")
Back to Journals » Open Access Journal of Contraception » Volume 12
Prevalence and Predictors of Contraceptive Use Among Women of Premenopausal Period in Ethiopia: A Retrospective Cross-Sectional Data Analysis
Authors Geleta D , Kebede A, Bulcha G, Usman H , Hajibediru K, kebede S , Dubale S , Degu G
Received 6 May 2021
Accepted for publication 13 July 2021
Published 27 July 2021 Volume 2021:12 Pages 149—156
DOI https://doi.org/10.2147/OAJC.S318486
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Daniel Geleta,1 Abebe Kebede,2 Gebeyehu Bulcha,3 Hyder Usman,2 Kunuz Hajibediru,4 Selass kebede,2 Sileshi Dubale,2 Getu Degu5
1Tropical & Infectious Diseases, Jimma University, Jimma, Oromia, Ethiopia; 2Pharmaceutical science, Jimma University, Jimma, Oromia, Ethiopia; 3Health Communication and Health Behavior, Jimma University, Oromia, Ethiopia; 4Reproductive Health,Jimma University, Jimma, Oromia, Ethiopia; 5Epidemiology and Biostatistics, Bahir Dar University, Bahir Dar, Amhara, Ethiopia
Correspondence: Daniel Geleta P.O.Box: 378 Tel +125 911723400
Fax +251 471111450
; +251 471112040
Email [email protected]
Background: Contraceptive use is internationally endorsed as a human right and an indicator of the highest standard of sexual and reproductive health life. But reports from countries including Ethiopia showed a lower and capricious rate due to wider factors. Thus, the current study aimed to determine the prevalence and the predictors of contraceptive use among women of the premenopausal period.
Methods: A retrospective cross-sectional data analysis was performed from Ethiopian Demographic and Health survey 2019 in January 2021. A total of 3260 premenopausal women were included by stratified sampling, and data were analyzed using SPSS version 25 software. Data were initially analyzed descriptively, and tests were done for variable multicollinearity, and model goodness of fit and predictive capacity. Subsequently, bivariate and multivariable logistic regression analyses were performed successively for the crude and adjusted odds ratio, and finally declared variables with a p-value of < 0.05 as predictors of contraceptive use.
Results: The study included 3260 women with an average age of 41.66 (standard deviation ± 3.9) years. The overall prevalence of contraceptive use was reported 17% and explained to vary by women’s age, place of residence, education level, wealth index, and current working statuses. However, only the age, education, and wealth index of women have predicted a statistical significance with contraceptive use. Accordingly, an increase in women’s age was found to increase contraceptive use more likely by 89% [AOR=0.89 (95% CI: 0.87, 0.92)]. Similarly, primary [AOR = 1.53, (95% CI: 1.20, 195)], secondary [AOR = 2.57, (95% CI: 1.70)] or higher [AOR = 2.64, (95% CI: 1.67, 4.20)] level educated women were about twice more likely to use contraceptive methods than uneducated women. Finally, women in poorer [AOR = 3.11 (95% CI: 2.17, 4.46)], middle [AOR = 3.03 (95% CI: 2.09, 4, 37)], rich [AOR = 3.70, (95% CI: 2.58, 5.31)] or richest [AOR = 3.42, (95% CI: 2.39, 4, 88)] wealth index were more than 3 times more likely use contraceptive methods when compared to women of the poorest wealth index.
Conclusion: The prevalence of contraceptive use among premenopausal women in Ethiopia is low and utmost related to age, education level, and wealth index of women.
