Back to Journals » Vascular Health and Risk Management » Volume 17
Prevalence and Correlates of Self-Reported Cardiovascular Diseases Among a Nationally Representative Population-Based Sample of Adults in Ecuador in 2018
Received 26 December 2020
Accepted for publication 2 March 2021
Published 4 May 2021 Volume 2021:17 Pages 195—202
DOI https://doi.org/10.2147/VHRM.S299272
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Takashi Kajiya
Supa Pengpid,1,2 Karl Peltzer3
1ASEAN Institute for Health Development, Mahidol University, Salaya, Nakhon Pathom, Thailand; 2Department of Research Administration and Development, University of Limpopo, Turfloop, South Africa; 3Department of Psychology, University of the Free State, Bloemfontein, South Africa
Correspondence: Karl Peltzer
Department of Psychology, University of the Free State, Bloemfontein, South Africa
Email [email protected]
Background: This study aimed to determine the prevalence and correlates of self-reported cardiovascular diseases (SRCVDs) among adults in Ecuador.
Methods: National cross-sectional survey data of 4638 persons aged 18– 69 years in Ecuador were analysed. Research data were collected with an interview-administered questionnaire, physical and biochemical measurements.
Results: The prevalence of SRCVDs was 8.7%, 8.5% among men and 8.9% among women. In adjusted logistic regression analysis, being Montubio (adjusted odds ratio-AOR: 1.66, 95% confidence interval-CI: 1.10– 2.50), family alcohol problems (AOR: 1.78, 95% CI: 1.19– 2.65), past smoking tobacco (AOR: 1.36, 95% CI: 1.02– 1.81), and poor oral health status (AOR: 1.74, 95% CI: 1.19– 2.54) were associated with SRCVD. In addition, in unadjusted analysis, older age, alcohol dependence, obesity, and having hypertension were associated with SRCVD.
Conclusion: Almost one in ten persons aged 18– 69 years had SRCVD in Ecuador. Several associated factors, including Montubio by ethnicity, family alcohol problems, past smoking, and poor oral health status, were identified, which can be targeted in public health interventions.
Keywords: chronic conditions, lifestyle factors, cardiovascular disease, adults, Ecuador
Introduction
Globally, an estimated 17.9 million people died from Cardiovascular disease (CVDs) in 2016, representing 31% of all global deaths. Of these deaths, 85% are due to heart attack and stroke.1 In persons 50 years and older in 2019, “ischaemic heart disease and stroke were the top-ranked causes of disability adjusted life years (DALYs).”2 More than three-quarters of deaths from CVDs occur in low- and middle-income countries.1 “Heart attacks and strokes are usually acute events and are mainly caused by a blockage that prevents blood from flowing to the heart or brain.”1
In studies in the Americas, a study (60 years and older) in seven urban centres in Latin America and the Caribbean, the prevalence of self-reported cardiovascular disease (SRCVD) was 20.3%,3 and in a study among persons aged 60 years and older in the highlands and coastal areas of Ecuador in 2009 found a prevalence of self-reported heart disease of 13.1% and stroke 6.4%.4 In urban-rural sites (35–70 years) in Argentina, Brazil, Chile and Colombia the prevalence of SRCVD was 3.9%, 6.9%, 3.3%, and 3.8%, respectively.5 In a national study in Brazil (18 years older) the SR stroke prevalence was 1.6%,6 in Colombia (18–69 years) SRCVD 5.5%,7 Mexico (50 years and older) the prevalence of SR stroke was 4.3% and angina 13.6%,8 and in USA in 2016 (20 years plus), SRCVD (congestive health failure 3.4%, angina 3.0%, heart attack 4.4%, or stroke 3.9%).9 In Nepal (24–64 years), 2% had major cardiovascular events,10 in China (35–74 years) 3.3% in men and 3.6% in women SRCVD,11 in Australia (≥25 years) (2007–2008) the prevalence of SRCVD (heart attack or stroke) was 4.5%.12 To our knowledge, we could not find national information on SRCVD in Ecuador.13,14 CVDs contribute to 24% of mortality in 2016 in Ecuador.15 Using the mortality national registry in Ecuador, the myocardial infarction mortality rate increased from 51 in 2012 to 157 in 2016 deaths per 100,000,16 and mortality due to ischemic heart disease increased in Ecuador in the period 2001–2016.17 Ecuador’s population (16.9 million) consists of a mixture various ethnic groups, ranging from Mestizo (71.9%) to Afro Ecuadorian (4.3%).18
Factors associated with SRCVD include sociodemographic factors, behavioural and biological CVD risk risk factors. Sociodemographic factors associated with SRCVD include, older age,9,19,20 men,9,20 women,4,19 low socioeconomic status,21 lower education,6,9,20 and ethnicity.22 Behavioural CVD risk factors associated with SRCVD may include, smoking/tobacco use,3,6,20 past smoking,4 physical inactivity,4,6,23 inadequate or low fruit and vegetable consumption,10,23 high intake of sodium and sodium chloride (regular salt),24,25 and psychological distress.12 Biological CVD risk factors associated with SRCVD may include, hypertension,3,19–23,26,27 diabetes,3,6,20–23,26 obesity,3,4,6,21,23,26 abnormal cholesterol values,19 and poor oral health (edentulism).28 This study aimed to determine the prevalence and correlates of SRCVDs in a national population-based survey among adults in Ecuador in 2018.
