Back to Archived Journals » Integrated Blood Pressure Control » Volume 17
Prevalence and Predictors of Depression Symptoms Among Afghan Hypertensive Patients: Secondary Analysis of a Multi-Center Cross-Sectional Study
Authors Stanikzai MH ![]() , Zafar MN, Akbari K, Baray AH, Sayam H
, Zafar MN, Akbari K, Baray AH, Sayam H
Received 22 July 2024
Accepted for publication 13 October 2024
Published 16 October 2024 Volume 2024:17 Pages 41—50
DOI https://doi.org/10.2147/IBPC.S488064
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Turgay Celik
Muhammad Haroon Stanikzai,1 Mohammad Nasim Zafar,2 Khalid Akbari,3 Ahmad Haroon Baray,1 Hadia Sayam1
1Department of Public Health, Faculty of Medicine, Kandahar University, Kandahar, Afghanistan; 2Department of Para-Clinic, Faculty of Medicine, Kandahar University, Kandahar, Afghanistan; 3Department of Internal Medicine, Faculty of Medicine, Paktia University, Gardez, Paktia, Afghanistan
Correspondence: Muhammad Haroon Stanikzai, Department of Public Health, Faculty of Medicine, Kandahar University, District # 10, 3801, Kandahar, Afghanistan, Tel +93704775578, Email [email protected]
Background: Although depression is a frequently occurring mental disorder in patients with hypertension, little is known about the symptoms of depression among Afghan hypertensive patients.
Objective: This study aimed to analyze the prevalence and predictors of depression symptoms among Afghan hypertensive patients.
Methods: This was a secondary analysis of a multi-center cross-sectional study conducted between August and December 2022 across three major provinces in Afghanistan. Socio-demographic and clinical characteristics of the eligible participants were used in the analysis. A score of ≥ 5 on the PHQ-9 (Patient Health Questionnaire) was considered the cut-off point for labeling hypertensive patients as screening positive for depressive symptoms. We performed binary logistic regression to determine the predictors of depression symptoms among hypertensive patients.
Results: Out of 853 hypertensive patients, 51.8% (95% CI: 48.4– 55.2%) had depressive symptoms. Binary logistic regression revealed that low monthly household income [AOR=1.42, 95% CI (1.01– 1.97), low education level [2.41 (1.57– 3.71)], physical inactivity [1.81 (1.22– 2.71)], poor blood pressure control [2.41 (1.57– 3.71)], and the presence of medical comorbidity [1.59 (1.15– 2.19)] were the predictors of depression symptoms.
Conclusion: This study showed a high prevalence of depressive symptoms among Afghan hypertensive patients. Moreover, we found that low monthly household income, physical inactivity, low education level, poor blood pressure control, and the presence of medical comorbidity were the predictors of depression symptoms. Our findings suggest that hypertensive patients should be screened for mental health symptoms, and those most at risk for depression should seek supportive counseling.
Keywords: hypertension, depression, determinants, Afghanistan
Introduction
Hypertension remains a pressing public health concern, contributing largely to global disability and mortality (19% of all deaths).1 In Afghanistan, hypertension is considered one of the major healthcare problems.2 The estimated prevalence of hypertension among the Afghan adult population is approximately 25%.3,4 Existing evidence highlights significant challenges in managing hypertension, partly due to an undermined health system and persistent sociopolitical and economic instability.2,5 Mental health is sensitive to chronic medical conditions and their health and economic consequences.6
Depression in patients with hypertension has generally been associated with dire consequences, including a higher likelihood of uncontrolled hypertension, poor medication adherence, financial stress, and a decreased quality of life (QOL).7–10 In a multi-center study, depression was associated with a substantially higher risk of cardiovascular death.11 Moreover, higher rates of clinical inertia and uncontrolled hypertension were reported in another study.12 Together, early findings suggest that depression in patients with hypertension is associated with adverse outcomes and should be an issue of great importance for policymakers and clinicians.
Previous research has reported on depression symptoms prevalence among hypertensive patients.7,13,14 A meta-analysis encompassing 41 studies found that the pooled prevalence of depression in hypertensive patients was 26.8%.13 Another meta-analysis by Dutta et al showed that the prevalence of depression among Indian hypertensive patients was 39.8%.15 According to a single-center study from Afghanistan, 58.1% of hypertensive patients were estimated to have depression symptoms.16 This study also reported a comorbid depression-anxiety prevalence of 28.2% in hypertensive patients.16 However, more representative data are needed to guide policy efforts and specific interventions targeted at hypertension treatment in the country.
