorp, 2015, Stata Statistical Software: Release 14 (College Station, TX, USA: StataCorp LP). Demographic characteristics were determined using descriptive statistics. Categorical data were presented as number and percentage while continuous data were presented as mean and standard deviation (SD). Prevalence of COPD was determined using descriptive statistics and reported as a percentage with 95% confidence interval (95% CI). Binary logistic regression analysis was used to determine the risk factors for COPD, and the magnitude of association was presented as crude odds ratio (OR) with 95% CI. The multicollinearity was tested. The variables significant in univariate analysis and in established relationship with the outcome were included in the final model. Multivariable analysis was performed to adjust confounders using logistic regression. Adjusted odds ratio (AOR) from multivariable analysis was presented with corresponding 95% CI. A p-value less than 0.05 was considered statistically significant.
Results
Characteristics of the Study Participants
Among the 648 enrolled individuals, a total of 546 participants met the acceptability criteria by spirometry and were included in the analysis. The average age of participants was 57.1±13.6 years. In all, 262 (48%) agriculturists were male. Most participants obtained their highest education level from primary school accounting for 74.5%. The agriculturists’ characteristics including cultivation, livestock and both accounted for 16.7%, 31.3% and 52.0%, respectively. Descriptive characteristics of the study participants are shown in Table 1.
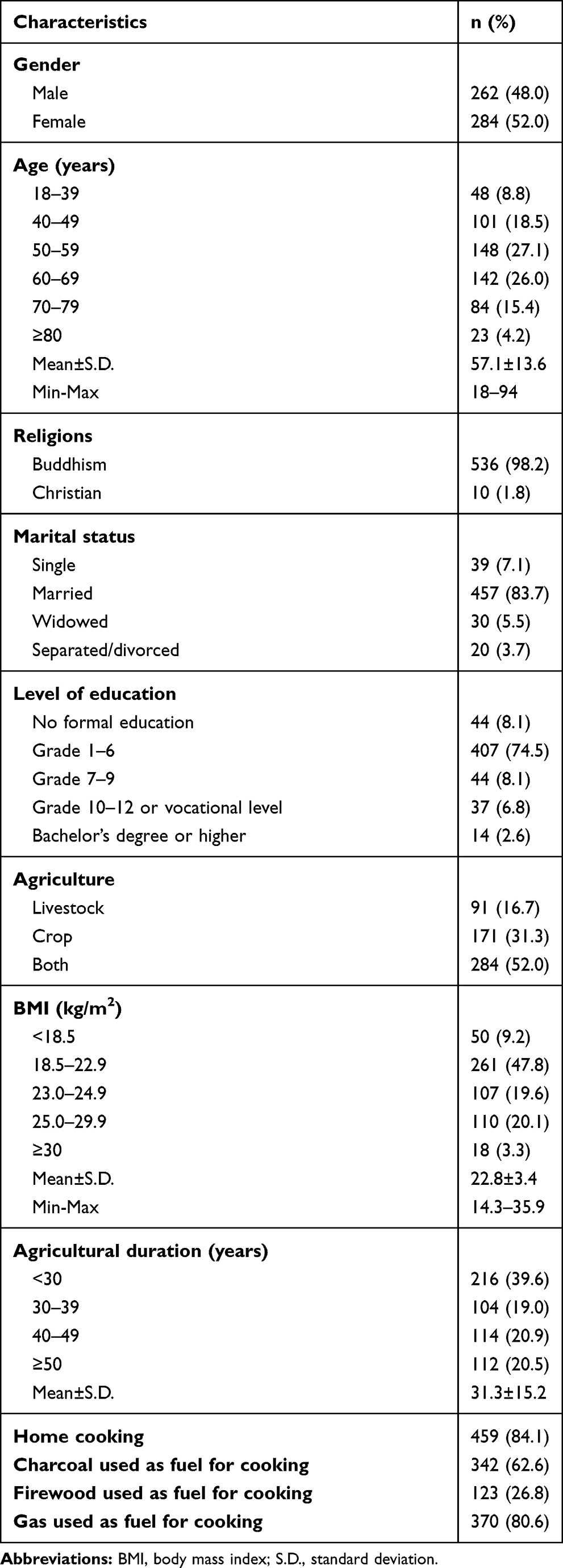 |
Table 1 Demographic Characteristics of Agriculturists in a Rural Community, Central Thailand (n=546) |
Prevalence of COPD Among Agriculturists in a Rural Community
Of the total 546, 46 participants showed FEV1/FVC (prebronchodilator) <0.7. After bronchodilator responsiveness testing, 30 subjects remained FEV1/FVC (postbronchodilator) <0.7. Thus, the overall prevalence of COPD was 5.5% (95% CI: 3.6–7.4). Of the 30 subjects with COPD, 22 (73.3%) were classified in GOLD 1 (mild symptom), and 8 (6.7%) subjects were classified in GOLD 2 (moderate symptom). The prevalence of COPD among males was 8.0% (95% CI: 4.7–11.3) while the prevalence was 3.2% (95% CI: 1.1–5.2) among females. The prevalence of COPD among agriculturists aged ≥60 years old was 9.2% (95% CI: 5.6–12.9). In agricultural jobs, the prevalence of COPD in crop cultivation was 5.3% (95% CI: 3.2–7.3), while in livestock rising was 7.8% (95% CI: 5.0–10.5).
Risk Factors for COPD Among Agriculturists in a Rural Community