Method
Sample and Procedures
This is a secondary analysis conducted using nationally representative population-based and cross-sectional data (18–69 years old) from the “2018 Ecuador STEPS survey.”29 The 2018 Ecuador STEPS survey data and more detailed sampling methods can be found elsewhere.30 Briefly, using a three-stage cluster sampling method, at the first stage primary sampling units (PSUs) were selected by stratum, at the second stage within each PSU selected in the first stage 12 occupied households were selected, and at the third stage, one participant (18–69 years) was selected from each household.30 Selected individuals were assessed with an interview-administered questionnaire, physical and biochemical measurements.30 Research data were collected using electronic tablet devices.30 The “Ethical Review Committee of the Ecuador Ministry of Health” approved the study.30
All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all participants included in the study.
Measures
Outcome variable: History of CVDs was assessed with the question, “Have you ever had a heart attack or chest pain from heart disease (angina) or a stroke (cerebrovascular accident or incident)?” (Yes, No).30
Sociodemographic covariates included age, sex, highest level of formal education, and ethnicity.30
Behavioural covariates included current and past smoking tobacco, daily servings of fruit and vegetable intake, and “low, moderate or high physical activity based on the Global Physical Activity Questionnaire”.30,31 Salt intake was assessed with the item, “Do you add salt to food at the table?”30 Responses were trichotomized into 1=never, 2=raley or sometimes, and 3=often or always. Alcohol dependence was sourced from the “Alcohol Use Disorder Identification Test=AUDIT” (items 4–6, ≥4 total scores).32 Alcohol family problems was sourced from the item, “During the past 12 months, have you had family problems or problems with your partner due to someone else’s drinking?” (1=yes: > monthly to 4=once or twice).30
Biological covariates included measured Body Mass Index (BMI) classified as “<18.5kg/m2 underweight, 18.5–24.4kg/m2 normal weight, 25–29.9kg/m2 overweight and ≥30 kg/m2 obesity”.33 Hypertension or raised blood pressure (BP) was defined as “systolic BP ≥140 mm Hg and/or diastolic BP ≥90 mm Hg or where the participant is currently on antihypertensive medication”.34 Diabetes was defined as “fasting plasma glucose levels ≥7.0 mmol/L (126 mg/dl); or using insulin or oral hypoglycaemic drugs; or having a history of diagnosis of diabetes”.35 Raised total cholesterol was defined as “fasting TC ≥5.0 mmol/L or currently on medication for raised cholesterol”.35 Self-rated oral health status (AROH) was sourced from two items, 1) “How would you describe the state of your teeth, and 2) How would you describe the state of your gums?”30 Poor SROH was defined as “having poor or very poor status of teeth and/or gums, and good oral health as having average, good, very good or excellent status of teeth and/or gums”, in line with previous research.36 Cronbach alpha’s for the two item SROH scale was 0.74 in this sample.
