Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Prevalence and Correlates of Sleep Problems in Children and Adolescents with Type 1 Diabetes: A Cross-Sectional Study
Authors Alqahtani YA, Shati AA, Dawood SA, Aldosari AA, Amer KA ![]() , Alamri HH, Alqahtani RF, Alamer RA, Alshehri SZ, Althomali RN, Mahmood SE
, Alamri HH, Alqahtani RF, Alamer RA, Alshehri SZ, Althomali RN, Mahmood SE ![]()
Received 21 November 2025
Accepted for publication 1 May 2026
Published 3 June 2026 Volume 2026:19 525998
DOI https://doi.org/10.2147/DMSO.S525998
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mark D. DeBoer
Youssef A Alqahtani,1 Ayed A Shati,1 Samy A Dawood,1 Abdulrahman A Aldosari,2 Khaled A Amer,2 Hend H Alamri,2 Reemah F Alqahtani,2 Rahaf A Alamer,2 Shuruq Z Alshehri,2 Rawan Naif Althomali,2 Syed Esam Mahmood3
1Department of Child Health, College of Medicine, King Khalid University, Abha, Saudi Arabia; 2College of Medicine, King Khalid University, Abha, Saudi Arabia; 3Department of Family and Community Medicine, College of Medicine, King Khalid University, Abha, Saudi Arabia
Correspondence: Syed Esam Mahmood, Department of Family and Community Medicine, College of Medicine, King Khalid University, Abha, Saudi Arabia, Email [email protected]
Background: In children and adolescents with Type 1 Diabetes Mellitus (T1DM), disrupted sleep such as frequent nighttime awakenings can impair daily functioning and glycemic control, creating a harmful cycle that affects overall health and treatment adherence.
Objective: To elucidate the relationships between health-related variables, sociodemographic factors, and the prevalence of sleep problems in children and adolescents with T1DM and to identify significant correlates.
Methods: A cross-sectional study was conducted from January to June 2024, involving 248 children and adolescents with T1DM in Abha, Saudi Arabia. Participants were recruited using consecutive sampling of eligible patients attending the clinic until the sample size of 248 was met. Participants aged 6– 18 years with confirmed T1DM were included, excluding those with other types of diabetes or comorbid sleep problems. Data collection involved validated sleep assessments, demographic surveys, and evaluations of diabetes-related factors during routine clinic visits. Chi-square analysis was employed to assess associations, with statistical significance set at P≤ 0.05 using Python Jupyter Notebook.
Results: Among children with T1DM (mean age 10– 12 years; 86.29% male), 37.5% had sleep problems. About 45.16% had glucose levels between 6– 8 mmol/L, and 48.79% tested daily. Nearly 48% were exposed to household smoking. Significant associations were found between sleep disturbance and guardian marital status (P=0.045), education level (P=0.001), household income (P< 0.001), glucose levels (P< 0.001), testing frequency (P< 0.001), and passive smoking (P=0.001). No link was observed with insulin method or comorbidities.
Conclusion: This study reveals a complex interplay of factors associated with sleep problems in children with T1DM. The findings highlight the importance of considering environmental factors (such as secondhand smoke), socioeconomic status, and glycemic control in T1DM management.
Keywords: sleep problems, children, adolescents, type 1 diabetes mellitus, prevalence, Saudi Arabia
A Letter to the Editor has been published for this article.
Introduction
Type 1 diabetes (T1DM) is a chronic condition characterized by the body’s inability to produce insulin, resulting in high blood glucose levels.1 Managing T1DM involves continuous blood sugar monitoring, insulin therapy, and lifestyle adjustments.2 Beyond glycemic control, individuals with T1DM face psychological and physiological challenges that affect their quality of life.3 Recent studies highlight the importance of assessing sleep quality in this population.
Sleep interacts with multiple biological systems, including the nervous system, regulating behavior, autonomic functions, cognitive processes, development, tissue repair, and energy conservation.4–6 It is a transient unconscious state, susceptible to disruption by various stimuli. The American Academy of Sleep Medicine recommends 7–8 hours of sleep for adults, 8–10 hours for adolescents (13–18 years), and 9–12 hours for school-age children (6–12 years).7,8 However, research shows that 50–70% of teenagers do not meet these sleep duration recommendations.
Pediatric sleep problems affect 25–40% of youth.9–11 Some studies find no sleep differences in adolescents with T1DM,12–14 while others report inadequate sleep in this group. Given sleep’s importance for metabolic health,15–17 this study examines sleep quality in adolescents with T1DM.
