")
Back to Journals » Clinical Ophthalmology » Volume 16
Prevalence and 11-Year Incidence of Cataract and Cataract Surgery and the Effects of Socio-Demographic and Lifestyle Factors
Authors Purola PKM , Nättinen JE, Ojamo MUI, Rissanen HA, Gissler M, Koskinen SVP, Uusitalo HMT
Received 21 December 2021
Accepted for publication 24 March 2022
Published 20 April 2022 Volume 2022:16 Pages 1183—1195
DOI https://doi.org/10.2147/OPTH.S355191
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Petri KM Purola,1,2 Janika E Nättinen,1 Matti UI Ojamo,2 Harri A Rissanen,3 Mika Gissler,4– 6 Seppo VP Koskinen,3 Hannu MT Uusitalo1,2,7
1Department of Ophthalmology, Faculty of Medicine and Health Technology, Tampere University, Tampere, Finland; 2Finnish Register of Visual Impairment, Finnish Federation of the Visually Impaired, Helsinki, Finland; 3Information Services Department of Public Health and Welfare, Finnish Institute for Health and Welfare, Helsinki, Finland; 4Department of Knowledge Brokers, Finnish Institute for Health and Welfare, Helsinki, Finland; 5Region Stockholm, Academic Primary Health Care Centre, Stockholm, Sweden; 6Karolinska Institute, Department of Molecular Medicine and Surgery, Stockholm, Sweden; 7Tays Eye Center, Tampere University Hospital, Tampere, Finland
Correspondence: Petri KM Purola, Department of Ophthalmology, Faculty of Medicine and Health Technology, Tampere University, Tampere, Finland, Tel/Fax +358 400 695309, Email [email protected]
Purpose: To assess the impact of cataract in ageing population by evaluating the prevalence, incidence, and background factors of cataract and cataract surgery.
Patients and Methods: Two health examination surveys representing Finnish population in 2000 and 2011 included 7380 and 5930 participants aged 30 years or older with cataract status known. An 11-year follow-up included 4840 persons who participated in both the surveys. The data include information on physician-made diagnoses, socio-demographic factors, and lifestyle factors based on self-reported assessment. Cataract diagnoses and surgeries recorded in the Finnish Care Register for Health Care were linked to the survey data. Cataract patients were compared to those without cataract using logistic regression. Differences in cataract surgery age were evaluated using linear regression. Univariable and multivariable models were included.
Results: During 2000– 2011, the prevalence of cataract increased from 8.8% to 13.6% and cataract surgery from 5.7% to 8.9% in a representative sample of the Finnish adult population. Cataract and cataract surgery were associated with age, smoking, and high alcohol consumption. Cataract was also associated with female gender and low income in 2000, but this association declined during the 11 years. Smoking and high alcohol consumption were associated with younger surgery age.
Conclusion: The prevalence of cataract and cataract surgery is increasing with the ageing of the population. The increase in cataract surgery is likely also reflecting the improvements in eye care. The possibility to equally use health-care services throughout a country can reduce the impact of socio-demographic status. Healthy lifestyle delays the development of cataract, whereas smoking and high alcohol consumption are associated with earlier cataract development. Therefore, the availability of cataract services and promotion of healthy lifestyle will be the key to prevent the detrimental effects of cataract on patients and the society in countries where the population is rapidly ageing.
Keywords: operated cataract, operation age, population study, smoking, alcohol consumption, living habits
Plain Language Summary
Cataract and related visual impairment are associated with various detrimental effects, such as decreased quality of life and increased risk of accidents. As ageing is the major risk factor for cataract, there is a need to evaluate the impact of the disease on ageing populations. To improve cataract care, more information is needed on the distribution of the disease and its treatment, as well as the effects of different background factors on the development of cataract and need for cataract surgery. Therefore, we investigated the prevalence and incidence of cataract and cataract surgery and their regional distribution in Finland, as well as the association of socio-demographic and lifestyle factors with cataract, cataract surgery, and cataract surgery age.
This study showed that the prevalence of cataract and cataract surgery is increasing with the ageing of population. However, the possibility to equally use health-care services throughout a country can reduce the impact of socio-demographic status. Persons with healthy lifestyle live longer and show delay in the development of cataract. On the other hand, those who smoke or consume high amounts of alcohol have a shorter life expectancy, yet they acquire cataract and are operated at a younger age, therefore increasing the demand for cataract care. By promoting easy and equal availability of cataract care, as well as healthy living habits, the detrimental effects of cataract and related visual impairment can be prevented.
Introduction
Cataract is the leading cause of visual impairment worldwide, with an estimation of over 13 million persons suffering from blindness due to the disease.1,2 In Western countries, population ageing and unfavorable changes in lifestyle are likely to increase the prevalence of cataract and related vision loss in the future.3–5 In Finnish population, Hirvelä et al reported that among people aged 70 years or over, the prevalence of cataract was 30% and the prevalence of vision loss caused at least partly by the disease was 18%.6
Cataract is classified into nuclear, cortical, and posterior subcapsular types based on its clinical appearance, all of which lead to opacification of the lens and subsequent decrease in vision.7 Even though permanent deterioration of visual acuity can usually be prevented by a surgical removal of cataract and replacement by an artificial intraocular lens, inadequate access to surgical services and high surgery expenses are a common barrier to cataract treatment, particularly in developed countries.8 Therefore, continuous efforts are needed to alleviate the social and economic burden of declined visual acuity and the subsequent decline in quality of life.1,9
Ageing is the major determinant of cataract,2,10 but many population-based studies have also linked various genetic and environmental risk factors to cataract development, including smoking,11 light exposure,12 alcohol consumption,13 diabetes,14,15 and high blood pressure.15 The use of drugs such as corticosteroids is also a well-established risk factor for cataract.16 Despite the current level of knowledge, more information is needed on the distribution and background factors of cataract and its treatment in order to improve the health services and promotion of healthy living habits in countries with ageing populations such as Finland.
In this study, our aim was to evaluate the prevalence and incidence of cataract and cataract-related surgery, as well as the effects of socio-demographic and lifestyle factors on cataract and its treatment in the Finnish adult population. We used data from two nationwide cross-sectional surveys conducted in 2000 and 2011, complemented with health register data. To our knowledge, this is the first report describing the effect of socio-demographic and lifestyle factors on the age when cataract surgeries are performed.
Materials and Methods
Study Population and Design
This study was based on two cross-sectional nationwide health examination surveys, Health 2000 and Health 2011, conducted by the Finnish Institute for Health and Welfare.17,18 The first survey was carried out in Finland in 2000–2001, and the second in 2011–2012. Both the surveys included an identical, comprehensive, self-reported assessment that included questions on, eg, physician-made diagnoses and treatments, socio-demographic factors, and lifestyle factors. Both the surveys also included a health examination conducted at a nearby screening center that included measurements on, eg, height and weight. If the invited participants did not attend the examination, an abridged examination was conducted at home or in an institution.