Data Analysis
Considering the clustered study design, all statistical analyses were done using “STATA software version 14.0 (Stata Corporation, College Station, TX, USA).” Unadjusted and adjusted logistic regression was used to calculate predictors of SRCVD. Variables with p-values <0.1 in univariate analysis (age group, educational level, ethnicity, family alcohol problems, smoking status, alcohol dependence, body weight status, hypertension, and self-rated oral health) were included in the final adjusted model. P-values of below 0.05 were accepted as significant and missing values were excluded from the analysis.
Results
Sample and Cardiovascular Diseases Prevalence Characteristics
The sample included 4,638 adults (18–69 years; with 39 median age), 58.1% were female, 30.5% had higher education, and majority (78.9%) belonged to the Mestizo ethnic group. The study response rate was 69.4%.30 One in five participants (24.7%) had low physical activity, 13.7% currently smoked tobacco, 11.8% were dependent on alcohol use, 7.0% had alcohol family problems, 58.8% had 1 or less serving of fruit and vegetables a day, and 12.45 often or always added salt to their meals. One in four respondents (25.7%) had obesity, 20.5% hypertension, 7.1% diabetes, 34.8% raised total cholesterol, and 9.7% poor oral health. The prevalence of SRCVDs was 8.7%, 8.5% among men and 8.9% among women (see Table 1).
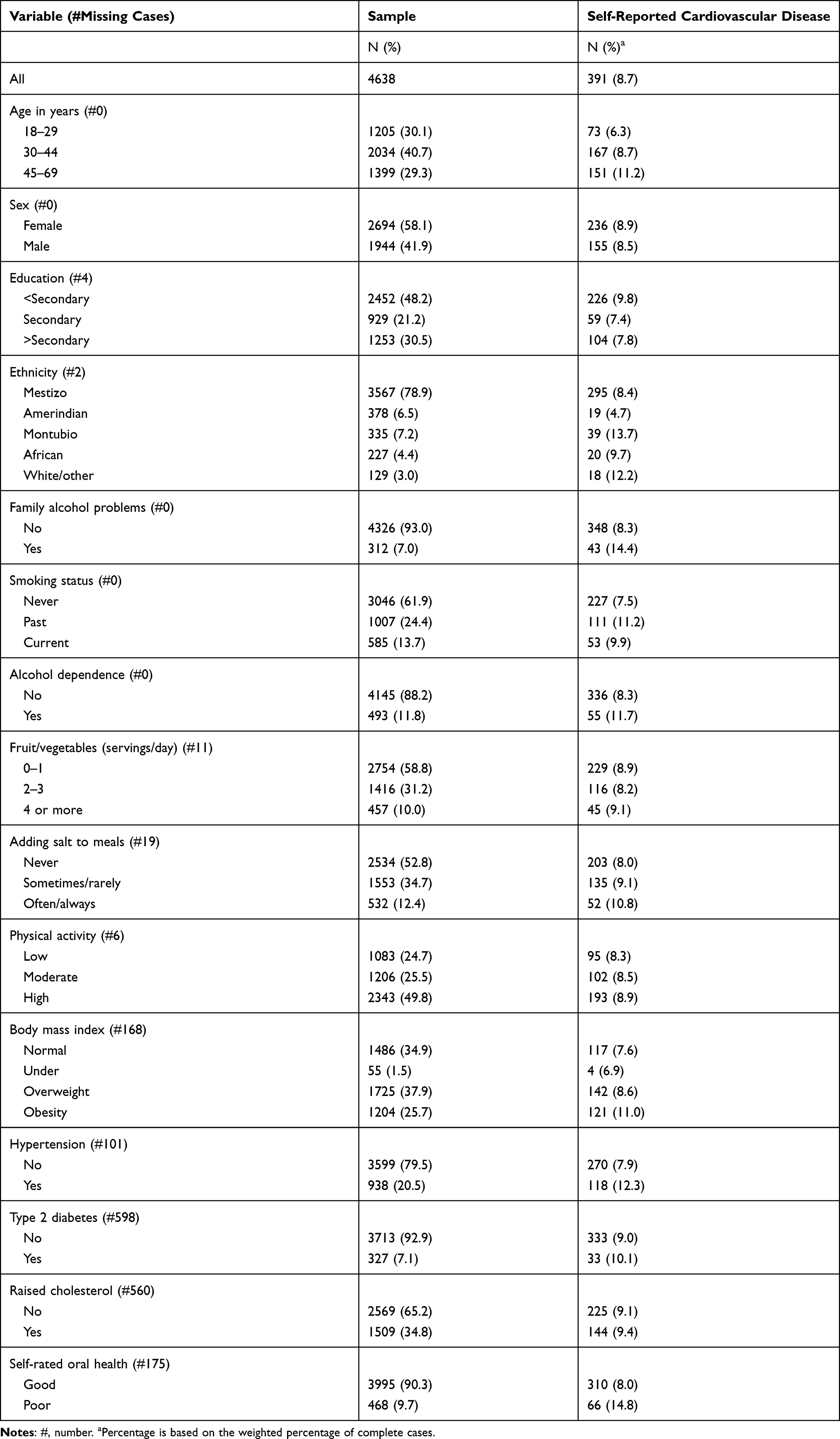 |
Table 1 Sample and Cardiovascular Disease Characteristics Among Adults, Ecuador, 2018 |
Associations with Self-Reported Cardiovascular Disease Prevalence
In adjusted logistic regression analysis, Montubio (Adjusted Odds Ratio-AOR: 1.66, 95% Confidence Interval-CI: 1.10–2.50), family alcohol problems (AOR: 1.78, 95% CI: 1.19–2.65), past smoking tobacco (AOR: 1.36, 95% CI: 1.02–1.81), and poor oral health status (AOR: 1.74, 95% CI: 1.19–2.54) were associated with SRCVD. In addition, in unadjusted analysis, older age, alcohol dependence, obesity, and having hypertension were associated with SRCVD (see Table 2).
 |
Table 2 Multivariable Associations with Self-Reported Cardiovascular Disease |
Discussion