The existing literature highlights that adolescents with T1DM often experience disrupted sleep patterns, which are associated with poor glycemic control and adverse health outcomes.18–21 Sleep problems such as sleep-disordered breathing and nocturnal hypoglycemia are increasingly recognized as complicating factors in T1DM management, with evidence suggesting they may impair glycemic control and quality of life.22–25 A recent review in Saudi Arabia emphasizes that sleep disturbances are prevalent among individuals with T1DM and may negatively impact disease management, underscoring the need for routine sleep assessments.26
However, there remains a gap in localized research examining the specific prevalence, risk factors, and correlates of sleep problems among Saudi adolescents with T1DM. Most existing studies are either international or limited in scope within the Saudi context, leaving a critical need to understand these relationships in this population.
This study aims to: (1) assess the prevalence and types of sleep disturbances among adolescents with T1DM in Saudi Arabia; (2) identify sociodemographic, clinical, and psychological factors associated with sleep quality; and (3) explore the relationship between sleep quality, glycemic control, and psychological health to inform targeted interventions and improve clinical outcomes in this population.
Methods
Study Design
This cross-sectional study investigated the prevalence and associated factors of sleep problems among 248 children and adolescents diagnosed with Type 1 Diabetes (T1DM). The study population consisted of individuals aged 6 to 18 years with a confirmed diagnosis of T1DM who attended the Diabetic Center Clinics in Abha, Saudi Arabia, from January to June 2024. Sleep problems included difficulty falling asleep, nighttime awakenings, snoring, daytime sleepiness, and impaired functioning. Assessment of sleep quality was done using Pittsburgh Sleep Quality Index [PSQI]. The PSQI evaluated the sleep over the past month using seven component scores (0–3). These were summed to produce a global score (0–21), where higher scores mean worse sleep quality. The first nine items influenced the score, but item 10 did not.27
Subjects
Inclusion Criteria
- Age between 6 and 18 years.
- Confirmed diagnosis of Type 1 Diabetes.
- Consent from both participants and their guardians.
Exclusion Criteria
- Children with other types of diabetes (eg, Type 2 Diabetes).
- Individuals with previously diagnosed primary sleep disorders (eg, narcolepsy, diagnosed obstructive sleep apnea) prior to study enrollment.
- Inability or refusal to provide informed consent.
Sampling Technique
Participants were recruited using consecutive sampling of eligible patients attending the clinic until the sample size of 248 was met. In the current study, out of 260 eligible participants approached, 248 (95.4%) consented to participate, while 12 (4.6%) declined.
Data Collection
Participants meeting the inclusion criteria were approached during their routine clinic visits. Informed consent was obtained from both the participants and their guardians. The study utilized validated sleep disorder assessment tools, demographic surveys, and examinations of diabetes-related factors. Sleep disorder status was assessed through standardized tools, and data on socioeconomic factors, including average monthly household income and parental education, were collected. Diabetes-related factors such as duration since diagnosis, treatment modalities, and glycemic control were also gathered.
Instruments
A comprehensive set of instruments was employed to assess sleep problems, collect demographic information, and capture diabetes-related factors among children and adolescents with Type 1 Diabetes (T1DM). The survey items were developed from a thorough literature review25,26 and refined by field experts. A pilot test with 30 participants assessed clarity and relevance, leading to adjustments in wording and structure Based on the pilot results, minor adjustments were made to the questionnaire wording to improve clarity, but no substantial changes affecting data collection or analysis were implemented. The pilot responses were excluded from the final responses of the study. Reliability analysis yielded a Cronbach’s alpha of 0.85, indicating strong internal consistency. This structured survey collected information on age, gender, household income, and parental education. Diabetes-specific details, including the duration since T1DM diagnosis, treatment modalities, and glycemic control, were obtained through medical record reviews and participant self-reports.
Sample Size
The sample size is calculated using the following formula:

N = sample size, Z = 1.96 at 95% level of significance and 80% power P = prior prevalence of knowledge of screening tests (59.3%),26 and C = degree of precision (0.05). The margin of error is 6.12%. The estimated minimum sample size is 248.
Data Analysis
Descriptive statistics were used to characterize the study population. Chi-square analysis was employed to assess the association between sleep problems and various factors. Given the cross-sectional nature of the study, the analysis focused on identifying correlations rather than causal risk factors. Confidence intervals (95% CI) were calculated for prevalence rates. The threshold for statistical significance was set at P≤0.05. Statistical analyses were performed using Python Jupyter Notebook version 6.4.5.
Operational Definitions
- Cumulative Glucose Level Over the Past Three Months (Glycated Hemoglobin – HbA1c levels)
Less than 6%: Indicates optimal glycemic control, reflecting well-managed blood glucose levels over the past three months.
6–8%: Represents acceptable or moderate glycemic control, with some room for improvement.
8–12%: Signifies poor glycemic control, indicating that blood glucose levels have been consistently high.
Greater than 12%: Denotes very poor glycemic control, associated with increased risk of complications.
