")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Prevalence and Predictors of Self-Medication with Antifungal Drugs and Herbal Products Among University Students: A Cross-Sectional Study from Egypt
Authors Khairy WA , Nasser HA, Sarhan MD, El Shamy A , Galal YS
Received 2 March 2021
Accepted for publication 9 May 2021
Published 27 May 2021 Volume 2021:14 Pages 2191—2200
DOI https://doi.org/10.2147/RMHP.S308400
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Walaa Ahmed Khairy,1 Hebatallah A Nasser,2 Mai D Sarhan,3 Aliaa Ali El Shamy,2 Yasmine Samir Galal1
1Public Health and Community Medicine Department, Faculty of Medicine, Cairo University, Cairo, Egypt; 2Microbiology Department, Faculty of Pharmacy, Heliopolis University, Cairo, Egypt; 3Family Medicine Department, Faculty of Medicine, Cairo University, Cairo, Egypt
Correspondence: Walaa Ahmed Khairy
Public Health and Community Medicine Department, Faculty of Medicine, Cairo University, Kasr Alainy Street, Cairo, 11562, Egypt
Tel +20-1223682081
Email [email protected]
Background and Purpose: Irrational use of drugs for self-medication (SM) is a worldwide public health problem which results in treatment failure, economic loss, and increased burden of morbidity and mortality. Thus, the purpose of this study was to explore SM with antifungal drugs and herbal products among university students in Egypt.
Methods: A cross-sectional sectional study was conducted over 7 months among 403 university students in Egypt. The students were invited to complete a self-administered questionnaire through an online Google form. Questionnaire items included socio-demographic characteristics of the students, practice of and attitude towards SM with antifungal drugs, and SM with herbal products.
Results: Prevalence of SM with antifungal drugs among students stood at 38.2%. The main reasons for SM with antifungal drugs were perceiving their health problem as being minimal, followed by having fears of a doctor’s visit. About 73% of the students thought that SM was not a safe practice. Older age (AOR = 1.5, 95% CI= 1.3– 1.8), affiliation to a private university (AOR = 3.7, 95% CI= 2.2– 6.4), and being a medical student (AOR =2.4, 95% CI= 1.3– 4.5) were the significant predictors of SM with antifungal drugs. A high prevalence of SM with herbal products (70.7%) was reported, with most students having used some form of herbal weight loss preparation (64%). Being a Cairo resident (AOR= 2.4, 95% CI =1.5– 3.8, P< 0.05) and being a medical student (AOR= 2.1, 95% CI =1.3– 3.4, P< 0.05) were the significant predictors of SM with herbal products.
Conclusion: In the current study, SM was common among Egyptian university students. Providing counseling and public health education to university students with regards to SM is crucial. Implementing strict regulations and the full enforcement of excitant laws pertaining to the use of medication supplies is also needed. Herbal products should face the scrutiny of evidence-based medicine. Further studies are needed to evaluate the impact of SM among university students.
Keywords: self-medication, antifungal, herbal, university, Egypt
Introduction
Self-medication (SM) refers to the consumption of drugs without medical prescription or consultation for the treatment of self-identified medical conditions or symptoms. It includes the use of leftover medicines already present at home, and the purchase of drugs through resubmitting previously dispensed prescriptions. The most frequently self-medicated are analgesics, antibiotics, multivitamins, as well as cough and common cold medicines.1
Over-the-counter (OTC) drugs are the most commonly self-medicated drugs, due to their accessibility without the need for a physician’s prescription. However, due to unregulated access in developing countries, SM practices may also involve prescription-only medications (POMs).2 SM with either POMs or OTC drugs is a global health problem with serious public health consequences, including drug interactions, drug resistance, organ failure, and even death.3 The prevalence of SM has been rising recently all over the world with marked variability across developed and developing countries, with rates ranging from 12.1% to 92.8%, respectively.4,5 Several studies have shown that SM represents a common problem among university students with prevalence rates ranging from 64.8% to 77.2% in the Middle East,6,7 71.7% to 95.3% in Asia8,9 and 24% to 91.4% in Africa.10,11 In a study conducted in Egypt, the prevalence of SM among university students stood at 62.9%.12
Factors contributing to SM practices among university students include their higher exposure to social media and pharmaceutical advertisements,13 perceptions of encountered health problems as being trivial, lack of time to seek medical care, a sense of having adequate information to self-medicated, and cost-effectiveness considerations.14–16 Moreover, these practices vary according to each student’s socio-demographic characteristics including age, gender, socio-economic status, educational level, residence, and field of study.17
In the past three decades, invasive life threatening opportunistic fungal infections have markedly increased from 18% to over 60% due to antibiotic abuse, widespread use of anticancer therapy, and the high prevalence of immunosuppressive infections, which in turn led to a higher consumption of antifungal agents.18 Moreover, switch from POMs to OTC drugs has facilitated the misuse of antifungal drugs and emergence of antifungal resistant strains, resulting in a higher probability of inappropriate treatment, inaccurate diagnosis, drug interactions and increased morbidity.19
Herbal medicine consumption is widely practiced all over the world as a form of alternative therapy for the treatment of a large number of health problems, including heart disease, diabetes, high blood pressure and even certain types of cancer. The US Food and Drug Administration requires that pharmaceutical drugs be guaranteed as safe before being released to the market. This, however, this is not the case with herbal products, which do not fall under the category of medicines if they are not explicitly labeled as treatment for a certain disease. Herbal medicines are considered as food supplements and are easily accessed in the market without prescription.20 According to the World Health organization (WHO), 70–80% of the world population depends on non-conventional medicine, mainly herbs, for their primary health care (PHC) needs. In developing countries, herbs are mainly reserved as alternative treatments to the more expensive POMs.21 However, various studies have illustrated that herbal medicines, taken irrationally or in combination with other medicines, may lead to delayed or missed diagnosis, unfavorable side effects and toxicities.22,23
Unlike most previous studies which either conducted a general investigation of SM or focused on the abuse of antibiotics or analgesics,12,24,25 the current study is novel study which addressed SM with antifungal drugs and herbal products among university students in Egypt. This represents a serious problem that needs tailored interventions. Moreover, this study should be regarded as a starting point for researchers to further probe the area of SM with antifungal drugs and herbal products; a topic of limited published work worldwide.19,26
Methods
Study Design, Setting, and Participants
This cross-sectional study was conducted over 7 months to explore the SM practice of antifungal drugs and herbal products among Egyptian undergraduate university students. It was conducted in two randomly selected universities in Cairo (one private: Heliopolis University; and one public: Cairo University). The study targeted both medical and non-medical students during the first semester of the academic year 2019/2020.
