Back to Journals » Clinical Interventions in Aging » Volume 18
Prevalence and Associated Predictors of Inappropriate and Omitted Medications Prescribing in Older Patients with Advanced Cancer: A Cross-Sectional Study
Authors Al-Azayzih A ![]() , Bani-Ahmad E, Jarab AS
, Bani-Ahmad E, Jarab AS ![]() , Kharaba Z, Al-Kubaisi K
, Kharaba Z, Al-Kubaisi K ![]()
Received 4 August 2023
Accepted for publication 25 September 2023
Published 2 October 2023 Volume 2023:18 Pages 1653—1661
DOI https://doi.org/10.2147/CIA.S430208
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Ahmad Al-Azayzih,1 Enas Bani-Ahmad,1 Anan S Jarab,1,2 Zelal Kharaba,2,3 Khalid Al-Kubaisi4
1Department of Clinical Pharmacy, Faculty of Pharmacy, Jordan University of Science and Technology, Irbid, 22110, Jordan; 2College of Pharmacy, AL Ain University, Abu Dhabi, United Arab Emirates; 3Honorary Associate Lecturer, Faculty of Medical Sciences, Newcastle University, Newcastle Upon Tyne, UK; 4Department of Pharmacy Practice and Pharmacotherapeutics, College of Pharmacy, University of Sharjah, Sharjah, United Arab Emirates
Correspondence: Ahmad Al-Azayzih, Clinical Pharmacy Department, Faculty of Pharmacy-Jordan University of Science and Technology, Irbid, 22110, Jordan, Email [email protected]
Aims of the Study: This study aimed to identify the prevalence and significant predictors of both potentially inappropriate medications (PIMs) and potentially omitted medications (POMs) events among geriatric patients with advanced cancer using the STOPP (Screening Tool of Older Persons’ Prescriptions) and START (Screening Tool to Alert to Right Treatment) criteria.
Methods: This retrospective cross-sectional study included patients aged ≥ 65 years who were diagnosed and treated for advanced stage of cancer. Patients’ medical charts were evaluated to identify polypharmacy (≥ 5 medications) prevalence as well as potential PIMs and POMs incidents and their associated predictors. SPSS software was used to perform the analysis. Multivariate logistic regression models were used to identify factors associated with dependent variables including PIMs use and POMs.
Results: Electronic medication charts of 510 patients were evaluated. The average age of the patients was 73.25 years, and 264 (51.8%) patients were males. The average number of medications prescribed per patient was 10.3 (range– 2– 26). Polypharmacy was present in 85.9% of patients, while excessive polypharmacy prevalence was 52.2%. At least one PIM was encountered in 253 patients (49.6%), while at least one POM was encountered in all patients owing to the omission of pneumococcal vaccines. The most common PIMs were opioid analgesics, followed by benzodiazepines, and hypnotics. Additionally, the most omitted medications, excluding vaccinations, were cardiovascular agents and laxatives in patients on regular opioid analgesics. Polypharmacy and diagnosis with solid cancer compared to hematological cancer were associated with increased odds for PIMs occurrence (ORs = 1.293 (p < 0.001) and 3.022 (p = 0.03), respectively), while coexistence of hypertension diagnosis in cancer patients was associated with increased the odds for POMs events (OR = 2.286 (p = 0.007)).
Conclusion: Polypharmacy, PIMs, and POMs were highly prevalent among older cancer patients based on the polypharmacy definition and STOPP/START Criteria.
Keywords: START, STOPP, geriatrics, inappropriate medications, omitted medications, cancer
Introduction
Geriatric patients who present with chronic medical conditions, including cancer, and thus, a high number of prescribed treatment regimens, are at a high risk of developing medication-related problems.1,2 Cancer treatment in this group is generally associated with a high level of medical burden and adverse drug events owing to the nature of the disease itself and the requirement for complex regimens to palliate or cure cancer.3
The geriatric population is growing worldwide, and the need for medical healthcare is increasing. Reports from the United Nations expected a fast growth in geriatric population, as it is expected that approximately 16% of the world population will be 65 years old or older by the year of 2050.4 Evaluating the appropriateness of medications and the rationality of their use in the geriatric population is essential and fundamental for improving health outcomes and quality of life.5
Several studies have emphasized that polypharmacy and inappropriate prescribing could lead to greater utilization of healthcare facilities, such as more frequent hospitalization, emergency visits, re-admission, and lengthening the hospital stay for older cancer patients.6,7
Several criteria have been developed to identify inappropriate prescription of medication among geriatric groups8,9 as well as to identify the omission of necessary drugs for their health conditions.9
The Screening Tool of Older Persons’ Potentially Inappropriate Prescriptions (STOPP) and Screening Tool to Alert Doctors to Right Medication Treatments (START) were developed and validated in 2008 and updated by 2015 and 2023 to address inappropriate prescribing and omitted medications in the older patients, respectively.9–12
According to the STOPP/START criteria, Potentially Inappropriate Medications (PIMs) prescribing means that medications have no additional value; in contrast, they could lead to drug-related problems in patients. Potentially Omitted Medications (POMs) are generally identified as medications that should be prescribed for patients owing to their additional beneficial clinical value for their disease conditions.9
Reports of the department of statistics in Jordan in 2022 indicated that older people (≥65 years) represented 7.52% of total Jordanian population.13 In addition to that, prevalence of cancer in Jordan is increasing in a higher rate compared to other age groups among Jordanian population.14
PIMs and POMs are considered serious concerns for healthcare facilities worldwide. A few studies have been conducted previously to assess both PIMs and POMs prevalence and predictors of both PIMs and POMs among geriatric patients in Jordan.15,16 However, no study has evaluated the prevalence and burden of PIMs and POMs among geriatric cancer patients in Jordan. Therefore, we aimed to examine and identify PIMs and POMs and specific factors that might lead to more associated increases in PIMs and POMs incidence in Jordanian older patients.
