Back to Journals » Infection and Drug Resistance » Volume 12
Prevalence and risk factors for colonization by extended-spectrum β-lactamase-producing or ST 131 Escherichia coli among asymptomatic adults in community settings in Southern Taiwan
Authors Wu PC, Wang JL ![]() , Hsueh PR, Lin PH, Cheng MF
, Hsueh PR, Lin PH, Cheng MF ![]() , Huang IF, Chen YS
, Huang IF, Chen YS ![]() , Lee SS
, Lee SS ![]() , Guang-Yuan M, Yu HC, Hsu CL, Wang FW, Chen CS, Hung CH, Ko WC
, Guang-Yuan M, Yu HC, Hsu CL, Wang FW, Chen CS, Hung CH, Ko WC ![]()
Received 11 January 2019
Accepted for publication 29 March 2019
Published 3 May 2019 Volume 2019:12 Pages 1063—1071
DOI https://doi.org/10.2147/IDR.S201086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sahil Khanna
Pin-Chieh Wu,1,2,* Jiun-Ling Wang,3,4,* Po-Ren Hsueh,5 Po-Hsiang Lin,6 Ming-Fang Cheng,7–10 I-Fei Huang,7 Yao-Shen Chen,8,11 Susan Shin-Jung Lee,8,11 Mar Guang-Yuan,1,11 Hsien-Chung Yu,1,8,11–12 Chiao-Lin Hsu,1,2 Fu-Wei Wang,2,13 Chi-Shen Chen,1 Chih-Hsin Hung,9 Wen-Chien Ko3,4
1Department of Physical Examination Center, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan; 2Department of Nursing, Meiho University, Pingtung, Taiwan; 3Department of Internal Medicine, National Cheng Kung University Hospital, Tainan, Taiwan; 4Department of Medicine, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 5Departments of Laboratory Medicine and Internal Medicine, National Taiwan University Hospital, National Taiwan University College of Medicine, Taipei, Taiwan; 6Department of Emergency Medicine, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan; 7Department of Pediatrics, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan; 8School of Medicine, National Yang-Ming University, Taipei, Taiwan; 9Department of Chemical Engineering and Institute of Biotechnology and Chemical Engineering, I-Shou University, Kaohsiung, Taiwan; 10Department of Nursing, Fooyin University, Kaohsiung, Taiwan; 11Department of Internal Medicine, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan; 12Institute of Health Care Management, Department of Business Management, National Sun Yat-sen University, Kaohsiung, Taiwan; 13Department of Family Medicine, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
*These authors contributed equally to this work
Purpose: Fecal carriage of extended-spectrum β-lactamase-producing Escherichia coli (ESBL-EC) is common in Asia, especially in China and Southeast Asia. There are no data about fecal carriage of ESBL-EC and mcr-1-positive E. coli in Taiwan, and few studies focusing on the risk factors of asymptomatic fecal carriage of epidemic ST131 E. coli have been published.
Patients and methods: From healthy inhabitants attending health examinations at a medical center in southern Taiwan in 2017, we collected 724 stool samples, which were examined for ESBL-EC fecal carriage using chromogenic medium. ST131 and mcr1-positive E. coli were also investigated using multiplex PCR. Clinical data from all participating adults were collected to analyze the risk factors for fecal ESBL-EC or ST131 E. coli carriage.
Results: The prevalence rate of asymptomatic ESBL-EC fecal carriage in adults was 1.9% (14/724). ST131 was found in 22 (3.0%) adults and mcr-1-positive E. coli was found in three (0.4%) adults. A multivariate analysis showed that the risk factors associated with ESBL-EC carriage were diabetes mellitus (adjusted odds ratio [aOR]: 5.5, 95% confidence interval [CI]: 1.3–22.7), a history of colonic polyps (aOR: 6.4, 95% CI: 1.6–24.9), and chronic renal insufficiency (aOR: 20.7, 95% CI: 1.4–305.7). Underlying cancer (aOR: 4.8, 95% CI: 1.0–22.5) and stroke (aOR: 18.0, 95% CI: 1.6–207.5) were associated with ST131 E. coli fecal carriage. In our cohort, travel to Asian countries and food habit were not associated with ST131 or ESBL-EC fecal carriage.
Conclusions: The ESBL-EC or ST131 E. coli fecal carriage rate is low among asymptomatic adults in Taiwan. Certain underlying medical conditions were associated with their fecal carriage.
Keywords: fecal colonization, extended-spectrum β-lactamase, sequence type, MCR1, Escherichia coli
Introduction
Escherichia coli is a normal inhabitant in the human gastrointestinal tract. However, it is also an important pathogen in adults. In previous decades, the occurrence of extended-spectrum beta-lactamases (ESBL)-producing Enterobacteriaceae, which causes treatment failure of cephalosporin therapy, has become a remarkable epidemiological event. The prevalence of ESBL-E.coli (ESBL-EC) fecal carriage in healthy adults has been increasing alarmingly, at an annual rate of 5.4% worldwide.1 Recently, the prevalence of asymptomatic ESBL-EC carriage was about 5–8% in Europe, 2% in America, 6% in Japan, 19% in India, 30% in China, and 30–50% in Thailand.2–6 Antibiotic exposure within 6 months, daily animal contact, or travelling to Africa or Asia, had been linked to asymptomatic ESBL-EC fecal carriage.2–6 Colistin was considered to be the last-line antimicrobial agent for treating patients with multidrug-resistant bacteria,7,8 but in 2015, the plasmid-mediated colistin resistance gene, mcr-1, was first described in China. Since then, mcr-1 has been identified in the environment, animals, and humans.7 However, there are no data on fecal carriage of ESBL-EC and mcr-1 E. coli in asymptomatic people in other Asian regions including Taiwan. Moreover, few studies have focused on the risk factors for fecal carriage of ST131 E. coli, an epidemic strain, in the asymptomatic population. Therefore, the aims of this study were to determine the prevalence and risk factors for asymptomatic carriage of ESBL-EC, mcr-1 E. coli, or ST131 E. coli in Taiwan.
