Back to Archived Journals » Open Access Surgery » Volume 15
Prevalence and Factors Associated with Postoperative Pain After Cesarean Section at a Comprehensive Specialized Hospital in Northwest Ethiopia: Prospective Observational Study
Authors Demelash G, Berhe YW ![]() , Gebregzi AH
, Gebregzi AH ![]() , Chekol WB
, Chekol WB ![]()
Received 10 November 2021
Accepted for publication 21 December 2021
Published 6 January 2022 Volume 2022:15 Pages 1—8
DOI https://doi.org/10.2147/OAS.S347920
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Luigi Bonavina
Getamesay Demelash,1 Yophtahe Woldegerima Berhe,2 Amare Hailekiros Gebregzi,2 Wubie Birlie Chekol2
1Department of Anesthesia, College of Medicine and Health Sciences, Debre-Markos University, Debre-Markos, Ethiopia; 2Department of Anesthesia, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Yophtahe Woldegerima Berhe
Department of Anesthesia, College of Medicine and Health Sciences, University of Gondar, Postal Address: 196, Ethiopia
Tel +251-912-494282
Email [email protected]
Background: Cesarean section is the commonest obstetric procedure worldwide and pain is the leading compliant during the postoperative period. The objective of this study was to assess the prevalence and factors associated with postoperative pain after cesarean section at a University Hospital in Northwest Ethiopia.
Materials and Methods: A prospective observational study was conducted among parturients who underwent cesarean section. After obtaining ethical approval, 299 parturients were approached. The numerical rating scale was used to measure pain severity. The association between variables was determined at 95% CI with binary logistic regression. A p-value < 0.05 was considered significant.
Results: A total of 290 parturients were included with a response rate of 97%. The overall prevalence of moderate to severe postoperative pain after a cesarean section was 85.5% (95% CI: 81.4– 89.0%) within the first 24 postoperative hours. On the multi-variable analysis, preoperative anxiety (AOR: 2.3, 95% CI: 1.1– 4.9), history of previous cesarean section (AOR: 2.3, 95% CI: 1.1– 5.0), Pfannenstiel incision (AOR: 3.2, 95% CI: 1.3– 8.0) and absence of regional analgesia (AOR: 3.7, 95% CI: 1.7– 7.9) were significantly associated with moderate to severe postoperative pain after cesarean section.
Conclusion: The prevalence of moderate to severe pain in the first postoperative day was unacceptably very high. Parturients who had preoperative anxiety, history of previous cesarean section, Pfannenstiel incisions, and those who did not receive regional analgesia have significantly suffered from postoperative pain. Pain severity needs to be assessed and documented by using pain-rating scales and interdisciplinary pain management should be provided.
Keywords: pain, post-cesarean section pain, postoperative pain, cesarean section, obstetric anesthesia and analgesia
Introduction
Cesarean section (CS) is the commonest obstetric procedure in Ethiopia and worldwide.1,2 Pain is the leading anticipated problem in the postoperative period.3 Pain is a sensory and emotional experience that is influenced by physiologic, sensory, affective, cognitive, sociocultural, and behavioral factors.4 Moderate to severe pain after CS can cause morbidities, patient discomfort, dissatisfaction, poor wound healing, delayed recovery, prolonged hospital stay, poor quality of life, and chronic pain; all of which have cost implications.5–9 If postoperative pain is poorly treated particularly in mothers who underwent CS, it will interfere with ambulation, breastfeeding, and other maternal care of the newborn. Having a baby is considered as a pleasant event, but it can be traumatic if the mother is suffering in pain.10 Therefore, adequate pain relief after CS by using safe and effective analgesic modalities is a universal concern since pain relief is one of the basic human rights.11
The most popular pain management modalities are systemic and intrathecal administration of opioids, patient-controlled analgesia, non-steroidal anti-inflammatory drugs, and regional nerve blocks. These modalities can be combined in multimodal analgesia, which results in synergistic analgesia with lowered side effects.7,8,12,13 Despite advances in pain management, parturients experience moderate to severe pain in the acute postoperative period.10 As previous studies reported, 78.4% to 92% of parturients had experienced moderate to severe pain.Furthermore, very little is known about the magnitude and factors associated with post-cesarean section pain in developing countries, especially in sub-Saharan Africa where multiple dimensions of challenges to assess and manage postoperative pain. These challenges are commonly associated with the scarcity of well-trained clinicians, materials, drugs, and facilities.5–8 The objective of this study was to assess the prevalence and factors associated with postoperative pain after CS at University of Gondar Comprehensive Specialized Hospital (UoGCSH), Northwest Ethiopia.
Materials and Methods
Study Design, Period, Population, and Variables
A prospective observational study was conducted at UoGCSH from February 15 to April 20, 2019. The hospital is located in Gondar town, Northwest Ethiopia and CS was the commonest surgical operation in the hospital with an average of 120–160 per month. The source population was all parturients who underwent CS and the study population was all parturients who underwent CS at UoGCSH during the study period. All volunteer adult (18+) parturients that underwent CS were included. Parturients who had pre-existing cognitive dysfunction and chronic pain with ongoing treatment were excluded. The dependent variable was postoperative pain which was measured by using a numerical rating scale (NRS) and independent variables were sociodemographic factors, clinical factors, intraoperative factors, and postoperative factors.