Keywords: contraceptive, predictors, premenopausal, prevalence, women
Introduction
Contraceptive is the intentional prevention of conception and related risks through the use of modern or traditional methods to optimize the health of women, children, and families. Contraceptive use is a proven strategy to minimize virtually 230 million births every year, 44% of maternal mortality, and prevent 75% of unwanted pregnancies and unsafe abortions. It also carries a principal role to promote gender equality, educational and economic empowerment of women, and reduction of poverty and hunger.1–8 Contraceptive use is also an indicator of health, population, development, and women’s empowerment beyond its proxy measure of access to reproductive health services. Consequently, the World Health Organization (WHO) recommends contraceptive use as a human right and selects practices on how to use contraceptives safely and effectively to attain the highest standard of sexual and reproductive health.9–11 Despite its proven principal importance, contraceptive use among reproductive-age women varies and has not reached its optimal target. Particularly, the level of contraceptive use among an average age group of 35–49 year women that literary named premenopausal period was neglected in low- and middle-income countries.12,13 Although the contribution of the neglected age to low contraceptive use, the global level of contraceptive use exceeded 58%, while it was reported 32% in Africa and 37% in Ethiopia. The current position of Ethiopia in contraceptive use has been considered a fascinating progress,14 though the rate of utilization characteristically varies among different regions of the country as well as women’s age group. Accordingly, previous studies revealed that the contraceptive prevalence rate of the regions (local political administrative divisions) in Ethiopia ranges from 3.4% to 50%.15 On the other hands, the rate of contraceptive use was not uniform across women age group with account of 37% among 15–19, 52% in 20–24 and 18% in 45–49 years due to several factors.1–3
The factors that influence contraceptive use are multifaceted and arduous; however, majority of the factors are related to socio-demographic, socio-economic, and awareness prestige of an individual women.16 Accordingly, the disparity of contraceptive use has been reported among age groups, place of residence, level of education in different countries17–20 like Kenya.19,21,22 Further, a longer female education enhances the participation of women in the workforce and emboldens them to potentially delay motherhood.23 Study reports also revealed high fertility as the manifestation of inequality in wealth distribution, and the problem is higher in sub-Saharan Africa.24,25 Subsequently, the prevalence of contraceptive use among women in the richest wealth quartile was higher (82.4%) than the women with the poorest wealth index (66.8%). Women within the richest wealth quartile were more likely to the contraceptive methods26 with a similar utilization gap been being reported between the highest (52%) and lowest wealth quintiles (35%).27 Finally, the work status of the women was reported to influence contraceptive use. According to previous studies, women who work outside and earn cash income have shown high contraceptive use tendencies than their counterparts.17,28 On the other hand, different studies showed that hearing a contraceptive message on the radio has no association with contraceptive uses among women including Ethiopians.29,30 For these several reasons, the government holds the valued principle of equitable access to safe, effective, and affordable contraception services across the country though the contraceptive utilization prevalence rate remains low and frequently changing.31
Finally, most studies done so far were focused on modern contraceptive methods and crude reproductive age groups; as a result, a lack of studies existed about contraceptive use of premenopausal age groups particularly in Ethiopia. So, this study aimed to determine the prevalence and the predictors of contraceptive use among women of premenopausal age in the study area using the following conceptual framework as a flow guide in Figure 1.
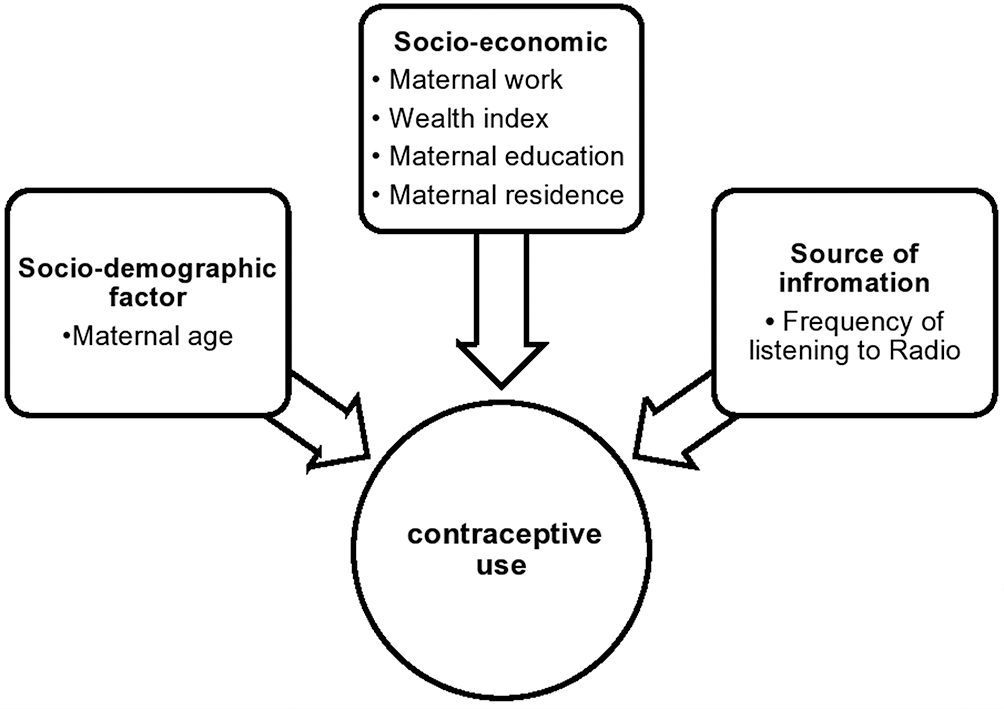 |
Figure 1 Conceptual framework of reviewed literature for predictors of contraceptive use among premenopausal women in Ethiopia, January 2021. |
Methods
Setting and Design Description