The Health 2000 Survey included a sample of 9922 adults aged 18 years or older living in Finland. The sample was drawn by a two-stage stratified cluster sampling, and persons aged 80 or older were oversampled by doubling the sampling fraction. The Health 2011 Survey included all living members of the Health 2000 Survey sample, who had not refused further contacts. For this study, we only included participants aged 30 years or older representing the Finnish adult population at both the time points. In both the surveys, the sample weights were calibrated by post-stratification, defined by age, sex, region, and native language to account for non-response and missing data. The unweighted participation rates were 93% in the Health 2000 Survey and 73% in the follow-up. Separate weights were applied for the surveys to produce results representing the Finnish population at different time points. More details on the study design and sampling have been reported previously.19–21
Information on the region of residence was available for all survey participants and classified according to the five university hospital districts that represent Southern, Western, Central, Eastern, and Northern Finland, respectively. The age at death of all participants who died between 2000 and 2011 (n = 1279) was obtained from the Digital and Population Data Services Agency.
Cataract Status
Both self-reported and register-based data on cataract and its treatment were collected. Self-reported information was asked at both the time points with an interview question “Has a doctor ever diagnosed you with the following diseases”, followed by a list including cataract, glaucoma, degenerative fundus changes, and other visual defect or eye trauma. Participants who reported having a cataract diagnosis were further asked “Have you had an eye operation because of it?”. The register data were obtained from the Finnish Care Register for Health Care, including inpatient care between 1968 and 2011, outpatient visits between 1998 and 2011, and operations between 1985 and 2011. This register includes cataract patients who had been operated in public health sector which covers more than 90% of all cataract operations in Finland. The indications for cataract surgery under the Finnish public healthcare system are: 1) best-corrected visual acuity in the better eye of ≤0.5 (20/40); 2) best-corrected visual acuity in the worse eye of ≤0.32 (20/60); or 3) cataract-dependent difficulties in everyday life.22
In this study, cataract patients included persons who had self-reported cataract and/or cataract surgery, and those who according to the register data had a cataract-related diagnosis (International Classification of Diseases codes version 8: 37401–37409, 37871–37872; version 9: 3660–3669, 3793; or version 10: H25–H28, Z96.1) and/or had undergone cataract-related surgery (Operation procedure codes of Finnish Hospital League: 3623–3628, 3631, 3633; NOMESCO Classification for Surgical Procedures: CJC, CJD, CJE; or presence of intraocular lens [International Classification of Diseases codes version 9/10: 3793C/Z96.1]).23–25 Participants who had self-reported or register-based cataract surgery were considered operated. The age at the time of the first cataract-related surgery was obtained for all operated cataract patients included in the register data.
Socio-Demographic and Lifestyle Factors
Both the surveys included self-reported interview questions on four socio-demographic factors: marital status, education, income, and occupation. In addition, three lifestyle factors were included: self-reported smoking and alcohol consumption, as well as measured body mass index.
Marital status was categorized as those living in a relationship (married, in a civil union, or living with partner) and those not living in a relationship (single, divorced or separated, or widowed).
To assess the level of education, the participants were asked if they had received any further education in addition to basic education, and based on the answers, they were assigned to the following three categories: higher education (a degree of higher vocational qualification, a lower university qualification, a higher university qualification, licentiate examination, or doctor’s degree); vocational education (training or technical certificate for courses completed, vocational school certificate, apprenticeship contract, vocational school [eg, technical school], a technical college qualification, or special vocational qualification [eg, a mastership examination]); only basic education.
Income was evaluated with the following question: “How would you describe the current balance between income and expenditure in your household?”. Based on the answer, the following income categories were constructed: insufficient income (“We have to compromise considerably in our consumption but we can manage with our income” or “We have to make major compromises in our consumption and despite of that we do not manage with our own income”); limited income (“We have to some extent to compromise when deciding what we do with the money”); sufficient income (“We have more than enough money to cover our needs” or “There is enough money to cover our needs”).
Occupation was classified into three categories: employee; farmer (farmer or working on a family member’s farm without salary); other entrepreneur or freelancer (other entrepreneur, self-employed professional or freelancer, or working in a family member’s enterprise without salary).
Self-reported smoking (cigarettes, cigars, or pipe tobacco) was classified into three categories: daily or occasional smokers, former smokers (last smoked at least one month ago), and never smokers.
Body mass index was calculated based on measurements of height and weight in the health examinations, and it was classified as normal (18.5–24.9 kg/m2), underweight (<18.5 kg/m2), or overweight/obese (≥25.0 kg/m2) according to the World Health Organization classification.26
Self-reported alcohol consumption was measured with a beverage-specific quantity-frequency method. Beverage-specific quantities were first transformed into standard Finnish drinks (12 g of pure alcohol) and then multiplied by the frequency of the given beverage.16,17 We classified alcohol consumption into high alcohol consumption (≥25 g/day), low consumption (1–25 g/day), and no consumption (0 g/day), as the limit of 25 g/day has been associated with an increasing risk to various diseases.27
A healthy lifestyle is relative and may vary greatly among cultures. In this study, we have defined persons with healthy lifestyle as those who have normal body mass index, are never smokers, and have low or no consumption of alcohol.
Statistical Analyses
All analyses were performed using R software (v. 3.5.1, R Core Team, R Foundation for Statistical Computing, Austria). The sampling design in the surveys was accounted for using Survey package 3.37 for R28 and weighting scheme calculated by the Finnish Institute for Health and Welfare. Persons with missing data in relevant variables were excluded. The total number of cataract patients and operated cataract patients were estimated using function svytotal in the Survey package. Prevalence rates were estimated as the percentage of all participants with known cataract status at each time point using function svyratio in the Survey package. Using same function, incidence rates were estimated as the percentage of all participants without cataract or cataract surgery at the baseline. The distribution of participants according to the socio-demographic and lifestyle variables were estimated using function svytable in the Survey package. Chi-squared test was used for categorical variables. The Kaplan–Meier estimator (function svykm in the Survey package) was used to produce the survival curve of all participants. Because age was not normally distributed, Mann–Whitney U-test was used for the between-group comparisons. The potential association between different socio-demographic and lifestyle factors with cataract was assessed using age-adjusted Odds Ratios (ORs) with 95% confidence intervals (CIs) calculated using univariable logistic regression analysis. Univariable linear regression was used to estimate the differences between subgroups’ ages at the time of the first cataract surgery. For all regression analyses, socio-demographic and lifestyle factors were dichotomized by using manual stepwise method. Cataract patients were compared to persons with no cataract, and operated cataract patients to persons with no cataract and unoperated cataract patients. For controlling confounding factors, multivariable linear and logistic regression models were also created. The models were evaluated with adjusted R2 and Nagelkerke’s pseudo-R2, respectively. The collinearity of the predictors was assessed using generalized variance inflation factor. All predictors resulted in values below 2, therefore showing no indication of collinearity. The interactions between predictors were assessed, but they did not improve the final models, and therefore were excluded. For all analyses, a two-tailed P<0.05 was used as the cut-off point for statistical significance.
Ethics Approval and Informed Consent
All procedures in the Health 2000 and 2011 studies involving human participants were performed in accordance with the ethical standards of the institutional and/or national research committee, and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Health 2000 study was approved by the Ethical Committee for Research in Epidemiology and Public Health at the Hospital District of Helsinki and Uusimaa and the follow-up by the Coordinating Ethics Committee at the Hospital District of Helsinki and Uusimaa. The ethical approval process details are discussed in previous publications.19,20 All the participants received an information letter regarding the study beforehand. Two informed consents were obtained at the beginning of the Health 2000 study from everyone: one for the health interview and the other for the health examinations.19 The participants were provided with appropriate information concerning the study and asked to sign an informed consent again before the follow-up examination in 2011.20
Data Availability
Full study protocol, contact details, publications, and the process for collaborating and data requests can be found on the website (thl.fi/health2000).
