Back to Journals » International Journal of General Medicine » Volume 14
Preprocedural Ticagrelor Treatment was Associated with Improved Early Reperfusion and Reduced Short-term Heart Failure in East-Asian ST-segment Elevation Myocardial Infarction Patients Undergoing Primary Percutaneous Coronary Intervention
Authors Zhang Y, Hui J, Chen X
Received 24 February 2021
Accepted for publication 27 April 2021
Published 18 May 2021 Volume 2021:14 Pages 1927—1938
DOI https://doi.org/10.2147/IJGM.S307404
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yunke Zhang,1,2 Jie Hui,1 Xia Chen2
1Department of Cardiology, The First Affiliated Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China; 2Department of Cardiology, Shanghai University of Medicine and Health Sciences Affiliated Jiading Central Hospital, Shanghai, 201800, People’s Republic of China
Correspondence: Jie Hui
Department of Cardiology, The First Affiliated Hospital of Soochow University, 889 Pinghai Road, Suzhou, Jiangsu, People’s Republic of China
Tel +86-0512-65223637
Email [email protected]
Purpose: The purpose of this monocentric retrospective observational study is to investigate whether a loading dose of ticagrelor treatment before percutaneous coronary intervention (PCI) procedure improves the early reperfusion and short-term heart function in East-Asian ST segment elevation myocardial infarction (STEMI) patients.
Patients and Methods: The study included 326 STEMI patients undergoing primary PCI in Jiading Central Hospital. One hundred and forty patients received a loading dose of ticagrelor before entering the catheter laboratory. One hundred and eighty-six patients received a loading dose of ticagrelor in the catheter laboratory before the initiation of PCI. Reperfusion endpoints included the presence of self-patency in the culprit artery, the ST-segment elevation resolution over 50% within 24 h after PCI, and the presence of no-reflow in the culprit artery. Clinical endpoints included all-cause mortality, new-onset heart failure, reinfarction and stent thrombosis within 28 days after PCI. Secondary clinical endpoints included mechanical complications and bleeding events.
Results: In comparison with the in-lab treatment group, the preprocedural treatment group had a significant higher proportion of self-patency in the culprit artery (25.71% vs 16.67%, P=0.045) and early ST-segment elevation resolution (48.57% vs 27.96%, P< 0.001). Preprocedural ticagrelor treatment was associated with a significant reduction of new-onset heart failure (9.29% vs 18.82%, p=0.016). Stent thrombosis risks were numerically reduced in the preprocedural treatment group (0.71% vs 1.61%, P=0.466). The rates of major cardiovascular adverse events, reinfarctions and mortality did not differ between the two groups. Bleeding events in the preprocedural treatment group was notn significantly higher than the in-lab treatment group (4.39% vs 1.39%, P=0.142).
Conclusion: Preprocedural administration of a loading dose of ticagrelor was associated with improved early reperfusion and reduced short-term heart failure in East-Asian STEMI patients undergoing primary PCI, but care should be taken for excess bleeding events.
Keywords: antiplatelet therapy, P2Y12 receptor inhibitors, prehospital management, coronary catheterization
Introduction
The most important treatment for patients with ST-segment elevation myocardial infarction (STEMI) is the early recovery of the infarct-related artery blood flow.1–4 Enhanced platelet activity contributes a lot to the highly prothrombotic state during the early stage of STEMI onset, so that an effective early antiplatelet treatment is crucial in the preprocedural management of the STEMI patients undergoing primary percutaneous coronary intervention (PPCI). Prehospital administration of intravenous platelet glycoprotein (GP) IIb/IIIa inhibitors is associated with better and earlier reperfusion,5,6 but its actual use is very limited.7 As an easier prehospital option, early administration of P2Y12 inhibitors at the prehospital stage is concerned in recent years.
Current guidelines1,2 recommended using P2Y12 inhibitors as soon as possible after the diagnosis of STEMI, but the clinical benefit of the upstream antiplatelet therapy was debated. In recent years, two large clinical studies were unfavorable to the early ticagrelor pretreatment before primary PCI, as the antiplatelet pretreatment did not improve the early reperfusion of the culprit arteries8 or the clinical outcomes within 30 days after PCI procedure.9 However, some researchers questioned the principal role of ticagrelor as a merely reperfusion supporting agent. Distal embolization of thrombus during the precatheterization setting was reported to be associated with reduced flow in the infarction-related artery, an increased infarct size and reduced recovery of ventricular function.3,4 The effects of upstream ticagrelor administration in reducing risk of heart failure, however, remained unclear so far.
Furthermore, both of the previous studies were conducted in European countries. Previous studies indicated that the East-Asian populations that present with ACS or undergo PCI display a dissimilar platelet reactivity following PCI or ACS compared with the European population, which presented with a similar or lower rate of ischemic events after PCI procedure, in spite of a higher level of platelet reactivity during P2Y12 inhibitor treatment.10 This phenomenon suggested that East-Asian specific evidence should be taken into consideration to adopt the Western P2Y12 inhibitor treatment strategies to the regional guidelines for East-Asian patients with STEMI. Data from clinical studies on this matter was very limited.
The purpose of our study is to investigate whether ticagrelor administration before catheterization procedure is associated with better early reperfusion and preservation of heart function in the East-Asian STEMI patients undergoing percutaneous coronary intervention in real-world practice.
Patients and Methods
Study Populations
This was a monocentric retrospective observational study. We included 428 consecutive STEMI patients presenting at Jiading Central Hospital from January 2017 to October 2019. The diagnosis of STEMI was established when the patient had continuous typical chest pain or discomfort ≥30 minutes or other symptoms suggestive of STEMI, and ST-segment elevation ≥2mm in at least two contiguous electrocardiography leads. Ninety-one patients admitted to hospital after 12 h from symptom onset were excluded. Five patients without PCI treatment were excluded. Three patients receiving thrombolysis therapy before PCI procedure were excluded. Furthermore, since this study was focused on STEMI patients in the East-Asian population, we excluded three Caucasian patients from the study cohort.
The remaining 326 patients were divided into two groups due to their antiplatelet loading strategy. All the patients had a clear record of ticagrelor administration before coronary angiography procedure. For the patients directly admitted to the emergency department (ED) of the research center, early ticagrelor administration was suggested according to the following indications: (1) confirmation of STEMI by electrocardiography, (2) estimated time for catheter laboratory preparation >20 min, (3) no evidence of contraindications of loading ose antiplatelet treatment, especially the aortic dissection. Thus, patients with high D-dimer levels (>800 ng/mL) were not recommended to take a loading dose of ticagrelor until exclusion of aortic dissection was made by aortic ultrasound or computed tomography. Patients estimated to be accessible to the catheter laboratory within 10 min after STEMI confirmation were recommended to receive in-lab ticagrelor treatment in order to reduce the length of time in the ED. Transported patients tended to receive in-lab treatment due to the lack of ticagrelor in local emergency medical service (EMS) ambulances and non-PCI hospitals, and their rapid transfer from ED to catheter laboratory (usually ≤10 min), but early ticagrelor loading was still preferred if the drug was available in the first-aid institutions. Patients without contraindications were also administrated with a chewable loading dose of aspirin (300 mg) with ticagrelor or after confirmation of STEMI, due to the physician’s discretion and the access to ticagrelor. Detailed data on demographics, symptoms, history of hypertension, diabetes mellitus, dyslipidemia, stroke, coronary heart disease, myocardial infarction and stent implantation were obtained from the electronic medical recording system (EMRS). The time segments of first medical contact, coronary catheterization, and P2Y12 inhibitor administration were retrieved from the Chest Pain Data Reporting Platform. Clinical data on serum troponin I, creatinine, lipid profiles, PCI results, echocardiography, and clinical outcomes were also obtained from the EMRS.