Several studies have identified factors associated with depression symptoms in hypertensive patients.7,13,16 These include female gender, older age, low education level, presence of comorbid illness, poor blood pressure (BP) control, single marital status, physical inactivity, family history of depression, low social support, poor medication adherence, and lower socioeconomic status.7,15,17,18 A previous study conducted in Afghanistan found that older age and diabetes mellitus are associated with depression symptoms in hypertensive patients.16 More details on context-specific factors predicting depression symptoms among hypertensive patients might further focus interventions on the patients most affected.
In a meta-analysis of 27 randomized clinical trials (RCTs), combination treatment for depression and hypertension significantly improved blood pressure control.14 Furthermore, it enhanced the efficiency of anti-hypertensive therapy.14 Moreover, an observational cohort study in Estonia found that depression therapy improves adherence to anti-hypertensive medications (AHMs).19 Despite these benefits, almost no data are available on the screening and management of depression symptoms among hypertensive patients in Afghanistan.
Research on the prevalence and predictors of depression symptoms among Afghan hypertensive patients is limited.20 Previous research regarding the prevalence and associated factors of depression in hypertensive patients was undertaken at a single outpatient department.16 Therefore, we conducted this multi-center study to analyze the prevalence and predictors of depression symptoms among Afghan hypertensive patients. The findings of this study may help policymakers and clinicians to develop effective interventions for patients with both depression and hypertension.
Methods
Data Source
This was a secondary analysis of a multi-center cross-sectional conducted between August and December 2022 across three major provinces in Afghanistan. Briefly, the study sites were Mirwais Regional Hospital in Kandahar province, Paktia Regional Hospital in Paktia province, and Ibn Sina Hospital in Kabul province. Each of these hospitals has a designated site for hypertension treatment services. The study population consisted of randomly selected adult hypertensive patients (who received anti-hypertensive treatment for at least three months) visiting the study sites for follow-up treatment during the study period. Details on the sample size, sampling procedure, and data collection procedures are described previously.3
Study Variables
Outcome Variable
In our study, depression was classified as the outcome variable and assessed using the Pashtu version of the Patient Health Questionnaire (PHQ-9). The PHQ-9 consists of nine items and mainly evaluates depressive symptoms over the past two weeks using a 4-point (0–3) Likert scale.21 The PHQ-9 severity ratings were used to define levels of depression: none/minimal depression (0–4), mild depression (5–9), moderate depression (10–14), moderately severe depression (15–19), and severe depression (≥ 20).21 A score of ≥ 5 on PHQ-9 was considered the cut-off point for labeling hypertensive patients as screening positive for depressive symptoms.3,21 The Pashtu version of PHQ-9 has been used in multiple previous studies,3,22,23 and demonstrated acceptable internal reliability in this study (Cronbach’s α=0.92).
Independent Variables
The sociodemographic variables we examined included age, sex, education, residence, marital status, occupation, income, and Body Mass Index (BMI).
Clinical characteristics were current smoking status, physical activity, disease duration, knowledge of hypertension, number of AHMs, hypertension control status, presence of medical comorbidity, and compliance with anti-hypertensive treatment. Compliance was assessed using the Hill-Bone compliance scale, which is described in detail elsewhere.3,22
Blood pressure was measured in accordance with the American Heart Association’s guidelines for blood pressure assessment.21 To measure BP, we used a portable sphygmomanometer, recording the average of three readings.3,21 Hypertensive patients, with medical treatment who had a systolic blood pressure (SBP) greater than or equal to 140 mmHg and/or diastolic blood pressure (DBP) greater than or equal to 90 mmHg were classified as having poor BP control.3
In this study, we have employed the term “presence of medical comorbidity” to denote a chronic health problem, such as cardiovascular disease (CVD), chronic kidney disease, Diabetes Mellitus (DM), and chronic respiratory diseases, that a patient might have suffered in addition to hypertension.
Statistical Analysis
We used Statistical Package for the Social Sciences (SPSS) version 26 for data analysis in July 2024. Descriptive statistics, such as frequency and percentage were used to describe sociodemographic and clinical variables using tables and graphs. We conducted bivariate analysis for all independent covariates. Variables with a p-value of < 0.25 were retained in the multivariable logistic regression model. The binary logistic regression was conducted to determine the predictors of depression symptoms in the sampled population. A p-value of <0.05 was considered significant.
Results
As shown in Table 1, there were 853 patients receiving anti-hypertensive follow-up treatment in the designated study sites between August and December 2022. The mean age was 47.5 (SD 9.5) years, with 45.5% of the patients in the 40–49 years age group. Of all the participants, around half (431; 50.5%) were males, 445 (52.2%) were urban residents, and most patients (777; 91.1%) were married. The majority (584; 68.5%) of patients had no formal education, 239 (28%) were self-employed, and 397 (46.5%) lived in families with more than eight members. Moreover, 573 (67.2%) had a household income < 10,000/month (equivalent to 150 USD, July 2024), and 195 (22.9%) of them were overweight/obese (Table 1).
