Back to Journals » Risk Management and Healthcare Policy » Volume 13
Prevalence and Drivers of Self-Medication Practices among Savar Residents in Bangladesh: A Cross-Sectional Study
Authors Moonajilin MS, Mamun MA ![]() , Rahman ME
, Rahman ME ![]() , Mahmud MF, Al Mamun AHMS, Rana MS, Gozal D
, Mahmud MF, Al Mamun AHMS, Rana MS, Gozal D ![]()
Received 31 March 2020
Accepted for publication 12 June 2020
Published 8 July 2020 Volume 2020:13 Pages 743—752
DOI https://doi.org/10.2147/RMHP.S256272
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Mst Sabrina Moonajilin,1 Mohammed A Mamun,1,2,* Md Estiar Rahman,1 Md Firoz Mahmud,1 AHM Shamim Al Mamun,1 Md Sajib Rana,1 David Gozal3,*
1Department of Public Health and Informatics, Jahangirnagar University, Dhaka, Bangladesh; 2Undergraduate Research Organization, Dhaka, Bangladesh; 3Child Health Research Institute, Department of Child Health, University of Missouri School of Medicine, Columbia, MO 65201, USA
*These authors contributed equally to this work
Correspondence: David Gozal
Child Health Research Institute, Department of Child Health, University of Missouri School of Medicine, Columbia, MO 65201, USA
Email [email protected]
Background: Self-medication practice (SMP) is widely adopted among residents of such countries as Bangladesh. However, the major determinants of SMP have only scarcely been evaluated. Therefore, this cross-sectional study aimed to fill this knowledge gap by assessing the prevalence and determining factors of SMP.
Methods: A convenience sample of individuals residing in Savar (Dhaka, Bangladesh) > 16 years of age and suffering from an illness > 2 months underwent face-to-face interviews during January–February, 2019.
Results: Among 520 interviewees fulfilling entry criteria, the prevalence of SMP was reported as 60.2%. Drug shops, previous knowledge or prescription, and consulting with peers (friends or relatives) were the most sought sources of SMP, whereas simple illness, higher consulting fees, unsatisfactory health-care services, and delayed access were reported as the motives. From the regression analysis, the sociodemographic risk factors of SMP were reported as being older (compared to < 18 years), married, illiterate (compared to having higher education), having engaged in any occupation (ie, service, business, homemaker, and others compared to student), and suffering from chronic illness.
Conclusion: SMP is highly prevalent and exhibits significant socioeconomic determinants. Development of proper health care–access systems and public education should be implemented to reduce the rate of SMP.
Keywords: self-medication practice, prevalence, risk factors, sociodemographic, rural Bangladeshi people
Plain-Language Summary
Self-medication is a common, yet deleterious approach to disease management, and may lead to substantial delays in diagnosis of serious conditions or increase the risk of adverse outcomes. Here, we examined the prevalence of self-medication among residents of Bangladesh and also assessed whether socioeconomic factors played a role. We found an inordinately elevated rate of self-medication among Dhaka residents and that socioeconomic factors accounted for a significant proportion of such practice. We believe that improved access to health care coupled with public education on the risks and dangers of self-medication are urgently needed.
Introduction
The term “medication” usually refers to the act of consuming medicines for prevention and treatment of illness and diseases,1 whereas “self-medication” (SM) is defined as the selection and use of medicines by an individual to treat self-diagnosed physical and psychological ailments without a health-care provider’s supervision.2–4 SM usually manifests as the use of herbs and medicines that are available in the home, taking advice from friends or relatives pertaining to the nature and treatment of their condition, or the direct purchase of drugs to address current perceived or real medical problems.5–8 SM practice (SMP) is currently viewed as potentially being both beneficial or deleterious in public health, contingent on the individual practices that are implemented to deal with common health problems. SMP has been favorably advocated by the World Health Organization, and if practiced appropriately can bring about many possible benefits, including financial advantages, self-empowered health care, rapid access to treatment, and self-reliance in the care of minor illness.9–11 However, SMPs can promote the occurrence of drug addiction, enhance the risk of drug interactions and adverse drug reactions, foster the occurrence of drug toxicity, increase resistance to pathogens, waste resources, increase polypharmacy, and ultimately lead to incorrect diagnosis and poor outcomes.3,9,12,13
According to several recent studies, the rate of SMP appears to be increasing due to a number of socioeconomic and lifestyle factors that include ready access to drugs, increased potential to manage certain illnesses through self-care, and greater availability of medicinal products,3,14 in addition to advancing age.15 In addition, when the health-care services available are associated with poor access, uneven distribution of drugs, long distance to hospitals and clinics from home, and elevated physician fees, the likelihood of SMP is further enhanced.5,10 The prevalence of SMP in developing countries is 36.7%–95%.16–20 In Bangladesh, the prevalence of SMP in urban areas among a selected (highly literate) sector of the population is about 16%–81%.5,21–25 The health infrastructure and coverage in the country is clearly suboptimal, and fiscal allocation to national health care is reported as being one of the lowest in the South Asia region (ie, only 2.64% of GDP is spent on health care), such that no health insurance, either national or private, de facto exists.26 Besides, the presence of unethical drug sellers, improper regulation, and the fact that the vast majority of stocked drugs are sold without any prescription has undoubtedly contributed to furthering the prevalence of SMP in Bangladesh.27 One common consequence of SMP in Bangladesh, similar to other countries, has been the emergence of high levels of resistance to commonly used antimicrobials, whereby higher rates of resistant bacterial infections persist, due to lack of appropriate administration of antibiotics in the context of self-administration practices.3,23,28 A recent petition to the High Court of Bangladesh sought juridical decision against immoral drug selling, as up to 80% deaths from infections occurred due to antimicrobial resistance.29