Materials and methods
Participants
This study was conducted from April 2016 to June 2017 at the health check center in Kaohsiung Veterans General Hospital, which is located in southern Taiwan. All individuals visiting the health check center routinely fill out a standardized questionnaire, which including demographic data, personal history, medical history, and underlying chronic illness (such as peptic ulcer or colonic polyps, antibiotic therapy, or probiotic use in the past 3 months), boiled or unboiled drinking water, and diet habits.
The aforementioned data was recorded by one physician at our center during health exam interview. The participants were randomly selected and their residual fecal samples for fecal occult blood tests were collected. Only individuals whose data in the dataset of the questionnaires was intact were included in this study. Hyperuricemia was defined as a serum uric acid level ≥7 mg/dL,9 and chronic renal diseases were defined as serum creatinine >1.5 mg/dL. With a high prevalence of ESBL-EC in Asia, especially in Southeast Asia, India, and China, we also collected the participants’ travel information.2–6 The study was approved by the Ethics Committee at the Kaohsiung Veterans General Hospital (VGHKS16-CT2-04). The ethics committee waived the need for written informed consent provided by participants due to the noninterventional and retrospective nature of the study. Because all patient data were analyzed in anonymity, no additional informed consent was required.
Isolation of bacteria and microbiological analysis
Each stool sample was spread on a CHROMagar™ ECC plate (CHROMagar, Paris, France) and incubated at 37 °C for 24 h and up to two E. coli colonies were selected. If the colony color was dark pink to reddish, it was spread onto a CHROMagar™ ESBL plate (CHROMagar, Paris, France) to identify ESBL-EC isolates. ESBL genes, including blaCTX-M, blaSHV, blaTEM, blaOXA-1, blaIMP, and blaVIM, were assessed using the polymerase chain reaction (PCR) using previously described primers and methods,10–13 if ESBL-EC fecal carriage was found using chromogenic medium. PCR amplification was performed as follows: initial denaturation at 94 °C for 10 min; 30 cycles of 94 °C for 40 s, 60 °C for 40 s, and 72 °C for 1 min; and a final elongation step at 72 °C for 7 min.12 Four E. coli sequence types, including ST69, ST73, ST95, and ST131, were studied using primers and a PCR method, which were previously described, with the following cycling conditions: an initial denaturation at 94 °C for 3 min; 30 cycles of 94 °C for 30 s, 60 °C for 30 s, and 72 °C for 30 s; and one final cycle of 72 °C for 5 min.14 The ESBL-EC multilocus sequence types (MLST) were confirmed by testing seven housekeeping gene sequences (adk, fumC, gyrB, icd, mdh, purA, and recA).10 Screening mcr-1 in E. coli isolates was conducted using PCR with the primers CLR5-F (5ʹ-CGGTCAGTCCGTTTGTTC-3ʹ) and CLR5-R (5ʹ-CTTGGTCGGTCTGTA GGG-3ʹ) with the initial denaturation conditions of 94 ºC for 15 min; 25 cycles of 94 ºC for 30 s, 58 ºC for 90 s, and 72 ºC for 60 s; and a final cycle of 72 ºC for 10 min.7 ST131-positive control isolates and ESBL gene-positive and mcr-1-positive isolates were obtained from previous study.15,16
Antimicrobial susceptibility
Cefazolin, ceftriaxone, and levofloxacin antibiotic susceptibility was measured using the disk diffusion technique on Muller-Hinton medium, according to the Clinical Laboratory Standard Institute (CLSI) guidelines.17 Antimicrobial susceptibility of ampicillin/sulbactam, piperacillin/tazobactam, cefazolin, cefmetazole, cefotaxime, ceftazidime, cefepime, ertapenem, meropenem, imipenem, amikacin, gentamycin, ciprofloxacin, levofloxacin, trimethoprim/sulfamethoxazole, and tigecycline for the mcr-1-positive E. coli isolates was measured using the Vitek 2 system (Vitek AMS; bioMerieux Vitek Systems Inc., Hazelwood, MO, USA). The minimum inhibitory concentration (MIC) of colistin was determined using the broth microdilution test and interpreted based on the 2017 CLSI guidelines.17
Statistical analysis
Categorical variables were analyzed using the chi-square and Fisher’s exact tests and the independentsamplest-test was used to analyze continuous variables in univariate analysis. Multivariable analyses in the logistic regression model were used to study risk factors of asymptomatic ESBL-EC and ST131 E. coli carriage. Variables with a P-value of ≤0.1 in univariate analyses were entered into a forward logistical regression analysis. P-values <0.05 were considered to be statistically significant. The adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Statistical analyses were performed using SPSS version 20.0 for Windows (SPSS Inc., Armonk, NY, USA).
Results
During the study period, fecal occult blood tests were performed in 5,042 individuals. Among them, 743 individuals were randomly selected for enrollment and 724 participants were finally included in the study due to 19 individuals with incomplete data in the dataset of the questionnaires. There were 513 E. coli isolates found in the stool in the PCR study. The participants’ mean age was 46.9 years, and females predominated, accounting for 52.1% of the study population. Common underlying diseases included hypertension (101/724 individuals, 14%), diabetes mellitus (31/724, 4.3%), and cancer (17/724, 2.3%). Antibiotic therapy in the previous 3 months was recalled in 8.4% (61/724) of participants. Half (367/724, 50.7%) of the participants had travelled abroad recently, including 44.6% (323/724) who travelled to Asia, 4.1% (30/724) who travelled to Europe, 5.2% (38/724) who travelled to North America, 0.4% (3/724) who travelled to Africa, and 1.2% (8/724) who travelled to Oceania. The prevalence rate of fecal ESBL-EC carriage was 1.9% (14/724) and that of ST131 E. coli carriage was 3.0% (22/724). Two (14.3%) of 14 ESBL-EC isolates belonged to ST131.
