Back to Journals » Clinical Interventions in Aging » Volume 18
Prevalence and Factors Associated with Depression Among Older Adults During the COVID-19 Pandemic: A Cross-Sectional Study in Urban Areas in Thailand
Authors Tangthong A, Manomaipiboon B ![]()
Received 18 April 2023
Accepted for publication 30 June 2023
Published 10 July 2023 Volume 2023:18 Pages 1055—1065
DOI https://doi.org/10.2147/CIA.S417719
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Aksornanong Tangthong, Basmon Manomaipiboon
Department of Urban Medicine, Faculty of Medicine, Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand
Correspondence: Basmon Manomaipiboon, Department of Urban Medicine, Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, 10300, Thailand, Tel +6683-0953300, Email [email protected]
Purpose: This study examined the prevalence of and factors associated with depression symptoms among Thai older adults during the COVID-19 pandemic.
Patients and Methods: A cross-sectional survey was conducted among older adults in urban areas in Bangkok, Thailand, between July and October 2021. The 15-item Thai Geriatric Depression Scale (TGDS-15) was used to determine the prevalence of depression symptoms, and multiple logistic regression was conducted to identify the associated factors.
Results: A total 156 older adults survey responses were received. The largest group of participants (80.8%) was aged below 70, women (50.6%), married (67.9%), retired (41%), having sufficient income (67.9%), living with their families (89.1%). More than half (71.8%) had an underlying disease, with hypertension being the most common (39.1%). In addition, 17.3% of the participants had received compulsory COVID-19 vaccination. Only 0.6% had a history of COVID-19 infection. The prevalence of depression among Thai older adults was 20.5%. Univariate analysis demonstrated occupation and income sufficiency was associated with depression symptoms. The results of the multivariate analysis found that the “non-worker” group was 3.54 times more likely to experience depression symptoms than the reference group (OR = 3.54, 95% CI = 1.25– 10.02, p = 0.018) when controlling for the confounding factors.
Conclusion: This study highlights the importance of addressing depression symptoms among Thai older adults, in which occupation and income sufficiency were the main variable factors for depression. Our study further suggested that the importance of interventions such as increasing job availability and establishing financial aid policies may ameliorate depression symptoms among older adults, especially in high-risk groups during the pandemic situation such as the COVID-19.
Keywords: depression, older adult, COVID-19, urban areas
Introduction
Thailand has been experiencing an ageing society since 2005. In 2019, the older population aged 60 years and above accounted for 18% of the total population and was predicted to reach 20% in 2025.1,2 Older adults are more susceptible to infection than their younger counterparts owing to the physiological changes associated with ageing, such as immune system deterioration. Therefore, older adults have been categorised as a high-risk group, more prone than the general population to become infected with the novel and widespread coronavirus disease 2019 (COVID-19).3 In Thailand, the COVID-19 pandemic presented occurred in three waves over a period of 17 months, with the number of cases increasing by over 100,000 as a result of a number of risk factors, including close contact with a confirmed patient, community risk, cluster communities, and active and community surveillance.4,5 COVID-19 pandemic not only effect on physical health but also has a negative impact on quality of life and well-being.6 COVID-19 patients are likely to be more vulnerable to stressful situation.
COVID-19 has affected a significant portion of the population globally including students, older adults and physically active individuals who have faced increased stress and anxiety during the pandemic.7 Moreover, the pandemic has also resulted in increased depression symptoms worldwide.8,9 These psychological effects can be detrimental to health, quality of life, and well-being.9,10 During the pandemic, psychological effects commonly occur with anxiety, anger, stress, confusion, and social isolation during the pandemic leading to stress and depression.11–13 The prevalence of depression symptoms was increase comparing between before and during lockdown was 14.3% to 33.2%, respectively, with the increase of anxiety symptoms, insufficient sleep, unsatisfactory sleep, and unsatisfactory quality of life.14 The worsen of depressive symptoms, anxiety symptoms, sleep quantity were also reported during lockdowns.14
Currently, depression has become a disease burden with a prevalence of 4.4% accounting for the sixth-ranked disease causing the most disability in Thailand.15 Depression in older adults is associated with an increased risk of morbidity, increased risk of suicide, impaired cognitive and social function, and self-neglect which of all leads to increased mortality risk.16
While early detection of depression among older adults is limited since the symptoms are likely to be unrecognized, underestimated, and interfered with normal aging. The diagnostic criteria for major depression for the general population according to the Diagnostic and Statistical Manual of Mental Disorders, fifth edition, include sadness and anhedonia, although older adults are less likely to present with affective symptoms. In addition, depression symptoms among older people are more likely to display changes in cognitive, somatic symptoms, impaired daily function, and loss of interest.16,17 Thus, the screening instruments such as the 15-question Thai Geriatric Depression Scale (TGDS-15) had been developed and validated. TGDS-15 has been widely used to early detect the depression symptoms typically presented in older adults such as feeling of loneliness, helplessness, hopelessness, emptiness, worthlessness, impaired memories, and loss of their energy. TGDS-15 has been translated into Thai and validated among the Thai older population.18
Since COVID-19 pandemic could impact on psychological illness, especially depression symptoms among older people. Our study aimed to determine the prevalence of depression symptoms and their associated risk factors during the COVID-19 pandemic among older adults who visited a family medicine clinic. Such an attempt could guide the healthcare system to endorse mental health promotion, preventive mental health programs, appropriate screening programs, and referral systems to promote quality of life and well-being in older adults. Furthermore, psychological support should be provided to help relieve older adults of adverse psychological events effects and overcome this challenging situation.19
Materials and Methods
Study Design
A cross-sectional design was adopted to collect data from older adults aged 60 and older who attended a family medicine clinic at the Faculty of Medicine Vajira Hospital, Bangkok, Thailand, from July to October 2021. The study was approved by the ethics committee of the Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand. (COA 121/2564). All experiments were performed in accordance with relevant guidelines and regulations, in the Declarations section.