Results
Cataract and Cataract Surgery in Finland
The sample size was 8028 in the 2000 survey, 8006 in the 2011 survey, and 6360 were invited to take part in both the surveys. Of these sample members, 7380 and 5930 had known cataract status in 2000 and 2011, respectively, and 4840 at both the time points. Summary of the study population is shown in Figure 1 and more detailed information in Supplemental Table 1. In 2000, according to the Finnish Care Register for Health Care, 466 survey participants had a cataract diagnosis and of these, 422 (91%) had been operated. In 2011, the respective numbers were 663 and 629 (95%). When self-reported and register-based cataract information was combined, a total of 796 cataract patients participated in 2000, of which 521 (65%) had been previously operated. In 2011, 954 cataract patients participated, of which 677 (71%) had been previously operated. In the 11-year follow-up, 691 participants had incident cataract, 507 had incident cataract surgery, 253 had cataract at both the time points, and 165 had operated status at both the time points. Because there were no significant differences in the results when register-based data and self-reported data were compared, we included both self-reported and register-based cataract in a single group.
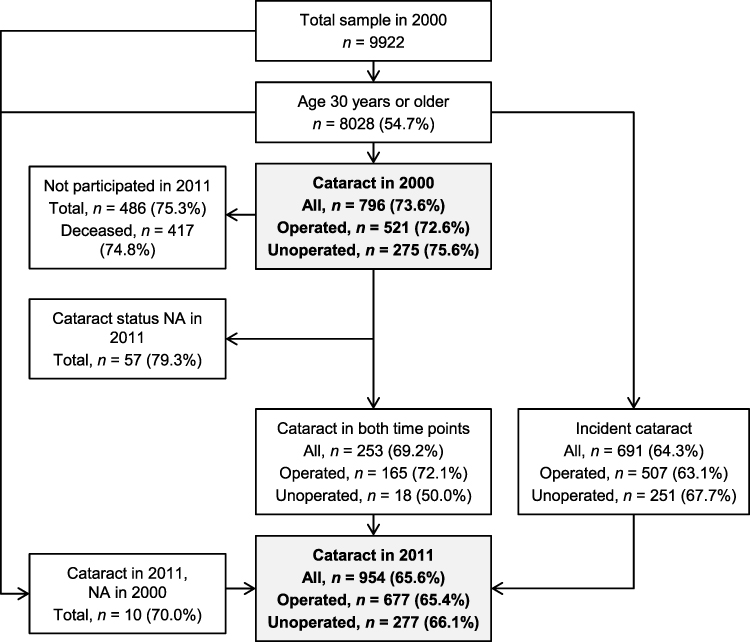 |
Figure 1 Number of study participants and percentage of women in the Health 2000 survey and in the follow-up. Final numbers in the Health 2000 survey and in the follow-up are bolded. Abbreviation: NA, not applicable. |
The prevalence and incidence of cataract patients in Finland by age and sex is shown in Table 1. The age-adjusted prevalence of cataract increased from 8.80% (95% CI 8.10–9.50) to 13.57% (95% CI 12.55–14.59) and cataract surgery from 5.67 (95% CI 5.09–6.25) to 8.92 (95% CI 8.08–9.77) in the Finnish population aged 30 years or older between 2000 and 2011 (P<0.0001). The prevalence and incidence of cataract and cataract surgery increased with age at both the time points and in the follow-up (P<0.0001). Although cataract and operated cataract were more prevalent in women at both the time points and in the follow-up, the sex difference was not statistically significant when adjusted for age.
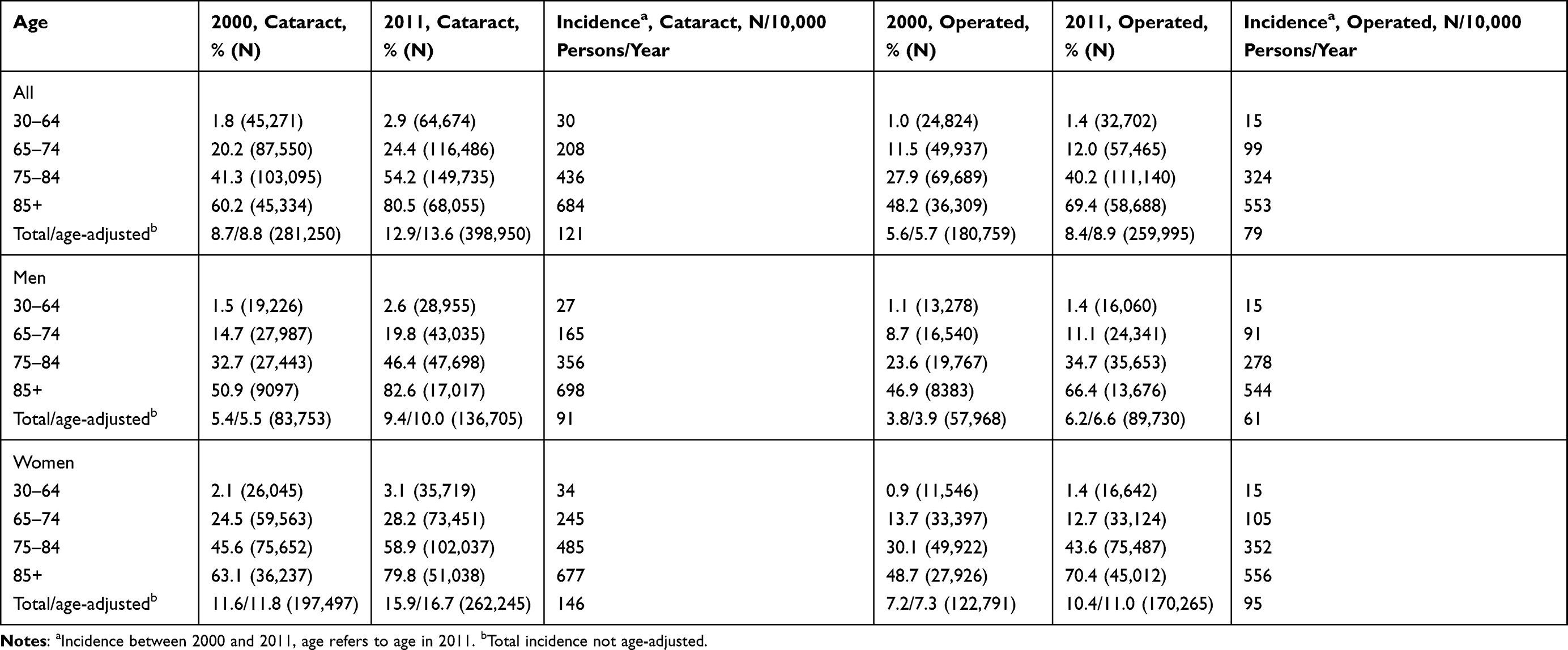 |
Table 1 Estimated Prevalence and Incidence of Cataract and Operated Cataract (and Total Number of Patients) by Age and Sex in Finland |
The percentage of persons with lens-related diagnoses in the Finnish adult population was observed at both the time points, based on the Finnish Care Register for Health Care data (Table 2). Senile cataract was the most common lens-related diagnosis (76% in 2000, 72% in 2011), followed by after-cataract (7% in 2000, 13% in 2011) and presenile cataract (6% in 2000 and 2011). There were no significant sex differences.