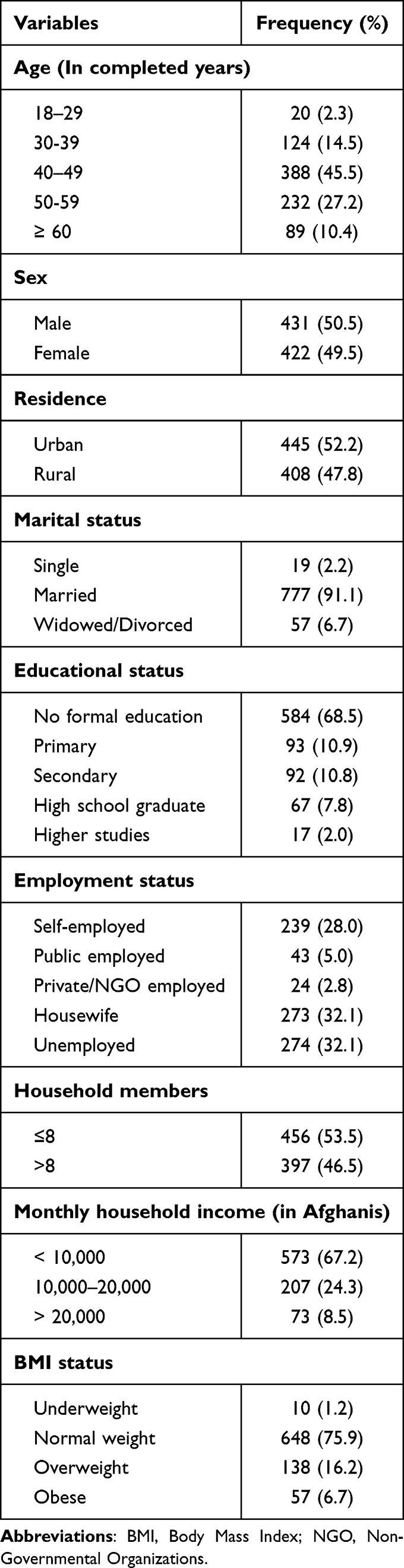 |
Table 1 Socio-Demographic Characteristics of the Hypertensive Patients (n=853) |
Of the total participants, 452 (53%) had hypertension for more than five years, 659 (77.3%) had uncontrolled hypertension, 415 (48.7%) had a family history of hypertension, and more than one-third (328; 38.5%) had a medical comorbidity. Further, 575 (67.4%) patients had poor knowledge of hypertension, 333 (39%) were on three or more AHMs, and 359 (42.1%) had poor compliance with anti-hypertensive treatment. Moreover, most (683; 80.2%) patients were physically inactive, and nearly one-third (245; 28.7%) of them were currently smoking (Table 2).
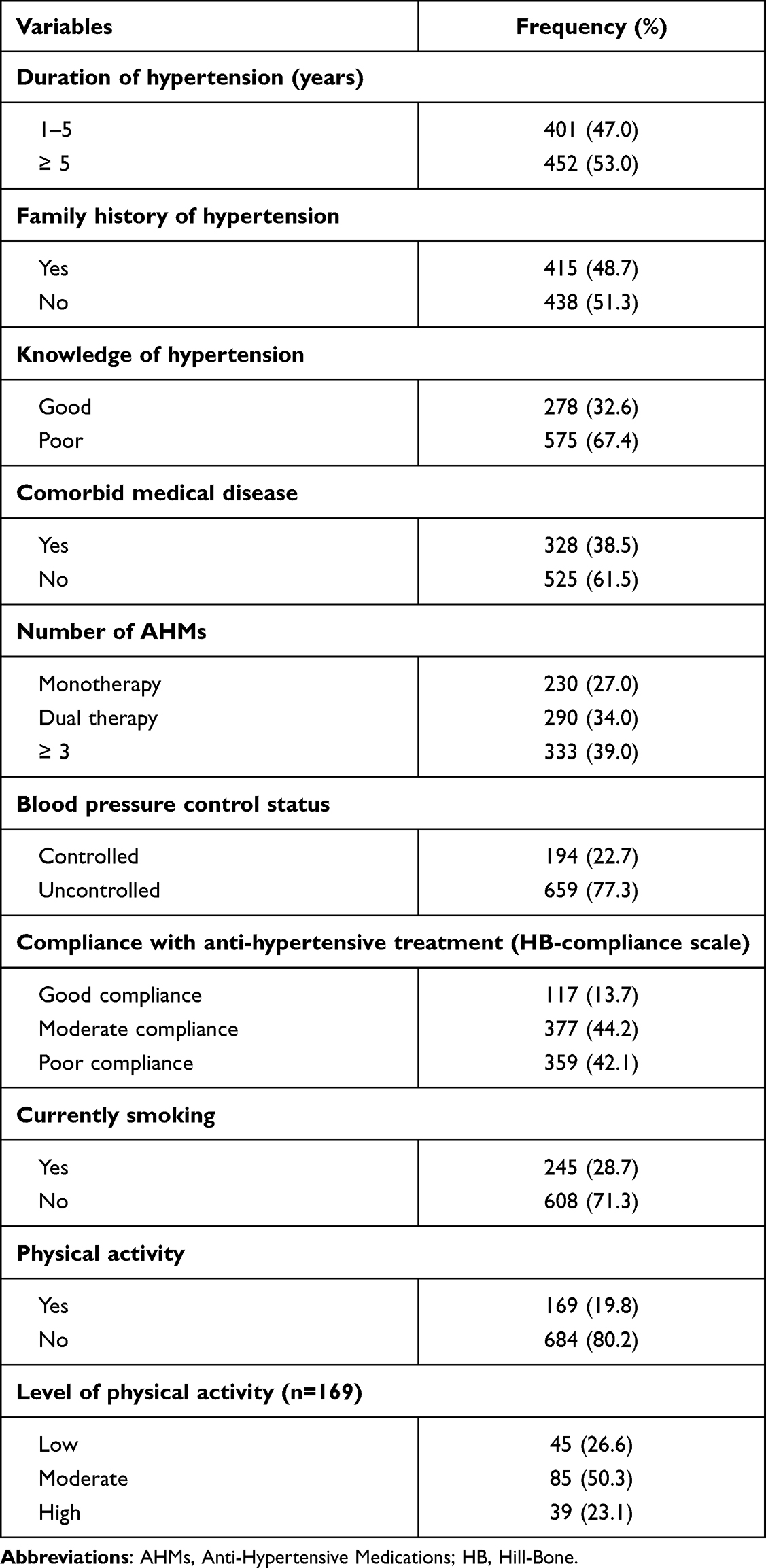 |
Table 2 Clinical Characteristics of the Hypertensive Patients (n=853) |