In the univariate analyses, two variables were associated with asymptomatic ESBL-EC fecal carriage: diabetes mellitus (OR 6.6, 95% CI 1.8–25.2) and colonic polyps (OR 6.0, 95% CI 1.6–22.5; Table 1). The multivariate logistic regression model showed that diabetes mellitus (aOR 5.5, 95% CI 1.3–22.7), colonic polyps (aOR 6.4, 95% CI 1.6–25.0), and chronic renal insufficiency (aOR 20.7, 95% CI 0.4–305.7) were significantly associated with ESBL-EC carriage (Table 1). Among 14 isolates with the ESBL-production phenotype, six isolates had blaTEM, six had blaSHV, four had blaCTX-M, one had blaVIM, one had blaOXA-1, and one had blaIMP (Table 2). Five isolates had more than one ESBL gene. The major CTX-M enzyme was CTX-M-14, which was found in three isolates. Among 14 isolates of ESBL-EC, the sequence types (STs) included ST131 (n=2), S1193 (n=2), ST10 (n=1), ST38 (n=1), ST101 (n=1), ST127 (n=1), ST349 (n=1), ST410 (n=1), ST963 (n=1), ST1972 (n=1), ST2607 (n=1), and S3045 (n=1).
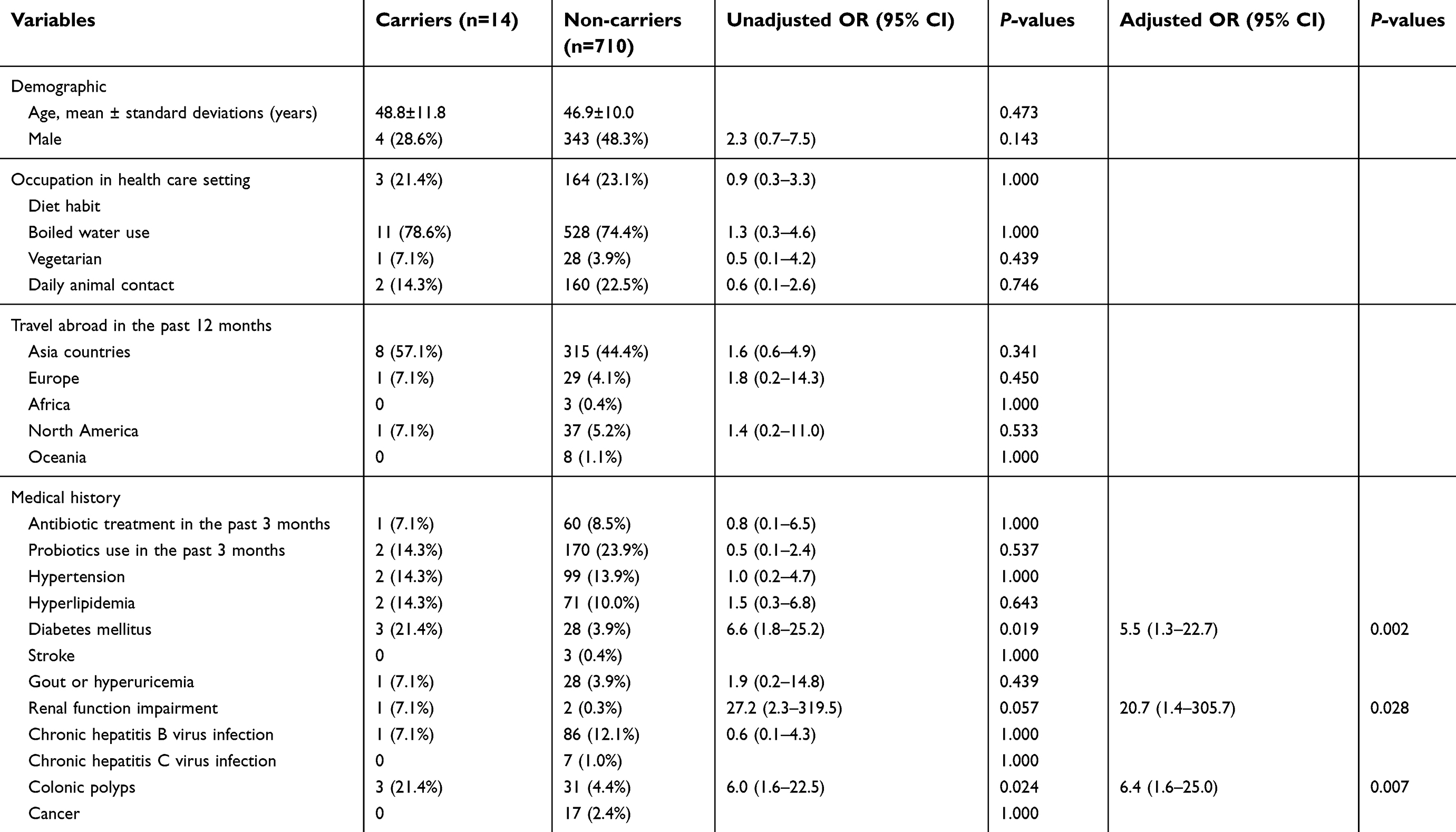 | Table 1 Characteristics of 724 subjects with and without fecal extended-spectrum beta-lactamase-producing Escherichia coli carriage |
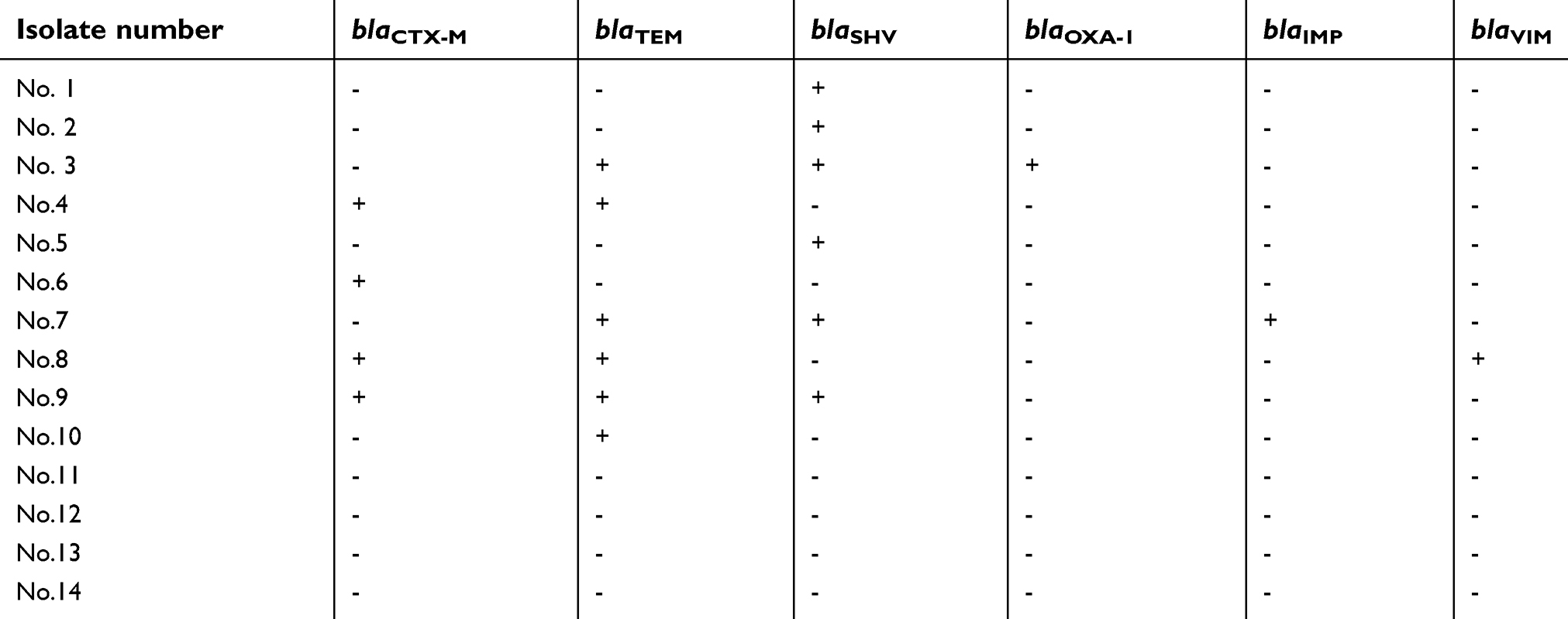 | Table 2 The distribution of beta-lactamase genes in 14 Escherichia coli isolates with the extended-spectrum beta-lactamse-production phenotype |
Underlying disease of cancer (OR 4.8, 95% CI 1.02–22.5) or stroke (OR 18.0, 95% CI 1.6–207.5) was associated with asymptomatic ST131 E. coli fecal carriage using the univariate analysis and multivariable logistic regression analysis (Table 3).
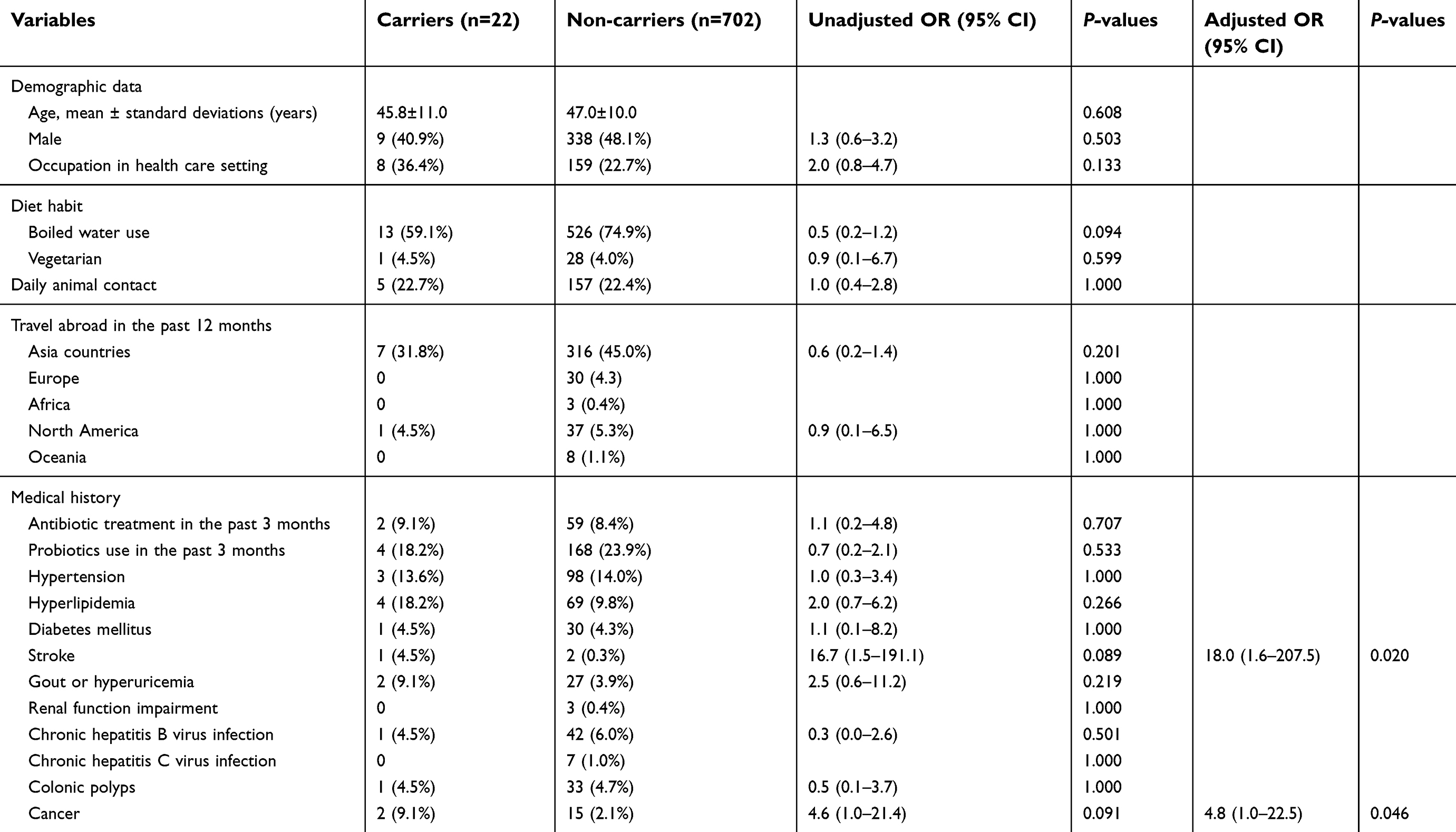 | Table 3 Characteristics of 724 subjects with and without fecal ST131 Escherichia coli carriage |
For antibiotic susceptibility, ST131 isolates had a higher resistance rate to cefazolin (68.2% vs 58.6%, P=0.380), ceftriaxone (22.7% vs 9.7%, P=0.070), and levofloxacin (50% vs 29.5%, p=0.045) than non-ST131 isolates. ESBL-EC isolates were more likely to be resistant to cefazolin (92.9% vs 57.7%, P=0.009), ceftriaxone (78.6% vs 7.3%, P<0.001), and levofloxacin (42.9% vs 30.4%, P=0.377) than non-ESBL-EC isolates.