The study protocol was approved by the Ethics Review Board of Jiading Central Hospital (No. 2017-ZD-03). The authors, except for the corresponding author, were licensed cardiology physicians of Jiading Central Hospital and preserved the legal rights to review the patients’ medical records. All the patients were anonymized during data processing and statistical analysis. Personal information such as name, address, telephone number and citizen ID number was not recorded in the database. The study protocol was carried out in full compliance with the Declaration of Helsinki. Informed consent was not required because of the retrospective nature of this study.
Definitions and Endpoints
We define the initiation of the PCI procedure as the moment when the patient reached the operating table of the catheter laboratory and preparation started for the radial puncture. Thus, preprocedural treatment was defined as the administration of the loading dose of ticagrelor at any time before entering the catheter laboratory, and in-lab treatment was defined as the administration of the loading dose of ticagrelor between entering the catheter laboratory and the radial artery puncture. Primary transported patients were defined as the patients directly transferred from the first-aid scene to the catheter laboratory by local EMS ambulances. Secondary transported patients were defined as the patients transferred from other non-PCI hospitals. First medical contact (FMC) was defined as any kind of the earliest medical contact to the patient, including the emergency departments, the ambulances of local EMS, or other medical institutions in the local medical service network. FMC-to-wire time was defined as the time interval from FMC to the definite moment when the guide wire was running through the culprit artery. Ticagrelor-to-angiography time was defined as the time interval between the administration of ticagrelor and the initiation of coronary angiography to the culprit artery.
The combined reperfusion evaluations included the following aspects: (1) the presence of self-patency, which was defined as thrombolysis in myocardial infarction (TIMI) grade 2 or 3 flow in the culprit artery at the initiation of angiography, which was present in the reperfusion condition before the angiography procedure; (2) the presence of no-reflow, regarded as a TIMI grade 0–1 flow in the culprit artery after primary PCI, in presentation of the instant reperfusion after balloon inflation and stenting; (3) the presence of ST-segment elevation resolution of 50% or above within 24 h after PCI procedure, which indicated the microvascular reperfusion after PPCI. Rate of adverse events was analyzed at 28 days after catheterization. Primary clinical endpoints included composite cardiovascular adverse events of all-cause mortality, new-onset heart failure, stroke, reinfarction and definite stent thrombosis. Patients with suggestive symptoms of heart failure and one of the following indications at any time after PCI were defined as new-onset heart failure: (1) acute pulmonary edema or cardiac shock; (2) new bilateral basal pulmonary rales covering ≥30% of lung fields, or the area of rales spreading ≥50% compared with baseline levels within 72 h; (3) left ventricular ejection fraction (LVEF) <45% without definite evidence of chronic heart failure history; (4) re-hospitalization due to acute heart failure onset during the observation period. Bleeding events and mechanical complications were defined as secondary clinical endpoints.
Statistical Analysis
Statistical analysis was performed by SPSS 16.0 (SPSS Inc., Chicago, IL, USA). Continuous parametric variables were represented as mean ±SD values. Categorical variables were expressed as frequency (percentage). Parametric data between the pretreatment group and the in-lab treatment group were compared with Student's t-test. Nonparametric variables were compared between groups by chi-squared tests or the Wilcoxon rank sum test. Effects of different antiplatelet strategies on reperfusion of culprit coronary artery were compared by multivariate logistic regression. Association between different antiplatelet strategies and clinical endpoints was calculated in a Cox proportional hazards model, with cardiovascular risk factors, lipid profiles and other time-related variables chosen using a backward stepwise selection algorithm. Kaplan–Meier estimates of new-onset heart failure events were calculated for different antiplatelet therapies.
Results
Study Population
The general characteristics of the study population were listed in Table 1, and clinical profiles were listed in Table 2. One hundred and forty patients received a 180 mg loading dose of ticagrelor before entering the catheter laboratory. One hundred and eighty-six patients received a 180 mg loading dose of ticagrelor between arrival at the catheter laboratory and radial artery puncture. The main reasons of in-lab ticagrelor administration in the patients directly admitted to the ED were delayed diagnosis due to irregular ECG performance at FMC (41 of 100 patients), and rapid transfer from ED to catheter laboratory within 10 min after the confirmation of STEMI (28 of 100 patients). For the secondary transported patients in the in-lab treatment group, irregular ECG at FMC (16 of 52 patients), unavailability of ticagrelor (14 of 52 patients) and inadequate early antiplatelet treatment with 100 mg aspirin alone (11 of 52 patients) were major reasons for late ticagrelor administration, while 64.71% primary transported patients in the in-lab treatment group (22 of 34 patients) received delayed ticagrelor loading dose due to the unavailability of the oral antiplatelet agents in the ambulances, as neither aspirin nor ticagrelor were routinely employed by the local EMS by the end of 2018. The factors associated with the delayed ticagrelor loading in the patients admitted directly, primary transported, and secondary transported to the research center were illustrated in Figure 1.
