Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 11
Prevalence and Factors Associated with Neonatal Mortality at Ayder Comprehensive Specialized Hospital, Northern Ethiopia. A Cross-Sectional Study
Authors Hadgu FB ![]() , Gebretsadik LG
, Gebretsadik LG ![]() , Mihretu HG, Berhe AH
, Mihretu HG, Berhe AH
Received 23 October 2019
Accepted for publication 11 January 2020
Published 28 January 2020 Volume 2020:11 Pages 29—37
DOI https://doi.org/10.2147/PHMT.S235591
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Roosy Aulakh
Fikaden Berhe Hadgu,1 Letekirstos GebreEgziabher Gebretsadik,2 Hagos Gidey Mihretu,1,3 Amanuel Hadgu Berhe1
1Department of Pediatrics and Child Health, College of Health Sciences, Mekelle University, Tigray, Ethiopia; 2Department of Biostatistics, School of Public Health, College of Health Sciences, Mekelle University, Tigray, Ethiopia; 3Department of Obstetrics and Gynecology, College of Health Sciences, Mekelle University, Tigray, Ethiopia
Correspondence: Fikaden Berhe Hadgu
PO Box: 1871, Tigray, Ethiopia
Tel +251 914 748 441
Email [email protected]
Background: The neonatal period is the most vulnerable time of human life for diseases. Neonatal morbidity and mortality are significant contributors to under-five morbidity and mortality in sub-Saharan Africa.
Objective: To assess prevalence and factors associated with neonatal mortality at Ayder Comprehensive Specialized Hospital.
Methods: A facility-based cross-sectional study was conducted on neonates admitted to the neonatal intensive care unit of Ayder Comprehensive Specialized Hospital from June 1, 2018 to May 30, 2019. Data were taken retrospectively from patient records during admission, discharge, and death certificate issue. The data were entered and analyzed using SPSS version 23. Descriptive and logistic regression analysis was done to describe and identify associated factors with neonatal mortality. P-values < 0.05 were considered statistically significant.
Results: During the study period, 1785 neonates were seen and 1069 (60%) were males. Neonatal mortality rate was 298 (16.7%). Of all the deaths, 98.3% occurred during the first 7 days of age. Respiratory distress syndrome (AOR: 12.56; 95% CI: 6.40– 24.66:), perinatal asphyxia (AOR: 19.64; 95% CI: 12.35– 31.24), congenital anomaly (AOR: 2.42; 95% CI: (1.48– 4.01), early neonatal sepsis (AOR: 3.68; 95% CI: 2.32– 5.81), late onset sepsis (AOR: 8.9; 95% CI: 4.14– 19.21), gestational age, 34– 36+6 weeks (AOR: 0.09; 95% CI: 0.014– 0.59), 3741+6 weeks (AOR: 0.025; 95% CI: 0.0030.218), > 42 weeks (AOR: 0.039; 95% CI: 0.004– 0.4250), parity (AOR: 0.64; 95% CI: 0.44– 0.93) and hospital stay (AOR: 0.09; 95% CI: 0.05– 0.14) were significantly associated with neonatal mortality. Neonates with a birth weight of less than 1500 g were at 49%, 70%, and 80% increased odds of mortality compared to those 1500-2499 g, 2500-3999 g, and more than 4000 g, respectively.
Conclusion: In this study neonatal mortality was significantly high. Neonatal mortality was highly associated with primipara, prematurity, low birth weight, perinatal asphyxia, respiratory distress syndrome, congenital anomaly, neonatal sepsis and duration of hospital stay. Many of those cases could be prevented by improving antenatal care follow up, emergency obstetric services, and the enhancement of neonatal resuscitation skills and management of sick neonates.
Keywords: prevalence, neonate, cross-sectional, mortality, Ayder Comprehensive Specialized Hospital
Introduction
The neonatal period is defined as the first 28 days from birth and may be classified into the very early (birth to <24 hr), early (birth to <7 days), and late neonatal periods 7 days to <28 days.1 Neonatal period is the most vulnerable time of human life for diseases and most of these are preventable.2 Globally yearly, 2.6 million infants die before reaching 1 month old. One million of them will die on their first day. Another 2.6 million are born dead. Mortality of children 1 month to 5 years old have reduced significantly in the last decades. But in neonates, it was not significant with 7000 newborns dying daily. The reason is partially due to neonatal diseases are difficult to treat with one drug or intervention; neonates need a systematic approach. Greater than 80% of neonatal mortality are because of prematurity, perinatal asphyxia and infections such as sepsis, meningitis and pneumonia.3 Neonatal disease pattern and outcomes are important indicators for sufficient health care planning and the outcomes are the changes in health status on which nursing and medical care have direct influence.4 A neonate is 500 times highly likely to die on his first 24 hrs than at rest of the month where 50% of all deaths occur while 75% are within the first 7 days of life.5,6 Neonates born to the poorest families are greater than 1.4 times highly likely to die during their first 28 days than those born to the richest.7 Neonatal morbidity and mortality rates show a country's socioeconomic status, as well as the efficiency and effectiveness of their healthcare deliveries. These important indicators are useful in planning to improve healthcare services.8 Out of 10 countries with the highest newborn mortality rates, 8 are in sub-Saharan Africa and two in south Asia. Ethiopia ranks fifth from these 10 countries with highest in newborn death in 2016 (90/1000).3 Despite this huge neonatal mortality rate, there are very few studies on the prevalence and neonatal mortality in Tigray region and to our knowledge no similar study done in the study hospital. So this study was aimed to assess prevalence and factors associated with neonatal mortality in Ayder Comprehensive specialized hospital so as to provide a baseline data for further better studies that could be done in the near future especially in ACSH and likely to the country, to design appropriate management protocol and recommendations.