Income Brackets (Monthly Household Income in Saudi Riyals – SR):
- Less than SR5000: Household income below 5000 SR per month.
- SR5000 – SR10,000: Household income between 5000 SR and 10,000 SR per month.
- SR10,000 – SR15,000: Household income between 10,000 SR and 15,000 SR per month.
- More than SR15,000: Household income exceeding 15,000 SR per month.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki, adhered to ethical guidelines and received approval from the Institutional Review Board (IRB) of Diabetic Center Clinics, Abha, Saudi Arabia. Informed consent was obtained from both participants and their legal guardians prior to inclusion in the study.
Results
In Table 1, the study population primarily consisted of males (86.29%) and children aged 10–12 years (43.95%). A significant portion of guardians were single (50.4%). Guardians’ educational levels varied, with a significant proportion holding a Master’s or Bachelor’s degree. Monthly household incomes were relatively evenly distributed across different income brackets.
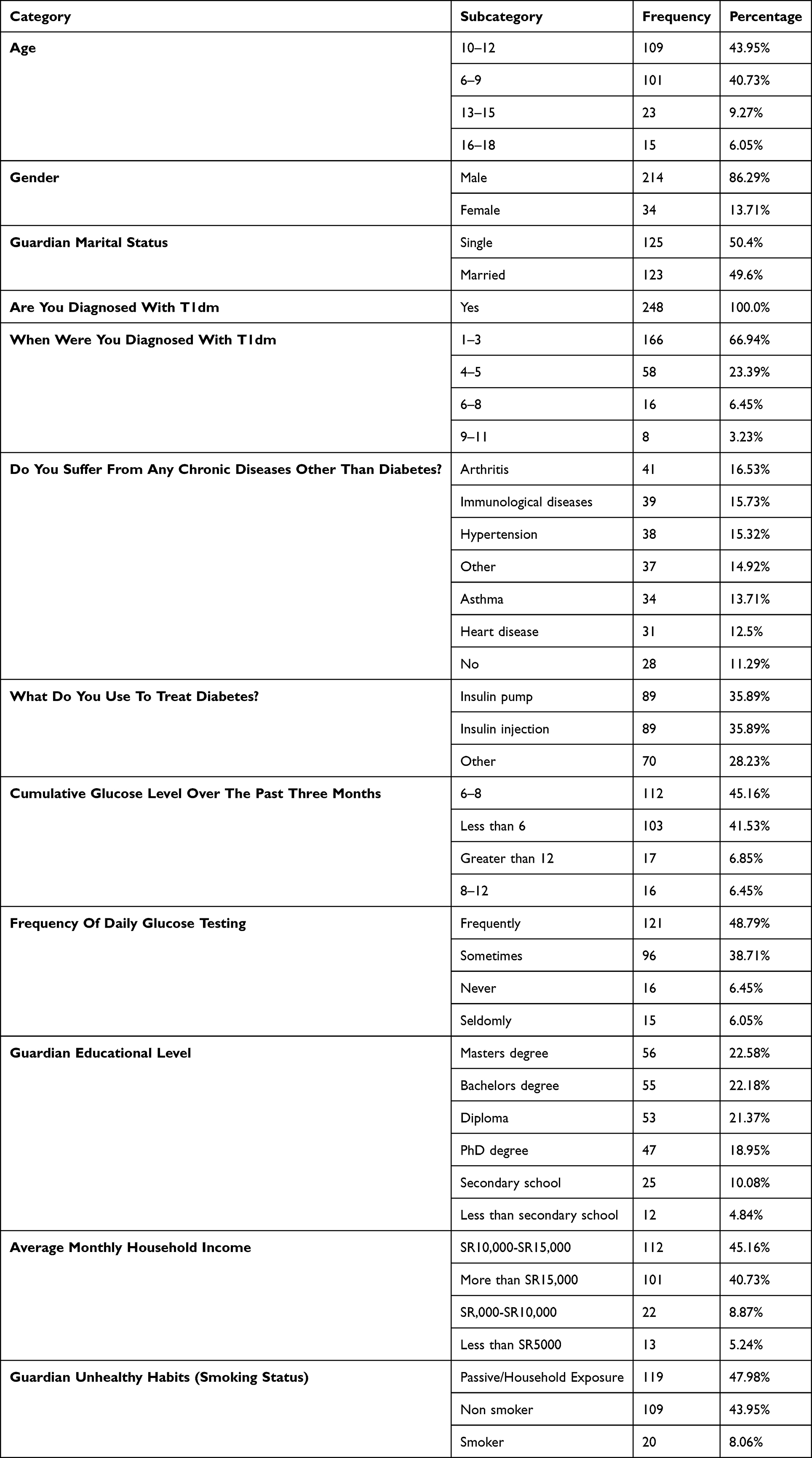 |
Table 1 Demographic, Health, and Lifestyle Profile of Children and Adolescents with Type 1 Diabetes |
All respondents were diagnosed with Type 1 Diabetes (T1DM), with the majority diagnosed within the past 1–3 years (66.94%). Common chronic diseases co-occurring with T1DM included arthritis (16.53%), immunological disorders (15.73%), and hypertension (15.32%). Treatment modalities for diabetes were equally split between insulin pumps and injections (35.89% each). Cumulative glucose levels varied, with 45.16% of respondents having levels between 6–8. Frequent daily glucose testing was reported by 48.79% of participants. Regarding lifestyle factors, unhealthy Habits (passive/guardian smoking status) were prevalent, with 47.98% of respondents reported to have household exposure (Table 1).