Table 2 presents the univariate logistic regression analysis for the risk factors of COPD among agriculturists. After adjusting for potential confounders, the risk factors for COPD included age, smoking intensity, cattle farming, swine farming, and home cooking; multivariate logistic regression analysis showed that agriculturists, aged ≥60 years old, tended to be at high risk of COPD compared with those aged <60 years old (AOR 2.7, 95% CI: 1.1–7.0). A dose–response relationship between smoking intensity and COPD was identified (AOR 1.1, 95% CI: 1.0–1.1). We found that cattle raising was associated with COPD (AOR 3.3, 95% CI: 1.4–8.2). In addition, the prevalence of COPD among the agriculturists with swine farming was higher than those without swine farming (AOR 4.1, 95% CI: 1.7–10.3). Those having a history of home cooking tended to be at higher risk for COPD; however, without association (AOR 2.7, 95% CI: 0.8–9.7).
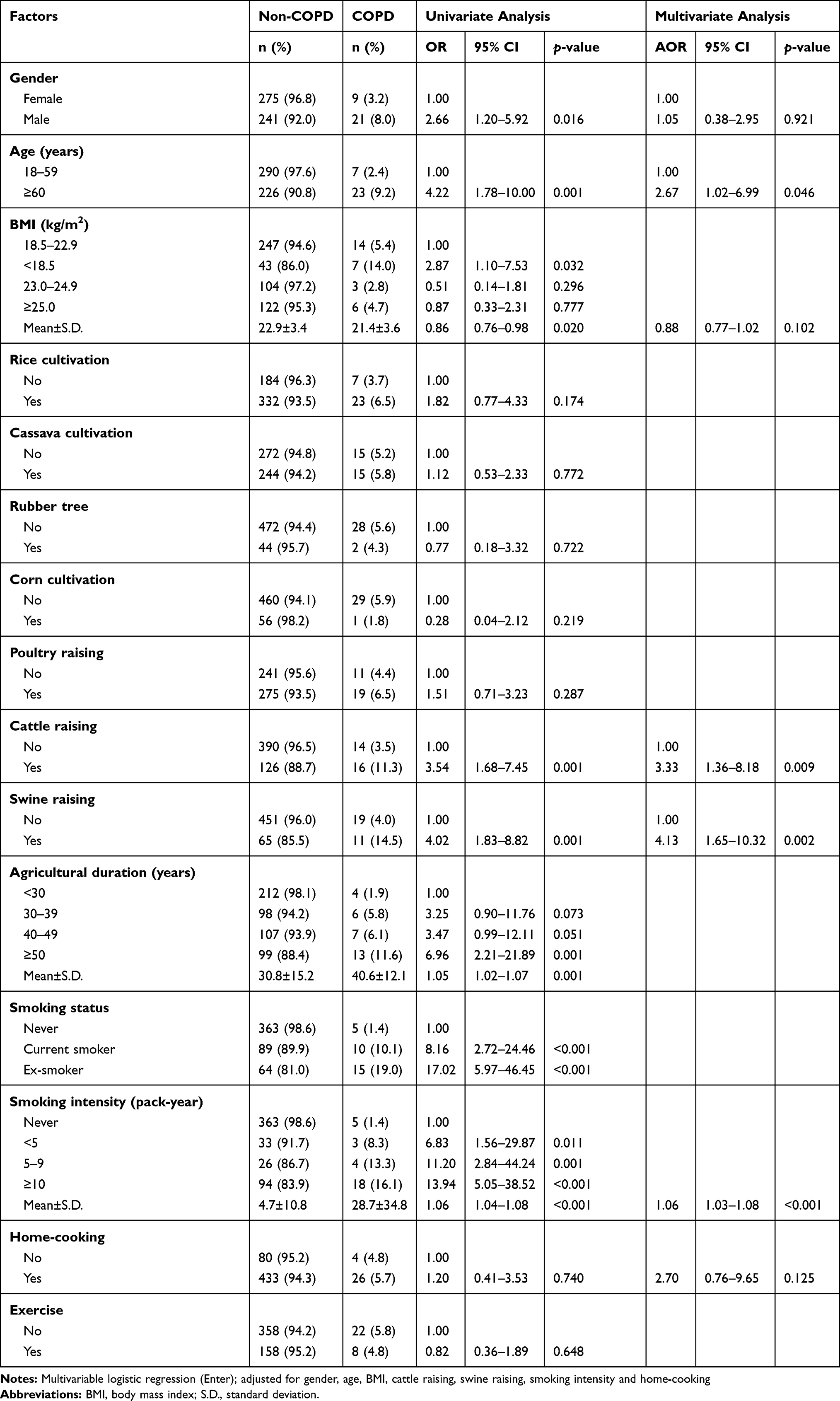 |
Table 2 Risk Factors for COPD Among Agriculturists in a Rural Community, Central Thailand, 2020 (n=546) |
Discussion
The present study determined the prevalence and risk factors of COPD among agriculturists in a rural community in Thailand using the GOLD guideline 2019.23 The prevalence of COPD in this rural community was 5.5% which was relatively low compared with the previous population-based study conducted in northern Thailand in 2010.28 This previous study was conducted among people aged at least 40 years, while the villagers aged at least 18 years were included in our study. However, when the same age groups were analyzed, the prevalence of COPD was comparable. The prevalence of COPD among males was significantly higher than that found in the female group. This finding was compatible with other related studies.27–29 Compared with the prevalence of COPD among crop cultivation workers, the prevalence of that among livestock raising workers was relatively high, similar to the recent studies conducted in France12 and Norway.29
We found that agriculturists aged ≥60 years were more likely to present COPD compared with those aged <60 years old. Similarly, recent studies in Sweden, Denmark and the United Arab Emirates reported that people with older age especially more than 60 years old were positively associated with COPD.30–32 This phenomenon could be explained by the fact that lung function progressively declines with rising age as a consequence of structural and physiological changes to the lungs including reduced elastic recoil and compliance of the chest wall. Additionally, FEV1 and FVC decreases with increasing age among both males and females.33–35 Other evidence has illustrated via the possible roles regarding aging hallmarks including genomic instability, deregulated nutrient sensing, cellular senescence and stem cell exhaustion that disturb the repair and remodeling structural cells and lung tissues, resulting in COPD.35–38