Patients and Methods
Study Setting
This study was conducted at Ayder Comprehensive Specialized hospital, located in Tigray region Mekelle town, which is 778km from the capital city, Addis-Ababa. It started as a referral and specialized medical center in 2008 GC. It delivers clinical service to more than 8 million populations in the catchment areas of Tigray, Afar and South-eastern parts of the Amara regional state. It provides a broad range of medical services to both in and outpatient for all age groups. It also serves as a teaching hospital for medical and other health science disciplines in both undergraduate and postgraduate programs. Pediatrics and child health department provides services at outpatient clinics, at the emergency department, under-five and above-five wards, pediatric intensive care units and NICU. Our NICU (neonatal intensive care unit) ward provides service for approximately 200 neonates per month with a total of 43 beds and one room for KMC (Kangaroo mother care). There are 65 BSC nurses, 1 Neonatologist and 1 General pediatrician, 4 residents and 8 interns. It is equipped with 4 radiant warmers, 6 incubators, 5 phototherapy two mechanical ventilation and x-ray machines.
Study Design
A facility-based cross-sectional study was conducted.
Study Population
All neonates admitted to NICU from June 1, 2018 to May 30, 2019 were included.
Sample Size
All neonates admitted to NICU from June 1. 2018 to May 30, 2019 were included.
All neonates admitted to Ayder Comprehensive Specialized Hospital during the study period.
Neonates kept for observation and neonates with incomplete charts were excluded from the study.
Data Collection Procedures
Semi-structured data collection format was used to collect the data. Data were collected by trained medical interns who were practicing in NICU (after receiving ethical clearance from Institutional Review Board of Mekelle University, College of Health sciences). Before the actual data collection; training was given to data collectors on the data collection techniques. Socio-demographic character of the neonate and mothers, gestational age, birth weight, mode and place of delivery, diagnosis and outcome (discharge improved, left against medical advice, deaths) and laboratory data were included retrospectively from patient charts. The diagnosis of specific disease was made by an experienced physician (residents, pediatricians and a neonatologist).
Statistical Analysis
Data were checked, cleaned and entered into SPSS version 23 (IBM Corp., Armonk, NY: USA). Descriptive analysis was performed using frequency distribution and tables. Multicollinearity between independent variables was checked. This was investigated by using the variance inflation factor in SPSS to produce co-linearity statistics. To compute a variance inflation factor for an independent variable to test for multicollinearity, a multiple regression was performed with that variable as the new dependent and all of the other independent variables in the model as independent variables. In SPSS, colinearity statistics were produced to help determine the variance inflation factor greater than three meant that variables were considered as a linear combination of other independent variables. But, the results of a variance inflation factor test did not reveal issues with multicollinearity.
Crude odds ratio and adjusted odds ratio (AOR) were computed at 95% CI (confidence interval). Bivariate and multiple logistic regression analysis was done to identify the association between dependent and independent factors. Stepwise regression where variables with P-value<0.25 during bivariate analysis were included in the multiple logistic regression model. Finally, variables with P-value<0.05 were expressed as associated factors of neonatal mortality.
Ethical Considerations
Ethical clearance was obtained from the Institutional Review Board (Health Research Ethics Review Committee) of the College of Health Sciences of Mekelle University. Permission was taken from Ayder comprehensive specialized hospital medical director offices; a support letter from the chief clinical director was obtained. This study was conducted “ in accordance with the Declaration of Helsinki.” Data were taken from patient records. Therefore, confidentiality of data was kept and the data were not used for other purposes other than the purpose of the current study. Patient consent was not needed for this chart review study, as the college reserves the right to own the medical charts of patients.