However, all aforementioned studies in Bangladesh were conducted in urban areas and involved overall literate participants (ie, medical or university students), such that these individuals could have increased knowledge and access to SMP when compared to rural parts or poor neighborhoods in urban areas of the country where literacy is highly variable.5,21–24,30 Indeed, both knowledge and education level can have an important impact on SM, whereas illiteracy has been regarded as a silent epidemic in the context of SMP.31–33 For example, 77% of literate people in Bangladesh were reported to seek advice from retail medicine sellers for minor ailments, such as fever, common cold, allergies, and diarrhea,30 but we are unaware of any study evaluating SMP among illiterate people. Moreover, the role of professional occupation in SMP has not been investigated, with all aforementioned studies having been conducted among students. However, students usually have free health-care services available on campus, which should negatively influence the prevalence of SMP. As such, the present study was conducted to evaluate the prevalence of SMP and identify potential sociodemographic factors and other drivers among the residents of Savar Upazila, Dhaka, Bangladesh.
Methods
Study Area and Population
The study site was neighborhood areas of Jahanginagar University in Savar Upazila, Dhaka, Bangladesh, situated about 24 kilometers to the northwest of Dhaka, the capital city. Savar is a municipal area consisting of nine wards and 55(neighborhoods). It is 24.1 km2 and has an estimated population of 124,885 (Figure 1). The existing literacy rate, ie, capable of writing one’s name, is 58.2% in this area.
Study Procedure and Inclusion Criteria
This community-based cross-sectional study using convenience sampling was conducted during January and February 2019. Offline face-to-face interviews were conducted in neighborhoods (ie, homes and schools) and working places of Savar. Of the 930 individuals approached, 800 aged >16 years completed the survey. Incorporation of an inclusion criterion consisting of “being ill over the last 2 months”, indicative of having severe disabling long-term medical or psychological conditions (eg, intellectual deficits, comorbid medical conditions, child or parental psychiatric conditions)14 led to the retention of 520 participants (mean age 40.1±13.6 years, 55.6% male) whose interview responses were included in the final analysis.
Measurements
After preliminary observations and review of the literature, a semistructured questionnaire was developed and administered by trained interviewers under the supervision of the principal investigator. The questionnaire required approximately 30 minutes to complete, and consisted of three parts: sociodemographics, common diseases and care-seeking attitudes, and sources and motives of SM (see Supplemental Online Appendix).
Sociodemographics
Common sociodemographic information, ie, age, sex, marital status, education level, occupation, and religious status, was gathered. For assessment of educational status, “illiterate” was defined as no writing or reading knowledge, “primary education” completing up to fifth grade, “secondary education” completing up to tenth grade, “higher secondary” completing up to 12th grade, and “12+” studying or graduating from university.34 Common occupations were classified as student, service, business, homemaker, and “other” including farmer, motor-vehicle driver, rickshaw puller, day laborer, etc.
 |
Figure 1 Study location (ie, Savar Upazila, Dhaka, Bangladesh).35 Note: Reprinted from Creative Commons license and disclaimer available from: Hossain S, Hossain S, Ahmed F, Islam R, Sikder T, Rahman A. Prevalence of tobacco smoking and factors associated with the initiation of smoking among university students in Dhaka, Bangladesh. Central Asian Journal of Global Health. 2017;6(1): e244.Creative Commons license and disclaimer available from: http://creativecommons.org/licenses/by/4.0/legalcode“http://creativecommons.org/licenses/by/4.0/legalcode |
Care-Seeking Attitudes and Self-Medication
Participants were asked if any diseases had affected them over the preceding 2 months (the short period was implemented to reduce recall bias). For accessing health care–seeking attitudes, we used categories of no action taken, consultation with health-care provider, and SM. SM was defined as: “Did you consume medicines by seeking information about drugs from such sources as drugstores, previous experience or prescription, friends or relatives, mass and social media without interaction or prescription of a health-care provider?”5 Regarding motives for SM, inadequate and dissatisfactory health services near residence, higher cost of consultation with physician, simple illness, lack of time, and others were evaluated.
Ethical Issues
The study was approved by the Biosafety, Biosecurity, and Ethical Committee of Jahangirnagar University (reference BBEC, JU/M 2019[1]4), and conducted in accordance with the Declaration of Helsinki. The purpose of the interview was clearly explained to all prospective study subjects, and formal written and/or verbal (only for the illiterate) consent was obtained. Parental consent was obtained for adolescents. Study subjects were informed that the information collected would be kept anonymous and that their role in the study would be completely voluntary.