Operational Definitions
The Numerical rating scale with 11 points (NRS-11): is a valid and reliable pain assessment tool. Number assigned from 0 to 10 to represent the severity of pain: 0 = no pain, 1–3 = mild pain, 4–6 = moderate pain, 7–10 = severe pain.14 The NRS-11 was preferred due to its simplicity to understand by the parturients.15,16
Full return of consciousness: a state of consciousness of an individual after general anesthesia and become able to be easily arousable, aware of, and identity the surroundings.17
Spinal anesthesia wear-off: a point of time at which the action of spinal anesthesia ends up and patients gradually start to feel and move their legs.18
Sample Size Determination and Sampling Technique
The sample size was determined by single population proportion formula. Murray and Retief reported that the prevalence of moderate to severe pain during the first 24 postoperative hours after CS was 87%.19 The sample size was calculated, assuming a 95% confidence interval with a 4% margin of error.

We have p = 0.87, ɛ = 0.04, Zα/2 at 95% CI = 1.96
n = (1.96)2 x (0.87 x 0.13)/(0.04)2
n = 271.6 ≈ 272
A ten percent non-response rate was added and the final sample size was 299.
Data Collection, Quality Control, and Analyses
After obtaining ethical approval from the Ethical Review Committee of the School of Medicine, data were collected by using a pre-tested structured questionnaire. A pilot study was conducted on 30 (10%) clients who were not incorporated in the main study. The participants have received adequate information about the study and informed consent was obtained. Pain severity was assessed and documented by using NRS-11 at 2nd, 12th, 24th postoperative hours. The data were analyzed by using SPSS version-20 (IBM Corporate). Normality was tested by the Shapiro–Wilk test. The Hosmer and Lemeshow test was used for model