Back to Journals » Cancer Management and Research » Volume 12
Pretreatment Apparent Diffusion Coefficient as a Predictor of Response to Transcatheter Arterial Chemoembolization Immediately Combined with Radiofrequency Ablation for Treatment of Solitary Large Hepatocellular Carcinoma
Authors Tang J, Liu F, Yuan H, Li X, Tian X, Ji K, Li X, Wang W
Received 10 July 2020
Accepted for publication 8 September 2020
Published 14 October 2020 Volume 2020:12 Pages 10127—10138
DOI https://doi.org/10.2147/CMAR.S270470
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eileen O'Reilly
Jing Tang,1,2 Fengyong Liu,2 Hongjun Yuan,2 Xin Li,2 Xiaomei Tian,2 Kan Ji,2 Xueping Li,3 Wei Wang3
1Medical School of Chinese PLA, Beijing, People’s Republic of China; 2Department of Interventional Radiology, The First Medical Center, Chinese PLA General Hospital, Beijing, People’s Republic of China; 3Department of Radiology, The First Medical Center, Chinese PLA General Hospital, Beijing, People’s Republic of China
Correspondence: Fengyong Liu
Department of Interventional Radiology, The First Medical Center, Chinese PLA General Hospital, No. 28, Fuxing Road, Haidian District, Beijing 100853, People’s Republic of China
Tel +8613371668617
Fax +86-10-66939340
Email [email protected]
Purpose: To evaluate whether the pretreatment apparent diffusion coefficient (ADC) measured with diffusion weighted imaging (DWI) of tumor can be used as an imaging biomarker for predicting prognosis in solitary large hepatocellular carcinomas (HCCs) treated with transcatheter arterial chemoembolization (TACE) immediately combined with radiofrequency ablation (RFA).
Patients and Methods: In this single institution retrospective study, 40 solitary large HCCs that underwent treatment with TACE immediately combined with RFA were analyzed. All patients underwent abdominal dynamic contrast-enhanced magnetic resonance imaging within one month before treatment with DWI, and ADC values in the lesions were measured by two independent radiologists. Associations among patients’ preoperative ADC values and objective response (OR), progression-free survival (PFS) and overall survival (OS) were examined. Survival curves were drawn with the Kaplan–Meier method, and differences were determined with the Log rank test. The Cox proportional-hazards model was used for univariate and multivariate analyses of PFS and OS.
Results: Forty solitary large HCCs (mean 9.54 cm, range 5.04– 16.06 cm) were successfully treated with TACE in immediate combination with RFA (OR 75%). The ADC values were significantly higher in the response group than the non-response group (1.51± 0.32× 10− 3 mm2/s vs 1.09± 0.17× 10− 3 mm2/s; P< 0.001). As predicted on the basis of the ADC values, the optimal cutoff value for the efficacy of TACE combined with RFA was 1.32× 10− 3 mm2/s, with a predictive sensitivity of 0.63 and a specificity of 1.00. Patients with high ADC had longer PFS than those with low ADC (14.9 months vs 5.3 months; P< 0.001) and had significantly longer survival rates (22.6 months vs 12.1 months; P=0.004).
Conclusion: Preoperative ADC values < 1.32× 10− 3 mm2/s are an independent predictor of poorer prognosis in patients with solitary large HCCs who have undergone TACE immediately combined with RFA.
Keywords: solitary large hepatocellular carcinoma, apparent diffusion coefficient, TACE, radiofrequency ablation
Introduction
Liver cancer, the fourth most common cause of cancer-related death, ranks sixth in terms of cancer incidence; hepatocellular carcinoma (HCC) accounts for most primary liver cancers.1 Even if screening programs for cirrhosis allow for increased diagnosis of small HCC, large tumors still remain common.2 Solitary large HCCs, which exhibit only solitary nodes with diameters larger than 5 cm and grow expansively within intact capsules or pseudocapsules, are a special type of liver cancer that commonly has a more benign biological behavior than multinodular type cancer.3 Although solitary large HCCs can be resected safely in certain patients,4 elevated bilirubin, portal hypertension or vascular invasion excludes patients with a single large HCC from liver hepatectomy.5 In patients with unresectable solitary large HCC, the combination of transcatheter arterial chemoembolization (TACE) and radiofrequency ablation (RFA) is synergistic: each method overcomes the limitations of the other, thereby significantly improving the local tumor inactivation rate, recurrence-free survival rate and overall survival (OS), as compared with either RFA or TACE monotherapy.6–9 With the development of cone-beam CT and angio-CT, a single-session combination of TACE and RFA has become a new and effective choice for the treatment of solitary large HCCs with satisfactory outcomes.10–13 In solitary large HCCs, as in many other cancers, identifying potential predictors of locoregional therapy response remains important.
Diffusion weighted imaging (DWI) can be used to evaluate the random Brownian motion of water molecules inside and outside tumor cells through the apparent diffusion coefficient (ADC), thereby indirectly reflecting the changes in the tumor tissue microenvironment, including tumor cell density, hypoxia, interstitial pressure level and metastasis tendency.14 Prior studies have found that the ADC is inversely correlated with the histological grade and microvascular invasion of HCC.15,16 Many studies also have confirmed that increases in the ADC at different times after TACE are consistent with different TACE response results (mRECIST, histopathological necrosis and progression-free survival [PFS]).17–19 However, pretreatment ADC has been investigated as an imaging predictor of HCC response to locoregional therapies and overall survival (OS), and conflicting results have been reported.20–26 Some studies20,21,23 have shown that a high pretreatment mean ADC is predictive of poor HCC response to intraarterial therapies, whereas Mannelli et al22 have demonstrated the opposite conclusion, in which lower ADC is associated with poorer response to chemoembolization. As for the combination therapy, especially for the immediate combination of TACE and RFA, the predictive value of ADC remains unknown.
Hence, we conducted this study to evaluate whether the preoperative ADC value might be used as an imaging predictor of the short-term prognosis of solitary large HCCs treated with TACE immediately combined with RFA, as well as of long-term patient survival.
Patients and Methods
Study Population
This single institution retrospective study complied with the Declaration of Helsinki, and the study protocol was approved by the Ethics Committee of the Chinese PLA General Hospital. An institutional interventional radiology database was searched for all patients with solitary large HCC between December 2014 and July 2018. The selection criteria were as follows: (1) solitary large HCCs diagnosed with imaging criteria defined by the European Association for the Study of the Liver (EASL) guidelines or by biopsy, with a maximum tumor diameter of >5 cm; (2) patient refusal of surgery or patient not being a candidate for surgery; (3) Child-Pugh grade for liver function rated A or B, or Barcelona Clinic Liver Cancer (BCLC) stage A, B, or C; (4) treatment with TACE immediately combined with RFA; (5) MRI including DWI performed within 30 days before the procedure. The exclusion criteria were as follows: (1) multiple HCCs; (2) macrovascular invasion of the main portal vein or the main portal branches and extrahepatic metastases; (3) no regular postoperative follow-up performed by the PLA General Hospital; (4) serious image artifacts that affect measurement. All patients were discussed in a multidisciplinary team (MDT) involving interventional radiologists, oncologists, radiation oncologist and surgical oncologists and considered for TACE immediately combined with RFA.
