Back to Journals » Journal of Blood Medicine » Volume 13
Prevalence and Associated Factors for Post-Caesarean Delivery Blood Transfusion in Eastern Sudan: A Cross-Sectional Study
Authors Mandar O, Hassan B ![]() , Abdelbagi O, Eltayeb R, ALhabardi N, Adam I
, Abdelbagi O, Eltayeb R, ALhabardi N, Adam I ![]()
Received 25 December 2021
Accepted for publication 5 May 2022
Published 9 May 2022 Volume 2022:13 Pages 219—227
DOI https://doi.org/10.2147/JBM.S355846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Omer Mandar,1 Bahaeldin Hassan,2 Omer Abdelbagi,1 Reem Eltayeb,1 Nadia ALhabardi,3 Ishag Adam3
1Department of Obstetrics and Gynecology, Faculty of Medicine, Gadarif University, Gadarif, Sudan; 2Department of Obstetrics and Gynecology, College of Medicine, King Khalid University, Abha, Saudi Arabia; 3Department of Obstetrics and Gynecology, Unaizah College of Medicine and Medical Sciences, Qassim University, Unaizah, Kingdom of Saudi Arabia
Correspondence: Omer Mandar, Department of Obstetrics and Gynecology, Faculty of Medicine, Gadarif University, P.O Box 449, Gadarif, 32211, Sudan, Fax +249 44143162, Email [email protected]
Background: Obstetric haemorrhage is a leading cause of maternal mortality and morbidity worldwide. Caesarean delivery (CD) is associated with significant blood loss, which may require blood transfusions. This study aimed to determine the prevalence and associated factors for post-CD transfusion.
Methods: A cross-sectional study was conducted in Gadarif maternity hospital, eastern Sudan, from March to September 2020. Sociodemographic, obstetric and clinical data, including pre- and postoperative haemoglobin levels, were collected. A multivariate logistic regression analysis was performed.
Results: A total of 539 women were enrolled in the study; the median (interquartile range) age of these women was 28.0 (8.0) years. The overall post-CD transfusion rate was 8.2%. Emergency CD (adjusted odds ratio [AOR]=2.57, 95% confidence interval [CI]=1.25‒5.28) and antepartum haemorrhage (AOR=44.70, 95% CI=11.18‒178.76) were associated with increased risk of post-CD blood transfusion. Preoperative haemoglobin (AOR=0.48, 95% CI=0.36‒0.64) and rural residence (AOR=0.45, 95% CI=0.22‒0.93) were associated with reduced risk for post-CD blood transfusion.
Conclusion: The overall prevalence of post-CD transfusion in this part of Sudan is 8.2%. Women with emergency CD, low preoperative haemoglobin levels and antepartum haemorrhage were at higher risk for post-CD transfusion. Risk identification and correction of antenatal anaemia can reduce the hazard of blood transfusion among CD women.
Keywords: caesarean delivery, blood transfusion, haemoglobin, antepartum haemorrhage, Sudan
Introduction
Postpartum haemorrhage (PPH) is a major public health problem that can lead to maternal near miss, mortality and morbidity.1 Caesarean delivery (CD) is the main risk for both intraoperative and postpartum haemorrhage.2 Blood loss of more than 1000 mL after CD is considered as a postpartum haemorrhage.3 Consequently, blood transfusion following CD is not an uncommon practice in obstetrics.4–6
There is a global increase in the rate of CD, particularly in the Sub-Saharan African region.7 The rate of post-CD blood transfusion varies from 0.36% in developed countries8 to 25.2% in developing countries.9
There are several preoperative, intraoperative and postoperative factors such as anaemia, previous uterine scar, multiparity,4,5,10 operation time, adhesions5,6,10 and uterine atony10,11 were associated with post-CD blood transfusion. Moreover, placenta previa and abruption, repeated scar, prolonged second stage CD and cephalopelvic disproportion were associated with post-CD blood transfusion.5,12,13
Blood transfusion is a life-saving procedure; however, it carries the risk of infections, transfusion reactions (including anaphylactic shock) and death.14 These risks necessitates the use of blood transfusion only for genuine indications. A haemoglobin level of less than 8g/dl has been recommended as a cut-off for blood transfusion.15
In the Sub-Saharan African region, reservation of two units of blood for elective CD is commonly practiced.5 Early detection of the risk factors for post-CD blood transfusion alerts physicians to prepare blood for timed interventions.
In Sudan, there is an increase in CD rates.16 Haemorrhage following CD has been reported as the major cause of maternal near miss and mortality in Sudan.17,18
We aim to assess the prevalence of blood transfusion and its associated factors among Sudanese women who have undergone CD in Gadarif maternity hospital, eastern Sudan. Data from this study are expected to reduce maternal mortality and morbidity related to post-CD blood transfusion in Sudan. This can be achieved through risk identification and proper intervention.
Methods
A cross-sectional study was conducted at Gadarif maternity hospital, eastern Sudan, during the period of March 1 to September 30, 2020.