assessment. The association of variables was determined by binary logistic regression at a 95% confidence interval and presented in crude and adjusted odds ratio. A p-value less than 0.05 was considered as statistically significant. This prospective observational study was appraised and reported by using STROCSS guideline. Additionally, it complies with the Declaration of Helsinki and its Research Registry Unique Identification Number is researchregistry7303.
Results
A total of 290 parturients who underwent CS were included in this study. Nine patients were excluded from analysis due to incomplete data. The age of most parturients was between 18 and 34 years and the median age (IQR) was 28 (25–30.3) years (Table 1). Most of the clients did not receive preemptive analgesia other than spinal anesthesia. The larger proportion of parturients underwent CS with spinal anesthesia and only 21 (7.2%) with general anesthesia. Predominantly, emergency CS was performed during the study period (Table 2).
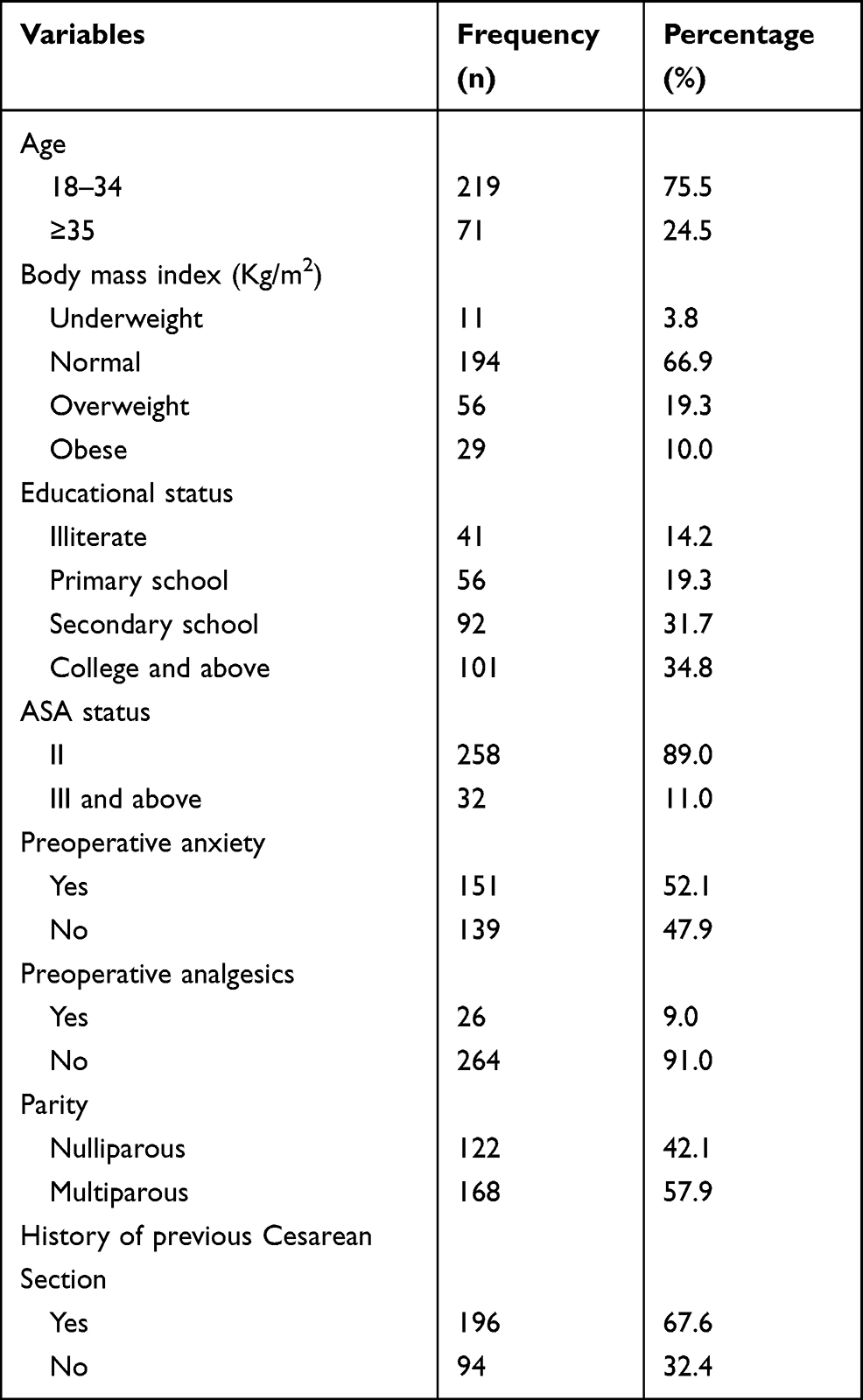 |
Table 1 Socio-Demographic and Clinical Characteristics of the Parturients Who Delivered with Cesarean Section at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia; 2019 (N = 290) |
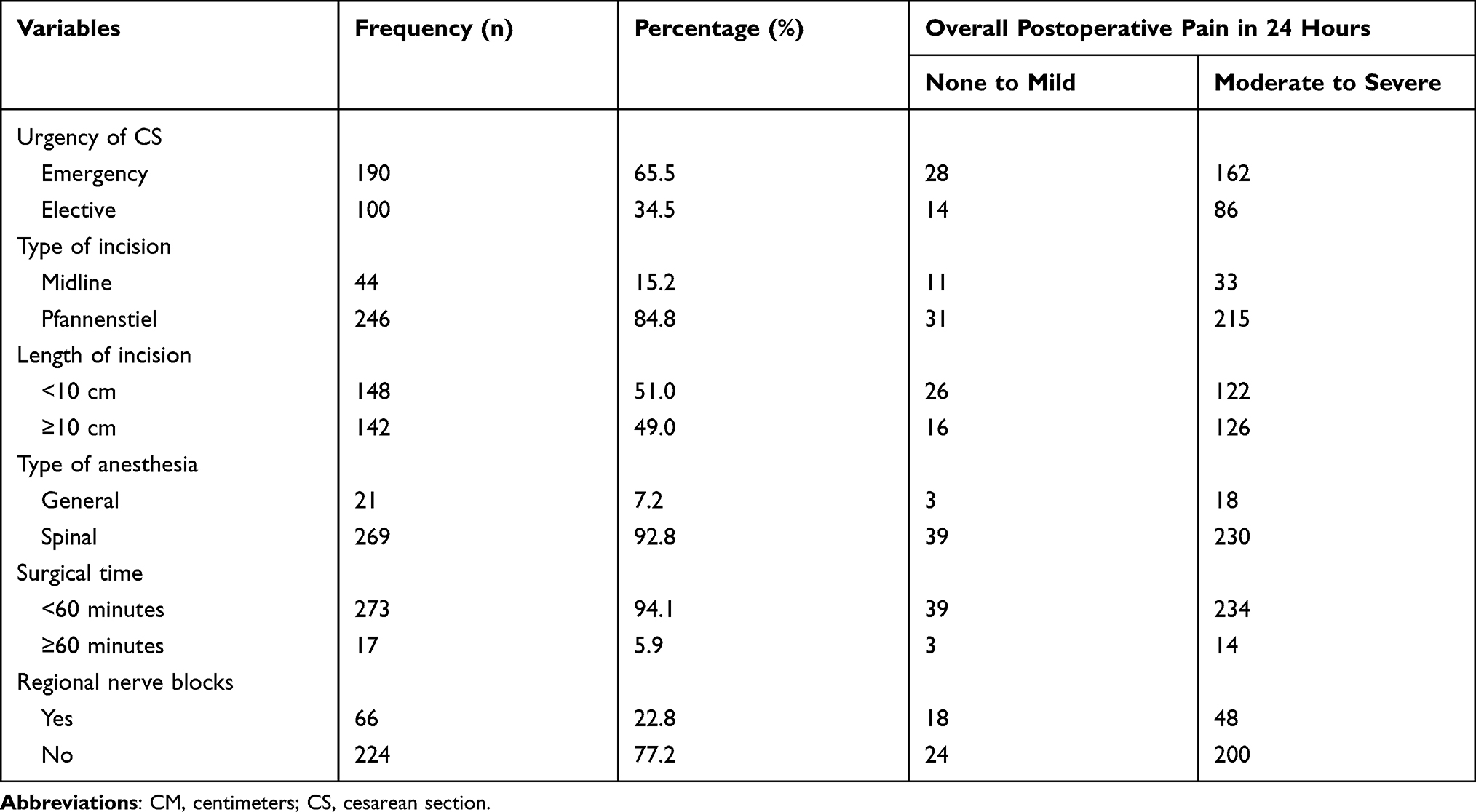 |
Table 2 A Cross-Tabulation of the Intraoperative Factors with Postoperative Pain After Cesarean Section in University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia; 2019 (N = 290) |
The NRS-11 score at the 2nd postoperative hour shows that 24.5% of parturients experienced none to mild pain, whereas 75.5% of parturients reported having moderate to severe pain. At the 12th hr, 80.0% of parturients had moderate to severe pain and only 20.0% had scored no to mild pain. At the 24th hr, 41.4% had experienced no to mild pain while 58.6% experienced moderate to severe pain. The overall prevalence of postoperative pain was 85.5% in the first 24 postoperative hours (95% CI: 81.4%, 89.0%) (Figure 1).
