")
Back to Journals » Clinical Ophthalmology » Volume 18
Prevalence and Causes of Blindness and Visual Impairment Among Nigerian Children: A Systematic Review
Authors Eze UA , Obasuyi OC , Salihu DV, Bature M, Yeye-Agba OO, Kanmodi KK
Received 9 October 2023
Accepted for publication 19 January 2024
Published 1 February 2024 Volume 2024:18 Pages 289—301
DOI https://doi.org/10.2147/OPTH.S440744
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ugochukwu Anthony Eze,1,2 Osamudiamen Cyril Obasuyi,3 Dora Valerie Salihu,4 Mustapha Bature,5,6 Olabisi Olayemi Yeye-Agba,7 Kehinde Kazeem Kanmodi8– 11
1Department of Ophthalmology, Federal Medical Centre, Asaba, Nigeria; 2School of Sciences, Health Sciences Technology Engineering University of Suffolk-Unicaf, Ipswich, UK; 3Department of Ophthalmology, Irrua Specialist Teaching Hospital, Irrua, Nigeria; 4Department of Ophthalmology, Garki Specialist Hospital, Abuja, Nigeria; 5Department of Ophthalmology, Usmanu Danfodiyo University, Sokoto, Nigeria; 6University Teaching Hospital, Sokoto, Nigeria; 7Department of Ophthalmology, Federal Teaching Hospital, Lokoja, Nigeria; 8School of Dentistry, University of Rwanda, Kigali, Rwanda; 9Faculty of Dentistry, University of Puthisastra, Phnom Penh, Cambodia; 10Cephas Health Research Initiative Inc, Ibadan, Nigeria; 11School of Life Sciences, Teesside University, Middleborough, UK
Correspondence: Kehinde Kazeem Kanmodi, School of Dentistry, University of Rwanda, Kigali, Rwanda, Email [email protected] Ugochukwu Anthony Eze, Department of Ophthalmology, Federal Medical Centre, Asaba, Nigeria, Email [email protected]
Background: Low/middle-income countries have the highest burden of blindeness and visual impairment, which directly affects the children and indirectly affects their community. Furthermore, the number of blind years suffered by children with low vision or blindness creates a self-perpetuating ripple effect on their development, health and the socio-economic development of their communities. This systematic review aims to interrogate the existing evidence on the prevalence and causes of blindness and visual impairment in Nigerian children to provide evidence to drive health policy.
Methods: This was a systematic review without meta-analysis (SwiM) using a narrative synthesis of the evidence reported using the PRISMA guidelines. All primary cross-sectional studies (in English) reporting the prevalence and causes of visual impairment among Nigerian children under 20 years old between 2003 and 2022 were included in this review. PUBMED, AJOL, BASE and ProQuest databases were searched for eligible studies between 6 June and 15 July 2023. The quality of the included studies was assessed using the AXIS tool. Results were extracted and summarised using descriptive statistics. Visual impairment and blindness using the presenting visual acuity in the better eye were reported using the WHO classification.
Results: Seventeen studies, involving 16,924 children from 13 states across five geo-political zones in Nigeria, were included in the final analysis of this review. The prevalence of visual impairment was 3.9%, 2.7% and 0.3% for mild, moderate and severe visual impairments, respectively, due to ametropia, cataracts, glaucoma, etc. The prevalence of blindness was 0.2% due to cataracts, corneal scars and optic atrophy.
Conclusion: Blindness and visual impairment is still a significant clinical and public health burden among Nigerian children. Hence, there is still a need for clinicians, especially opthalmologists, public health specialists, policy-makers, and other relevant stakeholders to intensify efforts towards the prevention and control of this burden.
Keywords: visual impairment, blindness, childhood blindness, childhood visual impairment, Nigeria, systematic review
Introduction
Visual impairment occurs when any eye condition affects the visual system and its function and may be categorised as distance and near visual impairment.1 Globally, an estimated 2.2 billion people suffer from a near or distant visual impairment (VI), mainly caused by refractive errors or cataracts.1,2 Unfortunately, over 80% of vision impairment is found among the underserved population in low- and middle-income countries,1,2 with an attendant significant impact on the socio-economic status of these countries. The financial burden of VI is estimated to cost about USD 411 billion in productivity losses globally.3
The leading aetiologies of VI and Blindness in children are uncorrected refractive errors, cataracts, congenital ocular abnormalities, corneal scarring from trauma or traditional eye medications, cerebral visual impairments and retinopathy of prematurity. Blindness in children can have a significant impact on their early and long-term psychosocial and intellectual development. Currently, an estimated 450 million children have a form of visual impairment, and 90 million are blind.4
A recent systematic review reported the respective global prevalence of visual impairment and blindness in 1.7% and 0.2% using the best corrected visual acuity (BCVA), with refractive errors (ametropias) and cataract being the commonest causes of VI and blindness, respectively.5 Using different definitions, different regions were reported to have the highest prevalence rates of VI. However, using the BCVA of <20/40 (6/12), the pacific region had the highest prevalence of 0.9%. On the other hand, the African region and the East Mediterranean had the highest prevalence of blindness of approximately 1.9%.5 In Ghana, Ceesay et al6 reported a prevalence of 4.3% for VI and ametropias were the most common causes of blindness.