In concordance with related reports,39–41 we found that COPD was linked to cigarette smoking intensity with a significant dose–response relationship. The finding was consistent with the related study of Forey et al (2011) reporting that the amount smoked and packs-years was attributable to increased risk of COPD, and affirming the causal relationship between COPD and cigarette smoking.42 Cigarette smoke contains a high concentration of reactive oxidant substances inducing chronic inflammatory changes in the central and peripheral airways, and lung parenchyma.43,44 The inflammatory process leads to infiltrated mucosa, submucosa and glandular tissue resulting in increased mucus contents, epithelial-cell hyperplasia and wall thickening in the small conducting airways.45 Additionally, structural remodeling and loss of elastic recoil by emphysematous destruction of the parenchyma lead to ongoing decline of FEV1.45–47 In the rural community, cigarette smoking rates among high school students were approximately 15%,48 moreover, one-third of the agriculturists especially among males had ever smoked both packed cigarettes and hand-rolled tobacco cigarettes; thus, smoking cessation should be suggested to smokers. Furthermore, smoking cessation was associated with reduced non-communicable diseases including cardiovascular disorders and cancers, and it was associated with an increased quality of life.46,49,50
Swine raising was identified as a risk factor of COPD in a few studies.51,52 Swine farmworkers are often exposed to various types of inhalable dust, eg, wood dust, litter, fecal material and a complex mixture of organic materials derived from feed.41,53 The related report suggested that chronic exposure to these organic materials leads to increased adaptive immune mechanisms. Then, an increase in pro-inflammatory agents would affect the inflammatory responses leading to chronic respiratory disorders.54–56 Additionally, cattle farmworkers were associated with COPD which was similar to the related studies conducted in France12 and Norway.29 A 12-year longitudinal study reported that dairy farmers presented a more progressive decline in FEV1/FVC than controls.57 The related studies have reported that a high concentration of gases due to byproducts of animal waste including hydrogen sulfide and ammonia was linked to reduced FEV1 and associated with COPD.58,59 The recent study of Marescaux et al (2016) found that the prevalence of COPD in a traditional farm was relatively high compared with those found among dairy farmers in a modernity farm.60 Most swine and cattle farms in remote rural communities in Thailand are traditional farms; thus, this situation may impact COPD among agriculturists in rural settings.