 |
Figure 1 Pain after cesarean section at 2nd, 12th and 24th postoperative hours at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia (N = 290). |
A 52.4% of parturients did not receive any analgesics at the 2nd hr. Out of those who received analgesics at this point, 73.2% were treated by diclofenac. The numbers of parturients that received analgesics were increased at the 12th hr and 77.2% of clients had received certain types of systemic analgesics. Diclofenac and tramadol were the commonest analgesics administered to treat pain. At the 24th hr, 36.9% of parturients did not receive any analgesics (Figure 2).
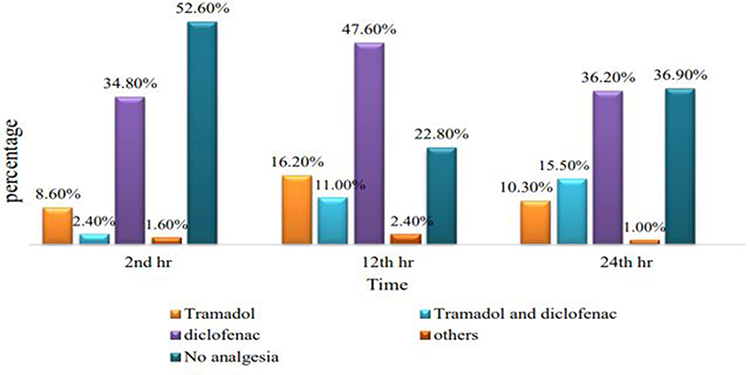 |
Figure 2 Systemic analgesics postoperatively given after cesarean section at the 2nd hr, 12th hr and 24th hr at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia (N = 290). |
The most commonly practiced regional analgesic options for postoperative pain relief after CS in the hospital were epidural analgesia, and abdominal blocks (TAP block, Ilioinguinal/Iliohypogastric nerve blocks and para-incisional wound infiltration). However, regional analgesics were provided only for 66 (22.8%) parturients, while the remaining 224 (77.2%) did not receive regional analgesia and TAP block was the most frequently performed 35 (53.0%) (Figure 3).
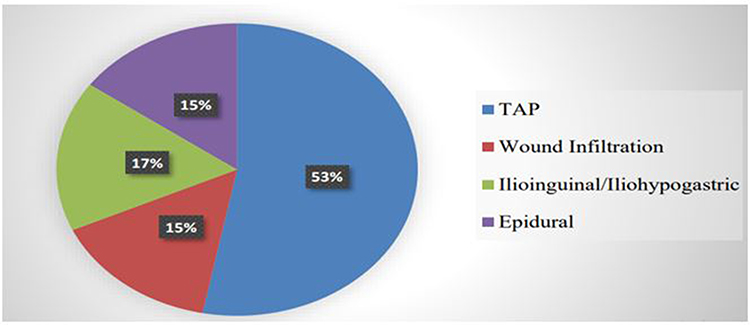 |
Figure 3 Regional analgesics provided for postoperative analgesia after cesarean section at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia (N = 66). |
In the multivariate logistic regression analysis, preoperative anxiety, history of previous cesarean section, type of incision, and administration of regional nerve blocks were found significantly associated with postoperative pain (p < 0.05) (Table 3).