Out of 853 hypertensive patients, 442 had depressive symptoms according to the PHQ-9 scale, giving a depression prevalence of 51.8% (95% CI: 48.4–55.2%). The prevalence of mild, moderate, moderate to severe, and severe depression was 10.9%, 27.4%, 13%, and 0.5%, respectively (Figure 1).
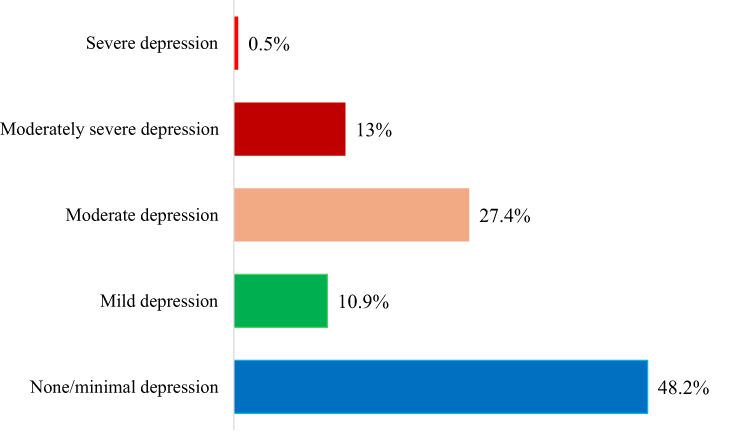 |
Figure 1 Prevalence of depression symptoms among Afghan hypertensive patients (n=853). |
As shown in Table 3, binary logistic regression indicated that low monthly household income [AOR=1.42, 95% CI (1.01–1.97), low education level [1.67 (1.19–2.33)], physical inactivity [1.81 (1.22–2.71)], poor blood pressure control [2.41 (1.57–3.71)], and the presence of medical comorbidity [1.59 (1.15–2.19)] were associated with depressive symptoms among the sampled patients (Table 3).
