Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Prevalence and Risk Factors of Chronic Obstructive Pulmonary Disease in Kazakhstan in a Nationwide Population-Based Epidemiological Study
Authors Vinnikov D, Mukatova I, Tulekov Z, Raushanova A, Romanova Z, Sadibekova M
Received 14 October 2025
Accepted for publication 17 February 2026
Published 23 February 2026 Volume 2026:21 574409
DOI https://doi.org/10.2147/COPD.S574409
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Denis Vinnikov,1,2 Irina Mukatova,3 Zhangir Tulekov,1 Aizhan Raushanova,4 Zhanna Romanova,4 Malika Sadibekova5
1Environmental Health Lab, Al-Farabi Kazakh National University, Almaty, Kazakhstan; 2Occupational Health Risks Lab, Peoples’ Friendship University of Russia (RUDN University), Moscow, Russian Federation; 3Department of Internal Diseases with Courses of Nephrology, Hematology, Allergology, and Immunology, Astana Medical University, Astana, Kazakhstan; 4Department of Epidemiology, Biostatistics and Evidence-Based Medicine, Al-Farabi Kazakh National University, Almaty, Kazakhstan; 5Department of Internal Medicine, Karaganda Medical University, Karagandy, Kazakhstan
Correspondence: Denis Vinnikov, Environmental Health Lab, Al-Farabi Kazakh National University, al-Farabi Avenue 71, Almaty, 050040, Kazakhstan, Tel +7 727 3773333, Email [email protected]
Purpose: Until recently, reports on chronic obstructive pulmonary disease (COPD) in Kazakhstan have been sporadic and reflected the disease burden in only one largest city, Almaty. We, therefore, aimed to characterize the prevalence and risk factors of COPD confirmed with a high-quality spirometry in a nationwide population-based study.
Patients and Methods: We enrolled 5058 subjects, and hereinafter analyzed complete data for 4626 (age 47; interquartile range (IQR) 31;60 years) participants from the general population from five cities in Kazakhstan representing the West, North, South, East and the central part to fill in a questionnaire and undergo spirometry with bronchodilation. COPD was confirmed when post-bronchodilation forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) was below − 1.64 z-scores. The association of selected predictors with COPD was tested in multivariate regression models.
Results: Seven percent of the entire group (9% in men vs 6% in women) had COPD. The corresponding prevalence in the group 40 years and older was 10.7% (14.5% in men and 7.6% in women). For ΔFVC, 78% could achieve A or B quality, whereas 83% could attain A or B quality for ΔFEV1. Only 30% of COPD patients were told they had it before. Ever-smoking (OR 2.44; 95% CI 1.81;3.33), low educational level (OR 1.80; 95% CI 1.42;2.28), exposure to vapors, gases, dusts and fumes (VGDF) (OR 1.41; 95% CI 1.10;1.82) and tuberculosis in the past (OR 4.12. 95% CI 2.19;7.45), adjusted for each other, age, sex and physical activity put subjects at risk for COPD.
Conclusion: COPD in Kazakhstan remains a highly underdiagnosed disease. Most COPD patients do not yet have a timely diagnosis and remain untreated. Smoking, occupational exposures and even tuberculosis in the past significantly increase the risk of this disease.
Keywords: spirometry, occupational, smoking, respiratory, population-based
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive inflammatory disease, which usually develops in subjects over 40, exhibits increasing burden worldwide and is associated with enormous financial burden.1,2 Low- and middle-income countries may experience greater challenges in combatting the disease due to the need for a lifelong need for treatment, poor excess to timely and high-quality spirometry and increasing smoking prevalence and ambient and indoor air pollution.1,3–5 COPD patients suffer not only from symptoms but face early disability, constantly deteriorating quality of life and usually emerging comorbidities.3,6,7 Although potent pharmacological treatment, including combined bronchodilators, is available in most countries, COPD remains the third leading cause of death all over the world, because smoking,4,8–10 ambient11–14 and indoor4,5,15,16 air pollution and exposure to aerosol in the workplace4,5,17 need colossal public health effort, yet unattainable in many countries.
The true prevalence of COPD is unclear, whereas the reported and estimated prevalence depend largely on the methodology.18 The number of patients officially reported by the governmental agencies differs dramatically from the estimates within the population-based epidemiological studies, and the discrepancy may be dramatic. Thus, our preceding study in Almaty, in which COPD was defined as FEV1/FVC below lower limit of normality (LLN), demonstrated that only 24% patients with confirmed diagnosis ever heard they had COPD, and most of these patients were of middle age with minimum or no symptoms.19 Similarly, in patients who reported the disease and received treatment, only 22% had obstructive ventilation defect. Furthermore, there exists a considerable difference in the exposure to ambient and indoor air pollution and smoking rates in the country,20 given that Kazakhstan is a large country with contrasting climate, population employment in the industry, and ambient air pollution level.
In addition, fine particulate matter concentrations during the heating season in most cities exceed recommendations threshold values, including the cities of the current study.15,21–24 Preceding studies showed that fine PM concentrations during the heating season may exceed exposure limits 10–20-fold and sometimes more.15,24 However, the extent to which biomass fuel, which is a dominating source of pollution,21,22 is used for heating during the cold season may explain disparities in the concentrations and the populational exposure. In fact, the fraction of exposed population and thus number of COPD cases in more industrialized central and eastern Kazakhstan may contrast with those elsewhere in the country. Taken together, this prompts that the burden of COPD in Kazakhstan may be severely understudied and most patients with a disease remain undiagnosed with no treatment.
Given that population-based studies designed specifically to assess COPD prevalence and its risk factors have never been published from Kazakhstan, except from one largest city,19 there has been a vital need for a systematic approach to ascertain the burden of COPD in the country, considering pronounced heterogeneity in air pollution, occupational exposure to aerosol and smoking rates. In addition, spirometry protocols were updated in 2019, but were never applied to test Kazakhstan population. Because spirometry quality protocols are essential for accurate diagnosis, including the approach to rely on LLN instead of 70% threshold for FEV1/FVC, a population-based study with a standardized questionnaire and lung function testing protocols was needed. Therefore, the aim of this study was to characterize the prevalence and risk factors of COPD confirmed with a high-quality spirometry in five major geographical locations (west, east, north, south and center) of Kazakhstan.
Materials and Methods
Study Design and Sample
This was a population-based nationwide epidemiological study, which included subjects from all five major geographical locations of Kazakhstan. The study was approved by the Committee on Bioethics of al-Farabi Kazakh National University (approval IRB-A387, dated 17.03.2022), whereas all participants provided a written informed consent to participate. This study was completed in compliance with the Declaration of Helsinki and local legislation on studies in humans. Because Kazakhstan is a large country with notable change in population employment structure, socioeconomic status, smoking rates, air pollution and even access to care between the regions, we divided the country into five locations (Aktobe (West), Kostanay (North), Shymkent (South), Ust-Kamenogorsk (East) and Karagandy (Center)) and chose one city in each location where a qualified medical doctor was trained. Five medical doctors from these regions were offered a full in-person training on spirometry using a standard methodology.