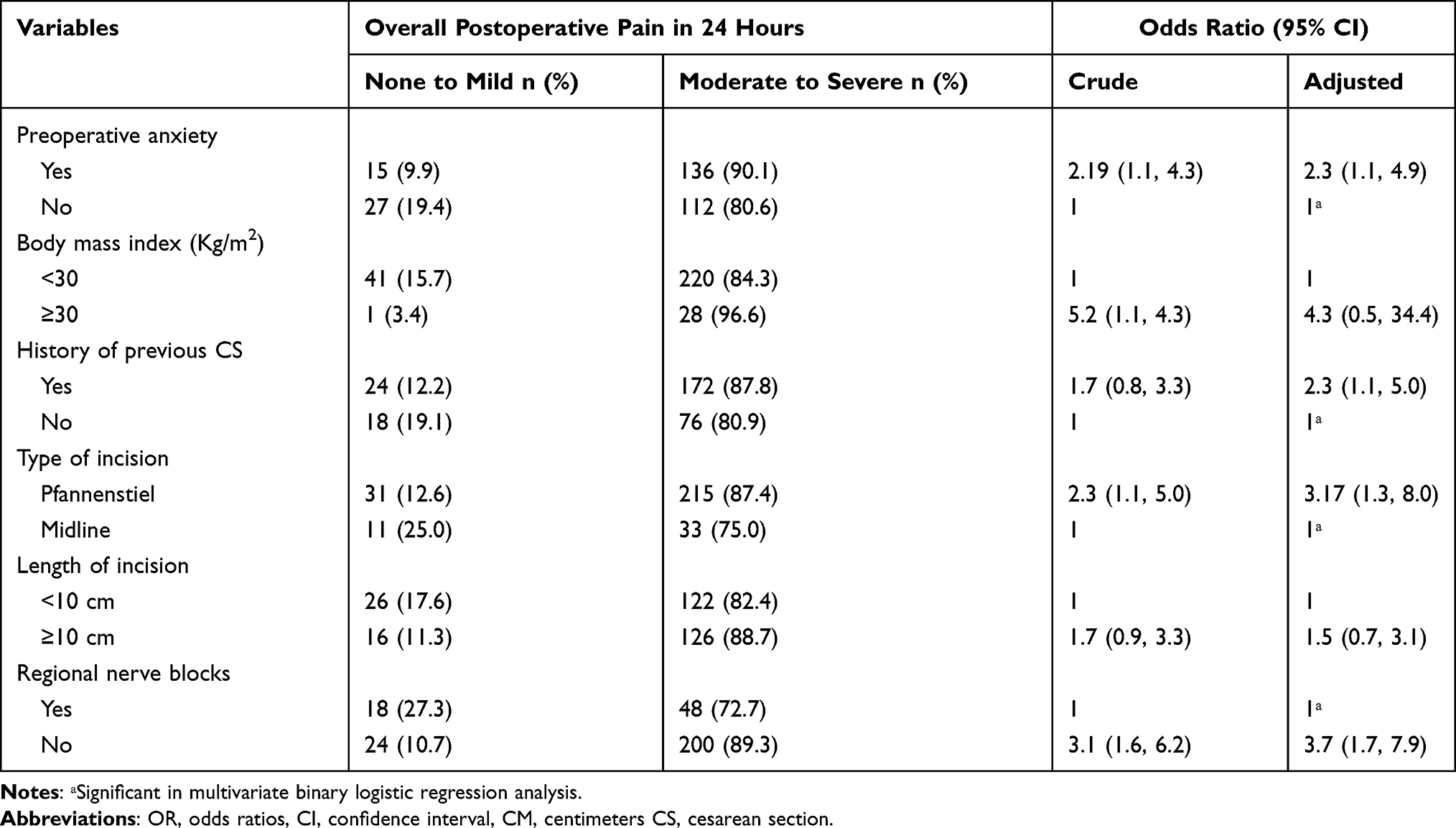 |
Table 3 Bivariate and Multivariate Binary Logistic Regression: Factors Associated with Postoperative Pain After Cesarean Section at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia; 2019 (X-Tab and OR with 95% CI) (N = 290) |
Discussion
The overall prevalence of moderate to severe postoperative pain in the first 24 postoperative hours was 85.5% (95% CI: 81.4–89.0%). Moderate to severe pain was reported in 75.5% of parturients at the 2nd hr, 80% at the 12th hr, and 58.6% at the 24th hr. These figures showed that there was inadequate treatment of pain during the postoperative period. Pain was the prevalent problem and undermanaged among surgical patients.19,20 Postoperative pain after CS is still poorly controlled and results in adverse outcomes in the wellbeing of both the mother and her newborn. Several studies have revealed a high prevalence of moderate to severe postoperative pain (78–93%) after CS.19,21–25
Moderate to severe postoperative pain was perceived in 88.2% non-CS surgical patients in Jimma, Southwest Ethiopia, and 57% at 2nd hr and 78% at 12th hr in Gondar, Northwest Ethiopia.19,26 These results exposed the inadequate treatment of postoperative pain in the country. As Eisenach et al publicized, 10.9% of participants had severe acute pain within the first 36 postoperative hours,24 which is much lower compared to our findings. The variations can be explained by a larger and multicenter sample and better practice of pain management in the developed United States of America. A survey conducted by Kintu et al reported that the prevalence of severe acute pain after CS was 33%, 39%, and 29% at Zero, 6th and 24th postoperative hours, respectively.25 However, in our study, the prevalence of postoperative pain was much higher at all time points (2nd, 12th, and 24th hr). The discrepancy could be due to the difference in assessment time points. In the earlier study, pain assessment was started on arrival to recovery area (Zero hours) at which time-point spinal anesthesia might not wear-off. Furthermore, a visual analog scale was used in the previous study while we used NRS-11. The most commonly prescribed analgesia for postoperative pain management was intramuscular diclofenac followed by tramadol. The finding is similar to the Ugandan study and showed the underuse of multiple classes of analgesics to manage postoperative pain in low-income countries.25 It was 3.7 times more likely to develop moderate to severe postoperative pain if regional analgesics were not administered as parts of multimodal analgesia. Multiple studies have supported that para-incisional wound infiltration and abdominal field nerve blocks after both spinal and general anesthesia can alleviate pain after CS and reduce opioid consumption.27–29
Preoperative anxiety was found associated with pain after CS. Parturients who had anxiety during the preoperative period were 2.3 times more likely to complain about moderate to severe postoperative pain. Comparably, a study in Brazil has revealed that the occurrence of moderate to severe postoperative pain was 1.6 times in anxious mothers preoperatively.22 Additionally, a previous study in our study area showed that 51.7% of patients had preoperative anxiety due to a fear of postoperative pain.30 Anxiety and fear of pain can predict postoperative pain after CS.31