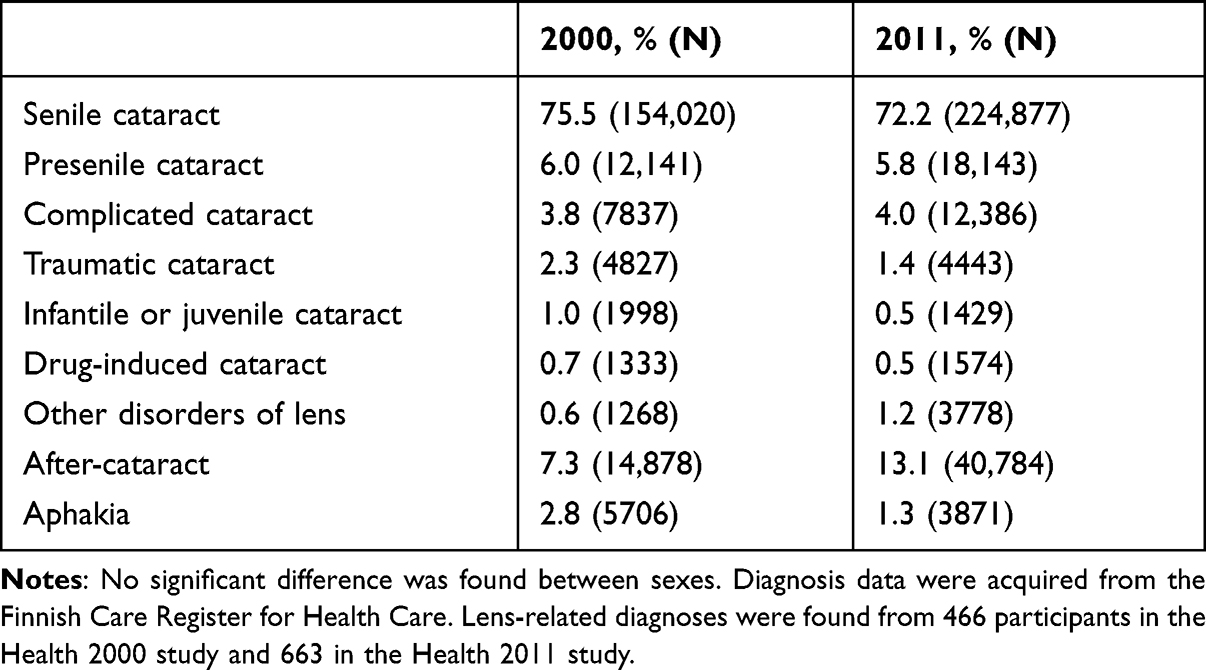 |
Table 2 Percentage and Estimated Number of Patients with Lens-Related Diagnoses in the Finnish Population Aged 30 Years or Older in 2000 and 2011 |
The regional prevalence and incidence of cataract was observed at both the time points (Supplemental Table 2). While the prevalence of cataract and cataract operations was the highest in Eastern Finland, this was statistically significant only in 2011 among women (P=0.048).
Analysis of the Association Between Background Factors and Cataract and Cataract Surgery
Socio-demographic status and lifestyle factors of all cataract patients and operated cataract patients in 2000, 2011, and 11-year follow-up are shown by prevalence and incidence in Table 3, and by age-adjusted and sex-stratified univariable ORs in Tables 4 and 5. More detailed information is shown in Supplemental Figures 1 and 2, including age-stratified prevalence and survival curves. The following results are based on age-adjusted data.