Sample Size
The sample size was calculated using Epi Info program, version 7. Based on the findings of the study conducted by Helal and Abou-Elwafa,12 where the prevalence of SM practice among undergraduate university students in Mansoura city in Egypt was estimated to have stood 62.9%, and after employing a 95% confidence interval precision of ±5%, the minimal required sample size was estimated to be 358 participants. An additional 20% were added in order to compensate for potential non-responses and incomplete questionnaires. The final sample size was adjusted to 430 participants. The sample size was proportionally allocated to each university according to their corresponding average number of enrolled students, whereby the designated share of Cairo University stood at two thirds of the total sample. Inclusion criteria for the current study were: (i) an age of 18 years or above; (ii) university student status; (iii) mental stability; and (iv) willingness to participate in the study. On the other hand, there were no exclusion criteria. Students were recruited through an online Google form after approval of the ethical committees of the two target universities namely: Research Ethics Committee of Cairo University (approval number: F-11-2018) and the Institutional Review Board of Heliopolis University (approval number: 201809010.3).
Data Collection Tool
The data were collected using an online self-administrated, anonymous and structured Arabic language questionnaire. The questionnaire was adapted from the available literature.5,12,27 Accordingly, it included three sections. The first section included items covering background characteristics of the students, namely; age, gender, residence (within or outside Cairo), type of university (public or private), and type of education (medical/non-medical). The second section explored the practice of SM with antifungal drugs during the year preceding the study covering self-prescribing of antifungal drugs either for themselves or for family and friends; reading the pamphlet instructions and seeking information about antifungal drugs before use; interest in following social media drug advertisements; frequency and reasons of SM practices with antifungal drugs; and the most frequently utilized antifungal drugs for SM. The third section assessed attitudes of participants towards SM with antifungal drugs and their readiness to discontinue SM if they knew they had dangerous side effects; whether or not they considered SM a safe practice; and if they encouraged family or friends to self-medicate. Finally the last section addressed the utilization of herbal products for the treatment of self-reported medical conditions or symptoms in the year prior to the survey. Items covered self-prescribing of herbal products; the most frequently self-medicated herbal products; and the main sources of knowledge of herbal products. All items in the questionnaire were designed as close-ended questions, with the multiple options format being employed for the design of questions addressing the reasons for SM with antifungal agents and the sources of knowledge of herbal products.
Pilot Testing
The preliminary questionnaire was tested on 40 students to assess comprehension, clarity and time required to complete the questionnaire. Accordingly, some questions were modified to be more concise, while others were omitted in order to avoid repetition, leading to the final questionnaire form.
Procedures
The participants were approached during their scheduled elective course classes (at the end of each class) by study coordinators. They were invited to fill in the study questionnaire via the online Google forms link, after receiving a complete orientation of the objectives and expected outcomes of the study, with emphasis on their right not to participate, and assuring them of the confidentiality of data. The first section in the online form included all relevant information about the study including the purpose and objectives of the work in addition to the contact number and e-mail address of the principal investigator, in case of any inquiries. The first section ended with the following statement: “By completing this questionnaire, you agree to participate with us in this study.” Continuing to respond to items beyond this statement was considered as an indication of informed consent to participate in the study (as it was unfeasible to sign the questionnaire online). Study procedures were carried out according to the ethical requirements of the Declaration of Helsinki.
Statistical Analysis
Pre-coded data were statistically analyzed using the Statistical Package for Social Sciences (SPSS) software, version 21. Qualitative variables were displayed as numbers and percentages. Quantitative variables were presented as means ± standard deviations (SD). Univariate logistic regression analysis was carried out using Pearson’s chi-square test to calculate the crude association between the SM practice with antifungal drugs and herbal products with the study’s independent variables. Finally, two multivariate logistic regression models were built in order to decide on the significant predictors for SM with antifungal drugs and herbal products among the independent variables by using the binary logistic regression test. Results were presented as adjusted odds ratios (AOR) and 95% confidence intervals (CI). P values of ≤ 0.05 were considered statistically significant.