The type of incisions significantly affected the patterns of postoperative pain. The Pfannenstiel incisions caused moderate to severe pain by 3.2 folds than midline incisions. Habib et al concluded no significant difference between midline or Pfannenstiel incisions in terms of postoperative pain.32 Despite this, another study has concluded that midline incision was associated with intense postoperative pain.33 A randomized controlled trial found that pain of vertical incisions was higher than Pfannenstiel incisions in primary CS. However, in the consecutive CS, the pain of Pfannenstiel incisions was higher.34 In the current study, a larger proportion of clients (67.6%) had a history of previous CS. Additionally, the dissimilarities can be explained by the length of incisions. The recommended optimal length of incision for CS is <10 cm.35 In the current study, larger proportions of parturients (49%) had incision length of ≥10 cm, hence, increased injury to the abdominal wall nerves and increased the rate/intensity of postoperative pain. Pfannenstiel is the commonest type of incision since it was considered to offer adequate pelvic exposure, excellent postoperative strength, reduced risk of disruption, incisional hernia, hypertrophic scar, and good cosmetic results.33 Furthermore, recent studies have shown that extra-peritoneal French Ambulatory cesarean section technique was safe and can reduce postoperative pain while accelerating recovery, suggesting that this technique should be more widely used.36,37
Our study has proved a significant association between previous CS and postoperative pain. When there was an experience of previous CS, suffering from moderate to severe pain increased by more than 2 folds and can be explained by increased risks of uterine dehiscence, bleeding, postoperative infection, adhesion, longer operating time, and hospital stay.34,38,39 Even though the study was the first for its type in the country, its limitation was the inability to show cause and effect relations since its design was observational.
Conclusion
The prevalence of moderate to severe pain in the first 24 postoperative hours was unacceptably very high at UoGCSH and pain management in the recovery rooms and maternity wards was overlooked. Parturients who had preoperative anxiety, history of previous CS, Pfannenstiel incisions, and those who did not receive regional analgesia have significantly suffered from moderate to severe postoperative pain. Pain severity needs to be assessed and documented by using pain-rating scales and there should be interdisciplinary approaches to provide adequate pain management.
Abbreviations
AOR, adjusted odds ratio; ASA, American Society of Anesthesiologists; CS, cesarean section; NRS, Numerical Rating Scale; TAP, Transverse Abdominus Plane; UoGCSH, University of Gondar Comprehensive Specialized Hospital.
Data Sharing Statement
Data and materials used in this study are available and can be presented by the corresponding author upon reasonable requests.
Ethics Approval and Consent to Participate
Ethical approval to conduct the research was obtained from Ethical Review Committee of School of Medicine, College of Medicine and Health Sciences, University of Gondar. Informed consent was taken from each study patients after brief explanation. Every participant was allowed to discontinue participation if did not want to finish it. The participants were assured that their treatment and other benefits they can gain from the hospital will not be interrupted due to their withdrawal. Confidentiality was ensured by removing identifiers and locking the questionnaires after data collection in a secured area. Additionally, when patients found experiencing pain in the postoperative period, the data collectors had reported for the corresponding care givers (Anesthetist, Surgeon or Nurse) to provide the appropriate pain management.
Acknowledgments
University of Gondar and data collectors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
College of Medicine and Health Sciences, University of Gondar.