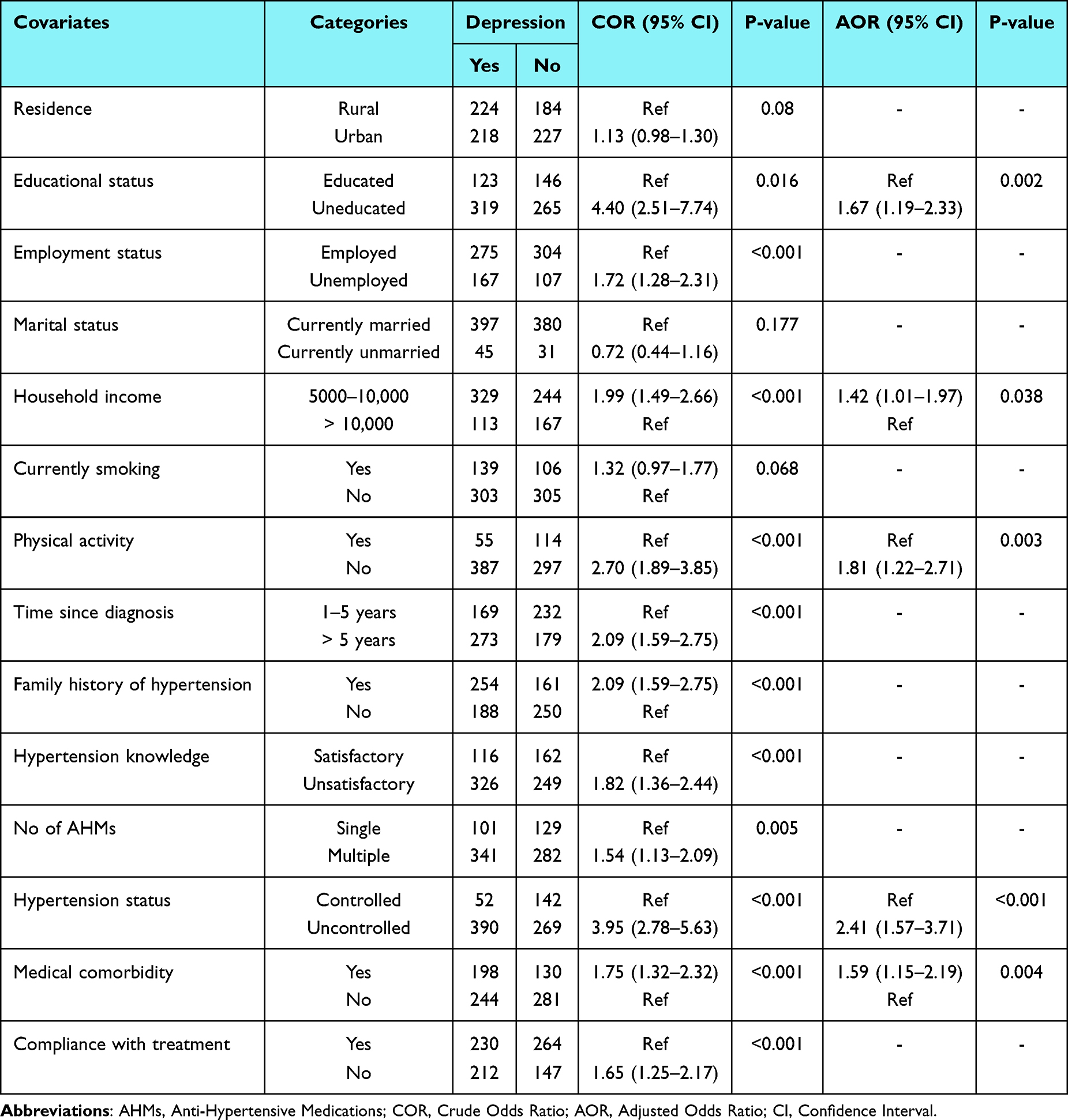 |
Table 3 Logistic Regression Analysis Results on Predictors of Depression Symptoms Among Afghan Hypertensive Patients; Crude and Adjusted Odds Ratios with 95% CIs |
Discussion
Depression is a prevalent mental disorder among patients with hypertension.13 It carries a heightened risk of poor prognosis, financial stress, and functional impairment.7 In this multi-center cross-sectional study, we found that more than half (51.8%) of the patients had depressive symptoms. Moreover, we found that low monthly household income, low education level, physical inactivity, poor blood pressure control, and medical comorbidity were significant predictors of depressive symptoms in the studied population.
Literature documenting the prevalence of depression among hypertensive patients in low and middle-income countries (LMICs) showed various results. For example, in Ethiopia, 32.4% of hypertensive patients were found to have depression.7 In contrast, in India, the prevalence rate of depressive symptoms among hypertensive patients was about 39.8%.15 The prevalence of depression (51.8%) in our sample of hypertensive patients was comparable to previous findings (58.1%) in Afghanistan,16 but notably higher than in LMICs.7,15,18 Compared to LMICs, persistent sociopolitical instability, higher illiteracy rates, financial stress, limited psychosocial help, and more traumatic life events could be factors in Afghanistan that may contribute to our observation of higher levels of depression in our study.24 Taken together, our findings call on clinicians to screen for depression symptoms in hypertensive patients, and those most at risk for depression should be given supportive counseling.