Methodology
Ethical Approval
Ethical approval was obtained from the Institutional Review Board (IRB) committee at Jordan University of Science and Technology (JUST) and its affiliated teaching hospital, the King Abdullah University Hospital (KAUH) with approval number: 61/147-2022. Prior to data collection and study conduction. As the data were evaluated retrospectively and were only obtained for treatment purposes, the requirement for informed consent was waived by the Institutional Review Board (IRB) committee at JUST and KAUH. All methods were performed in accordance with the relevant guidelines and regulations of the KAUH and Jordan University of Science and Technology (JUST) Research Council. This study complies with the Declaration of Helsinki recommendations.
Study Population, Setting, and Characteristics
This retrospective cross-sectional study assessed potentially inappropriate prescriptions and omitted medications according to the STOPP and START criteria version 3.9 The study was led by licensed pharmacists who conducted an extensive medication chart review for geriatric patients (≥65 years old) between the period of January 2020 and January 2023 who were admitted to King Abdullah University Hospital (KAUH), which is considered a leading tertiary hospital in Jordan, to receive chemotherapy under the supervision of hematologist/oncologist physicians. Only patients with advanced-stage cancer (stage 3 and 4 for solid tumors and their counterpart classification for hematological cancers) were included in this study. Patients admitted for palliative care, patients without kidney function test or other tests (eg, blood pressure, electrolytes level, pulmonary functions test), patients at their early stage of cancer therapy were not included in the study.
The medication charts of 510 patients were included for further evaluation during the study period. Data on patient demographics and clinical parameters were collected for this study. Patient age, height, sex, chronic medical conditions (comorbidities), and cancer type were obtained from the electronic medical system of KAUH. The Cockcroft-Gault formula was used to assess the creatinine clearance values for each patient.
Polypharmacy, PIMs, and POMs Identifications
Polypharmacy was assessed in the study sample based on the total number of medications prescribed, excluding chemotherapy medications (STOPP and START criteria do not include chemotherapy in their assessment). We further classified polypharmacy prevalence into either polypharmacy (more than or equal to 5 medications but less than 10) and excessive polypharmacy (≥10 medications per patient).17
STOPP criteria version 2 was used to identify potentially inappropriate medications prescribed to geriatric patients. The START criteria with all their details were used for potentially omitted prescriptions from the same patient group. The Anatomical Therapeutic Chemical (ATC) and STOPP/START classifications were used to identify the prevalence of both PIMs and POMs among patients.
Statistical Analysis
Data were analyzed utilizing the Statistical Package for Social Sciences (SPSS Statistics for Windows, version 22). Continues variable (age) was evaluated using mean ±standard deviation. Categorical variables such as gender, comorbidities, type of cancer, PIMs, and POMs were described using frequencies and percentages. Univariable logistic regressions for each dependent variable including PIMs use according to STOPP criteria and POMs according to START criteria were applied to determine the association of independent variables (age, gender, chronic comorbidities, polypharmacy, and type of cancer) with the dependent variables. All independent variables with p ≤0.20 determined by the univariate analysis were included in the multivariate logistic regression analysis to determine the factors that are independently associated with dependent variables (PIMs use or POMs). For each logistic model, dependent variable responses were categorized as yes response (1) for being prescribed PIMs according to STOPP criteria or no responses (0) for being not prescribed PIMs. Same applied (Yes = 1, No = 0) responses were applied for other dependent variables (POMs according to START criteria). Results from multivariate logistic regression were presented to include odd ratio (OR), 95% confidence interval, and P-value. P value of less than 0.05 was assumed statistically significant.
Results
This study included 510 medical records of geriatric cancer patients. The average age of patients in years ± standard deviation was 73.25± 7.20. The study included 264 men (51.8% of the total subjects). Hypertension, diabetes mellitus, and ischemic heart disease were the three most common comorbid conditions found among patients. Solid cancers represented the majority of the cancer cases among studied subjects, with total number of 454 cases (89.0%) (Table 1).