The present study showed that agriculturists in a remote rural area with a history of home cooking tended to be at higher risk for COPD; however, without association. A study conducted in South China also showed similar findings suggesting that indoor pollutants from biomass fuel cooking may be an important risk factor for COPD.61 Almost all populations in the Thai countryside used a traditional stove with biofuel including charcoal and firewood for their home cooking. The combustion of biofuel is very incomplete in traditional stoves resulting in substantial emissions and contributing high levels of household air pollution.62 Pollutants from biomass combustion comprised a mixture of droplets, small solid particles and gasses such as carbon monoxide, nitrogen dioxide and others penetrating deep in the lungs.63 Furthermore, evidence has suggested that replacing biomass with biogas for cooking and improving kitchen ventilation leads to a decreased risk of COPD.64,65
This study employed a cross-sectional design, making it difficult to establish a cause–effect relationship between the associated factors and COPD. Another limitation was the small sample size in the study. Further study is needed to identify either environmental or biological agents that cause COPD to develop in each subgroup of farmers in Thailand. However, the study used spirometry testing as a diagnostic test for COPD which is the gold standard according to GOLD 2019 and ATS/ERS statement. Moreover, the association between factors and outcomes was able to be presented. In the study, bronchodilator responsiveness testing was performed when the FEV1/FVC ratio was <0.7; however, the case of FVC may have been underestimated, and participants with COPD may have been missed. On the other hand, COPD was defined by a postbronchodilator fixed ratio of FEV1/FVC <0.70. The prevalence of COPD among the elderly may have been overestimated while the prevalence of COPD among young adults may have been underestimated.66,67 Although social desirability bias might also have existed in the study due to conducting face-to-face interviews, a standardized questionnaire of the study was reviewed and approved by a pulmonologist, epidemiologist and the institutional review board. Additionally, the interviews were conducted by well-trained interviewers.
