")
Back to Journals » Journal of Blood Medicine » Volume 13
Prevalence and Predictors of Cytopenias in HIV-Infected Adults at Initiation of Antiretroviral Therapy in Mehal Meda Hospital, Central Ethiopia
Received 27 December 2021
Accepted for publication 22 April 2022
Published 26 April 2022 Volume 2022:13 Pages 201—211
DOI https://doi.org/10.2147/JBM.S355966
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Temesgen Fiseha, Hussen Ebrahim
Department of Clinical Laboratory Science, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia
Correspondence: Temesgen Fiseha, Email [email protected]
Background: Hematologic abnormalities are common complications of patients infected with HIV associated with accelerated deterioration in CD4+ cell counts, disease progression, poor quality of life and death. Few studies have evaluated the magnitude of cytopenias at the initiation of antiretroviral therapy (ART) in sub-Saharan Africa. The aim of this study was to determine the prevalence and predictors of cytopenias among HIV-infected adults at initiation of ART in a resource-limited setting in Ethiopia.
Methods: A cross-sectional study was conducted among HIV-infected adults initiating ART at the HIV care and treatment clinic of Mehal Meda Hospital between September 2008 and June 2019. Demographic, clinical and laboratory data of patients were collected from medical records. Anemia was defined according to WHO guidelines as hemoglobin concentration < 12 g/dl for non-pregnant females and < 13 g/dl for males. Leucopenia was defined as total white blood cell count < 4.0 × 103 cells/μL and thrombocytopenia as platelet count < 150 × 103 cells/μL. Logistic regression analysis was used to determine factors associated with the presence of cytopenias.
Results: Out of the total 566 patients included, 36.6% (95% CI 32.7– 40.6%) had anemia, 17.1% (95% CI 14.2– 20.4%) had leucopenia and 14.5% (95% CI 11.8– 17.6%) had thrombocytopenia. A total of 53.2% (95% CI 49.1– 57.3%) of patients had at least one form of cytopenia, 14.1% (95% CI 11.4– 17.2%) had bicytopenia, and only 0.5% had pancytopenia. Factors associated with the presence of any cytopenia in multivariable analysis were male sex, advanced clinical disease stage, low CD4+ cell count, low BMI, and decreased renal function.
Conclusion: A substantial burden of cytopenias was detected among HIV-infected adults enrolled for care and treatment services in our setting. Patients with HIV infection should be screened for hematological abnormalities at initiation of ART because of its potential for morbidity and mortality during ART.
Keywords: hematological abnormalities, cytopenia, HIV, Ethiopia
Introduction
Hematologic abnormalities especially cytopenias (anemia, leucopenia and thrombocytopenia) are common complications of patients infected with Human Immunodeficiency Virus (HIV). These abnormalities occur mainly due to direct effects of the virus on the bone marrow, suppression of bone marrow by secondary infections or neoplasms, nutritional deficiencies or side effects of the drugs used.1–3 Hematologic abnormalities can occur at all stages of HIV infection, but are more prevalent in patients with advanced disease and in ART naive patients than treated patients.4–7 In patients with HIV, cytopenias have been associated with accelerated deterioration in CD4+ cell counts, disease progression, poor quality of life and subsequent death.8–11 Hematologic abnormalities have also been demonstrated to predict poor responses to ART, Acquired Immunodeficiency Syndrome (AIDS)-related morbidity and mortality, and have been suggested as important parameters for predicting the clinical course of patients living with HIV infection.12,13
Anemia is the most common hematologic abnormality seen in HIV infection, occurring in 1.3% to 95% of patients and has been associated with impaired quality of life, poor immune recovery, progression of disease and a high risk of hospitalization or mortality.14–16 It is also an independent predictor of morbidity and mortality even upon initiation of therapy.12,13,17 The pathogenesis of anemia in HIV patients is complex and may result from opportunistic infections, nutritional deficiencies, AIDS-associated malignancies, medications, and alteration in hematopoiesis induced by HIV itself or the drugs included in ART.3,8,18 Factors that are associated with anemia among HIV-infected antiretroviral-naive patients include older age, gender, presence of opportunistic infection, advanced clinical HIV disease stages, low CD4+ cell counts, low body mass index and decreasing renal function.19–21
Leucopenia is the common hematologic abnormality that occurs in patients with HIV-infection and results from a direct effect of HIV virus, autoimmune disease, neoplasm and ART drugs and opportunistic infection.3 It can occur in as many as 26.8% of patients and is associated with adverse HIV-related outcomes including both death and AIDS-related morbidity.6,13 Studies indicated that worsening HIV disease parameters, ie, advanced clinical stages and low CD4+ cell counts, are associated with an increased risk of leucopenia among antiretroviral-naive patients.20,21 Thrombocytopenia is a frequent hematologic abnormality in HIV patients and can occur at all stages of HIV infection. It can be found in about 4–40% of HIV-infected patients and results from decreased production or accelerated destruction of platelets, with immune thrombocytopenic purpura the most common cause.2,10,22 Thrombocytopenia is associated with a substantial decline in CD4+ cell count, poor quality of life and increased morbidity and mortality.9–12,22 Advanced clinical stages and immunosuppression were the factors significantly related to thrombocytopenia among antiretroviral-naive HIV patients.
Although previous studies have demonstrated the importance of hematological alterations at baseline as influences of treatment failure and mortality during ART among patients treated in sub-Saharan African countries,9,12,23 few studies have evaluated the magnitude of cytopenias at the initiation of ART among HIV patients in sub-Saharan Africa. The aim of this study was to determine the prevalence and predictors of cytopenias among adult HIV-infected patients at initiation of ART in a resource-limited setting in Ethiopia.
Methods
Study Design and Population
We performed a cross-sectional study of HIV-infected adult patients initiating ART at the HIV care and treatment clinic of Mehal Meda Hospital, Central Ethiopia between September 2008 and June 2019. Mehal Meda Hospital is found in Mehal Meda town in Menz Gera Midir Woreda NorthShewa Zone of the Amhara Region, Ethiopia. Mehal Meda town is about 280 km away from the capital city Addis Ababa and 148 km from Debre Birhan city, the capital of Amhara Region. The hospital provides comprehensive health-care services including HIV/AIDS diagnosis, treatment and monitoring. Patients were included in this study if they were 18 years and older, and had full blood count results available at baseline before the initiation of ART. Patients with missing data for essential variables, and pregnant women were excluded from the study analysis.