Results
Background Characteristics of the Studied Group
A total of 403 out of 430 questionnaires were completed and returned with a response rate of 93.7%. The mean age of respondents was 21.1 ±1.7 years, with a range of 18–25 years. About two thirds of respondents (65.5%) were residents of Cairo, and more than half were males (55.3%). More than three quarters of respondents (77.2%) were medical students at the faculties of Medicine, Dentistry and Pharmacy. About 60% of respondents were public university students (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Participants, University Students in Egypt |
Practice of SM with Antifungal Drugs
The practice of SM with antifungal drugs and herbal products among the respondents is summarized in Supplementary Table 1. One hundred fifty-four students (38.2%) reported SM with antifungal drugs during the past year. The most commonly self-medicated antifungal drug, as reported by 70.1% of respondents who were self-medicating, was Diflucan (fluconazole). The most frequently reported reasons for SM with antifungal drugs (Figure 1) were perceiving the health problem as being minimal, followed by fears of the doctor’s visit (54.5% and 37%, respectively), while the least frequently reported reasons were a desire to save time and cost-effectiveness considerations (3.2% each). The vast majority of the self-medicating students (95.5%) stated that it was easy to dispense antifungal drugs without a prescription. When the respondents were asked about the frequency of SM practice with antifungal drugs during the past year, most of the respondents (88.9%) reported occasional use on need, while only 7.8% and 3.2% reported regular monthly and weekly use, respectively. On the other hand, approximately half of the medical students (50.5%) admitted to prescribing antifungal drugs to their families and friends.
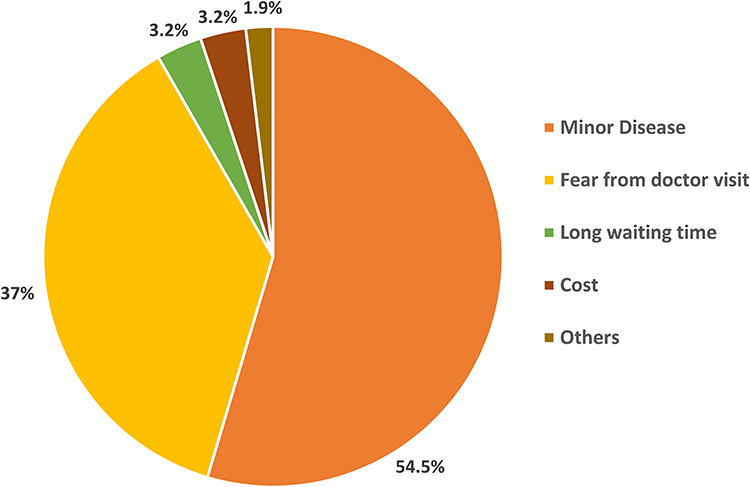 |
Figure 1 Percent distribution of reported reasons of self-medication with antifungal drugs. |
Attitudes Towards SM with Antifungal Drugs
Attitudes of self-medicating students towards SM with antifungal drugs are presented in Table 2. About 73% of the students thought that SM was not a safe practice and 82.5% mentioned they would discontinue SM if they knew it had dangerous side effects. Nearly 68% of the students claimed that they did not encourage their family or friends to self-medicate and the majority (96.8%) expressed their willingness to seek additional information about SM with antifungal drugs and its possible side effects.
 |
Table 2 Attitudes Towards Self-Medication with Antifungal Drugs Among Self-Medicated University Students |
Predictors of SM with Antifungal Drugs
Sex, age, residence, type of university and education, reading medication pamphlets and seeking information regarding antifungal drugs prior to use, as well as an interest in following social media drug advertisements were the variables tested for potential association with SM with antifungal drugs (Table 3). Results of chi-square statistical analysis revealed that sex, residence, type of university and interest in following antifungal drug advertisements were significantly associated with the practice of SM with antifungal drugs (P<0.05). Male respondents self-medicated more frequently than female respondents (COR =1.7, 95% CI= 1.2–2.6). Private university students more commonly self-medicated compared with those attending a public university (COR = 6.1, 95% CI= 3.9–9.6). In addition, respondents interested in following social media drug advertisements self-prescribed more frequently than their peers (COR = 0.5, 95% CI= 0.3–0.8). No significant association was detected between SM practice with antifungal drugs and reading medication pamphlets before use (P<0.05).
 |
Table 3 Univariate and Multivariate Logistic Regression Analysis of Self-Medication Practice with Antifungal Drugs Among the Respondents |
Multivariate logistic regression analysis was performed to single out significant predictors associated with SM with antifungal drugs as shown in Table 3. Older age was independently associated with the likelihood of SM with antifungal drugs (AOR = 1.5, 95% CI= 1.3–1.8). Students affiliated to a private university were nearly four times more likely to practice SM with antifungal drugs than their counterparts in a public university (AOR = 3.7, 95% CI= 2.2–6.4). Medical students were almost two and half times more likely to self-medicate with antifungal drugs compared with non- medical students (AOR =2.4, 95% CI= 1.3–4.5).