Children are the future workforce of a nation; hence, all efforts need to be put in place to ensure that they remain in good health and wellbeing. There is a growing proportion of children under 18 years in the overall population of Nigeria.7,8 Current UNICEF data estimated the 2023 population of children under 18 years of age in Nigeria to be 110,797,959, which is about half of the country’s population.8 Unfortunately, nationally representative data required to drive the necessary health policy to protect this vulnerable group does not exist in Nigeria. The lack of nationally representative data on the causes and prevalence of visual impairment and blindness in children makes it necessary to aggregate the available evidence in one report to help drive policy.
This systematic review aims to determine the prevalence and causes of blindness and visual impairment among children in Nigeria by interrogating the evidence in the last 20 years.
Methods
Study Design
This study was a systematic review without meta-analysis (SwiM) of literature reported using the Preferred Reporting Items for Systematic Reviews and Meta-analysis Statement (PRISMA) guidelines.9 An initial search was carried out on the International Prospective Register for Systematic Reviews (PROSPERO) to determine if there were any recent or ongoing systematic reviews on the topic. After that, the study was pre-registered in PROSPERO on 12 June 2023 (CRD42023430374).
Screening and Eligibility
All primary cross-sectional studies reporting the prevalence and causes of visual impairment in Nigerian children under 18 years between 2003 and 2022 were included in this review. Studies not in English, grey literature, letters to editors, or editorials were excluded from this review.
Literature Sources
The African Journal Online (AJOL), Bielefeld University Search Engine (BASE), PubMed, and the ProQuest online library databases were searched for relevant literature between 16 June and 15 July 2023.
Search Strategy
An initial search was carried out on PubMed to identify the availability of reports on the prevalence and causes of VI and blindness in Nigerian children. Furthermore, this also aided the identification of relevant keywords used to design the search strategy. The final database search used relevant keywords, phrase searching and controlled vocabulary searching through database-specific indexing terms. Boolean operators truncation and field tags were used. The search terms containing relevant keywords were combined as follows: (“prevalence” OR “frequency” OR “occurrence” OR “pattern” OR “commonness” OR “regularity”) AND (“causes OR aetiology” OR “risk factor”) AND (“blindness” OR “visual loss”) AND (“visual impairment” OR “poor vision”) AND (“children” OR “childhood” OR “paediatric”) AND (Niger*). The search was further refined to include literature published within the past 20 years (AND “2003–2022”).
Study Selection Process
Identified studies from the respective databases were exported to Rayyan, which was used to manage and organise the screening process. Following de-duplication by Rayyan, EUA and OOC independently screened the titles and abstracts of the retrieved studies in line with the inclusion and exclusion criteria. Title and abstract screening was followed by a screening of the complete texts independently by EUA, OOC, DVS, MB, and YOO. Any conflicts arising from the screening process were resolved by consensus, and where an agreement was impossible, KKK resolved the dispute. Studies included in the review were studies that reported prevalence of visual impairment, or blindness among children in Nigeria, studies that reported the causes of blindness and visual impairment in Nigeria. According to UNICEF, a child is defined as an individual less than 18 years old; this was the benchmark used for this systematic review.10
Quality Appraisal
The Appraisal tool for cross-sectional studies (AXIS) was used to assess the included studies’ quality and risk of bias.11 The tool has a 20-point questionnaire that addresses the quality of a cross-sectional study covering seven areas – study design, sample size justification, target population, sampling frame, sample selection, validity and reliability measurement, and overall methods.