A retrospective cross-sectional study was conducted in Ethiopia, one of the countries in the Horn of Africa, based on secondary data that extracted from the Ethiopian Demographic and Health survey 2019 (EDHS-2019). Total women of reproductive age group were considered as a source population and women of premenopausal period were taken as a study population. A two-stage stratified sampling technique was use for the selection of the study subjects. Each division was stratified into 305 enumeration areas (93 urban and 212 rural) each containing 131 households that were selected with probability proportional to enumeration area size (based on the 2019 primary health care frame), and with independent selection in each sampling stratum. At the second stage from the sampling frame of households under selected enumeration areas, a fixed number of 30 households per cluster were selected with an equal probability of systematic selection. A total of 3260 women of reproductive age of 35–49 years who were either permanent residents of the selected households or visitors who slept in the household the night before the survey were selected and included using a women’s questionnaire from January 19–25, 2020.32
Variables Under the Study
The EDHS was delineated with a lot of variables; however, the current study was purposely designed to analyze the relation of one dependent and six independent variables. The dependent variable is one categorical outcome variable (contraceptive use) and dichotomized with responses of not using any method (coded 0) and using methods (coded 1). Whereas a continuous variable (maternal age) and five categorical explanatory variables (residence, maternal education, maternal work, frequency of listening to the radio, and wealth index) were assumed to predict contraceptive use among women of the premenopausal period. Each categorical data were given different codes. Accordingly, the residence was coded as urban (coded 1) and rural (coded 2) residents, maternal education labeled as no education (coded 0), primary (coded 1), secondary (coded 2), and higher (coded3). Maternal work coded as currently working (coded 0) and not currently working (coded 1). Likewise, the frequency of listening to the radio was categorized into not at all (coded 0), less than once a week (coded 2), and at least once a week (coded 2). A wealth index also similarly classified as poorest (coded 0), poorer (coded 1), middle (coded 2), rich (coded 4) and richest (coded 5) and respondent currently working was categorized as no (coded 0) and yes (coded 1).
Data Analysis
To build predictors of contraceptive use, the extracted data were entered into the Statistical Package for Social Sciences (SPSS) version-25-software, and data were descriptively analyzed to have an insight into the data. After a clear understanding of the data, we have checked the variables for multicollinearity using the variance inflation factor (VIF) in linear logistic regression that assumes VIF <10/tolerance >0.1 to have no multi-collinearity. For this particular dataset multicollinearity was ruled-out with VIF <2.1/tolerance >0.45. We have also checked for the Goodness of Fit and explanation capacity for the model using the Hosmer and Lemeshow test that assumes a good fit for p-value >0.05, and the receiver operating character curve (ROC Curve), respectively. Accordingly, the model demonstrated a p-value of 0.48, and the receiver operating character curve laid above the 45-degree diagonal line indicating the reasonable goodness of fit and predictive power of the variables in respective order.
After confirmation of the fulfillment of assumptions and variable discrimination power, the logistic regression method was applied to identify the predictors of contraceptive use. During the application of the regression, a sequential bivariate analysis was performed to determine the crude association of each covariate variable with the outcome variable at a p-value of below 0.20. The variables in bivariate analysis with a p-value less than 0.20 were simultaneously included in the multivariable forward logistic regression procedure to control the confounding variables and describe the final determinants of contraceptive use among women of the premenopausal period. During the process of the outcome measurements, odds ratio with a 95% confidence interval was used to indicate an association. Finally, covariate variables with a p-value of <0.05 in the multivariable logistic regression model were considered as statistically significant predictors of contraceptive use.
Results
Socio-Demographic and Other Characteristics of the Participant Women
A total of 3260 women were participated in the study, with an average age of 41.66 years (standard deviation ± 3.9). About 25.5% of the participants were constituted by urban and 74.5% rural residents. Educationally, 73.7% of participants have no education at all where the remaining proportion was complemented with 8.5% primary, 4.5% secondary, and 3.3% higher levels. More than half of women (54.4%) did not listen to the radio at all, while 28.2% used to listen less than once a week and 17.5% listened at least once a week during the study. The respondents’ wealth index was analyzed and revealed 26% being in the poorest, 19.6% in poorer, 15.4% in the middle, 15.4% in richer, and 26.3% in the richest category. About 61% of the women were not working during the study unlike 38.9% of their counterparts who were working during the study period as indicated in Table 1.