The present study identified a few modifiable risk factors for COPD which would be useful for prevention and control strategies at the community level. Agriculturists especially those residing in rural communities should be targeted for more educational interventions in raising awareness about COPD, its associated complications and adjusting their behaviors especially smoking cessation. The authorities in the rural communities such as healthcare workers at primary care units should provide screening for COPD and suggestions, advice and support for the agriculturists using various measures. For instance, personal protective equipment such as hygienic masks for animal farmworkers should be provided, as well as improving kitchen ventilation for home cooking and promoting smoking cessation. Our study may not be generalized to the whole country but may reflect challenges of agriculturists residing in rural communities in Thailand.
Conclusion
Our data emphasized that COPD is a significant health problem among agriculturists in a rural community in Thailand. Animal farmers and behavioral factors such as smoking were associated with COPD. Effective public health interventions, especially modifying risk factors, should be provided in remote rural areas to alleviate the progression of COPD and its associated serious complications.
Abbreviations
COPD, chronic obstructive pulmonary disease; GOLD, the Global Initiative for Chronic Obstructive Lung Disease; ATS/ERS, an official American Thoracic Society and European Respiratory Society technical statement; TLC, total lung capacity; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; MDI, metered dose inhaler; OR, odds ratio; AOR, adjusted odds ratio; 95% CI, 95% confidence interval; BMI, body mass index.
Acknowledgments
The authors express their grateful thanks to Ms. Sawitree Samsee and village health volunteers of Baan-Na-Yao Health Promoting Hospital, Chachoengsao Province. The authors thank all the staff members of the Department of Military and Community Medicine, Phramongkutklao College of Medicine, for their support in completing this study.
Disclosure
The authors report no potential conflicts of interest in this work.
References
1. GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 19802017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1736–1788. doi:10.1016/S0140-6736(18)32203-7
2. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. doi:10.1371/journal.pmed.0030442
3. Varmaghani M, Dehghani M, Heidari E, Sharifi F, Moghaddam SS, Farzadfar F. Global prevalence of chronic obstructive pulmonary disease: systematic review and meta-analysis. East Mediterr Heal J. 2019;25(1):47–57. doi:10.26719/emhj.18.014
4. Saenghirunvattana S, Kongngeon V, Aeimrerksiri B, et al. Chronic obstructive pulmonary diseases in Thailand: incidence, prevalence, present status and future trends. J Med Assoc Thai. 2001;84(10):1407–1411.
5. Gunen H, Hacievliyagil SS, Kosar F, et al. Factors affecting survival of hospitalised patients with COPD. Eur Respir J. 2005;26(2):234–241. doi:10.1183/09031936.05.00024804
6. Postma DS, Bush A, van den Berge M. Risk factors and early origins of chronic obstructive pulmonary disease. Lancet. 2015;385(9971):899–909. doi:10.1016/S0140-6736(14)60446-3
7. Weitzenblum E, Chaouat A. Cor pulmonale. Chron Respir Dis. 2009;6(3):177–185. doi:10.1177/1479972309104664
8. Huang X, Mu X, Deng L, et al. The etiologic origins for chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2019;14:1139–1158. doi:10.2147/COPD.S203215
9. Ulvestad B, Bakke B, Eduard W, Kongerud J, Lund MB. Cumulative exposure to dust causes accelerated decline in lung function in tunnel workers. Occup Environ Med. 2001;58(10):663–669. doi:10.1136/oem.58.10.663
10. Love RG, Miller BG. Longitudinal study of lung function in coal-miners. Thorax. 1982;37(3):193–197. doi:10.1136/thx.37.3.193