A considerable percentage of children and adolescents with Type 1 Diabetes Mellitus (T1DM) in Abha city, Saudi Arabia, experience sleep problems. Specifically, 37.5% (93 individuals; 95% CI: 31.5–43.5%) of the study population were found to have sleep problems, while 62.5% did not exhibit any signs of sleep disturbance (Table 2).
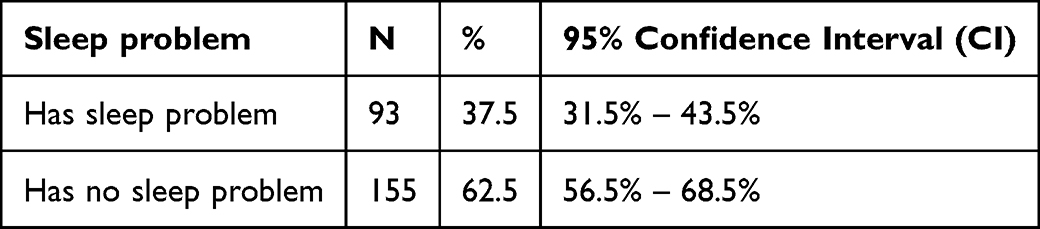 |
Table 2 Prevalence of Sleep Problems Among Children and Adolescents Diagnosed with T1DM |
The Chi-Squared test identified significant associations between sleep problems and specific demographic, clinical, and lifestyle factors. Guardian-related characteristics were strongly correlated with sleep disturbances, including, marital status (P = 0.045), educational level (P = 0.001), and average monthly household income (P < 0.001). In terms of diabetes management, both the cumulative glucose level over the preceding three months (P < 0.001) and the frequency of daily glucose testing (P < 0.001) showed significant associations with the presence of sleep problems. Furthermore, Guardian unhealthy Habits was significantly linked to sleep outcomes (P = 0.001). Conversely, the analysis found no significant correlations between sleep problems and other variables, including the method of insulin delivery (P = 0.306) or the presence of comorbidities such as hypertension, cardiac conditions, asthma, or arthritis (P > 0.05) (Table 3 and Table 4).This data illustrates the distribution of sleep disorder status within the sample population (Figure 1).
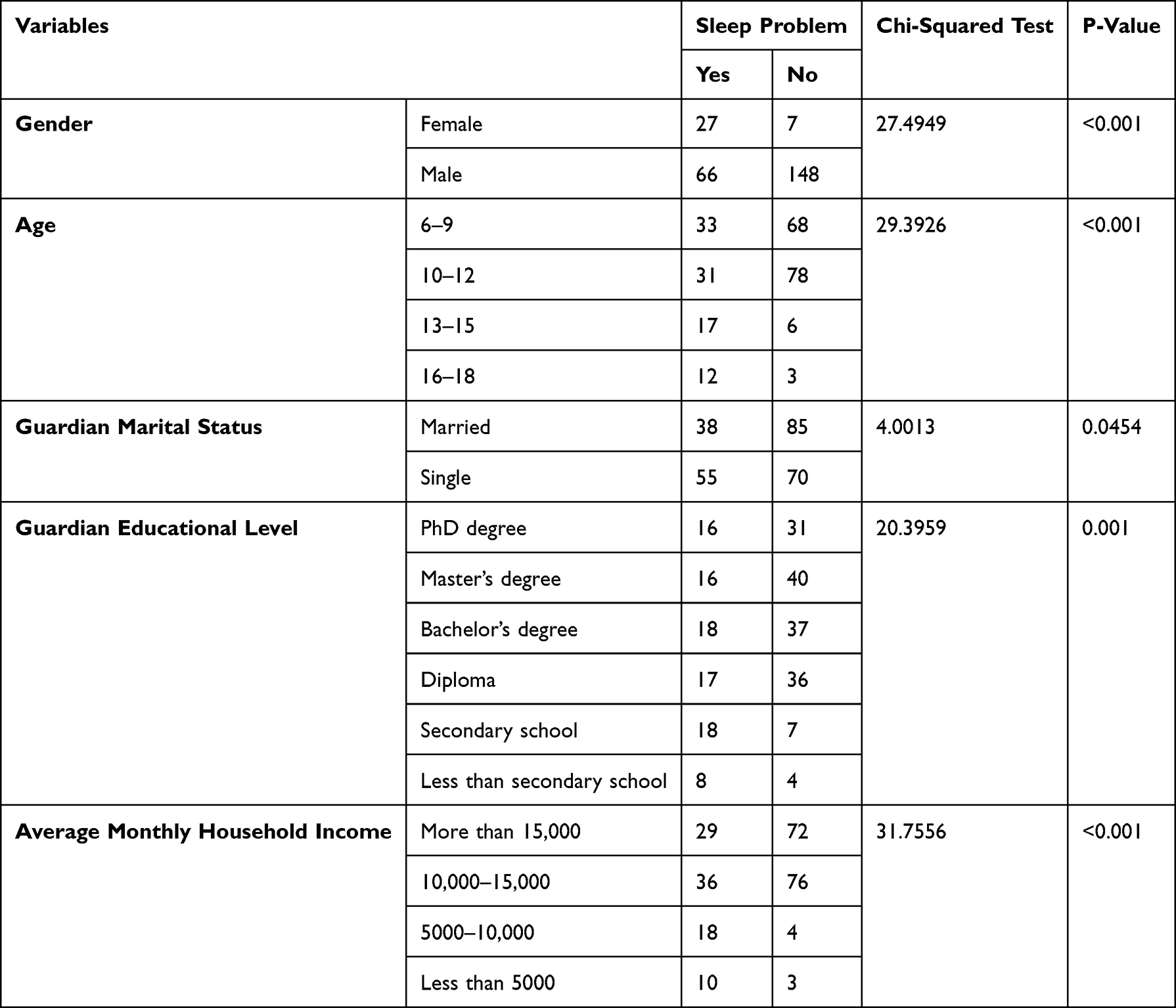 |
Table 3 Association of Sleep Problems with Demographic and Socioeconomic Variables |
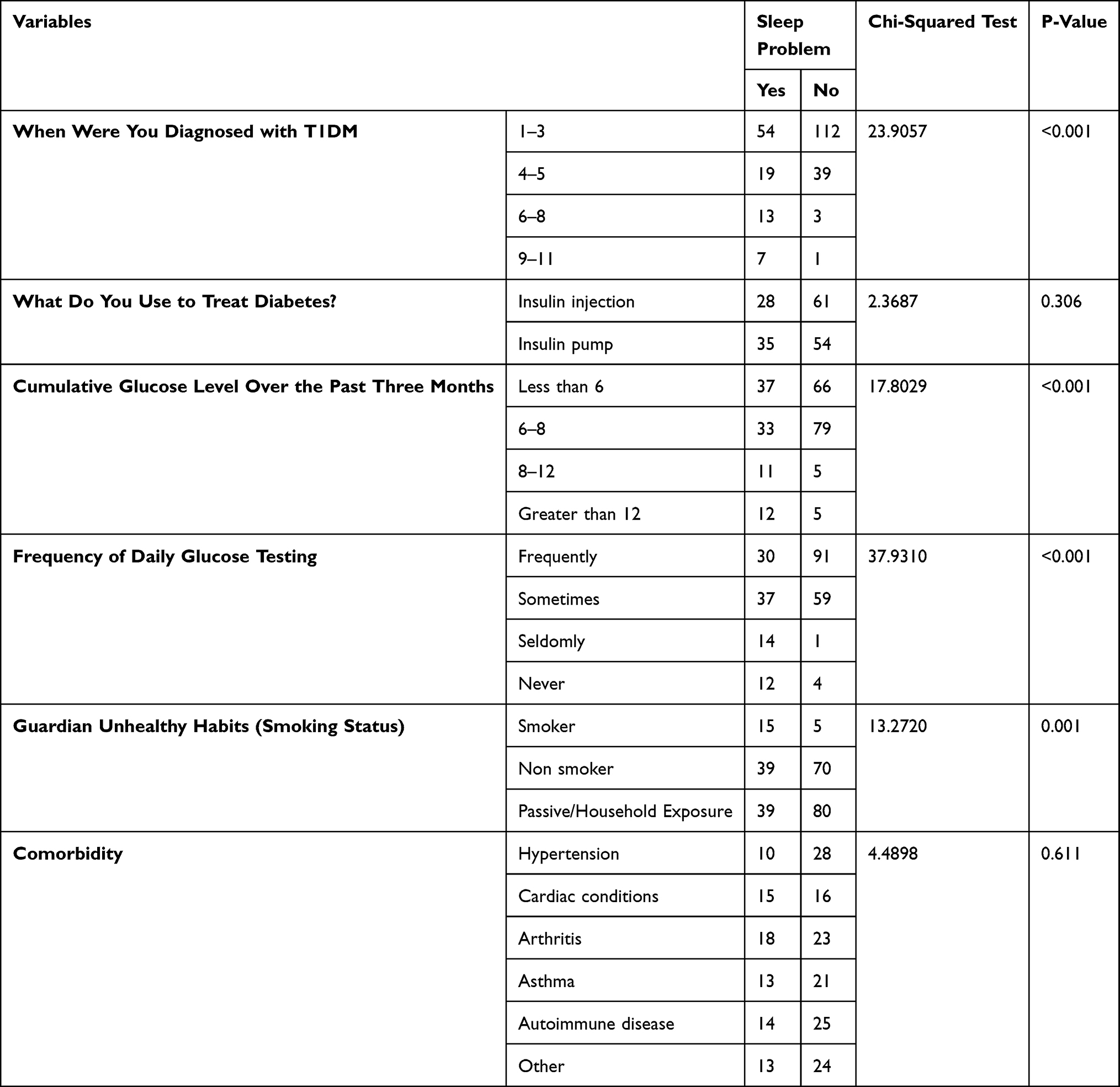 |
Table 4 Association of Sleep Problems with Clinical and Lifestyle Factors |
 |
Figure 1 Prevalence of sleep problem among children and adolescents diagnosed with T1DM. |
Discussion