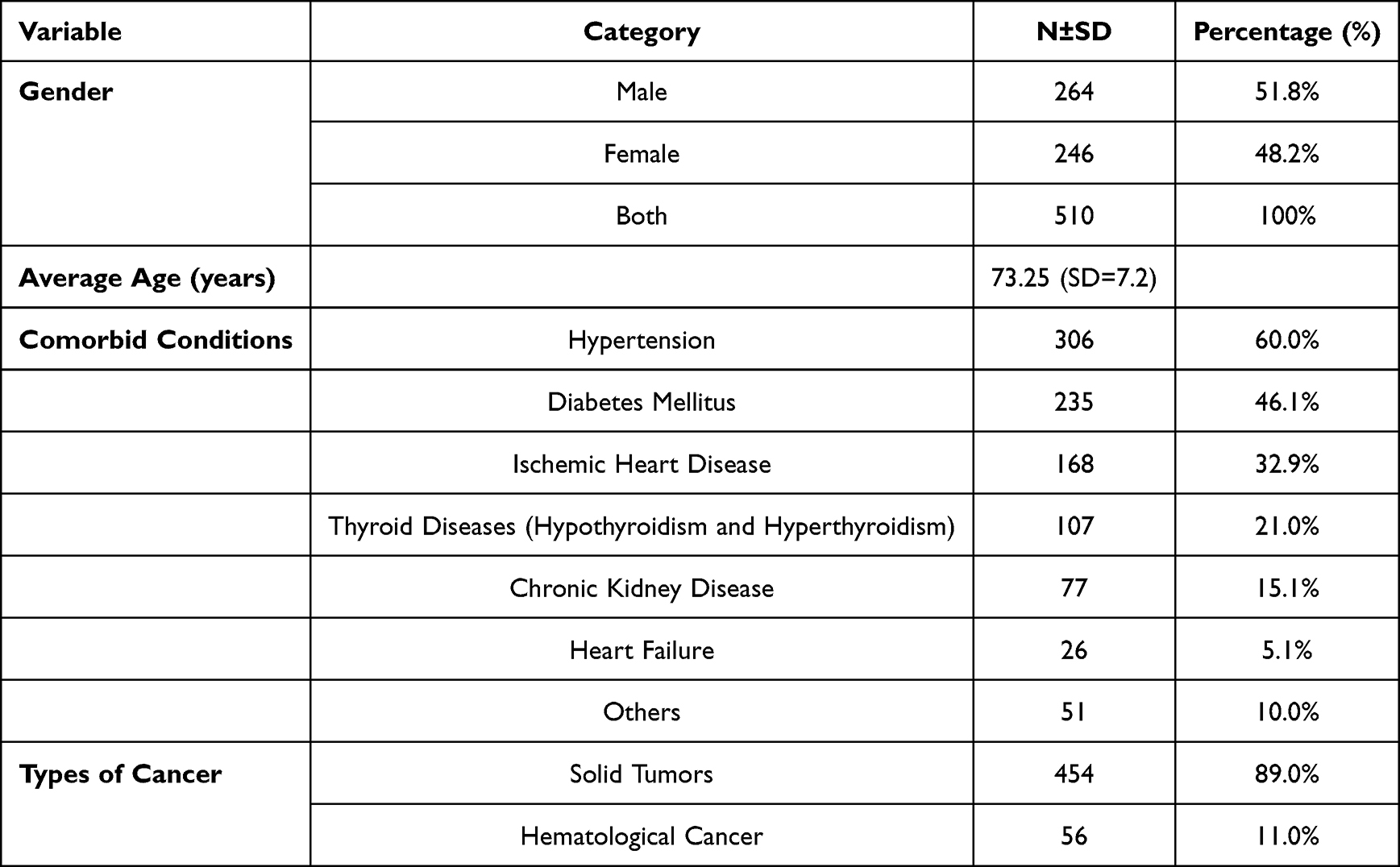 |
Table 1 Patients Characteristics |
In total, geriatric cancer patients in this study were prescribed 5253 medications excluding either chemotherapy or supportive care medicines, with an average number of 10.3 medications per patient (range 2–26).
According to standard definition of polypharmacy (using five or more medications), 438 (85.9%) patients were identified as having a polypharmacy prescription, on the other hand, excessive polypharmacy was identified in 266 patients (52.2%).
This study showed that a total of 270 PIMs based on STOPP criteria were identified among 253 patients who had at least one PIM in their medication prescribed (Table 2). Moreover, the study found that at least one POM was prevalent in all patients (did not receive pneumococcal vaccine) with a total number of POMs identified equal to 658 medications (Table 3).