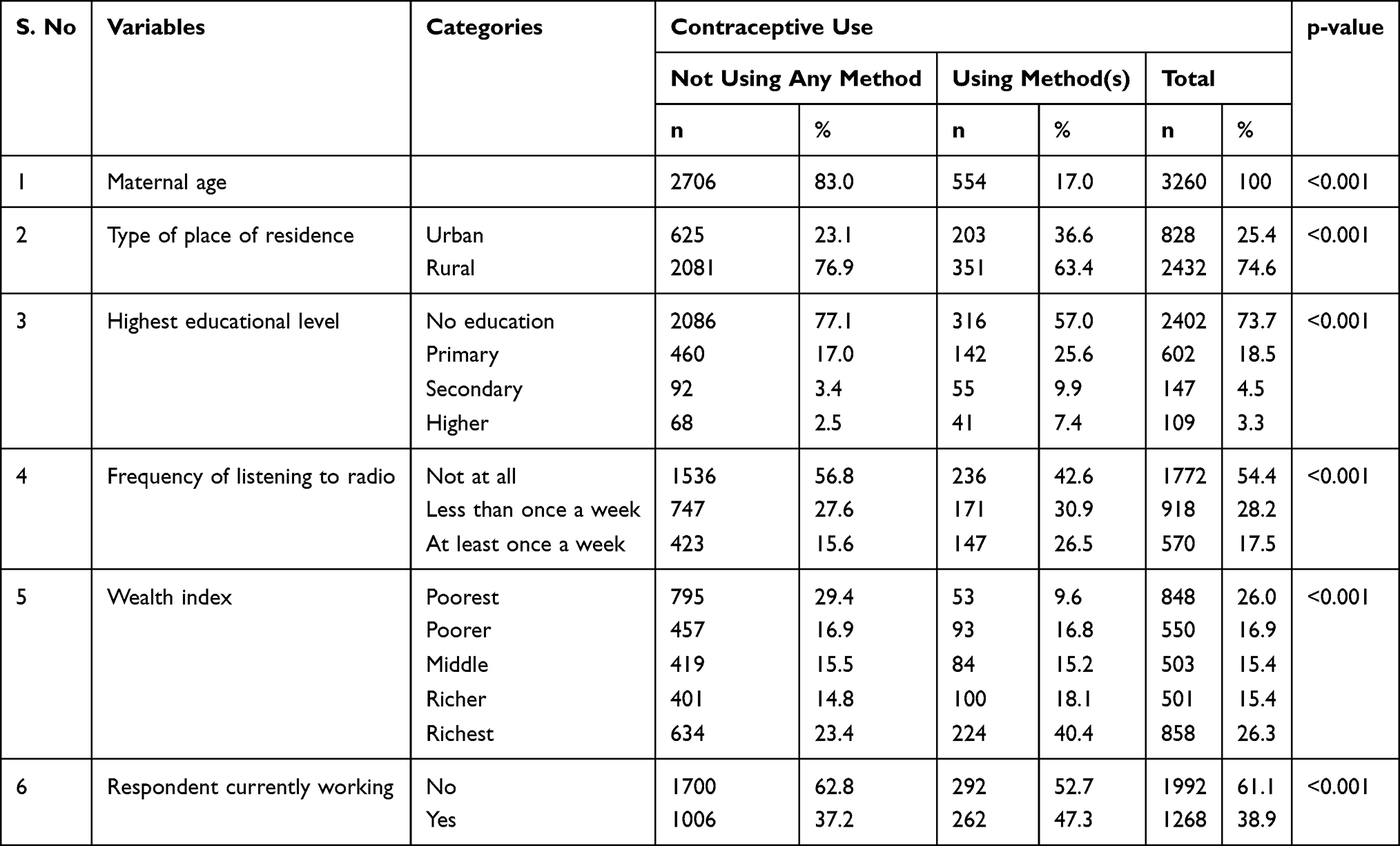 |
Table 1 The Characteristics of the Study Participants (N=3260) in Ethiopia, EDHS- 2019 |
Contraceptive Utilization by Women Characteristics
The contraceptive use varies by the age (p-value=<.001) of women with the overall prevalence being 17%. The prevalence of contraceptive users contributed by different places of residents even though it varies across settings (p-value=<.001) indicating 36.6% urban and 63.4% rural users. It also varies by education (p-value=<.001), where the most (57%) contraceptive users were uneducated women followed by women of primary level (25.6%) with women of higher education level being the least (7.4%) users of contraceptive methods. The variation is also related to listening to the radio (p-value=<.001) in which women who did not listen to the radio at all used contraceptive methods (42.6%) more than both women who listen to the radio at least once a week (30.9%) and less than once a week (26.5%). It was also noted that women of the richest wealth index (40.4%) found to be more contraceptive utilizers as compared to women of rich, middle, poorer, or poorest wealth index who reported their contraceptive use being 18.1%, 15.2%, and 16.8%, respectively (p-value=<.001). Finally, work was found a reason for variation (p-value=<.001) in which women who have no work (52.7%) during the study were identified to use a contraceptive method more than those women who have been working during the study period (47.3%) as indicated in Table 1. To explore the significance of the associations obtained in cross-tabulation, we further performed a logistic regression model.