Data Extraction and Synthesis
Data were extracted from the included studies using a bespoke data extraction sheet. Information retrieved from the studies included the author(s) name(s), year of publication, essential demographic details of study participants, geographic location of the study, study setting, design and methods, sample size, sampling technique, and results on prevalence and causes of blindness. Visual impairment was defined as presenting visual acuity worse than 6/12 in the better eye and characterised as mild (<6/12–6/18), moderate (≤6/18–6/60) and severe (≤6/60–3/60).12 Blindness was defined as presenting visual acuity in the better eye ≤3/60.12 If there were any missing data, attempts were made to contact the author(s) to clarify and supply the data where possible. EUA and OCO independently extracted data, and any conflicts were resolved by consensus. Meta analysis could not be accomplished in this review due to heterogeneity of the included studies as not all the included papers reported effect estimates and measures of precision such as standard error of confidence interval. Descriptive statistics (mean and range) was used to estimate the prevalence from the nine (9) included community-based studies.13–16 Community-based studies were used to estimate the prevalence because they give a better representation of the general population.17 Clinic-based studies included mainly provided more detailed causes of blindness and visual impairment.
Ethical Considerations
Being a systematic review, and the respective included studies had obtained ethical clearances, primary ethical approval was not obtained for this review.
Results
Search Findings
A total of 536 literature were retrieved from the database search. After deduplication and screening, a total of 17 studies (reports) were included into the systematic review for quality appraisal, data extraction, and data synthesis (Figure 1).
 |
Figure 1 PRISMA 2020 flowchart of included studies. |
Study Characteristics
Seventeen studies comprising 15,810 from thirteen states across five of the country’s six geo-political zones (GPZ) were included in this review. The studies included were all cross-sectional studies (Table 1).
 |
Table 1 Descriptive Summary of Studies Reporting the Prevalence of Blindness and Visual Impairment Among Nigerian Children |