For sample size calculation, we assumed the prevalence of 10%, also guided by our preceding study of a similar design in the largest Kazakhstan city, Almaty, margin error 3% and up to 10% missing data, 1000 participants from each geographical location would be needed. The overall sample for 5 regions was set to 5000 participants. Study participants were recruited from local outpatient medical facilities in all locations. Because all local population is covered by these centers, the latter can provide the best representation of the population of all ages. Participants were invited to participate from the list of enlisted population using random numbers. Should the person fail to attend, the person next to the assigned number was invited. Participants arrived at the medical center for an appointment and were asked to complete a questionnaire and undergo spirometry.
Questionnaire
Our questionnaire was offered either in Russian or Kazakh following the written informed consent signature. In this study, we used the core of our previous questionnaire in the preceding study,19 supplemented with a few more questions. Basic demographic information consisted of full name, mobile phone, ID, date of birth, biological gender, residential address, ethnicity, highest attained education, and the estimated family income per person per month (stratified into (a) below 100,000 tenge a month; (b) 101–500,000 tenge a month, and (c) 501,000 tenge or more a month). We then collected information on all occupational history, including all places of work in a lifetime with positions held and work duration in years. Employment history was considered for positions held for at least one year.
We asked a detailed history on cigarette smoking, electronic device smoking, and waterpipe smoking. With regard to cigarette smoking and with a set of a few questions, subjects could be then classified into (a) never-smokers; (b) ex-smokers; (c) current occasional smokers, and (d) current daily cigarette smokers. For the latter, we asked for a number of cigarettes smoked a day and the overall smoking duration in years. For ex-smokers, we collected information on the years of smoking overall and the duration of smoke-free history since quitting. For waterpipe smokers, we offered an additional question on smoking frequency per month. Finally, all subjects were also asked whether they were exposed to environmental tobacco smoke (secondhand smoke) at home or in the workplace.
In addition, we also considered other environmental COPD risk factors, including exposure to woodsmoke or burning coal for heating at home and for cooking (any fuel other than natural gas or electricity). Living with a cat or dog was also considered with one more question. Finally, we asked whether a subject was born in pre-term deliveries and whether he/she was hospitalized for in-patient treatment for COVID-19 sometime in the past.
Medical history of COPD and symptoms were ascertained with a set of ten questions. We first offered a validated CAT questionnaire, which consisted of eight items, scoring from 0 to 5, and the overall score thus ranged from 0 to 40. The tool allowed to discriminate between “fewer symptoms” to “more symptoms”, as well as to score the symptoms severity on a continuous scale. Shortness of breath (if any) was assessed using mMRC tool, in which the score of only one question ranged from 0 to 4. We then asked if a subject ever experienced wheezing (more on expiration) and whether he/she ever woke up at night from wheezing. Finally, we asked if a participant had ever been diagnosed with chronic bronchitis, COPD, bronchial asthma, allergic rhinitis, or pulmonary tuberculosis. The last section of our questionnaire consisted of eight questions of general health-related quality of life, for which we used SF-8 widely used instrument, but these are not analyzed in the current presentation.
JEM-Defined Exposure to Vapors, Gases, Dusts, Fumes and Mists
In a preceding study,19 we defined exposure to vapors, gases, dusts and fumes (VGDF) based on a consilium, and a detailed occupational history with job lists throughout work history was collected in each participant. Following debate on the accuracy of such occupational exposure definition vs the use of job-exposure matrices (JEM),25–27 we decided to convert all jobs held into exposures using an airborne chemical job exposure matrix (ACE JEM) in the current study. ACE JEM has been reported as a reliable instrument to develop information on the occupational exposure via inhalational route from the UK Biobank.28 We identified each position held for a year or more, linked it to the Standard Occupational Classification (SOC) 2000 codes and then produced occupational exposure to either vapor, gas, dust, biodust, mineral dust, fume, diesel exhaust, fiber, mist, asbestos, metal, as well as for a composite exposure to VGDF. These exposures were reported as binary variables. We did not consider work positions held for less than one year. In addition, we also computed the overall years in service for all positions defined as VGDF-associated.
Spirometry
In all subjects, we completed reproducible forced expiratory spirometry using a calibrated spirometer “MAS-2PC” (Belintelmed LLN, Belarus), which operated with a licensed software on a notebook. We applied GLI-2012 reference values for all participants. For a forced spirometry, we aimed to perform as many attempts as needed to attain repeatable curves graded A for either forced expiratory volume in 1 second (FEV1) or for forced vital capacity (FVC).29 ΔFEV1 or ΔFVC could be achieved when at least three repeatable (difference less than 150 mL) were received. We also ensured high quality by checking the end-curve errors, back extrapolation volume and curved acceptability as required by the guidelines.29 We analyzed z-scores (N standard deviations from the predicted values), and subjects with FEV1/FVC below lower limit of normal (LLN) were asked to do bronchodilation with salbutamol with a spacer. To consider a patient having an irreversible obstructive ventilation defect and COPD, we relied on post-bronchodilation FEV1/FVC < LLN. All procedures, including criteria for reversibility, time of repeated test and salbutamol dose were guided by the international recommendations.29,30 COPD patients were defined as those with irreversible obstructive defect (post-bronchodilator FEV1/FVC below −1.64 z-scores). We also measured other volumes and flows, but only FEV1, FVC and FEV1/FVC are analyzed in the current context.
Statistical Analysis
The primary outcome of interest in this study was the overall COPD prevalence in the studied population aged 18 years and older, as well as the prevalence in those aged 40 and older. Secondary outcomes were the odds of COPD from a list of exposures, which we considered in the questionnaires. We first tested all variables for normality, and most of them were non-normally distributed; therefore, we only used and presented non-parametric tests hereinafter. Medians with interquartile ranges (IQR) were shown for all continuous variables, whereas the binary variables were characterized with percent to the whole group. Non-parametric tests to compare two groups were Mann–Whitney U-test or χ2 tests for binary data from contingency tables. Multiple groups were compared in the univariate analyses using Kruskall–Wallis test (or χ2 tests for binary data). A range of univariate comparisons included tests of men vs women; subjects with obstruction vs those with no obstruction and even mild with moderate and severe COPD. Such tests included all variables from the questionnaires, including demographics, smoking, exposure to VGDF, exposure to the use of fossil fuel for cooking and heating, secondhand smoke, regular exercise 3 times a week or more, tuberculosis in the past, preterm birth and so on.