Data Collection and Definitions
The medical records of HIV-infected patients enrolled to receive first-line ART, comprised of at least three drugs from September 2008 and June 2019 were reviewed. Patients’ baseline socio-demographic (age, gender, residence, education, weight and height), clinical (WHO clinical stage of disease, CD4+ cell count and presence/history of opportunistic infection), and hematological data (hemoglobin level, total white blood cell count and platelet count) were collected. Serum creatinine results available at baseline were collected and renal function was assessed by estimated glomerular filtration rate (eGFR) calculated using the Modification of Diet in Renal Disease (MDRD) equation.24 Complete blood count including hemoglobin concentration, total white blood cell count and platelet count (Sysmex KX-21N, Sysmex corporation Kobe, Japan) and CD4 cell count (BD Facscount system, Becton Dickenson, California, USA) were performed as part of a routine evaluation. Anemia was defined in accordance with the WHO guidelines,25 as hemoglobin concentrations <12.0 g/dL for non-pregnant females and <13.0 g/dL for males. We further classified anemia as mild (11–11.9 g/dL for females and 11–12.9 g/dL for males), moderate (8–10.9 g/dL) and severe (<8 g/dL in both genders). Leucopenia was defined as total white blood cell count <4.0×103 cells/μL and thrombocytopenia as platelet count <150×103 /μL.20 Any cytopenia, bicytopenia and pancytopenia were defined as presence of at least one form of cytopenias (anemia, leucopenia or thrombocytopenia), two forms and all forms of cytopenias, respectively.
Statistical Analysis
Data were entered into an “EpiData version 3.1” and analysed with SPSS version 25 software (SPSS Inc., Chicago, IL, USA). The normal distribution of the data was tested by the Kolmogorov–Smirnov test. Comparisons of continuous variables between groups were carried out using Student’s t-test and chi-square (x2) test was used for categorical variables. A logistic regression analysis was used to identify predictors of anemia, leucopenia, thrombocytopenia and any cytopenia at the initiation of ART. Age, gender, WHO clinical stage of disease, CD4+ cell count, presence/history of opportunistic infections, body mass index (BMI), and eGFR were entered into a univariable model. Variables with P-value <0.25 in the univariable analysis were included in the multivariable models using forward stepwise method. Odds ratio (OR) with 95% confidence interval (CI) was used to measure the strength of statistical association. All tests were two-sided and a P < 0.05 was considered to be statistically significant.
Results