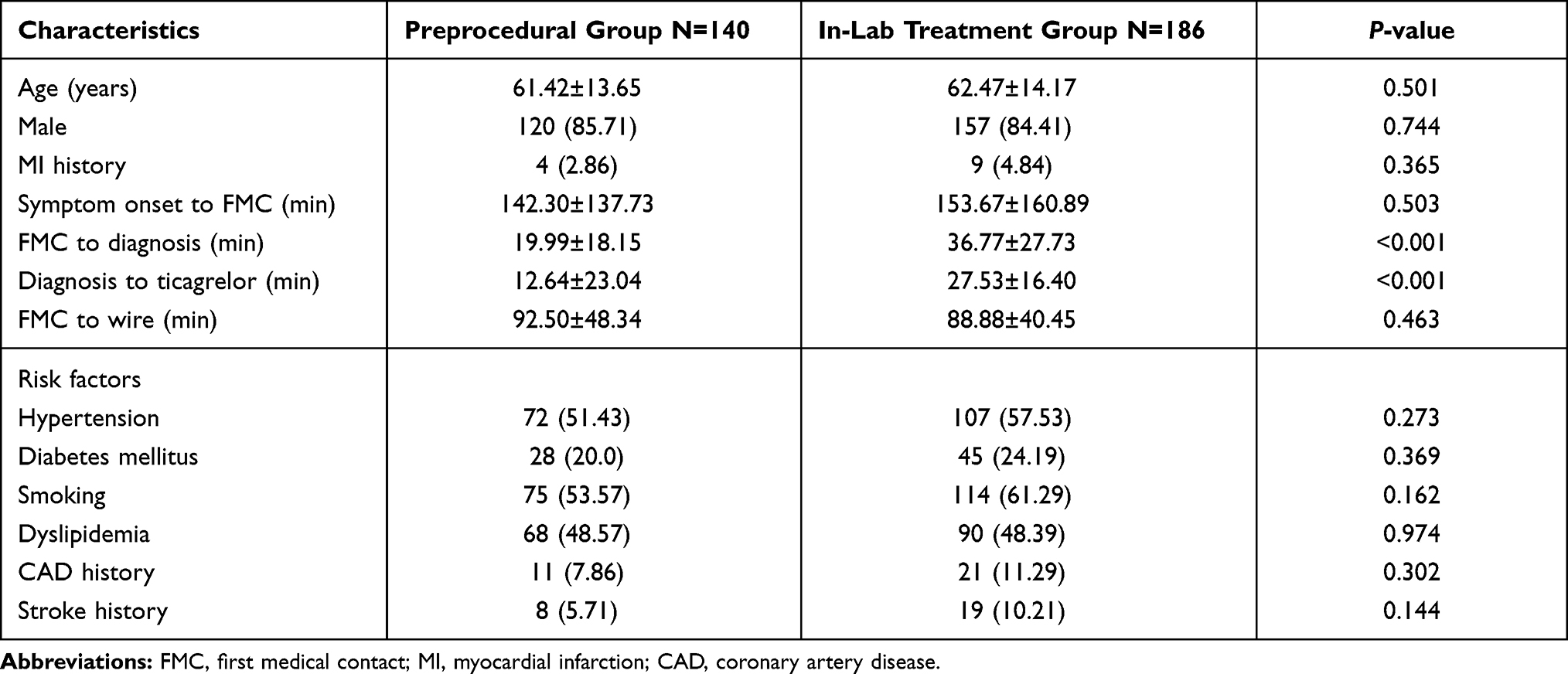 |
Table 1 Patient Characteristics and Risk Factors |
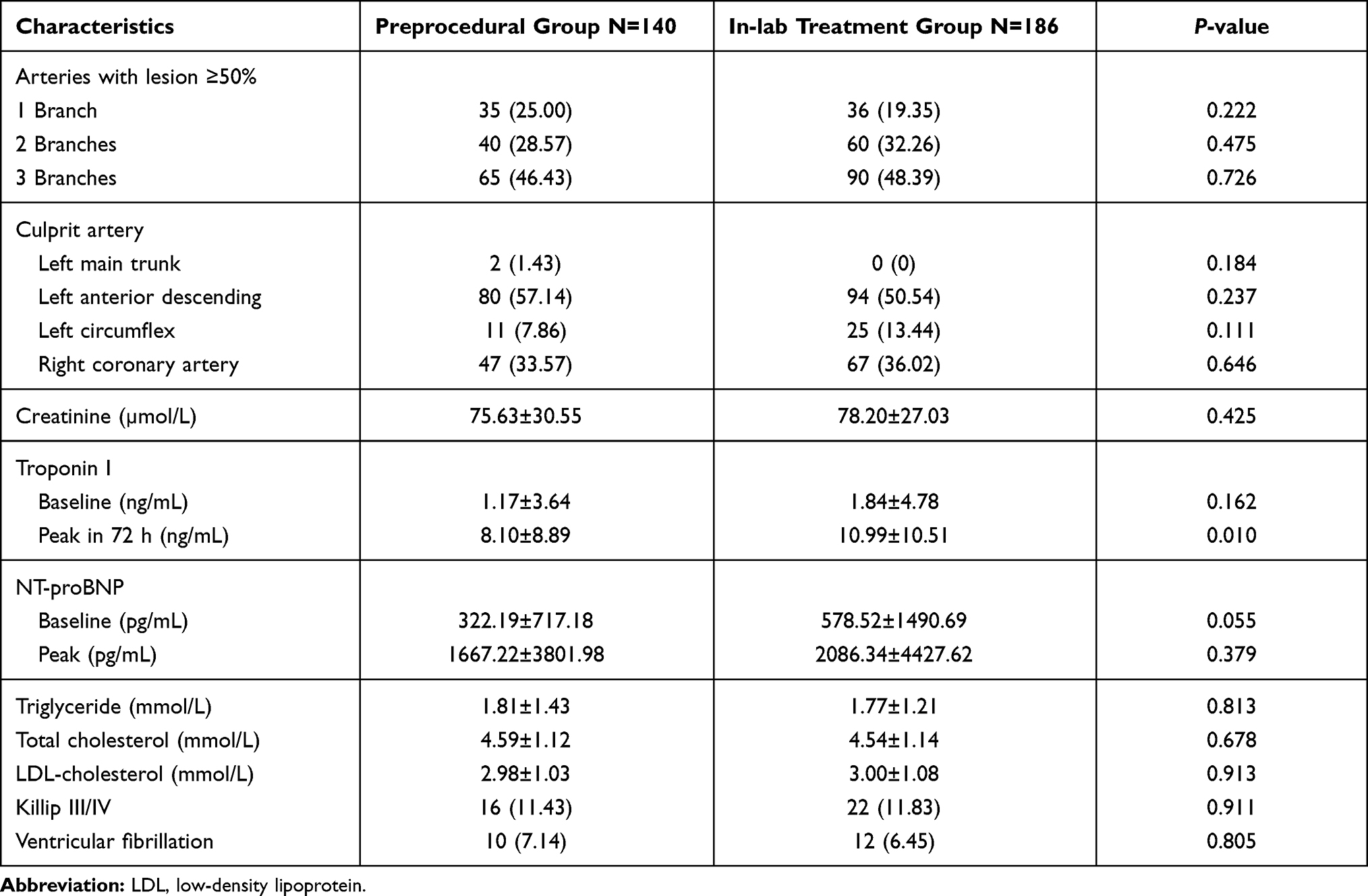 |
Table 2 Clinical and Angiography Profiles of the Patients |
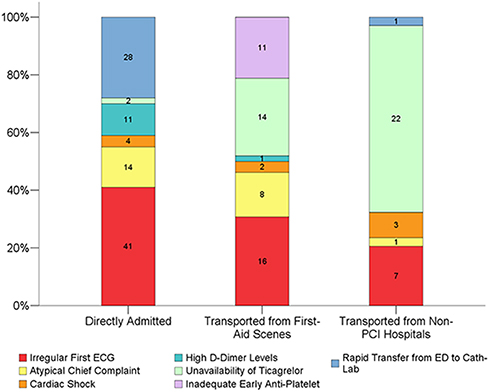 |
Figure 1 The influence factors of delayed ticagrelor administration in the STEMI patients admitted in different ways. Atypical chief complaints included non-chest pain chief symptoms such as abdominal pain, throat discomfort, sudden dyspnea and syncope. High D-Dimer level was defined as ≥800 ng/mL. Monotherapy of 100 mg aspirin after prehospital confirmation of STEMI was demonstrated as inadequate early antiplatelet. Rapid transfer was defined as ≤10 min from STEMI confirmation to the patient’s arrival at the cath-lab. Abbreviations: PCI, percutaneous coronary intervention; ECG, electrocardiography; ED, emergency department. |
The two groups were well balanced in baseline characteristics. The proportions of smokers, stroke history and myocardial infarction history were higher in the in-lab treatment group, but the difference was not statistically significant. No arterial fibrillation history was observed in the study population. The troponin I level at baseline was not significantly different between the two groups (1.17±3.64 ng/mL vs 1.84±4.78 ng/mL, P=0.162), but the peak value in 72 h after admission was significantly lower in the preprocedural treatment group (8.10±8.89 ng/mL vs 10.99±10.51 ng/mL, P=0.010). Serum NT-proBNP in the preprocedural group at baseline (322.19±717.18 pg/mL vs 578.52±1490.69 pg/mL, P=0.055) and at the peak level during hospitalization (1667.22±3801.98 pg/mL vs 2086.34±4427.62 pg/mL, P=0.323) were both numerically lower than the in-lab treatment group. The time interval from FMC to the confirmation of STEMI (19.99±18.15 min vs 36.77±27.73 min, P<0.001), and from confirmation to ticagrelor administration (12.64±23.64 min vs 27.53±16.40 min, P<0.001) were significantly shorter in the preprocedural group. The median FMC-to-wire time interval was 99 min, with no significant difference between the two groups. The proportions of patients with high Killip class or ventricular fibrillation attack during precatheterization settings did not differ between the two groups.