Prevalence of Visual Impairment and Blindness
The mean prevalence of mild, moderate and severe visual impairment and blindness for respective geo-political zones are shown in Table 2. The overall mean (range) prevalence of blindness was 0.3% (0.2–0.4%) while that of mild, moderate, severe visual impairments were 3.9% (0.2–15.9), 2.9% (0.1–10), and 0.2% (0.1–0.5), respectively.
 |
Table 2 Population-Based Prevalence of Blindness and Visual Impairment |
Causes of Visual Impairment and Blindness
The leading causes of mild to severe visual impairment in children were refractive errors, cataracts (congenital or acquired), corneal opacities (congenital, presumed vitamin A deficiency, infectious or traumatic), glaucoma, and amblyopia. Other less common causes were strabismus, retinal diseases (including dystrophies and macular scars) and ptosis (Tables 3–5).
 |
Table 3 Causes of Visual Impairment Among Nigerian Children |
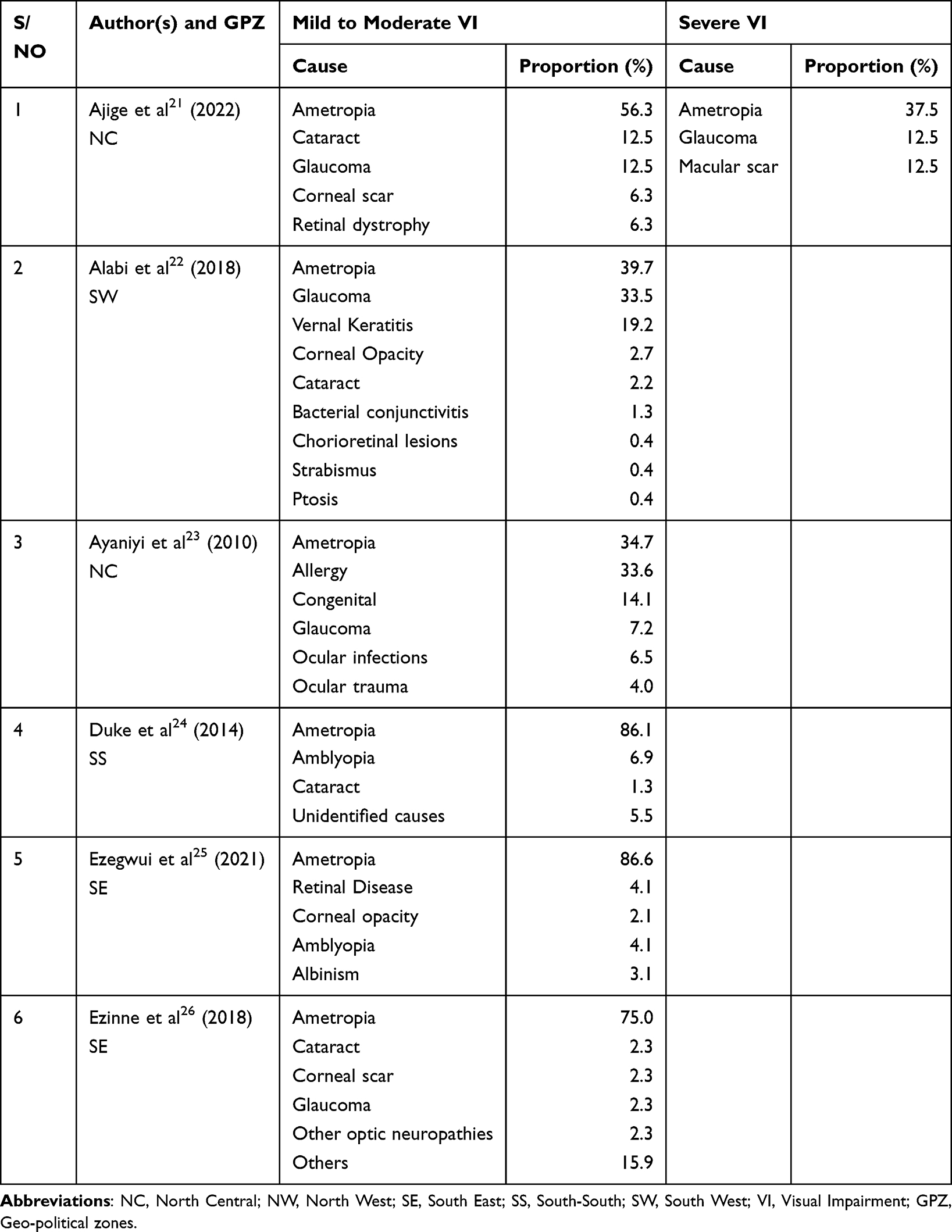 |
Table 4 Causes of Mild-Moderate, Severe Visual Impairment in Nigerian Children |
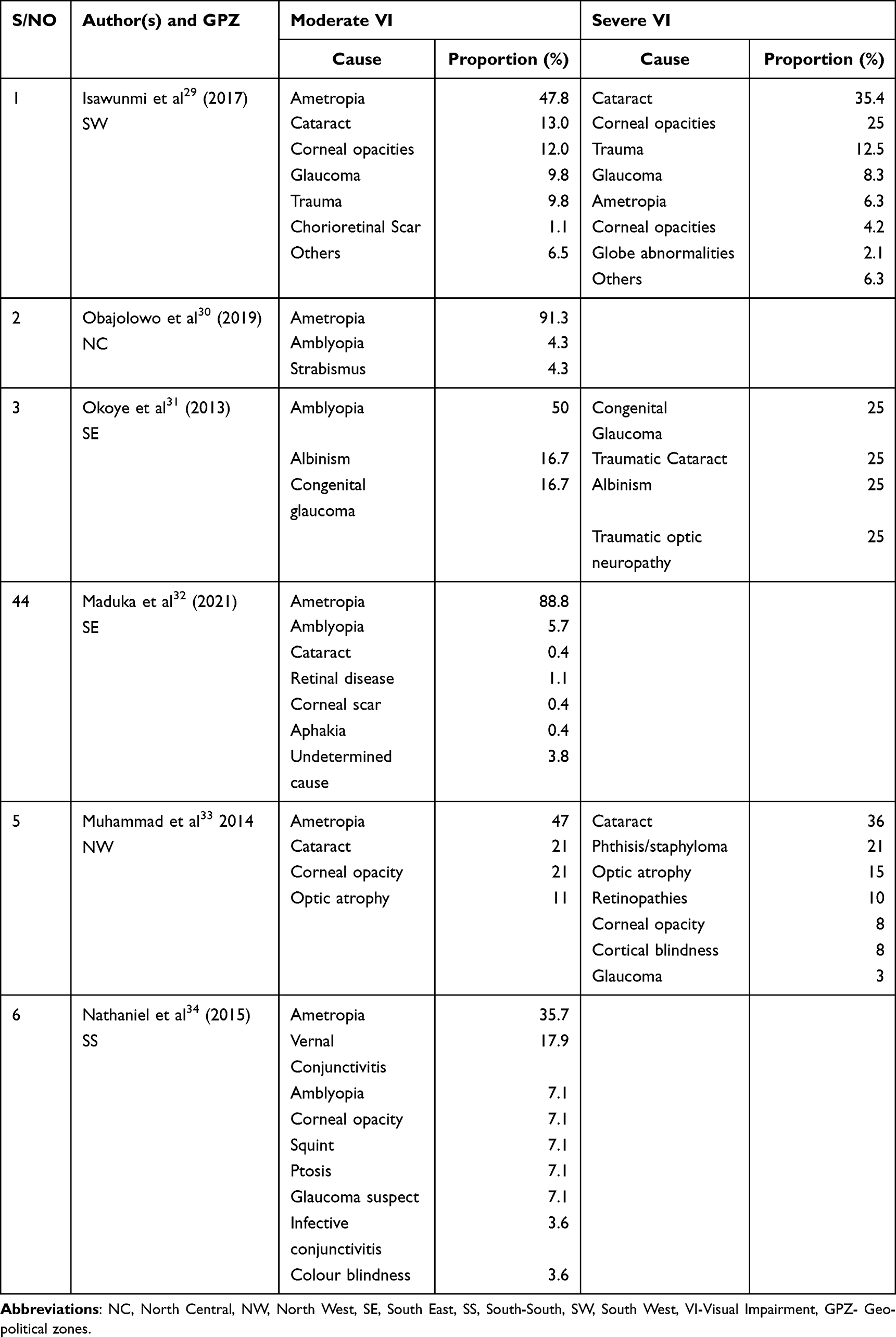 |
Table 5 Causes of Moderate and Severe Visual Impairment Among Nigerian Children |
The causes of blindness were cataracts, optic atrophy, cornea scars and cornea-related pathologies, and trauma (Table 6). Other less common causes were globe abnormalities, malignancies and glaucoma.
 |
Table 6 Causes of Blindness in Nigeria Children |
Quality Appraisal and Risk of Bias
The quality of the studies was adjudged moderate to good. However, almost all studies did not report how non-responders were handled or how missing data were categorised. The quality of the included studies is described in Table S1.
Discussion
The findings obtained in this systematic review are insightful and of importance to clinical and public health research, practice, and policy. To start with, this review is believed to be the first to estimate a representative national prevalence of visual impairment and blindness among Nigerian children. The mean national prevalence (and range) of 3.9 (0.2–15.9), 2.9 (0.1–1.0) and 0.2 (0.1–0.5) percent (%) for mild, moderate and severe visual impairments, respectively, using descriptive statistics. Furthermore, the mean prevalence rate of visual impairment in children per geopolitical zone of Nigeria was determined too. The lowest mean prevalence rate of visual impairment was reported in the south-south geo-political zone (0.75%),34 while the highest prevalence was reported in the north-central geopolitical zone.30 The study found a prevalence rate of 15.9% and 8% for mild and moderate visual impairment, respectively.30 (Table 2).