A total of 374 consecutive large liver carcinomas treated with TACE immediately combined with RFA were identified. After application of the exclusion criteria, a total of 40 patients with large solitary HCCs (mean 9.54±3.18 cm, range 5.04–16.06 cm) who underwent treatment with TACE immediately combined with RFA were enrolled our study (34 males, 6 females; mean age 55 years, range 28–82 years). The flowchart is shown in Figure 1. The diagnosis of solitary large HCC was confirmed through biopsy in 12 patients and on the basis of imaging criteria in 28 patients. All included patients volunteered to receive TACE immediately combined with RFA treatment and provided signed informed consent at the time of treatment.
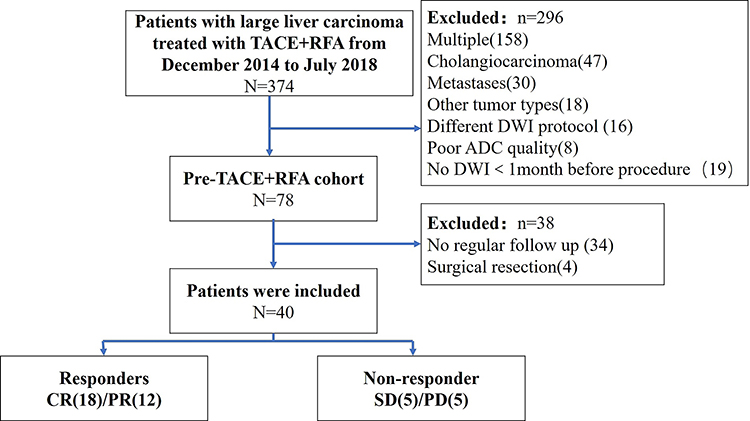 |
Figure 1 Flow chart of patients included in the study. |
MRI Technique
All pretreatment magnetic resonance imaging (MRI) was performed with a 3.0-T MRI system (Discovery 750, GE Healthcare, Minneapolis, USA) with a combined 32-channel body and spine phased-array coil. The routine liver protocol included T2 weighted sequences, respiratory-triggered gradient spin shot echo-planar DWI, in/out phase T1 weighted sequences and 3D postcontrast dynamic contrast-enhanced T1fat suppressed sequences (Table 1). The dynamic contrast-enhanced phase was injected at a rate of 1.5 mL/s with gadopentetate dimeglumine (Magnevist, Bayer, Berlin, Germany) at a dose of 0.1 mmol/kg followed by 20 mL of saline solution. The dynamic contrast-enhanced images included arterial-phase (15s), venous-phase (70s) and delayed-phase (180s) after the contrast agent injection.
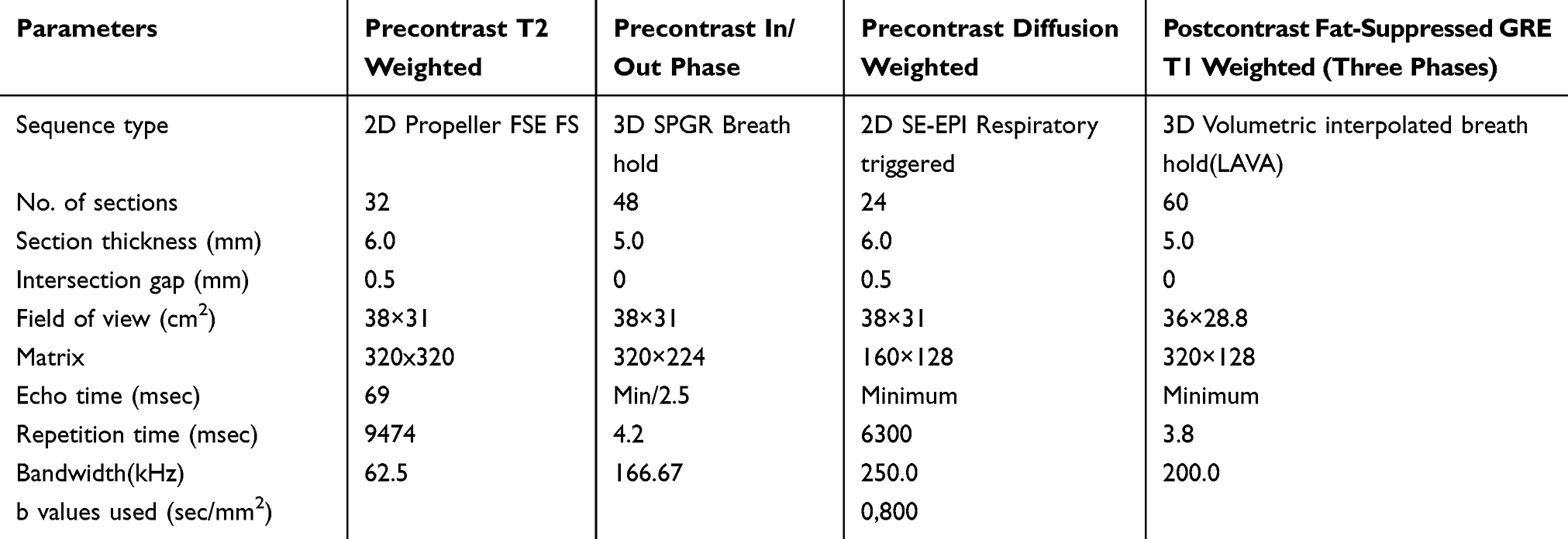 |
Table 1 Sequence Parameters for Upper Abdominal 3.0-T MR Imaging |
The respiratory-triggered fat suppressed single shot echo-planar imaging (SS EPI) DWI protocol with tridirectional diffusion was performed by using two b-values of 0 and 800 s/mm2 (echo time, minimum; slice thickness/gap, 6/0.5 mm; matrix, 160×128; FOV, 39×31 cm2) (Table 1). ADC maps were calculated on a workstation (GE Healthcare, Minneapolis, MN, USA).
TACE Treatment
TACE was performed via Siemens Artis Zee digital subtraction angiography (DSA) (Siemens AG, Germany) by an interventional radiologist (FYL, with 15 years of interventional therapy experience). The modified Seldinger vascular puncture method was adopted to perform femoral artery puncture after routine disinfection. Celiac and superior mesenteric artery angiography was performed with a 4F general catheter (RH, Terumo Corporation, Japan), and selective hepatic arteriography was also performed if necessary. A 2.6F super-selective microcatheter (Progreat, Terumo Corporation, Tokyo, Japan) was then used to perform chemoembolization into the tumor blood supply artery. Preoperative drugs were determined according to the tumor volume, patient weight and general physical conditions, generally including two to four chemotherapeutic agents selected from among epirubicin (30–50 mg), mitomycin (8–12 mg), pirarubicin hydrochloride (40–50 mg), 5-FU (500–750 mg), calcium folinate (75–100 mg), and oxaliplatin (100–150 mg) or cisplatin (40–60 mg). Each chemotherapy drug powder was mixed preoperatively with iodized oil (lipiodol; Laboratoire Guerbet, Roissy, France) to form an emulsion. The total amount of iodide in a single treatment depended on the tumor size but did not exceed 20 mL. Meanwhile, gelatin sponge particles and polyvinyl alcohol were added (300–700 µmol/L, Cook Medical, Bloomington, IN, USA) for patients with tumors with extensive blood supply. In addition, extrahepatic collateral artery embolization was performed if there were collateral arteries supplying the tumor (such as the subphrenic artery or omental artery).