The finding that 37.5% of participants have sleep problems highlights the underexplored area of sleep in the context of T1DM, urging further research and healthcare provider attention to this aspect of well-being. This study provides a comprehensive exploration of Type 1 Diabetes Mellitus (T1DM) among children and adolescents in Abha, Saudi Arabia, offering valuable insights into their health, lifestyle, and demographic profiles. The statistical rigor of Chi-Squared Analysis lends quantitative weight to the observed correlations, enhancing the robustness of the findings.
The identified correlations support existing research on the multifactorial nature of sleep disorders in diabetes, emphasizing the interconnectedness of health, lifestyle, and demographic variables.20 The study underscores the importance of comprehensive health interventions beyond diabetes management, echoing the growing body of evidence linking sleep problems with diabetes.22 Specifically, the frequency of daily glucose testing underscores the diligence in diabetes management, consistent with literature that emphasizes glycemic control as a cornerstone of diabetes care.1 The prevalence of frequent testing aligns with the proactive approach healthcare professionals advocate to empower patients in managing their condition.19
Comparing the demographic findings with established literature, the age distribution aligns with global trends observed in pediatric diabetes studies.10 The male predominance mirrors patterns seen in T1DM prevalence, where males are often reported to be at a higher frequency.9 The high prevalence of single guardians underscores the crucial role family structures play in managing chronic conditions in adolescents.2 Additionally, the guardians’ educational attainment aligns with studies highlighting education’s role in managing diabetes and health-related quality of life.16 The income distribution corresponds with research on the impact of socioeconomic factors on health outcomes in diabetes.3
Beyond demographics, the study highlights the intricate web of chronic diseases intertwined with T1DM. The coexistence of chronic diseases resonates with studies emphasizing the challenges of managing multiple conditions in individuals with diabetes.13 The balance between insulin pumps and injections reflects ongoing discussions about personalized diabetes care, acknowledging diverse treatment preferences and needs.15