The antiplatelet treatment time segments and other periprocedural medications were listed in Table 3. The median time intervals from ticagrelor loading to angiography overall, for the preprocedural treatment group, and for the in-lab treatment group were 31, 55, and 21 min, respectively. Loading dose aspirin was administrated before PPCI in 98.47% patients (321 of 326) except for five patients in the in-lab treatment group who had already taken 100 mg aspirin before seeking medical care. The proportion of early aspirin loading dose administration (defined as ≥30 min before angiography to the culprit artery), however, was significantly higher in the preprocedural treatment group (86.42% vs 41.94%, P<0.001), which was in line with the significantly higher proportion of early ticagrelor administration (≥30 min before angiography) in this group (86.42% vs 23.12%, P<0.001). Delayed aspirin administration was more likely to occur with the patients directly admitted to ED (76 of 153, 49.67%) and primary transported patients (31 of 48 cases, 64.58%), which was partly due to the unavailability of antiplatelet medications in the ambulances, and partly because of our “one-package” method of antiplatelet drug management, that is, the loading dose pills of dual antiplatelet agents (three pills of 100 mg aspirin and two pills of 90 mg ticagrelor) were contained in a single package and delivered to the patient as a whole in order to avoid repeated or missed medication. Secondary transported patients, however, tended to take loading dose aspirin separately in their first-aid institutions. Opioid use before ticagrelor administration did not differ between the two groups (7.14% vs 6.45%, P=0.805). The proportion of patients with thrombus aspiration or tirofiban bail-out therapy during PCI procedure did not differ between the two groups.
 |
Table 3 Antiplatelet Treatment Time Segments and Other Medications |
Culprit Artery Reperfusion
Table 4 demonstrated the reperfusion endpoint in the two study groups. Presence of self-patency in the culprit artery was significantly higher in the preprocedural treatment group than in the in-lab treatment group (25.71% vs 16.67%, P=0.045). The proportion of instant TIMI3 flow before angiography was numerically higher in the preprocedural group, but the difference was not statistically significant (20.0% vs 12.37%, P=0.060). The proportion of patients with ST-segment elevation resolution ≥50% within 24 h after PCI was significantly higher in the preprocedural treatment group (48.57% vs 27.96%, P<0.001). Presence of no-reflow after PCI, however, showed no significant difference between the two groups.
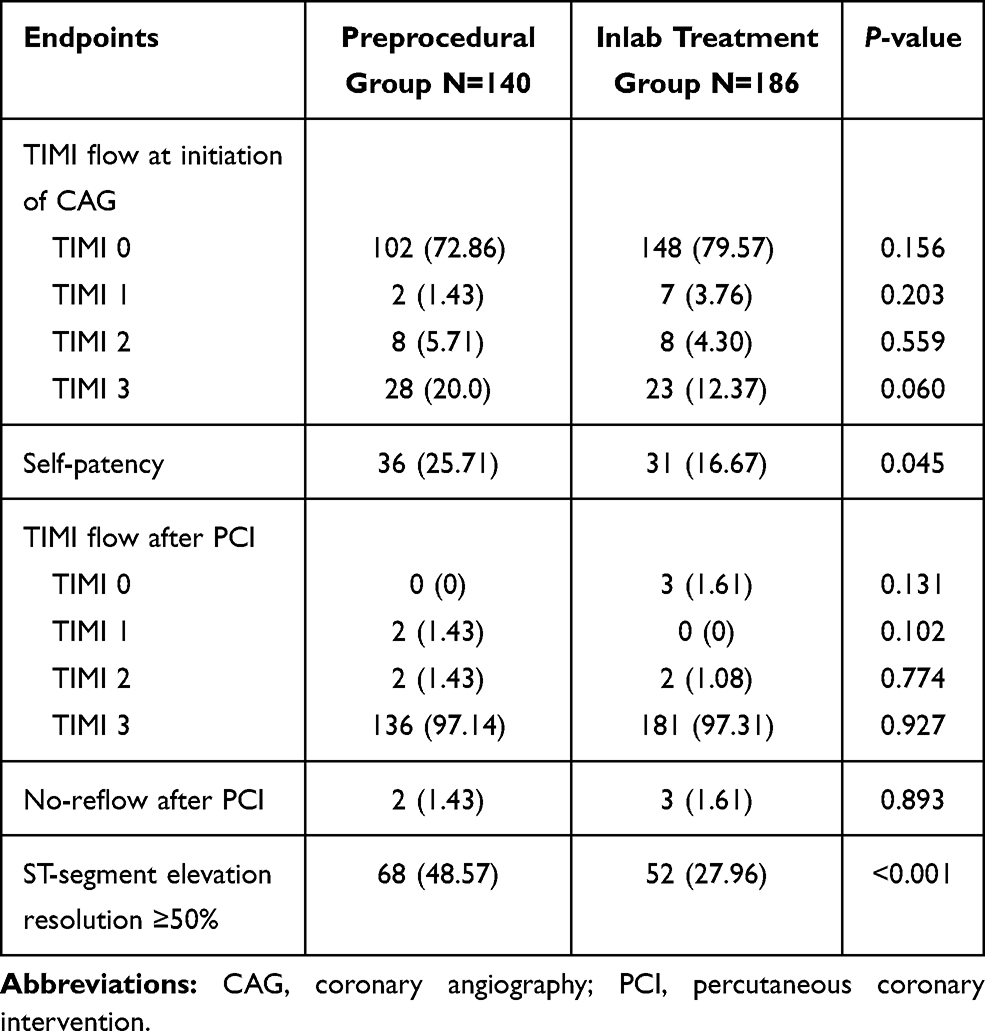 |
Table 4 Culprit Artery Reperfusion Endpoints |
In the multivariate logistic regression analysis adjusted for gender, age, history of hypertension, diabetes, dyslipidemia, smoking and previous coronary artery disease, preprocedural ticagrelor treatment was found to be an independent influence factor to the increasing early ST-segment elevation resolution after primary PCI (OR: 3.057, 95%CI: 1.538–6.075, P=0.001, Table 5).