Participants
Older people aged 60 years old and older living in urban setting of Thailand, with the ability to read Thai was included. The exclusion criteria were declining participation and diagnosis of cognitive impairment(s), such as severe depression, excluded by screening the individual’s medical history. The sample size was calculated using an infinite population proportion formula to achieve a suitable power level.20
Data Collection
Data was collected by face-to-face, which the participants were given an information sheet and provided written informed consent. The voluntary participants were provided the instructions to fill in the questionnaire. All participants have been performed in accordance with the Declaration of Helsinki and have been approved by an appropriate ethics committee.
Questionnaire
The questionnaire was self-reported (see Supplementary Files 1 for details). For older adults with reading and writing limitations, trained research staff read out all the items to the participants in a clear monotone while maintaining a neutral facial expression. They then filled in their responses for them.
Measures were divided into two sections. First, the demographic section included 11 items: gender, age, educational level, occupation, marital status, income sufficiency, debt, underlying diseases, residence, history of substance use such as alcohol and tobacco, and history of COVID-19 infection. Second, the Thai Geriatric Depression Scale (TGDS-15) was used to ascertain depression symptoms.21,22 The TGDS-15 is a self-administered assessment that focuses on psychiatric symptoms such as mood (eg, emptiness, boredom, and life satisfaction) and cognitive changes rather than somatic symptoms (eg, weight loss and sleep disturbances).
The TGDS-15 has demonstrated good internal consistency (Cronbach’s alpha of 0.85) among the older Thai population.21,22 It comprises 15 yes/no questions, with yes and no scored as 1 and 0, respectively, and a maximum score of 15 points. A total score ≥5 was classified as the cutoff to detect significant depression symptoms, demonstrating a sensitivity of 86% and specificity of 91%.18
Statistical Analysis
Demographic data were analyzed and reported using descriptive statistics. The prevalence of depression was demonstrated by frequency and incidence rate with a 95% confidence interval (CI). Univariate analysis was performed using a simple logistic regression analysis to identify the factors associated with depression symptoms; these factors were presented with crude odds ratios (ORs). We then identified potential confounding factors that were significant (p-value <0.100) using a multivariate analysis; these factors were further analyzed using a multiple logistic regression analysis and presented with adjusted odds ratios (AORs) and 95% CIs. Data were analyzed using SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA), at a statistical significance of p > 0.05.
Results
Participants’ Characteristics
A total of 156 questionnaire responses were obtained, and socio-demographic and clinical characteristics are presented in Table 1. The largest group of participants (80.8%) was aged below 70 old (range 60–69 years old), women (50.6%), married (67.9%), education higher than bachelor (55.1%). Approximately half were retired (41%), having sufficient income (67.9%). Most participants lived with their families (89.1%).