For secondary outcomes, we first tested all variables for their association with COPD in the entire group in the univariate comparisons (in detail specified in the Results) and then checked multicollinearity. Those significantly associated with COPD using χ2 tests, were then included in the adjusted for each other multivariate model, in which we reported adjusted odds ratio (OR) with the corresponding 95% confidence intervals (CI) for each predictor. For convenience, in addition to univariate comparisons of risk factors using χ2 tests for binary data or Mann–Whitney U-test for continuous variables, we also present crude ORs with their corresponding 95% CIs in the unadjusted (crude) logistic regression models. Therefore, such adjusted ORs for a selected predictor reflected its effect independent of all other included variables. In all tests, p-values below 0.05 were considered significant, and all tests were completed in NCSS2025 (Utah, USA).
Results
Overall Sample Descriptive Data
Overall, we collected data for 5058 participants, but excluded 432 subjects due to missing or unacceptable quality spirometry. Therefore, our analysis was based on 4626 study participants (age 47; IQR 31;60 years), equally distributed from all five regions. Participants’ demographic, lifestyle and exposure data are presented in Table 1. This study participants demonstrated educational and socioeconomic profile typical for the general public portrait in Kazakhstan, with 33% possessing university or academic degree and most having an income of below 500,000 tenge a month. Women were significantly more educated, but men were younger and taller. Thirty-eight percent of our population were either current or former cigarette smokers, with rates of current smoking notably greater in men compared to women (Table 1). Waterpipe smoking or electronic cigarette use was reported by a small number of subjects in the study. Furthermore, much more men were exposed to environmental (secondhand) tobacco smoke (41% vs 20%, p < 0.001) and were employed for occupations with VGDF exposure (62% vs 46%, p < 0.001). However, their overall occupational exposure was shorter in years compared to women, apparently because women were generally older.
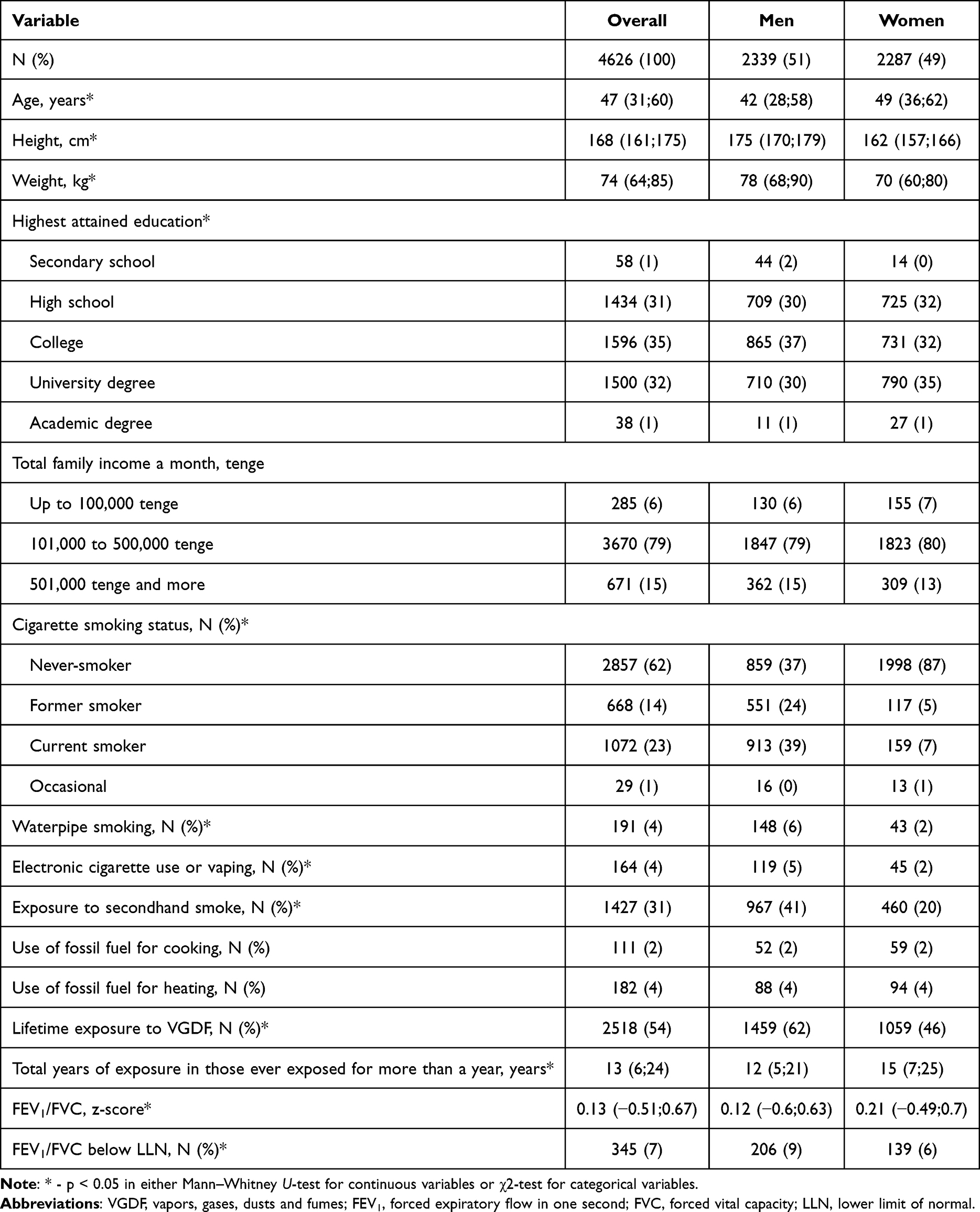 |
Table 1 Demographic, Lifestyle and Exposure Data of Study Participants |
Lifetime exposure to VGDF for more than one year was the most prevalent environmental exposure. More than half of the population under study has ever been exposed, as assessed with JEM. Within this group of airborne exposures, study participants could be exposed to only one inhalant domain or in their combination. Thus, 1320 subjects (29%) were exposed to vapor, 1462 (32%) to gas, 2129 (46%) to dust, 1142 (25%) to biodust, 1500 (32%) to mineral dust, 1247 (27%) to fume, 903 (20%) to diesel, 812 (18%) to fiber, 891 (19%) to mist, 1377 (30%) to asbestos, and 379 (8%) to metal. Any lifetime exposure to VGDF was not only associated with sex (Table 1) but also with ever-smoking (unadjusted OR 2.33 (95% CI 2.04;2.63)) and poorer education (data not shown).