Patient Characteristics
A total of 566 HIV-infected adult patients who enrolled in the HIV care from September 2008 through November 2019 were included in this study. The mean age was 36.1 years (standard deviation [SD] ± 9.7) and 324 patients (67.1%) were females (Table 1). The median CD4+ cell count was 264 cells/mm3 (IQR: 192–500), and 439 patients (71.9%) had WHO clinical stage I/II at the time of enrollment. The mean BMI was 20.4 kg/m2 (SD ± 3.6). The mean eGFR was 99.2 mL/min/1.73 m2 (SD ± 58.2). The mean hemoglobin was 12.7 g/dl (SD ± 2.68), the median total white blood cell count was 5.7×103 cell/μL (IQR: 4.5–7.5), and the median platelet count was 240 × 103/μL (IQR: 176–310).
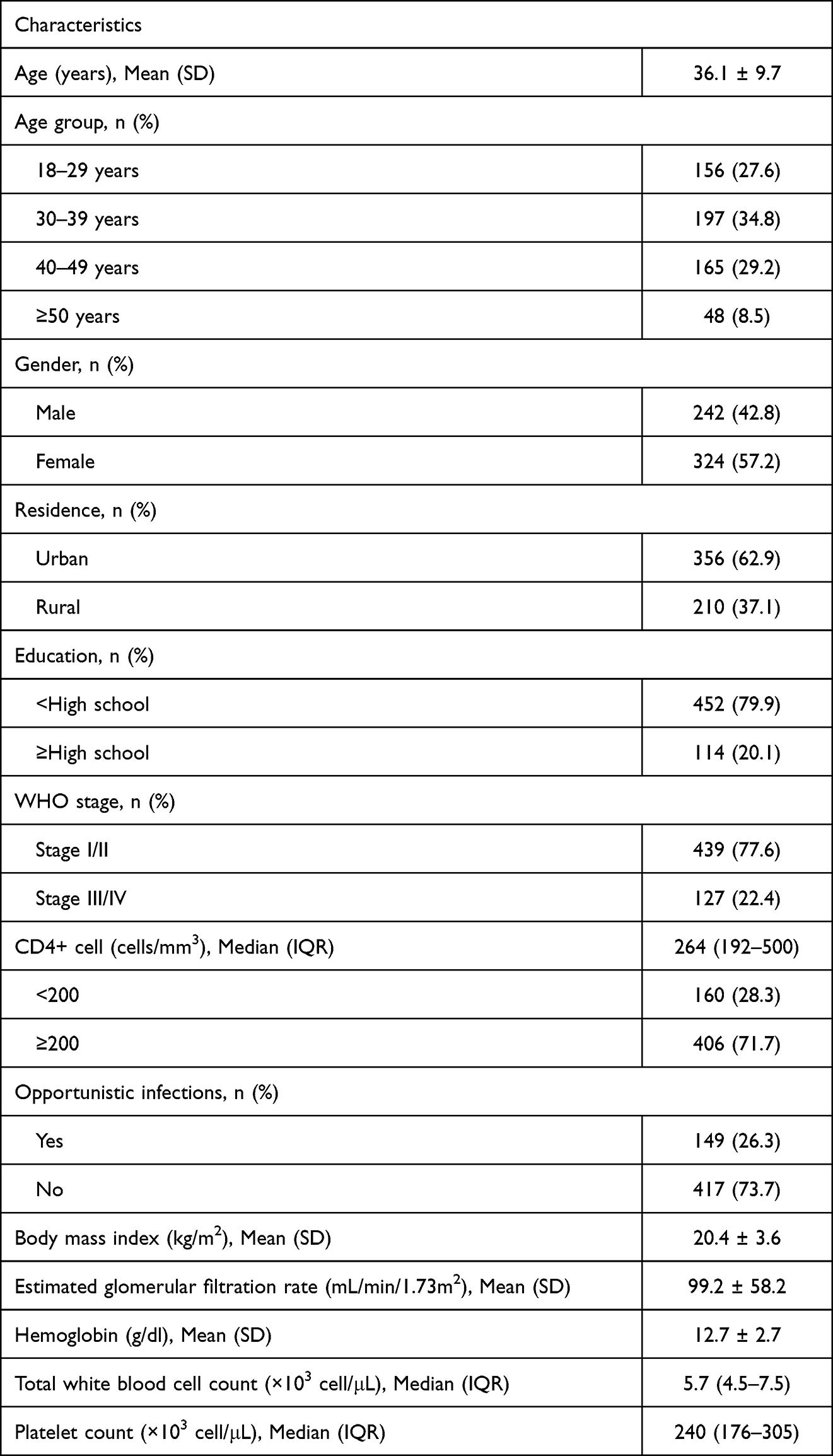 |
Table 1 Characteristics of the Study Patients at the Initiation of ART (N = 566) |
Prevalence and Factors Associated with Cytopenias
Two-hundred and seven patients (36.6%; 95% CI 32.7–40.6%) had anemia, including 92 patients (16.3%) with mild, 85 (15.0%) with moderate and 30 (5.3%) with severe anemia. Advanced clinical HIV/AIDS disease stage (WHO stage III/IV), low CD4+ cell count, history of opportunistic infections, low BMI and low eGFR were associated with anemia in the univariate analysis (Table 2). The multivariable analysis indicated that advanced clinical disease stage (AOR 2.07; 95% CI 1.37–3.18), CD4+ cell count <200 cells/mm3 (AOR 2.00; 95% CI 1.20–3.32), BMI < 18.5 kg/m2 (AOR 2.89; 95% CI 1.46–5.69) and low eGFR: <60 mL/min/1.73 m2 (AOR 2.41; 95% CI 1.46–3.98) and 60–89.9 mL/min/1.73 m2 (AOR 1.92; 95% CI 1.27–2.89) were independently associated with anemia.
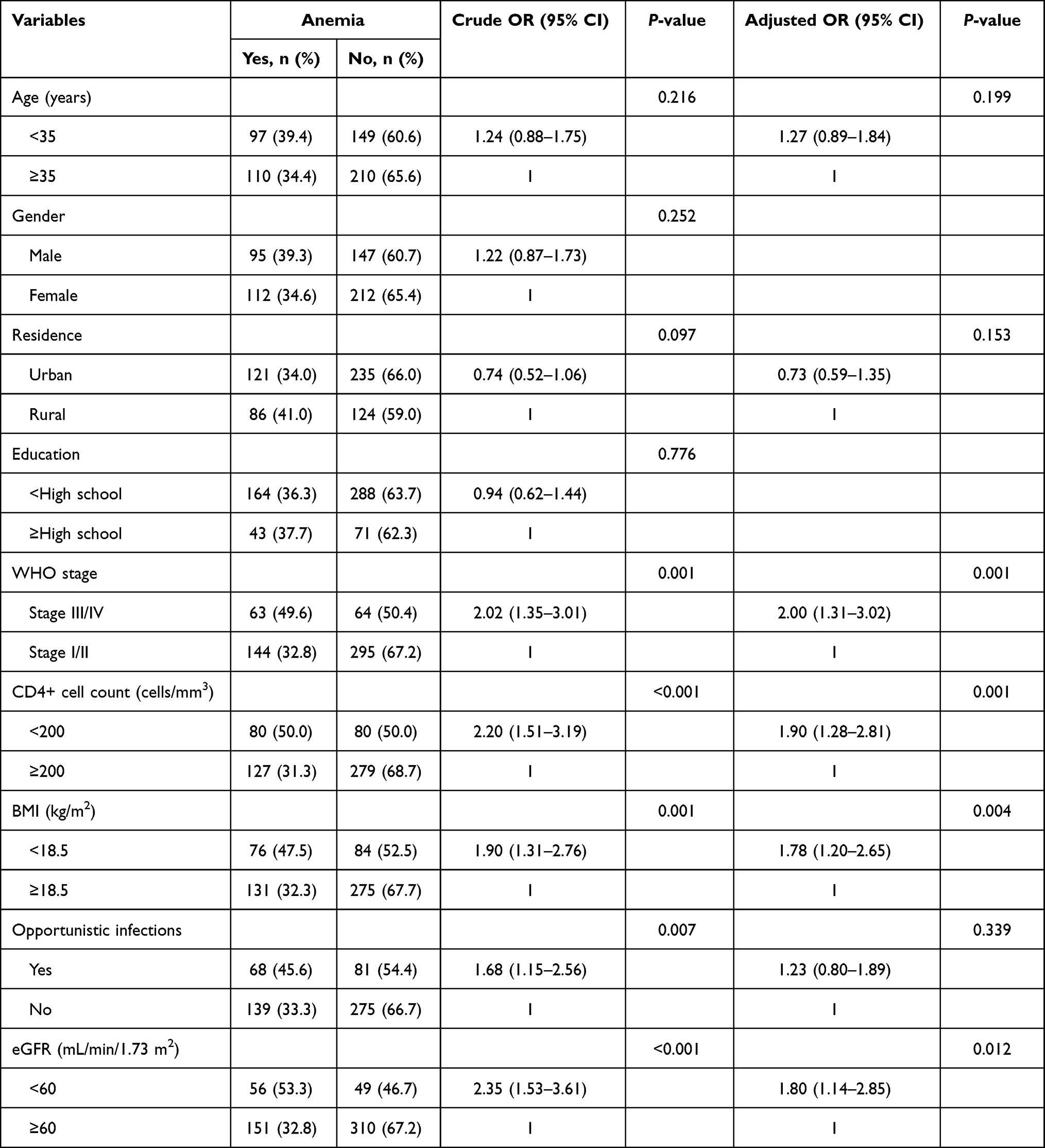 |
Table 2 Factors Associated with the Presence of Anemia at Initiation of ART |
Leucopenia was present in 97 patients (17.1%; 95% CI 14.2–20.4%). In univariate analysis, several risk factors met the pre-defined criteria for inclusion in the multivariable model (age, residence, education, WHO clinical disease stage and CD4+ cell count) (Table 3). In the multivariable analysis, only CD4+ cell count <200 cells/mm3 (AOR 1.93; 95% CI 1.22–3.07) was independently associated with leucopenia. Thrombocytopenia was observed in 82 patients (14.5%; 95% CI 11.8–17.6%). The univariate analysis showed a significant association between thrombocytopenia and male sex, education, WHO clinical disease stage, CD4+ cell count and history of opportunistic infections (Table 4). In multivariable analysis, male sex (AOR 3.22; 95% CI 1.93–5.38), advanced clinical disease stage (AOR 1.72; 95% CI 1.01–2.91) and CD4+ cell count <200 cells/mm3 (AOR 2.07; 95% CI 1.08–3.97) were independently associated with thrombocytopenia.