In this nationally representative sample of adults (18–69 years) in Ecuador, the prevalence of SRCVD (8.7%) was higher than in Argentina (3.9%, 35–70 years), Brazil (6.9%, 35–70 years), Chile (3.3%, 35–70 years) and Colombia (3.8%, 35–70 years),5 in Brazil (SR stroke, 1.6%, 18 years older),6 Colombia (5.5%, 18–69 years),7 in Nepal (SRCVD, 2.0%, 24–64 years),10 in China (SRCVD, 3.5%, 35–74 years),11 in Australia (SRCVD, 4.5%, ≥25 years),12 and USA (SR congestive health failure 3.4%, angina 3.0%, heart attack 4.4%, or stroke 3.9%, 20 years and older).9 However, it should be noted that the prevalence rates of SRCVD are difficult to compare because of different measurements and different age groups. The high prevalence of SRCVD found in Ecuador calls for community-based massive education campaigns and health care provision of people with CVD, including the identification of a cerebral-vascular event and emergency care.3,37
Consistent with previous research,9,19,20 older age (45–69 years) was positively associated with SRCVD in unadjusted analysis. Some previous studies found sex differences4,9,19,20 in the prevalence of SRCVD, while in our study sex differences were not reaching significance. Other research found an association between low socioeconomic status or lower education6,9,20,21 and SRCVD, while this survey did not show such associations. Compared to Mestizo Ecuadorean, Montubio Ecuadorean were more likely and Amerindian less likely (marginally significant) to have SRCVD. In a previous study among Amerindians in Ecuador, a low prevalence of atrial fibrillation was found, which can be explained by, both, “racially determined short stature and frequent dietary oily fish intake.”38 The most significant predictors of the increasing mortality rate from myocardial infarction in Ecuador were living in the coast belonging to a mixed race.16 The Montubio (“an aboriginal mestizo group that originates from the coastal part of Ecuador”)18 may form part of this mortality rate from myocardial infarction. In the study among older adults in Ecuador,4 people living on the coast had an increased risk of heart disease and stroke compared to those in the highlands.