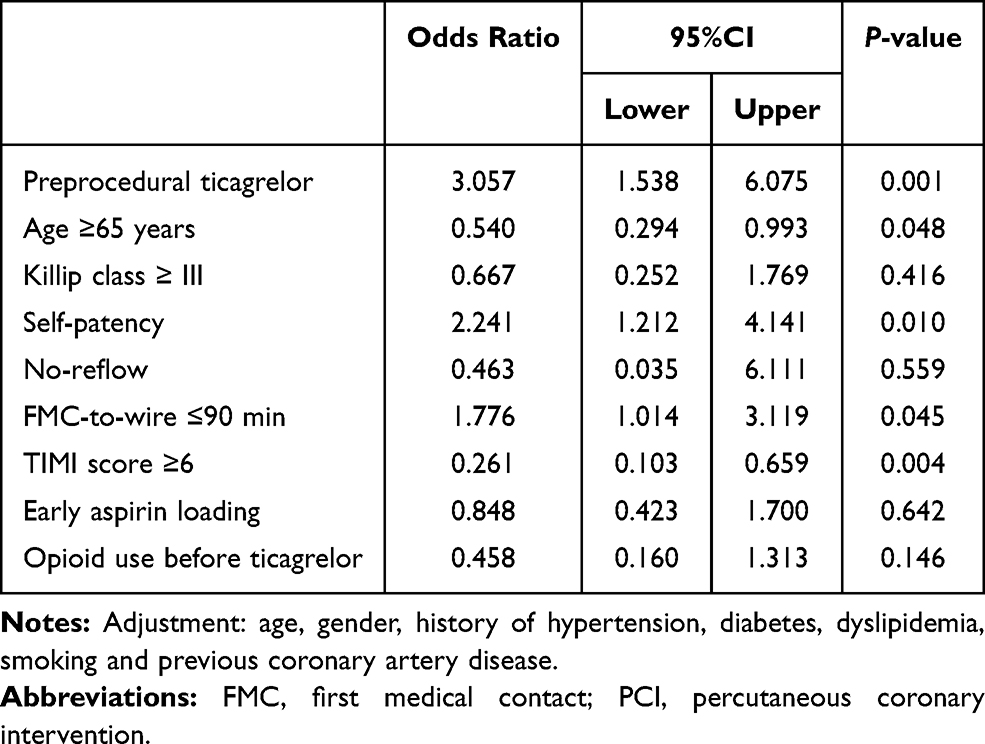 |
Table 5 Multivariate Logistic Regression Analysis for Influence Factors of Early ST-segment Elevation Resolution Within 24 Hours After PCI |
Clinical Outcomes
Clinical outcome data within 28 days after primary PCI was listed in Table 6. The proportions of patients with new-onset heart failure in the preprocedural treatment group was significantly lower than the in-lab treatment group (9.29% vs 18.82%, P=0.016, Figure 2). Mean left ventricular ejection fraction (LVEF) in the preprocedural group was nonsignificantly lower than the in-lab treatment group at admission (59.74±10.43% vs 60.52±10.03%, P=0.507), but showed a greater increasing trend during hospitalization and turned out to be higher than the in-lab treatment group before discharge, although the difference was not statistically significant (62.68±10.93% vs 61.42±9.62%, P=0.286). The proportions of patients with definite stent thrombosis (0.71% vs 1.61%, P=0.466) was numerically lower in the preprocedural treatment group, but the difference was not statistically significant compared with the in-lab treatment group. All-cause mortality and reinfarction did not differ between the two groups. No stroke cases were found during the observation. The proportion of bleeding events in the preprocedural treatment group was numerically higher than in the in-lab treatment group (4.29% vs 1.62%, P=0.145). No life-threatening or cerebral bleeding events were observed in the study populations.
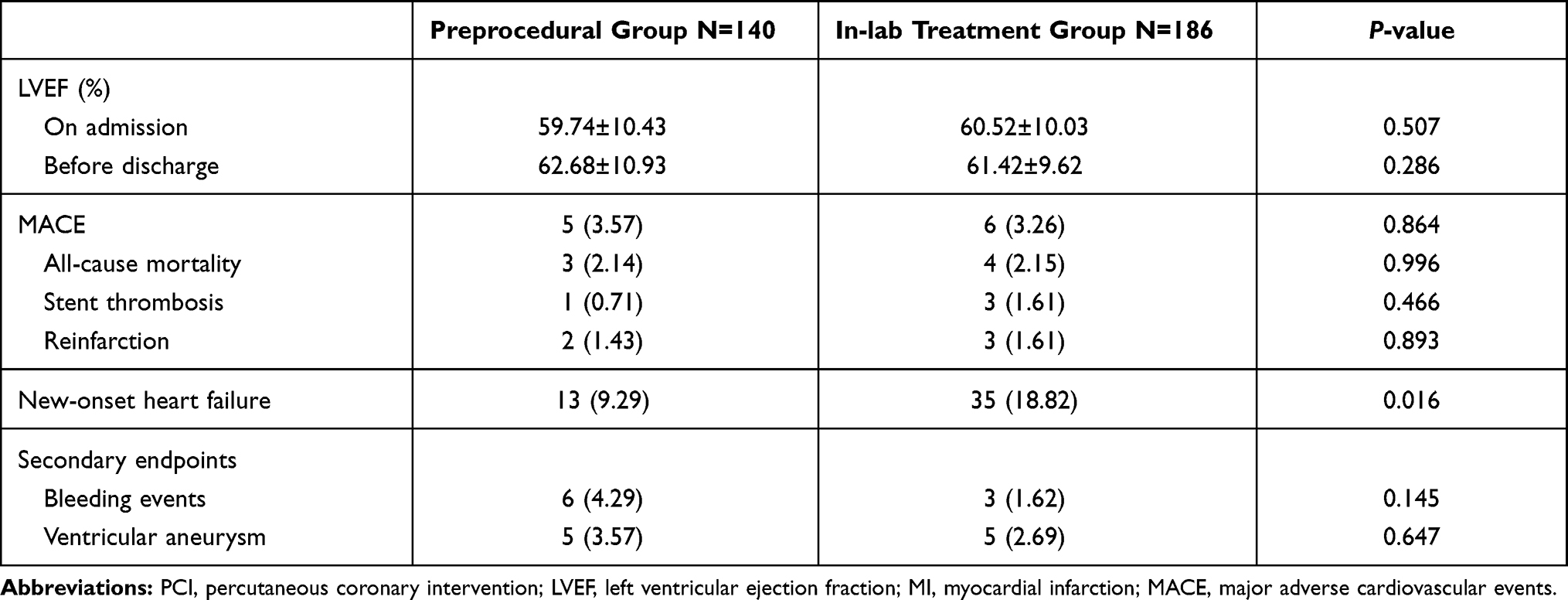 |
Table 6 Clinical Outcomes Within 28 Days After PCI |
 |
Figure 2 Kaplan–Meier curve of the 28-day heart failure events between preprocedural and in-lab treatment groups. Log rank (Mantel–Cox)=5.294, P=0.021. |
In the Cox-regression hazard model adjusted by age, gender and multiple cardiovascular risk factors, delayed FMC-to-wire time, high TIMI score and no-reflow were independently related to the increasing risk of short-term heart failure after PCI procedure, while ticagrelor pretreatment was indicated to be protective to the heart failure events (adjusted HR: 0.517, 95%CI: 0.276–0.967, P=0.039, Table 7).