There were notable differences in the mean prevalence of blindness that we reported concerning the different geo-political zones of the country (Table 2); these may have been attributable to various factors including the varying differences in the number of studies reporting the prevalence of visual impairment and blindness in the different geo-political zones. Other reasons include the lack of data from the Northeastern geo-political zone of the country (this geopolitical zone accounts for 12% of the total Nigerian population).35 In addition, data from the National Eye Care program of Nigeria’s Federal Ministry of Health and Social Welfare show that there is a gap in the availability for all cadres of eye care workers.36 The gap in the eye care workforce may translate to a higher prevalence of blindness among children. The highest gap was reported in the north-western geo-political zone, which has the least ophthalmologist to-patient ratio among all the geopolitical zones in Nigeria.36 It is also the most populous geopolitical zone in the country.37
Cataract was found to be the most common cause of blindness in this review. This is similar to the global picture reported in another systematic review by Yekta et al in 2022.5 According to the National Blindness and Visual Impairment Survey, cataracts were the most common cause of blindness among Nigerian adults, while uncorrected ametropia and cataract were the most important causes of visual impairment.38 While earlier studies (ie, studies conducted before the year 2003) in Nigeria reported corneal opacities and vitamin A deficiency (VAD) as the leading cause of childhood blindness,39 the prevalence of these aetiological factors has profoundly decreased over time due to the implementation of public health policies that had tackled vitamin A deficiency by improving uptake of vitamin A in different parts of Nigeria, and fortification of foods in Nigeria with vitamin A. Other leading causes of blindness were corneal opacities or scars (from diverse causes other than VAD) and optic atrophy.