 |
Table 2 Potentially Inappropriate Medications According to STOPP Criteria |
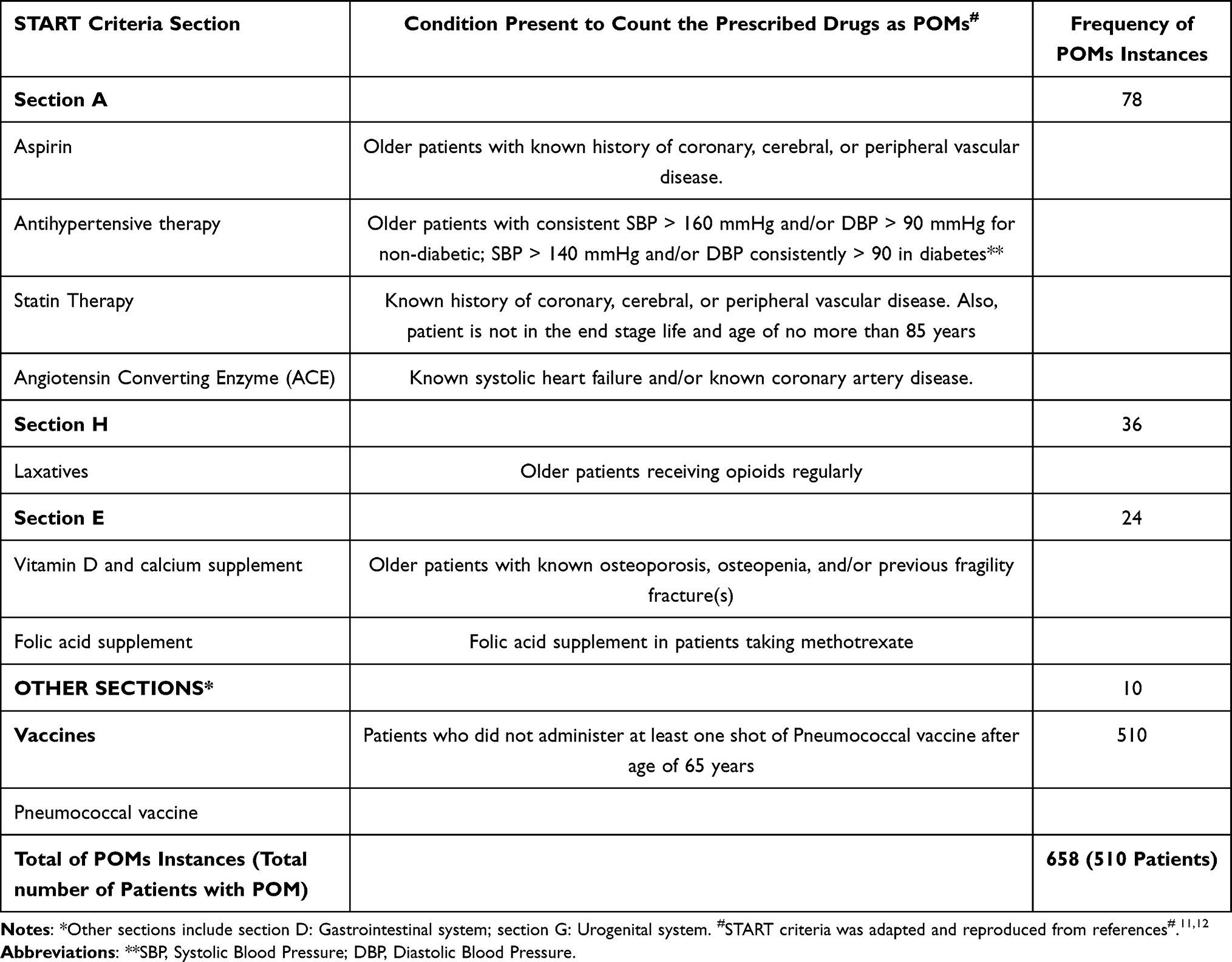 |
Table 3 Potentially Omitted Medications (POMs) According to START Criteria |
Furthermore, our study found that the most common PIMs were analgesics (n = 103), followed by drugs that increase the risk of falls in geriatric patients (n = 66), such as benzodiazepines and hypnotics, and drugs with an anticholinergic/antimuscarinic burden (n = 26) (Table 2).
The most common POMs encountered in this study were vaccines (charts revealed that none of the patients received a pneumococcal vaccine according to the START criteria). The second most common (n = 78) POMs identified in this study were section A medications for cardiovascular diseases, including aspirin, antihypertensive, and statin therapies, as well as angiotensin converting enzyme inhibitors. Lack of laxative administration in patients receiving opioid medications was the third most common POMs encountered (n = 36) (Table 3).
Identifying at least one PIMs was associated significantly with polypharmacy (adjusted OR = 1.293; 95% CI: 1.201–1.391, p < 0.001) and type of cancer. Solid cancer found to increase odd of PIMs occurrence by around 3 folds when compared to hematological cancers (adjusted OR = 3.022; CI: 1.114–8.199, p < 0.030). The other studied predictors (female sex and age, comorbidities including diabetes and ischemic heart disease) were not associated with a significant increase in PIMs incidence (Table 4).