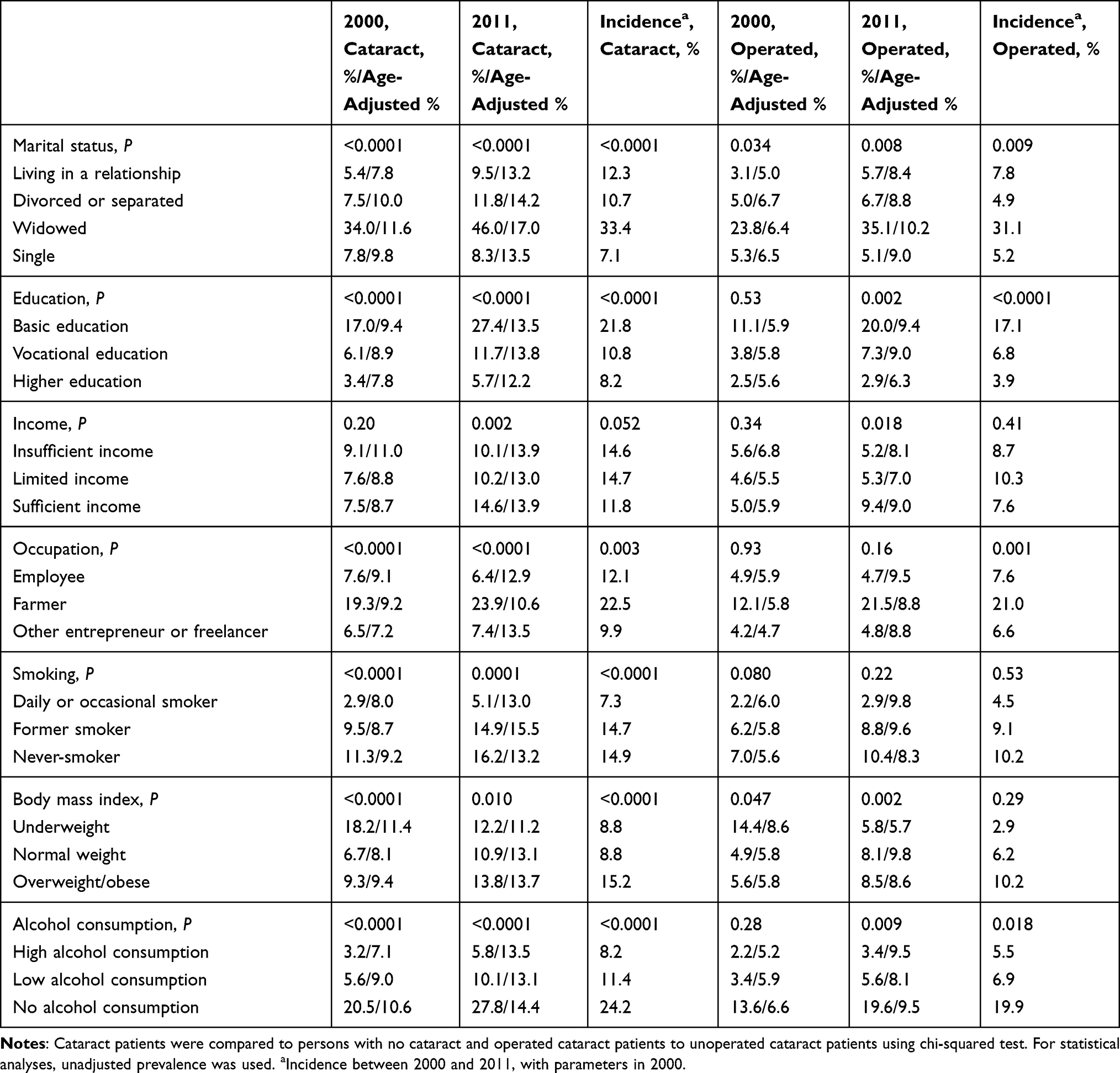 |
Table 3 Prevalence of Cataract and Operated Cataract by Socio-Demographic and Lifestyle Factors |
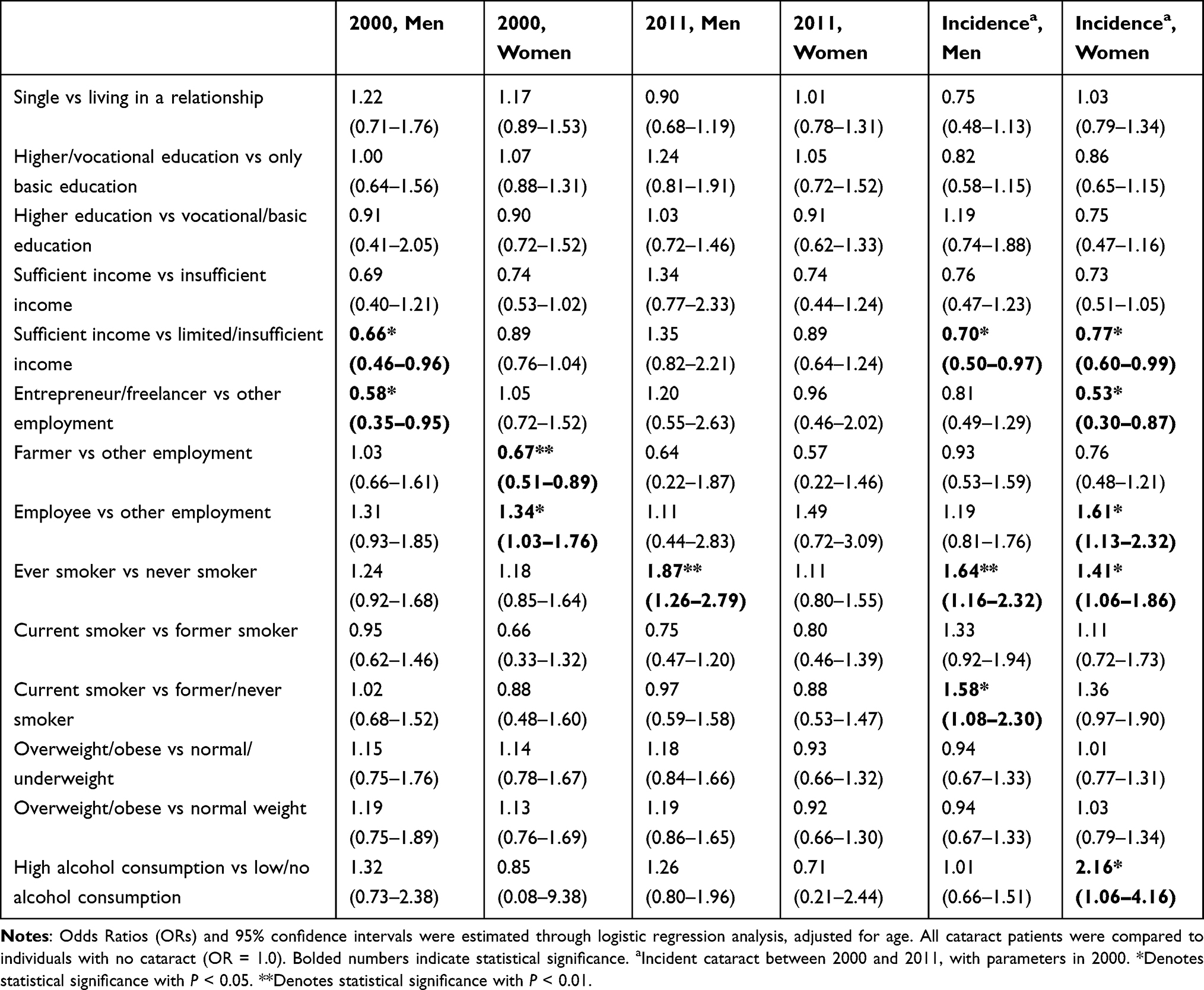 |
Table 4 Age-Adjusted Associations of Socio-Demographic and Lifestyle Factors with Cataract |
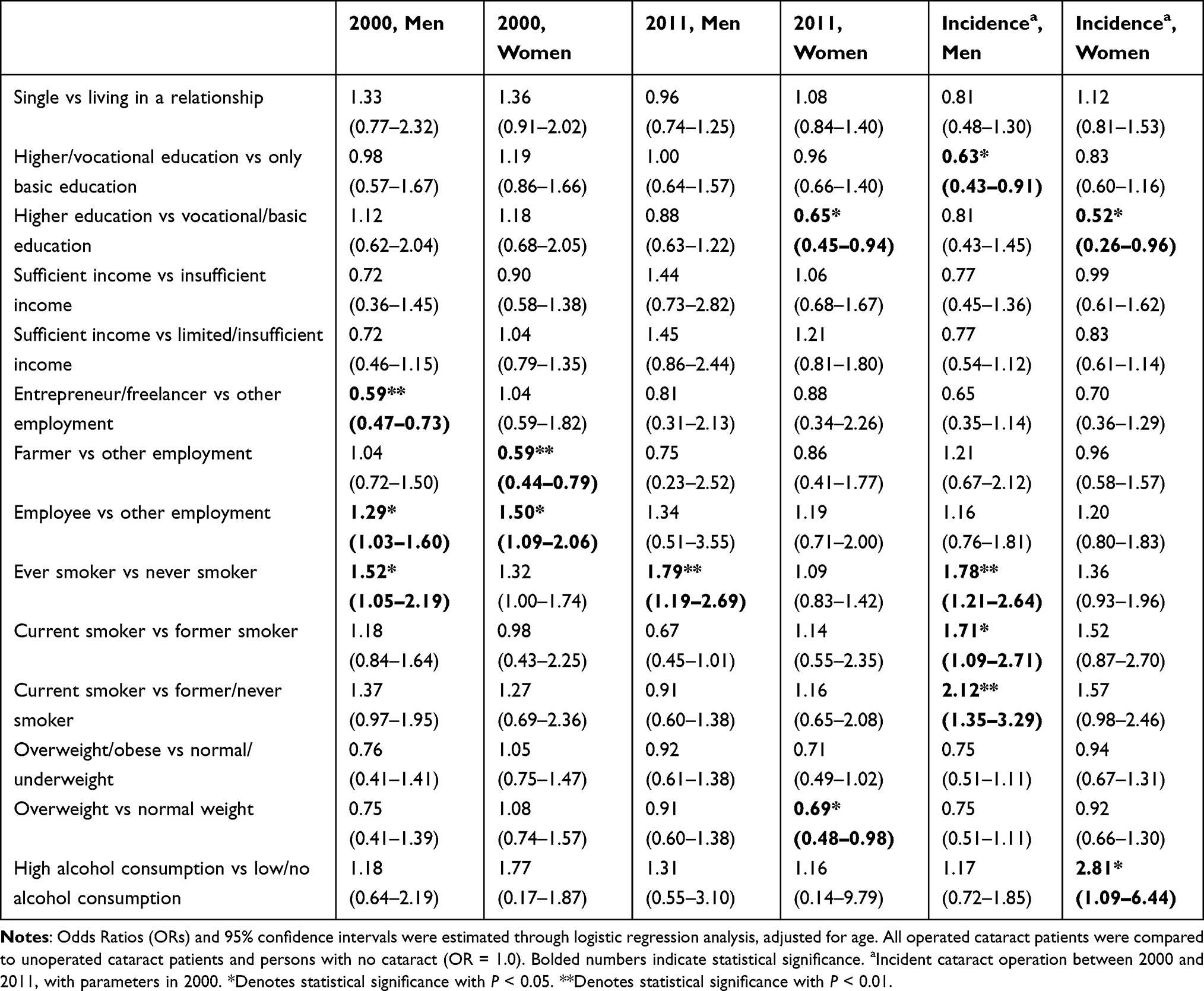 |
Table 5 Age-Adjusted Associations of Socio-Demographic and Lifestyle Factors with Operated Cataract |
Operated female cataract patients had more often received lower education compared to unoperated patients in 2011. Male cataract patients were more likely to have limited or insufficient income compared to those without cataract in 2000. Cataract was most prevalent among female employees when compared to other occupations in 2000. Similarly, operated female and male cataract patients were more often employees than farmers, entrepreneurs, or freelancers compared to unoperated patients in 2000.