Quality of Spirometry
The overall number of spirometric maneuvers ranged from 1 to 27, whereas the median number of maneuvers was four (Table 2). As a whole, quality criteria attainment for FEV1 was generally easier compared to FVC. The median ΔFVC was far below the threshold value of 0.15 L for adults, indicative of high maneuvers reproducibility, and 78% of participants could achieve A or B grade for ΔFVC quality (Table 2). ΔFEV1 quality criteria were achieved in even more participants (median ΔFEV1 was 0.06) with 93% of subjects to fall below 0.15 L. Similarly, the quality of such tests was graded high, because 83% subjects could reach quality A or B for ΔFEV1. Of note, COPD patients performed significantly better on ΔFEV1 criteria than ΔFVC, and more COPD patients could reach A quality for ΔFEV1 compared to non-obstructive patients. As Table 1 shows, the median z-score of FEV1/FVC was 0.13, and 345 (7%) participants had obstruction, because their post-bronchodilator FEV1/FVC was below LLN. This represented the prevalence of COPD in the general population of population 18 years and older in this study.
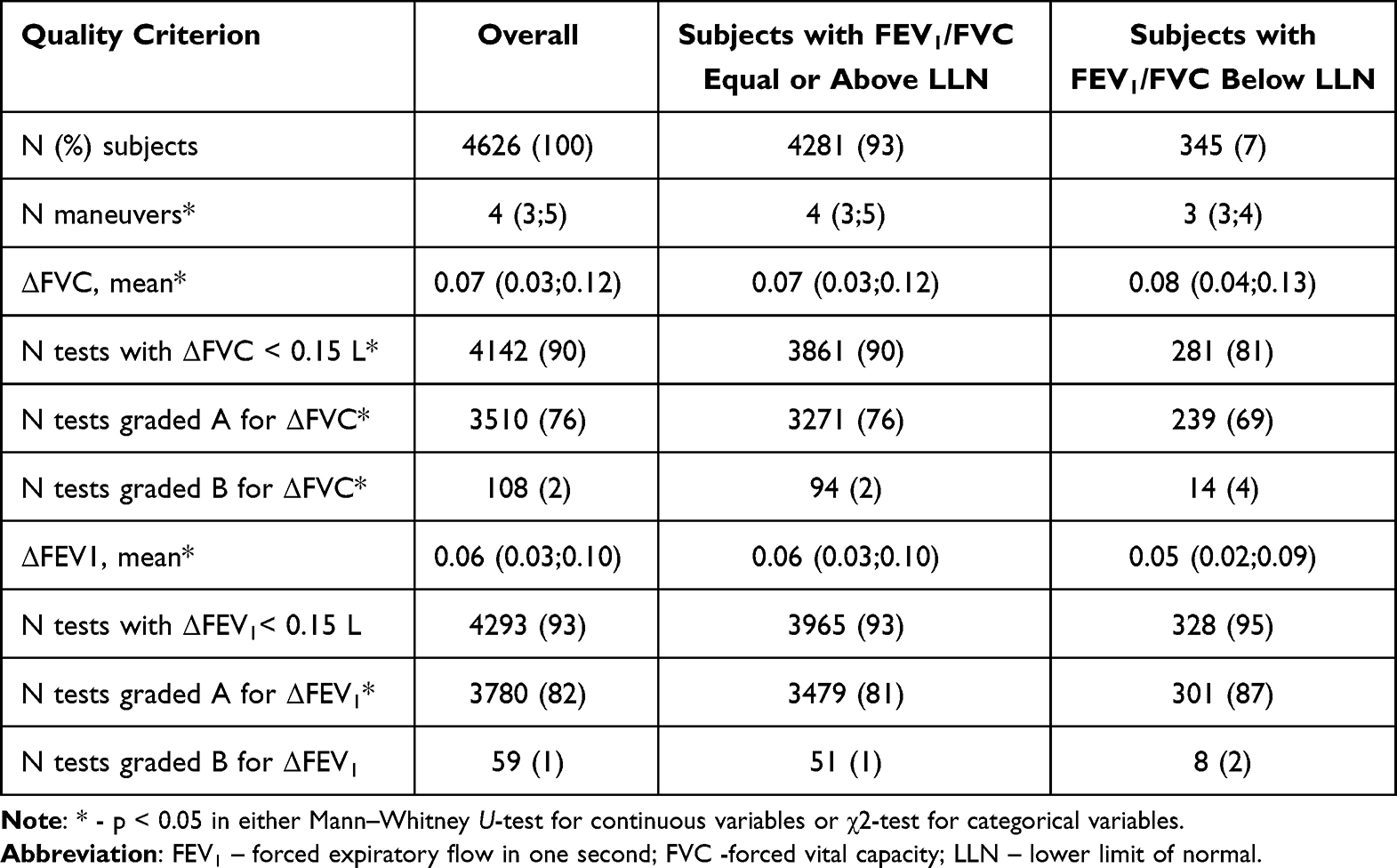 |
Table 2 Summary Table of Spirometry Quality Overall and in COPD Patients as Compared to Non-Obstructive Participants |
COPD Prevalence
Seven percent of the entire studied group had COPD (N = 345), more in men compared to women (9% vs 6%, Table 1). Despite having a brisk clinical presentation (median CAT score 13 in COPD patients vs 0 in non-obstructive participants), only 105 of these 345 (30%) COPD patients were ever told they had COPD, leaving 70% of such patients with no diagnosis before. Chronic bronchitis as a diagnosis ever mentioned by a doctor to these patients was reported by 75 (22%) of them, bronchial asthma by 102 (30%) and allergic rhinitis in 33 (10%). On the other hand, out of 268 subjects who stated they were told by a doctor they had had COPD before, obstructive defect was found in only 103 of them (38%). Should subjects of age 40 and older be considered (N = 2853), 304 subjects had COPD (prevalence 10.7%). In this age group, men again demonstrated greater COPD prevalence (14.5%, 184 of 1266) compared to women (7.6%, 120 of 1587), but the difference now increased dramatically.
COPD patients exhibited high exposure to all studied environmental exposures, including cigarette ever-smoking, secondhand tobacco smoke and VGDF (Table 3). With advancing disease, classified with FEV1/FVC z-score, patients were older, had significantly greater symptoms burden and were more exposed to all studied exposures, except secondhand smoke. Of note, the number of smoking subjects and percent of exposed to VGDF in their lifetime reached 71% and 76%, accordingly in the group of most severe FEV1 lessening.