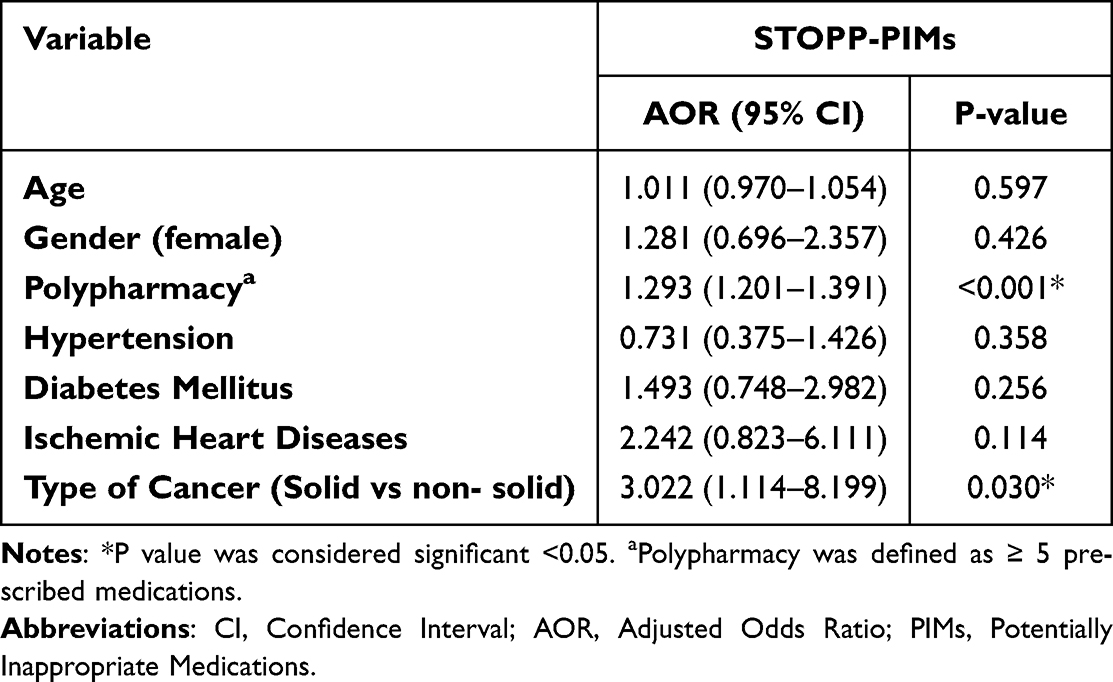 |
Table 4 Predictors of Potentially Inappropriate Medications Prescribing in Geriatrics Patients |
Finally, identifying at least one POMs was associated significantly with co-existence of hypertension condition among patients. Hypertension associated with increase in the odds of developing POMs events by more than 2 folds (adjusted OR = 2.286; C.I: 1.259–4.149, P = 0.007). In opposite to that, patients diagnosed with ischemic heart diseases (IHD) showed lower odds for having POMs events compared to those with no IHD (adjusted OR = 0.333; C.I: 0.159–0.695, P = 0.003) (Table 5).
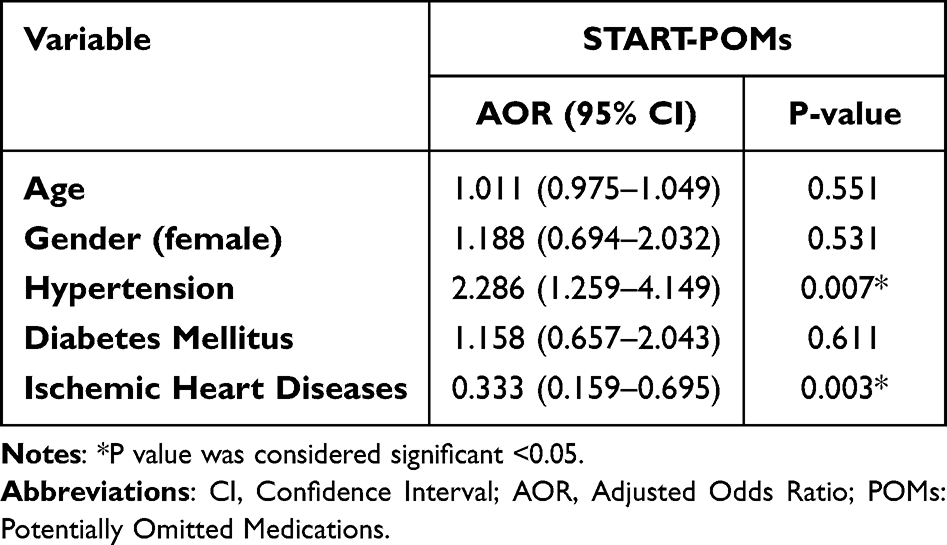 |
Table 5 Predictors of Potentially Omitted Medications Prescribing in Geriatrics Patients |
Discussion
To the best of our knowledge, this study is the first to identify the prevalence and potential predictors of potentially inappropriate (PIMs) and omitted medications (POMs) used in Jordanian older patients diagnosed with cancer, where STOPP/START criteria were utilized to identify PIMs and POMs events, respectively.
This study found that both PIMs (49.6% of the study patients) and POMs (100% of the study patients) are highly prevalent among patients with cancer in Jordan. PIMs were comparable to previous reports, where they were found to range from 18% to 73.3%.18–22 A recent study has shown a higher prevalence of PIMs compared to other studies because of their different study approaches depending not only on medical record evaluation but also on utilizing a detailed medication review to identify PIMs based on both STOPP/START regular criteria and experienced pharmacist evaluation for PIMs.21 Similar study from Jordan which included patients with chronic conditions who were admitted to hospital reported high prevalence of PIMs on admission and during their stay at the hospital (72% and 92% respectively).15 In addition, our previous study indicated that 62.5% of geriatric patients who visited outpatient clinics for their chronic conditions, but not cancer had at least 1 PIMs prescribed based on Beers criteria definition for PIMs.16
Analgesics, benzodiazepines, and anticholinergic medications were the three most common groups of medications associated with PIMs in our study. Such prescriptions are not surprising, as they are frequently used in patients with cancer. Results from previous studies have shown that cardiovascular medications,23 benzodiazepines,24 and proton pump inhibitors21 were the most prevalent PIMs prescribed among geriatric patients with either hematological or solid types of cancer.