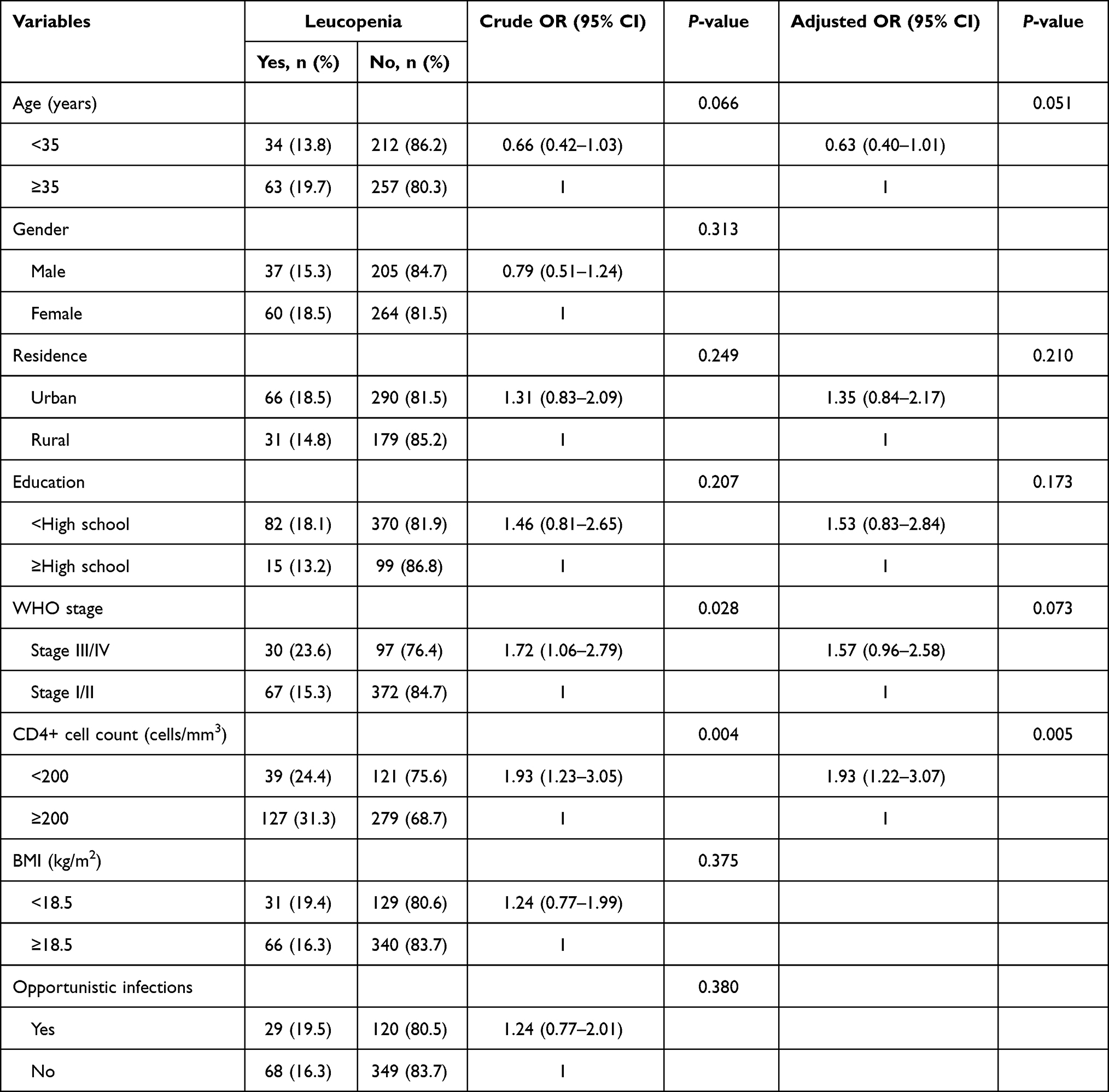 |
Table 3 Factors Associated with the Presence of Leucopenia at Initiation of ART |
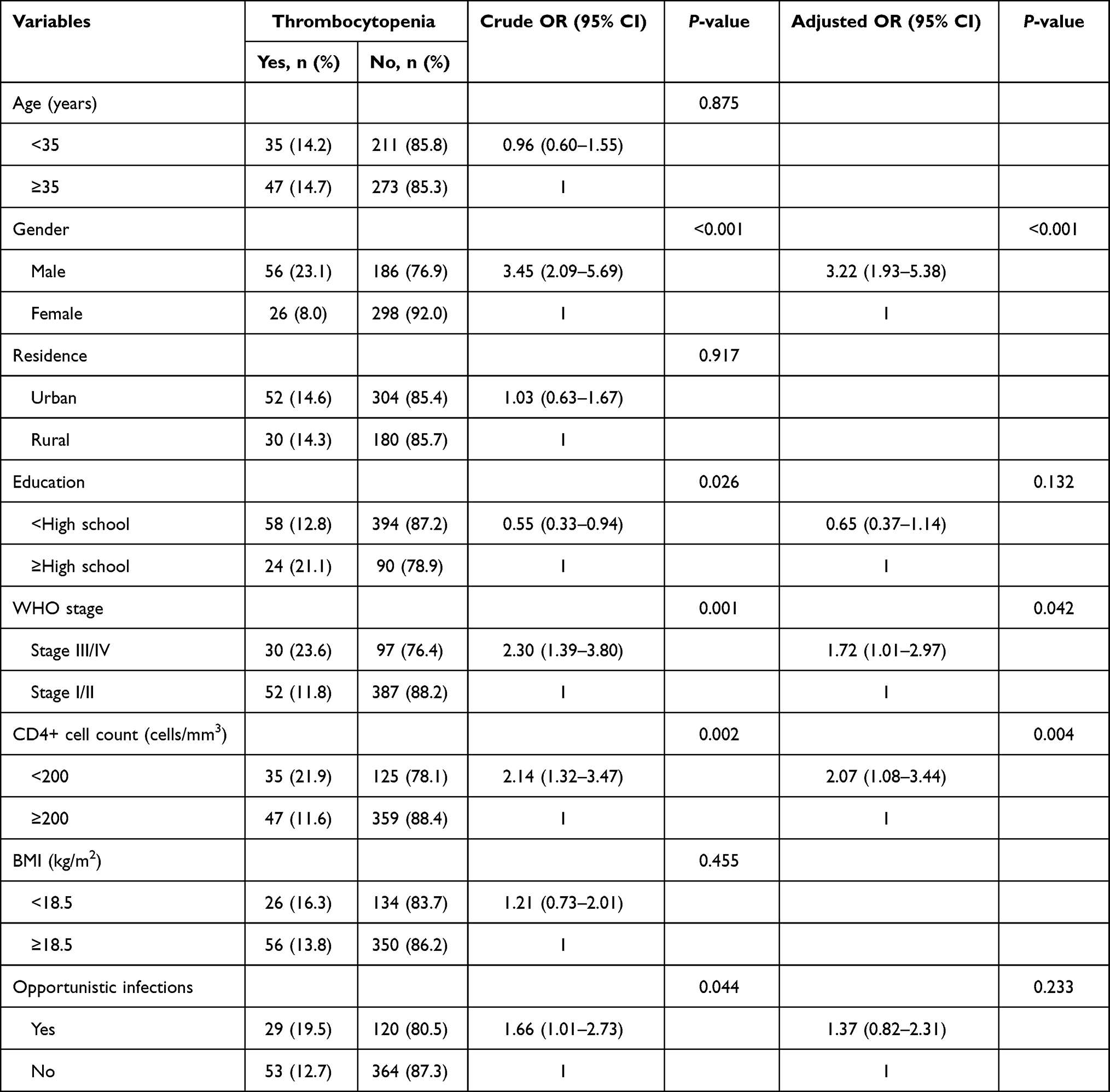 |
Table 4 Factors Associated with the Presence of Thrombocytopenia at Initiation of ART |
A total of 301 patients (53.2%; 95% CI 49.1–57.3%) had at least one form of cytopenia, 80 (14.1%; 95% CI 11.4–17.2%) had bicytopenia, and only 3 (0.5%) had pancytopenia. The anemia-leucopenia combination was the most frequent bicytopenia 41 (7.3%), followed by anemia-thrombocytopenia 28 (4.9%) and leucopenia-thrombocytopenia 11 (1.9%). Factors associated with the presence of any cytopenia in multivariable regression were male sex (AOR 1.73; 95% CI 1.20–2.48), advanced clinical disease stage (AOR 1.72; 95% CI 1.10–2.70), CD4+ cell count <200 cells/mm3 (AOR 2.24; 95% CI 1.49–3.37), BMI < 18.5 kg/m2 (AOR 1.50; 95% CI 1.02–2.44) and decreased renal function (eGFR: <60 mL/min/1.73 m2) (AOR 2.50; 95% CI 1.52–4.12) (Table 5).
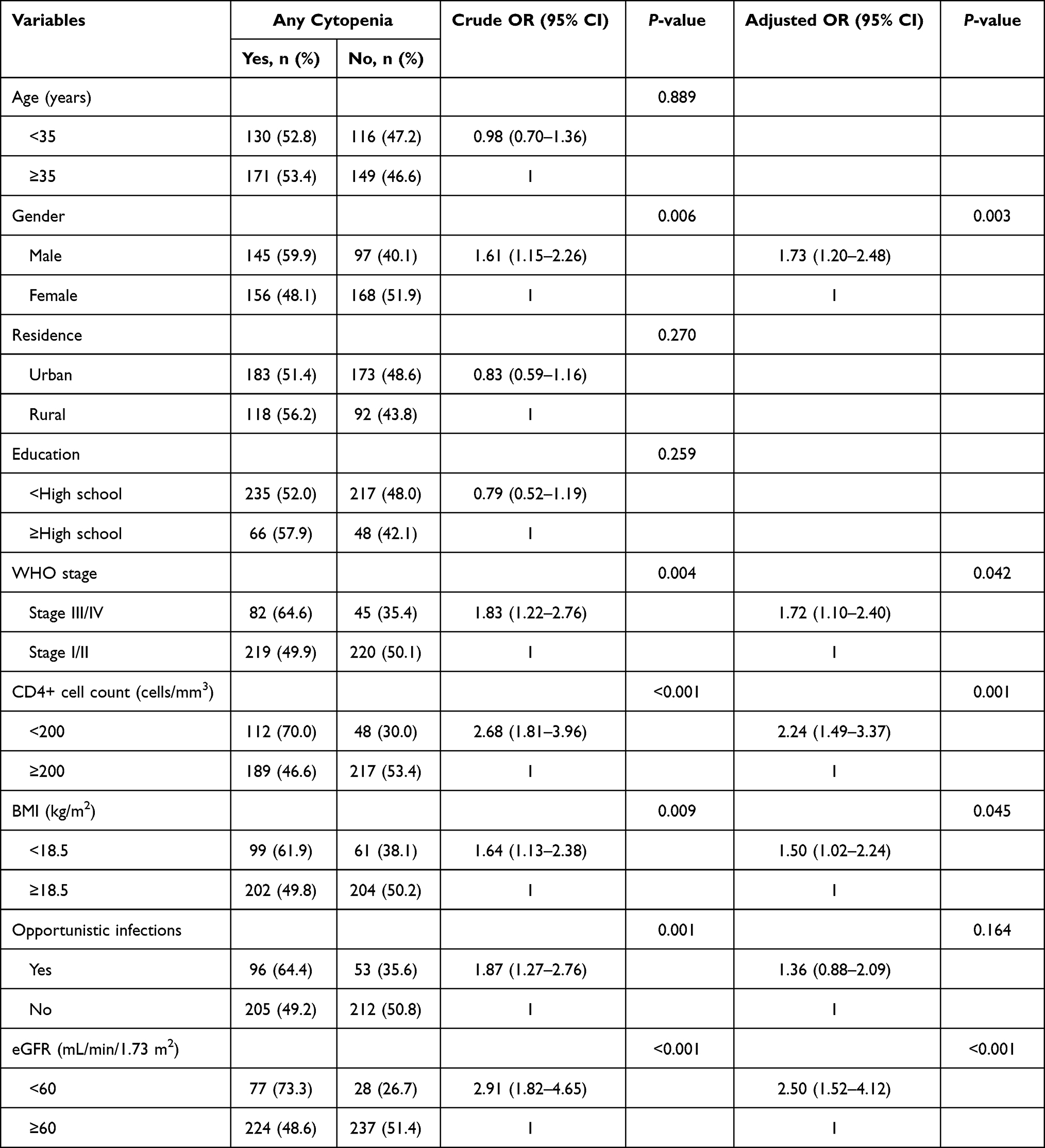 |
Table 5 Factors Associated with the Presence of Any Cytopenia at Initiation of ART |
Discussion
In this study, the prevalence of anemia, leucopenia and thrombocytopenia among antiretroviral–naive adult HIV-positive patients enrolled for care and treatment services in Mehal Meda Hospital, central Ethiopia were 36.6%, 17.1% and 14.5%, respectively. About 53.2% of the patients had at least one form of cytopenia (anemia and/or leucopenia and/or thrombocytopenia). The main factors associated with the presence of any cytopenia were male sex, advanced clinical disease stage, low CD4+ cell count, low BMI, and decreased renal function.
Anemia was the most prevalent cytopenia in this study, occurring in 36.6% of antiretroviral-naive adult HIV-infected patients at initiation of ART. This high prevalence of anemia, already noted by other studies from sub-Saharan Africa,11,14,20,21,26,27 could be explained by the more advanced immunodeficiency at enrollment as well as the higher prevalence of anemia in the general population in sub-Saharan Africa.28,29 The presence of anemia prior to the initiation of combination ART may complicate the treatment of HIV, associated with poor response to ART, treatment failure and clinical disease progression to AIDS and predict decreased survival in HIV-infected patients after ART initiation.9,14,23 Without intervention, anemia can lead to significant symptoms like fatigue, breathlessness, difficulty in concentration and other effects on functionality and quality of life. Targeted screening for anemia at initiation of ART and modifying the potential risk factors are primary needs to improve disease outcomes in people living with HIV.