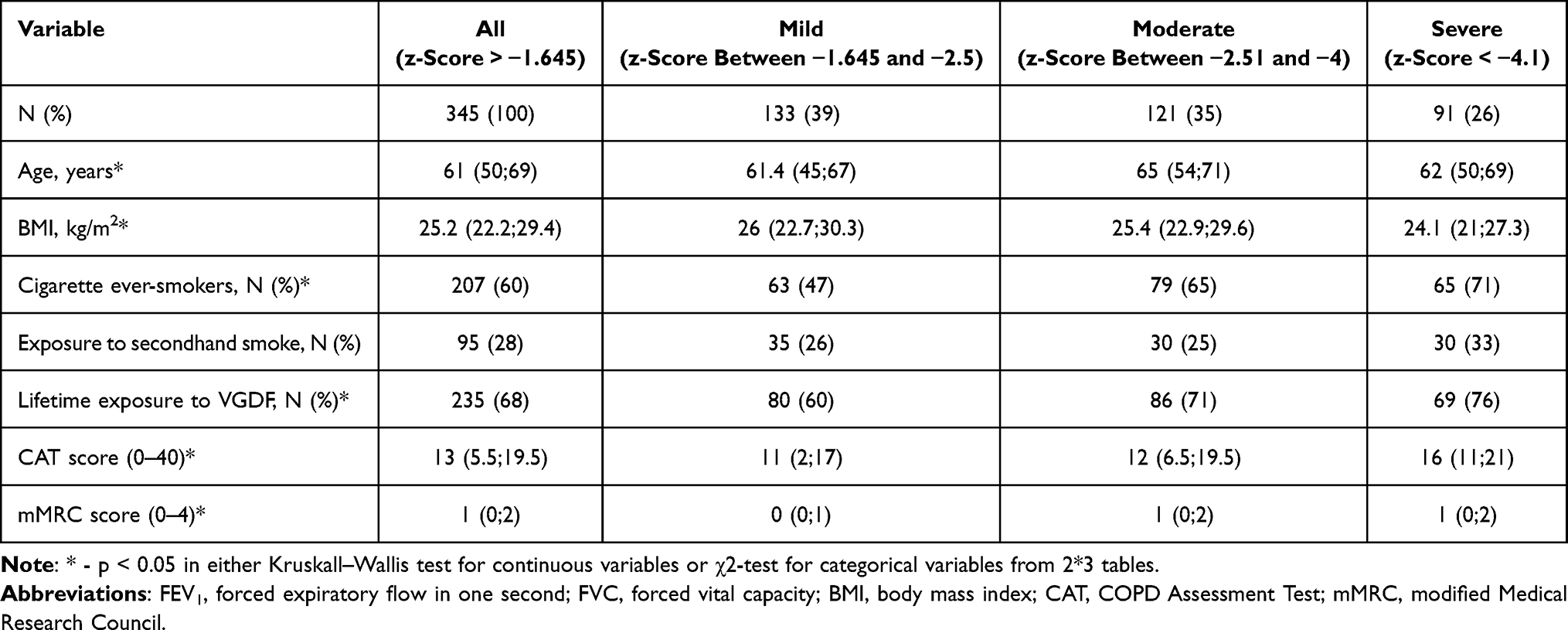 |
Table 3 Exposure and Symptoms Scores in COPD Patients as a Whole and in Different Severity Groups Classified with FEV1 z-Scores |
COPD Risk Factors
In the univariate analyses of selected risk factors for COPD in the entire group, COPD was associated with age, male sex, cigarette ever-smoking, lifetime exposure to VGDF, lower education, regular physical activity and tuberculosis sometime in the past, but not with exposure to secondhand smoke, low income or pre-term birth (Table 4). All significant predictors, non-collinear, were included in the multivariate model to test their association with COPD. Such model showed highly significant associations of age (OR 1.05; 95% CI 1.04;1.05), ever-smoking (OR 2.44; 95% CI 1.81;3.33), low educational level (OR 1.80; 95% CI 1.42;2.28), exposure to VGDF (OR 1.41; 95% CI 1.10;1.82), regular exercise (OR 0.37; 95% CI 0.21;0.63) and tuberculosis in the past (OR 4.12. 95% CI 2.19;7.45) with COPD, with all these predictors putting humans at risk for the disease, except exercise. Sex had no association with COPD when other predictors were considered. Figure 1 demonstrates the magnitude of effects for selected predictors of interest adjusted for each other, sex and age.
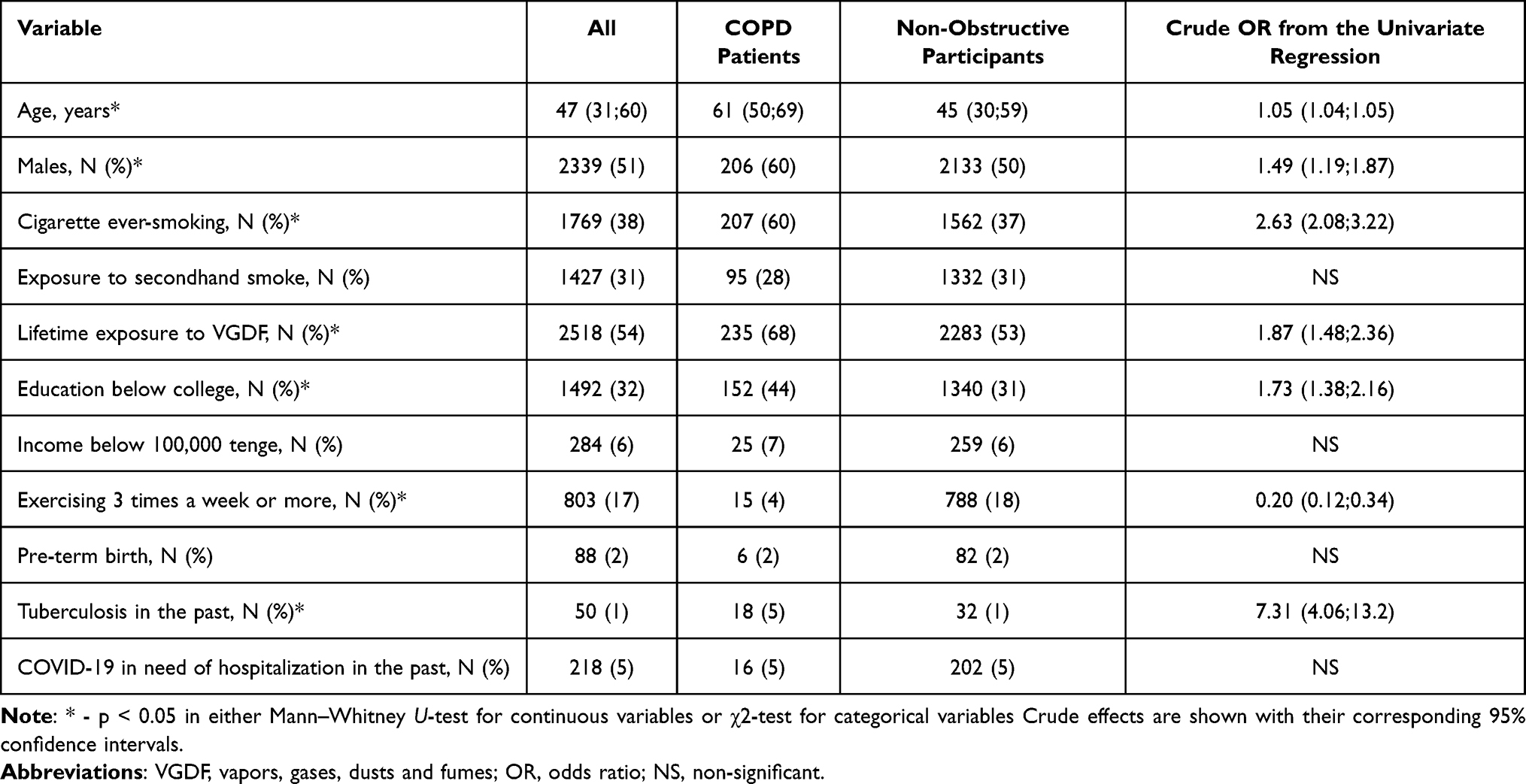 |
Table 4 Selected Risk Factors for COPD in the Univariate Comparisons |
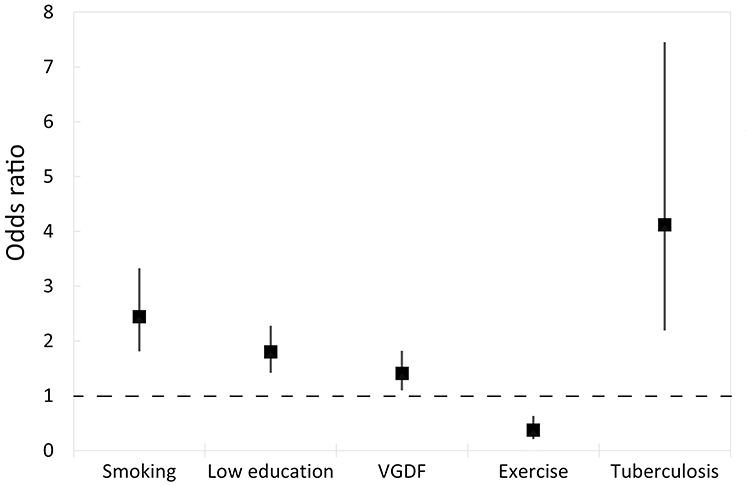 |
Figure 1 Odds ratios with their corresponding 95% CIs for selected predictors for COPD adjusted for each other, sex and age in a multivariate model. |
Discussion
This is the first study in Kazakhstan that assessed the prevalence of COPD all over the country, including central, southern, northern, eastern and western cities and which applied FEV1/FVC < LLN criterion for obstruction along with graded quality approach. This study is also a pioneer population-based nationwide study, which ascertained occupational exposure status using JEM in Kazakhstan. This study demonstrated that, overall, COPD was a common disease with the prevalence of 7% in the age group 18 years and older, greater in men. In subjects aged 40 years and older, the prevalence dramatically rises in men, reaching 15%. Lower socioeconomic status, age, cigarette smoking, occupational exposure to VGDF and tuberculosis in the past were also significantly positively and independently associated with COPD in the general population, whereas regular exercise had an independent protective effect.
The overall prevalence of COPD in the country reached 7%, somewhat similar to the data in Almaty only from the study completed six years ago.19 Although we did not observe the increase in the disease prevalence, higher burden of this disease in men over 40 years is a worrisome trend for the country, likely resulting from the growing ambient air pollution,15 high smoking prevalence,20 occupational exposures and wide use of coal for heating. Data from Central Asian countries have long remained scarce, when most reported studied and those included in the systematic reviews and meta-analyses were from high-income countries, including USA and Western Europe, along with China recently. Moreover, smaller studies from the region in the local literature are often based on the FEV1/FVC < 70% outdated criterion,31 not taking age into account and with no spirometry quality control. Such disparity in the data presentation in the literature results in underrepresentation of Central Asian data in the world estimates of disease burden. Furthermore, unlike smoking, occupational exposures as a major risk factor are yet insufficiently characterized in these countries, creating a gap in understating the overall burden on COPD in the region.17 The current study now fills thus gap assessing the risk from a range of external predictors.
