Back to Journals » Drug Design, Development and Therapy » Volume 18
Prescribing Trends of Fixed-Dose Combination Antibiotics Not Recommended by the WHO (FNRs) for ICU Patients in Six Major Areas of China During a Seven-Year Period
Authors Zhou L, Zhao Y, Zhu J ![]() , Liu J
, Liu J ![]() , Liang G, Yang Y, Han G, Yu Z
, Liang G, Yang Y, Han G, Yu Z ![]()
Received 31 August 2024
Accepted for publication 23 November 2024
Published 6 December 2024 Volume 2024:18 Pages 5781—5791
DOI https://doi.org/10.2147/DDDT.S493980
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Liujun Zhou,1,* Yuhua Zhao,1,2,* Jianping Zhu,1 Jieqiong Liu,1 Gang Liang,1 Yi Yang,1 Gang Han,1 Zhenwei Yu1
1Department of Pharmacy, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, People’s Republic of China; 2Department of Pharmacy, Affiliated Xiaoshan Hospital, Hangzhou Normal University, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Gang Han; Zhenwei Yu, Email [email protected]; [email protected]
Objective: To evaluate the prescribing trends of fixed-dose combination antibiotics not recommended by the WHO (FNRs) for intensive care unit (ICU) patients in six major areas of China from 2013 to 2019.
Methods: A descriptive analysis was conducted using the pharmacy prescription data. Prescription data for patients admitted to the ICU were extracted from the Hospital Prescription Analysis Cooperative Project. Trends in FNR use were analyzed over a seven-year period, and the trends were further analyzed at the specific drug and hospital levels.
Results: A total of 15,596,620 prescriptions were eligible for analysis, and 1,492,793 patients were included. Among these patients, 91,515 (6.13%) received FNRs. The annual number of ICU patients who received FNR showed an increasing trend (P=0.007), but the percentage per year did not (P=0.764). The FNR use was usually higher in male patients than in female patients (P< 0.001). Patients aged > 60 years had the highest percentage of patients who received FNRs (P< 0.001). Among the eight FNRs identified in this study, cefoperazone/sulbactam was the most commonly used FNR in both patient numbers and prescribed hospitals, followed by piperacillin/sulbactam. The use of cefotaxime/sulbactam was less common but showed an increasing trend. There were significant differences among the regions.
Conclusion: This study investigated the national landscape of FNR use among ICU patients. Attention should be given to the frequent use of FNRs in these patients. Data on the real-world effectiveness and safety of FNRs are urgently required.
Keywords: antibiotic use, fixed-dose combination, irrational, prescription, cefoperazone, sulbactam
Introduction
Antibiotics play a pivotal role in combating infectious diseases, necessitating their rational use. Severe infections are prevalent in patients admitted to intensive care units (ICUs), and antibiotics are commonly administered to these patients.1 The rational use of antibiotics is paramount for preserving drug efficacy, minimizing adverse effects, conserving medical resources, and safeguarding the health of patients.2–5 Conversely, inappropriate use of antibiotics has led to decreased effectiveness, emergence of drug-resistant bacteria, and increased costs.6,7 Therefore, rational use of antibiotics is crucial for ICU infection management.2,8,9
Among all antibiotics, fixed-dose combination antibiotics (FDCAs) have become increasingly widespread.10–12 These drugs combine multiple active ingredients in a fixed ratio to improve treatment convenience, compliance, and potential synergistic effects.13,14 However, pharmacokinetic mismatches, insufficient evidence-based support, individual differences and regulatory and compliance issues may render certain FDCAs inappropriate for use in specific clinical scenarios.3,15 The WHO listed 103 combinations of FDCAs not recommended (FNR) in the 2021 AWaRe classification. These FNRs are not evidence-based or recommended by international guidelines, and concerns are raised about their efficacy, safety and emergence of antimicrobial resistance (AMR).10,16–18 Despite these potential disadvantages, multiple FNRs have been approved and widely used in various countries, including China.16,19 There is little data regarding the use of FNR in ICU patients, which is important for antimicrobial stewardship. This study aimed to provide national data on FNR use in ICU patients for a seven-year period utilizing a comprehensive prescription database, and the results will be helpful for clinical practice, pharmacovigilance, and regulation.
Methods
Study Design
This study was designed as a retrospective descriptive study based on prescription data. Ethical approval was obtained from the Ethics Committee of Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University (Reference Number KEYAN2023-0209). The requirement for informed consent was waived as part of the study. The patients’ personal information was confidential to the researchers, and the study was conducted in compliance with the Declaration of Helsinki.