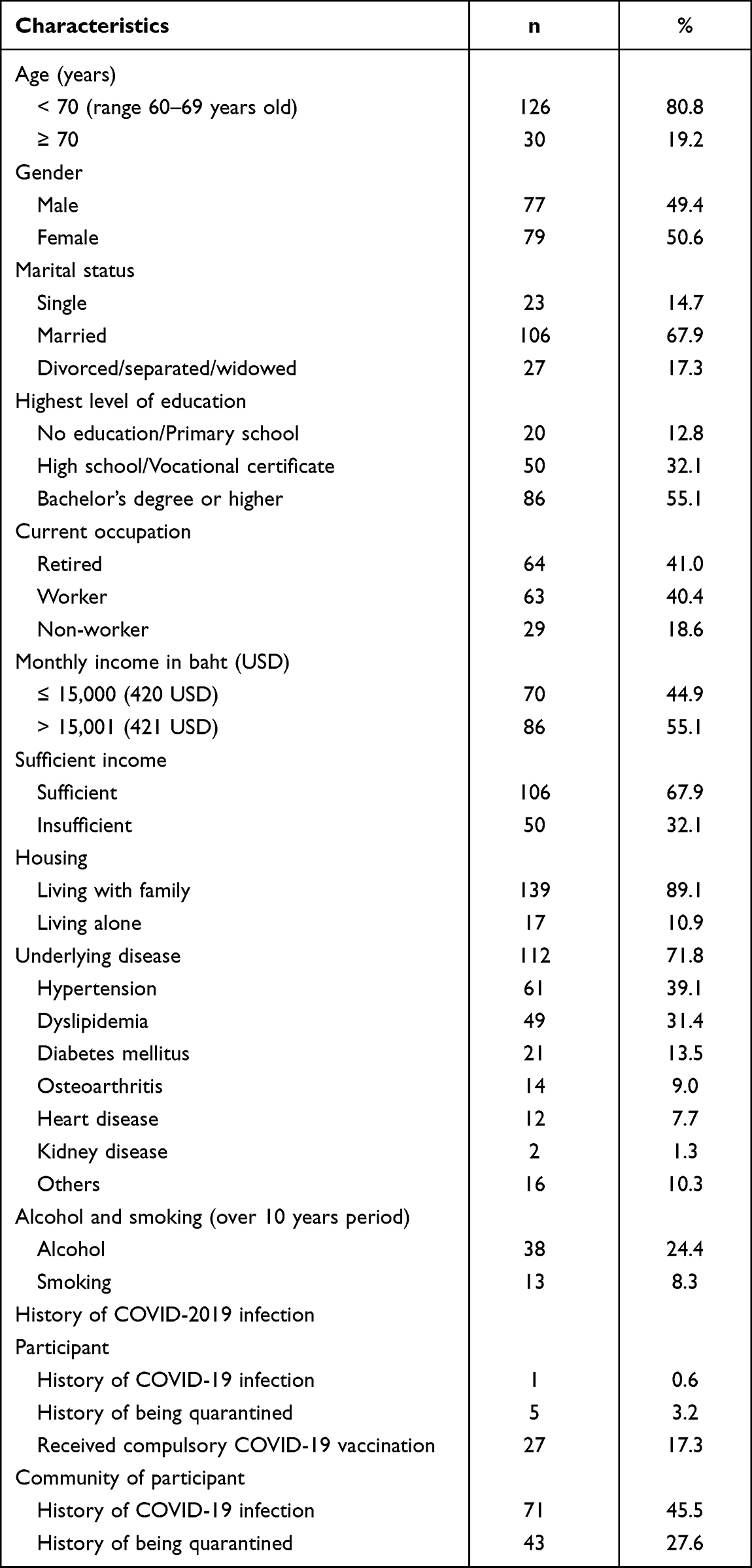 |
Table 1 Participants’ Demographic Characteristics (n = 156) |
In terms of clinical characteristics, more than half (71.8%) had an underlying disease, with hypertension being the most common (39.1%). Almost one-fourth (24.4%) had a history of alcohol use, whereas only 8.3% had a history of smoking over 10 years period. In addition, regarding vaccine history, 17.3% of the participants had received compulsory COVID-19 vaccination. Only 0.6% had a history of COVID-19 infection.
Prevalence of Depression Among Older Adults
The prevalence of depression symptom is presented in Table 2, which is 20.5%, using the TGDS-15 as the criteria for depression symptoms. Current occupations and income insufficiency were significantly associated with depression symptoms. Gender, age group, marital status, level of education, monthly income, housing, underlying diseases, history of substance use, and history of COVID-19 infection among the participants and their communities were not associated with depression symptoms.
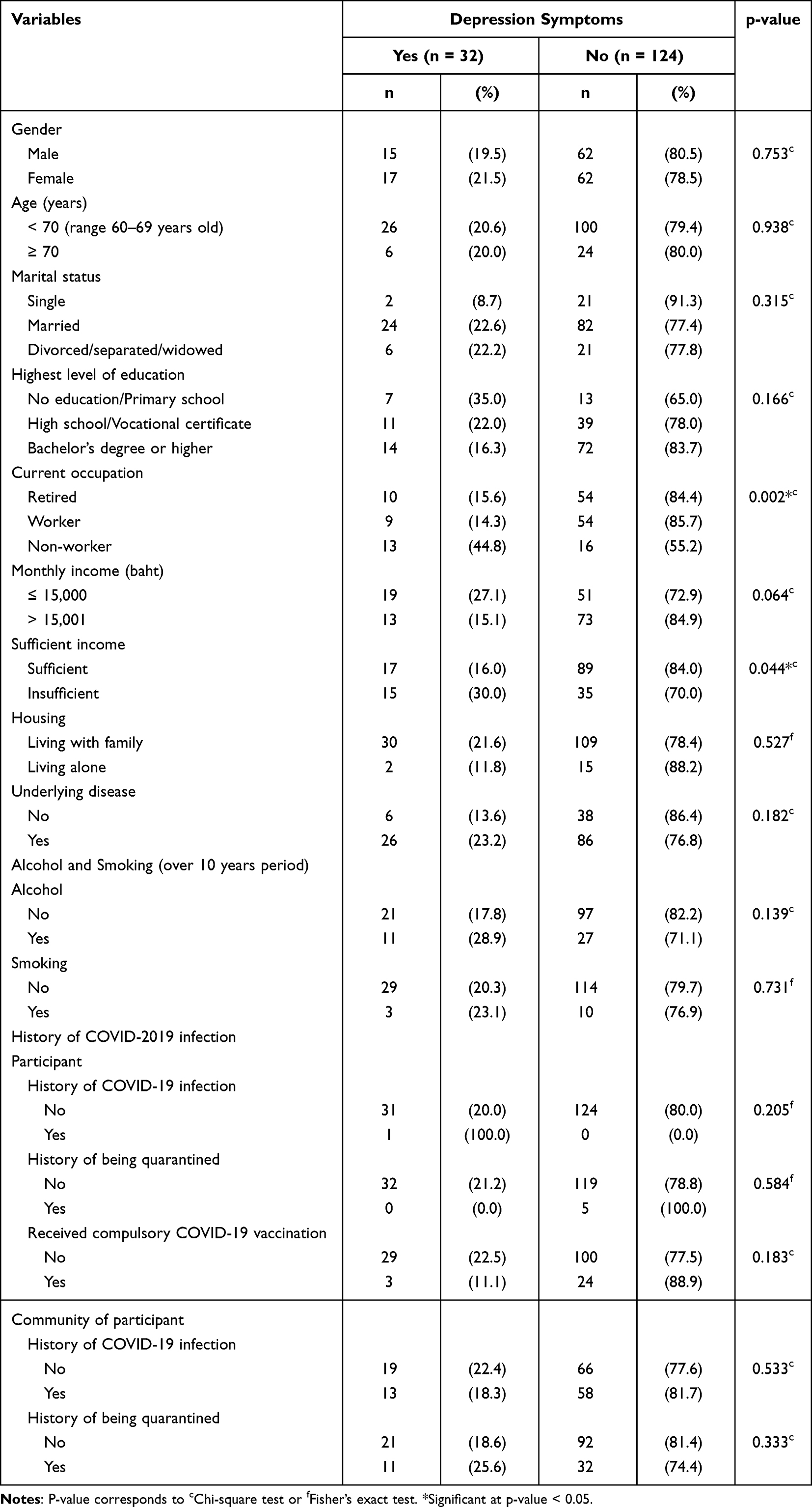 |
Table 2 Prevalence of Depression Symptoms (TGDS ≥ 5) by Demographic Characteristics |
Association Between Factor Variables and Depression Among Older Adults
Table 3 shows the association of the factor variable depression score among older adults during the COVID-19 pandemic based on logistic regression models. The univariate analysis showed that the factors significantly related to depression symptoms were current occupation and income sufficiency. First, the “non-worker” group was 4.39 times more likely to experience depression symptoms than reference group (OR = 4.39, 95% CI = 1.62–11.87, p-value = 0.004). Second, the “insufficient income” group was 2.24 times more likely to experience depression symptoms than reference group (OR = 2.24, 95% CI = 1.01–4.98, p-value = 0.047). Then, the following factors with a significance level of 0.100 (p-value < 0.100) were included in the multivariate analysis: level of education, current occupation, monthly income, and income sufficiency.
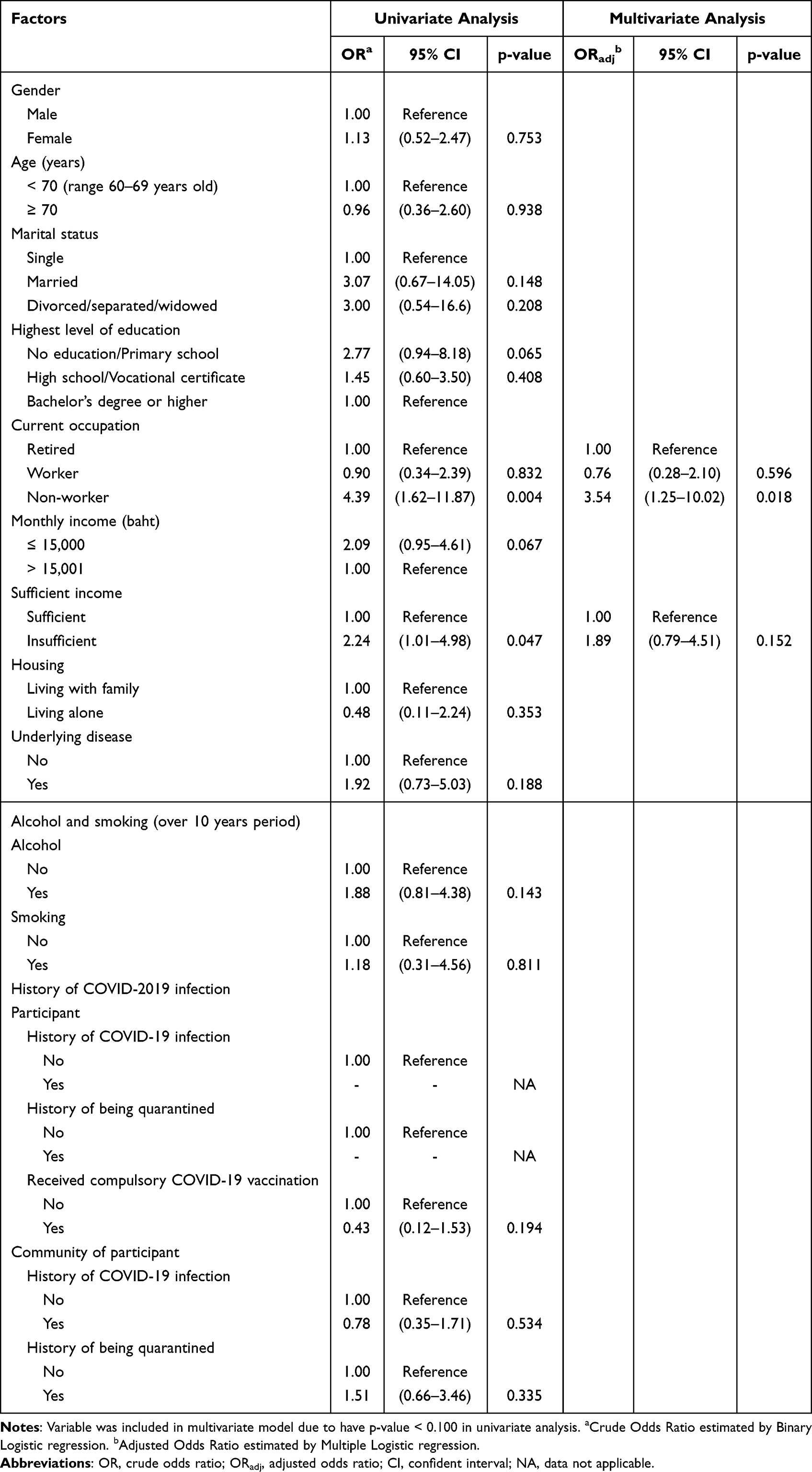 |
Table 3 Multiple Logistic Regression Analysis for Factors Associated with Depression Symptoms Among Older Adults |