Male cataract patients showed significantly higher odds for being a current or former smoker in 2011. Similarly, operated male cataract patients were more likely current or former smokers in 2000 and 2011. Operated female cataract patients had more likely normal weight than overweight/obesity in 2011 in comparison to unoperated cataract patients.
Based on results concerning cataract incidence during 2000–2011, age-adjusted risk factors for cataract included limited or insufficient income and smoking among men, and occupation as employee and high alcohol consumption among women. The probability of having one’s cataract operated was highest among patients with only basic education, as well as smoking among men and high alcohol consumption among women.
Age, sex, and all evaluated background factors were included in fitted multivariable models, which are shown in Supplemental Table 3A and 3B. Based on the final models, age was the most significant risk factor of cataract and cataract surgery. Female sex and low income were significant risk factors of cataract in 2000 and the 2000–2011 follow-up. Female sex and single marital status were significant risk factors of cataract surgery in 2000, whereas smoking was a significant risk factor both in 2000 and the 2000–2011 follow-up.
The mean age at a person’s first cataract-related surgery was 72.0 years (95% CI 70.8–73.1) in 2000 and 71.6 years (95% CI 71.0–72.1) in 2011, showing no significant change in the mean age. The associations between age at the first cataract surgery and socio-demographic and lifestyle factors are shown in Table 6, stratified for sex. Female cataract patients who were single were operated at an older age compared to those living in a relationship at both the time points and in the follow-up. Cataract patients with higher education level were operated at a younger age compared to those with only basic education at both time points and in the follow-up. Female cataract patients who had sufficient income were operated at an older age compared to those with limited or insufficient income in 2000. Cataract patients who were farmers were operated at an older age, whereas employees were operated at a younger age at both time points and in the follow-up. Those who were current or former smokers were operated at a younger age compared to non-smokers at both time points and in the follow-up. This difference was also between current smokers and former or never smokers. In 2000 and in the follow-up, cataract patients with high alcohol consumption were operated at a younger age compared to those with lower levels of consumption. Finally, based on a fitted multivariable model (Supplemental Table 4), high education, employee as an occupation, smoking, and high alcohol consumption were associated with lower surgery age in the 2000–2011 follow-up, whereas being single was associated with higher surgery age.
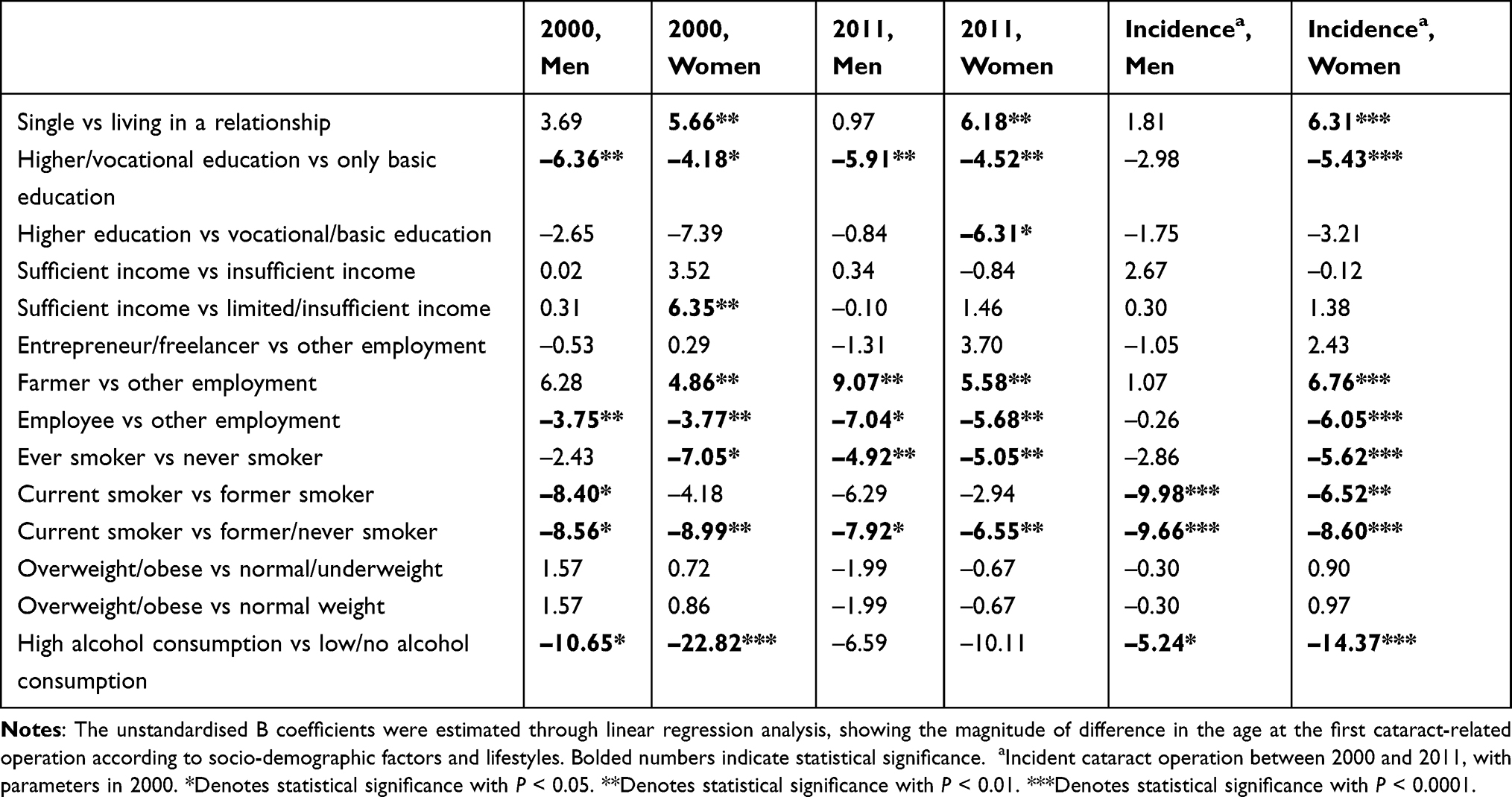 |
Table 6 Difference in the Age at the First Cataract Operation According to Socio-Demographic and Lifestyle Factors |
Discussion
The prevalence of cataract is increasing in Finland, following similar trend in other ageing populations.1,29 In previous literature, the association of cataract with sex has been inconclusive.2 In our study, women had a higher overall prevalence and incidence, although this difference was insignificant after age-adjustment. Furthermore, when adjusted for all evaluated background factors, this difference in sex was significant only in 2000. Therefore, the higher prevalence of female cataract patients is related to the higher life expectancy of women. The regional difference in the prevalence of cataract and cataract operations was relatively even throughout Finland. Somewhat higher prevalence of cataract was observed in Eastern Finland, where also many other diseases and health conditions are more prevalent in comparison to other regions of Finland.17,18
The prevalence of cataract surgery has increased between 2000 and 2011 in Finland. This trend is likely reflecting the increasing prevalence of cataract, as well as the improvement of eye care in Finland, including better awareness and improved detection of cataract, and the new Finnish legislation (National Guaranteed Access to Healthcare) in 2005, obligating cataract operations to be performed within six months after the notification. Because vision can have a significant impact on the quality of life of a patient, and other diseases and injuries caused by visual impairment increase the costs of health care, the availability of cataract surgery has a major role in maintaining quality of life and reducing the burden of health services.30
Low education and low income have been associated with cataract in previous studies.31,32 According to our results, even though cataract patients had received a lower level of education in comparison to those without cataract, this difference was not significant after adjusting for all background factors. Nevertheless, cataract patients with high education undergo surgery at a younger age compared to cataract patients with lower education, even after adjusting for potentially confounding factors. This may be explained that those with high education are working in professions where vision plays an important role and are likely to seek treatment earlier than those with lower education. The association between low income and cataract became insignificant between 2000 and 2011, and income showed no significant impact on operation age in 2011. This is most probably due to the Nordic welfare system attempting to provide equal use of health-care services.