Regarding lifestyle, the analysis reveals a tapestry of habits, specifically passive/guardian smoking status, that contribute to the backdrop of T1DM. The prevalence of these environmental habits is consistent with studies linking lifestyle factors to diabetes development.17 This association highlights the impact of household environment on child health outcomes.
In terms of clinical implications, complex emotional and behavioral factors related to T1DM both influenced and were influenced by sleep difficulties in a qualitative study conducted in United States.28 Since diabetes-related mood may play a significant role in sleep among young adults with T1D, implementing routine screening and providing behavioral support for sleep health and diabetes distress may be advisable.28 Prior findings suggest incorporating sleep education into care for children and young adults with T1DM.29 First-generation automated insulin delivery systems did not enhance sleep patterns in individuals with T1DM, but alternative approaches such as coaching and counselling have demonstrated effectiveness.30,31 Our study reveals that passive smoking and guardian education significantly influence sleep problems in Saudi Arabian children with T1DM, highlighting key environmental and socioeconomic factors. However, the study has certain limitations. The sample was drawn from a single diabetic center, limiting generalizability. There is a potential selection bias. The results may not be generalizable to a broader Saudi Arabian or global context due to the limited geographic scope of Abha.: Self-reported data, particularly regarding lifestyle habits and household tobacco exposure, may introduce recall bias. The cross-sectional design precludes the examination of temporal trends or causality. Future research would benefit from exploring the complexities of sleep problems using qualitative methods and expanding the geographic scope to enhance generalizability.