mcr-1 was identified in three E. coli isolates, which were not ST131 or ESBL-EC. The prevalence of fecal mcr-1 E. coli carriage was 0.4% (3/724). Clinical characteristics of the three subjects with fecal mcr-1E. coli carriage and E. coli isolates with colistin MICs and STs are shown in Table 4. All three subjects were healthy without chronic underlying diseases, but one had traveled to China within the past year. Three isolates were susceptible to piperacillin/tazobactam, cefazolin, cefmetazole, cefotaxime, ceftazidime, cefepime, ertapenem, meropenem, imipenem, amikacin, gentamycin, ciprofloxacin, levofloxacin, and tigecycline. The colistin MIC in three isolates was 2, 2, and 4 mg/L, respectively (Table 4).
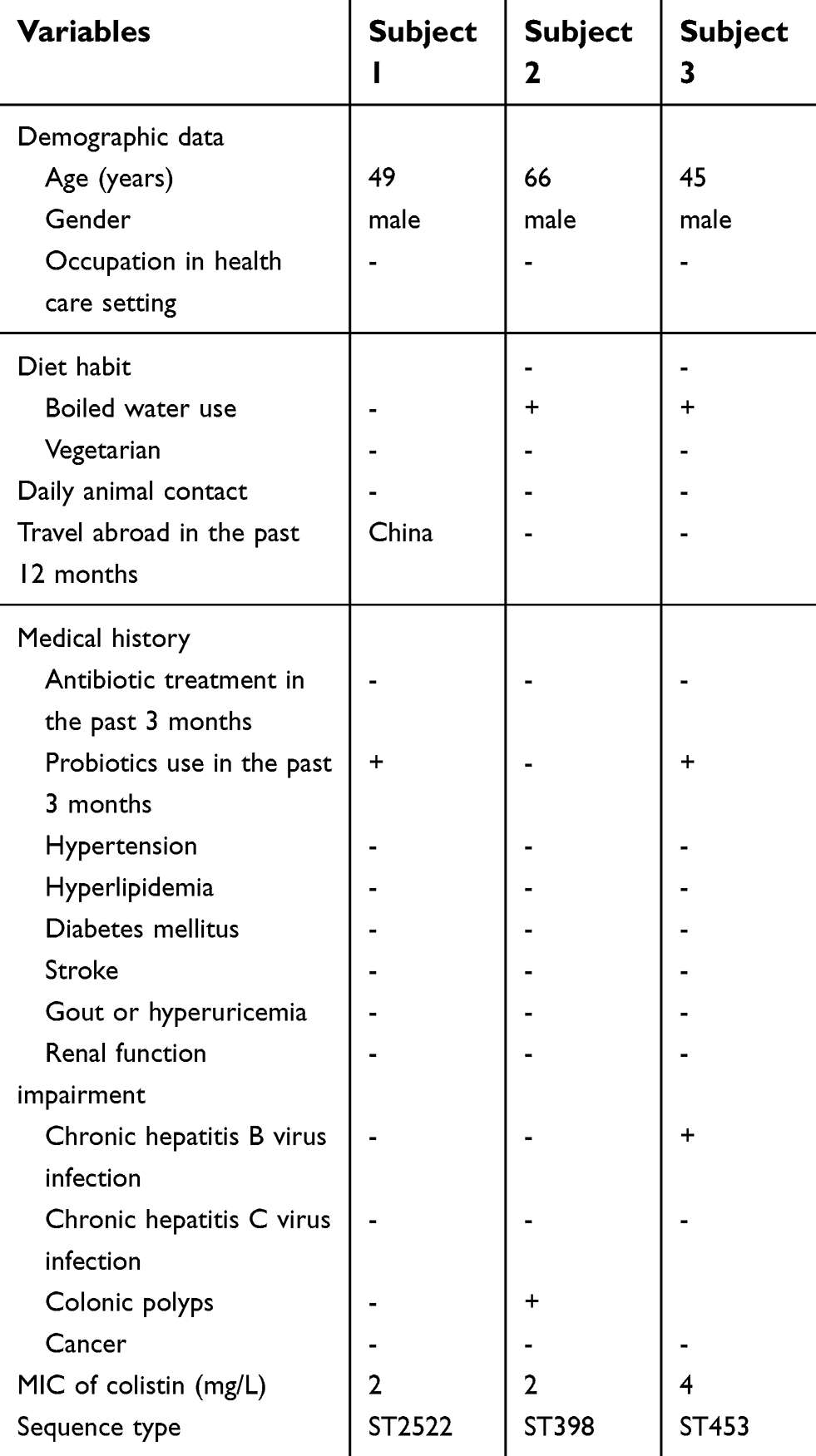 | Table 4 Characteristics of three subjects with mcr-1 harboring Escherichia coli carriage |
Discussion
The prevalence and risk factors for ESBL-EC carriage in asymptomatic individuals have been described previously in many regions of the world.2–6 In this study, the prevalence of ESBL-EC carriage in healthy people in Taiwan was about 2%, lower than those in other areas of Asia. We found that people with a medical history of diabetes mellitus, chronic renal diseases, or colonic polyps had an increased risk of fecal ESBL-EC carriage, in accordance with earlier studies indicating that individuals with diabetes and chronic renal diseases were more likely to have ESBL-producing Enterobacteriaceae colonization or infection.18,19 Although a recent study suggested that gut microbes may influence the development of colonic polyps,20 the relationship between colonic polyps and ESBL-EC carriage requires further confirmation. Spread of ESBL-EC in the community may be related to the transmission of ESBL-EC by food, environmental dissemination, and carriage in domestic and wild animals.21 However, in this study, fecal carriage of ESBL-EC was not associated with meat consumption, unboiled water use, occupation in the health care setting, or daily animal contact, and previous antibiotic use did not increase the risk of ESBL-EC carriage in asymptomatic people. These results were consistent with previous studies.4,6,22