Statistical Analysis
Data were analyzed using SPSS version 22.. Descriptive statistics (eg, frequencies, percentages, means, and χ2) were derived. All categorical variables were compared using χ2. To identify predictors of SMP, all variables in bivariate analyses were entered into a binary logistic regression model, both unadjusted and adjusted, with SMP as the dependent variable. The results of logistic regression are reported with 95% CIs, and all tests were two-tailed with statistical significance set at 0.05.
Results
Of the 800 participants who completed the interviews, only 520 subjects had suffered from illness in the preceding 2-month period and were retained for final analysis. Their mean age was 40.1±13.6 years, 55.6% were male, and most (48.8%) were in the 18- to 24–year age-group. About 58.3% of the respondents were single, 40.6% had an educational level of higher secondary or more, 43.1% were students, and 94.6% were Muslim. Approximately 23% of respondents reported having chronic illness (Table 1).
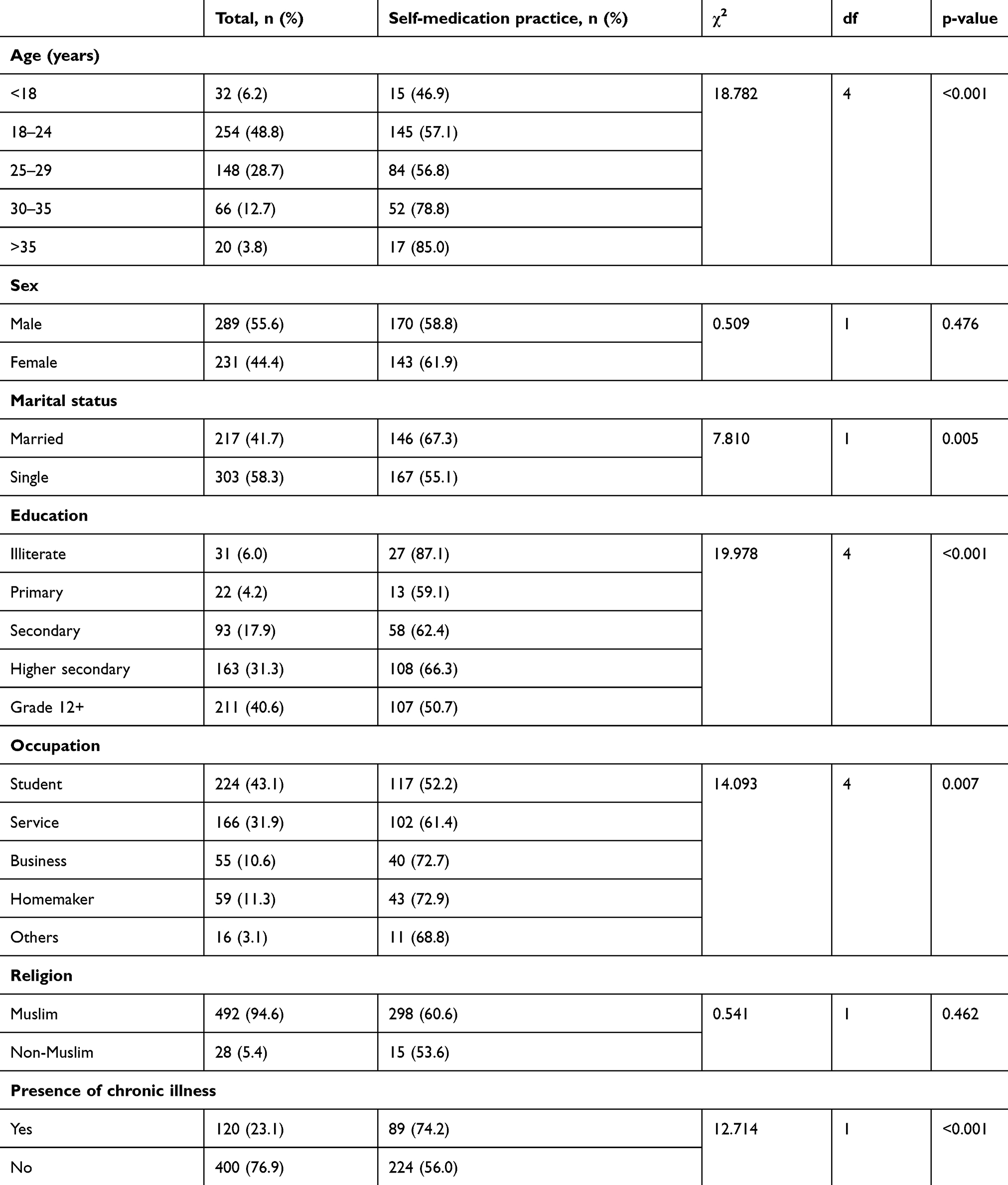 |
Table 1 Distribution of sociodemographic characteristics and health-related factors with SMP (n=520) |
Interventional measures initiated by respondents during their illness are presented in Table 2. Results revealed that 60.2% of respondents (n=313) had used SMP. The most common sources of SM were drugstores (32.3%), previous experience (26.2%), advice of friends or relatives (19.2%), mass media (12.8%), and the Internet (9.6%). Moreover, perception of minor illness (58.5) and cost of consultations with doctors (19.2%) were the predominant reasons for SMP among respondents (Table 2).