11. Balmes J, Becklake M, Blanc P, et al. American thoracic society statement: occupational contribution to the burden of airway disease. Am J Respir Crit Care Med. 2003;167(5):787–797. doi:10.1164/rccm.167.5.787
12. Guillien A, Puyraveau M, Soumagne T, et al. Prevalence and risk factors for COPD in farmers: a cross-sectional controlled study. Eur Respir J. 2016;47(1):95–103. doi:10.1183/13993003.00153-2015
13. Mayer AS, Stoller JK, Bucher Bartelson B, James Ruttenber A, Sandhaus RA, Newman LS. Occupational exposure risks in individuals with PI*Z α1 antitrypsin deficiency. Am J Respir Crit Care Med. 2000;162(2):553–558. doi:10.1164/ajrccm.162.2.9907117
14. Jaén A, Zock JP, Kogevinas M, Ferrer A, Marín A. Occupation, smoking, and chronic obstructive respiratory disorders: a cross sectional study in an industrial area of Catalonia, Spain. Environ Health. 2006;5:2. doi:10.1186/1476-069X-5-2
15. Mendy A, Salo PM, Cohn RD, Wilkerson J, Zeldin DC, Thorne PS. House Dust Endotoxin Association with Chronic Bronchitis and Emphysema. Environ Health Perspect. 2018;126(3):37007. doi:10.1289/EHP2452
16. Liu S, Ren Y, Wen D, et al. Prevalence and risk factors for COPD in greenhouse farmers: a large, cross-sectional survey of 5880 farmers from northeast China. Int J Chron Obstruct Pulmon Dis. 2015;10:2097–2108. doi:10.2147/COPD.S79264
17. Hu G, Zhou Y, Tian J, et al. Risk of COPD from exposure to biomass smoke: a metaanalysis. Chest. 2010;138(1):20–31. doi:10.1378/chest.08-2114
18. Fontana L, Lee S-J, Capitanelli I, et al. Chronic obstructive pulmonary disease in farmers: a systematic review. J Occup Environ Med. 2017;59(8):775–788. doi:10.1097/JOM.0000000000001072
19. United Nations Secretariat. Department of Economic and Social Affairs. World Urbanization Prospects the 2018 Revision; 2019.
20. Cochran WG. Sampling Techniques. John Wiley & Sons; 2007.
21. Organization WH. WHO STEPS Surveillance Manual: The WHO STEPwise Approach to Chronic Disease Risk Factor Surveillance. World Health Organization; 2005.
22. Graham BL, Steenbruggen I, Miller MR, et al. Standardization of spirometry 2019 update. an official american thoracic society and european respiratory society technical statement. Am J Respir Crit Care Med. 2019;200(8):e70e88. doi:10.1164/rccm.201908-1590ST
23. Agusti A, Chen R, Criner G. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2019 report. Glob Initiat Chronic Obstr Lung Dis. 2018.
24. Committee ECRHSIIS. The European community respiratory health survey II. Eur Respir J. 2002;20(5):1071–1079. doi:10.1183/09031936.02.00046802
25. Prevention C for DC and. Adult tobacco use information. Available from: https://www.cdc.gov/nchs/nhis/tobacco/tobacco_glossary.htm.
26. Institute NC. Pack year. Available from: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/pack-year?redirect=true.
27. Inoue S, Zimmet P, Caterson I, et al. The Asia-Pacific perspective: redefining obesity and its treatment. Sydney Heal Commun Aust Pty Ltd. 2000.
28. Pothirat C, Chaiwong W, Phetsuk N, Pisalthanapuna S, Chetsadaphan N, Inchai J. A comparative study of COPD burden between urban vs rural communities in northern Thailand. Int J Chron Obstruct Pulmon Dis. 2015;10:1035–1042. doi:10.2147/COPD.S82303
29. Eduard W, Pearce N, Douwes J. Chronic bronchitis, COPD, and lung function in farmers: the role of biological agents. Chest. 2009;136(3):716–725. doi:10.1378/chest.08-2192
30. Hagstad S, Backman H, Bjerg A, et al. Prevalence and risk factors of COPD among never-smokers in two areas of Sweden occupational exposure to gas, dust or fumes is an important risk factor. Respir Med. 2015;109(11):1439–1445. doi:10.1016/j.rmed.2015.09.012
31. Fabricius P, Løkke A, Marott JL, Vestbo J, Lange P. Prevalence of COPD in Copenhagen. Respir Med. 2011;105(3):410–417. doi:10.1016/j.rmed.2010.09.019
32. Al Zaabi A, Asad F, Abdou J, et al. Prevalence of COPD in Abu Dhabi, United Arab Emirates. Respir Med. 2011;105(4):566–570. doi:10.1016/j.rmed.2010.12.008