In terms of educational attainment, patients with a low level of education had a higher risk of developing depression symptoms, which is consistent with previous studies from LMICs.25,26 Moreover, the relationship between educational attainment and depression symptoms in chronic medical conditions is consistently reported across studies.27 We argue that limited access to crucial healthcare information and difficulties in navigating healthcare resources could be associated with symptoms of depression in such patients. Other factors linked to low education levels, such as limited employment opportunities and financial stress, may also contribute to depression symptoms.25 Our study was conducted in a country where numerous sociocultural and political barriers to education have historically existed, especially for women.28 The majority of participants (68.5%) in this study had no formal education, and a great need for targeted mental health services and counseling is warranted. Therefore, interventions to curtail mental health symptoms in hypertensive patients should prioritize patients with lower levels of education.
Previous studies have suggested that household socioeconomic status is one of the demographic factors contributing to depression symptoms in hypertensive patients, and those with lower socioeconomic status were more likely to have depression symptoms.7,15,29 Our findings support this, showing that patients with a low monthly household income were at high risk of developing depression symptoms. Low income alone is a risk factor for depression, and the challenges in managing this chronic medical condition superadd to the psychological burden, exacerbating the symptoms of depression.15,27 The persistent economic difficulties in Afghanistan, which are now compounded by the arduous economic conditions, and by the global economic sanctions imposed in August 2021, may place Afghan hypertensive patients under further financial stress.30 In terms of policy relevance, policy efforts and interventional strategies against depressive symptoms should specifically focus on low-income patients.
This study found a higher depression prevalence among physically inactive hypertensive patients, which was consistent with studies conducted in India,31 and Korea.32 In a meta-analysis of 18 studies, Gan et al reported that physical inactivity was associated with a 3.42 times greater risk of developing depression in adults with hypertension.25 Moreover, the benefits of physical activity in mitigating complications related to hypertension are well documented.33 In Afghanistan, many sociocultural and infrastructural challenges present important obstacles to sufficient physical activity.34 Considering these challenges, physical inactivity remains high (80.2%), as indicated by our findings. The study’s findings will help clinicians encourage their patients to engage in sufficient physical activity, not only to alleviate depression symptoms but also to control blood pressure and prevent further cardiovascular complications.
The odds of depression were 2.41 times greater in patients who had poor blood pressure control. Depression is also a risk factor for uncontrolled hypertension,35 and several studies report that depression is prevalent in patients with uncontrolled hypertension.3,7,15,18,31 In our previous study, we also found that patients with depressive symptoms were 1.9 times more likely to have uncontrolled hypertension.3 Non-adherence to AHMs is linked to depressive symptoms in hypertensive patients.22 Both uncontrolled hypertension and non-adherence to AHMs increase the risk of cardiovascular complications to a greater extent. Therefore, patients with uncontrolled hypertension should be given supportive psychotherapy.
Consistent with previous studies,7,15,17,18 we observed a higher depression prevalence in patients with concomitant medical conditions. Generally speaking, comorbid medical patients have a high risk of depression due to the added physical and emotional burden of managing multiple health conditions.36 Additionally, the complexity of treatment regimens and the potential for reduced quality of life can further exacerbate depressive symptoms.9 Hence, attention should also be given to hypertensive patients with medical comorbidities for screening and management of depression.
Limitations
This study has some limitations. First, depressive symptoms were self-reported, which may introduce bias (social desirability bias) into our findings. Second, PHQ-9 based diagnosis of depression symptoms, rather than clinical diagnosis, can be highly variable. However, PHQ-9, as a diagnostic tool for depression symptoms, has good psychometric properties in patients with chronic medical conditions.21 Third, the secondary data limited our investigation of diverse factors predicting depression symptoms. Therefore, future studies should consider other potential factors, such as social support level, the use of anti-depressants, and history of mental health problems in their analysis. Finally, the cross-sectional study design precludes us from establishing causality between depression symptoms and study variables.
Conclusion
This study showed a high prevalence of depressive symptoms among Afghan hypertensive patients. Moreover, we found that low monthly household income, physical inactivity, low education level, poor blood pressure control, and the presence of medical comorbidity were the predictors of depression symptoms. Our findings suggest that hypertensive patients should be screened for mental health symptoms, and those most at risk for depression should seek supportive counseling.
Data Sharing Statement
The primary data used to support the findings of this study are available from the corresponding author upon request.