Factors Associated with Contraceptive Use
Six variables selected from socio-demographic, socio-economic, and source of information were independently entered into bivariable logistic regression analysis using an enter procedure, and all of them were demonstrated in association with the independent variable at p-value <0.20. Specifically, maternal age (p-value=<.001), place of residence (p-value=<.001), educational level (p-value=<.001), listening the radio (p-value=<.001), wealth index (p-value=<.001) and current working status (p-value=<.001) were associated with the independent variable as in Table 2. Subsequently, variables that show an association to the dependent variable at the bivariate level were simultaneously adjusted to the binary logistic regression, and finally maternal age (p-value=<.001), an education level (p-value=<.001), and wealth index (p-value=<.001) experienced an association with contraceptive use. From the final model of Table 2, then, a one-year increase in maternal age was found to increase a contraceptive use more likely by 89% [AOR=0.89, (95% CI: 0.87, 0.92)]. The women of primary education level were found to use a contraceptive method 1.53 times [AOR= 1.53, (95% CI: 1.20, 195)] more likely than the women with no education level. Similarly, the women who attained secondary education level were 2.57 times [AOR=2.57, (95% CI: 1.70, 3.89)] more likely to use contraceptive methods than women of no education level. The result also showed that contraceptive utilization increases by 64% [AOR=2.64, (95% CI: 1.67, 4.20)] more likely among women who attained higher education as compared to women with no education. Finally, the study identified that women of poorer wealth index were 3.11 times [AOR=3.11 (95% CI: 2.17, 4.46)] more likely to use contraceptive methods as compared to those women who were in the poorest wealth index. The women among middle wealth index were found to be 3.03 times [AOR=3.03 (95% CI: 2.09, 4.37)] more likely to use contraceptive methods as compared to those women of the poorest wealth index. When compared with the women of the poorest wealth index, the women with rich wealth index were showed 3.70 times [AOR=3.70, (95% CI: 2.58, 5.31)] more tendencies to use contraceptive methods. Lastly, the women of the richest wealth index were identified to have 3.42 times [AOR=3.42, (95% CI: 2.39, 4.88)] higher likelihood of contraceptive use as compared to the women of the poorest wealth index in Table 2. As it can be noted from Table 2 again, the observed association between predicting factors and contraceptive use is statistically significant. Whereas place of residence, radio listening, and current work status were identified as they have no associations with contraceptive use and therefore, excluded from the model.
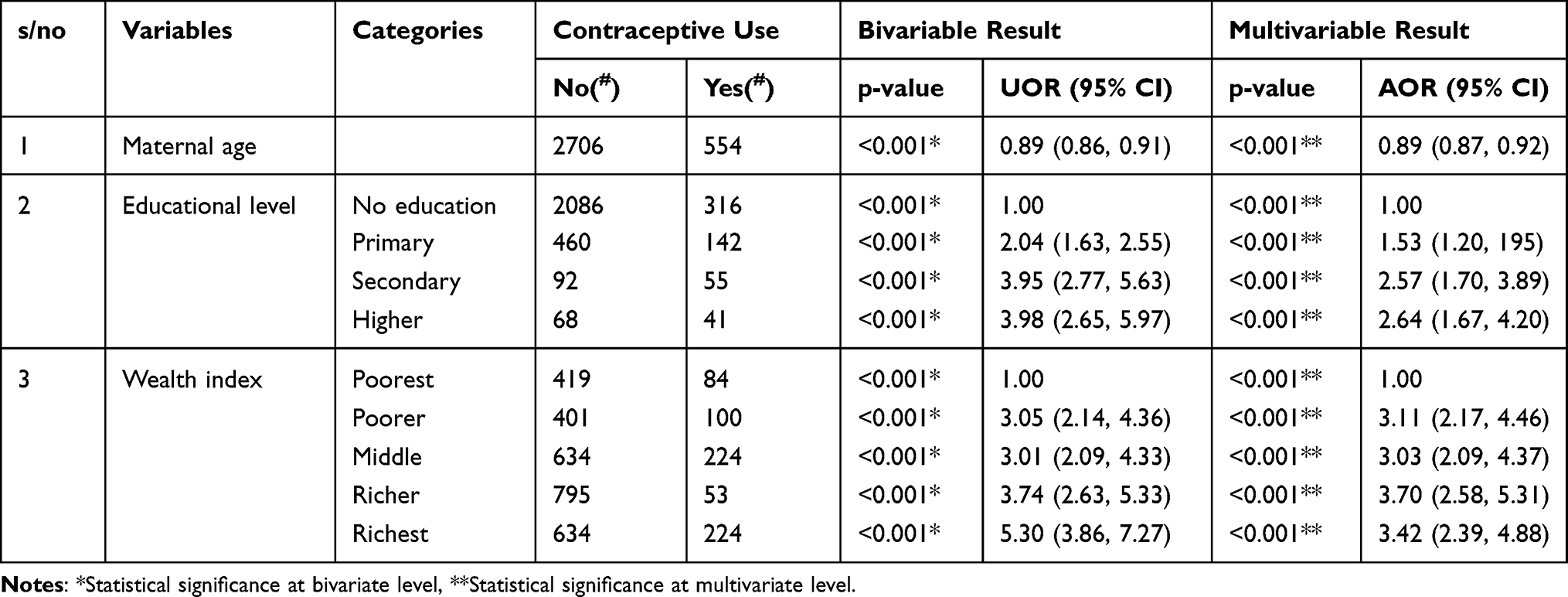 |
Table 2 Predictors of Contraceptive Use Among Women of Premenopausal Period in Ethiopia, EDHS-2019 |
Discussion
According to the current analysis, the prevalence of contraceptive use among premenopausal women was low (17%) in Ethiopia. This result is lower as compared to many African countries where the overall percentage was 26%.11 It is also lower than the prevalence rate in countries like Uganda 29%,31 and Kenya 42.6%,32 and another similar studies in Ethiopia 42%.29 However, the result is consistent with the study result in Gambia 17%.11 The principal reason for the variation might be the variation of culture, some relax their norms and cultures, across countries and age- related conditions of women including infrequent sexual relation. Moreover, as the premenopausal age is a transition phase from younger to the menopausal stage in women’s menstrual chronological age, an age-related side effect of hormonal contraceptives noticeably affects contraceptive use. In the premenopausal period, the level of estrogen fluctuates; causing irregular menstrual bleeding that further synergizes minor bleeding from hormonal contraceptive use. Likewise, the decline in estrogen during the premenopausal period decreases the secretion of lubricants in female genitalia, producing dryness and painful coitus. This coincident effect of contraceptives and hormonal fluctuation during the premenopausal period perplexes the perception of women and some health workers against the contraceptive use. In such circumstance, women of premenopausal stage preferred to exempt contraceptive, and consequently accounted for low contraceptive use.33,34