Disclosure
The authors report that they have no competing interests in this work.
References
1. Yisma E, Smithers LG, Lynch JW, Mol BW. Cesarean section in Ethiopia: prevalence and sociodemographic characteristics. J Mater Fetal Neonatal Med. 2017;32:1–6.
2. Hehir MP, Ananth CV, Siddiq Z, Flood K, Friedman AM, D’Alton ME. Cesarean delivery in the United States 2005 through 2014: a population-based analysis using the Robson 10-Group Classification System. Am J Obstet Gynecol. 2018;219(1):
3. Caumo W, Schmidt AP, Schneider CN, et al. Preoperative predictors of moderate to intense acute postoperative pain in patients undergoing abdominal surgery. Acta Anaesthesiol Scand. 2002;46(10):1265–1271. doi:10.1034/j.1399-6576.2002.461015.x
4. Loeser JD, Melzack R. Pain: an overview. The Lancet. 1999;353(9164):1607–1609. doi:10.1016/S0140-6736(99)01311-2
5. Wang LZ, Wei CN, Xiao F, Chang XY, Zhang YF. Incidence and risk factors for chronic pain after elective caesarean delivery under spinal anaesthesia in a Chinese cohort: a prospective study. Int J Obstet Anesth. 2018;34:21–27. doi:10.1016/j.ijoa.2018.01.009
6. Sinatra R. Causes and consequences of inadequate management of acute pain. Pain Med. 2010;11(12):1859–1871. doi:10.1111/j.1526-4637.2010.00983.x
7. Recker DC, Perry PM. Postsurgical pain syndromes: chronic pain after hysterectomy and cesarean section. Tech Reg Anesth Pain Manag. 2011;15(3):133–139. doi:10.1053/j.trap.2011.08.002
8. Gamez BH, Habib AS. Predicting severity of acute pain after cesarean delivery: a narrative review. Anesth Analg. 2018;126(5):1606–1614. doi:10.1213/ANE.0000000000002658
9. Niklasson B, Georgsson Öhman S, Segerdahl M, Blanck A. Risk factors for persistent pain and its influence on maternal wellbeing after cesarean section. Acta Obstet Gynecol Scand. 2015;94(6):622–628. doi:10.1111/aogs.12613
10. Pereira TRC, Souza FGD, Beleza ACS. Implications of pain in functional activities in immediate postpartum period according to the mode of delivery and parity: an observational study. Braz J Phys Ther. 2017;21(1):37–43. doi:10.1016/j.bjpt.2016.12.003
11. Pan PH. Post cesarean delivery pain management: multimodal approach. Int J Obstet Anesth. 2006;15(3):185–188. doi:10.1016/j.ijoa.2006.04.004
12. Cançado TO, Omais M, Ashmawi HA, Torres ML. Chronic pain after cesarean section influence of anesthetic/surgical technique and postoperative analgesia. Revista Brasileira de Anestesiologia. 2012;62:768–774.
13. Bamigboye AA, Hofmeyr GJ. Local anaesthetic wound infiltration and abdominal nerves block during caesarean section for postoperative pain relief. Cochrane Database Syst Rev. 2009;3. doi:10.1002/14651858.CD006954.pub2
14. Breivik H, Borchgrevink PC, Allen SM, et al. Assessment of pain. BJA. 2008;101(1):17–24. doi:10.1093/bja/aen103
15. Gerbershagen HJ, Rothaug J, Kalkman C, Meissner W. Determination of moderate-to-severe postoperative pain on the numeric rating scale: a cut-off point analysis applying four different methods. Br J Anaesth. 2011;107(4):619–626. doi:10.1093/bja/aer195
16. Birnie KA, McGrath PJ, Chambers CT. When does pain matter? Acknowledging the subjectivity of clinical significance. Pain. 2012;153(12):2311–2314. doi:10.1016/j.pain.2012.07.033
17. Misal US, Joshi SA, Shaikh MM. Delayed recovery from anesthesia: a postgraduate educational review. Anesthesia Essays Res. 2016;10(2):164. doi:10.4103/0259-1162.165506
18. Imarengiaye CO, Song D, Prabhu AJ, Chung F. Spinal anesthesia: functional balance is impaired after clinical recovery. J Am Soc Anesthesiol. 2003;98(2):511–515.
19. Murray AA, Retief FW. Acute postoperative pain in 1231 patients at a developing country referral hospital: incidence and risk factors. Southern Afr J Anaesthesia Anal. 2016;22(1):26–31. doi:10.1080/22201181.2015.1115608
20. Admassu WS, Hailekiros AG, Abdissa ZD. Severity and risk factors of post-operative pain in University of Gondar Hospital, Northeast Ethiopia. J Anesthesia Clin Res. 2016;7(10):675. doi:10.4172/2155-6148.1000675
21. Karlström A, Engström‐Olofsson R, Norbergh KG, Sjöling M, Hildingsson I. Postoperative pain after cesarean birth affects breastfeeding and infant care. J Obstetric Gynecol Neonatal Nurs. 2007;36(5):430–440. doi:10.1111/j.1552-6909.2007.00160.x
22. Borges ND, Pereira LV, Moura LA, Silva TC, Pedroso CF. Predictors for moderate to severe acute postoperative pain after cesarean section. Pain Res Manage. 2016;2016:1–6. doi:10.1155/2016/5783817
23. Borges NC. e Silva BC, Pedroso CF, Silva TC, Tatagiba BS, Pereira LV. Postoperative pain in women undergoing caesarean section. Enfermería Global. 2017;16(4):374–383.