Cataract blindness is largely both preventable and avoidable. Good-quality cataract surgery is the only acceptable intervention available for the prevention/elimination of cataract blindness across all age groups. Cataract surgery is a bit more challenging in children because of the nature of the paediatric eye, tissue inflammation, postsurgery visual rehabilitation and other peculiarities related to the postoperative care in children.40–42 This explains why after basic ophthalmic training, there is a special training for paediatric ophthalmology to optimize the surgical outcomes. This further justifies the need to train more eye care workers to cover the existing eye care manpower gap in Nigeria.
According to the WHO, spectacle correction (for refractive error) and cataract surgery rank high among all the available health-care interventions. However, distance visual impairment from refractive error and cataract-related visual impairment remain highly prevalent as only about 36% and 17%, respectively, have access to spectacle correction and quality cataract surgery globally.1 This could be largely attributable to poor access to eye care services in low-resource settings like Nigeria. Results from reviews like this are expected to guide planning of policies that help eliminate common causes of blindness and visual impairment.
Interventions such as continuous health education and legislations are effective strategies needed to prevent blindness and visual impairment from most causes reported in this review (such as cataract, ametropia, corneal opacity (from whatever cause), glaucoma, amblyopia, and ocular infections). It is particularly important that stakeholders at all levels remain steadfast in educating people about the negative effects of some harmful traditional eye practices which have been shown to constitute a burden on eye care.43 A recent narrative review in Nigeria has shown that about 16.7%–85.9% people with prior use of traditional eye medications (TEM) were legally blind at presentation to the hospital, while about 7.1–31.4%, 1.8–27.1% and 5.3%–20.8% had normal vision/mild, moderate and severe visual impairment, respectively, at presentation.44,45 The review also presented a comprehensive list of harmful TEM used in Nigeria.43 This further justifies the need for a massive public health enlightenment campaign in Nigeria on the benefits of seeking professional eye care services over traditional services.
We acknowledge the limitations of this systematic review as there were variabilities in the methods used in estimating prevalence of blindness and visual impairment in the included studies. This introduced some methodological and statistical heterogeneities in those included studies. This also prevented a meta-analysis and necessitated the use of descriptive estimates of prevalence values. While we understand this could be a potential source of bias, the results from this review have provided valuable verifiable information on the subject in Nigeria.
Regardless of the above-stated limitations, this review has its strength. To the best of the authors’ knowledge, this review is believed to be the first study to provide nationally representative estimates on the prevalence and causes of blindness among Nigerian children. Also, the findings synthesized in this review provide deep insights that can inform existing and future policies and strategies needed for the eradication of avoidable blindness and visual impairments among Nigerian children.
Conclusion
According to the review, cataract is the most common cause of blindness among Nigerian children, while ametropia and cataract are the most common causes of visual impairment. These and other causes are largely treatable and preventable and invariably render blindness from them avoidable. The prevalence rates of visual impairments and blindness in children in Nigeria may also seem low, but the number of blind years and disability-adjusted life years this may cause the affected children is the major source of concern to stakeholders. The data obtained can inform policies expected to provide strategies and interventions such as continuous health education and monitoring of existing interventions needed to mitigate all the avoidable causes of blindness and visual impairment among Nigerian children.
Data Sharing Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study. All authors have read and approved the final version of the manuscript. The lead author, Ugochukwu A Eze, had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.
Ethical Considerations
Not applicable. This study did not collect data from human or animal subjects but an open research repository.
Funding
This study was self-funded.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. WHO. Vision impairment and blindness [Internet]; 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment.
2. Steinmetz JD, Bourne RRA, Briant PS. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the right to sight: an analysis for the global burden of disease study. Lancet Glob Health. 2021;9(2):e144–e160. PMID: 33275949. doi:10.1016/S2214-109X(20)30489-7
3. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–e1234. PMID: 29032195. doi:10.1016/S2214-109X(17)30393-5
4. IAPB. Child eye health [Internet]. The International Agency for the Prevention of Blindness; 2023. Available from: https://www.iapb.org/learn/vision-atlas/magnitude-and-projections/child-eye-health/.
5. Yekta A, Hooshmand E, Saatchi M, et al. Global prevalence and causes of visual impairment and blindness in children: a systematic review and meta-analysis. J Curr Ophthalmol. 2022;34(1):1–15. PMID: 35620376. doi:10.4103/joco.joco_135_21
6. Ceesay W, Abaidoo B, Braimah IZ. Prevalence of visual impairment among primary school pupils in the Ga West Municipality, Ghana. Niger J Ophthalmol. 2022;30:85–91.