Inclusion Criteria
All women who underwent emergency or elective CD during the study period were included.
Exclusion Criteria
Women who transfused intraoperatively and those with chronic haemolytic anaemia were excluded.
Sample Size
Sample size (539) was calculated based on the assumption that prevalence of post-caesarean blood transfusion would be 20.0% (ratio of 4:1). This assumption was based on a similar study in the region.5 Moreover, assumed that 40.0% of women who required blood transfusion had preoperative anaemia while 25.0% of women who did not require blood transfused had anaemia. This sample had a 95% confidence level and a 5% confidence limit. The sample size was calculated using the OpenEpi.19
Data Collection
Two medical officers gathered sociodemographic information (age, parity, education, occupation and residence). Maternal weight and height were recorded, and body mass index (BMI) was calculated preoperatively. Preoperative data also included haemoglobin level, gestational age at time of delivery, history of uterine surgery and pregnancy complications (gestational or chronic hypertension and diabetes). Obstetric conditions such as placental abnormality (placenta previa and abruptio placenta) and history of previous scar were documented. Intraoperative data, such as indication of CD, emergency or elective CD and duration of operation, were recorded from the operation notes. The women were followed until discharge from the hospital. Operation time was calculated from skin incision to closure in minutes. Blood group and the number of transfused units were obtained from the medical records of the participants.
Definitions and Measurements
The BMI was measured at time of delivery and recorded from preoperative notes. The BMI was categorized to <25 (reference) and >25.20
The term other indications of CD includes macrosomia, multiple gestations, malpresentations, post-term pregnancy with failed induction of labors and others.
Haemoglobin was estimated by an automated haematology analyser according to the manufacturer’s instructions (Sysmex KX-21, Japan).
Anaemia was defined as haemoglobin <11.0 g/dL. Indications for blood transfusion were haemoglobin <8.0 g/dL with symptoms and signs suggestive of severe anaemia (such as palpitations, dizziness, shortness of breathing, severe pallor, tachycardia and hypotension)21 or active bleeding (more than 1000 mL). Women with haemoglobin level of <7.0 g/dL were transfused regardless of symptoms. Post-CD blood loss was estimated by visual inspection of active vaginal bleeding associated with hemodynamic instability of the pulse and blood pressure and weighting of the perineal pads. Moreover, digital weighing scale was used, with one gram is equal to one mL of blood volume.22
The patient was considered transfused in our study protocol if she received at least one unit of packed red cell or more after CD. All women in the study received only packed red cell.
Statistics
Data were entered into a computer, and SPSS for Windows was used for data analysis. Continuous data were checked for normality using the Shapiro–Wilk test and were found to be not normally distributed. The median (interquartile range), frequency and percentages were used to present the characteristics of the participants. Univariate analyses were performed with blood transfusion (yes, no) as the dependent factor and sociodemographic data (age, education, occupation, residence, parity, blood group, BMI) and obstetric and medical conditions (diabetes, hypertension, placenta previa and abruption, history of previous scar, gestational age, emergency or elective surgery, duration of operation and haemoglobin) as independent variables. Variables in univariate analysis were compared with Mann‒Whitney test, chi-squared test and Fisher exact test where applicable.
Variables with their P <0.2 were shifted to construct the multivariate analysis with backward likelihood ratio methods. The unadjusted and adjusted odds ratios and 95% confidence interval (CI) were computed to show the strength of the association. A two-sided p-value of <0.05 was considered statistically significant.
Results
Participant’s Characteristics
A total of 539 women who underwent CD during the study period were recruited. Of these, 387 (71.8%) underwent elective CD and 306 (56.8%) were due to repeated scar. The medians (IQR) of age and parity were 28.0 (8.0) years and 3.0 (2.0), respectively. In total, 298 (55.3%) women resided in rural areas. Overall, 504 (93.5%) were housewives and 389 (72.2%) had a level of education lower than secondary. The median (IQR) of BMI, gestational age and duration of operation was 25.3 (4.3) kg/m2, 38.0 (1.0) weeks and 45.0 (15.0) minutes, respectively. The patients who had medical diseases and antepartum haemorrhage were 56 (10.4%) and 15 (2.8%), respectively. The median (IQR) preoperative and postoperative haemoglobin levels were 11.2 (1.7) g/dl and 10.3 (1.6) g/dl, respectively (Table 1).