A recent systematic review and meta-analysis demonstrated that COPD prevalence in subjects aged 40 and older could fall within the range of 10.75%–14.65% based on a fixed ratio and 5.47%–9.55% based on below LLN ratio.18 Higher prevalence in men in our study was somewhat comparable to the world data.18 Despite higher precision of below LLN criterion to detect airway obstruction, fixed ratio is still widely used in many studies and some benefits of such approach have been demonstrated,32 although some studies debate whether fixed ration is more applicable for primary care settings.31 Irrespective of the approach to confirm COPD, there is still a notable discrepancy in the prevalence across the world, likely resulting from varying sampling approaches. Given that the disease is chronic, uncurable and progressing, our data of about 7% prevalence in adults is indicative of a very high medical and societal costs to manage these patients. The so-called early COPD33 and a small-airway disease34 with expected progression to COPD with time, will further increase that burden. Official data with patients with the diagnosis and on treatment in Kazakhstan, of note, are times smaller compared to our findings of 7% prevalence. This indicates that most COPD patients are yet unaware they have a disease, and a critical time when early interventions could be efficient, are missed. Furthermore, growing COPD prevalence in women,16 even with much lower burden of smoking and occupational exposures, will necessitate further action. This has, indeed, clear public health implications.
One of the novelties of this report was the use of JEM for occupational exposure classification in Kazakhstan. Despite no consensus in the academic community whether JEM are more accurate compared to self-reported exposure, this tool for airborne pollutants in COPD helps identify exposures in the workplace where subjects were uncertain whether they had been exposed.25,27,35 These JEMs are easy to use in the general population surveys, but the estimates of risk via JEM as compared to self-report may be different.35 Our current data from all over the country revealed a 41% greater risk in subjects with lifetime ever-exposure to VGDF, somewhat greater compared to estimates from the meta-analysis.35 These estimates imply that early interventions, increase in awareness, wider use of personal protective equipment may eventually dramatically increase the risk and lessen the burden to the health system for decades of life when these subjects would live with the disease.
Among other risk factors with significant associations with COPD in multivariate analyses, tuberculosis in the past was a variable with the largest magnitude of effect. This finding is consistent with preceding reports,36–38 also in low- and middle-income countries, especially in very low resource settings, such as in Africa.38 Meta-analyses of observational studies consistently demonstrated an increase of COPD incidence in subjects with tuberculosis in the past, greater in low-income countries.37,38 This has clear implications for COPD prevention, since subjects with tuberculosis in the past should probably be offered a more intense screening for COPD and other risk factors elimination, such as smoking.