The current study also identified three statistically significant factors to that influence contraceptive use.35 First, the age of women was identified as one of the predictors for contraceptive use, where the tendency of utilization increases with age. This study agrees with the study conducted in Bangladesh but contradicts with another study conducted in Ethiopia.13,14 But the reason for the increase of utilization with age could be because of older women were having more children and have more desire to limit or space the number of pregnancies than younger who had none or few children.
Secondly, the level of maternal education is positively associated independent predictors, henceforth women of primary education [AOR= 1.53, (95% CI: 1.20, 195)], secondary education [AOR= 1.53, (95% CI: 1.20, 1.95)] and higher education [AOR=2.57, (95% CI: 1.70, 3.89)] are more likely to utilize contraceptive methods than women of no education. Our finding fortifies those of antecedent studies. Findings from across the developing world show that the better educated a woman is, the more likely she is to utilize contraception.18,19 A study conducted in Kenya showed that maternal education was found to be significantly associated with contraceptive use.20 This denotes that, female education enhances the participation of women in the workforce, and women’s autonomous decision and economic potentiation, which in turn likely emboldening them to control their fertility and additionally delaying motherhood.35
Thirdly, wealth index is another consequential positively associated predictor for contraceptive utilization as depicted by the study. Based on the result for instance, women of poorer wealth index [AOR=3.11 (95% CI: 2.17, 4.46)], middle wealth index [AOR=3.03 (95% CI: 2.09, 4.37)], rich wealth index [AOR=3.70, (95% CI: 2.58, 5.31)] and richest wealth index [AOR=3.42, (95% CI: 2.39, 4.88)] were more liable to utilize contraceptive as compared to those women of the poorest wealth index. This finding in line with previous studies, that revealed inequality in wealth distribution is manifested by high fertility, the quandary is high in sub-Saharan Africa.22,23 Adebowale et al also found that the prevalence of ever utilization of contraceptives was higher among women in the richest wealth quartile (82.4%) than the poorest (66.8%). Women within the richest wealth quartile were more liable to ever use and currently utilizing the contraceptive, a wide gap has been visually perceived between the highest (52%) and lowest wealth quintiles (35%).24,25 This is justified as women potentiation through economic independence leads to autonomous decision-making over family affairs, which in turn leads to better contraceptive utilization and fertility control.
Limitations of the Study
Even though the study targeted a neglected age group with respect to contraceptive use and deployed a rigorous statistical analysis, it has certain inherent limitations. First, the EDHS data used a 2 weeks’ time preceding the survey, hence, may not be a vast representative. Secondly, as there were limited previous studies on the premenopausal period, some current study results were compared with the women of the reproductive age group. Thirdly, some factors such as the impact of partner on contraceptive use, degree of contraceptive side effects, perceptions of the women were not predicted because of the nature of secondary data use.