Operational Definition
In the present study gestational age was calculated from the last menstrual period (LNMP), but if the mother did not know her LNMP, the new Ballard score was used to estimate the gestational age. New Ballard score was used to estimate the gestational age for those who are less than 72 hrs of age. Prematurity was defined as neonates born before 37 completed weeks9 In our hospital diagnosis of neonatal disease is usually made clinically with a detailed history and physical examination and supported by important laboratory investigations (investigations like complete blood count (CBC), CXR, blood culture, and if needed imaging like MRI). But sometimes the diagnosis of neonatal sepsis was made with the following criteria. Clinical signs of Possible Serious Bacterial Infection, according to the Young Infants Clinical Signs Clinical Study criteria of WHO’s Integrated Management of Childhood Illness (IMCI) guidelines, are defined as the presence of any one of the following, history of difficulty feeding, history of convulsions, movement only when stimulated, respiratory rate of 60 or more breaths per min, severe chest retractions, or a temperature of 37.5°C or higher or 35.5°C or lower.10 Neonates who presented to the NICU with a diagnosis of sepsis within 72 hrs of birth were labeled as EONS, while those who came in after 72 hrs of birth are labeled as having late onset of neonatal sepsis (LONS). The diagnosis of respiratory distress syndrome (RDS) was made when a neonate is premature and had clinical criteria of rapid breathing, cyanosis, grunting, and chest indrawing, decreased air entry bilateral on the lung fields and low saturation of oxygen with pulse oximetry, chest X-ray examination with characteristic findings for RDS and onset of symptoms shortly after birth.11 Meconium aspiration syndrome is defined as respiratory distress (manifesting as tachypnea, cyanosis, and air trapping together with reduced pulmonary compliance) in a neonate born from MSAF whose symptoms cannot be explained due to other causes. The chest typically appears barrel-shaped, with an increased anterior-posterior diameter because of over inflation. On auscultation, there will be rales and rhonchi. These signs usually occur immediately after birth.12
Perinatal asphyxia was considered when the 5th APGAR score is <7 or a neonate who did not cry or needed resuscitation. For this study the definition of perinatal asphyxia defined by the national protocol with 5 minute Apgar score less than 7. For those neonates with no documentation on APGAR score, if the neonate did not cry immediately after birth; and if the neonate developed seizure unexplained due to other causes, had respiratory distress, floppiness, decreased level of mentation, presence of seizure, and depressed or absent neonatal reflexes. WHO definitions were used for prematurity, low birth weight (LBW), very low birth weight (VLBW), extreme low birth weight (ELBW) and congenital malformations (body deformity or deformities from the birth believed to have an impact on the health of the baby).13 Anthropometric interpretations were done using Lubchenco curve.14