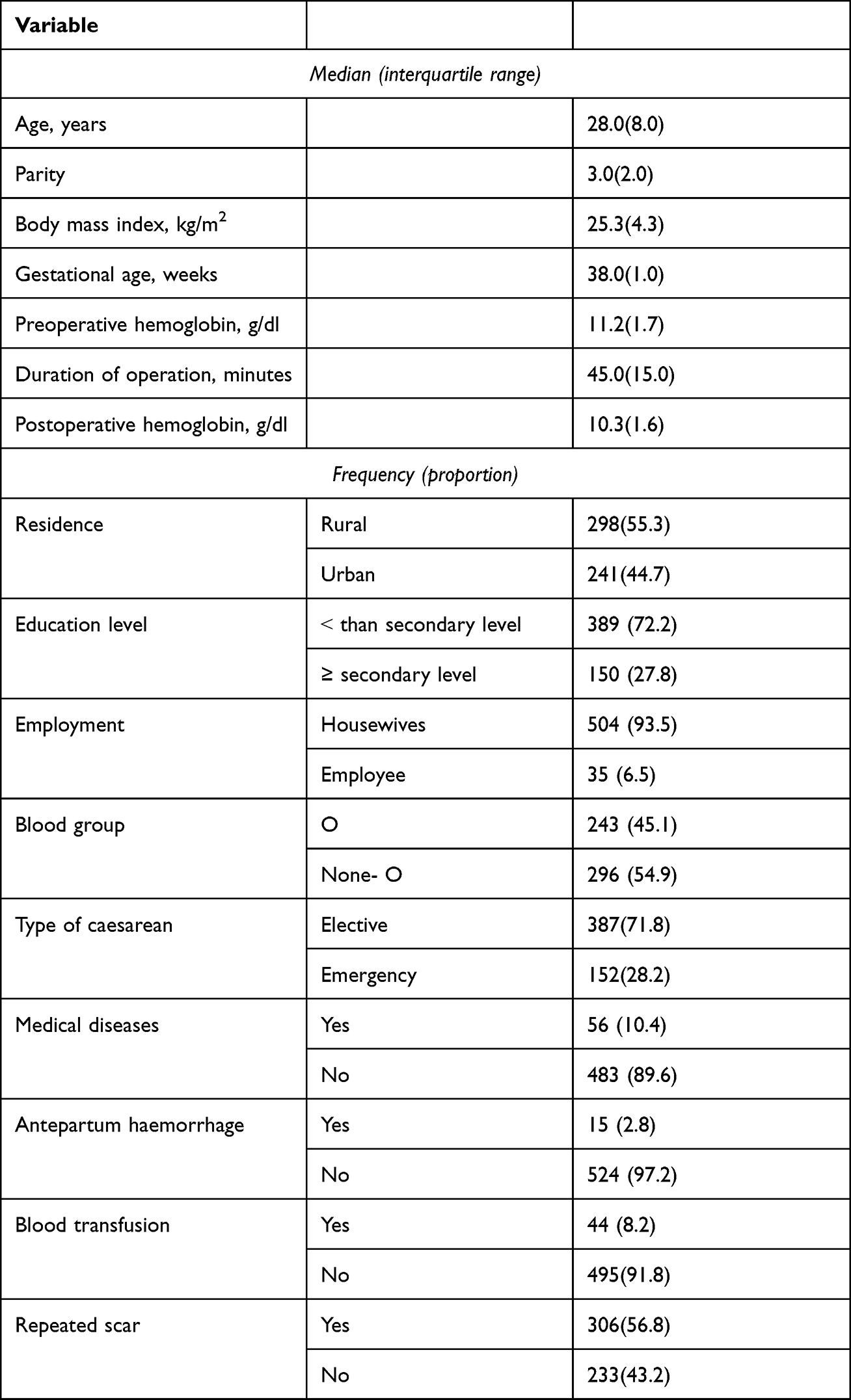 |
Table 1 Sociodemographic and Clinical Characteristics of the Women (Number =539) with Cesarean Delivery in Eastern Sudan, 2020 |
Caesarean Delivery Indications
The main indication for CD among the study population was repeated scar at 306 (56.8%), followed by other/combined at 120 (22.3%), cephalopelvic disproportion at 43 (8.0%), foetal distress at 28 (5.2%), pre-eclampsia/eclampsia at 19 (3.5%), second stage CD at 18 (3.3%) and placental abnormality at 5 (0.9%) (Table 2).
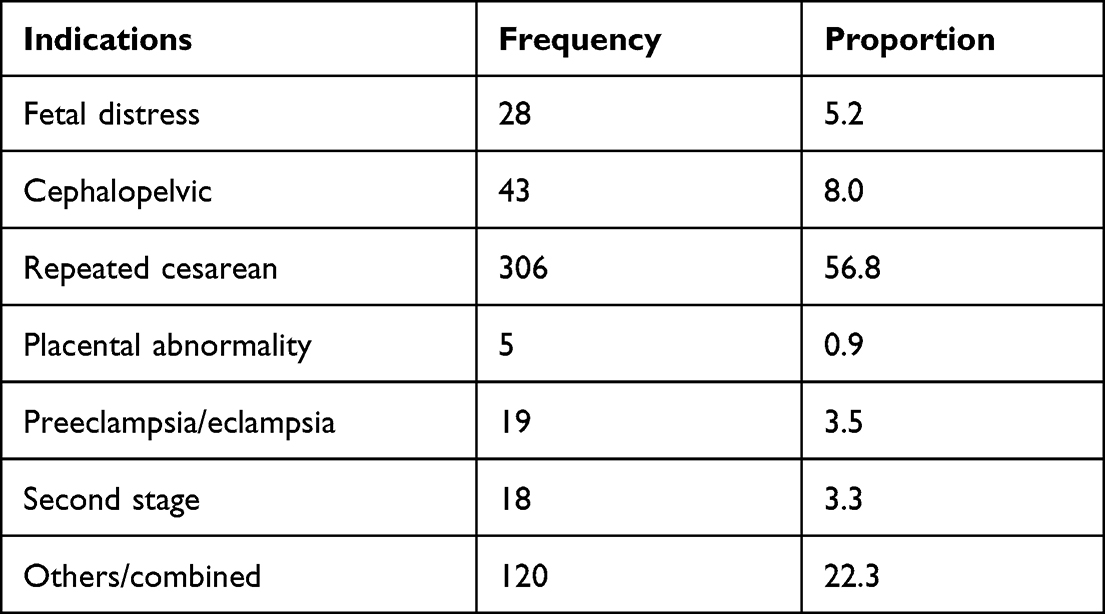 |
Table 2 Indications for Cesarean Delivery in Eastern Sudan, 2020 |
Prevalence of Post-CD Blood Transfusion
Of the 539 enrolled women, 44 (8.2%) were transfused (Table 1).