Conclusion and Recommendations
On top of determining contraceptive use prevalence, our study performed a logistical regression model to predict the association between selective independent variables and outcome variables (contraceptive use) for premenopausal women. The model predicted that the predictors are positively related and statistically significant with the outcome variable. Noticeably, the age of women was identified to increase with contraceptive use, while the prevalence among higher age was distinguished lower than the expected country project needing an improvement. Subsequently, the lower prevalence of contraceptive use in Ethiopia could be due to the role of the different predictors including women’s age, education, and wealth index as recognized by the current study result. Therefore, to increase the prevalence of contraceptive use in the country, integration of contraceptive service with other health services and diversification of family planning delivery modalities would be necessary with a special focus on entire age, the advancement of education, and the wealth index of women.
Abbreviations
AOR, adjusted odd ratio; CI, confidence interval; DHS, Demographic Health Survey; WHO, World Health Organization.
Data Sharing Statement
Data for this study were sourced from Demographic and Health surveys (DHS) and are available publicly.
Ethical Issues
The procedure for the 2019 EDHS was approved by the Institutional Review Board and the National Review Committee at the Ministry of Science and Technology. The authors obtained permission from the EDS program to download and analyze the data for the current paper.
Acknowledgments
The authors thank the MEASURE DHS project for their support and for free access to the original data.
Author Contributions
All authors (AK, DG, GB, HU, KH, SK, SD and GD) contributed to conceptualization, the study design, literature review, data analysis and drafted the first version of this paper. They have critically reviewed the manuscript for its intellectual content and agreed accountable for integrity of the work. Finally, all authors read and approved the final version for publication, and delegated DG as a contact author for submission and further communication.
Disclosure
The authors declare that there are no competing interests in this work.
References
1. Bevir M, Hurt SR. World development indicators; 2012. doi:10.4135/9781412952613.n571.
2. Cleland J, Bernstein S, Ezeh A, Faundes A, Glasier A, Innis J. Family planning: the unfinished agenda. Lancet. 2006;368(9549):1810–1827. doi:10.1016/S0140-6736(06)69480-4
3. Darroch JE, Singh S, Nadeau J. Contraception: an investment in lives, health and development. Issues Brief. 2008;(5):1–4.
4. Tsui AO, McDonald-Mosley R, Burke AE. Family planning and the burden of unintended pregnancies. Epidemiol Rev. 2010;32(1):152–174. doi:10.1093/epirev/mxq012
5. Haub C, Kent MM. 2009 World population data sheet; 2009:1–19.
6. Arquitectura EY, Introducci TI, Iv T. World population prospects; The 2015 revision. Key findings and advance tables. Acta Univ Agric et Silvic Mendelianae Brun. 2015;53(9):1689–1699.
7. Ayele W, Tesfaye H, Gebreyes R, Gebreselassie T. Trends and determinants of unmet need for family planning and programme options, Ethiopia. Further analysis of the 2000, 2005, and 2011 demographic and health surveys. J Chem Inf Model. 2013;1–32.
8. Cleland J, Conde-Agudelo A, Peterson H, Ross J, Tsui A. Contraception and health. Lancet. 2012;380(9837):149–156. doi:10.1016/S0140-6736(12)60609-6
9. WHO. A Guide to Family Planning for Community Health Workers and Their Clients.; 2014. http://apps.who.int/iris/bitstream/10665/44882/1/9789241503754_eng.pdf.
10. World Health Organization (WHO). 2014. Ensuring Human Rights in the Provision of Contraceptive Information and Services: Guidance and Recommendations. Luxembourg: WHO. Retrieved from http://www.who.int/reproductivehealth/publications/family_planning/huma.
11. Apanga PA, Kumbeni MT, Ayamga EA, Ulanja MB, Akparibo R. Prevalence and factors associated with modern contraceptive use among women of reproductive age in 20 African countries: a large population-based study. BMJ Open. 2020;10(9):e041103. doi:10.1136/bmjopen-2020-041103
12. Ethiopian Public Health Institute (EPHI) [Ethiopia] and ICF. 2019. Ethiopia Mini Demographic and Health Survey 2019: Key Indicators. Rockville, Maryland, USA: EPHI and ICF.https://www.unicef.org/ethiopia/reports/2019-ethiopia-mini-demographic-and-health-survey
13. Leone T. Women’s mid-life health in low and middle income Countries: a comparative analysis of the timing and speed of health deterioration in six countries. SSM Popul Health. 2018;7:100341. doi:10.1016/j.ssmph.2018.100341
14. FMOH. National Guideline for Family Planning Services In Ethiopia Third Edition. 2020;(July):15-18.
15. Edossa ZK, Debela TF, Mizana BA. Women’s Decision on Contraceptive Use in Ethiopia: Multinomial Analysis of Evidence From Ethiopian Demographic and Health Survey. Health Serv Res Manag Epidemiol. 2020;7:2333392820924565. doi:10.1177/2333392820924565.