Immediate RFA Treatment
RFA was performed immediately after TACE in patients under local anesthesia, under the guidance of a Somatom Emotion CT scanner (Medical Solutions AG, Siemens, Germany). A square grid bar was placed parallel to the right 8–10 costal margin or under the xiphoid, and then the target lesions were scanned with imaging 3D reconstruction. The puncture path was accurately designed by an interventional radiologist (FYL, with 20 years of experience in interventional treatment) according to tumor size, shape, location, adjacent relationship and intraoperative iodide oil deposition, and the body surface was marked. The puncture path avoided the intestine, gallbladder and lungs. After repeated CT scanning to confirm that the puncture needle was in the correct position, the multipole radiofrequency needle was slowly opened (Figure 2E and F). Because the patients had large HCC, all cases were treated with multipole radiofrequency needles with a maximum ablation diameter of 3–5 cm (RITA, Cristal Lake, IL, USA) and a needle length of 15–25 cm. The radiofrequency treatment parameters were as follows: treatment power of 150–200 W, target temperature of 105°C and radiofrequency ablation time of 15–20 min. RFA was routinely performed two or three times until the ablation range covered the tumor edge and its entire three-dimensional space. Finally, the puncture path was solidified at 70–90°C to decrease the risk of bleeding and tumor implantation metastasis via the path at the end of ablation. After surgery, the hepatoprotective treatment was routinely administered to protect against liver failure.
 |
Figure 2 A male patient aged 47 years with a large solitary hepatocellular carcinoma in V and VIII segment. (A, B) Pretreatment of TACE immediately combined with RFA, the lesion showed heterogeneous low signal on apparent diffusion coefficient map (A) with ADC value of 1.51×10−3mm2/s, heterogeneous enhancement (white arrow) in arterial phase (B). (C) Intra-operative digital subtraction angiography showed staining of the large tumor (black arrows). (D) TACE treatment. (E, F) RFA was performed immediately after TACE treatment. (G) Abdominal magnetic resonance imaging performed one month after the combined treatment, the tumor (white arrow) showed complete response. (H) The tumor (white arrow) was well controlled, and no recurrence was found after 12 months follow-up. This patient showed CR at 1month, with progression-free survival of 34.53 months and overall survival of 56.4 months. |
Image Processing and Data Acquisition
Two independent radiologists with four and five years of experience in abdominal MR (JT and HJY, observers 1 and 2, respectively) retrospectively reviewed DWI on a GE AW4.6 workplace (GE Healthcare, Minneapolis, MN, USA) in random order under the supervision of a third experienced radiologist with 20 years of experience in abdominal MR (FYL, observer 3). The three radiologists were blinded to the clinical data and histopathologic results. ADC maps from the pre-procedure MRI were obtained on a workstation (GE Healthcare, Minneapolis, MN, USA) by using two b-values (0 and 800 s/mm2). Because tumor visualization may be difficult on only ADC maps, the tumor was located on the ADC map (Figure 2A) in combination with contrast-enhanced images (Figure 2B). The observers 1 and 2 measured the mean ADC values of solitary large HCC lesions at the maximum tumor diameter level by drawing a region of interest (ROI) over the entire HCC lesion, including both viable and necrotic tissue components. The lesion ADC values from the pre-procedure MRI were recorded.
Response to therapy was assessed by observer 3 through the post-procedure dynamic-enhanced CT or MRI examinations. Categorization of response groups by efficacy evaluation was performed according to modified response evaluation criteria in solid tumor (mRECIST), which is designed to evaluate curative effects in liver cancer.27 Efficacy was divided into complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). The objective response (OR) was CR plus PR.
Postoperative Follow-Up and Efficacy Evaluation
All patients were reviewed at the PLA General Hospital. The routine blood examination and hepatorenal function tests were performed two days to one week after the operation. Patients underwent blood examination for hepatorenal function and tumor markers, abdominal contrast-enhanced MRI or CT one month after the operation. If the tumor was well controlled, follow-up examinations were performed once every 2–3 months. Patients were reevaluated in the MDT after each follow-up visit and additional TACE+RFA or TACE was done “on demand,” followed by clinical and radiological response assessment.
In cases with postoperative complications, patients were treated promptly, and the objective response rate, necrosis characteristics and patient survival condition were monitored during the follow-up. All patients had pain at the puncture site, which was relieved with morphine or oral central analgesics. After the operation, patients had fevers with a body temperature of 37.7–40.9°C. In some patients, the blood routine tests and liver function indicators were temporarily elevated after operation but returned to normal after one week of pain control, hypothermia therapy and hepatoprotective treatment. No serious complications, such as hepatapostema, liver/kidney failure and acute tumor lysis syndrome, occurred. PFS was defined as the time period from the start of treatment to disease progression at follow-up or the patient’s death, whichever came first; OS was defined as the time period from the start of treatment to the patient’s death.
Statistical Analysis
Data analysis was performed by using commercial software (SPSS Statistics for Windows, version 24.0; IBM, Armonk, USA). The inter-observer variability for ADC measurements was assessed with the intra-class correlation coefficient (ICC). ICC values of 0–0.4 were classified as poor reliability; ICC values of 0.40–0.75, fair to good reliability; ICC values of 0.75–1.00, excellent reliability. Measurement data are expressed as mean value ± standard deviation, whereas count data are described by frequency and percentage and were compared by chi-square test or Fisher’s exact test. The measurement data were analyzed by a t-test and one-way analysis of variance or rank sum test according to whether the data conformed to a normal distribution. Receiver operating characteristic (ROC) analysis of ADC values was performed to predict the short-term prognosis of SLHCC patients.
Survival curves were drawn with the Kaplan–Meier method, and intra-group comparisons were made with Log rank test. Univariate survival analysis was performed with the Cox proportional-hazards model, in which the variables with P<0.10 were included in Cox multivariate survival analysis. The hazard ratio and its 95% confidence interval (CI) were used to express the relative risk, and thus the relationship of each variate with the PFS and OS of patients was analyzed. P-values less than 0.05 were considered statistically significant.
Results
Patient Baseline Characteristics
The study examined 40 consecutive patients with solitary large HCC who were treated with TACE immediately combined with RFA and were 28 to 82 years of age (median 55 years) and included 34 (85%) males and 6 females (15%). Of these, 39 patients had a history of cirrhosis (97.5%), and most patients (85%) had good liver metabolism and liver function (Child-Pugh grade A). The patients were treated with immediately TACE combined with RFA for an average of 2.18 times (range:1~5 times), accounting for 60% of the total number of treatments (3.75 times) which was performed by the patients. A total of 12 (30%) patients presented with portal vein thrombosis (PVTT) including PV1 (segmentary branch, 4) and PV2 (secondary order branch, 8), 11 of whom received additional stereotactic body radiation therapy (SBRT). Patient baseline characteristics are summarized in Table 2.