The results of the multivariate analysis demonstrated that the “non-worker” group was 3.54 times more likely to experience depression symptoms than the reference group (OR = 3.54, 95% CI = 1.25–10.02, p = 0.018) when controlling for the confounding factors. The monthly income factor was not significantly associated with depression symptoms in the multivariate analysis. Therefore, gender, age, marital status, education, monthly income, housing, underlying diseases, history of substance use, and history of COVID-19 infection among the participants and their communities were not associated with depression symptoms.
Discussion
In the current situation, the COVID-19 pandemic has been one of the risks for depression to both individuals and communities. This is the first study (n = 156) on depression among older adult based on TGDS-15 in urban areas in Bangkok, Thailand, conducted during the COVID-19 pandemic. To the best of our knowledge, we found that older adult has a higher prevalence (20.5%) of depression than the pre-pandemic situation accounted for the prevalence rate of 9.6% reported in an outpatient study of a similar population in Songklanagarind, a provincial area of Thailand.23 In addition, factor variables were presented that occupation and income sufficiency were statistically significantly associated with depression (p < 0.05). Our results were similar to previous findings regarding the prevalence of depression in community-dwelling older adults during the COVID-19 pandemic: 22.9% among an urban population in Singapore and 19.8% in Ireland.9,24 Our study might indicate that the COVID-19 pandemic has enhanced depression among older adults in urban areas. In addition, the pandemic could result in negative health outcome such as insufficient sleep, unsatisfaction sleep, unsatisfactory quality of life; in addition, the used of at least one psychotropic drug increased compared to pre-lockdown.6,14,25
Association Between Factor Variables and Depression Among Older Adults
Our study found occupational presented that not having a job was associated with depression. As job is a crucial way to earn a living, unemployed participants might have been struggling financially and having a job could alleviate older adults’ problem and increase their self-esteem. Our study demonstrated the consistent finding with previous result from Malaysia,26 which found that depression was associated with unemployment and low-income older participants, as well as from Russia, which demonstrated