Data Source
Prescription data were extracted from the database of the Hospital Prescription Analysis Cooperative Project in China. The database contains prescription information of participating hospitals on 40 randomized days per year, and has been widely used in Chinese pharmacoepidemiology studies.20–25
In this study, prescription data from 66 hospitals in Beijing, Hangzhou, Chengdu, Guangzhou, Shanghai, and Tianjin were selected because these hospitals participated in the program continuously from 2013 to 2019 and were located in the north, west, south, and east, thus covering a wide area of China. Brief hospital information is shown in Table S1.
Prescription Inclusion and Data Extraction
Prescriptions meeting the following criteria were included in the analysis: (1) prescriptions written during 2013 and 2019, (2) prescriptions from the aforementioned hospitals, and (3) prescriptions written for patients admitted to the ICU. The following information about prescriptions was extracted: patient code, sex, age, date, location, diagnosis, and the generic name and price of antibiotics. Prescriptions with missing data were excluded. Patient codes were reorganized in the dataset so that individual participants could not be identified. The study was conducted between October 2023 and January 2024.
Analysis
The main results were the yearly proportion of patients who received FNRs and their trends. Any drug within the FDCAs not recommended by the WHO was defined as an FNRs. The yearly number of ICU patients was calculated using the patient code in the extracted prescriptions, and the yearly number of patients who received FNR was calculated by counting the number of patients who had at least one FNR prescription. The characteristics of the patients who received FNRs are descriptively presented. The proportion of patients receiving FNRs each year was calculated using the following equation, and the overall trends of FNR use were described for the 7-year observation period: trends in FNR use according to sex, region, and specific FNR were evaluated.

Subgroup analyses by age, sex, specific drugs and geographical religion were conducted. Four age groups were set to determine whether the trends in FNR use were driven by a particular age group. The four age groups were children and adolescents (2–17 years), young adults (18–45 years), middle-aged adults (46–59 years), and older adults (60 years and older).
The data were processed using Access software (Microsoft, Redmond, WA, United States). The chi-square test was used to compare patients in males vs females in each year, and the Mann–Kendall trend test was used to assess trends in prescribed drugs. A log-linear test was used to assess trends in proportions. All the statistical analyses were carried out using R V4.0.5 software. Statistical significance was set at a P value < 0.05.
Results
Characteristics and Overall Trends of FNR of Included Prescriptions
A total of 15596620 prescriptions were eligible for analysis, and 1492793 patients were included. Among these patients, 91515 (6.13%) received FNRs. As shown in Figure 1, the yearly number of ICU patients who received FNRs showed an increasing trend (P=0.007), while the percentage of these patients did not show a significant trend over 7 years (P=0.764). The demographic characteristics of the patients and those who received FNR treatment are shown in Table 1. The number of male patients was usually greater than that of female patients (chi-square test, P<0.001). Patients aged > 60 years had the highest percentage of patients who received FNRs (chi-square test, P<0.001). However, the proportion of FNR users among patients aged 18–45 years increased during the study period (P= 0.035).