In a systemic review and meta-analysis, travelling to Asia and Africa was linked to fecal colonization with ESBL-EC,1 which cannot be confirmed in our cohort. It is not surprising because most studies showing a positive relationship between travelling and ESBL-EC carriage were conducted in Europe and North America,23 and our participants were Taiwanese who had more opportunities to meet Asians or visit other environments, which decreased the impact of travel on ESBL-EC carriage.
The ST131 E. coli clone is an important cause of fluoroquinolone-resistant E. coli infections,24 which is consistent with our result that levofloxacin resistance was more common in ST131 E. coli. The emergence of ST131 in the community would pose a challenge to empirical therapy for many community-acquired infections. ST131 transmission among people was documented after household contact with ST131 carriers,25 highlighting the potential health impact of ST131 carriers. However, few studies focused on the risk factors for epidemic ST131 E. coli carriage in the asymptomatic population. In this study, individuals with underlying cancer or stroke had a higher risk of ST131 E. coli carriage. A previous study in Korea reported that ST131 was the most common sequence type of ESBL-EC bacteremia in cancer patients,26 suggesting an increased susceptibility to ST131 colonization in these patients. However, to the best of our knowledge, there is no evidence suggesting that people with prior stroke had an increased risk of ST131E. coli carriage; this warrants further confirmation. Moreover, we found that drinking boiled water tended to protect against ST131E. coli carriage (75% vs 59%; P=0.09). Human ST131 carriage has been relevant to the water source of ST131 isolates.27,28 However, direct evidence to verify that unboiled water is the source of ST131 E. coli have not yet been found.