33. Rojas M, Meiners S, Le Saux CJ. Molecular Aspects of Aging: Understanding Lung Aging. John Wiley & Sons; 2014.
34. Janssens J-P, Pache J-C, Nicod LP. Physiological changes in respiratory function associated with ageing. Eur Respir J. 1999;13(1):197–205. doi:10.1183/09031936.99.14614549
35. Brandsma C-A, de Vries M, Costa R, Woldhuis RR, Königshoff M, Timens W. Lung ageing and COPD: is there a role for ageing in abnormal tissue repair? Eur Respir Rev an off J Eur Respir Soc. 2017;26(146). doi:10.1183/16000617.0073-2017
36. López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G. The hallmarks of aging. Cell. 2013;153(6):1194–1217. doi:10.1016/j.cell.2013.05.039
37. Meiners S, Eickelberg O, Königshoff M. Hallmarks of the ageing lung. Eur Respir J. 2015;45(3):807–827. doi:10.1183/09031936.00186914
38. Mercado N, Ito K, Barnes PJ. Accelerated ageing of the lung in COPD: new concepts. Thorax. 2015;70(5):482–489. doi:10.1136/thoraxjnl-2014-206084
39. Montes de Oca M, Zabert G, Moreno D, Laucho-Contreras ME, Lopez VMV, Surmont F. Smoke, biomass exposure, and COPD risk in the primary care setting: the PUMA study. Respir Care. 2017;62(8):1058–1066. doi:10.4187/respcare.05440
40. Bartal M. COPD and tobacco smoke. Monaldi Arch Chest Dis. 2005;63(4):213–225. doi:10.4081/monaldi.2005.623
41. Salvi S. Tobacco smoking and environmental risk factors for chronic obstructive pulmonary disease. Clin Chest Med. 2014;35(1):17–27. doi:10.1016/j.ccm.2013.09.011
42. Forey BA, Thornton AJ, Lee PN. Systematic review with meta-analysis of the epidemiological evidence relating smoking to COPD, chronic bronchitis and emphysema. BMC Pulm Med. 2011;11(1):36. doi:10.1186/1471-2466-11-36
43. Saetta M. Airway inflammation in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999;160(5 Pt 2):S1720. doi:10.1164/ajrccm.160.supplement_1.6
44. Brody JS, Spira A. State of the art. Chronic obstructive pulmonary disease, inflammation, and lung cancer. Proc Am Thorac Soc. 2006;3(6):535–537. doi:10.1513/pats.200603-089MS
45. Decramer M, Janssens W, Miravitlles M. Chronic obstructive pulmonary disease. Lancet. 2012;379(9823):1341–1351. doi:10.1016/S0140-6736(11)60968-9
46. Laniado-Laborín R. Smoking and chronic obstructive pulmonary disease (COPD). Parallel epidemics of the 21 century. Int J Environ Res Public Health. 2009;6(1):209–224. doi:10.3390/ijerph6010209
47. Churg A, Cosio M, Wright JL. Mechanisms of cigarette smoke-induced COPD: insights from animal models. Am J Physiol Lung Cell Mol Physiol. 2008;294(4):L61231. doi:10.1152/ajplung.00390.2007
48. Yaimai W, Oopakarn K, Phumvichitr C, et al. Prevalence and associated risk factors of substance abuse among adolescents in rural communities, central thailand: a cross-sectional study. J Southeast Asian Med Res. 2019;3(2):73–81.