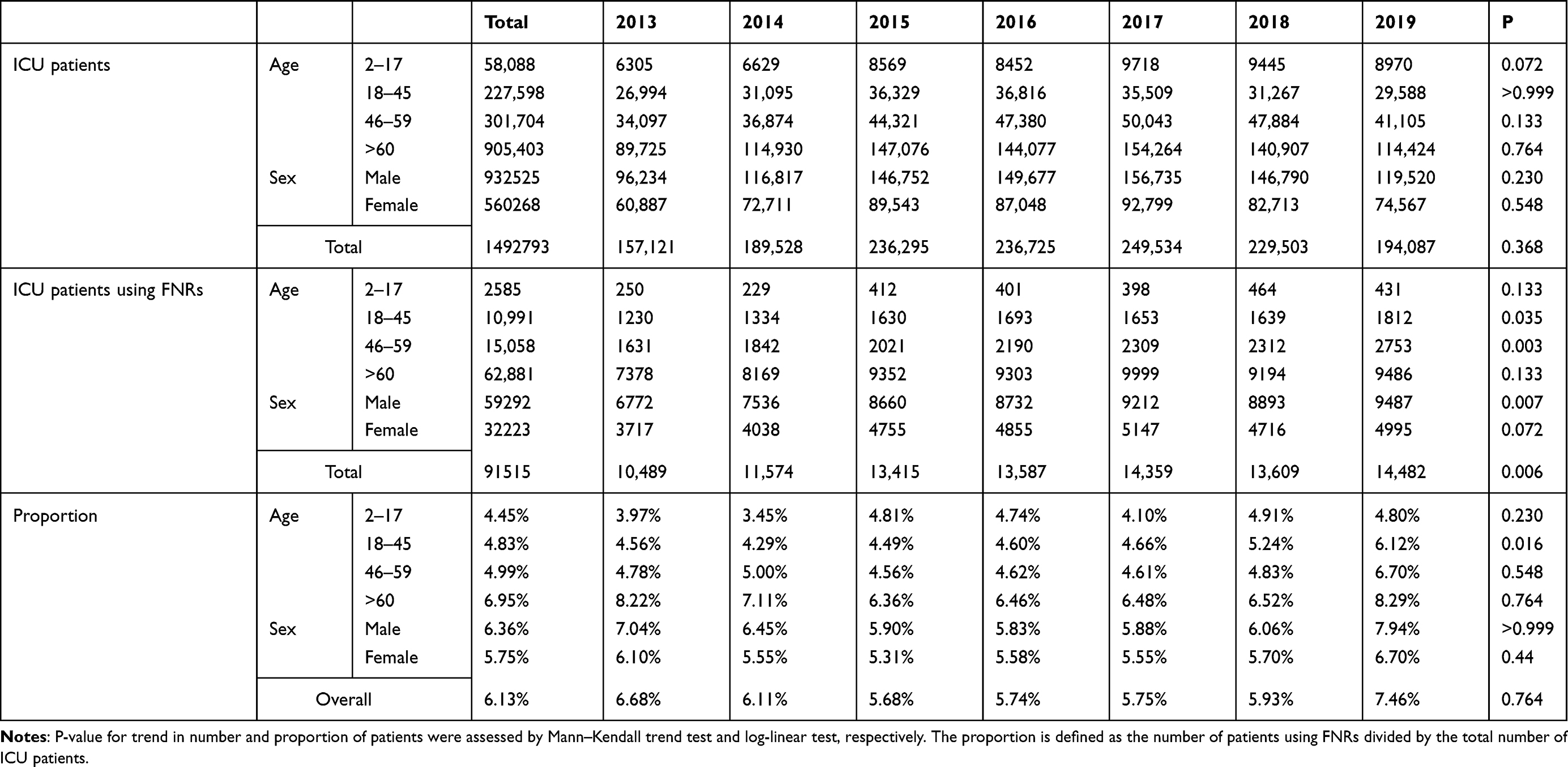 |
Table 1 Demographic Characteristics of Included Patients from 2013 to 2019 |
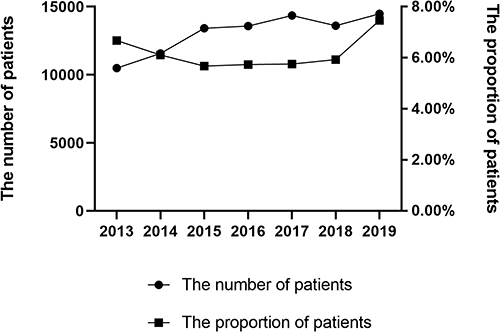 |
Figure 1 Trends in the yearly number and proportion of patients using FNRs. |
Trends in Specific Drugs
Eight FNRs were identified in the present study, seven of which were compound preparations of β-lactams and enzyme inhibitors. The prescription trends for each FNR were analyzed. As shown in Figure 2, the use of cefoperazone/sulbactam ranked first, followed by piperacillin/sulbactam, cefoperazone/tazobactam, mezlocillin/sulbactam, cefotaxime/sulbactam, ceftriaxone/tazobactam, and amoxicillin/sulbactam. Detailed data regarding the total amount of each medication used and the proportion of ICU patients using the medication are shown in Table 2. The use of cefoperazone/sulbactam and mezlocillin/sulbactam significantly increased prescription volume (both P <0.05). Concurrently, a notable decrease was observed in the proportion of piperacillin/sulbactam users (P=0.07), whereas a substantial increase in the proportion of cefotaxime/sulbactam users was detected (P=0.048).