Utilization of Herbal Products for Treatment of Self-Reported Medical Conditions or Symptoms
Two hundred eighty-five students (70.7%) reported having used herbal products for the treatment of self-reported medical conditions or symptoms during the past year. The most commonly reported self-medicated herbal products were weight-loss products (64%) and cough and cold medicines (30%). Figure 2 displays the main sources of knowledge regarding utilized herbal products, where advice from family or friends, internet websites, and pharmacists were the most prevalent sources (40.4%, 22.1% and 20%, respectively). Results of multivariate logistic regression analysis revealed that living in Cairo and being a medical student were the two significant predictors of SM with herbal products (AOR=2.4, 95% CI= 1.5–3.8 and AOR = 2.1,95% CI= 1.3–3.4, respectively) (Table 4).
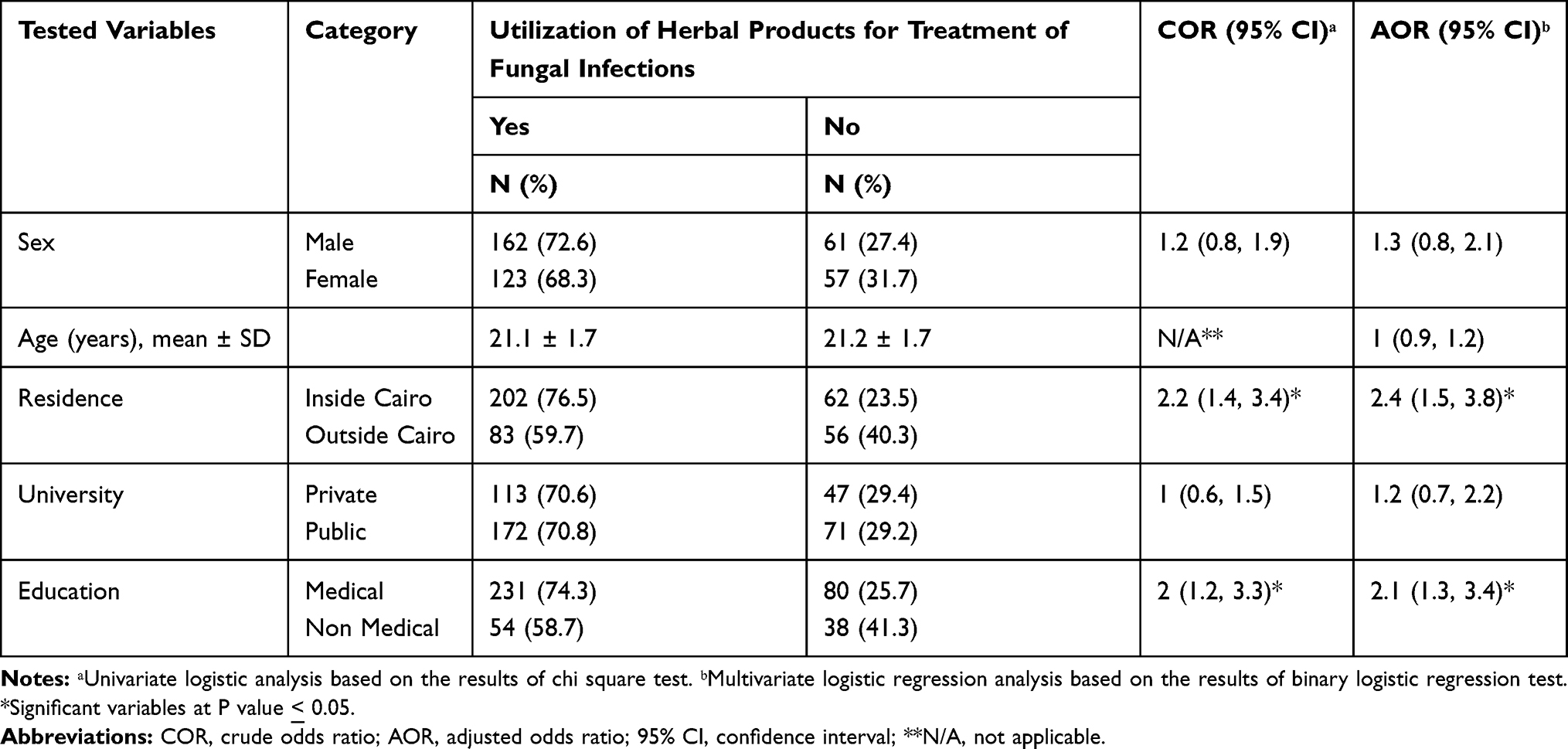 |
Table 4 Univariate and Multivariate Logistic Regression Analysis of Self-Medication with Herbal Products |
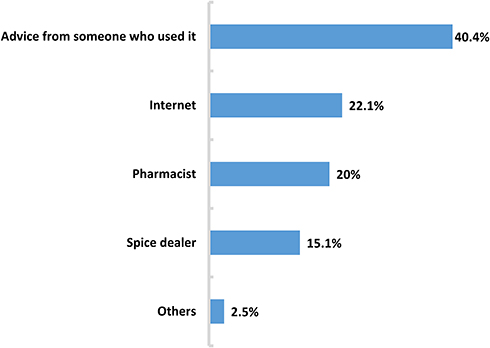 |
Figure 2 Percent distribution of main sources of knowledge regarding herbal products. |
Discussion
Irrational use of drugs for SM is a worldwide public health problem which results in treatment failure, economic loss, and increased burden of morbidity and mortality.28 The understanding of consumer characteristics associated with SM is crucial for proper planning of public health awareness efforts and the implementation of effective management strategies. Additionally, searching the literature revealed that the prevalence of fungal infections in Egypt is alarming. One study conducted by Abdel Fattah et al, for example, showed that the prevalence of fungal infections stood at 18.6%. Dermatophyte infections were more common than non-dermatophyte infections (51.2% vs 37.2%) among infected cases. The Egypt-wide prevalence of onychomycosis reportedly stood at 6.4%, whilst it stood at 1.2% among study participants. The most common type of superficial fungal infections was Candida (5.2%), followed by Tinea pedis (3.6%), T.cruris (2.1%), and T. capitis (1.7%).29 Hence, this study was conducted in order to assess the practice SM with antifungal drugs and herbal products among Egyptian university students. In the current study, about 38% of undergraduate students reported self-prescribing antifungal drugs, and nearly half of medical students indicated having prescribed these for families and friends. The majority of students (95.5%) claimed that it was easy to dispense antifungal drugs without prescription. Higher SM practices were observed in a study conducted by Mushi et al, where more than half of the patients surveyed (55.5%) reported self-medicating with OTC antifungal drugs.19 Prevalence of SM was also high among Egyptian university students in studies conducted by Helal and Abou-Elwafa and Kamal Elden et al; 62.9% and 77.7%, respectively.12,24 Variability in prevalence rates of SM could be explained by the different study populations and methodologies used. Moreover, some studies inquired about SM practices in general,12 while others assessed SM with specific drugs such as antibiotics24 or antifungal agents.19