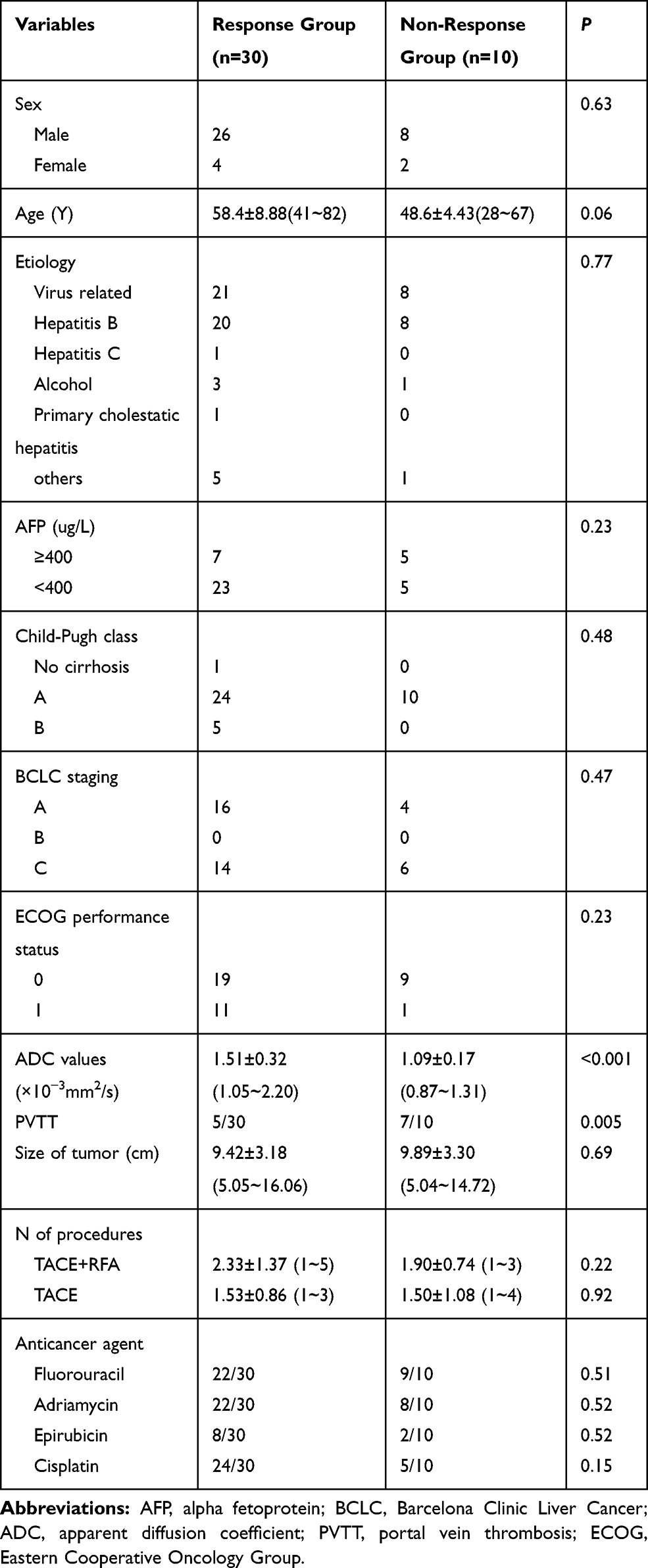 |
Table 2 Baseline Characteristics of Study Patients Based on Response |
The mean diameter of solitary large HCCs was 9.54±3.18 cm (range 5.04–16.06 cm). No significant differences in tumor size were observed between the responding group and the non-responding group (9.42 cm±3.18 vs 9.89 cm±3.30; P=0.69). There was no difference in the patients’ baseline characteristics (sex, age, serum AFP value, Child-Pugh classification, BCLC staging, ECOG performance status, anticancer agent and treatment times) between the responding and non-responding tumors (P>0.05). However, the difference in ADC values, and PVTT between the responding group and the non-responding group were statistically significant (P=0.005, P<0.001).
ADC Values and OR
The interobserver reliability with regard to the ADC measurements between the two radiologists was excellent (ICC = 0.98). The ADC values of 40 solitary large HCCs ranged from 0.87 ×10−3 mm2/s to 2.20 ×10−3 mm2/s, with a mean ADC value of 1.40×10−3 mm2/s. The mean time between pretreatment MR imaging and treatment (TACE immediately combined with RFA) was 6.1 days (range 1–26 days). At the one-month follow-up, 75% (30/40) of patients showed an objective response based on mRECIST criteria, among whom 45% had CR, and 30% had PR. The ADC value of the response group was significantly higher than that of the non-response group (1.51±0.32×10−3 mm2/s vs 1.09±0.17×10−3 mm2/s; P<0.001) (Figure 3).
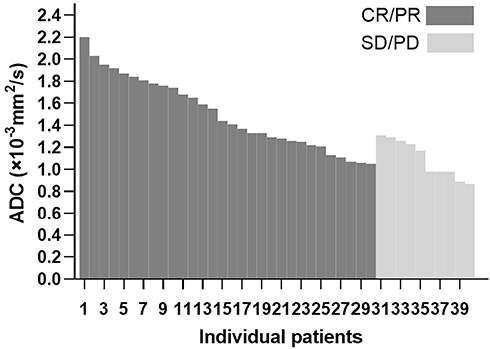 |
Figure 3 Histogram of individual treated lesions’ baseline ADC values and corresponding OR at 1month. |
The ADC values showed that the area under the ROC curve for the patients with solitary large HCCs treated with TACE immediately combined with RFA was 0.860 (95% CI: 0.740–0.980), the best cutoff value was 1.32×10−3 mm2/s, the prediction sensitivity was 63%, and the specificity was 100%. The OR of the high ADC value group (100%) was significantly higher than that of the low ADC group (52.4%) (P=0.001) (Table 3).