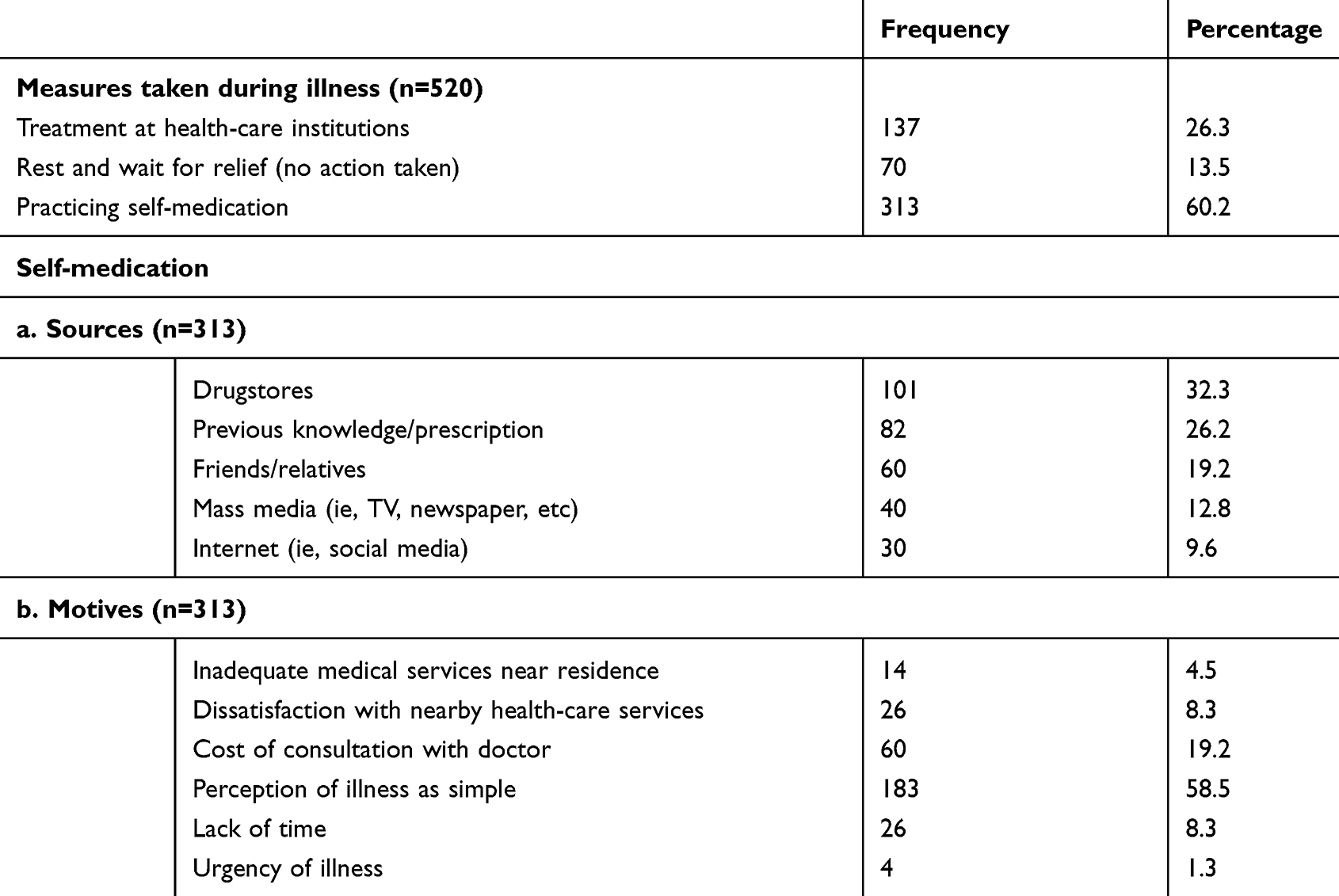 |
Table 2 Measures taken by participants with acute or chronic illness in preceding 2months |
Age, marital status, education level, occupation, presence of chronic illness, and satisfaction with nearby health services were significantly associated with SMP (p<0.05). There were no significant differences in SMP between males and females. SMP increased with increasing age (<18-year-old group served as control; χ2=18.782, df=4; p<0.001). The prevalence of SMP was higher among married respondents (67.3%) than those who were single (55.5%, χ2=7.810, df=1; p=0.005). Subjects with higher education were less likely to engage in SMP compared to illiterate or lower-education participants (χ2=19.978, df=4; p<0.001). Regarding profession, students (52.2%) were less likely to engage in SMP, whereas approximately 73% of nonstudent respondents practiced SMP if they were businessmen or housewives, 61.4% if they were in service jobs, and 68.8% in those with other occupations (χ2=14.093, df=4; p=0.007). A significantly higher percentage of SMP was reported by respondents with chronic illnesses (74.2% vs 56%, χ2=12.714, df=1; p<0.001; Table 1).