In addition to the novel use of JEM to classify occupational exposures, this study has also other strengths, including the use of z-scores of FEV1/FVC as opposed to fixed ratio; the use of a detailed questionnaire to elucidate a range of potential confounders, including smoking, secondhand smoke, use of fossil fuel for heating and even socioeconomic status. Moreover, this study is the first to include cities outside the list of three major locations usually involved in epidemiological studies, such as Aktobe, Kostanay and Ust-Kamenogorsk. Another strength is a strict quality control of spirometry with the subsequent analysis of quality criteria, never done before in Kazakhstan. Altogether, this makes this epidemiological study a pioneer report on the COPD burden in Kazakhstan. However, the limitations should also be noted. We could not match data on air quality in the selected cities so that the contribution of air pollution could be taken into account to explain COPD in never smoking and never exposed to VGDF patients. Secondly, we could not, due to logistic reasons, include subjects living outside the cities. Finally, we could not offer a detailed clinical assessment to patients with COPD, other than CAT and mMRC with history.
We believe that our study is important for policy in chronic disease management and has clear implications. First, a large fraction of patients with the disease, mostly at the initial stage, are unaware of the disease, have not been offered high-quality spirometry and did not receive treatment. Moreover, treatment effectiveness, compliance with treatment and performance in the use of inhaled are almost uncovered in Kazakhstan. Other countries reported high percent of COPD receiving treatment,39 but this may unlikely be the case of Kazakhstan, because most patients with COPD have yet not received the diagnosis. This study necessitates more active case finding in subjects at risk and even with symptoms, and this will save years of life for COPD patients in future, if the disease is timely recognized. At present, COPD patients in Kazakhstan have their condition recognized only with notable clinical signs and when they have access to high-quality spirometry.
Ways to mitigate the effects of established risk factors of COPD also need a deeper look both by the research community and decision makers. High smoking prevalence, severe air pollution in winter and high levels of exposure in some workplaces need a comprehensive policy plan, including monitoring, assessment and action. Population protection from heavy air pollution and secondhand smoke must be set as a public health priority in Kazakhstan for healthier living overall and reduced burden of chronic respiratory disease in particular.
Conclusion
This nationwide population-based study clearly articulated the problem of unacceptable case finding and poor access to screening to detect COPD at early stages in Kazakhstan. Disease prevalence was times greater compared to patients on treatment in the state registries. Independent of each other, smoking, occupational exposure, poorer socioeconomic status and even past tuberculosis increased the risk in Kazakhstan population. Primary prevention should be then targeted to smoking cessation, reducing exposure to airborne occupational hazards, active involvement in recreational physical activity and population’s active participation in early screening.
Acknowledgments
We would like to thank all regional coordinators in data collection, including Kaisar Anapin (Aktobe), Gulnara Bekmagambetova (TOO Kasaras, Kostanay), Mikhail Bugaitsov (East Kazakhstan Regional Hospital, Ust-Kamenogorsk), Yuliya Khokhlova (Karaganda Medical University, Karaganda), Assiya Кushekbayeva (South Kazakhstan Medical Academy, Shymkent), Dmitriy Sredin (City Center of Primary Health Care, Karaganda), Fariza Turdaly (Regional clinical hospital of the Turkestan region, Shymkent).
Funding
This research was funded by the Science Committee of the Ministry of Science and Higher Education of the Republic of Kazakhstan (Grant No. AP23484384).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Iheanacho I, Zhang S, King D, Rizzo M, Ismaila AS. Economic Burden of Chronic Obstructive Pulmonary Disease (COPD): a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2020;15:439–11. doi:10.2147/COPD.S234942
2. Boers E, Barrett M, Su JG, et al. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Netw Open. 2023;6(12):e2346598. doi:10.1001/jamanetworkopen.2023.46598
3. Dou L, Zheng Y, Feng J, et al. The humanistic and economic burden of COPD patients in urban china: a propensity score matching study. Int J Chronic Obstr. 2025;20:2993–3004. doi:10.2147/COPD.S524028
4. Wang Z, Lin J, Liang L, et al. Global, regional, and national burden of chronic obstructive pulmonary disease and its attributable risk factors from 1990 to 2021: an analysis for the global burden of disease study 2021. Respir Res. 2025;26(1):2. doi:10.1186/s12931-024-03051-2
5. Cioboata R, Balteanu MA, Mitroi DM, et al. Beyond smoking: emerging drivers of COPD and their clinical implications in low- and middle-income countries: a narrative review. J Clin Med. 2025;14(13):4633. doi:10.3390/jcm14134633
6. Miravitlles M, Ribera A. Understanding the impact of symptoms on the burden of COPD. Respir Res. 2017;18(1):67. doi:10.1186/s12931-017-0548-3
7. Chen W, Thomas J, Sadatsafavi M, FitzGerald JM. Risk of cardiovascular comorbidity in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Lancet Respir Med. 2015;3(8):631–639. doi:10.1016/S2213-2600(15)00241-6
8. He Y, Qian DC, Diao JA, et al. Prediction and stratification of longitudinal risk for chronic obstructive pulmonary disease across smoking behaviors. Nat Commun. 2023;14(1):8297. doi:10.1038/s41467-023-44047-8
9. Laniado-Laborín R. Smoking and Chronic Obstructive Pulmonary Disease (COPD). parallel epidemics of the 21st century. Int J Environ Res Public Health. 2009;6(1):209–224. doi:10.3390/ijerph6010209
10. Vinnikov D, Blanc PD, Brimkulov N, Redding-Jones R. Five-year lung function observations and associations with a smoking ban among healthy miners at high altitude (4000 m). J Occup Environ Med. 2013;55(12):1421. doi:10.1097/JOM.0b013e3182a641e7
11. FWS K, Hui DSC. Air pollution and chronic obstructive pulmonary disease. Respirology. 2012;17(3):395–401. doi:10.1111/j.1440-1843.2011.02112.x