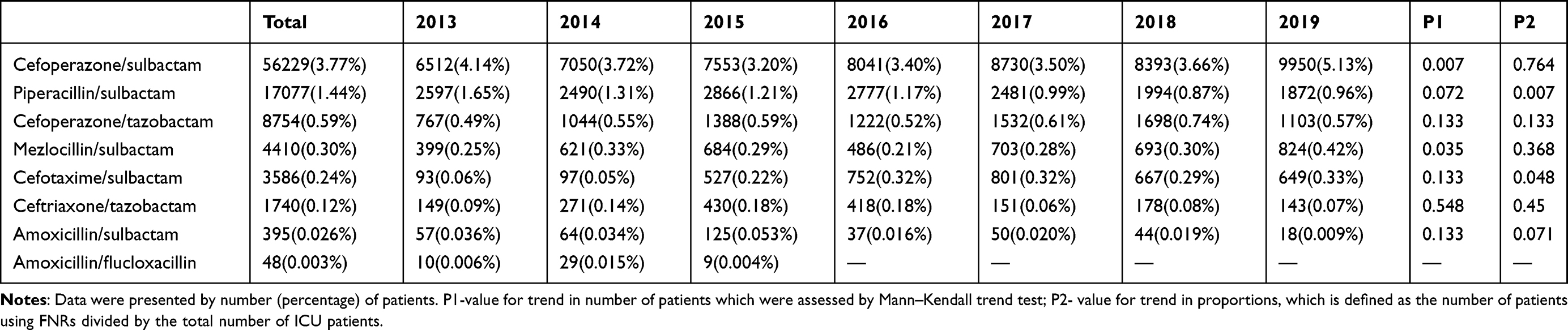 |
Table 2 Number of ICU Patients with a Specific FNR from 2013 to 2019 |
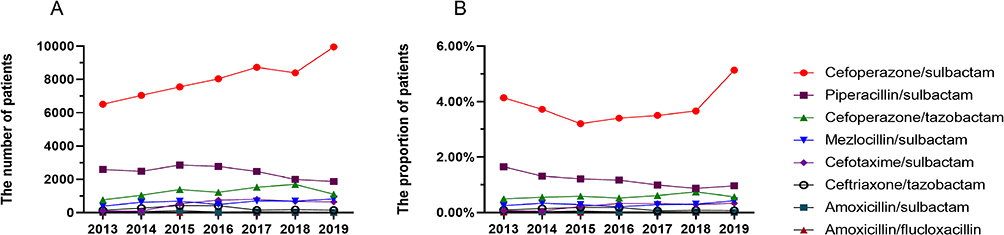 |
Figure 2 Trends in use of each FNR. (A) The number of patients. (B) The usage proportion trends by drug. |
Table 3 shows the number and proportion of hospitals providing each FNR. Cefoperazone/sulbactam is the most widely used treatment, followed by piperacillin/sulbactam. Other FNRs were prescribed in fewer than 30% of the hospitals, while cefotaxime/sulbactam showed an increasing trend (P=0.011).
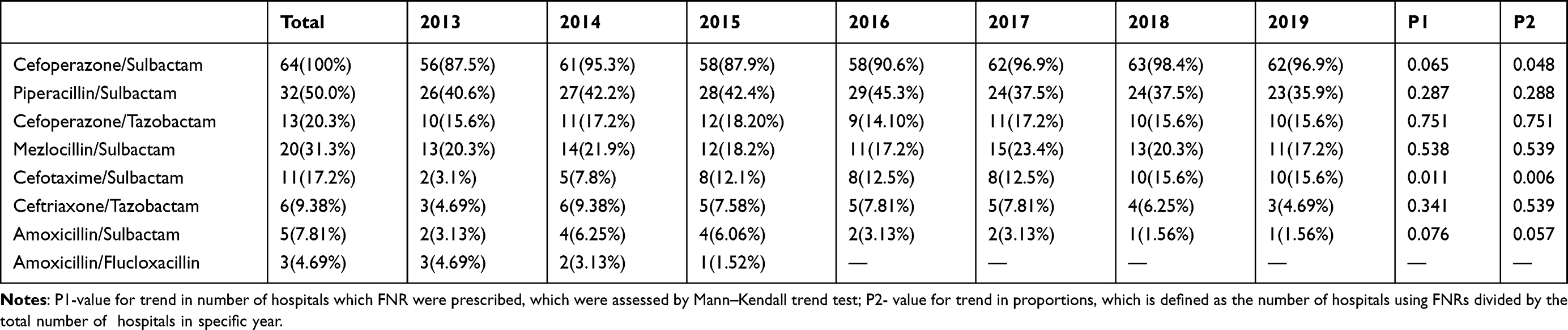 |
Table 3 Number and Proportion of Hospitals Providing Specific FNR from 2013 to 2019 |
Trends by Geographical Religions
The prescription trends of FNR were further analyzed according to different geographical regions. As shown in Table 4 and Table S2, significant differences exist among the regions. The proportion of patients receiving FNR was greater in Guangzhou (17.2%, chi-square test, P<0.001), while the proportions in Hangzhou and Chengdu were lower (3.82% and 3.83%, chi-square test, P<0.001). The number of patients receiving FNRs increased in three regions (Hangzhou, Tianjin, and Guangzhou) (all P<0.05), which calls for special attention.