7. O’Neil A. The age structure in Nigeria 2021 [Internet]. Statista; 2023. Available from: https://www.statista.com/statistics/382296/age-structure-in-nigeria/.
8. UNICEF. How many children live in Nigeria? [Internet]. UNICEF DATA. 2022. Available from: https://data.unicef.org/how-many/how-many-children-under-18-live-in-nigeria/.
9. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. PMID: 33782057. doi:10.1136/bmj.n71
10. UNICEF. The convention on the rights of the child: the children’s version. Available from: https://www.unicef.org/child-rights-convention/convention.
11. Downes MJ, Brennan ML, Williams HC, Dean RS. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open. 2016;6(12):e011458. PMID: 27932337. doi:10.1136/bmjopen-2016-011458
12. PHAO/WHO. Visual health. Available from: https://www.paho.org/en/topics/visual-health.
13. Higgins JPT, Lopez-Lopez JA, Becker BJ, et al. Synthesising quantitative evidence in systematic reviews of complex health interventions. BMJ Glob Health. 2019;4(Suppl 1):e000858.
14. Campbell M, Katikireddi SV, Sowden A, Thomson H. Lack of transparency in reporting narrative synthesis of quantitative data: a methodological assessment of systematic reviews. J Clin Epidemiol. 2019;105:1e9. doi:10.1016/j.jclinepi.2018.08.019
15. Ioannidis JPA, Patsopoulos NA, Rothstein HR. Reasons or excuses for avoiding meta-analysis in forest plots. BMJ. 2008;336(7658):1413e5. doi:10.1136/bmj.a117
16. McKenzie JE, Brennan SE. Chapter 12: synthesizing and presenting findings using other methods. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, editors. Cochrane Handbook for Systematic Reviews of Interventions.
17. Capili B. Cross-sectional studies. Am J Nurs. 2021;121(10):59–62. PMID: 34554991; PMCID: PMC9536510. doi:10.1097/01.NAJ.0000794280.73744.fe
18. Adejumo OO, Olusanya BA, Ajayi BG. Ocular disorders among preschool children in Southwest Nigeria. Middle East Afr J Ophthalmol. 2021;28(1):23–28. PMID: 34321819. doi:10.4103/meajo.MEAJO_191_19
19. Adekoya BJ, Balogun MM, Balogun BG, Ngwu RA. Spectrum of congenital defects of the eye and its adnexia in the pediatric age group; experience at a tertiary facility in Nigeria. Int Ophthalmol. 2015;35(3):311–317. PMID: 24743944. doi:10.1007/s10792-014-9946-4
20. Aghaji AE, Ezegwui IR, Shiweobi JO, Mamah CC, Okoloagu MN, Onwasigwe EN. Using key informant method to determine the prevalence and causes of childhood blindness in South-Eastern Nigeria. Ophthalmic Epidemiol. 2017;24(6):401–405. PMID: 2853229114. doi:10.1080/09286586.2017.1320412
21. Ajige J, Muhammad N, Hassan-Wali A. Childhood blindness and visual impairment in a local government area in North-Central Nigeria: a key informant survey: childhood blindness in North Central Nigeria. Niger Med J. 2022;63(1):10–15.
22. Alabi AS, Aribaba OT, Alabi AO, Ilo O, Onakoya AO, Akinsola FB. Visual impairment and ocular morbidities among schoolchildren in Southwest, Nigeria. Niger Postgrad Med J. 2018;25(3):166–171. PMID: 30264768. doi:10.4103/npmj.npmj_85_18
23. Ayanniyi A, Mahmoud AO, Olatunji FO. Causes and prevalence of ocular morbidity among primary school children in Ilorin, Nigeria. Niger J Clin Pract. 2010;13(3):248–253. PMID: 20857778.