SM with OTC antimicrobial agents has been linked with increased antimicrobial resistance. The effectiveness of azole agents, the most commonly prescribed antifungal drugs worldwide, has been reduced by the emergence of azole resistant strains. This represents a great challenge to the proper management of fungal infections.19 In the present study, the most commonly used self-medicated antifungal drug was fluconazole, as reported by 70.1% of the respondents. Similarly, in a study conducted in Tanzania, the commonest class of dispensed antifungal drugs was azoles, whereas fluconazole was the commonest OTC antifungal drug used.19
In the present study, the most common reasons for SM with antifungal drugs were believing in the mildness of illness and fears regarding the doctor’s visit. This finding goes in line with other studies conducted in Ethiopia,10 United Arab Emirates7 and Saudi Arabia.14 However, in contrast to other studies which reported that previous experience,30 lack of time,15 and cost-effectiveness16 were the most common reasons for SM; these were the least commonly reported reasons in ours. The variability between studies could be attributed to cultural variations, socio-economic factors and different healthcare systems.
Most of the students in the current study (68.2%) claimed that they did not encourage their family or friends to self-medicate and the majority (96.8%) expressed their willingness to seek more information regarding SM with antifungal drugs and its possible side effects. This goes in line with another study conducted in Egypt where 87.4% of the students mentioned that they discouraged family and friends from self-medicating.12 Moreover, 72.7% of students in the present study believed that SM with antifungal drugs was not a safe practice. Similarly, in a study conducted in Saudi Arabia, 69.7% of students thought that SM was not safe.31 Despite recognizing that SM was not a safe practice, frequent use was reported by student who explained that using these drugs relieved symptoms that they were suffering from and were easily accessible.
A number of findings from the current study with regards to the practice of SM are worth noting. Male students were found to have self-medicated more frequently than females (COR=1.7, 95% CI=1.2–2.6, P<0.05). A possible explanation is that males may have faced more fungal infections than their female counterparts which resulted in higher SM practices. In contrast, studies in Saudi Arabia,6 Ethiopia,28 and Ghana32 found relatively higher rates of SM among females and justified these findings by stating that females have relatively lower immunities than males and also probably have a greater need for pain-killers due to the monthly attacks of dysmenorrhea. Also, we found that students that were interested in following social media drug advertisements had practiced SM more significantly than their peers (COR=0.5, 95% CI=0.3–0.8, P<0.05), which could be explained by the high influence of advertisements on the attitudes and behavior of this age group.