24. Eisenach JC, Pan PH, Smiley R, Lavand’homme P, Landau R, Houle TT. Severity of acute pain after childbirth, but not type of delivery, predicts persistent pain and postpartum depression. Pain. 2008;140(1):87–94. doi:10.1016/j.pain.2008.07.011
25. Kintu A, Abdulla S, Lubikire A, et al. Postoperative pain after cesarean section: assessment and management in a tertiary hospital in a low-income country. BMC Health Serv Res. 2019;19(1):1–6. doi:10.1186/s12913-019-3911-x
26. Eshete MT, Baeumler PI, Siebeck M, et al. Quality of postoperative pain management in Ethiopia: a prospective longitudinal study. PLoS One. 2019;14(5):e0215563. doi:10.1371/journal.pone.0215563
27. Poudel A, Dutta PK. Postoperative analgesia with bilateral ilioinguinal and iliohypogastric nerve block in lower segment cesarean section. J Soc Anesthesiol Nepal. 2017;4(2):81–86. doi:10.3126/jsan.v4i2.21208
28. Bamigboye AA, Hofmeyr GJ. Caesarean section wound infiltration with local anaesthetic for postoperative pain relief–any benefit? South Afr Med j. 2010;100(5):313. doi:10.7196/SAMJ.3716
29. Boztosun A, Duger C, Kosar MI, et al. Abdominal blockage of iliohypogastric and ilio-inguinal nerves for management of post-caesarean pain: a novel method. S Afr J Obstet Gynaecol. 2012;18(1):23–27.
30. Woldegerima YB, Fitwi GL, Yimer HT, Hailekiros AG. Prevalence and factors associated with preoperative anxiety among elective surgical patients at University of Gondar Hospital. Gondar, Northwest Ethiopia, 2017. A cross-sectional study. Int J Surg Open. 2018;10:21–29. doi:10.1016/j.ijso.2017.11.001
31. Carvalho B, Zheng M, Harter S, Sultan P. A prospective cohort study evaluating the ability of anticipated pain, perceived analgesic needs, and psychological traits to predict pain and analgesic usage following cesarean delivery. Anesthesiol Res Pract. 2016;2016:1–8.
32. Habib AS, Wahl K, Gu J, Gan TJ, Adenosine Study Group. Comparison of postoperative pain outcomes after vertical or Pfannenstiel incision for major gynecologic surgery. Curr Med Res Opin. 2009;25(6):1529–1534. doi:10.1185/03007990902959168
33. Maaløe N, Aabakke AJ, Secher NJ. Midline versus transverse incision for cesarean delivery in low‐income countries. Int J Gynecol Obstetrics. 2014;125(1):1–2. doi:10.1016/j.ijgo.2013.09.030
34. Suwannarurk K, Kasemsin P, Pongrojpaw D, et al. Post-cesarean pain associated with skin incision: vertical versus Pfannenstiel. J Med Assoc Thai. 2017;100(5):S162–7.
35. Gizzo S, Andrisani A, Noventa M, et al. Caesarean section: could different transverse abdominal incision techniques influence postpartum pain and subsequent quality of life? A systematic review. PLoS One. 2015;10(2):e0114190. doi:10.1371/journal.pone.0114190
36. Dimassi K, Halouani A, Kammoun A, et al. The extraperitoneal French AmbUlatory cesarean section technique leads to improved pain scores and a faster maternal autonomy compared with the intraperitoneal Misgav Ladach technique: a prospective randomized controlled trial. PLoS One. 2021;16(1):e0245645. doi:10.1371/journal.pone.0245645
37. Dimassi K, Ami O, Fauck D, Simon B, Velemir L, Triki A. French ambulatory cesarean: mother and newborn safety. Int J Gynecol Obstetrics. 2020;148:198–204. doi:10.1002/ijgo.13013
38. Biler A, Ekin A, Ozcan A, Inan AH, Vural T, Toz E. Is it safe to have multiple repeat cesarean sections? A high volume tertiary care center experience. Pak J Med Sci. 2017;33(5):1074. doi:10.12669/pjms.335.12899
39. Bakhshi T, Landon MB, Lai Y, et al. Maternal and neonatal outcomes of repeat cesarean delivery in women with a prior classical versus low transverse uterine incision. Am J Perinatol. 2010;27(10):791–796. doi:10.1055/s-0030-1254238
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.