In contrast, POMs were highly prevalent among the study subjects. Almost all patients had at least one reported POM and were mainly attributed to omitted vaccine administration, including pneumococcal vaccines. Similarly, a study from Turkey linked the majority of POMs incidents to omitted vaccinations in geriatric cancer outpatients.18 Other studies on POMs identification have reported a POMs prevalence ranging from 40% to 98.3%.18,21,25 Excluding omitted vaccination from the POMs analysis led to a relatively low level of POMs occurrence in our patients compared to previous reports. In agreement to high extent with previous studies, omitted cardiovascular medications, including aspirin, statins, and antihypertensive medications, contributed to the high prevalence of POMs incidents, followed by omitted laxatives, calcium, vitamin D, and folic acid supplements.21,26,27
The STOPP/START criteria assess PIMs and POMs events based on regular drugs not including either chemotherapy or immunotherapy; thus, the STOPP/START criteria are considered highly applicable for evaluating inappropriate and omitted prescriptions in cancer patients with no difference to older patients without cancer. In addition, the START/STOPP criteria have been used extensively in other studies to assess and identify both PIMs and POMs in geriatric patients with cancer.
Polypharmacy has been associated with a significantly increased health burden among older patients, including adverse drug events, drug–drug interactions, poor medication adherence, and various geriatric syndromes resulting from a functional decline in organ function. However, polypharmacy could complicate the disease conditions of cancer patients and negatively affect their treatment outcomes negatively.6,28–30
The findings from this study showed that polypharmacy was significantly associated with a higher prevalence of PIMs reporting. Also, types of cancer showed significant correlation with PIMs occurrence. Patients with solid cancer were associated with higher odds of developing PIMs compared to those who had hematological type of cancer (eg, leukemia). In concordance with published studies, polypharmacy was a highly significant independent predictor for reporting a greater number of PIMs and adverse treatment outcomes in older patients with and without cancer.3,16,31 Higher odds in PIMs due to differences in type of cancer (solid vs hematological) might be explained by the higher prevalence of solid tumors collectively compared to hematological cancer among geriatric populations. According to retrospective analysis for Jordan cancer registry, solid tumors including colorectal, breast, lung, prostate, and bladder cancers were the most common cancers encountered among Jordanian population.14 In contrast to our findings, an earlier observational study indicated no statistically significant difference between solid and hematological malignancy from one side and the increased level of PIMs/POMs occurrence on the other side.21
Investigating the predictors for POMs among geriatric patients with advanced-stage cancer, this study revealed a significant association between hypertension comorbidity and increased risk of POMs occurrence. This study results were in agreement with earlier studies which showed that omissions of cardiovascular medications represent the most common omissions among geriatric patients with and without cancer.21,32,33
The limitations of this study include the retrospective nature of the medical record evaluations, even though researchers evaluated the medical charts carefully to ensure a high level of accuracy for patient data extraction. Second, some factors such as performance status of the patients and over the counter and self-medications taking which could contribute to PIMs and POMs occurrence were not evaluated in this study. Third, while the STOPP/START instrument is considered highly applicable for evaluating PIMs and POMs in geriatric patients, it is still not inclusive without clinical judgment based on evidence-based knowledge. Although this study has several limitations, it is the first to shed light on PIMs and POMs events among the understudied geriatric cancer population in Jordan.
Conclusion
This study showed that prescriptions of both PIMs and POMs are highly prevalent among geriatric patients with cancer. Polypharmacy and type of cancer (solid tumors) are significantly associated with predicting prevalence increases in PIMs. While co-existed hypertension condition was associated with increased prevalence of POMs. Clinical strategies implementation to identify and prevent omitted and inappropriate prescriptions must be promoted and supported.
Data Sharing Statement
The data will be available from the corresponding author on reasonable request.
Funding
This research was approved by the Deanship of Research at Jordan University of Science and Technology, Irbid, Jordan (Approval Number is 33-2022). No funding was received for this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Yeoh TT, Tay XY, Si P, Chew L. Drug-related problems in elderly patients with cancer receiving outpatient chemotherapy. J Geriatr Oncol. 2015;6(4):280–287. PubMed PMID: 26088749. doi:10.1016/j.jgo.2015.05.001
2. Ortland I, Mendel Ott M, Kowar M, et al. Medication risks in older patients (70 +) with cancer and their association with therapy-related toxicity. BMC Geriatr. 2022;22(1):716. PubMed PMID: 36042410; PubMed Central PMCID: PMCPMC9429305. doi:10.1186/s12877-022-03390-z
3. Mohamed MR, Mohile SG, Juba KM, et al. Association of polypharmacy and potential drug-drug interactions with adverse treatment outcomes in older adults with advanced cancer. Cancer. 2023;129(7):1096–1104. PubMed PMID: 36692475. doi:10.1002/cncr.34642