Logistic regression analysis (unadjusted model) further showed that higher age (>35, 30–35, 25–29, and 18–24 years vs <18 years, respectively: OR 6.42, 95% CI 1.57–26.31; OR 4.21, 95% CI 1.69–10.47; OR 1.49, 95% CI 0.69–3.20; OR 1.51, 95% CI 0.72–3.15), being married (OR 1.67, 95% CI 1.165–2.407), no education (OR 6.56, 95% CI 2.22–19.40 vs grade 12+), occupation (compared to students: service, OR 1.46, 95% CI 0.97–2.19; businessman, OR 2.44, 95% CI 1.27–4.67; homemaker, OR 2.46, 95% CI 1.31–4.62; other, (OR 2.01, 95% CI 0.68–5.98)), and presence of chronic illness (OR 2.26, 95% CI 1.43–3.55) were all significant and independent predictors in implementation of SMP over the preceding 2 months among respondents (p<0.05, Table 3).
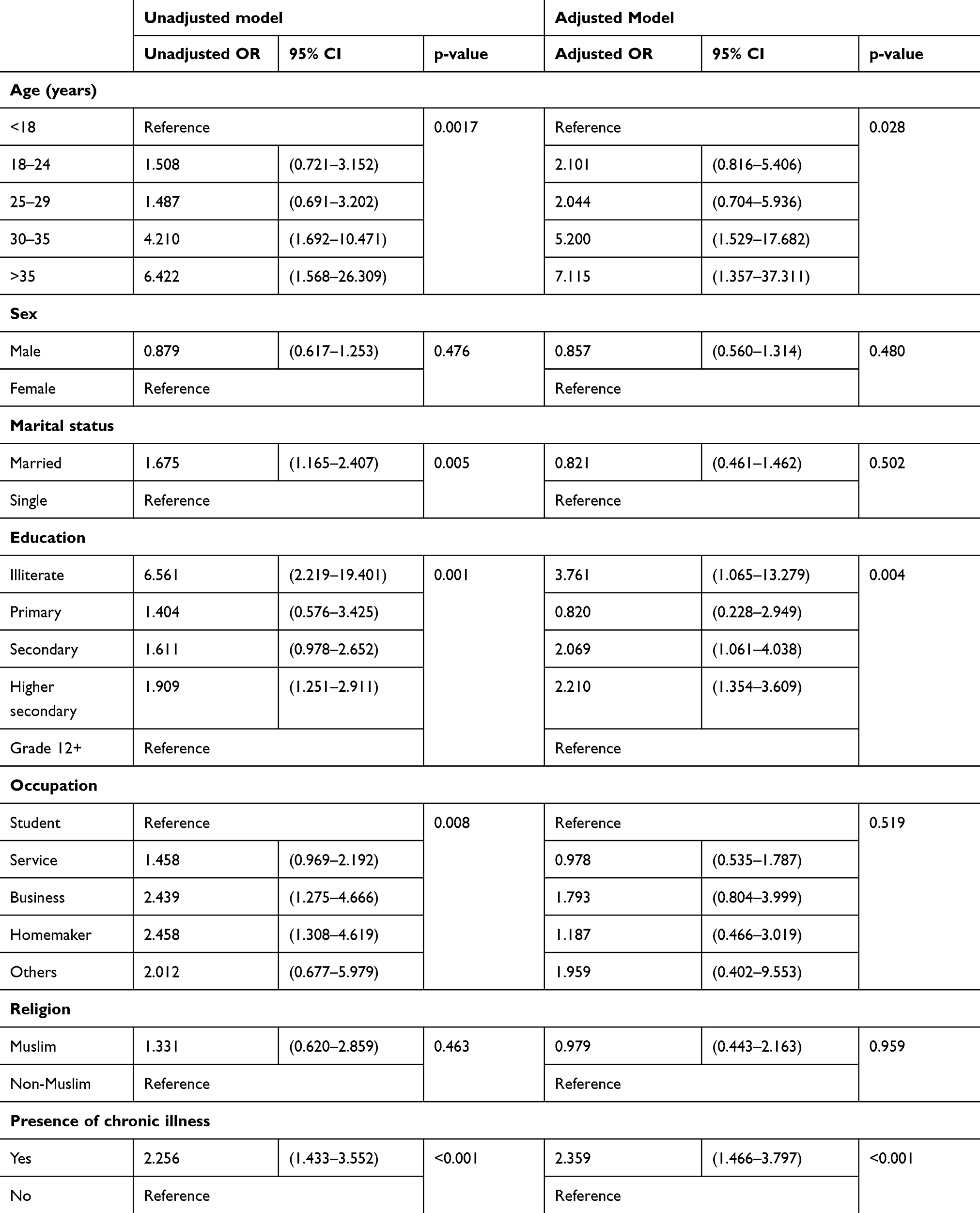 |
Table 3 Logistic regression analysis of sociodemographic characteristics and health-related factors with SMP (n=520) |
Discussion
SMP is a fairly common occurrence in developing countries, such as Bangladesh, where evaluation by a health-care provider is relatively costly and difficult to assume by a large majority in light of their monthly income and cost of living expenses.13,22 However, the role of age, education, occupation, and other sociodemographic factors in SMP has not been explored to date. Therefore, the current study provides initial observations on the determinants of SMP among a cohort of residents of Savar, Dhaka in Bangladesh.