In this study, older age, affiliation to a private university, and being a medical student were three significant predictors of SM with antifungal drugs. The finding that older age students had practiced SM more frequently could be explained by their deeper knowledge of drugs and diseases which possibly led to a higher uptake and purchase of medications without prescriptions; a practice which is particularly easy in a developing country such as Egypt, where the access to drugs is not controlled. Similarly, previous studies done in Malaysia,33 Ethiopia,34 and Uganda35 reported higher SM practices among students in their senior years compared with their freshmen and sophomore counterparts. A possible explanation for higher SM practices among students attending private universities found in the present study is that they most likely enjoy higher incomes compared with public university students, who usually attain free healthcare services provided by the health insurance system. Studies conducted in Pakistan and Southern China found that income and SM have direct relationship.15,36 Medical students in our study were almost two and half times more likely to self-medicate compared with their non-medical counterparts (AOR=2.4, 95% CI=1.3–4.5, P<0.05). This could be attributed to the medical knowledge gained through their studies which might have provided them with a perceived confidence to make their own decisions regarding SM.37 Similar findings were observed in a study conducted in Saudi Arabia, where medical students practiced SM more frequently than non-medical students. Authors of that study justified their findings by noting the medical students’ medical knowledge and the easy access to hospital facilities.31
SM with herbal products is increasing steadily in both developed and developing countries despite the lack of studies regarding their effectiveness, and despite the lack of control over the quality and safety of these preparations.20 The general community perception that herbal products are safe may result in inappropriate use and improper intake, leading to undesirable side effects and toxicities.38 In the current study, a high prevalence of SM with herbal products (70.7%) was reported among university students. Unfortunately, most people are attracted to the use of herbal weight loss products because of the faulty perception that these are safe.39 These products may however contain FDA-banned ingredients which have many side effects that could induce heart failure, cancer, and other life-threatening conditions.40 In addition, they contain stimulants such as caffeine that may cause insomnia, depression, addiction, suicidal thoughts, and heart attacks, which could be fatal.41 The consumption of herbal products to induce weight-loss is a common practice globally, ranging from 10% to 98%.42 In the current study, most of the students who had practiced SM with herbal products had used herbal weight loss preparations (64%). This prevalence was higher than that reported in a study conducted in Central Mexico,42 where the prevalence of SM with herbal preparations for weight loss stood at only about 43%. The recommendation of a family member or friend markedly affects the decision to use herbal products for weight loss.43 The most common sources of knowledge for SM practice with herbal products as reported by students in the present study were advice from family or friends (40.4%), internet websites (22.1%), and pharmacists (20%). The study conducted in Mexico by Alonso-Castro et al found that 67% of patients consumed herbal weight-loss products based on the recommendations of relatives and friends.42 In one study conducted in Jordan,44 the primary sources of knowledge regarding SM were pharmacists (52.6%), the internet (44.2%), and family members (36.9%). Significant predictors of SM with herbal products revealed by the current study were being a Cairo resident (AOR= 2.4, 95% CI =1.5–3.8, P<0.05) and being a medical student (AOR= 2.1, 95% CI =1.3–3.4, P<0.05). The significant association between residing in Cairo and SM of herbal products could be explained by the accessibility of these products in the city which is also the capital of Egypt. Age and gender were not significantly associated with SM with herbal products. In contrast, female gender was a common factor associated with this practice in many studies, possibly owing to the great influence of media and society on body appearance, especially for women.42,45
This study is the first to assess SM practice with antifungal drugs and herbal products among university students in Egypt; however, it has some limitations. The questionnaire was self-reported which may have led to the inconsistent understanding of questions between students on the one hand, and underreporting of SM practice on the other. Enquiring about SM practices in the past year may have resulted in recall bias.
Conclusion
The current study highlights the importance of providing counseling and public health education to university students with regards to the possible side effects of SM. Implementing strict regulations, and enforcing existent laws pertaining to pharmaceutical advertisements and medication supplies is crucial. Providing quality medical services to university students with appropriate diagnoses, prescriptions and treatments is also needed. Licensing of herbal products should only come after these products had passed the scrutiny of evidence-based medicine, including clinical trials, which are essential in order to provide convincing evidence of the safety and effectiveness of these products. Further studies are needed to evaluate the impact of this high SM rate among university students as well as more in-depth probing of the different aspects of SM with antifungal drugs and herbal products.
Acknowledgments
The authors are thankful to all students who agreed to participate in this study. Also, special thanks to our study coordinators Badr Eldin Adel Tawfiq and Alaa Gamal Maghwry (Cairo University) and Alzahraa Nasser, Mai Essam, Muteaa Zyad, Qamar Mohamed, Layla Abd Almonem, and Nour Mowafak (Heliopolis University).
Disclosure
The authors report no conflicts of interest in this work. This research did not receive grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
1. Biswas S, Ghosh A, Mondal K, Dalui S, Haldar M, Biswas S. Self-medication with antibiotics among undergraduate nursing students of a government medical college in Eastern India. Int J Pharmacol Res. 2015;5(10):239.
2. Ehigiator O, Azodo CC, Ehizele AO, Ezeja EB, Ehigiator L, Madukwe IU. Self-medication practices among dental, midwifery and nursing students. Eur J Gen Dent. 2013;2(1):54. doi:10.4103/2278-9626.106813
3. Osemene K, Lamikanra A. A study of the prevalence of self-medication practice among university students in Southwestern Nigeria. Trop J Pharm Res. 2012;11(4):683–689. doi:10.4314/tjpr.v11i4.21
4. Figueiras A, Caamano F, Gestal-Otero JJ. Socio-demographic factors related to self-medication in Spain. Eur J Epidemiol. 2000;16(1):19–26. doi:10.1023/a:1007608702063
5. Tuyishimire J, Okoya F, Adebayo AY, Humura F, Lucero-Prisno DE
6. Aljaouni ME, Hafiz AA, Alalawi HH, Alahmadi GM, AlKhawaja I. Self-medication practice among medical and non-medical students at Taibah University, Madinah, Saudi Arabia. Int J Acad Sci Res. 2015;3(4):54–65.