4. United Nations; 2023. Available from: https://www.un.org/en/global-issues/ageing.
5. Barlow A, Prusak ES, Barlow B, Nightingale G. Interventions to reduce polypharmacy and optimize medication use in older adults with cancer. J Geriatr Oncol. 2021;12(6):863–871. PubMed PMID: 33353854. doi:10.1016/j.jgo.2020.12.007
6. Choi DW, Kang H, Zhang HS, Jhang H, Jeong W, Park S. Association of polypharmacy with all-cause mortality and adverse events among elderly colorectal cancer survivors. Cancer. 2023;129(17):2705–2716. PubMed PMID: 37118834. doi:10.1002/cncr.34813
7. Feng X, Higa GM, Safarudin F, Sambamoorthi U, Tan X. Potentially inappropriate medication use and associated healthcare utilization and costs among older adults with colorectal, breast, and prostate cancers. J Geriatr Oncol. 2019;10(5):698–704. PubMed PMID: 30772191. doi:10.1016/j.jgo.2019.01.012
8. By the American Geriatrics Society Beers Criteria Update Expert P. American Geriatrics Society 2019 Updated AGS Beers Criteria(R) for potentially inappropriate medication use in older adults, J Am Geriatr Soc. 2019;67(4):674–694. PubMed PMID: 30693946. doi:10.1111/jgs.15767
9. O’Mahony D, Cherubini A, Guiteras AR, et al. STOPP/START criteria for potentially inappropriate prescribing in older people: version 3. Eur Geriatr Med. 2023. PubMed PMID: 37256475. doi:10.1007/s41999-023-00777-y
10. Gallagher P, Ryan C, Byrne S, Kennedy J, O’Mahony D. STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther. 2008;46(2):72–83. PubMed PMID: 18218287. doi:10.5414/cpp46072
11. O’Mahony D, O’Sullivan D, Byrne S, O’Connor MN, Ryan C, Gallagher P. STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing. 2015;44(2):213–218. PubMed PMID: 25324330; PubMed Central PMCID: PMCPMC4339726. doi:10.1093/ageing/afu145
12. Mahony DO, Sullivan DO, Byrne S, Connor MNO, Ryan C, Gallagher P. Corrigendum: STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing. 2018;47(3):489. PubMed PMID: 29182733; PubMed Central PMCID: PMCPMC5920325. doi:10.1093/ageing/afx178
13. Department of Statistics-Jordan; 2023. Available from: https://dosweb.dos.gov.jo/.
14. Abdel-Razeq H, Mansour A, Bater R. Trends, patterns, and treatment outcomes of cancer among older patients in Jordan: a retrospective analysis of national cancer registry and institutional outcome data. JCO Glob Oncol. 2020;6(6):745–751. PubMed PMID: 32437264; PubMed Central PMCID: PMCPMC7268897. doi:10.1200/GO.20.00044
15. Abu Hammour K, Abdel Jalil M, AlHabeis S, Abu Hammour G, Manaseer Q. Prevalence of potentially inappropriate prescribing in older adults in Jordan: application of the STOPP criteria. Australas J Ageing. 2021;40(1):e70–e78. PubMed PMID: 33247532. doi:10.1111/ajag.12855
16. Al-Azayzih A, Alamoori R, Altawalbeh SM. Potentially inappropriate medications prescribing according to Beers criteria among elderly outpatients in Jordan: a cross sectional study. Pharm Pract. 2019;17(2):1439. PubMed PMID: 31275497; PubMed Central PMCID: PMCPMC6594439. doi:10.18549/PharmPract.2019.2.1439
17. O’Dwyer M, Peklar J, McCallion P, McCarron M, Henman MC. Factors associated with polypharmacy and excessive polypharmacy in older people with intellectual disability differ from the general population: a cross-sectional observational nationwide study. BMJ Open. 2016;6(4):e010505. PubMed PMID: 27044582; PubMed Central PMCID: PMCPMC4823458. doi:10.1136/bmjopen-2015-010505
18. Paksoy C, Ozkan O, Ustaalioglu BB, et al. Evaluation of potentially inappropriate medication utilization in elderly patients with cancer at outpatient oncology unit. J Oncol Pharm Pract. 2019;25(6):1321–1327. PubMed PMID: 30045684. doi:10.1177/1078155218788698
19. Karuturi MS, Holmes HM, Lei X, et al. Potentially inappropriate medications defined by STOPP criteria in older patients with breast and colorectal cancer. J Geriatr Oncol. 2019;10(5):705–708. PubMed PMID: 30795923; PubMed Central PMCID: PMCPMC6699920. doi:10.1016/j.jgo.2019.01.024
20. Hong S, Lee JH, Chun EK, et al. Polypharmacy, inappropriate medication use, and drug interactions in older Korean patients with cancer receiving first-line palliative chemotherapy. Oncologist. 2020;25(3):e502–e511. PubMed PMID: 32162799; PubMed Central PMCID: PMCPMC7066695. doi:10.1634/theoncologist.2019-0085