In Taiwan, mcr-1-harboring Enterobacteriaceae isolates have been found in patients and food-producing animals.8,15,29,30 A recent study including ten cases of mcr-1-harboring Enterobacteriaceae bacteremia revealed that 50% of them were hospitalized within 3 months before bacteremia episodes and most subjects had chronic diseases.15 Notably, all ten patients denied recent travel abroad. Characteristically, our mcr-1-harboring E. coli isolates were discovered from three asymptomatic adults without chronic diseases or recent exposure to antibiotics. The relevance of recent travel to China in one participant with mcr-1 E. coli carriage remains undefined. Most mcr-1-harboring E. coli isolates were non-wild types, but some wild types were reported.31,32 The genetic relationship between our colonized isolates and the previously published isolates causing bloodstream infections or those obtained from pigs in Taiwan15 warrants further investigation.
In contrast to the prevalence data in China (4.9%)33 and Hong Kong (2.1%),34 fecal mcr-1 E. coli carriage in our adults visiting a health examination center was less common (0.4%), which was similar to results from The Netherlands (0.35%).32 The above data suggest geographic diversity of mcr-1 E. coli fecal carriage throughout the world and that mcr-1 E. coli is not widely spread in the community in Taiwan.
There are some limitations to this study. First, the participants only involved urban adults who received health examinations in one city, and the representativeness of the study cohort for the Taiwan population is limited. Second, the number of patients with ESBL-EC and ST131 E. coli carriage was too small to detect certain risk factors. Last, the association of colonic polyps and ESBL-EC may be biased because of recall bias for the diagnosis of colonic polyps. A prospective study enrolling individuals with colonic polyps that were diagnosed by colonoscopy and microbiological screening of fecal ESBL-EC carriage is warranted.