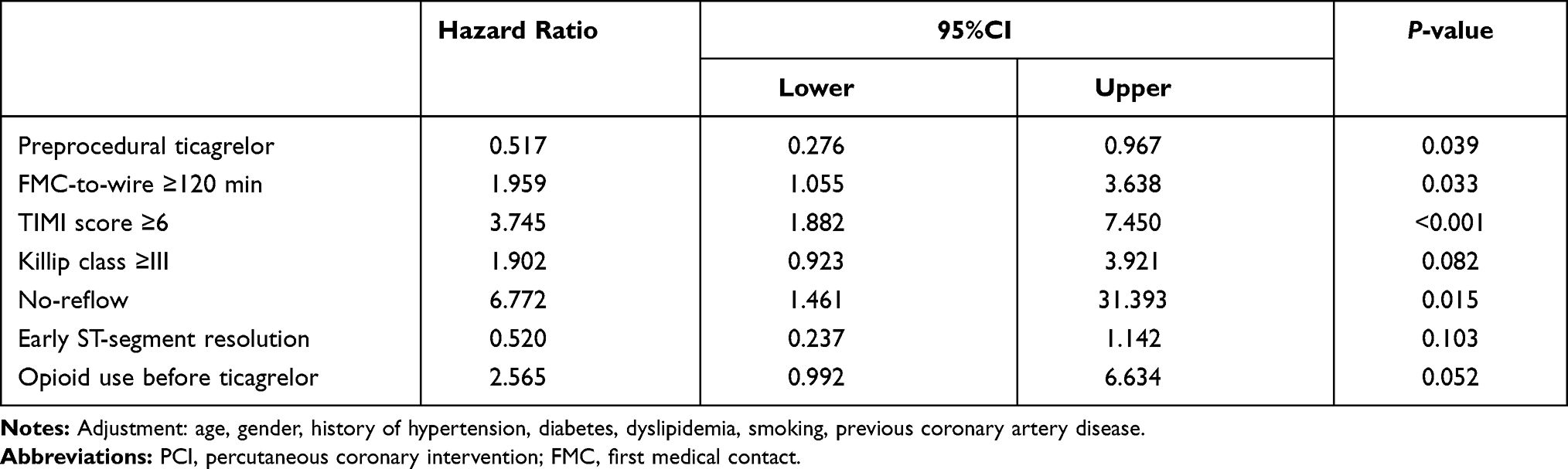 |
Table 7 Cox Regression for Risk Factors of New-onset Heart Failure in 28 Days After PCI |
Analysis Across Drug-to-angiography Time Quartiles
As an exploratory analysis, we divided the entire study cohort into four groups according to the quartiles of the time intervals from ticagrelor loading to the initiation of coronary angiography procedure (Tables 8–9). The patients in the fourth quartile (ticagrelor-to-angiography time >54 min) had a longer delay in the symptom onset to FMC time than the other quartiles. FMC-to-wire delays in the third and fourth quartiles were significantly longer than in the first and second quartiles. The proportion of early ST-segment resolution in the fourth quartile was nonsignificantly higher than the second quartile (44.30% vs 31.33%, P=0.086), while the early ST-segment elevation resolution rates between other groups showed no significant difference. The rates of self-patency both in the first quartile (28.41% vs 10.84%, P=0.004) and fourth quartile (26.58% vs 10.84%, P=0.010) were significantly higher than in the second quartile. The proportion of no-reflow did not differ significantly among the four quartile groups.
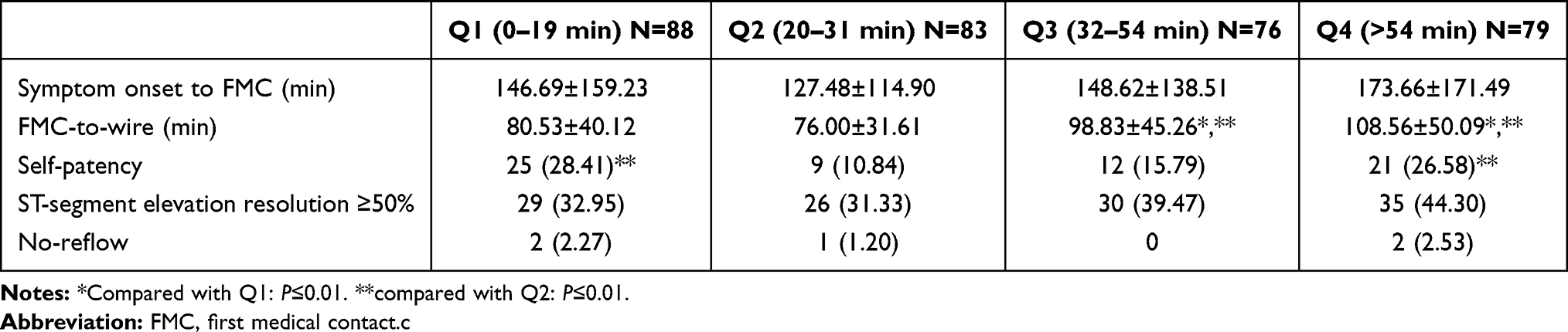 |
Table 8 Time Segments and Reperfusion Endpoints Across Ticagrelor-to-angiography Time Quartiles |
 |
Table 9 Clinical Outcomes Across Ticagrelor-to-angiography Time Quartiles |
In terms of 28-day outcomes, the proportion of overall MACE (4 of 79, 5.06%) and reinfarction events (2 of 79, 2.53%) was higher in the 4th quartile but the difference was not significant compared with the other quartile groups. All-cause mortality was nonsignificantly lower in the first quartile (1 of 88, 1.14%). The presentation of short-term heart failure events was numerically higher in the third quartile (15 of 76, 19.74%), but the difference was not statistically significant. The rates of reinfarction were nonsignificantly higher in the fourth quartile group. Stent thrombosis risks did not differ across the time quartiles.
Discussion
Main Findings
To our knowledge, this study was the first one on the relationship between ticagrelor loading dose treatment before PCI procedure and short-term heart function after PPCI in East-Asian STEMI patients. In our study, preprocedural ticagrelor treatment was associated with improved reperfusion of the infarct-related artery (IRA), presented by increased presentation of self-patency and early ST-segment elevation resolution. The pretreatment strategy was also associated with a significant reduction of new-onset heart failure risks within 28 days after PCI. These findings indicated that early ticagrelor loading before entering the catheter laboratory could be beneficial for East-Asian STEMI patients scheduled for urgent PCI in the preservation of ventricular function. It should be noted that preprocedural administration of ticagrelor was observed to be associated with an increasing risk of bleeding events in our study, although the difference was not statistically significant compared with the in-lab treatment group.
Culprit Artery Reperfusion Endpoints
In our study, preprocedural ticagrelor treatment before entering the catheter laboratory was associated with the increasing presence of the IRA’s self-patency and early ST-segment elevation resolution, which was in contrast to the results from the prior ATLANTIC trial. In the ATLANTIC, the prehospital ticagrelor administration was proved to be safe, but did not contribute to the improvement of pre-PCI reperfusion. Some researchers interpreted this result as being affected by the short time interval between ticagrelor administration and access to the catheterization laboratory.11 In our study, the median time interval from ticagrelor loading to angiography in the preprocedural group was 55 min, which was much longer than the ATLANTIC trial. Further analysis by drug-to-angiography time quartiles also indicated that despite a longer delay in the FMC-to-wire time, patients with a drug-to-angiography time of over 54 min presented with a higher rate of early ST-segment elevation resolution in the first 24 h after PCI than the patients with drug-to-angiography time around 30 min. The difference in the pretreatment-to-PCI time interval, in conjunction with the difference in results of reperfusion endpoints between our study and the ATLANTIC trial suggested that the time interval between ticagrelor preloading and the access of catheterization procedure could play a role in the manifestation of the benefits of the pretreatment strategy. Although patients in the first time quartile, in which the drug-to-angiography time was less than nine minutes, showed a similar proportion of early ST-segment elevation resolution in comparison with the fourth quartile, it should be noted that this quartile group had a much shorter FMC-to-wire time of around 80 min, which was an independent factor of improving early ST-segment elevation resolution by itself according to the logistic regression results (OR=1.776, P=0.045). Due to the small sample size of this study, the interaction of FMC-to-wire time and ticagrelor-to-angiography time in the contribution to early ST-segment elevation resolution remained unclear, which needs further investigation.