Conclusions
A study of children and adolescents with T1DM in Abha, Saudi Arabia, found that 37.5% experience sleep problems. These are linked to modifiable factors such as glycemic control, socioeconomic status, and household environmental factors like passive smoking. Treatment type (insulin pump vs injection) was not significantly associated with sleep outcomes. The findings emphasize the need for a comprehensive approach that includes routine sleep assessments and addresses broader health determinants, including sleep hygiene and smoking cessation, to improve overall well-being.
Abbreviations
T1DM, Type 1 Diabetes Mellitus; CGMs, Continuous Glucose Monitors; IRB: Institutional Review Board.
Data Sharing Statement
All data and materials related to the study are included in the current paper.
Ethical Considerations
The study was conducted in accordance with the Research Ethics Committee at King Khalid University (HAPO-06-B-001) approved on 10 March 2023 with approval number: ECM#2023-4703. Informed consent was obtained from the study participants’ parents and/or legal guardians prior to study commencement using a written consent form.
Consent for Publication
All parents of enrolled children signed written informed consent for publication of the current study.
Author Contributions
Youssef A. Alqahtani: Conceptualization, Methodology, Writing – Original Draft, Writing – Review & Editing, Supervision, Project Administration; Ayed A. Shati: Conceptualization, Methodology, Writing – Original Draft, Writing – Review & Editing, Supervision, Project Administration; Samy A. Dawood Snr: Methodology, Formal Analysis, Writing – Review & Editing; Abdulrahman A. Aldosari: Investigation, Writing – Review & Editing; Khaled A. Amer: Investigation, Writing – Review & Editing; Hend H. Alamri Snr: Investigation, Writing – Review & Editing; Reemah F. Alqahtani: Formal Analysis, Data Curation, Writing – Review & Editing; Rahaf A. Alamer Jnr: Data Curation, Writing – Review & Editing; Shuruq Zafer A. Alshehri Jnr: Visualization, Writing – Review & Editing; Rawan Naif Althomali: Investigation, Writing – Review & Editing; Syed Esam Mahmood: Formal Analysis, Writing – Original Draft, Writing – Review & Editing, Project Administration.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors extend their gratitude to the Dean of Research and Graduate Studies at King Khalid University for funding this work through Small Research Project under grant number RGP/100/46.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Diabetes Association Professional Practice Committee. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2022. Diabetes Care. 2022;45(Supplement_1):S17–10. doi:10.2337/dc22-S002
2. Borus JS, Laffel L. Adherence challenges in the management of type 1 diabetes in adolescents: prevention and intervention. Curr Opin Pediatr. 2010;22(4):405–411. doi:10.1097/MOP.0b013e32833a46a7
3. Speight J, Reaney MD, Barnard KD. Not all roads lead to Rome-a review of quality of life measurement in adults with diabetes. Diabet Med. 2009;26(4):315–327. doi:10.1111/j.1464-5491.2009.02682.x
4. Krueger JM, Frank MG, Wisor JP, Roy S. Sleep function: toward elucidating an enigma. Sleep Med Rev. 2016;28:46–54. doi:10.1016/j.smrv.2015.08.005
5. Buysse DJ. Sleep health: can we define it? Does it matter? Sleep. 2014;37(1):9–17. doi:10.5665/sleep.3298
6. Hillman DR. Postoperative sleep disoprderss: understanding and emerging therapies. Adv Anesth. 2017;35(1):1–24. doi:10.1016/j.aan.2017.07.001
7. Paruthi S, Brooks LJ, D’Ambrosio C, et al. Consensus statement of the American academy of sleep medicine on the recommended amount of sleep for healthy children: methodology and discussion. J Clin Sleep Med. 2016;12(11):1549–1561. doi:10.5664/jcsm.6288
8. Watson NF, Badr MS, Belenky G, et al. Recommended amount of sleep for a healthy adult: a joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep. 2015;38(6):843–844. doi:10.5665/sleep.4716
9. Reutrakul S, Thakkinstian A, Anothaisintawee T, et al. Sleep characteristics in type 1 diabetes and associations with glycemic control: systematic review and meta-analysis. Sleep Med. 2016;23:26–45. doi:10.1016/j.sleep.2016.03.019
10. Matricciani L, Olds T, Petkov J. In search of lost sleep: secular trends in the sleep time of school-aged children and adolescents. Sleep Med Rev. 2012;16(3):203–211. doi:10.1016/j.smrv.2011.03.005