7. Shehnaz SI, Sreedharan J, Khan N, Issa KJ, Arifulla M. Factors associated with self-medication among expatriate high school students: a cross-sectional survey in United Arab Emirates. Epidemiol Biostat Public Health. 2013;10(4).
8. Kasulkar AA, Gupta M. Self-medication practices among medical students of a private institute. Indian J Pharm Sci. 2014;77(2):178–182. doi:10.4103/0250-474X.156569
9. Shoaib MH, Yousuf RI, Anjum F, et al. Survey based study on the use of non-prescription drugs among pharmacists and non-pharmacists. Afri J Pharm Pharm. 2013;7(38):2652–2656. doi:10.5897/AJPP2013.3821
10. Bekele SA, Argaw MD, Yalew AW. Magnitude and factors associated with self-medication practices among university students: the case of Arsi University, College of Health Science, Asella, Ethiopia: cross-sectional survey based study. Open Access Lib J. 2016;3(06):1.
11. Abay S, Amelo W. Assessment of self-medication practices among medical, pharmacy, health science students in Gondar University, Ethiopia. J Young Pharm. 2010;2(3):306–310. doi:10.4103/0975-1483.66798
12. Helal R, Abou-ElWafa H. Self-medication in university students from the city of Mansoura, Egypt. J Environ Public Health. 2017;2017:1–7. doi:10.1155/2017/9145193
13. Burak LJ, Damico A. College students’ use of widely advertised medications. J Am Coll Health. 2000;49(3):118–121. doi:10.1080/07448480009596293
14. Albusalih FA, Ahmad R, Ahmad N, Ahmad N. Prevalence of self-medication among students of pharmacy and medicine colleges of a public sector university in Dammam City, Saudi Arabia. J Pharm. 2017;5(4):51. doi:10.3390/pharmacy5030051
15. Limaye D, Farah-Saeed AM, Ahmad M, Pitani RS, Fortwengel G. Self-medication practices among university students from Karachi, Pakistan. Int J Community Med Public Health. 2017;4(9):3076–3081. doi:10.18203/2394-6040.ijcmph20173635
16. AlRaddadi KK, Barakeh RM, AlRefaie SM, AlYahya LS, Adosary MA, Alyahya KI. Determinants of self-medication among undergraduate students at King Saud University: knowledge, attitude and practice. J Health Spec. 2017;5(2):95–101. doi:10.4103/2468-6360.205078
17. Fatima S, Akash S, Azhar S, Muhammad D, Bashir S. Medical students perception and practice of self-medication: vision of future practitioner in Pakistan. Br J Pharm Res. 2017;17(1):1–8. doi:10.9734/BJPR/2017/32524
18. Kwamin F, Nartey NO, Codjoe FS, Newman MJ. Distribution of Candida species among HIV-positive patients with oropharyngeal candidiasis in Accra, Ghana. J Infect Dev Ctries. 2013;7(1):41–45. doi:10.3855/jidc.2442
19. Mushi MF, Masewa B, Jande M, Mirambo MM, Mshana SE. Prevalence and factors associated with over –the-counter use of antifungal agents in Mwanza City, Tanzania. Tanzan J Health Res. 2017;19(1). doi:10.4314/thrb.v19i1.8
20. Kaur J, Kaur S, Mahajan A. Herbal Medicines: possible risks and benefits. Am J Phytomed Clin Ther. 2013;2:226–239.
21. World Health Organization. WHO Global Report on Traditional and Complementary Medicine 2019. Available from: https://www.who.int/traditional-complementary-integrative-medicine/WhoGlobalReportOnTraditionalAndComplementaryMedicine2019.pdf.
22. Stickel F, Patsenker E, Schuppan D. Herbal hepatotoxicity. J Hepatol. 2005;43(5):901–910. doi:10.1016/j.jhep.2005.08.002
23. Yang HN, Kim DJ, Kim YM, et al. Aloe- induced toxic hepatitis. J Korean Med Sci. 2010;25(3):492–495. doi:10.3346/jkms.2010.25.3.492
24. Kamal Elden NM, Nasser HA, Alli A, et al. Risk factors of antibiotics self-medication practices among university students in Cairo, Egypt. Open Access Maced J Med Sci. 2020;8(E):7–12. doi:10.3889/oamjms.2020.3323
25. Mekuria AB, Birru EM, Tesfa MT, Geta M, Kifle ZD, Amare T. Prevalence and predictors of self-medication practice among teachers’ education training college students in Amhara region, Ethiopia: a cross-sectional study. Front Pharmacol. 2020;11. doi:10.3389/fphar.2020.593764
26. Schneider CR, Emery L, Brostek R, Clifford RM. Evaluation of the supply of antifungal medication for the treatment of vaginal thrush in the community pharmacy setting: a randomized controlled trial. J Pharm Pract. 2013;11:132–137.