In addition to the influence of medication-to-catheterization interval, the difference in upstream administration of opioid before ticagrelor was also possible to contribute to the reperfusion endpoints. In the ATLANTIC trial, it was stated that morphine was administrated in half of the study population before randomization and ticagrelor loading. Several prior studies observed that morphine affected the antiplatelet effects of clopidogrel by lagging its absorption and decreasing the plasma levels of the P2Y12 agent as well as its active metabolite.12–14 Impaired antiplatelet effects of ticagrelor and prasugrel associated with morphine administration were reported by Parodi et al,15 which led to the hypothesis that morphine could affect the pharmacodynamics and pharmacokinetics of novel oral P2Y12 inhibitor agents, thus reducing the potent benefit of early P2Y12 inhibitor administration. In our study, the rate of opioid administration before ticagrelor loading was low (17 of 258 patients, 6.59%). In the logistic regression analysis, the association between preprocedural ticagrelor treatment and early ST-segment elevation resolution remained significant when upstream opioid administration was added into the model as a covariant. Thus, we considered that the interference morphine could have on the antiplatelet effects of ticagrelor were likely to be ruled out in our study.
Clinical Outcomes
Two large clinical studies concentrated on the benefits of ticagrelor pretreatment to the short-term outcomes of STEMI patients undergoing urgent PCI were published previously, the ATLANTIC and a sub-study of the SWEDEHEART register. Both of the studies showed neutral results in a composite ischemic endpoint of all-cause mortality, myocardial reinfarction and definite stent thrombosis. New-onset heart failure after PCI, however, was not taken as a clinical endpoint in the two studies. In the current study, the proportion of heart failure events in 28 days after urgent PCI was significantly lower in the preprocedural ticagrelor treatment group than in the in-lab treatment group. In conjunction with the positive findings in the presence of early ST-segment elevation resolution and early reperfusion of the IRAs, this finding suggested that early ticagrelor administration before PCI procedure was potentially of benefit to preserve left ventricular function after urgent PCI procedure by improving the early reperfusion in the IRA-related areas and preventing microvascular obstructions. In a recently published study, third generation P2Y12 inhibitors as ticagrelor and prasugrel were associated with reduced infarction size, lower prevalence of microvascular obstruction, and a significantly reduced risk of heart failure in comparison with clopidogrel, which was considered to be affected by the short onset of peak antiplatelet activities and lower drug resistance of these novel P2Y12 inhibitors.16 Furthermore, besides its antiplatelet effects, ticagrelor was reported to have the potency of increasing the plasma concentration of endogenous adenosine, which could reduce ischemia and reperfusion injury by interfering with the production of inflammatory mediators, oxygen species, and neutrophil trafficking, thus contributing to the preservation of microvascular function, the reduction of infarction size and the improvement of the left ventricular function during the peri-PCI period.17,18 In the current study, early and adequate microvascular reperfusion, which was indicated by early ST-segment elevation resolution, was proved to be associated with better short-term prognosis of STEMI patients. The patients with early ST-segment elevation resolution had a higher proportion of early ticagrelor (56.67% vs 34.95%, P<0.001) and aspirin preloading (61.67% vs 53.88%, P=0.171), and the prevalence of new-onset heart failure (6.67% vs 19.42%, P<0.001) and death (0.0% vs 3.39%, P=0.041) was significantly lower in comparison with the patients without early ST-segment elevation resolution. It should be noted that the early ST-segment elevation resolution did not enter the Cox survival model including preprocedural ticagrelor administration (HR=0.520, 95%CI: 0.237–1.142, P=0.103), but turned out to be an independent protective factor of short-term heart failure events when preprocedural ticagrelor administration was removed from the model (HR=0.453, 95%CI: 0.209–0.985, P=0.046). The abolished association between early ST-segment elevation resolution and reduction of new-onset heart failure in the Cox survival model containing early ticagrelor administration, in conjunction with the greater difference of the prevalence of heart failure events between early vs late ST-segment elevation resolution groups and early vs late ticagrelor groups, suggested that the reduction of short-term heart failure incidents should be considered to result from the interaction between early ticagrelor administration and preserved microvascular perfusion, which was difficult to exclude in the current study due to our low sample size. This issue should be further investigated in large-scale randomized trials.
The proportion of definite stent thrombosis and reinfarction within 28 days after PCI was numerically reduced in the patients with preprocedural ticagrelor treatment, which was in line with the results of the ATLANTIC trial, but the difference between the preprocedural and in-lab treatment groups did not reach statistical significance. Furthermore, a longer duration between ticagrelor loading and coronary angiography was not associated with fewer MACE, stent thrombosis or reinfarction events, which indicated that the potential benefit of early ticagrelor preloading before PPCI procedure might be manifested in other aspects such as ventricular function preservation and microvascular protection, rather than a direct prevention of periprocedural ischemic adverse events caused by macrovascular thrombosis.
All-cause mortality did not differ between the preprocedural and in-lab treatment groups, as was reported in several other studies.10,12,19–21 However, two of the three deaths in the preprocedural group were due to nonischemic events (one died from ventricular rupture, and the other from cardiac shock), while three of the four deaths in the in-lab treatment group were directly caused by stent thrombosis and reinfarction. This may reflect a bias in the mortality analysis caused by the imbalance between the groups in terms of severity of the patients, which required investigation in further large-scale studies.
Bleeding Events
Although no major bleeding events according to the PLATO criteria were observed in the current study, the preprocedural group showed a nonsignificant trend toward minor bleeding events. The proportion of patients with bleeding events in the preprocedural group was almost three times higher than the in-lab treatment group. This finding was in line with the result of a previous study, which reported ticagrelor was associated with increased bleeding risks in comparison with clopidogrel in East-Asian populations.20 This could be explained by the propensity for bleeding between East-Asian and Caucasian populations. Compared with the Caucasians, the East-Asians were reported to have a higher platelet reactivity that was associated with increased bleeding risks.22 Pharmacokinetic studies also showed higher active metabolite exposure rates and stronger pharmacodynamic responses in East-Asians than the Western counterparts when the same doses of novel P2Y12 inhibitors were administrated.23,24 The specific profiles for bleeding in East-Asian patients indicated that the potential risk of excess to hemorrhage events must be taken into consideration when ticagrelor pretreatment is planned in East-Asian STEMI patients in the case of scheduled primary PCI.