11. Owens J. Classification and epidemiology of childhood sleep disorders. Sleep Med Clinics. 2007;2(3):353–361. doi:10.1016/j.jsmc.2007.05.009
12. Caruso NC, Radovanovic B, Kennedy JD, et al. Sleep, executive functioning and behaviour in children and adolescents with type 1 diabetes. Sleep Med. 2014;15(12):1490–1499. doi:10.1016/j.sleep.2014.08.011
13. Adler A, Gavan MY, Tauman R, Phillip M, Shalitin S. Do children, adolescents, and young adults with type 1 diabetes have increased prevalence of sleep disorders? Pediatr Diabetes. 2017;18(6):450–458. doi:10.1111/pedi.12419
14. Kostkova M, Durdik P, Ciljakova M, et al. Short-term metabolic control and sleep in children and adolescents with type 1 diabetes mellitus. J Diabetes Complicat. 2018;32(6):580–585. doi:10.1016/j.jdiacomp.2018.03.010
15. Farabi S. Type 1 Diabetes and Sleep. Diabetes Spectr. 2016;29(1):10–13. doi:10.2337/diaspect.29.1.10
16. Jafari P, Forouzandeh E, Bagheri ZK, Karamizadeh Z, Shalileh K. Health-related quality of life of Iranian children with type 1 diabetes: reliability and validity of the Persian version of the PedsQLTM Generic Core Scales and Diabetes Module. Health Qual Life Outcomes. 2011;9(1):104. doi:10.1186/1477-7525-9-104
17. Ghorbani A, Esmailzadehha N, Mohammadpoorasl A, Ziaee A. Association of sleep quality and waking time with prediabetes: the Qazvin Metabolic Diseases Study, Iran. Sleep Disord. 2015;2015:480742. doi:10.1155/2015/480742
18. Patel N, Savin K, Williams L, Malow BA, Jaser SS. Inconsistent sleep is linked with poor diabetes management and glycemic control in adolescents. Ann Behav Med. 2017;51:S1718–S1719.
19. Jaser SS, Foster NC, Nelson BA, et al. Sleep in children with type 1 diabetes and their parents in the T1D exchange. Sleep Med. 2017;39:108–115. doi:10.1016/j.sleep.2017.07.005
20. Von Schnurbein J, Boettcher C, Brandt S, et al. Sleep and glycemic control in adolescents with type 1 diabetes. Pediatr Diabetes. 2018;19(1):143–149. doi:10.1111/pedi.12538
21. Hazen RA, Fehr KK, Fidler A, et al. Sleep disruption in adolescents with Type 1 diabetes mellitus: relationships with adherence and diabetes control. Diab Manag. 2015;5:257–265.
22. Banghoej AM, Nerild HH, Kristensen PL, et al. Obstructive sleep apnoea is frequent in patients with type 1 diabetes. J Diabetes Complicat. 2017;31(1):156–161. doi:10.1016/j.jdiacomp.2016.10.006
23. Porter PA, Byrne G, Stick S, Jones TW. Nocturnal hypoglycaemia and sleep disoprderss in young teenagers with insulin dependent diabetes mellitus. Arch Dis Child. 1996;75(2):120–123. doi:10.1136/adc.75.2.120
24. Herbert LJ, Monaghan M, Cogen F, Streisand R. The impact of parents’ sleep quality and hypoglycemia worry on diabetes self-efficacy. Behav Sleep Med. 2015;13:308–323.
25. Jaser SS, Lord JH, Simmons JH, Malow BA. Brief report. sleep disoprderss in young children with type 1 diabetes. Diabet Res Clin Pract. 2016;120:232–234. doi:10.1016/j.diabres.2016.08.012
26. Al-Anzi MA, Alsahabi RM, Alnaser YYM, et al. The association between type 1 diabetes and sleep quality: a systematic review. SMHJ. 2025;5(3):231–243. doi:10.54293/smhj.v5i3.161
27. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index (PSQI): a new instrument for psychiatric research and practice. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
28. Carreon SA, Cao VT, Anderson BJ, Thompson DI, Marrero DG, Hilliard ME. ‘I don’t sleep through the night’: qualitative study of sleep in type 1 diabetes. Diabet Med. 2022;39(5):e14763. PMID: 34875120. doi:10.1111/dme.14763
29. Carreon SA, Baudino MN, Minard CG, et al. Mood and sleep in young adults with type 1 diabetes. J Pediatr Psychol. 2025;50(8):811–819. PMID: 40607998. doi:10.1093/jpepsy/jsaf038
30. Ji X, Wang Y, Saylor J. Sleep and type 1 diabetes mellitus management among children, adolescents, and emerging young adults: a systematic review. J Pediatr Nurs. 2021;61:245–253. PMID: 34182231. doi:10.1016/j.pedn.2021.06.010
31. Arosemena M, Salguero MV, Greeley SAW, Naylor RN, Tasali E, Philipson LH. Sleep patterns in adults and children with less common forms of diabetes. Front Endocrinol. 2025;16:1388995. doi:10.3389/fendo.2025.1388995
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.