In agreement with previous research,12,39,40 this study showed that psychosocial stress in the form of alcohol family problems was associated with SRCVD. Stress can increase the cerebrovascular disease risk by modulating sympathomimetic activity, affecting the blood pressure reactivity, cerebral endothelium, coagulation, or heart rhythm.39 In line with former research,3,4,6,20 past tobacco use was positively associated with SRCVD. In a systematic review and meta analysis the importance of smoking as an independent risk factor for stroke was confirmed.41 Contrary to expectation,4,6,10,23–25 physical inactivity, inadequate or low fruit and vegetable consumption and frequent salt consumption were not associated with SRCVD in this study. Similarly to a study in Nepal,10 the consumption of fruit and vegetables was very low in this study, but was unlike in the Nepal study not associated with SRCVD.
Consistent with former research,3,4,6,19–23,26,27 this survey showed in univariate analysis an association between hypertension and obesity with SRCVD. Unlike some studies,3,6,19–23,26 this study did not find significant associations between diabetes, raised cholesterol and SRCVD. In line with some previous research,28 poor oral health (edentulism) was positively associated with SRCVD. Periodontal diseases have been shown to be associated with systematic diseases, such as CVD.42
The strength of the study includes a nationally representative sample of adults in Ecuador and the use of a standardized STEPS survey methodology and measurements. Study limitations include the cross-sectional design, the assessment of some variables, including CVD by self-report, and that certain relevant variables, such as psychological distress, were not assessed. Previous research compared self-reported versus hospital-coded diagnosis of CVD, and found SRCVD valid for epidemiological studies.43 Further, the study did not assess the duration of having a CVD and the CVD type, which prevents us from establishing a trend between time of CVD diagnosis and health risk behaviours. The study participants only included those that had survived CVD, and excluded those with CVD who had died prior to the survey, increasing the possible underestimates of our figures.44
Conclusion
Almost one in ten persons aged 18–69 years reported having been diagnosed with CVD in Ecuador. Several associated factors for CVD, such as being Montubio, family alcohol problems, past smoking tobacco, and poor oral health status were identified, which can be targeted in public health interventions.
Acknowledgment
The data source, the World Health Organization NCD Microdata Repository (URL: https://extranet.who.int/ncdsmicrodata/index.php/catalog), is hereby acknowledged.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization (WHO). Cardiovascular diseases (CVDs), 2017. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds).
2. GBD. Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2019;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9.
3. Hennis A, Hambleton I, Fraser H, Tulloch-Reid M, Barcelo A, Hassell T. Risk factors for cardiovascular disease in the elderly in Latin America and the Caribbean. Prevention and Control. 2006;2:175–185. doi:10.1016/j.precon.2007.04.003
4. Guevara PE, Andrade FC. Socioeconomic and lifestyle factors associated with chronic conditions among older adults in Ecuador. Rev Panam Salud Publica. 2015;38(3):226–232.
5. Murphy A, Palafox B, O’Donnell O, et al. Inequalities in the use of secondary prevention of cardiovascular disease by socioeconomic status: evidence from the PURE observational study. Lancet Glob Health. 2018;6(3):e292–e301. doi:10.1016/S2214-109X(18)30031-7
6. Ribeiro ÍJS, Cardoso JP, Freire IV, Carvalho MF, Pereira R. Determinants of stroke in Brazil: a cross-sectional multivariate approach from the national health survey. J Stroke Cerebrovasc Dis. 2018;27(6):1616–1623. doi:10.1016/j.jstrokecerebrovasdis.2018.01.013
7. Sánchez L, Barbosa JM, Arias SA. Morbilidad cardiovascular por autoreporte y su asociación con factores biopsicosociales en el Tolima. Rev. Fac. Nac. Salud Pública. 2014;32(1):80–87.
8. Ruan Y, Guo Y, Zheng Y, et al. Cardiovascular disease (CVD) and associated risk factors among older adults in six low-and middle-income countries: results from SAGE Wave 1. BMC Public Health. 2018;18(1):778. doi:10.1186/s12889-018-5653-9
9. Abdalla SM, Yu S, Galea S. Trends in cardiovascular disease prevalence by income level in the United States. JAMA Netw Open. 2020;3(9):e2018150. doi:10.1001/jamanetworkopen.2020.18150
10. Nepali S, Rijal A, Olsen MH, McLachlan CS, Kallestrup P, Neupane D. Factors affecting the fruit and vegetable intake in Nepal and its association with history of self-reported major cardiovascular events. BMC Cardiovasc Disord. 2020;20(1):425. doi:10.1186/s12872-020-01710-y
11. He J, Neal B, Gu D, et al. InterASIA Collaborative Group. International collaborative study of cardiovascular disease in Asia: design, rationale, and preliminary results. Ethn Dis. 2004;14(2):260–268.