Univariate Analysis of the Study
The univariate analysis showed that women who received post-CD transfusion were older, had longer operation times, had emergency CD, reported antepartum haemorrhage as an indication of their CD and were from rural areas. The preoperative haemoglobin was significantly lower among the transfused group of women. There was no significant difference in the education, occupation, parity, blood group and BMI in the women who underwent post-CD transfusion and those who had no blood transfusion (Table 3).
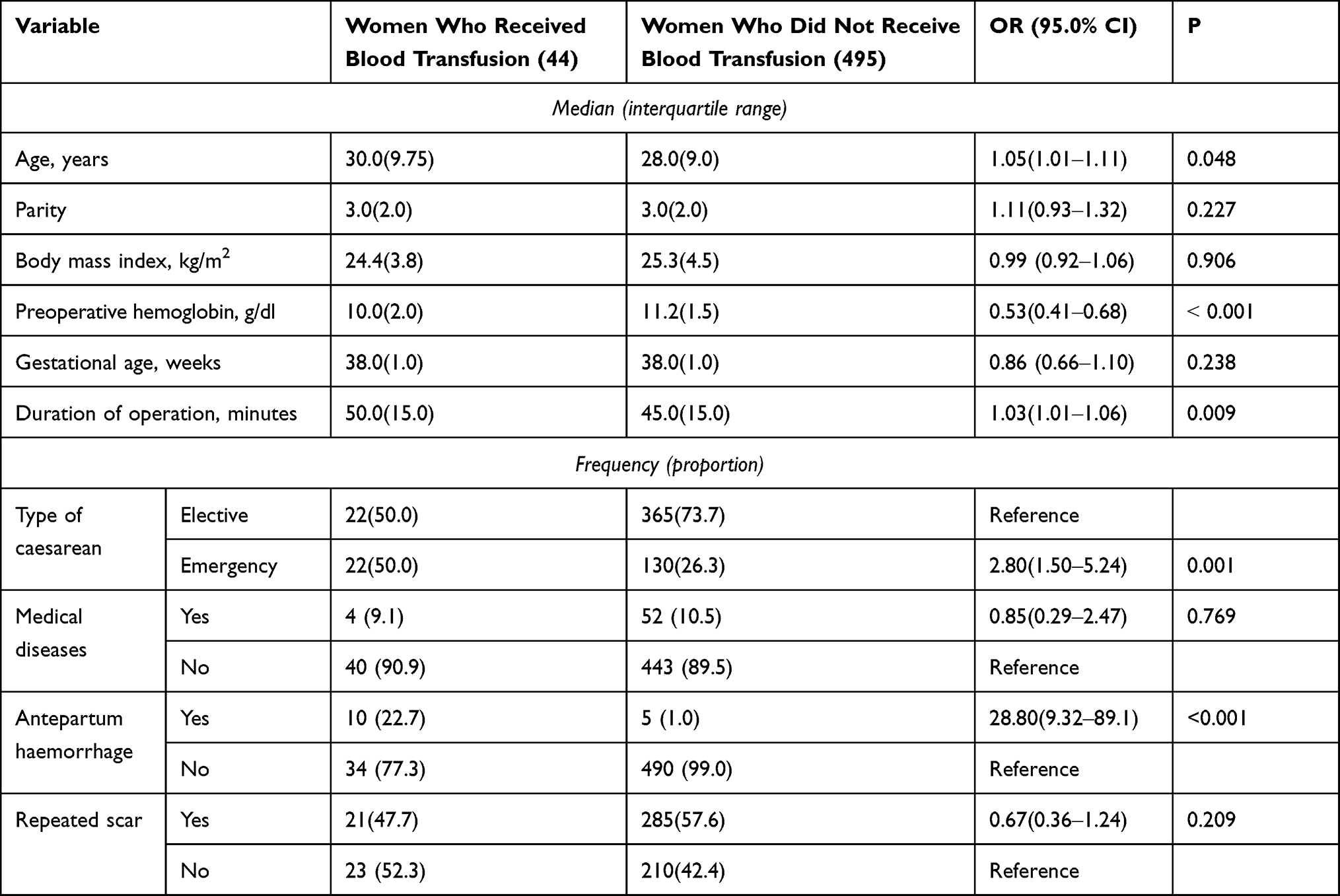 |
Table 3 Univariate Analysis of the Factors Associated with Blood Transfusion in Women with Cesarean Delivery in Eastern Sudan, 2020 |
Multivariate Logistic Analysis
A multivariable logistic regression analysis revealed a significant association between emergency CD (AOR=2.57, 95% CI=1.25‒5.28) and antepartum haemorrhage (AOR=44.70, 95% CI=11.18‒178.76) with post-CD transfusion. Preoperative haemoglobin (AOR=0.48, 95% CI=0.36‒0.64) and rural residence (AOR=0.45, 95% CI=0.22‒0.93) were associated with a lower risk of postpartum blood transfusion. After adjustment, there was no significant association between maternal age and operation time with post-CD transfusion (Table 4).