 |
Table 4 Trends in FNR Use by Geographical Regions from 2013 to 2019 |
Discussion
To our knowledge, this study is the first to analyze trends in the use of FNR over time at the national level using surveillance data. As the sample was large and covered six areas of China, the results are nationally representative. More than 6% of ICU patients have used FNR, and this proportion has been increasing in general (7.46% in 2019). The proportion of elderly patients using FNR was always greater than the average. Eight FNRs were identified in this study. Cefoperazone/sulbactam and piperacillin/sulbactam are frequently and widely used. The use of cefotaxime/sulbactam has also increased.
Currently, there are limited data available on the use of FNRs at the national level. The available information primarily pertains to the consumption of FDC antibiotics, and only a few literature reports mention the use of specific FNR.10,26–30 According to a previous report that analyzed antibiotic usage in 76 countries from 2000 to 2015, FNR antibiotics were employed in 20 (26.3%) countries.29 The contribution of FNR use to overall antibiotic consumption was less than 3%. However, the usage of specific countries, such as Egypt, India, and Pakistan, were significantly higher, at 9.6%, 7.5%, and 4.0%, respectively.29 Another study had reviewed global antibiotic sales data and identified 119 FDC antibiotics. The majority (92%) of these FDCs were not approved by the FDA and comprised 5.1% of total sales. China had the second highest FDC count (25/119). Although only 8 FNRs were identified in this study, more than 6% of the ICU patients had received FNR. This percentage was high compared with existed reports. Thus, special attention should be given to the better management of FNRs.
Cefoperazone/sulbactam was the most frequently used FNR in this study, as it has shown good clinical effectiveness and is recommended as a first-line empirical antibiotic in multiple anti-infection guidelines in China.31 A meta-analysis of 110 studies on the effectiveness and cure rate of cefoperazone/sulbactam showed that the effectiveness rate of cefoperazone/sulbactam was 80.3%, and the cure rate was 50.1% for the treatment of clinical infections.32 An in vitro study showed that the addition of sulbactam to cefoperazone could enhance the antibacterial activity of cefoperazone against carbapenem-resistant Acinetobacter baumannii but had no effect on carbapenem-resistant Pseudomonas aeruginosa.33 A literature review showed that if the combination of cefoperazone/sulbactam could achieve pharmacokinetic optimization in human serum, its clinical application could be expanded.34 The major concern regarding cefoperazone/sulbactam is its potential relationship with coagulopathy and bleeding events, but recent studies have shown that the risk is acceptable.35,36 Therefore, it is necessary to obtain more convincing data to support or discourage the use of cefoperazone/sulbactam.
Piperacillin/sulbactam, the second most frequently used FNR, has successfully addressed the issues of high chemical cost and frequent penicillin allergic reactions associated with piperacillin/tazobactam by replacing tazobactam with sulbactam. According to an in vitro experiment,37 the antibacterial activities of the two are similar for gram-positive bacteria. However, for gram-negative bacteria, especially Escherichia coli and Proteus vulgaris, the antibacterial activity of piperacillin/sulbactam was significantly higher than that of piperacillin/tazobactam. The antibacterial effects of other Enterobacteriaceae and Pseudomonas aeruginosa strains were comparable. Notably, for Stenotrophomonas maltophilia, the activity of piperacillin/sulbactam was greater. A randomized, single-blind, controlled clinical trial in China showed that piperacillin/sulbactam can be used as a suitable substitute for piperacillin/tazobactam for the treatment of community-acquired respiratory and urinary tract infections caused by β-lactamase-producing bacteria.38 In vitro experiments further confirmed that the addition of sulbactam to piperacillin improved the sensitivity of Pseudomonas aeruginosa and Acinetobacter baumannii to piperacillin.39
There are only some in vitro studies but little high-quality evidence-based medical evidence for cefoperazone/tazobactam, mezlocillin/sulbactam, cefotaxime/sulbactam, amoxicillin/sulbactam and amoxicillin/flucloxacillin.27,40,41
For drugs that are widely used in clinical settings and demonstrate clear therapeutic benefits, large-scale randomized controlled trials can be conducted to provide higher-level evidence of their efficacy and safety. This will enable a more comprehensive evaluation of drug effectiveness and safety, thereby providing doctors and patients with accurate information. For FNR, which has been proven to have no better clinical efficacy, standardized management systems should be established. These include developing guidelines for their use, limiting unnecessary utilization, promoting safer and more effective drug alternatives, and other measures. Additionally, healthcare facilities should strengthen supervision and management to ensure effective control of FNR.