12. Atlantis E, Sullivan T. Changes in cardiovascular disease burden associated with psychopathology in Australian adults 2004-2008. Gen Hosp Psychiatry. 2012;34(4):345–351. doi:10.1016/j.genhosppsych.2012.02.006
13. Sisa I. Gender differences in cardiovascular risk assessment in elderly adults in Ecuador: evidence from a national survey. J Investig Med. 2019;67(4):736–742. doi:10.1136/jim-2018-000789
14. Del Brutto OH, Mera RM. Stroke risk factors in couples. A population-based study in community-dwelling adults living in a remote rural setting (the Atahualpa Project). J Neurol Sci. 2019;398:98–100. doi:10.1016/j.jns.2019.01.037
15. World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, Ecuador, 2018. Available from: https://www.who.int/nmh/countries/ecu_en.pdf?ua=1.
16. Balda-Canizares JA, Tamariz L, Moreno-Zambrano D, et al. Increasing myocardial infarction mortality trends in a middle-income country. Cardiovasc Diagn Ther. 2018;Aug(4):493–499. doi:10.21037/cdt.2018.07.03
17. Núñez-González S, Aulestia-Ortiz S, Borja-Villacrés E, Simancas-Racine D. Mortalidad por enfermedades isquémicas del corazón en Ecuador, 2001-2016: estudio de tendencias [Mortality due to ischemic heart disease in Ecuador 2001-2016. A time trend study]. Rev Med Chil. 2018;146(8):850–856. doi:10.4067/s0034-98872018000800850
18. World fact book. Ecuador: Available from: https://www.cia.gov/library/publications/the-world-factbook/geos/ec.html. Accessed
19. Abbasi M, Neishaboury M, Koohpayehzadeh J, et al. National prevalence of self-reported coronary heart disease and chronic stable angina pectoris: factor analysis of the underlying cardiometabolic risk factors in the SuRFNCD-2011. Glob Heart. 2018;13(2):73–82.e1. doi:10.1016/j.gheart.2018.01.001
20. Gikas A, Lambadiari V, Sotiropoulos A, Panagiotakos D, Pappas S. Prevalence of major cardiovascular risk factors and coronary heart disease in a sample of greek adults: the Saronikos Study. Open Cardiovasc Med J. 2016;10:69–80. doi:10.2174/1874192401610010069
21. Ghaemian A, Nabati M, Saeedi M, Kheradmand M, Moosazadeh M. Prevalence of self-reported coronary heart disease and its associated risk factors in Tabari cohort population. BMC Cardiovasc Disord. 2020;20(1):238. doi:10.1186/s12872-020-01526-w
22. Teh WL, Abdin E, Vaingankar JA, et al. Prevalence of stroke, risk factors, disability and care needs in older adults in Singapore: results from the WiSE study. BMJ Open. 2018;8(3):e020285. doi:10.1136/bmjopen-2017-020285
23. Fuchs SC, Moreira LB, Camey SA, Moreira MB, Fuchs FD. Clustering of risk factors for cardiovascular disease among women in Southern Brazil: a population-based study. Cad Saude Publica. 2008;24(Suppl 2):S285–93. doi:10.1590/s0102-311x2008001400013
24. Poggio R, Gutierrez L, Matta MG, Elorriaga N, Irazola V, Rubinstein A. Daily sodium consumption and CVD mortality in the general population: systematic review and meta-analysis of prospective studies. Public Health Nutr. 2015;18(4):695–704. doi:10.1017/S1368980014000949
25. Mozaffarian D, Fahimi S, Singh GM, et al. Global Burden of Diseases Nutrition and Chronic Diseases Expert Group. Global sodium consumption and death from cardiovascular causes. N Engl J Med. 2014;371(7):624–634. doi:10.1056/NEJMoa1304127
26. Aniza I, Nurmawati A, Hanizah Y, Ahmad Taufik J. Modifiable risk factors of cardiovascular disease among adults in rural community of Malaysia: a cross sectional study. MJPHM. 2016;16(1):53–61.