that participants who were employed at the time of the study had low ORs for depression.27 Moreover, this might imply that not having a job might reflect the diminish of physical activity, since lack of physical activity has a negative effect on mental health outcome especially during the pandemic.28 Hence, our results present that the occupational status of non-workers may have effects on mental health, which should influence policy planners to increase job availability, such as volunteer work, for older adults, as this may decrease their depression symptoms.
In addition, insufficient income was associated with depression symptoms while the amount of income itself was not. Our result is comparable with findings from the US,29,30 showing that participants with lower social and economic resources had a higher Odds Ratios for depression,30 and the aforementioned study in Malaysia.26 Since the financial challenges are associated with poorer mental health outcome, older adult with insufficient income could led to negative impact toward their quality of life and well-being.31 Moreover, the pandemic crisis also affected the worldwide economic activity particularly during the lockdown which leads to economic challenges among older people. Our result might reinforce the policy planners to promote financial aid and security net to provide the daily needs for older adults facing financial challenges, especially during pandemics such as COVID-19, to alleviate their depression symptoms. Regarding housing factors, our study demonstrated that depression had no statistically significant relationship with either living alone or with family. This result is consistent with that of another study in a rural area in Thailand,32 which examined factors associated with depression among community-dwelling older adults with chronic diseases. This consistency in results might be underpinned by communication and how older adults keep in touch with others. As there are various ways to interact with others, such as via phone and social media platforms that allow them to communicate with others, hence living on their own was not associated with depression. Furthermore, the factor underlined in the housing factor could be loneliness, which is associated with depression.33 Further studies could investigate loneliness during a pandemic and its effect on depression.