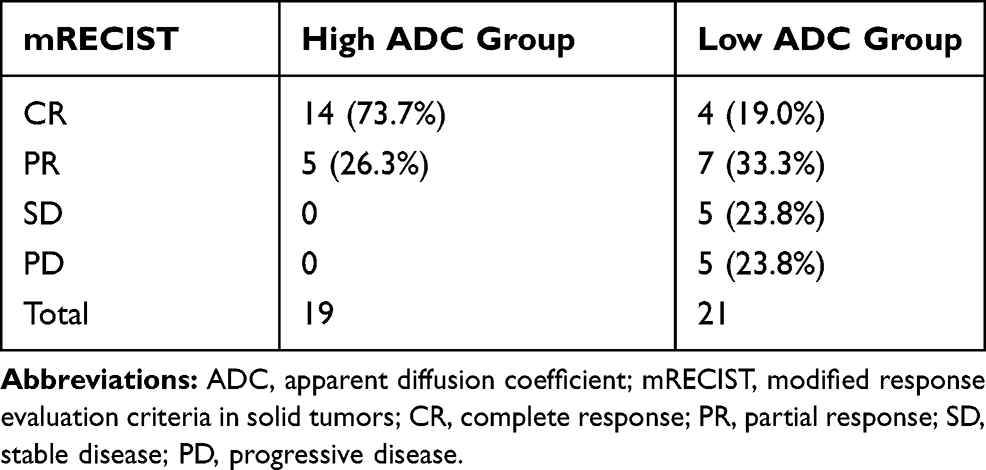 |
Table 3 ADC Groups and Response Rates According to mRECIST at 1 Month |
ADC Values and Survival Analysis
Long-term dynamic follow-up of 40 patients from the treatment to August 11, 2019, when the follow-up was terminated revealed that 18 patients had died (including 11 with metastases, 4 with hepatic encephalopathy and 3 with gastrointestinal bleeding). Among the 18 patients with complete responses (as illustrated in Figure 2), 3 patients died of lung metastasis, bone metastasis and digestive system hemorrhage at the 14th, 15th and 18th month of follow-up, respectively; among 12 patients with partial response, 5 patients died because of hepatic encephalopathy, pulmonary metastasis and osseous metastasis at the 7th, 8th, 12th, 13th and 14th month of follow-up.
The median PFS for all 40 patients was 5.98 months (range 1.2–35.7 months), and the median OS was 15.6 months (range 3.1–56.4 months). The postoperative PFS and OS curves of the two groups are shown in Figures 4 and 5. Patients in the high ADC group had a significant longer PFS (14.9 months vs 5.3 months; P<0.001) and OS (22.6 months vs 12.1 months; P=0.004) than those in the low ADC group. The results of univariate analysis revealed that serum AFP levels and ADC values were associated with PFS, whereas multivariate analysis showed that the ADC was an independent risk factor for PFS (Table 4). The univariate analysis of OS with the Cox proportional-hazards model demonstrated that serum AFP levels and ADC values were associated with OS, whereas multivariate analysis revealed that the ADC was an independent risk factor for OS (Table 5).
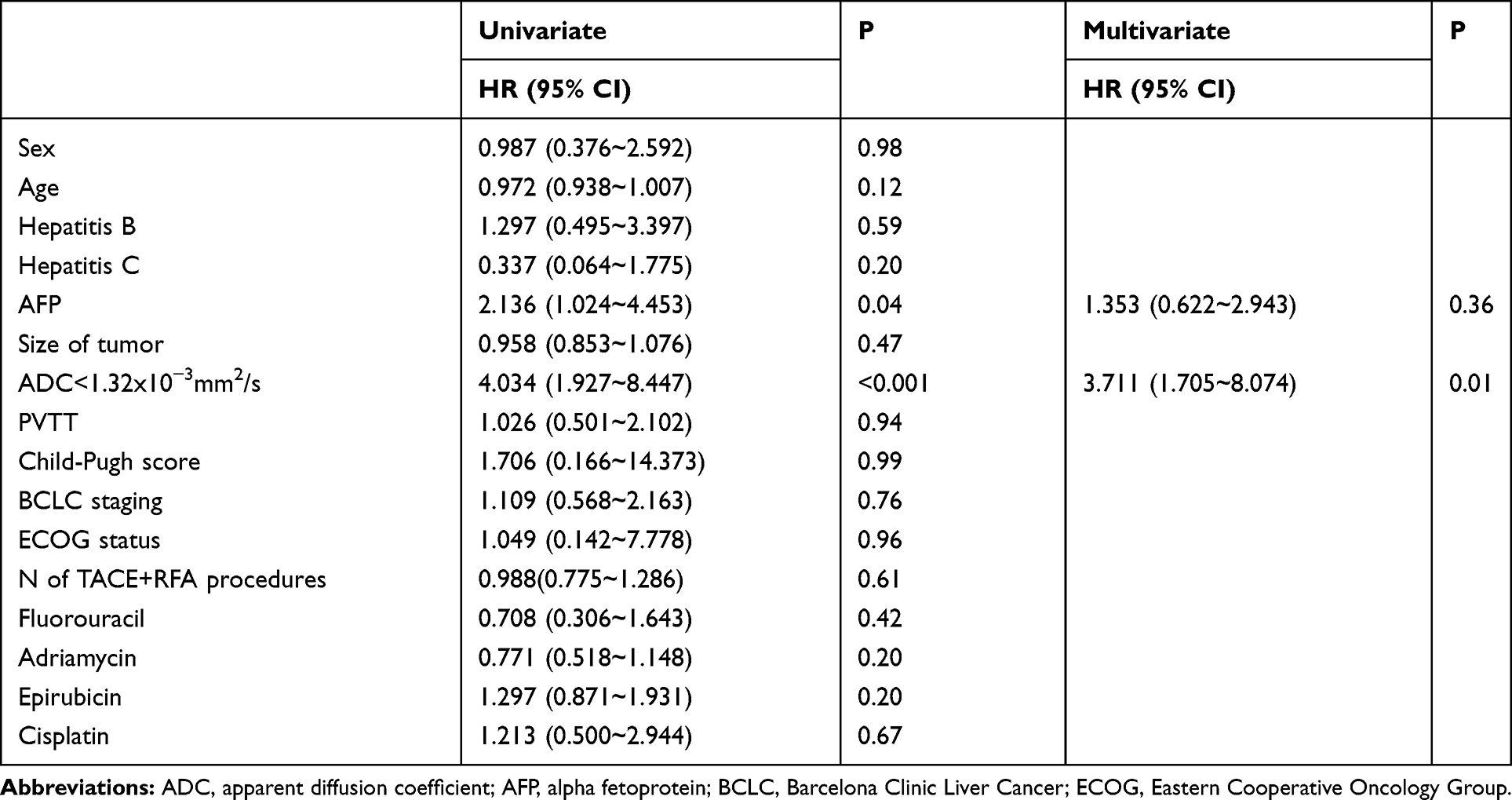 |
Table 4 Univariate and Multivariate Analysis of Demographic and Imaging Covariates for PFS |
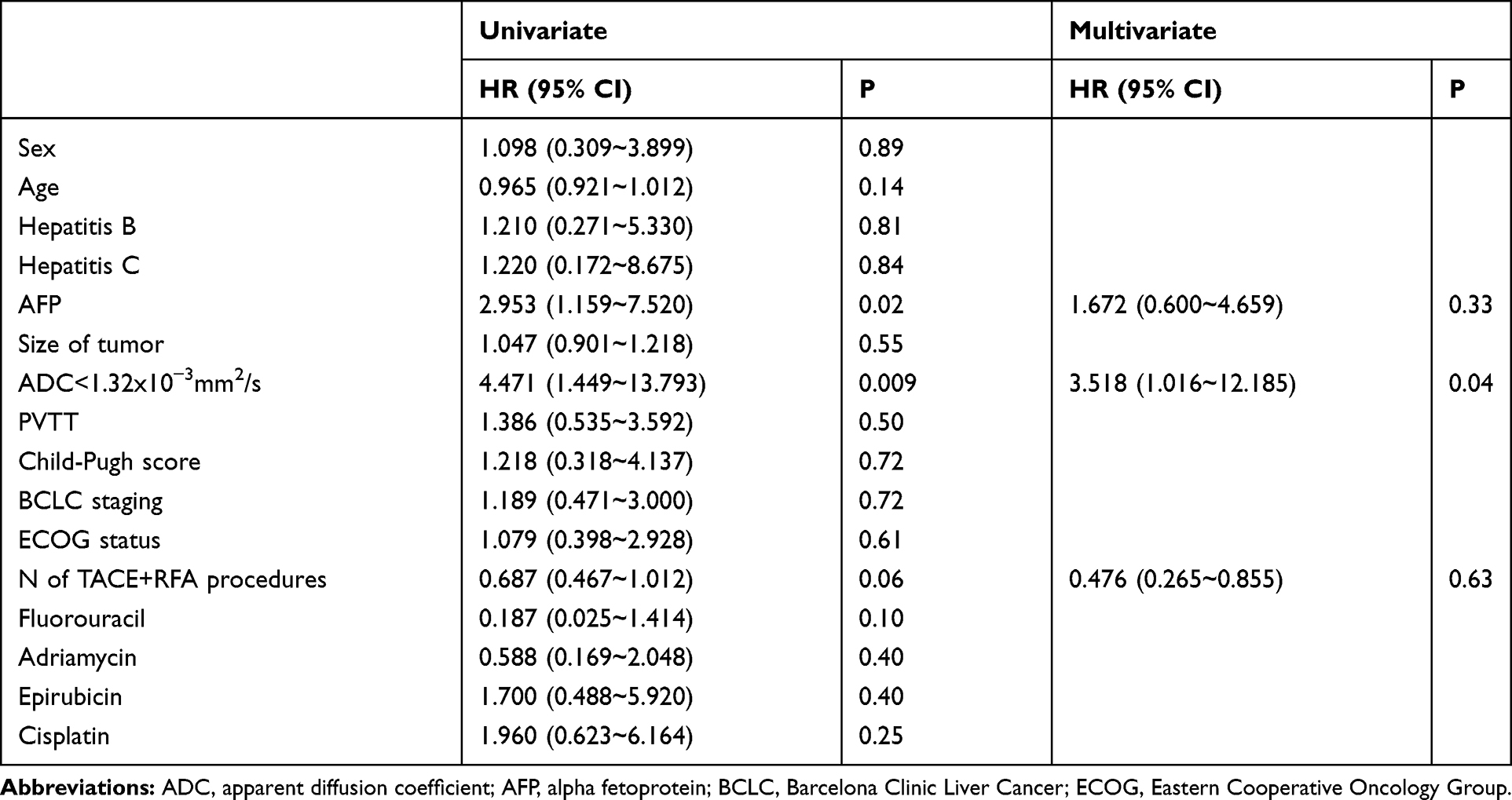 |
Table 5 Univariate and Multivariate Analysis of Demographic and Imaging Covariates for OS |
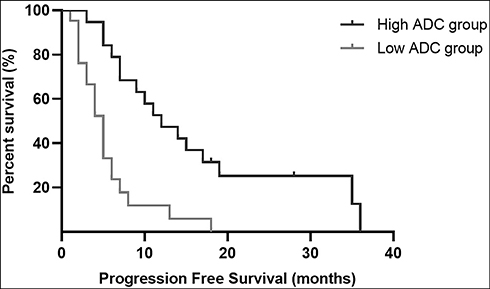 |
Figure 4 Kaplan–Meier curves show progression-free survival in patients with solitary large HCC in the High ADC and Low ADC groups. High apparent diffusion coefficient (ADC) values were significantly associated with better progression-free survival (PFS) (P<0.001). |
 |
Figure 5 Kaplan–Meier curves show overall survival in patients with solitary large HCC in the High ADC and Low ADC groups. High apparent diffusion coefficient (ADC) values were significantly associated with better overall survival (OS) (P=0.004). |
Discussion
To our knowledge, this is the first reported analysis of whether the pretreatment ADC in solitary large HCCs treated with chemoembolization immediately combined with RFA therapy is associated with short-term prognosis and long-term survival. In this study, among the factors associated with survival in patients with solitary large HCCs, including previously reported factors28 such as AFP level, tumor size, PVTT and TACE treatment, ADC<1.32×10−3 mm2/s was the strongest independent factor. In addition, ROC analysis of postoperative OR predicted by preoperative ADC values indicated that patients with high preoperative ADC values had a higher OR than those with low preoperative ADC values.