This study had several limitations. First, our analysis relied solely on prescription data, thereby rendering an evaluation of the adequacy of antimicrobial therapy as well as its outcomes infeasible. Additionally, there is a dearth of data pertaining to indications for prescribing antimicrobials, a subject that merits further exploration in subsequent research.
Conclusion
This study investigated the national landscape of FNR use among ICU patients in China. The overall FNR use in these patients was > 6%, which calls for special attention to rational use and better management. Among the eight FNRs identified in this study, cefoperazone/sulbactam and piperacillin/sulbactam were the most frequently used and widely distributed. Data on the real-world effectiveness and safety of these FNRs are urgently required to support or discourage their use.
Data Sharing Statement
The original contributions presented in this study are included in the article/supplementary material, and further inquiries can be directed to the corresponding authors.
Ethics Approval
Studies involving human participants were reviewed and approved by the Ethics Committee of Sir Run Run Shaw Hospital, College of Medicine, Zhejiang University (Reference Number KEYAN2023-0209). Written informed consent for participation was not required for this study, in accordance with national legislation and institutional requirements.
Acknowledgments
The authors would like to thank the Hospital Prescription Analysis Cooperative Project of China for collecting and providing data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Zhejiang Medical Doctors Association (YS2022-2-002).
Disclosure
No potential competing interest was reported by the authors.
References
1. Mokrani D, Chommeloux J, Pineton de Chambrun M, Hékimian G, Luyt CE. Antibiotic stewardship in the ICU: time to shift into overdrive. Ann Intensive Care. 2023;13(1):39. doi:10.1186/s13613-023-01134-9
2. Timsit JF, Bassetti M, Cremer O, et al. Rationalizing antimicrobial therapy in the ICU: a narrative review. Intensive Care Med. 2019;45(2):172–189. doi:10.1007/s00134-019-05520-5
3. Uddin TM, Chakraborty AJ, Khusro A, et al. Antibiotic resistance in microbes: history, mechanisms, therapeutic strategies and future prospects. J Infect Public Health. 2021;14(12):1750–1766. doi:10.1016/j.jiph.2021.10.020
4. Baran A, Kwiatkowska A, Potocki L. Antibiotics and bacterial resistance-A short story of an endless arms race. Int J Mol Sci. 2023;24(6):5777. doi:10.3390/ijms24065777
5. Principe L, Lupia T, Andriani L, et al. Microbiological, clinical, and PK/PD features of the new anti-gram-negative antibiotics: β-lactam/β-lactamase inhibitors in combination and cefiderocol-an all-inclusive guide for clinicians. Pharmaceuticals. 2022;15(4):463. doi:10.3390/ph15040463
6. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
7. Hariyanto H, Yahya CQ, Cucunawangsih C, Pertiwi CLP. Antimicrobial resistance and mortality. Afr J Infect Dis. 2022;16(2):13–20. doi:10.21010/Ajid.v16i2.2
8. Liu J, Zhang S, Huang S, et al. Rationality of time-dependent antimicrobial use in Intensive Care Units in China: a nationwide cross-sectional survey. Front Med Lausanne. 2021;8:584813. doi:10.3389/fmed.2021.584813
9. Abdelkarim OA, Abubakar U, Taha LO, et al. Impact of irrational use of antibiotics among Patients in the Intensive Care Unit on clinical outcomes in Sudan. Infect Drug Resist. 2023;16:7209–7217. doi:10.2147/IDR.S378645
10. Wushouer H, Hu L, Zhou Y, et al. Trends of fixed-dose combination antibiotic consumption in hospitals in China: analysis of data from the center for antibacterial surveillance, 2013–2019. Antibiotics. 2022;11(7):957. doi:10.3390/antibiotics11070957