Regarding the factors related to underlying disease, our results showed that diabetes mellitus, hypertension, dyslipidemia, heart disease, kidney disease, and osteoporosis, as well as the presence of two or more underlying diseases, were not statistically associated with depression. This could be because the participants, who attended a family medicine clinic, had stable conditions. Furthermore, the treatment of non-communicable diseases was well managed in cooperation with tertiary prevention programs. This result is comparable with that of a study among community-dwelling older adults demonstrating no association between chronic diseases such as diabetes and depression.32
Smoking and alcohol intake over 10 years period were not associated with depression. This finding is similar to the finding of Japanese study using the Geriatric Depression Scale demonstrating smoking status and current alcohol drinking were not associated with depression symptoms.34 Still, these two similar findings cannot clarify the causal link of smoking status and alcohol consumption with depression. Finally, in terms of socio-demographics including gender, age, marital status, education, income level, and history of COVID-19 infection among the participants and their communities were not associated with depression symptoms. The results regarding gender, age, marital status, education, and income level are consistent with those from another study.22 Although a history of COVID-19 infection among the participants and their communities was not associated with depression symptoms, the factors that we included had not been examined in the previous literature.
Our study has a few limitations. The survey was conducted at a family medicine clinic during the pandemic; therefore, these findings may not be generalizable to the general population of older adults or those at other clinics. The survey did not include patients using telemedical facilities or those who were unable to attend the clinic during the pandemic.
This study highlights the importance of addressing depression symptoms among older adults, with occupation and income sufficiency being statistically significantly associated with depression. Our study would suggest further that both identification and interventions are needed for older adults to prevent and reduce the risk of depression symptoms. Further studies should use qualitative methods such as in-depth or group interviews to investigate the underlying factors associated with depression in older adults and identify further interventions to decrease their depression symptoms. However, owing to the COVID-19 pandemic, data collection methods may need to be adjusted per the circumstances, such as by using online and telephone interviews. Our participants comprised only older adults who attended a specific family medicine clinic. Further studies could include participants from multiple centers and compare urban and rural areas to evaluate the factors associated with depression. Thus, the government should provide support in these areas to prevent a humanitarian crisis.
Implications for Research, Practice, and Policy
A geriatric depression screening tool should be applied to every older adult attending a primary care clinic, and those in high-risk groups, such as non-workers and those with insufficient incomes, should be monitored for early detection and prompt treatment. In addition, health promotion programs for older adults should be advocated during the COVID-19 pandemic to promote mental health and well-being and prevent depression. Moreover, policies planner could promote job availability and establish financial aid for older adults in high-risk group to diminish depression symptoms during events such as the COVID-19 pandemics.
Conclusion
During the COVID-19 pandemic, factors such as occupation and income sufficiency were the majority on depression symptoms prevalence in urban areas, Thailand. Depression can lead to deteriorations in health, quality of life, and well-being. The pandemic may alert healthcare personnel to the need for early recognition of psychological problems in older adults when stressful events occur. Policy planner could provide intervention such as increasing job availability and establishing financial aid policies that might ameliorate depression symptoms in high-risk groups during the events such as the COVID-19 pandemic.
Abbreviations
COVID-19, coronavirus disease; TGDS-15, The 15-item Thai Geriatric Depression Scale; WHO, World Health Organization; OR, odds ratio; CI, confidence interval.
Data Sharing Statement
The data sets generated and analyzed during the current study are not publicly available due to identifiable information but are available from the corresponding author on reasonable request answering the survey.
Ethical Approval
This study was approved by the ethics committees of Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand (Approval no. COA 121/2564). The Institutional Review Board of the Faculty of Medicine Vajira Hospital is in full compliance with the international guidelines for human research protection as Declaration of Helsinki, The Belmont Report, CIOMS Guideline and International Conference on Harmonization in Good Clinical Practice (ICH-GCP).
Acknowledgments
The authors would like to acknowledge the older adults who attended a family medicine clinic at the Faculty of Medicine Vajira Hospital, Bangkok, Thailand, from July to October 2021. This research was granted from Faculty of Medicine, Vajira Hospital and Navamindhradhiraj University Research Fund for the manuscript and pay for publication.
Author Contributions
All authors read and approved the final manuscript. ATmade a significant contribution to the work reported, conception, study design, execution, acquisition of data, analysis, interpretation, and drafting.BM made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, execution, acquisition of data, analysis and interpretation, revising or critically reviewing the article; gave final approval of the version to be published. All authors have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Supplementary Material
Additional File 1. The full English language version of the questionnaire.