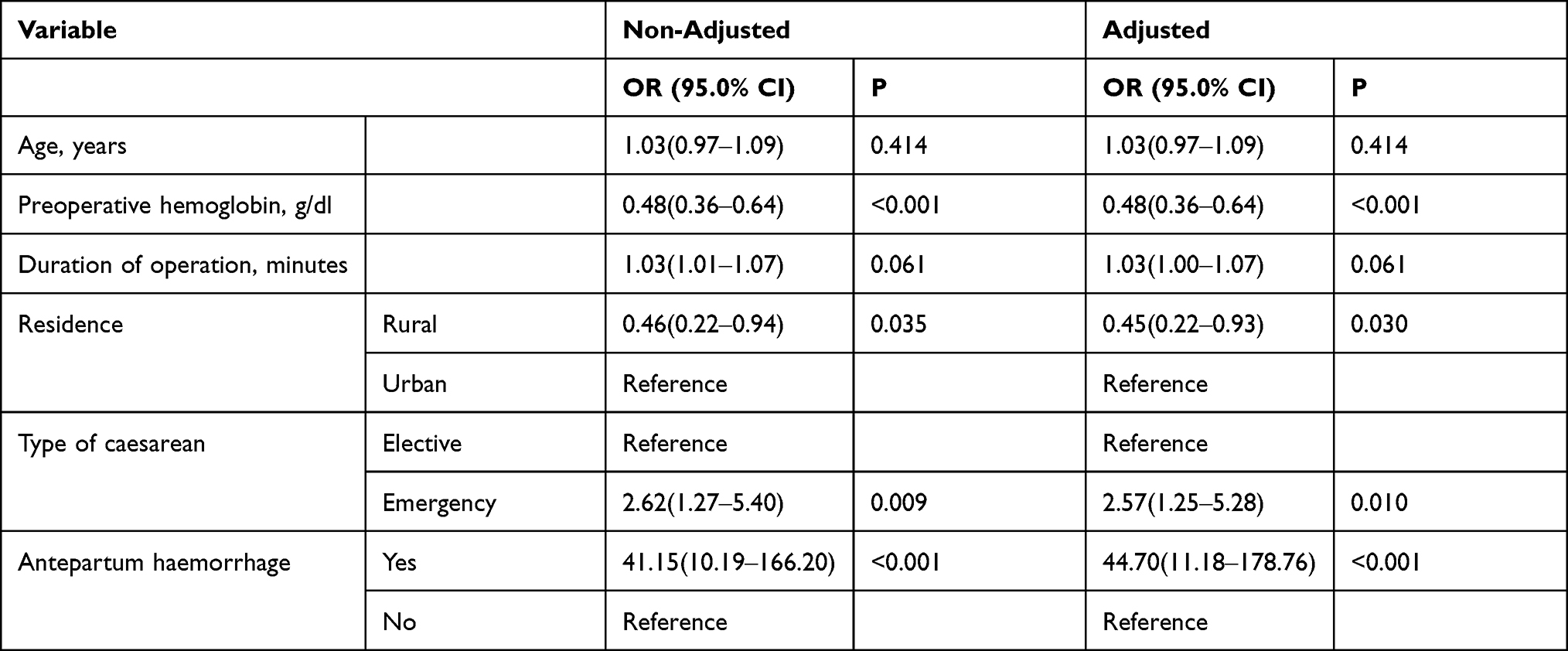 |
Table 4 Multivariate Analysis of the Adjusted and Non- Adjusted Factors Associated with Blood Transfusion in Women with Cesarean Delivery in Eastern Sudan, 2020 |
Discussion
This cross-sectional study was conducted at a tertiary maternity hospital in Gadarif, Eastern Sudan, to determine the prevalence of post-CD blood transfusion and its associated factors. To our knowledge, this is the first study addressing the prevalence and risk factors for transfusion among Sudanese women who underwent CD.