11. Anand P, Kaur N, Verma V, Shafiq N, Malhotra S. Assessment of rationality of available fixed dose combinations of antibiotics in India. Expert Rev Anti Infect Ther. 2022;20(5):797–808. doi:10.1080/14787210.2022.2015324
12. Brhlikova P, Mehta A, McGettigan P, Pollock AM, Roderick P, Farooqui HH. Regulatory enforcement of the marketing of fixed-dose combinations in India: a case study of systemic antibiotics. J Pharm Policy Pract. 2023;16(1):139. doi:10.1186/s40545-023-00644-y
13. Duda-Madej A, Viscardi S, Topola E. Meropenem/vaborbactam: β-lactam/β-lactamase inhibitor combination, the future in eradicating multidrug resistance. Antibiotics. 2023;12(11):1612. doi:10.3390/antibiotics12111612
14. Coates ARM, Hu Y, Holt J, Yeh P. Antibiotic combination therapy against resistant bacterial infections: synergy, rejuvenation and resistance reduction. Expert Rev Anti Infect Ther. 2020;18(1):5–15. doi:10.1080/14787210.2020.1705155
15. Tyers M, Wright GD. Drug combinations: a strategy to extend the life of antibiotics in the 21st century. Nat Rev Microbiol. 2019;17(3):141–155. doi:10.1038/s41579-018-0141-x
16. Bortone B, Jackson C, Hsia Y, Bielicki J, Magrini N, Sharland M. High global consumption of potentially inappropriate fixed dose combination antibiotics: analysis of data from 75 countries. PLoS One. 2021;16(1):e0241899. doi:10.1371/journal.pone.0241899
17. Vliegenthart-Jongbloed K, Jacobs J. Not recommended fixed-dose antibiotic combinations in low- and middle-income countries - The example of Tanzania. Antimicrob Resist Infect Control. 2023;12(1):37. doi:10.1186/s13756-023-01238-8
18. de la Fuente-Nunez C, Cesaro A, Hancock REW. Antibiotic failure: beyond antimicrobial resistance. Drug Resist Updat. 2023;71:101012. doi:10.1016/j.drup.2023.101012
19. Guan X, Tian Y, Song J, Zhu D, Shi L. Effect of physicians’ knowledge on antibiotics rational use in China’s county hospitals. Soc Sci Med. 2019;224:149–155. doi:10.1016/j.socscimed.2019.01.049
20. Yu Z, Zhang J, Zheng Y, Yu L. Trends in antidepressant use and expenditure in six major cities in China from 2013 to 2018. Front Psychiatry. 2020;11:551. doi:10.3389/fpsyt.2020.00551
21. Yu L, Ding K, Luo L, Yu Z. Prescribing trends of glaucoma drugs in six major cities of China from 2013 to 2017. PLoS One. 2020;15(1):e0227595. doi:10.1371/journal.pone.0227595
22. Yu L, Chen X, Yu Z, Yu L, Chen X, Yu Z. Trends of antidementia drugs use in outpatients with Alzheimer’s disease in six major cities of China: 2012–2017. Int Clin Psychopharmacol. 2019;34(6):312–316. doi:10.1097/YIC.0000000000000278
23. Han G, Han Y, Yu L, Zhao Y, Yu Z. Patterns and trends in pharmacological treatment for outpatients with postherpetic neuralgia in six major areas of China, 2015–2019. Healthcare. 2023;11(5):764. doi:10.3390/healthcare11050764
24. Yu Z, Zhao Y, Jin J, Zhu J, Yu L, Han G. Antiviral treatment in outpatients with herps zoster in six major areas of China, 2010–2019. Front Public Health. 2022;10:942377. doi:10.3389/fpubh.2022.942377
25. Yu Z, Zhu J, Jin J, Yu L, Han G. Trends in outpatient prescribing patterns for ocular topical anti-infectives in six major areas of China, 2013–2019. Antibiotics. 2021;10(8):916. doi:10.3390/antibiotics10080916
26. McGettigan P, Roderick P, Kadam A, Pollock A. Threats to global antimicrobial resistance control: centrally approved and unapproved antibiotic formulations sold in India. Br J Clin Pharmacol. 2019;85(1):59–70. doi:10.1111/bcp.13503