Funding
This research was granted from Faculty of Medicine, Vajira Hospital and Navamindhradhiraj University Research Fund for the manuscript and pay for publication.
Disclosure
The authors declare no potential conflicts of interest with respect to this research and authorship.
References
1. Foundation of Thai Gerontology Research and Development Institute. Situation of the Thai Elderly 2018. Bangkok: Duantula; 2019.
2. World Health Organization. Mental Health of Older Adults. Geneva: World Health Organization; 2017.
3. World Health Organization. Coronavirus Disease 2019 (COVID19) Situation Report by World Health Organization. Geneva: World Health Organization; 2020.
4. Kunno J, Supawattanabodee B, Sumanasrethakul C, Wiriyasivaj B, Kuratong S, Kaewchandee C. Comparison of different waves during the COVID-19 pandemic: retrospective descriptive study in Thailand. Adv Prev Med. 2021;2021:5807056. doi:10.1155/2021/5807056
5. Kunno J, Supawattanabodee B, Sumanasrethakul C, et al. Effect of Covid-19 pandemic on gender associated with risk factors: a retrospective data analysis, Thailand. Rocz Panstw Zakl Hig. 2022;73(3):333–340. doi:10.32394/rpzh.2022.0220
6. Nobari H, Fashi M, Eskandari A, Villafaina S, Murillo-Garcia Á, Pérez-Gómez J. Effect of COVID-19 on health-related quality of life in adolescents and children: a systematic review. Int J Environ Res Public Health. 2021;18(9):4563. doi:10.3390/ijerph18094563
7. Washif JA, Farooq A, Krug I, et al. Training during the COVID-19 lockdown: knowledge, beliefs, and practices of 12,526 athletes from 142 countries and six continents. Sports Med. 2022;52(4):933–948. doi:10.1007/s40279-021-01573-z
8. Motsamai TB, Mhaka-Mutepfa M. Depression: determinants that influence the mental health of older people (60 years +) in Botswana. Gerontol Geriatr Med. 2022;8:23337214211053121. doi:10.1177/23337214211053121
9. Briggs R, McDowell CP, De Looze C, Kenny RA, Ward M. Depressive symptoms among older adults pre- and post-COVID-19 pandemic. J Am Med Dir Assoc. 2021;22(11):2251–2257. doi:10.1016/j.jamda.2021.09.003
10. Levkovich I, Shinan-Altman S, Essar Schvartz N, Alperin M. Depression and health-related quality of life among elderly patients during the COVID-19 pandemic in Israel: a cross-sectional study. J Prim Care Commun Health. 2021;12:2150132721995448. doi:10.1177/2150132721995448
11. Hossain MM, Sultana A, Purohit N. Mental health outcomes of quarantine and isolation for infection prevention: a systematic umbrella review of the global evidence. Epidemiol Health. 2020;42:e2020038. doi:10.4178/epih.e2020038
12. Lai J, Ma S, Wang Y, et al. Factors associated with mental health outcomes among health care workers exposed to Coronavirus Disease 2019. JAMA Netw Open. 2020;3(3):e203976. doi:10.1001/jamanetworkopen.2020.3976
13. Dubey S, Biswas P, Ghosh R, et al. Psychosocial impact of COVID-19. Diabetes Metab Syndr. 2020;14(5):779–788. doi:10.1016/j.dsx.2020.05.035
14. Amerio A, Lugo A, Stival C, et al. COVID-19 lockdown impact on mental health in a large representative sample of Italian adults. J Affect Disord. 2021;292:398–404. doi:10.1016/j.jad.2021.05.117
15. Charoensakulchai S, Usawachoke S, Kongbangpor W, et al. Prevalence and associated factors influencing depression in older adults living in rural Thailand: a cross-sectional study. Geriatr Gerontol Int. 2019;19(12):1248–1253. doi:10.1111/ggi.13804
16. Fiske A, Wetherell JL, Gatz M. Depression in older adults. Annu Rev Clin Psychol. 2009;5(1):363–389. doi:10.1146/annurev.clinpsy.032408.153621
17. Taylor WD, Solomon CG. Clinical practice. Depression in the elderly. N Engl J Med. 2014;371(13):1228–1236. doi:10.1056/NEJMcp1402180
18. Wongpakaran N, Wongpakaran T, Van Reekum R. The use of GDS-15 in detecting MDD: a comparison between residents in a Thai long-term care home and geriatric outpatients. J Clin Med Res. 2013;5(2):101–111. doi:10.4021/jocmr1239w
19. Almeida OP. Prevention of depression in older age. Maturitas. 2014;79(2):136–141. doi:10.1016/j.maturitas.2014.03.005