27. Wasay M, Khatri IA, Kaul S. Stroke in South Asian countries. Nat Rev Neurol. 2014;10(3):135–143. doi:10.1038/nrneurol.2014.13
28. Del Brutto OH, Mera RM, Zambrano M, Del Brutto VJ. Severe edentulism is a major risk factor influencing stroke incidence in rural Ecuador (The Atahualpa Project). Int J Stroke. 2017;12(2):201–204. doi:10.1177/1747493016676621
29. World Health Organization (WHO). 2018. STEPwise approach to surveillance (STEPS). Available from: https://www.who.int/ncds/surveillance/steps/en/.
30. Subsecretaría Nacional de Vigilancia de la Salud Pública, Subsecretaría Nacional de Promoción de la Salud e Igualdad, Dirección Nacional de Estrategias de Prevención y Control, Dirección Nacional de Promoción de la Salud (MSP, INEC, OPS/OMS). Encuesta STEPS Ecuador 2018. Available from: https://extranet.who.int/ncdsmicrodata/index.php/catalog/774.
31. Armstrong T, Bull F. Development of theWorld Health Organization Global Physical Activity Questionnaire (GPAQ). J. Public Health. 2006;14:66–70. doi:10.1007/s10389-006-0024-x
32. Australian government. Alcohol screen (AUDIT): Available from: http://nceta.flinders.edu.au/files/3314/2257/4957/Right_Mix_3.pdf.
33. World Health Organization (WHO)- Europe. Body Mass Index Available from:https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi. . Accessed September 20 2020.
34. Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the joint national committee of prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003;42(6):1206–1252. doi:10.1161/01.HYP.0000107251.49515.c2
35. World Health Organization (WHO) WHO STEPS Surveillance Manual. Available from: https://www.who.int/ncds/surveillance/steps/STEPS_Manual.pdf.
36. Pengpid S, Peltzer K. Self-rated oral health status and social and health determinants among community dwelling adults in Kenya. Afr Health Sci. 2019;19(4):3146–3153. doi:10.4314/ahs.v19i4.37
37. Góngora-Rivera F. Perspective on stroke in Mexico. Medicina Universitaria. 2015;17(68):184–187. doi:10.1016/j.rmu.2015.04.001
38. Del Brutto OH, Costa AF, Cano JA, et al. Low prevalence of atrial fibrillation in Amerindians: a population-based study in frequent fish consumers living in rural coastal Ecuador (The Atahualpa Project). Aging Clin Exp Res. 2018;30(5):539–542. doi:10.1007/s40520-017-0810-z
39. Kotlęga D, Gołąb-Janowska M, Masztalewicz M, Ciećwież S, Nowacki P. The emotional stress and risk of ischemic stroke. Neurol Neurochir Pol. 2016;50(4):265–270. doi:10.1016/j.pjnns.2016.03.006
40. O’Donnell MJ, Xavier D, Liu L, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet. 2010;376(9735):112–123. doi:10.1016/S0140-6736(10)60834-3
41. Peters SA, Huxley RR, Woodward M. Smoking as a risk factor for stroke in women compared with men: a systematic review and meta-analysis of 81 cohorts, including 3,980,359 individuals and 42,401 strokes. Stroke. 2013;44(10):2821–2828. doi:10.1161/STROKEAHA.113.002342
42. Nazir MA. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int J Health Sci (Qassim). 2017;11(2):72–80.
43. Jamrozik E, Hyde Z, Alfonso H, et al. Validity of self-reported versus hospital-coded diagnosis of stroke: a cross-sectional and longitudinal study. Cerebrovasc Dis. 2014;37(4):256–262. doi:10.1159/000358583
44. Zaw KK, Nwe N, Hlaing SS. Prevalence of cardiovascular morbidities in Myanmar. BMC Res Notes. 2017;10(1):99. doi:10.1186/s13104-017-2422-2
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.