Lower pretreatment ADC values for HCC usually indicate poor histological differentiation.29,30 In fact, Mannelli et al22 have demonstrated that the lower the ADC of an HCC tumor, the poorer the response to chemoembolization. In addition, Barat et al25 have reported that a low ADC one month after RFA is associated with early local recurrence of HCC. The results of this study are consistent with these findings, demonstrating that low ADC may be an imaging biomarker predictor of poor response to immediate combination therapy of chemoembolization and RFA for unresectable solitary large HCCs. This finding may be associated with the tumor microenvironmental characteristics of tumor interstitial pressure (TIP),14 which is a basic barrier to cancer treatment.31,32 The lower the ADC, the higher the TIP.14 By increasing tumor vascular resistance and decreasing the uptake and heterogeneous distribution of drugs, TIP reduces the targeting of tumor therapy, thus resulting in poor tumor response. In addition, the elevated interstitial pressure leads to hypoxia in the tumor, which can increase anaerobic metabolism and promote cancer metastasis through multiple modes, thus further increasing the therapeutic resistance.32
However, pretreatment ADC has not been consistent in predicting the response to locoregional therapies in HCC lesions. Several studies of conventional chemoembolization for HCC lesions have shown that tumors with low preoperative ADC are more likely to respond to conventional chemoembolization. Tumor lesions with lower ADC values have been hypothesized to have higher density of vascularization, thus making it a more desirable target for intra-arterial therapy for these tumors.20,23 In contrast, tumor lesions with higher ADC are often accompanied by necrotic areas indicative of relatively poorly perfusion, and the antitumor efficacy of chemotherapy drugs is diminished because of the low oxygen/acid environment.21 The results of this study are inconsistent with the above findings, possibly because previous studies performed TACE or DEB-TACE alone for patients with HCC. However, in the present study, we performed TACE immediately combined with RFA for patients with solitary large HCCs, and the immediate combination was found to enhance the synergistic effects of chemoembolization and thermal ablation, thereby resulting in a satisfactory prognosis that TACE alone did not achieve. On the one hand, lipiodol deposits in lesions coat and inactivate the surrounding tissues of the tumor; on the other hand, after the complete deposition of iodide oil, RFA can maximize the heat conduction effect of iodide oil, and the heat generated by RF needles can therefore be concentrated at the deposition site of iodide oil to exert maximum anti-tumor effects.10,11 Furthermore, RFA can compensate well for the poor postoperative embolization effect of TACE in the treatment of large HCC, especially in areas with poor blood supply, thus potentially leading to residual lesions and significantly enhancing the therapeutic effect. A low preoperative ADC may suggest more restricted diffusion and a higher number of cell tumors, or that the tumor is more malignant and has stronger aggressiveness, and thus that patients will have a relatively poorer response.