Ethical Approval
The Ethics Committee at the Faculty of Medicine, Kandahar University approved the use of secondary data for this study. For data collection in the primary study,3 all participants provided written informed consent, and ethical principles outlined in the Declaration of Helsinki and the Good Clinical Practice (GCP) guidelines were meticulously followed.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Naghavi M, Ong KL, Aali A, et al. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2100–2132. doi:10.1016/S0140-6736(24)00367-2
2. Dadras O, Stanikzai MH, Jafari M, Tawfiq E. Risk factors for non-communicable diseases in Afghanistan: insights of the nationwide population-based survey in 2018. J Health Popul Nutr. 2024;43(1):129. doi:10.1186/s41043-024-00625-0
3. Baray AH, Stanikzai MH, Wafa MH, Akbari K. High Prevalence of Uncontrolled Hypertension Among Afghan Hypertensive Patients: a Multicenter Cross-Sectional Study. Integr Blood Press Control. 2023;16:23–35. doi:10.2147/ibpc.S417205
4. Neyazi A, Mohammadi AQ, Neyazi M, Timilsina S, Padhi BK, Griffiths MD. Hypertension, depression, and health-related quality of life among hospitalized patients in Afghanistan. J Hum Hypertens. 2024;38(6):529–537. doi:10.1038/s41371-024-00914-5
5. Neyazi N, Mosadeghrad AM, Afshari M, Isfahani P, Safi N. Strategies to tackle non-communicable diseases in Afghanistan: a scoping review. Front Public Health. 2023;11:982416. doi:10.3389/fpubh.2023.982416
6. Liao B, Xu D, Tan Y, Chen X, Cai S. Association of mental distress with chronic diseases in 1.9 million individuals: a population-based cross-sectional study. J Psychosom Res. 2022;162:111040. doi:10.1016/j.jpsychores.2022.111040
7. Tassew WC, Nigate GK, Assefa GW, Zeleke AM, Ferede YA. Systematic review and meta-analysis on the prevalence and associated factors of depression among hypertensive patients in Ethiopia. PLoS One. 2024;19(6):e0304043. doi:10.1371/journal.pone.0304043
8. Amaike C, Salami OF, Bamidele OT, et al. Association of depression and anxiety with uncontrolled hypertension: a cross-sectional study in Southwest Nigeria. Indian J Psychiatry. 2024;66(2):157–164. doi:10.21203/rs.3.rs-2384827/v1
9. Ang CW, Tan MM, Bärnighausen T, Reininghaus U, Reidpath D, Su TT. Mental distress along the cascade of care in managing hypertension. Sci Rep. 2022;12(1):15910. doi:10.1038/s41598-022-20020-1
10. Samuel N, Nigussie S, Jambo A, et al. Treatment Outcome and Associated Factors Among Patients Admitted with Hypertensive Crisis in Public Hospitals at Harar Town, Eastern Ethiopia: a Cross-Sectional Study. Integr Blood Press Control. 2022;15:113–122. doi:10.2147/ibpc.S386461
11. Maguire LK, Hughes CM, McElnay JC. Exploring the impact of depressive symptoms and medication beliefs on medication adherence in hypertension--A primary care study. Patient Educ Couns. 2008;73(2):371–376. doi:10.1016/j.pec.2008.06.016
12. Moise N, Davidson KW, Chaplin W, Shea S, Kronish I. Depression and clinical inertia in patients with uncontrolled hypertension. JAMA Intern Med. 2014;174(5):818–819. doi:10.1001/jamainternmed.2014.115
13. Li Z, Li Y, Chen L, Chen P, Hu Y. Prevalence of Depression in Patients With Hypertension: a Systematic Review and Meta-Analysis. Medicine. 2015;94(31):e2133. doi:10.1097/md.0000000000001317
14. Wang L, Liu Q, Sun D, Xie J, Lao D, Zhang L. Effects of Combination Treatment in Hypertensive Patients with Depression: a Systematic Review and Meta-Analysis of 27 Randomized Controlled Trials. Ther Clin Risk Manag. 2022;18:197–211. doi:10.2147/tcrm.S347622
15. Dutta A, Chaudhary V, Gupta AK, et al. Prevalence of depression in hypertensive patients and its associated factors in India: a systematic review and meta-analysis. Hipertens Riesgo Vasc. 2024. doi:10.1016/j.hipert.2024.05.003
16. Hamrah MS, Hamrah MH, Ishii H, et al. Anxiety and Depression among Hypertensive Outpatients in Afghanistan: a Cross-Sectional Study in Andkhoy City. Int J Hypertens. 2018;2018:8560835. doi:10.1155/2018/8560835
17. Abate MW, Nigat AB, Tigabu A, et al. Depression and its associated factors among adult hypertensive patients attending follow-up in South Gondar zone public hospitals, Ethiopia, 2023. BMC Psychiatry. 2024;24(1):360. doi:10.1186/s12888-024-05807-y