Limitations
This study was a single-center study with a small sample size, which was a limitation for the statistical power of the results. Grouping of patients was not randomized, making it difficult to rule out observational bias. Data on plasma adenosine, platelet reactivity and CMR for evidence of microvascular obstruction were not available, thus, whether the reduction of prevalence of heart failure in the pretreatment group was associated with early increasing of plasma adenosine or reducing microvascular obstructions was unclear. Large-scale randomized clinical studies should be considered for further investigations on these matters. Finally, as a retrospective observational study with a much smaller sample size than the other randomized clinical trials, the evidence strength of our results was very limited, and should be regarded as hypothesis-generating. The results should be checked in further extensive randomized trials.
Conclusion
Early administration of loading dose ticagrelor before coronary catheterization procedure was associated with improved peri-PCI reperfusion as well as reduced risks of new-onset heart failure in East-Asian STEMI patients undergoing primary PCI, but the excess to bleeding events should be taken care in clinical practice.
Acknowledgments
This study was funded by Shanghai Municipal Jiading District Health Commission Foundation (2019-KY-09). The funding source had no role in the design of the study; in the collection, analysis, and interpretation of data; or in the writing of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Roffi M, Patrono C, Collet J-P, et al. Management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology. 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: task force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016;37(3):267–315. doi:10.1093/eurheartj/ehv320
2. O’Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines. J Am Coll Cardiol. 2013;61(4):485–510. doi:10.1016/j.jacc.2012.11.018
3. Fröbert O, Lagerqvist B, Olivecrona GK. Thrombus aspiration during ST-segment elevation myocardial infarction. N Engl J Med. 2013;369(17):1587–1597. doi:10.1056/NEJMoa1308789
4. Ibanez B, James S, Agewall S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119–177. doi:10.1093/eurheartj/ehx393
5. Montalescot G, Borentain M, Payot L, et al. Early vs. late administration of glycoprotein IIb/IIIa inhibitors in primary percutaneous coronary intervention of acute ST-segment elevation myocardial infarction: a meta-analysis. JAMA. 2004;292(3):362–366. doi:10.1001/jama.292.3.362
6. De Luca G, Gibson CM, Bellandi F, et al. Early glycoprotein IIb-IIIa inhibitors in primary angioplasty (EGYPT) cooperation: an individual patient data meta-analysis. Heart. 2008;94(12):1548–1558. doi:10.1136/hrt.2008.141648
7. Yong H, Lee SWL, Sawhney JPS. Contemporary pre-hospital management of acute coronary syndromes patients: results from the EPICOR Asia Study. Circulation. 2013;128:A14546.
8. Montalescot G, Van’t Hof AW, Lapostolle F, et al. Prehospital ticagrelor in ST segment elevation myocardial infarction. N Engl J Med. 2014;371(11):1016–1027. doi:10.1056/NEJMoa1407024
9. Sasha Koul J, Smith G, Götberg M, et al. No benefit of ticagrelor pretreatment compared with treatment during percutaneous coronary intervention in patients with ST-segment–elevation myocardial infarction undergoing primary percutaneous coronary intervention. Circ Cardiovasc Interv. 2018;11(3):e005528.
10. Levine GN, Jeong Y-H, Goto S, et al. Expert consensus document: World Heart Federation expert consensus statement on antiplatelet therapy in East Asian patients with ACS or undergoing PCI. Nat Rev Cardiol. 2014;11(10):597–606. doi:10.1038/nrcardio.2014.104
11. Alexopoulos D, Moulias A, Kanakakis I, Xanthopoulou I. Pre-hospital ticagrelor in ST-segment elevation myocardial infarction: ready for prime time? Int J Cardiol. 2015;194:41–43. doi:10.1016/j.ijcard.2015.05.064
12. Parodi G, Bellandi B, Xanthopoulou I, et al. Morphine is associated with a delayed activity of oral antiplatelet agents in patients with ST-elevation acute myocardial infarction undergoing primary percutaneous coronary intervention. Circ Cardiovasc Interv. 2015;8(1):1–6. doi:10.1161/CIRCINTERVENTIONS.114.001593
13. Parodi G, Bellandi B, Xanthopoulou I, et al. Morphine decreases clopidogrel concentrations and effects: a randomized, double-blind, placebo-controlled trial. J Am Coll Cardiol. 2014;63(7):630–635. doi:10.1016/j.jacc.2013.10.068
14. Meine TJ, Roe MT, Chen AY, et al. Association of intravenous morphine use and outcomes in acute coronary syndromes: results from the CRUSADE quality improvement initiative. Am Heart J. 2005;149(6):1043–1049. doi:10.1016/j.ahj.2005.02.010
15. Parodi G, Valenti R, Bellandi B, et al. Comparison of prasugrel and ticagrelor loading doses in ST-segment elevation myocardial infarction patients: RAPID (rapid activity of platelet inhibitor drugs) primary PCI study. J Am Coll Cardiol. 2013;61(15):1601–1606. doi:10.1016/j.jacc.2013.01.024
16. Khan JN, Greenwood JP, Nazir SA, et al. Infarct size following treatment with second- versus third-generation P2Y12 antagonists in patients with multivessel coronary disease at ST-segment elevation myocardial infarction in the CvLPRIT Study. J Am Heart Assoc. 2016;5(6):e003403. doi:10.1161/JAHA.116.003403
17. Barletta KE, Ley K, Mehrad B. Regulation of neutrophil function by adenosine. Arterioscler Thromb Vasc Biol. 2012;32(4):856–864. doi:10.1161/ATVBAHA.111.226845
18. Csóka B, Németh ZH, Rosenberger P, et al. A2B adenosine receptors protect against sepsis-induced mortality by dampening excessive inflammation. J Immunol. 2010;185(1):542–550. doi:10.4049/jimmunol.0901295
19. Montalescot G, Van’t Hof AW, Bolognese L, et al. Effect of pre-hospital ticagrelor during the first 24h after primary percutaneous coronary intervention in patients with ST-segment elevation myocardial infarction: the ATLANTIC-H 24 analysis. JACC Cardiovasc Interv. 2016;9(7):646–656. doi:10.1016/j.jcin.2015.12.024
20. Alexopoulos D, Xanthopoulou I, Gkizas V, et al. Randomized assessment of ticagrelor versus prasugrel antiplatelet effects in patients with ST-segment-elevation myocardial infarction. Circ Cardiovasc Interv. 2012;5(6):797–804. doi:10.1161/CIRCINTERVENTIONS.112.972323
21. Cayla G, Lapostolle F, Ecollan P, et al. Pre-hospital ticagrelor in ST-segment elevation myocardial infarction in the French ATLANTIC population. Int J Cardiol. 2017;244:49–53. doi:10.1016/j.ijcard.2017.06.009
22. Morimoto T, Fukui T, Lee TH, Matsui K. Application of U.S. guidelines in other countries: aspirin for the primary prevention of cardiovascular events in Japan. Am J Med. 2004;117(7):459–468. doi:10.1016/j.amjmed.2004.04.017
23. Kwon TJ, Tantry US, Park Y, et al. Influence of platelet reactivity on BARC classification in East Asian patients undergoing percutaneous coronary intervention. Results of the ACCEL-BLEED Study. Thromb Haemost. 2016;115(5):979–992. doi:10.1160/TH15-05-0366
24. Small DS, Payne CD, Kothare P, et al. Pharmacodynamics and pharmacokinetics of single doses of prasugrel 30 mg and clopidogrel 300 mg in healthy Chinese and white volunteers: an open-label trial. Clin Ther. 2010;32(2):365–379. doi:10.1016/j.clinthera.2010.02.015
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.