To obviate the issues of no-recall or recall bias, we focused only on responses obtained from participants who had experienced illness during the 2 months preceding the survey. In these subjects, the prevalence of SMP was 60.2%, higher than that reported in several studies in Bangladesh involving students. Indeed, SMP prevalence was 47% among medical students in Dhaka22 and 16% among private university students in the same city.21 However, several other studies have shown a very wide range of SMP. In a study conducted by Seam et al,5 prevalence as high as 81% was found among undergraduate students attending five universities located in different regions of the country, whereas prevalence of 81.4% was reported among medical students in Dhaka.25 Furthermore, Biswas et al found SMP prevalence of 26.7% for antibiotics and 73.3% for other medication,23 and 62.2% of children (aged 0–12 years) residing in Dhaka have been reported as engaging in SMP by their parents or caretakers.24 Moreover, SMP prevalence varies greatly around the world, eg, up to 78.6% in India,1,15,36 61.2% in Pakistan,37 up to 94.5% in Saudi Arabia,2,4,17 up to 39% in Ethiopia,10,14 98% in Palestine,38 36.7% in Oman,16 53.4% in Italy,39 83% in Iran,20 79.9% in Serbia,18 78.5% in Jordan,40 and up to 73.5% (antibiotics) in China.41. Therefore, the prevalence of SMP found in the current study is clearly within the ranges previously reported elsewhere, although the time frame of SMP has not been compared.
Bangladesh is a country in which no systematic policies and regulations regarding proper drug administration, distribution, and control of drug sales are applied.23 As such, anyone can buy drugs without the need for a medical prescription. This situation leads to many drugstores acting in a consulting capacity to the public.22 Accordingly, it was not surprising that one of the principal sources of SMP resides in drugstores, a finding that has been corroborated by many studies conducted in different parts of the world.1,2,14,22 However, other important factors in this study leading to SMP included suffering from a simple illness (eg, fever, acidity, common cold, headache, abdominal pain, cough, back pain). The rationale for individuals with simple acute illnesses not willing to pay the relatively onerous fee of a health-care provider is quite obvious, yet for more complex or protracted conditions, the high rate of SMP is definitely concerning.1,5,10,14,16,22 Other reasons for SMP, including dissatisfaction with existing health-care services, lengthy waiting times to access health-care facilities, or inadequate medical services near residence, were also apparent, similar to previous reports.5
Herein, the prevalence of SMP increased with age, suggesting that older individuals are more experienced in handling common conditions, and when affected by minor or even chronic illness are more likely to resort to SMP.20,42 It is also worth noting that we found that individuals who suffered from the same illness repeatedly were more likely to adopt SMP and use previously prescribed drugs.2 We observed that marital status influenced SMP rates, with being married being associated with increased SMP rates,18,20,42 likely reflecting some degree of collinearity, since married status is more likely with older age and also with employment in which employed and particularly busier individuals may not have the necessary time to consult with health-care providers, particularly when simple ailments are affecting them.2
Illiterate individuals were significantly more likely to use SMP, with nearly a sevenfold increase in odds of SMP compared to those with education level of grade 12+. Education-attainment levels have been found to be significant predictors of SMP in other studies.32 Usually, illiterate individuals are less aware of potential side effects linked to concurrent use of medications and also less likely to scrutinize whether they are obtaining proper treatment.31,33 These issues predispose them to frequent purchases of medications suggested by drugstore employees, without seeking physician consultation or prescription.5,22,31 However, contrary to our findings, we should also point out that seeking information from online sources, magazines, or periodicals can promote SMP behavior among literate individuals.43
Limitations and Further Study
There were a number of limitations to this study. First, it was cross-sectional without any interventions seeking to alter SMP behaviors that might have provided improved insights into its determinants. Additionally, we did not consider detail in motives for SMP for each separate condition, but rather collapsed our findings by aggregating them over a period of 2 months. It is also possible that despite the relatively large sample, sampling approaches, and whether the cohort was representative of the population being evaluated might have reduced its generalizability to both Bangladesh and other countries. Moreover, self-reporting data aboutSM in the preceding 2 months requires recall and brings the possibility of desirability bias, which could have affected our findings. Potential extraneous influence by fellow respondents cannot be ruled out with certainty, even if precautions were taken for respondents to complete their survey independently. Therefore, this study suggests a need for further investigations among a nationwide representative population of the country in consideration of the yielded factors.
Implications of the Study
This study provides a static evaluation of the health care–delivery system in Bangladesh, with particular emphasis on the attitudes and practices of SM. Only 26.3% of participants had accessed health-care institutions for treatment and care, which illustrates the fact that SMP is driven by poor access, among other factors. Moreover, the rate of SMP was notably high, and several important risk factors were identified, which might be of interest and useful to policy-makers regarding more formal regulation of SMP. Indeed, such initiatives as those aiming to increase health education, social awareness, awareness regarding the illness, and which illnesses can be safely managed initially by SMP and which are not adequate for SMP could optimize the utilization of SMP without necessarily leading to some of its negative outcomes.