21. van Loveren F, van Berlo-van de Laar IRF, Imholz ALT, van ‘t Riet E, Taxis K, Jansman FGA. Prevalence and follow-up of potentially inappropriate medication and potentially omitted medication in older patients with cancer - The PIM POM study. J Geriatr Oncol. 2021;12(1):80–84. PubMed PMID: 32641251. doi:10.1016/j.jgo.2020.06.014
22. Martinez-Ruiz MG, Corona-Ruiz F, Solis-Rivera AP, et al. Potentially inappropriate prescriptions in geriatric patients hospitalized in the internal medicine department of a referral hospital in Mexico. Gac Med Mex. 2023;159(2):147–153. PubMed PMID: 37094248. doi:10.24875/GMM.M23000763
23. Ramsdale E, Mohamed M, Yu V, et al. Polypharmacy, potentially inappropriate medications, and drug-drug interactions in vulnerable older adults with advanced cancer initiating cancer treatment. Oncologist. 2022;27(7):e580–e588. PubMed PMID: 35348764; PubMed Central PMCID: PMCPMC9255971. doi:10.1093/oncolo/oyac053
24. Saarelainen LK, Turner JP, Shakib S, et al. Potentially inappropriate medication use in older people with cancer: prevalence and correlates. J Geriatr Oncol. 2014;5(4):439–446. PubMed PMID: 25127252. doi:10.1016/j.jgo.2014.07.001
25. Mohammed MA, Chan AHY, Chan S, et al. Potentially inappropriate medications and potential prescribing omissions in hospitalised older adults in New Zealand: a retrospective study. Australas J Ageing. 2023. PubMed PMID: 37170714. doi:10.1111/ajag.13210
26. Reis CM, Dos Santos AG, de Jesus Souza P, Reis AMM. Factors associated with the use of potentially inappropriate medications by older adults with cancer. J Geriatr Oncol. 2017;8(4):303–307. PubMed PMID: 28602709. doi:10.1016/j.jgo.2017.05.003
27. Dalleur O, Spinewine A, Henrard S, Losseau C, Speybroeck N, Boland B. Inappropriate prescribing and related hospital admissions in frail older persons according to the STOPP and START criteria. Drugs Aging. 2012;29(10):829–837. PubMed PMID: 23044639. doi:10.1007/s40266-012-0016-1
28. Faisal S, Zairina E, Nathishuwan S, Khotib J, Kristina SA, Nugraheni G. Prevalence and predictors of excessive polypharmacy in geriatric inpatients: a retrospective cross-sectional study in Indonesia. J Prim Care Community Health. 2023;14:21501319231178595. PubMed PMID: 37306336; PubMed Central PMCID: PMCPMC10272682. doi:10.1177/21501319231178595
29. Wang Y, Li X, Jia D, et al. Exploring polypharmacy burden among elderly patients with chronic diseases in Chinese community: a cross-sectional study. BMC Geriatr. 2021;21(1):308. PubMed PMID: 33985446; PubMed Central PMCID: PMCPMC8117611. doi:10.1186/s12877-021-02247-1
30. Schenker Y, Park SY, Jeong K, et al. Associations between polypharmacy, symptom burden, and quality of life in patients with advanced, life-limiting illness. J Gen Intern Med. 2019;34(4):559–566. PubMed PMID: 30719645; PubMed Central PMCID: PMCPMC6445911. doi:10.1007/s11606-019-04837-7
31. Prithviraj GK, Koroukian S, Margevicius S, Berger NA, Bagai R, Owusu C. Patient characteristics associated with polypharmacy and inappropriate prescribing of medications among older adults with cancer. J Geriatr Oncol. 2012;3(3):228–237. PubMed PMID: 22712030; PubMed Central PMCID: PMCPMC3375830. doi:10.1016/j.jgo.2012.02.005
32. Abukhalil AD, Al-Imam S, Yaghmour M, et al. Evaluating inappropriate medication prescribing among elderly patients in Palestine using the STOPP/ START criteria. Clin Interv Aging. 2022;17:1433–1444. PubMed PMID: 36193223; PubMed Central PMCID: PMCPMC9526426. doi:10.2147/CIA.S382221
33. Hanna V, Chahine B, Al Souheil F. Under-prescription of medications in older adults according to START criteria: a cross-sectional study in Lebanon. Health Sci Rep. 2022;5(5):e759. PubMed PMID: 35949679; PubMed Central PMCID: PMCPMC9358532. doi:10.1002/hsr2.759
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluating Inappropriate Medication Prescribing Among Elderly Patients in Palestine Using the STOPP/ START Criteria
Abukhalil AD, Al-Imam S, Yaghmour M, Abushama R, Saad L, Falana H, Naseef HA
Clinical Interventions in Aging 2022, 17:1433-1444
Published Date: 27 September 2022
Medication Adherence and Its Associated Determinants in Older Adults with Type 2 Diabetes and Cardiovascular Comorbidities
Al-Azayzih A, Kanaan RJ, Altawalbeh SM, Al-Qerem W, Smadi S
Patient Preference and Adherence 2023, 17:3107-3118
Published Date: 29 November 2023