27. Batool S, Almaghaslah D, Alqahtani A, et al. Aetiology and antimicrobial susceptibility pattern of bacterial isolates in community acquired pneumonia patients at Asir region, Saudi Arabia. Int J Clin Pract. 2021;75(2):e13667. doi:10.1111/ijcp.13667
28. Sayer B, Bortone B, Sharland M, Hsia Y. Fixed-dose combination antibiotics: the search for evidence using the example of ampicillin-cloxacillin. Br J Clin Pharmacol. 2021;87(7):2996–2999. doi:10.1111/bcp.14711
29. Klein EY, Milkowska-Shibata M, Tseng KK, et al. Assessment of WHO antibiotic consumption and access targets in 76 countries, 2000–15: an analysis of pharmaceutical sales data. Lancet Infect Dis. 2021;21(1):107–115. doi:10.1016/S1473-3099(20)30332-7
30. Koya SF, Ganesh S, Selvaraj S, Wirtz VJ, Galea S, Rockers PC. Consumption of systemic antibiotics in India in 2019. Lancet Reg Health Southeast Asia. 2022;4:100025. doi:10.1016/j.lansea.2022.100025
31. Pulmonary Infection Assembly of Chinese Thoracic Society. Chinese expert consensus on the management of lower respiratory tract infections of Pseudomonas aeruginosa in adults (2022). Zhonghua Jie He He Hu Xi Za Zhi. 2022;45(8):739–752. doi:10.3760/cma.j.cn112147-20220407-00290.
32. Lan SH, Chao CM, Chang SP, Lu LC, Lai CC. Clinical efficacy and safety of cefoperazone-sulbactam in treatment of intra-abdominal infections: a systematic review and meta-analysis. Surg Infect (Larchmt). 2021;22(8):763–770. doi:10.1089/sur.2020.468
33. Lai CC, Chen CC, Lu YC, Chuang YC, Tang HJ. In vitro activity of cefoperazone and cefoperazone-sulbactam against carbapenem-resistant Acinetobacter baumannii and Pseudomonas aeruginosa. Infect Drug Resist. 2018;12:25–29. doi:10.2147/IDR.S181201
34. Ku YH, Yu WL. Cefoperazone/sulbactam: new composites against multiresistant gram negative bacteria. Infect Genet Evol. 2021;88:104707. doi:10.1016/j.meegid.2021.104707
35. Wang W, Liu Y, Yu C, et al. Cefoperazone-sulbactam and risk of coagulation disorders or bleeding: a retrospective cohort study. Expert Opin Drug Saf. 2020;19(3):339–347. doi:10.1080/14740338.2020.1713090
36. Miao W, Guo J, Cheng H, Zhao Q. Risk factors for cefoperazone/sulbactam-induced coagulation disorder. Infect Drug Resist. 2023;16:6277–6284. doi:10.2147/IDR.S429706
37. Frank U, Mutter J, Schmidt-Eisenlohr E, Daschner FD. Comparative in vitro activity of piperacillin, piperacillin-sulbactam and piperacillin-tazobactam against nosocomial pathogens isolated from intensive care patients. Clin Microbiol Infect. 2003;9(11):1128–1132. doi:10.1046/j.1469-0691.2003.00786.x
38. Zhiyong Z, Xiaoju L, Yanbin L, et al. Piperacillin-sulbactam versus piperacillin-tazobactam: a multicentre, randomised, single-blind, controlled clinical trial. Int J Antimicrob Agents. 2005;26(1):22–27. doi:10.1016/j.ijantimicag.2005.02.018
39. Hung MN, Hsueh PR, Chang HT, et al. In vitro activities of various piperacillin and sulbactam combinations against bacterial pathogens isolated from Intensive Care Units in Taiwan: SMART 2004 programme data. Int J Antimicrob Agents. 2007;29(2):145–152. doi:10.1016/j.ijantimicag.2006.02.017
40. Aabed K, Moubayed N, Alzahrani S. Antimicrobial resistance patterns among different Escherichia coli isolates in the Kingdom of Saudi Arabia. Saudi J Biol Sci. 2021;28(7):3776–3782. doi:10.1016/j.sjbs.2021.03.047
41. Sanghavi S, Ghoshal U, Poddar S, et al. In vitro susceptibility of clinical isolates to ceftriaxone alone and ceftriaxone in combination with sulbactam or tazobactam: a comparative study of broad-spectrum β-lactam antibiotics in India. Cureus. 2023;15(9):e46014. doi:10.7759/cureus.46014
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.