Neonatal Mortality Rate
Refers to the number of deaths in less than 28 days of age per 1000 live births.
Results
During the study period, a total of 1829 neonates were admitted to the study hospital. Of those 44 patients were excluded from the study because they had incomplete charts. Therefore, neonates were included in the study. Out of 1785 of neonates, 1069 (60%) were males. The male to female ratio was 1.5:1. Eight neonates (0.4%) had a disorder of sex development. Of all neonates admitted 918 (51.40%) were born at Ayder Comprehensive Specialized Hospital. Majority 1587 (89%) of the neonates were singleton, 177 (10%) were twins and 14 (0.80%) were triplets. Among neonates with documented gestational age, 1294/1771 (73%) were term and 431 (24.30%) were preterms. Birth weight was documented for 1727 (97%) neonates, of which 1066 (61.70%) had normal birth weight. Concerning weight for gestational age, 1397/1631 (86.1%) neonates were appropriate for their gestational age (AGA) (Table 1).
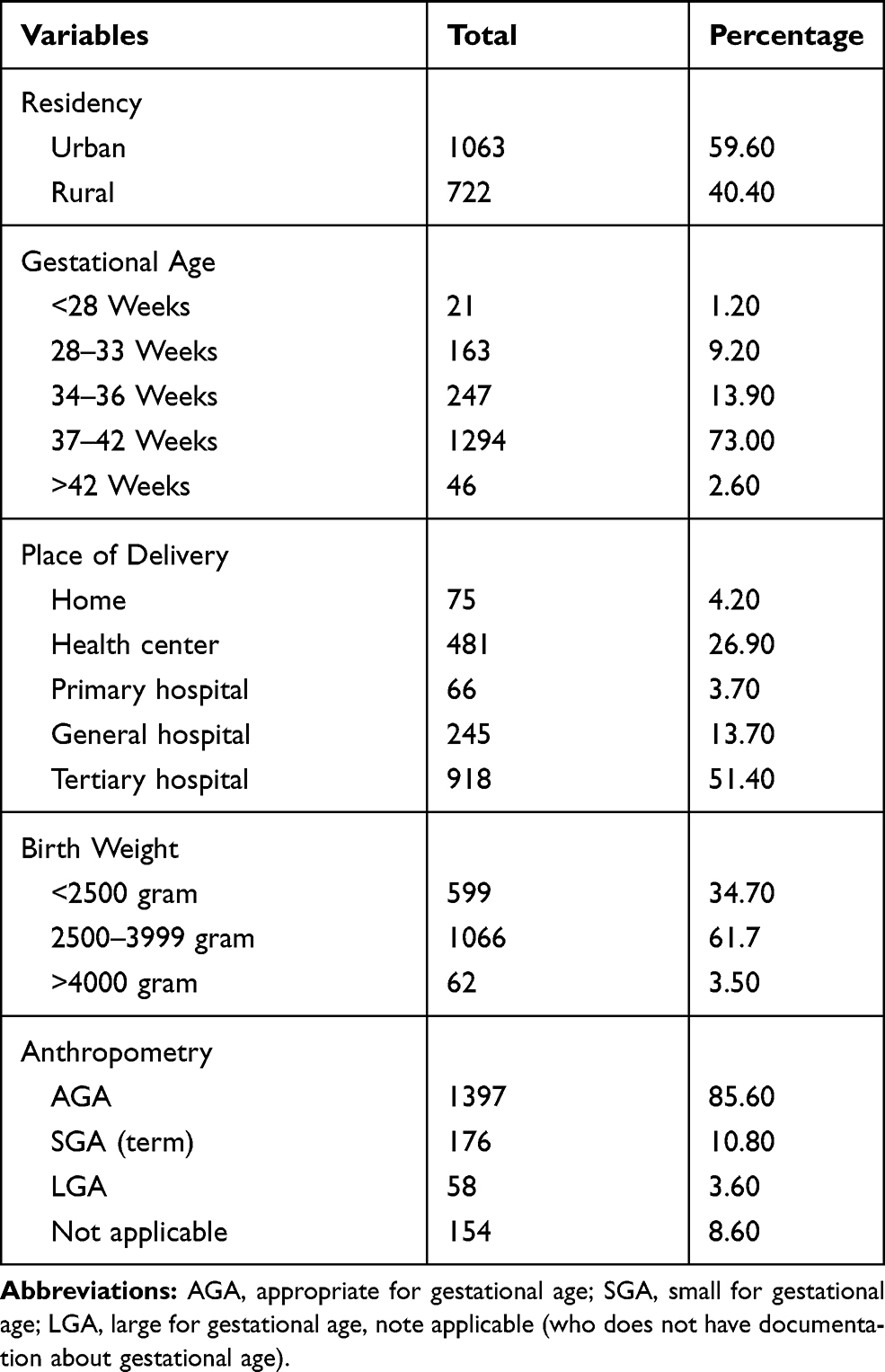 |
Table 1 Socio-Demographic and Clinical Characteristics of Neonates Admitted to ACSH from June 1, 2018 to May 30, 2019 (N=1785) |
Maternal median age was 27 years with (IQR 23–30). Of the 1785 mothers, 1603 (89.80%) were in the age range 18 to 35 years followed by 171 (9.60%) >35 years and 11 (0.60%) mothers were <18 years. The majority of the mothers, 990 (55.50%) were multiparous while 795 (44.50%) of them were primipara. Of the 1785 mothers, 26 (1.50%) had no ANC follow-up and of the mothers whose serologic status is documented 1704, 42/1704 (2.46%) were positive for human immunodeficiency virus (HIV), 45 (2.60%) had positive hepatitis B surface antibody (HBs AG). In most of the mothers, the mode of delivery was spontaneous vaginal delivery (SVD) 1166 (66.90%) and 510 (28.60%) of them were cesarean sections.
Clinical Characteristics of the Study Neonates
Of all admitted neonates 70% of the neonates were admitted in the first 24 hrs of age and 7.40% were admitted after 7 days of age. Neonatal sepsis was noted in 615 (34.40%) newborns among which 488 (79.30%) were admitted with early onset of sepsis and 127 (20.70%) with late-onset sepsis. Of the 615 septic neonates, one third (29.89%) of them were preterms. Prematurity was accounting for 431 (24.10%) of all admissions. Of these 127 (29.50%) and 183 (42.50%) were admitted with RDS and sepsis, respectively. A total of 196 (11%) neonates were admitted with perinatal asphyxia. Hyperbilirubinemia was accounting for 268 (15%) of the admissions. A total of 197 (11%) neonates were admitted with congenital anomalies, out of these 93 (47%) of them were meningocele/myelomeningocele cases, other congenital anomalies congenital heart disease 21 (1.2%), club foot 15 (0.8%), trisomies 25 (1.40%) (Table 2). Hypothermia was the commonest comorbidities seen in 844 (47.30%) of all admitted neonates, where 64 (3.60%) of had mild hypothermia, 756 (42.40%) had moderate hypothermia, and 27 (3.20%) had severe hypothermia and 59 (3.30%) were febrile. Of the hypothermic neonates, 531 (63%) were inborn (ACSH).