In this study, the prevalence of post-CD transfusion was 8.2%. This is comparable with previous studies published in southwestern Nigeria (8.68%)23 and Dhaka, Bangladesh (8.9%).24 This rate of post-CD transfusion (8.2%) in our study is lower than the rate in Lagos, Nigeria (20.8%).5 Our result for blood transfusion rate (8.2%) was higher than those reported from developed countries, eg in Australia (0.36%)8 and in New York, USA (3.5%).25
We have previously reported that 13.6% of the admitted children in the same settings (Gadarif, eastern Sudan) had blood transfusions.26 A possible explanation for this variation is the presence of different types of hereditary anaemia during childhood. Sickle cell anaemia, for example, is a common indication for recurrent transfusion in paediatrics.
In the present study, emergency CD (AOR=2.57, 95% CI=1.25‒5.28) was significantly associated with the requirement for blood transfusion. This finding is consistent with published data from South Western Nigeria27 and Pakistan.28 However, other studies did not show this association.8,29 Emergency CD carries the risk of intraoperative complications and haemorrhage with an increased need for blood transfusion.
The results from this study revealed that antepartum haemorrhage was associated with increased risk (AOR=44.70) for post-CD blood transfusion. Several other studies are in accordance with our results.6,30–32 This is probably due to the recurrent antepartum haemorrhage of placenta previa that can lead to preoperative anaemia. The interplay between antepartum haemorrhage and antenatal anaemia increased the risk for transfusion in our study. Furthermore, invasive placenta previa and disseminated intravascular coagulopathy of abruption have been associated with massive blood loss.13,30
The findings of this study indicate that each increase in preoperative haemoglobin decreased the risk of blood transfusion by 52.0% (AOR=0.48). Preoperative anaemia as a risk factor for transfusion has been reported in many studies.5,12,29,30 Women who had preoperative anaemia were less tolerant of any amount of blood loss during surgery. A recent meta-analysis showed that the pooled prevalence of anaemia among pregnant women in Sudan was 53%.33 In our study, antepartum haemorrhage was suggested as another factor for preoperative anaemia. This risk factor is modifiable; healthcare practitioners can correct antenatal anaemia preoperatively to reduce the risk of post-CD transfusion.
In the current study, rural residence reduced the risk for post-CD transfusion by 55.0% (AOR=0.45). Consistent with this observation, a study from Finland reported a higher rate of postpartum transfusion among those residing in urban areas.34 A possible explanation is that the majority of those residing in rural areas were referred for elective CD at our tertiary hospital. Women who resided in rural areas underwent emergency CD at peripheral hospitals near their residence. This meant that most of the women from rural areas who were included in our study were of the elective type. According to this study and other studies,8,35,36 the risk of transfusion among elective surgery patients is less than among emergency CD patients. However, in contrast to our results, rural residence was associated with an increased risk for blood transfusion in previous studies.37,38 The patients in those studies had their emergency surgery in the same study settings unlike this study.
In the univariate analysis, maternal age was higher among transfused patients than among non-transfused patients. After adjustment of this confounder, no association was detected. Results recorded from previous published studies reported advanced maternal age as a risk factor for post-CD transfusion.5,20,35 Advanced maternal age is associated with postpartum haemorrhage due to weak uterine contractions.39 Furthermore, advanced maternal age is a risk factor for placenta previa and abruption.31
The current study indicates that operation time was longer among transfused patients than non-transfused patients in the univariate analysis. This finding disappears after adjustment to other confounders. Studies from Nigeria5 and Pakistan6 observed longer operation times among transfused women who underwent CD. Prolonged operation time is associated with adhesion and intraoperative complications that increase the need for blood transfusion.6,40
Strengths and Limitations
The strength of the study comes from the novelty of being the first study in Sudan that addressed the prevalence and associated factors of post-CD blood transfusion. The study has enough power and adequate sample size. However, women with vaginal delivery and women who received intraoperative blood transfusion were not included in the study. Moreover, the study was conducted in one hospital, unlike multicentric studies which could produce different results.
In conclusion, the prevalence of post-CD blood transfusion among Sudanese women in Gadarif, eastern Sudan, was 8.2%. The need for transfusion was significantly associated with preoperative anaemia, antepartum haemorrhage and emergency CD. Women who resided in rural areas were found to have fewer blood transfusion requirements. Blood preparation for those at risk is of paramount importance, and correction of preoperative anaemia can assist in the reduction of transfusion rate.
Abbreviations
PPH, postpartum haemorrhage; CD, caesarean delivery; BMI, body mass index; CI, confidence interval; IQR, interquartile range; AOR, adjusted odds ratios.