Conclusion
This study revealed a high rate of SMP among the general population of Savar Upazila in Bangladesh, an observation that should draw the attention of policy-makers and other health-care organizations to this issue, while providing insights into socioeconomic determinants of such behaviors. Our findings should encourage greater exploration of the role of SM in health care, particularly in countries with a relatively inaccessible health infrastructure, while also enabling public information channels on the potential hazards posed by SMP.
Acknowledgment
The authors would like to thank all the participants.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ahmad A, Patel I, Mohanta GP, Balkrishnan R. Evaluation of self medication practices in rural area of town Sahaswan at Northern India. Ann Med Health Sci Res. 2014;4(8):73–78. doi:10.4103/2141-9248.138012
2. Alghanim SA. Self-medication practice among patients in a public health care system. East Mediterr Health J. 2011;17(05):409–417. doi:10.26719/2011.17.5.409
3. Montastruc J-L, Bondon-Guitton E, Abadie D, et al. Pharmacovigilance, risks and adverse effects of self-medication. Therapie. 2016;71(2):257–262. doi:10.1016/j.therap.2016.02.012
4. Al Essa M, Alshehri A, Alzahrani M, et al. Practices, awareness and attitudes toward self-medication of analgesics among health sciences students in Riyadh, Saudi Arabia. Saudi Pharm J. 2019;27(2):235–239. doi:10.1016/j.jsps.2018.11.004
5. Seam M, Bhatta R, Saha B, et al. Assessing the perceptions and practice of self-medication among Bangladeshi undergraduate pharmacy students. Pharmacy. 2018;6(1):6. doi:10.3390/pharmacy6010006
6. Alonso-Castro AJ, Ruiz-Padilla AJ, Ruiz-Noa Y, et al. Self-medication practice in pregnant women from central Mexico. Saudi Pharm J. 2018;26(6):886–890. doi:10.1016/j.jsps.2018.03.008
7. Nikolić G, Stojanović NM, Randjelović PJ, Manojlović S, Radulović NS. An epidemiological study on herbal product self-medication practice among psychotic outpatients from Serbia: a cross-sectional study. Saudi Pharm J. 2018;26(3):335–341. doi:10.1016/j.jsps.2018.01.009
8. Stojanović NM, Samardžić L, Randjelović PJ, Radulović NS. Prevalence of self-medication practice with herbal products among non-psychotic psychiatric patients from southeastern serbia: a cross-sectional study. Saudi Pharm J. 2017;25(6):884–890. doi:10.1016/j.jsps.2017.02.002
9. Shafie M, Eyasu M, Muzeyin K, Worku Y, Martín-Aragón S, Kumar N. Prevalence and determinants of self-medication practice among selected households in Addis Ababa community. PLoS One. 2018;13(3):e0194122. doi:10.1371/journal.pone.0194122
10. Suleman S, Ketsela A, Mekonnen Z. Assessment of self-medication practices in Assendabo town, Jimma zone, southwestern Ethiopia. Res Social Adm Pharm. 2009;5(1):76–81. doi:10.1016/j.sapharm.2008.04.002
11. WHO. Guidelines for the regulatory assessment of medicinal products for use in self-medication [Internet]; 2000 [
12. Eticha T, Mesfin K, Carvajal A. Self-medication practices in Mekelle, Ethiopia. PLoS One. 2014;9(5):e97464. doi:10.1371/journal.pone.0097464
13. Nepal G, Bhatta S. Self-medication with antibiotics in WHO Southeast Asian Region: a systematic review. Cureus. 2018;10.
14. Abay SM, Amelo W. Assessment of Self-medication practices among medical, pharmacy, health science students in Gondar University, Ethiopia. J Young Pharm. 2010;2(3):306–310. doi:10.4103/0975-1483.66798
15. Selvaraj K, Kumar SG, Ramalingam A. Prevalence of self-medication practices and its associated factors in Urban Puducherry, India. Perspect Clin Res. 2014;5(1):32–36. doi:10.4103/2229-3485.124569
16. Al Flaiti M, Al Badi K, Hakami WO, Khan SA. Evaluation of self-medication practices in acute diseases among university students in Oman. J Acute Dis. 2014;3(3):249–252. doi:10.1016/S2221-6189(14)60056-1
17. Albatti TH, Alawwad S, Aldueb R, Alhoqail R, Almutairi R. Self-medication among adolescents 13–18 years old in Riyadh, Kingdom of Saudi Arabia, from 2014 to 2015. Int J Pediatr Adolesc Med. 2016;4(1):19–25. doi:10.1016/j.ijpam.2016.05.001
18. Lukovic JA, Miletic V, Pekmezovic T, et al. Self-medication practices and risk factors for self-medication among medical students in Belgrade, Serbia. PLoS One. 2014;9(12):e114644. doi:10.1371/journal.pone.0114644
19. Ahmed N, Azam NK. Traditional knowledge and formulations of medicinal plants used by the traditional medical practitioners of Bangladesh to treat schizophrenia like psychosis. Schizophr Res Treat. 2014;2014:1–10. doi:10.1155/2014/679810
20. Jafari F, Khatony A, Rahmani E. Prevalence of self-medication among the elderly in Kermanshah-Iran. Glob J Health Sci. 2015;7(2):360–365. doi:10.5539/gjhs.v7n2p360
21. Chowdhury N, Matin F, Chowdhury SFUA. Medication taking behavior of students attending a private university in Bangladesh. Int J Adolesc Med. 2009;21(3):361–370. doi:10.1515/IJAMH.2009.21.3.361
22. Mosaddek ASM, Sharmin ZR, Sharmin R, et al. Practice of self-medication among students of a selected medical college of Dhaka city, Bangladesh. Int Med J. 2017;24:225–229.