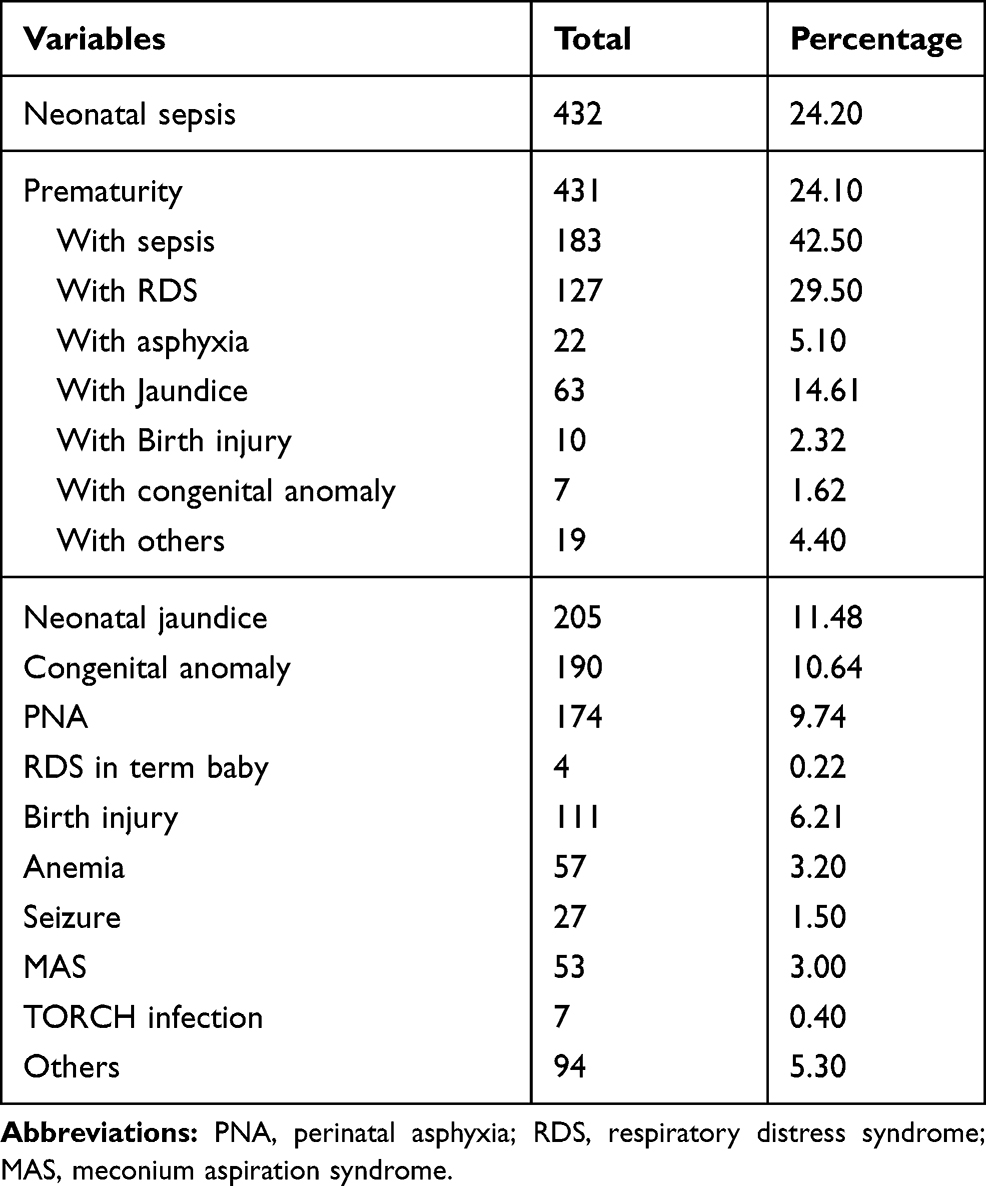 |
Table 2 Causes of Neonatal Admissions to ACSH from June 1, 2018 to May 30, 2019 (N=1785) |
Age of Neonatal Death
This study showed that 98.3% of neonatal death occurred during the first 7 days of age.
Factors Associated with Neonatal Mortality
Variables like residency, parity, prematurity, low birth weight, sepsis, perinatal asphyxia, jaundice, RDS, congenital anomaly, and birth injury, hypothermia and duration of hospital stay had significant associations in the bivariate logistic regression. But on multiple logistic regression analysis, maternal parity, prematurity, low birth weight, perinatal asphyxia, RDS, sepsis, congenital anomaly were significantly associated with mortality of neonates (Table 3). In multiple logistic regression analysis neonatal mortality was significantly associated with respiratory distress syndrome (AOR: 12.56; 95% CI: 6.40–24.66), perinatal asphyxia (AOR: 19.64; 95% CI: 12.35–31.24), congenital anomaly (AOR: 2.42; 95% CI: (1.48–4.01), early neonatal sepsis (AOR: 3.68; 95% CI: 2.32–5.81), late onset sepsis (AOR: 8.9; 95% CI: 4.14–19.21). Neonates born at a gestational age of 34–36+6 weeks were 91% at less odds of dying when compared to those who are less than 28 weeks of gestation. Neonates born at a gestational age of 37–41+6 weeks were 98% at less odds of dying when compared to that of less than 28 weeks of gestation. Neonates born at a gestational age of greater than 42 weeks were 96% at less odds of dying when compared to those who are less than 28 weeks of gestation. Neonates with birth weight less than 1500 g were at 49%, 70%, 80% increased odds of mortality compared to those 1500–2449 g, 2500–3999 g and more than 4000 g respectively. In the present study, neonates born to para 2–4 were 42% at less odds of dying when compared to neonates born from primipara mothers. Neonates born at hospitals were 70% at less odds of dying than those born at home. Neonates whose duration of hospital stay was greater than 7 days were 91% at less odds of dying than those neonates who stayed less than 7 days.
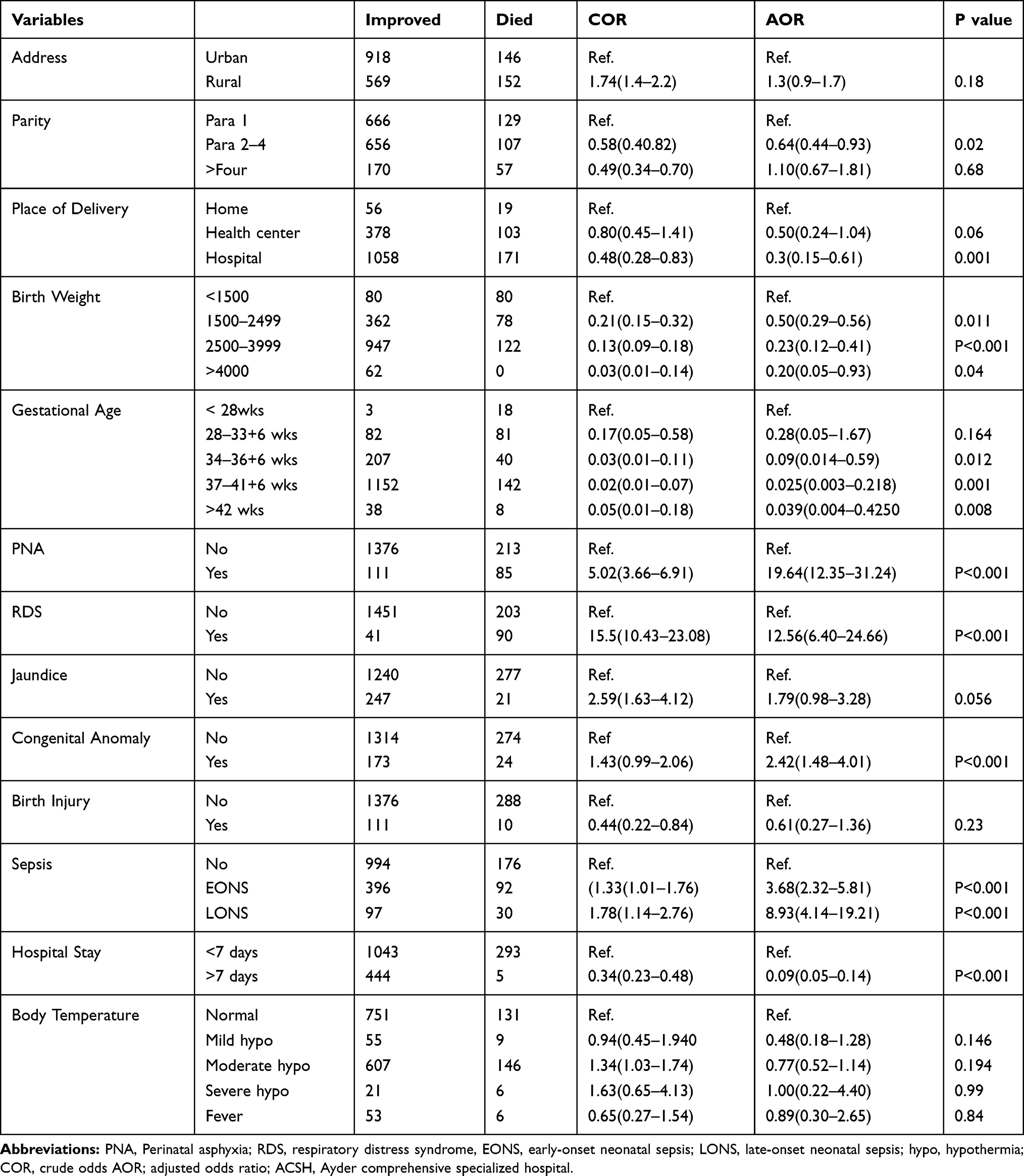 |
Table 3 Multiple Logistic Regression of Neonatal Mortality at ACSH from June 1, 2018 to May 30, 2019 (N=1785) |
Discussion
The aim of the current study was to identify prevalence and factors associated with neonatal mortality at Ayder Comprehensive Specialized Hospital, Northern Ethiopia. In this study neonatal mortality was significantly high.
In the current study, the term small for gestational age was accounted for 176 (10.8%) of the neonates. This is higher than the study done in the University of Gonder where 5.3%15 of neonates were admitted with small for gestational age. The reason could be due to the high prevalence of maternal malnutrition in Tigray because the prevalence of stunting in under-five children in Tigray in 2019 was 49%,16 but the cause should be studied well.