Ethics Approval and Informed Consent
This study complies with the Declaration of Helsinki. Ethics approval was obtained from the Ethics Committee of the Faculty of Medicine of Gadarif University, Sudan (Reference number #2020.07). Written informed consent was collected from each participant.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Sheldon WR, Blum J, Vogel JP, et al. Postpartum haemorrhage management, risks, and maternal outcomes: findings from the World Health Organization Multicountry Survey on Maternal and Newborn Health. BJOG. 2014;121(Suppl 1):5–13. doi:10.1111/1471-0528.12636
2. Stephens B, Sethna F, Crispin P. Postpartum obstetric red cell transfusion practice: a retrospective study in a tertiary obstetric centre. Aust NZ J Obstet Gynaecol. 2018;58(2):170–177. doi:10.1111/ajo.12680
3. Conner SN, Tuuli MG, Colvin R, Shanks AL, Macones GA, Cahill AG. Accuracy of estimated blood loss in predicting need for transfusion after delivery. Am J Perinatol. 2015;32(13):1225–1230. doi:10.1055/s-0035-1552940
4. Kolin DA, Shakur-Still H, Bello A, Chaudhri R, Bates I, Roberts I. Risk factors for blood transfusion in traumatic and postpartum hemorrhage patients: analysis of the CRASH-2 and WOMAN trials. PLoS One. 2020;15(6):e0233274. doi:10.1371/journal.pone.0233274
5. Akinlusi FM, Rabiu KA, Durojaiye IA, Adewunmi AA, Ottun TA, Oshodi YA. Caesarean delivery-related blood transfusion: correlates in a tertiary hospital in Southwest Nigeria. BMC Pregnancy Childbirth. 2018;18(1). doi:10.1186/s12884-017-1643-7
6. Abbas S, Mughal S, Hussain SNF, Hossain N. Blood transfusion and high-order cesarean delivery; Report from a developing country. Pak J Med Sci. 2019;35(6):1520–1525. doi:10.12669/pjms.35.6.539
7. Waniala I, Nakiseka S, Nambi W, et al. Prevalence, indications, and community perceptions of caesarean section delivery in Ngora District, Eastern Uganda: mixed method study. Obstet Gynecol Int. 2020;2020:5036260. doi:10.1155/2020/5036260
8. Chua SC, Joung SJ, Aziz R. Incidence and risk factors predicting blood transfusion in caesarean section: original article. Aust NZ J Obstet Gynaecol. 2009;49(5):490–493. doi:10.1111/j.1479-828X.2009.01042.x
9. Ozumba BC, Ezegwui HU. Blood transfusion and caesarean section in a developing country. J Obstet Gynaecol. 2006;26(8):746–748. doi:10.1080/01443610600955792
10. Hu J, Yu ZP, Wang P, Shi CY, Yang HX. Clinical analysis of postpartum hemorrhage requiring massive transfusions at a tertiary center. Chin Med J. 2017;130(5):581–585. doi:10.4103/0366-6999.200545
11. Thurn L, Wikman A, Westgren M, Lindqvist PG. Massive blood transfusion in relation to delivery: incidence, trends and risk factors: a population-based cohort study. BJOG. 2019;126(13):1577–1586. doi:10.1111/1471-0528.15927
12. Ahmadzia HK, Phillips JM, James AH, Rice MM, Amdur RL. Correction: predicting peripartum blood transfusion in women undergoing cesarean delivery: a risk prediction model. PLoS One. 2019;14(1):e0211360. doi:10.1371/journal.pone.0211360
13. Bao Y, Xu C, Qu X, Quan S, Dong Y, Ying H. Risk factors for transfusion in cesarean section deliveries at a tertiary hospital. Transfusion. 2016;56(8):2062–2068. doi:10.1111/trf.13671
14. Atterbury C, Wilkinson J. Blood transfusion. Nurs Stand. 2000;14(34):47–52. doi:10.7748/ns2000.05.14.34.47.c2837
15. Carson JL, Stanworth SJ, Roubinian N, et al. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2016;2016(10). doi:10.1002/14651858.CD002042.pub4
16. Rayis D. An epidemic of cesarean deliveries at Khartoum hospital in Sudan with over two-fifths of neonates delivered through the abdomen. J Womens Heal Issues Care. 2013;02(06). doi:10.4172/2325-9795.1000126
17. Ali AAA, Khojali A, Okud A, Adam GK, Adam I. Maternal near-miss in a rural hospital in Sudan. BMC Pregnancy Childbirth. 2011;11(1):48. doi:10.1186/1471-2393-11-48
18. Fazari AB, Eldeen NS, Mohammed W, Muror M, Gailii E. Re-laparotomy after caesarean section at Omdurman Maternity Hospital-Khartoum, Sudan. Open J Obstet Gynecol. 2015;05(08):448–454. doi:10.4236/ojog.2015.58065