We found that advanced clinical HIV disease stage (WHO clinical stage III/IV), low CD4+ count, low BMI and low eGFR are associated with an increased risk of anemia in antiretroviral-naive HIV-infected patients. Worsening parameters of HIV disease, ie, WHO clinical stage III/IV and CD4+ cell count <200 cells/mm3, are significantly associated with an increased risk of anemia at ART initiation, and this was consistent with findings of previous related studies.16,19,30,31 We also found evidence that low BMI is associated with an increased risk of anemia prior to ART initiation. Low level of BMI (<18.5 kg/m2) has been previously found to have significant association with the occurrence of anemia.19,31 Our results also support findings that impaired renal function is associated with a higher risk of anemia among HIV patients initiating ART.32 Impaired renal function in HIV infection has a significant impact on lowering hemoglobin levels, resulting in a higher risk of anemia.33 The multifactorial drivers of anemia in HIV-infected patients prior to initiation of ART require an integrated approach to help ameliorate anemia and its negative health effects while on ART.
The prevalence of leucopenia in our study (17.1%) was comparable with other studies of HIV-infected adults initiating ART in sub-Saharan Africa, ranging between 13.4% and 24.4%.20,21,26,27,34 A study from India indicated that 18.3% of HIV patients had leucopenia first at the time of presentation,35 while in the Chinese study, leucopenia was reported in 33.2% of antiretroviral-naive HIV-infected patients.36 In multivariate analysis, lower CD4+ cell count was independently associated with an increased risk of having leucopenia in HIV-infected antiretroviral-naive patients. This was consistent with other studies that have found HIV patients with low CD4+ cell count to have a higher odds of leucopenia than those with higher CD4+ cell count at the time of antiretroviral-treatment initiation.20,21,26,34,36
About 14.5% of our patients had thrombocytopenia at the time of initiation of ART. This was consistent with findings reported from Tanzania,26 China36 and India,35 where thrombocytopenia was found in 14.4%, 15.6% and 15.8% of HIV-infected adult antiretroviral-naive patients, respectively. This was; however, lower than the 18.7% prevalence reported in Northeast Ethiopia,20 and higher than 5.9% in Northwest Ethiopia37 and 8.3% in Uganda.21 These differences