Conclusion
Asymptomatic adults in Taiwan had a low prevalence rate of fecal ESBL-EC or ST131 E. coli carriage, which was associated with the presence of underlying medical conditions. However, only a small number of ESBL-EC and ST131 E. coli isolates were noted in the study, and the associated risk factors require further investigation.
Ethics approval and informed consent
The study was approved by the Ethics Committee at the Kaohsiung Veterans General Hospital (VGHKS16-CT2-04). This study was conducted in accordance with the Declaration of Helsinki. The Ethics committee waived the need for written informed consent provided by participants due to the noninterventional and retrospective nature of the study. Because all patient data were analyzed in anonymity, no additional informed consent was required.
Acknowledgments
We are grateful to the members of Dr. Chih-Hsin Hung’s laboratory at the I-Shou University, especially Miss Wan-Yu Hung, for their excellent work in completing the E. coli isolation and PCR. This work was supported by research grants from the Taiwan Ministry of Science and Technology, MOST 104-2314-B-075B-003-MY3, 106-2314-B-006-081-MY2, 107-2314-B-075B-004, and VGHKS107-039, 108-128
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there are no competing interests regarding the publication of this paper.
References
1. Karanika S, Karantanos T, Arvanitis M, Grigoras C, Mylonakis E. Fecal colonization with extended-spectrum beta-lactamase-producing enterobacteriaceae and risk factors among healthy individuals: a systematic review and metaanalysis. Clin Infect Dis. 2016;63(3):310–318. doi:10.1093/cid/ciw283
2. Luvsansharav UO, Hirai I, Niki M, et al. Prevalence of fecal carriage of extended-spectrum beta-lactamase-producing Enterobacteriaceae among healthy adult people in Japan. J Infect Chemother. 2011;17(5):722–725. doi:10.1007/s10156-011-0225-2
3. Luvsansharav UO, Hirai I, Niki M, et al. Analysis of risk factors for a high prevalence of extended-spectrum {beta}-lactamase-producing Enterobacteriaceae in asymptomatic individuals in rural Thailand. J Med Microbiol. 2011;60(Pt 5):619–624. doi:10.1099/jmm.0.026955-0
4. Nicolas-Chanoine MH, Gruson C, Bialek-Davenet S, et al. 10-fold increase (2006–11) in the rate of healthy subjects with extended-spectrum beta-lactamase-producing Escherichia coli faecal carriage in a Parisian check-up centre. J Antimicrob Chemother. 2013;68(3):562–568. doi:10.1093/jac/dks429
5. Ni Q, Tian Y, Zhang L, et al. Prevalence and quinolone resistance of fecal carriage of extended-spectrum beta-lactamase-producing Escherichia coli in 6 communities and 2 physical examination center populations in Shanghai, China. Diagn Microbiol Infect Dis. 2016;86(4):428–433. doi:10.1016/j.diagmicrobio.2016.07.010
6. Ny S, Lofmark S, Borjesson S, et al. Community carriage of ESBL-producing Escherichia coli is associated with strains of low pathogenicity: a Swedish nationwide study. J Antimicrob Chemother. 2017;72(2):582–588. doi:10.1093/jac/dkw419
7. Liu -Y-Y, Wang Y, Walsh TR, et al. Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: a microbiological and molecular biological study. Lancet Infect Dis. 2016;16(2):161–168.
8. Lai CC, Chuang YC, Chen CC, Tang HJ. Coexistence of MCR-1 and NDM-9 in a clinical carbapenem-resistant Escherichia coli isolate. Int J Antimicrob Agents. 2017;49(4):517–518.
9. Krishnan E, Akhras KS, Sharma H, et al. Relative and attributable diabetes risk associated with hyperuricemia in US veterans with gout. Qjm. 2013;106(8):721–729.
10. Chia JH, Chu C, Su LH, et al. Development of a multiplex PCR and SHV melting-curve mutation detection system for detection of some SHV and CTX-M beta-lactamases of Escherichia coli, Klebsiella pneumoniae, and Enterobacter cloacae in Taiwan. J Clin Microbiol. 2005;43(9):4486–4491. doi:10.1128/JCM.43.9.4486-4491.2005
11. Sidjabat HE, Paterson DL, Adams-Haduch JM, et al. Molecular epidemiology of CTX-M-producing Escherichia coli isolates at a tertiary medical center in western Pennsylvania. Antimicrob Agents Chemother. 2009;53(11):4733–4739. doi:10.1128/AAC.00533-09
12. Dallenne C, Da Costa A, Decre D, Favier C, Arlet G. Development of a set of multiplex PCR assays for the detection of genes encoding important beta-lactamases in Enterobacteriaceae. J Antimicrob Chemother. 2010;65(3):490–495. doi:10.1093/jac/dkp498
13. Belmar Campos C, Fenner I, Wiese N, et al. Prevalence and genotypes of extended spectrum beta-lactamases in Enterobacteriaceae isolated from human stool and chicken meat in Hamburg, Germany. Int J Med Microbiol. 2014;304(5–6):678–684. doi:10.1016/j.ijmm.2014.04.012
14. Doumith M, Day M, Ciesielczuk H, et al. Rapid identification of major Escherichia coli sequence types causing urinary tract and bloodstream infections. J Clin Microbiol. 2015;53(1):160–166. doi:10.1128/JCM.02562-14
15. Lai CC, Lin YT, Lin YT, et al. Clinical characteristics of patients with bacteraemia due to the emergence of mcr-1-harbouring Enterobacteriaceae in humans and pigs in Taiwan. Int J Antimicrob Agents. 2018;52(5):651–657. doi:10.1016/j.ijantimicag.2018.08.015
16. Chung HC, Lai CH, Lin JN, et al. Bacteremia caused by extended-spectrum-beta-lactamase-producing Escherichia coli sequence type ST131 and non-ST131 clones: comparison of demographic data, clinical features, and mortality. Antimicrob Agents Chemother. 2012;56(2):618–622. doi:10.1128/AAC.05753-11