In the present study, neonates born to para 2–4 were 36% at less odds of dying when compared to neonates born from primipara mothers. This finding is in line with other studies.17,18 This could be due to, primipara mothers might have poor knowledge and skills about newborn care. For example, about breastfeeding, many of them may not have enough knowledge about good positioning and attachment. And also primipara mothers might not have awareness about the importance of antenatal care follow up and postnatal period. So, all mothers should have regular ANC follow-up and should get awareness about the importance of giving birth at the health facilities.
In the current study, males were higher in number 1069 (60%) at admission which is in agreement with studies done in Ethiopia, Gonder (58.3%), in St Paul’s Hospital Millennium Medical College (61.1%) and other developing countries like South Africa (57.8%) India (63.3%) Pakistan (63%).15,19–22 The reasons could be due to cultural and societal factors in some society’s male babies have more attention from caregivers than females. Male neonates also outnumbered females with respect to mortality (62.4%). This is consistent with the report from South Africa where 63% of the deaths were males.20 The reason could be that boys are biologically weaker and more susceptible to diseases and premature death, as a result of sex differences in biologic and genetic makeup.23
In the present study, the overall neonatal mortality was 16.7%. This is in line with studies done in northern Nigeria 16.9%,24 and Ghana (16.0%).25 It is lower than the study done in MizanTepi, Ethiopia where mortality was (22.8%)26 But it was higher than studies done in Ethiopia, at University of Gonder14.3%, Felege Hiwot referral hospital 13.29% and India 11.41%.15,27,28 This high degree of variation in mortality rate could be due to the difference in the health facility setups because some of the setups could be well-equipped, the presence of skilled manpower, also the difference in methodology use and the study participants‘ economic status.
Neonates who stayed less than 7 days in the hospital were at high odds of dying than those who stayed more than 7 days. This is similar to the study done in Jimma, Ethiopia29 this could be due to the fact that 98.30% of the neonatal deaths occurred during the first 7 days of age. This is consistent with the study done at MizanTepi University, Ethiopia where 97.7% of neonatal deaths occurred in the first 7 days of admission.26 This high mortality in the first seven days of age could be due to the high number of prematurity-related deaths (majority of which are secondary to respiratory distress syndrome), where maximum deaths occurred in the first 72 hrs of age. As the first few hours of age after birth are very critical to adapt the environment, simple and inexpensive measures can decrease neonatal mortality in the first 24 hrs of life.