16. Feyisetan BJ. Spousal communication and contraceptive use among the Yoruba of Nigeria. Popul Res Policy Rev. 2000;19(1):29–45. doi:10.1023/A:1006388011947
17. Dennis PH, Berhanu B, Hailemariam A. Household organization, women`s autonomy, and contraceptive behavior in Southern Ethiopia. Stud Fam Plann. 1999;30(4):302–314. doi:10.1111/j.1728-4465.1999.t01-2-.x
18. Kwale C, Together T. Kwale county integrated development plan (2018–2022); 2022 (June 2018).
19. Mochache V, Lakhani A, El-Busaidy H, Temmerman M, Gichangi P. Pattern and determinants of contraceptive usage among women of reproductive age from the Digo community residing in Kwale, Kenya: results from a cross-sectional household survey. BMC Women's Health. 2018;18(1):1–11. doi:10.1186/s12905-017-0497-5
20. Curtis SL, Neitzel K. Contraceptive knowledge, use, and sources [Internet]. DHS Comparative Studies No. 19. 1996. Available from: http://dhsprogram.com/pubs/pdf/CS19/CS19.pdf.
21. Ainsworth M, Beegle K, Nyamete A. The impact of women’s schooling on fertility and contraceptive use: a study of fourteen Sub-Saharan African countries. World Bank Econ Rev. 1996;10(1):85–122. doi:10.1093/wber/10.1.85
22. Rutenburg N, Ayad M, Ochoa LH, Wilkinson M. Knowledge and use of contraception. Demographic and Health Surveys Comparative Studies No. 6. Institute for Resource Development, New York. 1991.]
23. Koch E, Calhoun B, Aracena P, Gatica S, Bravo M. Women’s education level, contraceptive use and maternal mortality estimates. Public Health. 2014;128(4):384–387. doi:10.1016/j.puhe.2014.01.008
24. Spinelli A, Lauria L. Patterns of contraceptive use in 5 European countries. European Study Group on infertility and subfecundity. Am J Public Health. 2000;90(9):1403–1408. doi:10.2105/ajph.90.9.1403
25. Skouby SO. Contraceptive use and behavior in the 21st century: a comprehensive study across five European countries. Eur J Contracept Reprod Health Care. 2004;9(2):57–68. doi:10.1080/13625180410001715681
26. Adebowale SA, Adedini SA, Ibisomi LD, Palamuleni ME. Differential effect of wealth quintile on modern contraceptive use and fertility: evidence from Malawian women. BMC Women's Health. 2014;14(1). doi:10.1186/1472-6874-14-40
27. Creanga AA, Gillespie D, Karklins S, Tsui AO. Faible recours à la contraception chez les femmes africaines pauvres: une question d’égalité. Bull World Health Organ. 2011;89(4):258–266. doi:10.2471/BLT.10.083329
28. Gage AJ. Women’s socioeconomic position and contraceptive behavior in Togo. Stud Fam Plann. 1995;26(5):264–277. doi:10.2307/2138012
29. Ahmed M, Seid A. Association between exposure to mass media family planning messages and utilization of modern contraceptive among urban and rural youth women in ethiopia. Int J Womens Health. 2020;12(December):719–729. doi:10.2147/IJWH.S266755
30. Habibov N, Zainiddinov H. Effect of TV and radio family planning messages on the probability of modern contraception utilization in post-Soviet Central Asia. Int J Health Plan Manag. 2017;32(1):e17–e38. doi:10.1002/hpm.2318
31. A. Korra, Attitudes towards family planning and reasons for nonuse among women with unmet need for family planning in Ethiopia. DHS Further Analysis Reports No. 40 (2002) (available at http://dhsprogram.com/pubs/pdf/FA40/FA40.pdf)
32. CSA. Ethiopia Mini Demographic and Health Survey; 2014.
33. Perimenopause: rocky road to menopause. Symptoms we call “menopausal“ often precede menopause by years. Harv Womens Health Watch. 2005 Aug; 12(12):1-4. PMID:16206381.https://read.qxmd.com/read/16206381/perimenopause-rocky-road-to-menopause-symptoms-we-call-menopausal-often-precede-menopause-by-years.
34. Bakour SH, Hatti A, Whalen S. Contraceptive methods and issues around the menopause: an evidence update. Obstet Gynecol. 2017;19(4):289–297. doi:10.1111/tog.12416
35. Ahmed S, Li Q, Liu L, Tsui AO. Maternal deaths averted by contraceptive use: an analysis of 172 countries. Lancet. 2012 Jul 14;380(9837):111-25. doi:10.1016/S0140-6736(12)60478-4. Epub 2012 Jul 10. PMID: 22784531.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.