could be due to the difference in the study population, sample size, study design and variation in the definition of thrombocytopenia. Male sex, advanced clinical disease stage and severe immunosuppression (CD4+ cell count <200 cells/mm3) were independent predictors of having thrombocytopenia in this study. This was consistent with the Ugandan study21 that has found males to be more likely to have thrombocytopenia than females at initiation of ART. Gender-dependent difference in platelet count, being lower in males than females, could be responsible. However, some of the studies failed to find a significant relationship between sex and thrombocytopenia.20,26,36,37 This study also confirms the findings of other studies that have shown an association between advanced HIV disease (WHO clinical disease stage III/IV and CD4+ cell count <200 cells/mm3) and the presence of thrombocytopenia in HIV-infected antiretroviral-naive patients.20,21,26,35–37
More than half (53.2%) of the patients had at least one form of cytopenia (anemia and/or leucopenia and/or thrombocytopenia) in this study. In the Northeast Ethiopian study,20 the overall magnitude of any cytopenia was 63.4% among ART naive HIV-infected patients. In the Ugandan study by Kyeyune et al,21 65% of the patients had at least one form of cytopenia at initiation of ART. In the Nigerian study, 59.4% of treatment-naive HIV-infected patients had cytopenia.38 The factors independently associated with the presence of any cytopenia in this study were male sex, advanced clinical HIV disease stage, low CD4+ cell count, low BMI, and decreased renal function. The Ugandan study21 reported females were more likely to have at least one form of cytopenia than males at initiation of ART, while other studies did not show any significant association between sex and the presence of any cytopenia.20,26 Our finding is however in line with the findings of other related studies, which reported a significant association of advanced HIV infection (advanced clinical stages and low CD4+ cell counts) with the presence of any cytopenia.20,21,26 The present study revealed a significant increase in the odds of anemia with decreasing BMI, which is consistent with the Ugandan study.21 The association of decreased renal function with any cytopenia may be due to the combined effect of impaired renal function and HIV infection on cytopenia and specifically anemia in this population.33 However, no studies were available to assess the possible contribution of decreased renal function to the occurrence of cytopenia.