In previous studies, the threshold value of ADC that is predictive of better OR significantly varies. Niekamp et al33 have reported a threshold of 1.01×10−3 mm2/s, whereas Mannelli et al22 have reported 1.24×10−3 mm2/s as the cutoff value. However, in this study, ADC values higher than 1.32×10−3 mm2/s predicted OR at one month after chemoembolization immediately combined with RFA therapy, with a sensitivity of 63% and a specificity of 100%. The differences in the cutoff ADC values may be due to two reasons. On the one hand, owing to the degree of organizational differentiation, solitary large HCCs have been proposed and shown in previous studies to have similar pathologic characteristics to those of small HCC,3 with relatively good differentiation characteristics, and thus may have relatively higher ADC values than multiple nodular HCCs. On the other hand, the different absolute ADC values may depend on the imaging equipment, coil systems, the equipment manufacturer, and the field intensity used for MRI.
Our multivariate survival analysis of patients with solitary large HCC treated with TACE immediately combined with RFA showed that patients in the low ADC group had a significantly poorer PFS and OS than those in the high ADC group, and preoperative ADC was an independent risk factor for PFS and OS. The poorer prognosis of the low pretreatment ADC group supports the hypothesis that low pretreatment ADC of SLHCCs represent relatively poorly differentiated HCC. One study with a limited sample size (n=23) has found a significant linear regression relation between pre-TACE ADC and OS (γ=−0.698, P<0.001).23 Labeur et al24 have not found that pre-TACE ADC is associated with OS. However, the differences in methodology across studies should be taken into account in considering these discrepant results. The previous studies reported only a univariate association between preoperative ADC values and OS,23 whereas this study adopted a more robust multivariable analysis. Of note, 16 patients (17.9%) received TACE before operation in Labeur’s study.24 The inclusion of previously locoregionally treated patients in studies may have led to limited predictive power of pretreatment ADC values as a predictor of OS, owing to inherent treatment-related changes.
Several factors were associated with the survival of patients with SLHCC, such as tumor size, tumor stage, AFP level and vascular invasion.28 In this study focusing on SLHCCs treated with TACE immediately combined with RFA therapy, except for AFP level, no other factors were associated with survival in univariate and multivariate analyses. Vascular invasion has been identified as an independent predictor of survival in patients with HCC after chemoembolization.34 However, in this study, multivariate analysis showed no significant correlation between vascular invasion and patient survival (P>0.05), possibly because we treated patients with PV tumor thrombi with additional radiotherapy. In this study, additional focused radiotherapy was performed in 91.7% (11 of 12) patients with portal vein tumor thrombi. Furthermore, our sample size was small, thus preventing us from distinguishing the predictive value of tumor stage.
Our study has several limitations. First, because our study is a retrospective study, and there is indeed a certain degree of bias in patient selection such as tumor staging (BCLC staging) and consistency of treatment strategy. As a result, we cannot exclude the possibility that differences in patient tumor staging and follow-up treatment will affect the results of the study, and this will warrant validation in different subgroups in the further studies. Second, we were unable to provide definitive histopathologically relevant DWI report findings because only a small number of patients underwent biopsy, and a non-invasive imaging-based diagnosis is accepted by the European Association for the Study of the Liver (EASL) in cirrhotic patients. Third, the cutoff value of ADC based on the study cohort was generated by analyzing the ROC curve, and for the values to reach consensus, improvement and verification of internal and external patient cohorts are needed. Forth, we focused on the pretreatment ADC values in the maximum tumor diameter level of a single axial plane, with possible measurement bias. And the histogram analysis of ADC values in the entire intrahepatic tumor volume should be performed in further studies.
Conclusion
In conclusion, preoperative ADC values are significantly associated with OR, PFS and OS of patients with large solitary HCC treated with TACE immediately combined with RFA, and ADC is an independent predictive factor of PFS and OS. Diffusion weighted imaging as a substitute for tumor biological characteristics, such as cell density, cell invasiveness and TIP, has the potential to identify tumor treatment resistance mechanisms.
Ethics Approval
The study was approved by the Ethics Committee of the Chinese PLA General Hospital and the IRB waived the consent due to the retrospective nature of the study. All data were compiled in a Microsoft Excel spreadsheet, which was password protected to maintain patient confidentiality. Each subject was assigned a unique number in consecutive order, not derived from any patient identifiers. There was no disclosure of the Personal Health Information (PHI) and study was conducted in compliance with the Declaration of Helsinki.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by National Natural Science Foundation of China (No.81671800) Beijing Municipal Natural Science Foundation (No.7172204).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Villanueva A. Hepatocellular carcinoma. N Engl J Med. 2019;380:1450–1462. doi:10.1056/NEJMra1713263
2. Tsoulfas G, Mekras A, Agorastou P, et al. Surgical treatment for large hepatocellular carcinoma: does size matter? ANZ J Surg. 2012;82(7–8):510. doi:10.1111/j.1445-2197.2012.06079.x
3. Yang LY, Fang F, Ou DP, et al. Solitary large hepatocellular carcinoma: a specific subtype of hepatocellular carcinoma with good outcome after hepatic resection. Ann Surg. 2009;249(1):118–123. doi:10.1097/SLA.0b013e3181904988
4. European Association for the Study of the Liver. European Association for the Study of the L. EASL Clinical Practice Guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69:182–236. doi:10.1016/j.jhep.2018.03.019
5. Stevens CL, Awad A, Abbas SM, et al. Systematic review and meta-analysis of hepatic resection versus transarterial chemoembolization for solitary large hepatocellular carcinoma. HPB (Oxford). 2017;19:653–658. doi:10.1016/j.hpb.2017.03.009
6. Wang X, Hu Y, Ren M, et al. Efficacy and safety of radiofrequency ablation combined with transcatheter arterial chemoembolization for hepatocellular carcinomas compared with radiofrequency ablation alone: a time-to-event meta-analysis. Korean J Radiol. 2016;17:93–102. doi:10.3348/kjr.2016.17.1.93