The age-adjusted risk of cataract was the highest among employees in comparison to farmers, entrepreneurs, and freelancers, although no differences in occupation were found after adjusting for other background factors. Those who were employees were operated at a younger age in comparison to other occupations, even after adjusting for potential confounders. This is likely due to the high range of occupations as employees. The high prevalence and incidence of cataract among farmers can be explained by the higher age in this occupation, as the age-adjusted risk of cataract among farmers was somewhat low and cataract was operated at older age than in other occupations. Even though outdoor work has been associated with increased risk for cataract, possibly due to solar radiation exposure, other studies have suggested that rural setting may provide a healthier environment and living habits that could be protective factors against cataract.33,34
People with healthy living habits are more likely to live longer,35,36 and therefore are more likely to acquire cataract in comparison to those with unhealthy lifestyle who are likely to die at a younger age. On the other hand, our results show that cataract patients with unhealthy lifestyle are operated at a younger age, indicating that they develop cataract earlier than those with healthy lifestyle. This appears to be true regarding smoking and alcohol consumption but is less evident regarding unfavorable body mass index. Even after age-adjustment, smoking was a potential risk factor for cataract and cataract operations among men, and high alcohol consumption among women, supporting similar results in previous studies.11,13 Men are known to smoke and consume alcohol more than women in Finland, although high alcohol consumption is becoming more common among middle-aged and older women.17,18 Therefore, by promoting healthy lifestyle, the increase in the demand for cataract surgery can be prevented, alleviating the costs and burden of cataract care.
Our study had many strengths. The data were based on two nationwide surveys that addressed public health issues more comprehensively than national health surveys do on average.19,20 Because of this, our data did not consist of specific patient groups collected from health-care units, which allows better generalization of the results. Both surveys had high participation rates, and the loss in the follow-up was relatively small and was further corrected by applying weights. As high proportion of the study subjects participated in both the surveys, we were able to also evaluate the longitudinal effects with a relatively long, 11-year follow-up. Furthermore, we were able to use comprehensive Finnish nationwide health registries to obtain data on cataract diagnoses and operations. The number of cataract operations in Finland is reliable because of the standardized visual criteria for these operations.22
Our study also had potential limitations. As in many other population-based studies, selective participation may have caused some bias in the results, although it is likely to be small because the participation rate was quite high in both studies and because of the nationwide complex sampling design with post-stratification. The interview did not include questions on whether the patient had uni- or bilateral cataract. However, in most cases, cataract is bilateral and often an asymmetric disease.7 The variation in the age of the participants was large, but we adjusted for age in the analyses.
Conclusion
In conclusion, the prevalence of cataract and cataract surgery is increasing with the ageing of the population. The increase in cataract surgeries is also likely reflecting the improvements in eye care. Cataract is associated with age-related socio-demographic factors, but the possibility to equally use health-care services throughout the country appears to reduce the impact of socio-demographic status. Healthy lifestyle is not preventing cataract because of the longer life expectancy, but it delays the development of cataract and need for cataract operations. On the contrary, persons with unhealthy lifestyle acquire cataract earlier and are operated at a younger age, therefore increasing the demand for cataract operations. These population-based findings from Finland are likely to apply to most Western countries where population is rapidly ageing. The availability of cataract services and promotion of healthy lifestyle will be the key to prevent the decrease of quality of life and increase of health-care costs due to cataract and related impaired vision.