19. OpenEpi menu. Available from: http://wwww.openepi.com/Menu/OE_Menu.htm.
20. Ahmadzia HK, Phillips JM, James AH, Rice MM, Amdur RL. Predicting peripartum blood transfusion in women undergoing cesarean delivery: a risk prediction model. PLoS One. 2018;13(12):e0208417. doi:10.1371/journal.pone.0208417
21. Juul SE, Derman RJ, Auerbach M. Perinatal iron deficiency: implications for mothers and infants. Neonatology. 2019;115(3):269–274. doi:10.1159/000495978
22. Lagoo J, Wilkinson J, Thacker J, Deshmukh M, Khorgade S, Bang R. Impact of anemia on surgical outcomes: innovative interventions in resource-poor settings. World J Surg. 2012;36(9):2080–2089. doi:10.1007/s00268-012-1615-z
23. Faponle AF, Makinde ON. Caesarean section: intra-operative blood loss and its restitution. East Afr Med J. 2007;84(1):31–34. doi:10.4314/eamj.v84i1.9488
24. Chowdhury F, Akhter S, Islam A, Rayen J, Begum N, Begum F. Evaluation of blood transfusion practices in obstetrics and gynecology in a Tertiary Hospital in Bangladesh. J Bangla Coll Physicians Surg. 2016;34(1):9–14. doi:10.3329/jbcps.v34i1.29116
25. Spiegelman J, Mourad M, Melka S, et al. Risk factors for blood transfusion in patients undergoing high-order cesarean delivery. Transfusion. 2017;57(11):2752–2757. doi:10.1111/trf.14274
26. Bishop D, Dyer RA, Maswime S, et al. Maternal and neonatal outcomes after caesarean delivery in the African Surgical Outcomes Study: a 7-day prospective observational cohort study. Lancet Glob Heal. 2019;7(4):e513–e522. doi:10.1016/S2214-109X(19)30036-1
27. Akinola OI, Fabamwo AO, Tayo AO, Rabiu KA, Oshodi YA, Onyekwere CA. Evaluation of blood reservation and use for caesarean sections in a tertiary maternity unit in south western Nigeria. BMC Pregnancy Childbirth. 2010;10. doi:10.1186/1471-2393-10-57
28. Ismail S, Siddiqui S, Shafiq F, Ishaq M, Khan S. Blood transfusion in patients having caesarean section: a prospective multicentre observational study of practice in three Pakistan hospitals. Int J Obstet Anesth. 2014;23(3):253–259. doi:10.1016/j.ijoa.2014.01.004
29. Sivahikyako SA, Owaraganise A, Tibaijuka L, et al. Prevalence and factors associated with severe anaemia post-caesarean section at a tertiary Hospital in Southwestern Uganda. BMC Pregnancy Childbirth. 2021;21(1):674. doi:10.1186/s12884-021-04157-x
30. Eyelade OR, Adesina OA, Adewole IF, Adebowale SA. Blood transfusion requirement during caesarean delivery: risk factors. Ann Ibadan Postgrad Med. 2015;13(1):29–35.
31. Kang J, Kim HS, Lee EB, et al. Prediction model for massive transfusion in placenta previa during cesarean section. Yonsei Med J. 2020;61(2):154–160. doi:10.3349/ymj.2020.61.2.154
32. Xie Y, Liang J, Mu Y, et al. Incidence, trends and risk factors for obstetric massive blood transfusion in China from 2012 to 2019: an observational study. BMJ Open. 2021;11(9):e047983. doi:10.1136/bmjopen-2020-047983
33. Adam I, Ibrahim Y, Elhardello O. Prevalence, types and determinants of anemia among pregnant women in Sudan: a systematic review and meta-analysis. BMC Hematol. 2018;18(1):31. doi:10.1186/s12878-018-0124-1
34. Jakobsson M, Gissler M, Tapper AM. Risk factors for blood transfusion at delivery in Finland. Acta Obstet Gynecol Scand. 2013;92(4):414–420. doi:10.1111/j.1600-0412.2012.01490.x
35. Rottenstreich A, Regev N, Levin G, et al. Factors associated with postcesarean blood transfusion: a case control study. J Matern Neonatal Med. 2020. doi:10.1080/14767058.2020.1724945
36. Kols T, Øian P, Skjeldestad FE. Risks for peroperative excessive blood loss in cesarean delivery. Acta Obstet Gynecol Scand. 2010;89(5):658–663. doi:10.3109/00016341003605727
37. Hartenbach EM, Kuo HHD, Greene MZ, Shrider EA, Antony KM, Ehrenthal DB. Peripartum blood transfusion among rural women in the United States. Obstet Gynecol. 2020;135(3):685–695. doi:10.1097/AOG.0000000000003718
38. Hartenbach E, Hsiang-Hui DK, Greene M, Shrider E, Antony KM, Ehrenthal D. More blood transfusions for rural women delivering low risk infants in the United States [37N]. Obstet Gynecol. 2019;133(1):160S–160S. doi:10.1097/01.AOG.0000559343.12931.9b
39. Pubu ZM, Bianba ZM, Yang G, et al. Factors affecting the risk of postpartum hemorrhage in pregnant women in Tibet health facilities. Med Sci Monit. 2021;27. doi:10.12659/MSM.928568
40. Rottenstreich M, Sela HY, Shen O, Michaelson-Cohen R, Samueloff A, Reichman O. Prolonged operative time of repeat cesarean is a risk marker for post-operative maternal complications. BMC Pregnancy Childbirth. 2018;18(1). doi:10.1186/s12884-018-2111-8
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.