12. Qian Y, Cai C, Sun M, Lv D, Zhao Y. Analyses of factors associated with acute exacerbations of chronic obstructive pulmonary disease: a review. Int J Chron Obstruct Pulmon Dis. 2023;18:2707–2723. doi:10.2147/COPD.S433183
13. Manisalidis I, Stavropoulou E, Stavropoulos A, Bezirtzoglou E. Environmental and health impacts of air pollution: a review. Front Public Health. 2020;8:14. doi:10.3389/fpubh.2020.00014
14. Wang Q, Liu S. The effects and pathogenesis of PM2.5 and its components on chronic obstructive pulmonary disease. COPD. 2023;18:493–506. doi:10.2147/COPD.S402122
15. Vinnikov D, Rapisarda V, Babanov S, et al. High levels of indoor fine particulate matter during the cold season in Almaty prompt urgent public health action. PLoS One. 2023;18(5):e0285477. doi:10.1371/journal.pone.0285477
16. Liu Z, Jiao M, Lv J, Han Q. Increased incidence of chronic obstructive pulmonary disease in women due to long-term passive smoking. Int J Chronic Obstr. 2025;20:2745–2752. doi:10.2147/COPD.S534060
17. Vinnikov D, Rybina T, Strizhakov L, Babanov S, Mukatova I. Occupational burden of chronic obstructive pulmonary disease in the commonwealth of independent states: systematic review and meta-analysis. Front Med. 2021;7. doi:10.3389/fmed.2020.614827
18. Al Wachami N, Guennouni M, Iderdar Y, et al. Estimating the global prevalence of chronic obstructive pulmonary disease (COPD): a systematic review and meta-analysis. BMC Public Health. 2024;24(1):297. doi:10.1186/s12889-024-17686-9
19. Vinnikov D, Raushanova A, Kyzayeva A, et al. Lifetime occupational history, respiratory symptoms and chronic obstructive pulmonary disease: results from a population-based study. Int J Chronic Obstr. 2019;14:3025–3034. doi:10.2147/COPD.S229119
20. Ibrayeva A, Shoranov M, Aipov R, Katarbayev A, Tanabayeva S, Fakhradiyev I. Prevalence and characteristics of tobacco use among adults in Kazakhstan: a cross-sectional National Survey. Global Epidemiol. 2025;9:100194. doi:10.1016/j.gloepi.2025.100194
21. Tursun K, Omarova A, Ibragimova OP, et al. Dominant sources of PM2.5 in Kazakhstan’s urban cities: a PMF and HYSPLIT-based study for air quality management in Central Asia. Urban Climate. 2025;64:102706. doi:10.1016/j.uclim.2025.102706
22. Muratuly A, Mukhtarov R, Radelyuk I, Karaca F, Baimatova N. Urban PM2.5 pollution in Kazakhstan: health burden and economic costs. Environ Sci Adv. 2026;5(1):281–291. doi:10.1039/D5VA00194C
23. Vinnikov D, Romanova Z, Raushanova A, et al. Exposure to respirable particulate matter and its association with respiratory outcomes in beauty salon personnel. Int J Environ Res Public Health. 2023;20(3):2429.
24. Vinnikov D, Tulekov Z, Raushanova A. Occupational exposure to particulate matter from air pollution in the outdoor workplaces in Almaty during the cold season. PLoS One. 2020;15(1):e0227447. doi:10.1371/journal.pone.0227447
25. Dopart PJ, Friesen MC. New opportunities in exposure assessment of occupational epidemiology: use of measurements to aid exposure reconstruction in population-based studies. Curr Envir Health Rpt. 2017;4(3):355–363. doi:10.1007/s40572-017-0153-0
26. Damerau LS, Herold R, Preisser AM, et al. Comparison of self-reported and job-exposure matrix assessed workplace inhalant exposures and their association with obstructive airways disease. Sci Rep. 2025;15(1):14099. doi:10.1038/s41598-025-95923-w
27. Descatha A, Fadel M, Sembajwe G, Peters S, Evanoff BA. Job-exposure matrix: a useful tool for incorporating workplace exposure data into population health research and practice. Front Epidemiol. 2022;2. doi:10.3389/fepid.2022.857316
28. Sadhra SS, Kurmi OP, Chambers H, Lam KBH, Fishwick D. The Occupational COPD Research Group. Development of an occupational airborne chemical exposure matrix. Occup Med. 2016;66(5):358–364. doi:10.1093/occmed/kqw027
29. Graham BL, Steenbruggen I, Miller MR, et al. Standardization of spirometry 2019 update. an official American Thoracic Society and European Respiratory Society technical statement. Am J Respir Crit Care Med. 2019;200(8):e70–e88. doi:10.1164/rccm.201908-1590ST
30. Stanojevic S, Kaminsky DA, Miller MR, et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur Respir J. 2022;60(1). doi:10.1183/13993003.01499-2021
31. Llordés M, Jaen A, Zurdo E, et al. Fixed ratio versus lower limit of normality for diagnosing COPD in primary care: long-term follow-up of EGARPOC study. Int J Chron Obstruct Pulmon Dis. 2020;15:1403–1413. doi:10.2147/COPD.S250720
32. Miller MR, Haroon S, Jordan RE, et al. Clinical characteristics of patients newly diagnosed with COPD by the fixed ratio and lower limit of normal criteria: a cross-sectional analysis of the TargetCOPD trial. Int J Chron Obstruct Pulmon Dis. 2018;13:1979–1986. doi:10.2147/COPD.S146914
33. Yang W, Li F, Li C, Meng J, Wang Y. Focus on early COPD: definition and early lung development. Int J Chron Obstruct Pulmon Dis. 2021;16:3217–3228. doi:10.2147/COPD.S338359
34. Wen G, Meng J, Xu Y, et al. Prevalence and risk factors of spirometry-defined small airway dysfunction in the high-risk population for COPD in Yunnan Province, China: a population based cross-sectional study. Int J Chron Obstruct Pulmon Dis. 2025;20:3005–3017. doi:10.2147/COPD.S543042
35. Sadhra S, Kurmi OP, Sadhra SS, Lam KBH, Ayres JG. Occupational COPD and job exposure matrices: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2017;12:725–734. doi:10.2147/COPD.S125980
36. Zavala MJ, Becker GL, Blount RJ. Interrelationships between tuberculosis and chronic obstructive pulmonary disease. Curr Opin Pulm Med. 2023;29(2):104–111. doi:10.1097/MCP.0000000000000938
37. Fan H, Wu F, Liu J, et al. Pulmonary tuberculosis as a risk factor for chronic obstructive pulmonary disease: a systematic review and meta-analysis. Ann Transl Med. 2021;9(5):390. doi:10.21037/atm-20-4576
38. Njoku CM, Hurst JR, Kinsman L, Balogun S, Obamiro K. COPD in Africa: risk factors, hospitalisation, readmission and associated outcomes-a systematic review and meta-analysis. Thorax. 2023;78(6):596–605. doi:10.1136/thorax-2022-218675
39. Larsson K, Ekberg-Jansson A, Stridsman C, Hanno M, Vanfleteren LEGW. Adherence to treatment recommendations for chronic obstructive pulmonary disease - results from the swedish national airway register. Int J Chron Obstruct Pulmon Dis. 2021;16:909–918. doi:10.2147/COPD.S300299
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.