Acknowledgments
This work was supported by Tampereen seudun Näkövammaisten tukisäätiö s.r, Tampere, Finland; Glaukooma Tukisäätiö Lux s.r, Helsinki, Finland; Sokeain Ystävät r.y, Helsinki, Finland; and Elsemay Björn Fund, Helsinki, Finland. Funding sources did not influence the study design, data collection, analysis, interpretation, or writing of the publication. The decision of publishing the results was completely made by the authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Mr Petri KM Purola reports grants from Tampereen seudun Näkövammaisten tukisäätiö s.r, grants from Glaukooma Tukisäätiö Lux s.r, grants from Sokeain Ystävät r.y, grants from Elsemay Björn Fund, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Flaxman SR, Bourne RRA, Resnikoff S, et al. Vision loss expert group of the global burden of disease study. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–1234. doi:10.1016/S2214-109X(17)30393-5
2. Hashemi H, Pakzad R, Yekta A, et al. Global and regional prevalence of age-related cataract: a comprehensive systematic review and meta-analysis. Eye. 2020;34(8):1357–1370. doi:10.1038/s41433-020-0806-3
3. NCD Risk Factor Collaboration. Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants. Lancet. 2016;387(10027):1513–1530. doi:10.1016/S0140-6736(16)00618-8
4. NCD Risk Factor Collaboration. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet. 2017;390(10113):2627–2642. doi:10.1016/S0140-6736(17)32129-3
5. NCD Risk Factor Collaboration. Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19·1 million participants. Lancet. 2017;389(10064):37–55. doi:10.1016/S0140-6736(16)31919-5
6. Hirvelä H, Luukinen H, Laatikainen L. Prevalence and risk factors of lens opacities in the elderly in Finland. A population-based study. Ophthalmology. 1995;102(1):108–117. doi:10.1016/S0161-6420(95)31072-X
7. Asbell PA, Dualan I, Mindel J, Brocks D, Ahmad M, Epstein S. Age-related cataract. Lancet. 2005;365(9459):599–609. doi:10.1016/S0140-6736(05)70803-5
8. Ono K, Hiratsuka Y, Murakami A. Global inequality in eye health: country-level analysis from the global burden of disease study. Am J Public Health. 2010;100(9):1784–1788. doi:10.2105/AJPH.2009.187930
9. Mangione CM, Phillips RS, Lawrence MG, Seddon JM, Orav EJ, Goldman L. Improved visual function and attenuation of declines in health-related quality of life after cataract extraction. Arch Ophthalmol. 1994;112(11):1419–1425. doi:10.1001/archopht.1994.01090230033017
10. Cedrone C, Culasso F, Cesareo M, et al. Prevalence and incidence of age-related cataract in a population sample from Priverno, Italy. Ophthalmic Epidemiol. 1999;6(2):95–103. doi:10.1076/opep.6.2.95.1562
11. Ye J, He J, Wang C, et al. Smoking and risk of age-related cataract: a meta-analysis. Invest Ophthalmol Vis Sci. 2012;53(7):3885–3895. doi:10.1167/iovs.12-9820
12. West SK, Duncan DD, Munoz B, et al. Sunlight exposure and risk of lens opacities in a population-based study: the Salisbury Eye Evaluation project. JAMA. 1998;280(8):714–718. doi:10.1001/jama.280.8.714
13. Ritter LL, Klein BE, Klein R, Mares-Perlman JA. Alcohol use and lens opacities in the Beaver Dam Eye Study. Arch Ophthalmol. 1993;111(1):113–117. doi:10.1001/archopht.1993.01090010117037
14. Kim TN, Lee JE, Lee EJ, et al. Prevalence of and factors associated with lens opacities in a Korean adult population with and without diabetes: the 2008–2009 Korea National Health and Nutrition Examination Survey. PLoS One. 2014;9(4):e94189. doi:10.1371/journal.pone.0094189
15. Richter GM, Torres M, Choudhury F, Azen SP, Varma R. Risk factors for cortical, nuclear, posterior subcapsular, and mixed lens opacities: the Los Angeles Latino Eye Study. Ophthalmology. 2012;119(3):547–554. doi:10.1016/j.ophtha.2011.09.005
16. Skalka HW, Prchal JT. Effect of corticosteroids on cataract formation. Arch Ophthalmol. 1980;98(10):1773–1777. doi:10.1001/archopht.1980.01020040625007
17. Aromaa A, Koskinen S. Health and functional capacity in Finland: baseline results of the health 2000 health examination survey (in Finnish). National Public Health Institute, Report 12B/2004. Available from: http://urn.fi/URN:NBN:fi-fe201204193452.
18. Koskinen S, Lundqvist A, Ristiluoma N. Health, functional capacity and welfare in Finland in 2011 (in Finnish). Finnish Institute for Health and Welfare, Report 68/2012. Available from: http://urn.fi/URN:ISBN:978-952-245-769-1.
19. Heistaro S. Methodology report: Health 2000 survey. Publications of the National Public Health Institute; 2008. Available from: http://urn.fi/URN:NBN:fi-fe201204193320.
20. Lundqvist A, Mäki-Opas T. Health 2011 Survey – methods. Publications of the National Institute for Health and Welfare, 8/2016. Available from: http://urn.fi/URN:ISBN:978-952-302-669-8.
21. Härkänen T, Karvanen J, Tolonen H, et al. Systematic handling of missing data in complex study designs - experiences from the Health 2000 and 2011 Surveys. J Appl Stat. 2016;43(15):15. doi:10.1080/02664763.2016.1144725
22. Välimäki J, Linnola R, Marttila L, Nieminen R, Suomalainen VP, Tuisku I. Current Care Guideline for Cataract. The Finnish Medical Society Duodecim; 2019. Available from: https://www.kaypahoito.fi/en/ccs00011.
23. World Health Organization. Manual of the international statistical classification of disease, injuries, and causes of death. Based on the recommendations of the eighth revision conference, 1965, and adopted by the Nineteenth World Health Assembly. World Health Organization; 1967.
24. World Health Organization. Manual of the international statistical classification of diseases, injuries, and causes of death: based on the recommendations of the ninth revision conference, 1975, and adopted by the Twenty-ninth World Health Assembly. World Health Organization; 1977.
25. World Health Organization. ICD-10: international statistical classification of diseases and related health problems: tenth revision. World Health Organization; 2004.
26. World Health Organization. BMI Classification. Global database on body mass index; 2006. Available from: https://web.archive.org/web/20150501075305/http://whqlibdoc.who.int/trs/WHO_TRS_894_(part1).pdf.
27. Corrao G, Bagnardi V, Zambon A, Arico S. Exploring the dose-response relationship between alcohol consumption and the risk of several alcohol-related conditions: a meta-analysis. Addiction. 1999;94(10):1551–1573. doi:10.1046/j.1360-0443.1999.9410155111.x
28. Lumley T. Analysis of complex survey samples. J Stat Softw. 2004;9(8):1–19. doi:10.18637/jss.v009.i08
29. Congdon N, Vingerling J, Klein B, et al. Prevalence of cataract and pseudophakia/aphakia among adults in the United States. Arch Ophthalmol. 2004;122:487–494.
30. Purola PKM, Nättinen JE, Ojamo MUI, et al. Prevalence and 11-year incidence of common eye diseases and their relation to health-related quality of life, mental health, and visual impairment. Qual Life Res. 2021;30(8):2311–2327. doi:10.1007/s11136-021-02817-1
31. Delcourt C, Cristol JP, Tessier F, Leger CL, Michel F, Papoz L. Risk factors for cortical, nuclear, and posterior subcapsular cataracts: the POLA study. Pathologies Oculaires Liees a l’Age. Am J Epidemiol. 2000;151(5):497–504. doi:10.1093/oxfordjournals.aje.a010235
32. Rim TH, Kim MH, Kim WC, Kim TI, Kim EK. Cataract subtype risk factors identified from the Korea national health and nutrition examination survey 2008–2010. BMC Ophthalmol. 2014;14(1):4. doi:10.1186/1471-2415-14-4
33. Modenese A, Gobba F. Cataract frequency and subtypes involved in workers assessed for their solar radiation exposure: a systematic review. Acta Ophthalmol. 2018;96(8):779–788. doi:10.1111/aos.13734
34. Rim TH, Kim DW, Kim SE, Kim SS. Factors associated with cataract in Korea: a Community health survey 2008–2012. Yonsei Med J. 2015;56(6):1663–1670. doi:10.3349/ymj.2015.56.6.1663
35. Östergren O, Martikainen P, Tarkiainen L, Elstad JI, Brønnum-Hansen H. Contribution of smoking and alcohol consumption to income differences in life expectancy: evidence using Danish, Finnish, Norwegian and Swedish register data. J Epidemiol Community Health. 2019;73(4):334–339. doi:10.1136/jech-2018-211640
36. Knudsen AK, Allebeck P, Tollånes MC; Nordic Burden of Disease Collaborators. Life expectancy and disease burden in the Nordic countries: results from the global burden of diseases, injuries, and risk factors study 2017. Lancet Public Health. 2019;4(12):e658–e669. doi:10.1016/S2468-2667(19)30224-5
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.