27. El Ezz N, Ez-Elarab H. Knowledge, attitude and practice of medical students towards self-medication at Ain Shams University, Egypt. J Prev Med Hyg. 2011;52(4):196–200.
28. Zeru N, Fetene D, Geberu DM, Melesse AW, Atnafu A. Self-medication practice and associated factors among university of Gondar College of Medicine and Health sciences students: a cross-sectional study. Patient Prefer Adherence. 2020;14:1779–1790. doi:10.2147/PPA.S274634
29. Abdel Fattah NS, Mostafa NS, Afify AA, Husain AE. Epidemiology and risk factors of superficial fungal infections in Toukh primary Health care Centre. Egypt J Hosp Med. 2018;72(7):4898–4902. doi:10.21608/ejhm.2018.10171
30. Furreh FH, Eltayeb AAM, Hamza M, et al. Self-medication practice among health science students in International University of Africa (Iua), Khartoum, Sudan. World J Pharm Res. 2016;5(5):61–69.
31. Alshahrani SM, Alavudeen SS, Alakhali KM, Al-Worafi YM, Bahamdan AK, Vigneshwaran E. Self-medication among King Khalid University students, Saudi Arabia. Risk Manag Healthc Policy. 2019;12:243–249. doi:10.2147/RMHP.S230257
32. Donkor ES, Tetteh-Quarcoo PB, Nartey P, Agyeman IO. Self- medication practices with antibiotics among tertiary level students in Accra, Ghana: a cross-sectional study. Int J Environ Res Public Health. 2012;9(10):3519–3529. doi:10.3390/ijerph9103519
33. Haque M, Rahman NAA, McKimm J, et al. Self-medication of antibiotics: investigating practice among university students at the Malaysian National Defence University. Infect Drug Resist. 2019;12:1333–1351. doi:10.2147/IDR
34. Abebe D, Tenaw G, Dessalegn H, et al. Knowledge, attitude and practice of self-medication among health science students at DebreMarkos University, Northwest Ethiopia. J Public Health Epidemiol. 2017;9(5):106–113. doi:10.5897/JPHE
35. Niwandinda F, Lukyamuzi EJ, Ainebyona C, Ssebunya VN, Murungi G, Atukunda EC. Patterns and practices of self-medication among students enrolled at Mbarara University of Science and Technology in Uganda. Integr Pharm Res Pract. 2020;9:41–48. doi:10.2147/IPRP.S237940
36. Pan H, Cui B, Zhang D. Prior knowledge, older age, and higher allowance are risk factors for self-medication with antibiotics among University Students in Southern China. PLoS One. 2012;7:e41314. doi:10.1371/journal.pone.0041314
37. Alkhatatbeh MJ, Alefan Q, Alqudah MA. High prevalence of self-medication practices among medical and pharmacy students: a study from Jordan. Int J Clin Pharmacol Ther. 2016;54(5):390–398. doi:10.5414/CP202451
38. Eichhorn T, Greten HJ, Efferth T. Self-medication with nutritional supplements and herbal over-the-counter products. Nat Prod Bioprospect. 2011;1:62–70. doi:10.1007/s13659-011-0029-1
39. Ahmed N, Nounou MI, Abouelfetouh A, El-Kamel A. Over-the-counter herbal weight loss supplements in Egypt: label claim, microbiological and pharmaceutical quality, and safety assessments. Med Princ Pract. 2019;28:167–177. doi:10.1159/000495986
40. Khazan M, Hedayati M, Kobarfard F, Askari S, Azizi F. Identification and determination of synthetic pharmaceuticals as adulterants in eight common herbal weight loss supplements. Iran Red Crescent Med J. 2014;16(3):e15344. doi:10.5812/ircmj.15344
41. Rebiere H, Guinot P, Civade C, Bonnet PA, Nicolas A. Detection of hazardous weight-loss substances in adulterated slimming formulations using ultra-high-pressure liquid chromatography with diode-array detection. Food Addit Contam Part a Chem Anal Control Expo Risk Assess. 2012;29(2):161–171. doi:10.1080/19440049.2011.638676
42. Alonso-Castro AJ, Ruiz-Padilla AJ, Ramírez-Morales MA, et al. Self-treatment with herbal products for weight-loss among overweight and obese subjects from Central Mexico. J Ethnopharmacol. 2019;234:21–26. doi:10.1016/j.jep.2019.01.003
43. Eldalo AS, Alotaibi MN, Alenazi TO, Albogami HA, Mohamed KM. Use of herbal medicines in the treatment of obesity in Taif, Saudi Arabia. Saudi J Med Med Sci. 2017;5(2):149–154. doi:10.4103/1658-631X.204862
44. Alshogran OY, Alzoubi KH, Khabour OF, Farah S. Patterns of self-medication among medical and non-medical university students in Jordan. Risk Manag Healthc Policy. 2018;11:169–176. doi:10.2147/RMHP.S170181
45. Garcia-Alvarez A, Mila-Villarroel R, Ribas-Barba L, et al. Usage of Plant Food Supplements (PFS) for weight control in six European countries: results from the PlantLIBRA PFS Consumer Survey 2011–2012. BMC Complement Altern Med. 2016;16:254–268. doi:10.1186/s12906-016-1227-5
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.