The limitations of this study include its cross-sectional design, which makes determination of temporal relationships between cytopenias and associated factors difficult. We did not assess the various causes of cytopenia and specifically anemia in this population. Well-controlled cohort studies would be appropriate to evaluate the potential impact of cytopenias on clinical outcomes of people living with HIV in our settings.
Conclusions
We detected a substantial burden of cytopenias (anemia, leucopenia and thrombocytopenia) among HIV-infected adult patients enrolled for care and treatment services in resource-limited setting in Ethiopia. The findings indicate that patients with HIV infection should be screened for hematological abnormalities at initiation of ART, with a special attention to be focused on males, patients with advanced disease stages, low CD4+ cell count, low BMI and low eGFR, because of its potential for morbidity and mortality during ART.
Abbreviations
AIDS, acquired immunodeficiency syndrome; AOR, adjusted odds ratio; ART, antiretroviral therapy; BMI, body mass index; CD4, cluster of differentiation; CI, confidence interval; eGFR, estimated glomerular filtration rate; HIV, human immunodeficiency virus; IQR, inter quartile range; MDRD, modification of diet in renal disease; OR, odds ratio; SD, standard deviation; WHO, World Health Organization.
Data Sharing Statement
The data of this study cannot be shared publicly due to presence of sensitive (confidential) participants’ information and additional data than that used in this publication. But the data are available from the corresponding author on reasonable request.
Ethics and Consent Statement
Ethical approval of the protocol was achieved from the Institutional Review Board of College of Medicine and Health Sciences, Wollo University. As only routine data were analyzed, informed consent was not required; but patient’s identifiers were removed and only code numbers were used throughout the study. This study was conducted in accordance with the declaration of Helsinki.
Acknowledgments
The authors acknowledge the health staff at the Mehal Meda Hospital HIV care and treatment clinic for their assistance in gathering the data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study did not receive any official funding.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Koka PS, Reddy ST. Cytopenias in HIV Infection: mechanisms and alleviation of hematopoietic inhibition. Curr HIV Res. 2004;2:275–282. doi:10.2174/1570162043351282
2. Evans RH, Scadden DT. Haematological aspects of HIV infection. Baillieres Best Pr Res Clin Haematol. 2000;13:215–230. doi:10.1053/beha.1999.0069
3. Coyle TE. Hematologic complications of human immunodeficiency virus infection and the acquired immunodeficiency syndrome. Med Clin North Am. 1997;81(2):449–470. doi:10.1016/S0025-7125(05)70526-5
4. Møller T, Hasselbalch HC. Hematological changes associated with human immunodeficiency virus (HIV-1) infection. Ugeskr Laeger. 1993;155(19):1442–1446.
5. Basu A, Ghosh K, Banerjee K. Bone marrow involvement in HIV infection: light, electron and immuno electron microscopic studies. Indian J Hematol Blood Transf. 1999;17(4):76–86.
6. Akinbami A, Oshinaike O, Adeyemo T, et al. Hematologic abnormalities in treatment-naïve HIV patients. Infect Auckl. 2010;3:
7. Enawgaw B, Alem M, Addis Z, Melku M. Determination of hematological and immunological parameters among HIV positive patients taking highly active antiretroviral treatment and treatment naïve in the antiretroviral therapy clinic of Gondar University Hospital, Gondar, Northwest Ethiopia: a comparative cross-sectional study. BMC Hematol. 2014;14(1):8. doi:10.1186/2052-1839-14-8
8. Volberding PA, Baker KR, Levine AM. Human immunodeficiency virus hematology. Hematol Am Soc Hematol Educ Program. 2003;2003:294–313.