49. Thakur JS, Garg R, Narain JP, Menabde N. Tobacco use: a major risk factor for non communicable diseases in South-East Asia region. Indian J Public Health. 2011;55(3):155–160. doi:10.4103/0019-557X.89943
50. Sarna L, Bialous SA, Cooley ME, Jun H-J, Feskanich D. Impact of smoking and smoking cessation on health-related quality of life in women in the nurses’ health study. Qual Life Res an Int J Qual Life Asp Treat Care Rehabil. 2008;17(10):1217–1227. doi:10.1007/s11136-008-9404-8
51. Jouneau S, Marette S, Robert A-M, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in dairy farmers: aIRBAg study. Environ Res. 2019;169:1–6. doi:10.1016/j.envres.2018.10.026
52. Costa M, Teixeira PJZ, Freitas PF. Respiratory manifestations and respiratory diseases: prevalence and risk factors among pig farmers in Braço do Norte, Brazil. J Bras Pneumol Publicacao of Da Soc Bras Pneumol e Tisilogia. 2007;33(4):380–388. doi:10.1590/s1806-37132007000400006
53. Matheson MC, Benke G, Raven J, et al. Biological dust exposure in the workplace is a risk factor for chronic obstructive pulmonary disease. Thorax. 2005;60(8):645–651. doi:10.1136/thx.2004.035170
54. Sahlander K, Larsson K, Palmberg L. Altered innate immune response in farmers and smokers. Innate Immun. 2010;16(1):27–38. doi:10.1177/1753425909106317
55. Robbe P, Spierenburg EAJ, Draijer C, et al. Shifted T-cell polarisation after agricultural dust exposure in mice and men. Thorax. 2014;69(7):630–637. doi:10.1136/thoraxjnl-2013-204295
56. Hendrick DJ. Occupational and chronic obstructive pulmonary disease (COPD). Thorax. 1996;51(9):947–955. doi:10.1136/thx.51.9.947
57. Gainet M, Thaon I, Westeel V, et al. Twelve-year longitudinal study of respiratory status in dairy farmers. Eur Respir J. 2007;30(1):97–103. doi:10.1183/09031936.00150405
58. van Kersen W, Oldenwening M, Aalders B, et al. Acute respiratory effects of livestock-related air pollution in a panel of COPD patients. Environ Int. 2020;136:105426. doi:10.1016/j.envint.2019.105426
59. May S, Romberger DJ, Poole JA. Respiratory health effects of large animal farming environments. J Toxicol Environ Health B Crit Rev. 2012;15(8):524–541. doi:10.1080/10937404.2012.744288
60. Marescaux A, Degano B, Soumagne T, Thaon I, Laplante -J-J, Dalphin J-C. Impact of farm modernity on the prevalence of chronic obstructive pulmonary disease in dairy farmers. Occup Environ Med. 2016;73(2):127–133. doi:10.1136/oemed-2014-102697
61. Liu S, Zhou Y, Wang X, et al. Biomass fuels are the probable risk factor for chronic obstructive pulmonary disease in rural South China. Thorax. 2007;62(10):889–897. doi:10.1136/thx.2006.061457
62. Bruce N, Perez-Padilla R, Albalak R. Indoor air pollution in developing countries: a major environmental and public health challenge. Bull World Health Organ. 2000;78(9):1078–1092.
63. de Koning HW, Smith KR, Last JM. Biomass fuel combustion and health. Bull World Health Organ. 1985;63(1):11–26.
64. Zhou Y, Zou Y, Li X, et al. Lung function and incidence of chronic obstructive pulmonary disease after improved cooking fuels and kitchen ventilation: a 9-year prospective cohort study. PLoS Med. 2014;11(3):e1001621. doi:10.1371/journal.pmed.1001621
65. Chapman RS, He X, Blair AE, Lan Q. Improvement in household stoves and risk of chronic obstructive pulmonary disease in Xuanwei, China: retrospective cohort study. BMJ. 2005;331(7524):1050. doi:10.1136/bmj.38628.676088.55
66. Wanchai Dejsomritrutai MD, Benjamas Chuaychoo MD. Impact of GLI-2012 spirometric references and lower limit of normal on prevalence of COPD in older urban Thai persons. J Med Assoc Thai. 2016;99(3):276–281.
67. Güder G, Brenner S, Angermann CE, et al. GOLD or lower limit of normal definition? A comparison with expert-based diagnosis of chronic obstructive pulmonary disease in a prospective cohort-study. Respir Res. 2012;13(1):13. doi:10.1186/1465-9921-13-13
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.