7. Takaki H, Yamakado K, Uraki J, et al. Radiofrequency ablation combined with chemoembolization for the treatment of hepatocellular carcinomas larger than 5 cm. J Vasc Interv Radiol. 2009;20:217–224. doi:10.1016/j.jvir.2008.10.019
8. Yamakado K, Nakatsuka A, Ohmori S, et al. Radiofrequency ablation combined with chemoembolization in hepatocellular carcinoma: treatment response based on tumor size and morphology. J Vasc Interv Radiol. 2002;13:1225–1232. doi:10.1016/s1051-0443(07)61969-1
9. Iezzi R, Pompili M, La Torre MF, et al. Radiofrequency ablation plus drug-eluting beads transcatheter arterial chemoembolization for the treatment of single large hepatocellular carcinoma. Dig Liver Dis. 2015;47:242–248. doi:10.1016/j.dld.2014.12.007
10. Yuan H, Liu F, Li X, et al. Transcatheter arterial chemoembolization combined with simultaneous DynaCT-guided radiofrequency ablation in the treatment of solitary large hepatocellular carcinoma. Radiol Med. 2019;124:1–7. doi:10.1007/s11547-018-0932-1
11. Wang ZJ, Wang MQ, Duan F, et al. Transcatheter arterial chemoembolization followed by immediate radiofrequency ablation for large solitary hepatocellular carcinomas. World J Gastroenterol. 2013;19(26):4192–4199. doi:10.3748/wjg.v19.i26.4192
12. Yuan H, Liu F, Li X, et al. Angio-CT-guided transarterial chemoembolization immediately in combination with radiofrequency ablation for large hepatocellular carcinoma. Acad Radiol. 2019;26(2):224–231. doi:10.1016/j.acra.2018.04.007
13. Yan JY, Zhang JL, Wang MQ, et al. Combined transcatheter arterial chemoembolization and radiofrequency ablation in single-session for solitary hepatocellular carcinoma larger than 7 cm. Asia Pac J Clin Oncol. 2018;14(4):300–309. doi:10.1111/ajco.12817
14. Hompland T, Ellingsen C, Galappathi K, et al. DW-MRI in assessment of the hypoxic fraction, interstitial fluid pressure, and metastatic propensity of melanoma xenografts. BMC Cancer. 2014;14:92–100. doi:10.1186/1471-2407-14-92
15. Gluskin JS, Chegai F, Monti S, et al. Hepatocellular carcinoma and diffusion-weighted MRI: detection and evaluation of treatment response. J Cancer. 2016;7:1565–1570. doi:10.7150/jca.14582
16. Shenoy-Bhangle A, Baliyan V, Kordbacheh H, et al. Diffusion weighted magnetic resonance imaging of liver: principles, clinical applications and recent updates. World J Hepatol. 2017;9(26):1081–1091. doi:10.4254/wjh.v9.i26.1081
17. Vandecaveye V, Michielsen K, De Keyzer F, et al. Chemoembolization for hepatocellular carcinoma: 1-month response determined with apparent diffusion coefficient is an independent predictor of outcome. Radiology. 2014;270(3):747–757. doi:10.1148/radiol.13130591
18. Yuan Z, Li WT, Ye XD, et al. Utility of diffusion-weighted imaging to assess hepatocellular carcinoma viability following transarterial chemoembolization. Oncol Lett. 2014;8(2):831–836. doi:10.3892/ol.2014.2228
19. Wu L, Xu P, Rao S, et al. ADC total ratio and D ratio derived from intravoxel incoherent motion early after TACE are independent predictors for survival in hepatocellular carcinoma. J Magn Reson Imaging. 2017;46(3):820–830. doi:10.1002/jmri.25617
20. Kokabi N, Ludwig JM, Camacho JC, et al. Baseline and early MR apparent diffusion coefficient quantification as a predictor of response of unresectable hepatocellular carcinoma to doxorubicin drug-eluting bead chemoembolization. J Vasc Interv Radiol. 2015;26(12):1777–1786. doi:10.1016/j.jvir.2015.08.023
21. Yuan Z, Ye XD, Dong S, et al. Role of magnetic resonance diffusion-weighted imaging in evaluating response after chemoembolization of hepatocellular carcinoma. Eur J Radiol. 2010;75(1):e9–e14. doi:10.1016/j.ejrad.2009.05.040
22. Mannelli L, Kim S, Hajdu CH, et al. Serial diffusion-weighted MRI in patients with hepatocellular carcinoma: prediction and assessment of response to transarterial chemoembolization. Preliminary experience. Eur J Radiol. 2013;82(4):577–582. doi:10.1016/j.ejrad.2012.11.026
23. Dong S, Ye XD, Yuan Z, et al. Relationship of apparent diffusion coefficient to survival for patients with unresectable primary hepatocellular carcinoma after chemoembolization. Eur J Radiol. 2012;81(3):472–477. doi:10.1016/j.ejrad.2010.12.081
24. Labeur TA, Runge JH, Klompenhouwer EG, et al. Diffusion-weighted imaging of hepatocellular carcinoma before and after transarterial chemoembolization: role in survival prediction and response evaluation. Abdom Radiol. 2019;44:2740–2750. doi:10.1007/s00261-019-02030-2
25. Barat M, Fohlen A, Cassinotto C, et al. One-month apparent diffusion coefficient correlates with response to radiofrequency ablation of hepatocellular carcinoma. J Magn Reson Imaging. 2017;45:1648–1658. doi:10.1002/jmri.25521
26. Shao GL, Zheng JP, Guo LW, et al. Evaluation of efficacy of transcatheter arterial chemoembolization combined with computed tomography-guided radiofrequency ablation for hepatocellular carcinoma using magnetic resonance diffusion weighted imaging and computed tomography perfusion imaging: a prospective study. Medicine. 2017;96:e5518. doi:10.1097/MD.0000000000005518
27. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. doi:10.1016/j.ejca.2008.10.026
28. Liu PH, Su CW, Hsu CY, et al. Solitary large hepatocellular carcinoma: staging and treatment strategy. PLoS One. 2016;11:e0155588. doi:10.1371/journal.pone.0155588
29. Nakanishi M, Chuma M, Hige S, et al. Relationship between diffusion-weighted magnetic resonance imaging and histological tumor grading of hepatocellular carcinoma. Ann Surg Oncol. 2012;19(4):1302–1309. doi:10.1245/s10434-011-2066-8
30. Nishie A, Tajima T, Asayama Y, et al. Diagnostic performance of apparent diffusion coefficient for predicting histological grade of hepatocellular carcinoma. Eur J Radiol. 2011;80(2):e29–e33. doi:10.1016/j.ejrad.2010.06.019
31. Sheth RA, Hesketh R, Kong DS, et al. Barriers to drug delivery in interventional oncology. J Vasc Interv Radiol. 2013;24:1201–1207. doi:10.1016/j.jvir.2013.03.034
32. Ariffin AB, Forde PF, Jahangeer S, et al. Releasing pressure in tumors: what do we know so far and where do we go from here? A review. Cancer Res. 2014;74:2655–2662. doi:10.1158/0008-5472.CAN-13-3696
33. Niekamp A, Abdel-Wahab R, Kuban J, et al. Baseline apparent diffusion coefficient as a predictor of response to liver-directed therapies in hepatocellular carcinoma. J Clin Med. 2018;7:83. doi:10.3390/jcm7040083
34. Hu HT, Kim JH, Lee LS, et al. Chemoembolization for hepatocellular carcinoma: multivariate analysis of predicting factors for tumor response and survival in a 362-patient cohort. J Vasc Interv Radiol. 2011;22:917–923. doi:10.1016/j.jvir.2011.03.005
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.