Neonatal sepsis (24.2%), prematurity-related complications (24.1%), was the most common causes of neonatal admission. This is comparable to a study done in Ghana where the predominant causes of neonatal admissions were neonatal sepsis (29.2%) and prematurity/low birth weight (26.9%).25 When we see the prevalence of neonatal sepsis, it was higher than the study done in South Africa, 21%,20 Pakistan 20.3%30 but it was lower than study in Gonder, 67.9%.15 This high rate of difference in the prevalence of neonatal sepsis in developing countries could result by the different diagnostic criteria used to diagnose neonatal sepsis and there could also be a difference in sample size. Neonatal infection in low resource countries is high when it is compared to the developed world, the reason could be due to low socioeconomic status and the presence of other high-risk factors like prematurity, low birth weight, prolonged labor, and rupture of membrane.31 An appropriate infection prevention method should be applied in this study hospital. Neonatal jaundice was contributing to 15% of admission which is similar to a study done in Enugu, Nigeria, 16%.32
In the present study, parity, prematurity, low birth weight, perinatal asphyxia, respiratory distress syndrome, congenital anomaly, and neonatal sepsis were predictors of neonatal mortality. This is supported by other research29 This implies that the majority of the associated factors of neonatal mortality are preventable and treatable conditions that could be addressed by identifying high-risk pregnant mothers, the provision of proper and timely interventions and intensifying neonatal care.
Limitations of the Study
This study had limitations because it is a retrospective study, a significant number of patient charts were incomplete.
This study was done in a single center as a result; the prevalence may not reflect the overall prevalence in the community.
In addition, as a cross-sectional study design, this study does not show cause-and-effect relationships.
Some variables had wide confidence intervals on multivariable logistic regression.
Conclusion and Recommendations
This study shows a high rate of neonatal mortality. Neonatal mortality was highly associated with primipara, prematurity, low birth weight, perinatal asphyxia, respiratory distress syndrome, congenital anomaly, neonatal sepsis and duration of hospital stay. All responsible stakeholders should work hard to improve care for all neonates with special attention to the care of high-risk neonates. For instance, the obstetrics ward should work on improving the delivery facility by providing skilled manpower (health care providers that advice pregnant mothers to deliver in a health facility, midwives and obstetricians that follow laboring mothers with partograph) to improve obstetrics care services and early referral of neonates. Tigray regional health bureau should give capacity building training to health care providers especially for those who are working in remote health facilities. The neonatal intensive care unit should work on early diagnosis and appropriate management of neonates at admission, and there should be good continuous nursing care. Moreover, the hospital management should work to improve service provision at the labor ward and neonatal intensive care unit. Further prospective studies should be done to know where the gap is (maternal, neonatal intensive care unit or health care facility-related factor).
Data Sharing Statement
All important data are included in the manuscript.
Acknowledgment
The authors are thankful to the data collectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Carlo WA. Overview of mortality and morbidity. In: Kleigman RM, Stanton BF, SP Geme JW
2. UNICEF. United Nations Inter-agency Group for Child Mortality Estimation (UN IGME). Monit Situation Children Women. 2019;386:2276–2286.
3. United Nations Children’s Fund. Every Child Alive, the Urgent Need to End Newborn Deaths. Switzerland; 2018.Available from: https://www.unicef.org/publications/files/Every_Child_Alive_The_urgent_need_to_end_newborn_deaths.pdf. Accessed January 22, 2020.
4. Sharma A, Ford S, Calvert J. Adaptation for life: a review of neonatal physiology. Anaesth Intensive Care Med. 2010;12(3):85–90. doi:10.1016/j.mpaic.2010.11.003
5. UNICEF. The State of the World's Children 2008: Child Survival. 2008:4114. Available from: https://www.unicef.org/publications/files/Every_Child_Alive_The_urgent_need_to_end_newborn_deaths.pdf. Accessed 22 January, 2020.
6. Lawan JE, Cousens S, Zupan J. 4 million neonatal deaths: when? where? why? Lancet. 2005;365(9462):891–900. doi:10.1016/S0140-6736(05)71048-5
7. United Nations Children’s Fund, Committing to Child Survival: a promise renewed – Progress report 2014. New York: UNICEF; September 2014.
8. Bhutta ZA, Qadir M. Addressing maternal nutrition and risks of birth asphyxia in developing countries. Arch Pediatr Adolesc Med. 2009;163:671–672. doi:10.1001/archpediatrics.2009.97
9. Ballard JL, Khoury JC, Wedig K, Wang L, Eilers-Walsman BL, Lipp R. New Ballard score, expanded to include extremely premature infants. J Pediatr. 1991;119:417–423. doi:10.1016/S0022-3476(05)82056-6
10. Fuchsa A, Bielickia J, Mathur S, Sharlan M, Johannes N. Antibiotic use for sepsis in neonates and children evidence update WHO-reviews. WHO Rev. 2016.
11. Martin RJ, Fanaroff AA, Walsh MC, editors. Respiratory Distress in the Neonate. In: Fanaroff and Martins Neonatal Perinatal Medicine 10th Edition. Philadelphia: Elsevier; 2015:1074–1083. Available from :https://en.softonic.com/s/.-fanaroff-andmartins-neonatal-perinatalmedicine-10th-edition.Philadelphia.2015?query=
12. Fanaroff A. Meconium aspiration syndrome: historical aspects. J Perinatol. 2008;28:S3–S7. doi:10.1038/jp.2008.162
13. World Health Organization. Promoting Optimal Fetal Development: Report of a Technical Consultation. Geneva: World Health Organization; 2006:3. Available from:https://www.who.int/nutrition/topics/fetal/_dev_report_EN.pdf. Accessed 22 January 2020.