9. Ciccacci F, Lucaroni F, Latagliata R, et al. Hematologic alterations and early mortality in a cohort of HIV positive African patients. PLoS One. 2020;15(11):e0242068. doi:10.1371/journal.pone.0242068
10. Miguez-Burbano MJ, Jackson J, Hadrigan S. Thrombocytopenia in HIV disease: clinical relevance, physiopathology and management. Curr Med Chem Cardiovasc Hematol Agents. 2005;3(4):365–376. doi:10.2174/156801605774322364
11. Durandt C, Potgieter JC, Mellet J, et al. HIV and haematopoiesis. Afr Med J. 2019;109(8b):40–45. doi:10.7196/SAMJ.2019.v109i8b.13829
12. Johannessen A, Naman E, Ngowi BJ, et al. Predictors of mortality in HIV-infected patients starting antiretroviral therapy in a rural hospital in Tanzania. BMC Infect Dis. 2008;8:52. doi:10.1186/1471-2334-8-52
13. Anastos K, Shi Q, French A, et al. Total lymphocyte count, hemoglobin, and delayed-type hypersensitivity as predictors of death and AIDS illness in HIV-1-infected women receiving highly active antiretroviral therapy. J Acquir Immune Defic Syndr. 2004;35(4):383–392. doi:10.1097/00126334-200404010-00008
14. Ezeamama AE, Guwatudde D, Sikorskii A, et al. Impaired hematologic status in relation to clinical outcomes among HIV-infected adults from Uganda: a prospective cohort study. Nutrients. 2018;10(4):475. doi:10.3390/nu10040475
15. Volberding PA, Levine AM, Dieterich D, et al. Anemia in HIV infection: clinical impact and evidence-based management strategies. Clin Infect Dis. 2004;38(10):1454–1463. doi:10.1086/383031
16. Belperio PS, Rhew DC. Prevalence and outcomes of anemia in individuals with human immunodeficiency virus: a systematic review of the literature. Am J Med. 2004;116(Suppl 7A):27S–43S. doi:10.1016/j.amjmed.2003.12.010
17. Noor RA, Abioye AI, Hertzmark E, et al. Impaired hematological status increases the risk of mortality among HIV-infected adults initiating antiretroviral therapy in Tanzania. J Nutr. 2020;150(9):2375–2382. doi:10.1093/jn/nxaa172
18. Redig AJ, Berliner N. Pathogenesis and clinical implications of HIV-related anemia in 2013. Hematology. 2013;2013(1):377–381. doi:10.1182/asheducation-2013.1.377
19. Subbaraman R, Devaleenal B, Selvamuthu P, et al. Factors associated with anaemia in HIV-infected individuals in southern India. Int J STD AIDS. 2009;20(7):489–492. doi:10.1258/ijsa.2008.008370
20. Tamir Z, Seid A, Haileslassie H. Magnitude and associated factors of cytopenias among antiretroviral therapy naïve human immunodeficiency virus infected adults in Dessie, Northeast Ethiopia. PLoS One. 2019;14(2):e0211708. doi:10.1371/journal.pone.0211708
21. Kyeyune R, Saathoff E, Ezeamama AE, Löscher T, Fawzi W, Guwatudde D. Prevalence and correlates of cytopenias in HIV-infected adults initiating highly active antiretroviral therapy in Uganda. BMC Infect Dis. 2014;14:496. doi:10.1186/1471-2334-14-496
22. Getawa S, Aynalem M, Bayleyegn B, Adane T. The global prevalence of thrombocytopenia among HIV-infected adults: a systematic review and meta-analysis. Int J Infect Dis. 2021;105:495–504. doi:10.1016/j.ijid.2021.02.118
23. Anude CJ, Eze E, Onyegbutulem HC, et al. Immuno-virologic outcomes and immunovirologic discordance among adults alive and on anti-retroviral therapy at 12 months in Nigeria. BMC Infect Dis. 2013;13:113. doi:10.1186/1471-2334-13-113
24. Levey A, Greene T, Kusek J, Beck G. A simplified equation to predict glomerular filtration rate from serum creatinine. J Am Soc Nephrol. 2000;11:A0828.
25. World Health Organization. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity; [cited July 25, 2021]. Available from: https://apps.who.int/iris/handle/10665/85839.
26. Gunda DW, Godfrey KG, Kilonzo SB, Mpondo BC. Cytopenias among ART-naive patients with advanced HIV disease on enrolment to care and treatment services at a tertiary hospital in Tanzania: a cross-sectional study. Malawi Med J. 2017;29(1):43–52. doi:10.4314/mmj.v29i1.9
27. Fekene TE, Juhar LH, Mengesha CH, Worku DK. Prevalence of cytopenias in both HAART and HAART naïve HIV infected adult patients in Ethiopia: a cross sectional study. BMC Hematol. 2018;18:8. doi:10.1186/s12878-018-0102-7
28. Marchionatti A, Parisi MM, Bygbjerg IC. Anemia and thrombocytopenia in people living with HIV/AIDS: a narrative literature review. Int Health. 2020;12:1–12. doi:10.1093/inthealth/ihz011
29. Firnhaber C, Smeaton L, Saukila N, et al. Comparisons of anemia, thrombocytopenia, and neutropenia at initiation of HIV antiretroviral therapy in Africa, Asia, and the Americas. Int J Infect Dis. 2010;14(12):e1088–92. doi:10.1016/j.ijid.2010.08.002
30. Woldeamanuel GG, Wondimu DH. Prevalence of anemia before and after initiation of antiretroviral therapy among HIV infected patients at Black Lion Specialized Hospital, Addis Ababa, Ethiopia: a cross sectional study. BMC Hematol. 2018;18:7. doi:10.1186/s12878-018-0099-y
31. Negesse A, Getaneh T, Temesgen H, Taddege T, Jara D, Abebaw Z. Prevalence of anemia and its associated factors in human immuno deficiency virus infected adult individuals in Ethiopia. A systematic review and meta-analysis . BMC Hematol. 2018;18:32. doi:10.1186/s12878-018-0127-y
32. Fiseha T, Tamir Z, Seid A, Demsiss W. Prevalence of anemia in renal insufficiency among HIV infected patients initiating ART at a hospital in Northeast Ethiopia. BMC Hematol. 2017;17:1. doi:10.1186/s12878-017-0071-2
33. Abraham AG, Palella FJ, Li X, et al. The impact of impaired kidney function and HIV infection on the risk of anemia. AIDS Res Hum Retroviruses. 2012;28(12):1666–1671. doi:10.1089/aid.2011.0188
34. Talargia F, Teshome Y, Aynalem YA, Asefa A. Prevalence of leucopenia and associated factors before and after initiation of ART among HIV-infected patients, North East Ethiopia: cross-sectional study. J Blood Med. 2021;12:269–276. doi:10.2147/JBM.S306369
35. Bhardwaj S, Almaeen A, Wani FA, Thirunavukkarasu A. Hematologic derangements in HIV/AIDS patients and their relationship with the CD4 counts: a cross-sectional study. Int J Clin Exp Pathol. 2020;13(4):756–763.
36. Shen Y, Wang J, Wang Z, et al. A cross-sectional study of leukopenia and thrombocytopenia among Chinese adults with newly diagnosed HIV/AIDS. Biosci Trends. 2015;9(2):91–96. doi:10.5582/bst.2015.01024
37. Wondimeneh Y, Muluye D, Ferede G. Prevalence and associated factors of thrombocytopenia among HAART naive HIV positive patients at Gondar university hospital, northwest Ethiopia. BMC Res Notes. 2014;7(5). doi:10.1186/1756-0500-7-5
38. Denue BA, Gashau W, Bello HS, Kida IM, Bakki B, Ajayi B. Relation between some haematological abnormalities, degree of immunosuppression and viral load in treatment-naïve HIV-infected patients. East Mediterr Health J. 2013;19(4):362–368. doi:10.26719/2013.19.4.362
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.