18. Gebre BB, Deribe B, Abeto M. Magnitude and Associated Factors of Depression Among Hypertensive Patients Attending Treatment Follow Up in Chronic OPD at Hawassa University Comprehensive Specialized Hospital, Hawassa, Southern Ethiopia. Integr Blood Press Control. 2020;13:31–39. doi:10.2147/ibpc.S240015
19. Kariis HM, Kasela S, Jürgenson T, et al. The role of depression and antidepressant treatment in antihypertensive medication adherence and persistence: utilising electronic health record data. J Psychiatr Res. 2023;168:269–278. doi:10.1016/j.jpsychires.2023.10.018
20. Stanikzai MH, Wafa MH, Rahimi BA, Sayam H. Conducting Health Research in the Current Afghan Society: challenges, Opportunities, and Recommendations. Risk Manag Healthc Policy. 2023;16:2479–2483. doi:10.2147/rmhp.S441105
21. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
22. Stanikzai MH, Wafa MH, Tawfiq E, et al. Predictors of non-adherence to antihypertensive medications: a cross-sectional study from a regional hospital in Afghanistan. PLoS One. 2023;18(12):e0295246. doi:10.1371/journal.pone.0295246
23. Stanikzai MH, Ishaq N, Zafar MN, et al. Depression symptoms among Afghan TB patients: a multi-center study. Indian J Tuberc. 2024;71:S264–S268. doi:10.1016/j.ijtb.2024.08.016
24. Kovess-Masfety V, Keyes K, Karam E, Sabawoon A, Sarwari BA. A national survey on depressive and anxiety disorders in Afghanistan: a highly traumatized population. BMC Psychiatry. 2021;21(1). doi:10.1186/s12888-021-03273-4
25. Gan Q, Yu R, Lian Z, Yuan Y, Li Y, Zheng L. Unraveling the link between hypertension and depression in older adults: a meta-analysis. Front Public Health. 2023;11:1302341. doi:10.3389/fpubh.2023.1302341
26. Taple BJ, Chapman R, Schalet BD, Brower R, Griffith JW. The Impact of Education on Depression Assessment: differential Item Functioning Analysis. Assessment. 2022;29(2):272–284. doi:10.1177/1073191120971357
27. Katon WJ. Epidemiology and treatment of depression in patients with chronic medical illness. Dialogues Clin Neurosci. 2011;13(1):7–23. doi:10.31887/DCNS.2011.13.1/wkaton
28. Stanikzai MH, Wafa MH, Akbari K, et al. Afghan medical students’ perceptions, and experiences of their medical education and their professional intentions: a cross-sectional study. BMC Med Edu. 2023;23(1):569. doi:10.1186/s12909-023-04577-7
29. Shah RM, Doshi S, Shah S, Patel S, Li A, Diamond JA. Impacts of Anxiety and Depression on Clinical Hypertension in Low-Income US Adults. High Blood Press Cardiovasc Prev. 2023;30(4):337–342. doi:10.1007/s40292-023-00584-3
30. Safi N, Anwari P, Safi H. Afghanistan’s health system under the Taliban: key challenges. Lancet. 2022;400(10359):1179–1180. doi:10.1016/S0140-6736(22)01806-2
31. Sekhri S, Verma A. Study of Depression and Its Associated Factors Among Patients of Diabetes Mellitus (DM) and Hypertension (HTN) Attending a Primary Health Center (PHC) in a Rural Area of New Delhi, India. Cureus. 2023;15(1):e33826. doi:10.7759/cureus.33826
32. Son Y-J, Park C, Won MH. Impact of Physical Activity and Sleep Duration on Depressive Symptoms in Hypertensive Patients: results from a Nationally Representative Korean Sample. Int J Environ Res Public Health. 2018;15(12):2611. doi:10.3390/ijerph15122611
33. Pearce M, Garcia L, Abbas A, et al. Association Between Physical Activity and Risk of Depression: a Systematic Review and Meta-analysis. JAMA Psychiatry. 2022;79(6):550–559. doi:10.1001/jamapsychiatry.2022.0609
34. Pengpid S, Noormal AS, Peltzer K. High sedentary behavior and low physical activity among adults in Afghanistan: results from a national cross-sectional survey. Front Public Health. 2023;11:1248639. doi:10.3389/fpubh.2023.1248639
35. Wang L, Li N, Heizhati M, et al. Association of Depression with Uncontrolled Hypertension in Primary Care Setting: a Cross-Sectional Study in Less-Developed Northwest China. Int J Hypertens. 2021;2021(1):6652228. doi:10.1155/2021/6652228
36. Gold SM, Köhler-Forsberg O, Moss-Morris R, et al. Comorbid depression in medical diseases. Nat Rev Dis Prim. 2020;6(1):69. doi:10.1038/s41572-020-0200-2
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.