20. Daniel WW. Biostatistics: A Foundation of Analysis in the Health Sciences.
21. Wongpakaran N, Wongpakaran T. Prevalence of major depressive disorders and suicide in long-term care facilities: a report from northern Thailand. Psychogeriatrics. 2012;12(1):11–17. doi:10.1111/j.1479-8301.2011.00383.x
22. Shin C, Park MH, Lee SH, et al. Usefulness of the 15-item geriatric depression scale (GDS-15) for classifying minor and major depressive disorders among community-dwelling elders. J Affect Disord. 2019;259:370–375. doi:10.1016/j.jad.2019.08.053
23. Anantapong K, Wiwattanaworaset P, Sriplung H. Association between social support and frailty among older people with depressive disorders. Clin Gerontol. 2020;43(4):400–410. doi:10.1080/07317115.2020.1728002
24. Wee LE, Yong YZ, Chng MW, et al. Individual and area-level socioeconomic status and their association with depression amongst community-dwelling elderly in Singapore. Aging Ment Health. 2014;18(5):628–641. doi:10.1080/13607863.2013.866632
25. Ambrosetti J, Macheret L, Folliet A, et al. Impact of the COVID-19 pandemic on psychiatric admissions to a large Swiss emergency department: an observational study. Int J Environ Res Public Health. 2021;18(3):1174. doi:10.3390/ijerph18031174
26. Leong OS, Ghazali S, Hussin EOD, et al. Depression among older adults in Malaysian daycare centres. Br J Community Nurs. 2020;25(2):84–90. doi:10.12968/bjcn.2020.25.2.84
27. von Fingerhut G, Mizukami K, Yam D, et al. Social and physical factors related to depression in the older population of Siberia, Russia: a cross-sectional study. BMC Geriatr. 2021;21(1):272. doi:10.1186/s12877-021-02225-7
28. Trabelsi K, Ammar A, Masmoudi L, et al. Sleep quality and physical activity as predictors of mental wellbeing variance in older adults during COVID-19 lockdown: ECLB COVID-19 international online survey. Int J Environ Res Public Health. 2021;18(8):4329. doi:10.3390/ijerph18084329
29. Rudenstine S, McNeal K, Schulder T, et al. Depression and anxiety during the COVID-19 pandemic in an urban, low-income public university sample. J Trauma Stress. 2021;34(1):12–22. doi:10.1002/jts.22600
30. Ettman CK, Abdalla SM, Cohen GH, Sampson L, Vivier PM, Galea S. Prevalence of depression symptoms in US Adults before and during the COVID-19 pandemic. JAMA Netw Open. 2020;3(9):e2019686. doi:10.1001/jamanetworkopen.2020.19686
31. Samuel LJ, Wright R, Granbom M, et al. Community-dwelling older adults who are low-income and disabled weathering financial challenges. Geriatr Nurs. 2021;42(4):901–907. doi:10.1016/j.gerinurse.2021.04.025
32. Sonthitham K, Palapol T, Injimpa C, Sayeun C, Phengphol N, Jantanam W. Factors correlated with depression among the elderly people with chronic disease in community. J Roi Et Rajabhat Univ. 2020;14(2):192–204.
33. Singh A, Misra N. Loneliness, depression and sociability in old age. Ind Psychiatry J. 2009;18(1):51–55. doi:10.4103/0972-6748.57861
34. Tsutsumimoto K, Makizako H, Doi T, et al. Prospective associations between sedentary behaviour and incident depressive symptoms in older people: a 15-month longitudinal cohort study. Int J Geriatr Psychiatry. 2017;32(2):193–200. doi:10.1002/gps.4461
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Psychological Impact of Quarantine During the COVID-19 Pandemic on Quarantined Non-Healthcare Workers, Quarantined Healthcare Workers, and Medical Staff at the Quarantine Facility in Saudi Arabia
Alfaifi A, Darraj A, El-Setouhy M
Psychology Research and Behavior Management 2022, 15:1259-1270
Published Date: 17 May 2022
Factors Affecting the Psychological Well-Being of Health Care Workers During the COVID-19 Crisis
Alharthi MH, Alshomrani AT, Bazaid K, Sonpol HMA, Ibrahim IAE, Alashkar AM
Psychology Research and Behavior Management 2022, 15:1931-1942
Published Date: 28 July 2022
Falls Among Older Adults During the COVID-19 Pandemic: A Multicenter Cross-Sectional Study in Vietnam
Nguyen HT, Nguyen CC, Le Hoang T
Clinical Interventions in Aging 2022, 17:1393-1404
Published Date: 21 September 2022
Pre- and Post-Pandemic (COVID-19) Mental Health of International Students: Data from a Longitudinal Study
Jamshaid S, Bahadar N, Jamshed K, Rashid M, Imran Afzal M, Tian L, Umar M, Feng X, Khan I, Zong M
Psychology Research and Behavior Management 2023, 16:431-446
Published Date: 15 February 2023
Depression Among University Students in Jordan After the COVID-19 Pandemic: A Cross-Sectional Study
Alhemedi AJ, Qasaimeh MG, Abdo N, Elsalem L, Qaadan D, Alomari E, lssa Q, Alhadeethi M, Abdul Kareem HM, Almasri A, Elkhateeb O, Naser AY
Psychology Research and Behavior Management 2023, 16:4237-4249
Published Date: 18 October 2023