14. Lubchenco L, Hansman C, Dressler M, Boyd E. Intrauterine growth as estimated from live born birth weight data at 24 to 42 weeks of gestation. Pediatrics. 1963;32:793–800.
15. Demisse AG, Alemu F, Gizaw MA, et al. Patterns of admission and factors associated with neonatal mortality among neonates admitted to the neonatal intensive care unit of University of Gondar Hospital, Northwest Ethiopia. A cross-sectional study. Dove Press. 2017;8:57.
16. Federal Democratic Republic of Ethiopia. Ethiopa; Mini Demographic and Health Survey; 2019. Addis Ababa, Ethiopia: Ethiopian Public Health Institute; Federal Ministry of Health; July 2019. Available from:https://dhsprogram.com/pubs/pdf/PR120/PR120.pdf. Accessed 22 January 2020.
17. Yego F, Stewart Williams J, Byles J, Nyongesa P, Aruasa W. A retrospective analysis of maternal and neonatal mortality at a teaching and referral hospital in Kenya. Reprod Health. 2013;10:13. doi:10.1186/1742-4755-10-13
18. Ronel D, Wiznitzer A, Sergienko R, Zlotnik A, Sheiner E. Trends, risk factors and pregnancy outcome in women with uterine rupture. Arch Gynecol Obstet. 2012;285(2):317–321. doi:10.1007/s00404-011-1977-8
19. Tekleab AM, Amaru GM, Tefera YA. Reasons for admission and neonatal outcome in the neonatal care unit of a tertiary care hospital in Addis Ababa: a prospective study. Res Reports Neonatol. 2016;201:17–23. doi:10.2147/RRN.S95455
20. Hoque M, Haaq S, Islam R. Causes of neonatal admissions and deaths at a rural hospital in KwaZulu-Natal, South Africa. South Afr J Epidemiol Infect. 2011;25(1):26–29. doi:10.1080/10158782.2011.11441416
21. Anand K, Kant S, Kumar G, et al. Neonatal morbidity and mortality of sick newborns admitted in a teaching hospital of Uttarakhand. CHRISMED J Health Res. 2014;1(4):247–253.
22. Ali SR, Ahmed S, Lohana H. Disease patterns and outcomes of neonatal admissions at a secondary care hospital in Pakistan. Sultan Qaboos Univ Med J. 2013;13(3):418–421. doi:10.12816/0003265
23. Pongou R. Why is infant mortality higher in boys than in girls? A new hypothesis based on preconception environment and evidence from a large sample of twins. Demography. 2013;50(2):421–444. doi:10.1007/s13524-012-0161-5
24. Mukhtar-Yola M, Iliyasu Z. A review of neonatal morbidity and mortality in Aminu Kano teaching hospital, Northern Nigeria. Trop Doct. 2007;37:130–132. doi:10.1258/004947507781524683
25. Walana W, Acquah Ekuban KS, Abdul-Mumin A, et al. Pattern, causes and treatment outcomes of neonatal admission in the Tamale teaching hospital. Clin Mother Child Health. 2016;13:252. doi:10.4172/2090-7214.100025
26. Mekonnen T, Tenu T, Aklilu T, Abera T. Assessment of neonatal death and causes among admitted neonates in neonatal intensive care unit of Mizan Tepi University Teaching Hospital, Bench Maji Zone, South-West Ethiopia, 2018. Clin Mother Child Health. 2018;15:305. doi:doi:10.4172/2090-7214.1000305
27. Tewabe T, Mehariw Y, Negatie E, Yibelta B. Neonatal mortality in the case of Felege Hiwot referral hospital, Bahir Dar, Amhara Regional State, North West Ethiopia 2016: a one year retrospective chart review. Ital J Pediatr. 2018;44::57. doi:10.1186/s13052-018-0498-5
28. Kumar R, Mundhra JA, Jain S. Morbidity and mortality profile of neonates admitted in special newborn care unit of a teaching hospital in Uttarakhand, India. Int J Res Med Sci. 2019;7(1):241–246. doi:10.18203/2320-6012.ijrms20185388
29. Seid SS, Ibro SSA, Ahmed AA, Akuma AO, Reta EY, Haso TK. Causes and factors associated with neonatal mortality in Neonatal Intensive Care Unit (NICU) Jimma University Medical Center, Jimma, South West Ethiopia. Pediatr Health Med Ther. 2019;10:39. doi:10.2147/PHMT.S197280
30. Ali SR, Ahmed S, Lohana H. Disease patterns and outcomes of neonatal admissions at a Secondary Care Hospital in Pakistan. Sultan Qaboos Univ Med J. 2013;13(3):424–428.
31. Steer P. The epidemiology of preterm labor a global perspective. J Perinat Med. 2005;33:273 276. doi:10.1515/JPM.2005.053
32. Ekwochi U, Ndu IK, Nwokoye IC, Ezenwosu OU, Amadi OF, Osuorah D. Pattern of morbidity and mortality of newborns admitted into the sick and special care baby unit of Enugu State University Teaching Hospital, Enugu state. Niger J Clin Pract. 2014;17(3):346–351. doi:10.4103/1119-3077.130238
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.