23. Biswas M, Roy MN, Manik MIN, et al. Self medicated antibiotics in Bangladesh: a cross-sectional health survey conducted in the Rajshahi City. BMC Public Health. 2014;14(1):847. doi:10.1186/1471-2458-14-847
24. Akter T A study on the prevalence and pattern Self-medication practices in Dhaka [Internet]; East West University. 2017. Available from: http://dspace.ewubd.edu/handle/123456789/1710.
25. Haque S, Alam NN, Mushroor S, Sultana N. Association between knowledge of self medication and adherence among medical students in Dhaka, Bangladesh. Res J Pharm Technol. 2017;10(5):1376–1382. doi:10.5958/0974-360X.2017.00245.1
26. Joarder T, Chaudhury TZ, Mannan I. Universal Health Coverage in Bangladesh: activities, challenges, and suggestions. Adv Public Health. 2019;2019:e4954095. doi:10.1155/2019/4954095
27. Babu MM. Factors contributing to the purchase of over the counter (OTC) drugs in Bangladesh: an empirical study. Internet J Third World Med. 2008;6:9–24.
28. Alghadeer S, Aljuaydi K, Babelghaith S, Alhammad A, Alarifi MN. Self-medication with antibiotics in Saudi Arabia. Saudi Pharm J. 2018;26(5):719–724. doi:10.1016/j.jsps.2018.02.018
29. The Daily Star. Take steps to stop sale of antibiotic drugs without prescriptions, HC tells govt [Internet]; 2019 [
30. Islam MS. Self-medications among higher educated population in Bangladesh: an email-based exploratory study. Internet J Health. 2007;5:20–25.
31. Alam N, Saffoon N, Uddin R. Self-medication among medical and pharmacy students in Bangladesh. BMC Res Notes. 2015;8(1):763. doi:10.1186/s13104-015-1737-0
32. Carrasco‐Garrido P, Jiménez‐García R, Barrera VH, Gil de Miguel A. Predictive factors of self-medicated drug use among the Spanish adult population. Pharmacoepidemiol Drug Saf. 2008;17(2):193–199. doi:10.1002/pds.1455
33. Zafar SN, Syed R, Waqar S, et al. Self-medication amongst university students of Karachi: prevalence, knowledge and attitudes. J Pak Med Assoc. 2008;58:214.
34. Disu TR, Anne NJ, Griffiths MD, Mamun MA. Risk factors of geriatric depression among elderly Bangladeshi people: a pilot interview study. Asian J Psychiatr. 2019;44:163–169. doi:10.1016/j.ajp.2019.07.050
35. Hossain S, Hossain S, Ahmed F, Islam R, Sikder T, Rahman A. Prevalence of tobacco smoking and factors associated with the initiation of smoking among university students in Dhaka, Bangladesh. Cent Asian J Glob Health. 2017;6(1):e244. doi:10.5195/CAJGH.2017.244
36. Kumar N, Kanchan T, Unnikrishnan B, et al. Perceptions and practices of self-medication among medical students in coastal South India. PLoS One. 2013;8(8):e72247. doi:10.1371/journal.pone.0072247
37. Aqeel T, Shabbir A, Basharat H, et al. Prevalence of self-medication among urban and rural population of Islamabad, Pakistan. Trop J Pharm Res. 2014;13(4):627–633. doi:10.4314/tjpr.v13i4.22
38. Sawalha AF. A descriptive study of self-medication practices among Palestinian medical and nonmedical university students. Res Social Adm Pharm. 2008;4(2):164–172. doi:10.1016/j.sapharm.2007.04.004
39. Garofalo L, Di Giuseppe G, Angelillo IF. Self-medication practices among parents in Italy. Biomed Res Int. 2015;2015.
40. Alkhatatbeh MJ, Alefan Q, Alqudah MAY. High prevalence of self-medication practices among medical and pharmacy students: a study from Jordan. Int J Clin Pharmacol Ther. 2016;54(05):390–398. doi:10.5414/CP202451
41. Zhu X, Pan H, Yang Z, Cui B, Zhang D, Ba-Thein W. Self-medication practices with antibiotics among Chinese university students. Public Health. 2016;130:78–83. doi:10.1016/j.puhe.2015.04.005
42. Balbuena FR, Aranda AB, Figueras A. Self-medication in older urban mexicans. Drugs Aging. 2009;26(1):51–60. doi:10.2165/0002512-200926010-00004
43. Kumari R, Kiran K, Kumar D, Bahl R, Gupta R. Study of knowledge and practices of self-medication among medical students at Jammu. JMS SKIMS. 2012;15(2):141–144. doi:10.33883/jms.v15i2.252
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.