17. Jean B, Mpw P, Eliopoulos GM, Jenkins SG. M100 Performance Standards for Antimicrobial Susceptibility Testing.
18. D BP S, Grimmelprez A, de Saint-Hubert M, et al. Clinical profiles of patients colonized or infected with extended-spectrum beta-lactamase producing Enterobacteriaceae isolates: a 20 month retrospective study at a Belgian University Hospital. BMC Infect Dis. 2011 Jan 12;11:12. doi:10.1186/1471-2334-11-12
19. Johnson JR, Thuras P, Johnston BD, et al. The pandemic H30 subclone of Escherichia coli sequence type 131 is associated with persistent infections and adverse outcomes independent from its multidrug resistance and associations with compromised hosts. Clin Infect Dis. 2016;62(12):1529–1536. doi:10.1093/cid/ciw193
20. Peters BA, Dominianni C, Shapiro JA, et al. The gut microbiota in conventional and serrated precursors of colorectal cancer. Microbiome. 2016;4(1):69. doi:10.1186/s40168-016-0218-6
21. Oteo J, Pérez-Vázquez M, Extended-Spectrum CJ. β-lactamase producing Escherichia coli: changing epidemiology and clinical impact. Curr Opin Infect Dis. 2010;23(4):320–326.
22. PL AC W, Jacquier H, Clermont O, et al. Characterization of fecal extended-spectrum-β-lactamase-producing Escherichia coli in a remote community during a long time period. Antimicrob Agents Chemother. 2013;57(10):5060–5066. doi:10.1128/AAC.00848-13
23. Woerther PL, Andremont A, Kantele A. Travel-acquired ESBL-producing Enterobacteriaceae: impact of colonization at individual and community level. J Travel Med. 2017;24(suppl_1):S29–S34. doi:10.1093/jtm/taw101
24. Johnson JR, Johnston B, Clabots C, Kuskowski MA, Castanheira M. Escherichia coli sequence type ST131 as the major cause of serious multidrug-resistant E. coli infections in the United States. Clin Infect Dis. 2010;51(3):286–294. doi:10.1086/653932
25. Torres E, Lopez-Cerero L, Morales I, Navarro MD, Rodriguez-Bano J, Pascual A. Prevalence and transmission dynamics of Escherichia coli ST131 among contacts of infected community and hospitalized patients. Clin Microbiol Infect. 2018;24(6):618–623. doi:10.1016/j.cmi.2017.09.007
26. Ha YE, Kang CI, Cha MK, et al. Epidemiology and clinical outcomes of bloodstream infections caused by extended-spectrum beta-lactamase-producing Escherichia coli in patients with cancer. Int J Antimicrob Agents. 2013;42(5):403–409. doi:10.1016/j.ijantimicag.2013.07.018
27. Johnson JR, Nicolas-Chanoine MH, DebRoy C, et al. Comparison of Escherichia coli ST131 pulsotypes, by epidemiologic traits, 1967–2009. Emerg Infect Dis. 2012;18(4):598–607. doi:10.3201/eid1804.111627
28. M MA C-L, López C, Mamani R, et al. Detection of quinolone-resistant Escherichia coli isolates belonging to clonal groups O25b: H4-B2-ST131and O25b: H4-D-ST69in raw sewage and river water in Barcelona, Spain. J Antimicrob Chemother. 2013;68(4):758–765. doi:10.1093/jac/dks477
29. SC HW K, Wang HY, Shiau YR, Cheng MF, Lauderdale TL. Colistin resistance gene mcr-1 in Escherichia coli isolates from humans and retail meats, Taiwan. J Antimicrob Chemother. 2016;71(8):2327–2329. doi:10.1093/jac/dkw122
30. CS CY C, Wang YW, Liu YY, et al. Dissemination of mcr-1-carrying plasmids among colistin-resistant salmonella strains from humans and food-producing animals in Taiwan. Antimicrob Agents Chemother. 2017;61:7.
31. Pham Thanh D, Thanh Tuyen H, Nguyen Thi Nguyen T, et al. Inducible colistin resistance via a disrupted plasmid-bornemcr-1gene in a 2008 VietnameseShigella sonneiisolate. J Antimicrob Chemother. 2016;71(8):2314–2317. doi:10.1093/jac/dkw173
32. Terveer EM, Nijhuis RHT, Crobach MJT, et al. Prevalence of colistin resistance gene (mcr-1) containing Enterobacteriaceae in feces of patients attending a tertiary care hospital and detection of a mcr-1 containing, colistin susceptible E. coli. PLoS One. 2017;12(6):e0178598. doi:10.1371/journal.pone.0178598
33. Bi Z, Berglund B, Sun Q, et al. Prevalence of the mcr-1 colistin resistance gene in extended-spectrum beta-lactamase-producing Escherichia coli from human faecal samples collected in 2012 in rural villages in Shandong Province, China. Int J Antimicrob Agents. 2017;49(4):493–497. doi:10.1016/j.ijantimicag.2016.12.018
34. Chan WS, Au CH, Ho DN, Chan TL, Ma ES, Tang BS. Prospective study on human fecal carriage of Enterobacteriaceae possessing mcr-1 and mcr-2 genes in a regional hospital in Hong Kong. BMC Infect Dis. 2018;18(1):81. doi:10.1186/s12879-018-3109-6
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.