24. Duke R, Otong E, Iso M, et al. Using key informants to estimate prevalence of severe visual impairment and blindness in children in Cross River State, Nigeria. J AAPOS. 2013;17(4):381–384. PMID: 23911130. doi:10.1016/j.jaapos.2013.05.004
25. Ezegwui IR, Oguego NC, Okoye OI, et al. Prevalence of refractive errors and visual impairment in school children in Enugu South-East Nigeria. Niger J Clin Pract. 2021;24(3):380–386. PMID: 33723112. doi:10.4103/njcp.njcp_521_19
26. Ezinne NE, Mashige KP. Refractive error and visual impairment in primary school children in Onitsha, Anambra State, Nigeria. Afr Vision Eye Health. 2018;77(1):8. doi:10.4102/aveh.v77i1.455
27. Ezinne NE, Ojukwu CS, Ekemiri KK, Akano OF, Ekure E, Osuagwu UL. Prevalence and clinical profile of glaucoma patients in rural Nigeria-a hospital-based study. PLoS One. 2021;16(12):e0260965. doi:10.1371/journal.pone.0260965
28. Isawumi MA, Adebayo M. Child abuse and the eye in an African population. Korean J Ophthalmol. 2017;31(2):143–150. PMID: 28367043. doi:10.3341/kjo.2017.31.2.143
29. Isawumi MA. Childhood blindness and visual impairment in an underserved population in South West Nigeria: a clinic-based study. East Central Afr J Surg. 2017;22(3):2–10. doi:10.4314/ecajs.v22i3.1
30. Obajolowo TS, Ademola-Popoola DS, Olatunji FO. Prevalence and causes of visual impairment among Nigerian children aged 3 to 5 years. Niger J Ophthalmol. 2019;27(2):76. doi:10.4103/njo.njo_2_19
31. Okoye O, Umeh RE, Ezepue FU. Prevalence of eye diseases among school children in a rural south-eastern Nigerian community. Rural Remote Health. 2013;13(3):2357. PMID: 24093438.
32. Maduka-Okafor FC, Okoye O, Ezegwui I, et al. Refractive error and visual impairment among school children: result of a South-Eastern Nigerian regional survey. Clin Ophthalmol. 2021;15:2345–2353. PMID: 34113078. doi:10.2147/OPTH.S298929
33. Muhammad. Finding children with blindness and visual impairment in five local government areas of Sokoto state using the key informant method [Internet]; 2023. Available from: https://www.sjopthal.net/article.asp?issn=1858-540X;year=2014;volume=6;issue=1;spage=19;epage=23;aulast=Muhammad.
34. Nathaniel G, Pedro-Egbe CN. Vision screening in primary school children in Kegbara-Dere, a rural community in Rivers State, Nigeria. Port Harcourt Med J. 2015;9(1):21–27. doi:10.4314/phmedj.v9i1
35. North East (Nigeria). Wikipedia; 2023.
36. National Eye Health Strategic Development Plan (2024–2028). Federal Ministry of Health & Social Welfare, Nigeria; 2023.
37. Nigerian North West State Governors visit African Development Bank to boost cooperation. African Development Bank; 2023. Available from: https://www.afdb.org/en/news-and-events/press-releases/nigerian-north-west-state-governors-visit-african-development-bank-boost-cooperation-65956.
38. Abdull MM, Sivasubramaniam S, Murthy GV, et al.; Nigeria National Blindness and Visual Impairment Study Group. Causes of blindness and visual impairment in Nigeria: the Nigeria national blindness and visual impairment survey. Invest Ophthalmol Vis Sci. 2009;50(9):4114–4120. doi:10.1167/iovs.09-3507
39. Rabiu MM, Kyari F. Vitamin A deficiency in Nigeria. Niger J Med. 2002;11(1):6–8. PMID: 12073301.
40. Pavlović S. Hirurgija katarakte kod dece [Cataract surgery in children]. Med Pregl. 2000;53(5–6):257–261. Croatian. PMID: 11089366.
41. Vijayalakshmi P, Njambi L. Postoperative care for paediatric cataract patients. Community Eye Health. 2016;29(94):32–34. PMID: 27833262; PMCID: PMC5100472.
42. Mohammadpour M, Shaabani A, Sahraian A, et al. Updates on managements of pediatric cataract. J Curr Ophthalmol. 2019;31(2):118–126. ISSN 2452-2325. doi:10.1016/j.joco.2018.11.005
43. Nathaniel GI, Eze UA. Harmful traditional eye practices in Nigeria and its burden on eye care: a review of literature. Glob J Cataract Surg Res Ophthalmol. 2023;1–9. doi:10.25259/GJCSRO_29_2023
44. Ukponmwan CU, Momoh N. Incidence and complications of traditional eye medications in Nigeria in a teaching hospital. Middle East Afr J Ophthalmol. 2010;17:315–319. doi:10.4103/0974-9233.71596
45. Ajite KO, Fadamiro OC. Prevalence of harmful/traditional medication use in traumatic eye injury. Glob J Health Sci. 2013;5:55–59. doi:10.5539/gjhs.v5n4p55
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.