Back to Journals » Clinical Ophthalmology » Volume 20
Preoperative Surgical Site Vessel Density Is Predictive for Secondary Intervention after Preserflo Microshunt Implantation
Authors Kallab M ![]() , Hinterberger S, Schneider S, Murauer O, Schöllhorn J, Bolz M, Strohmaier CA, Reisinger AS
, Hinterberger S, Schneider S, Murauer O, Schöllhorn J, Bolz M, Strohmaier CA, Reisinger AS
Received 16 December 2025
Accepted for publication 15 March 2026
Published 19 April 2026 Volume 2026:20 586241
DOI https://doi.org/10.2147/OPTH.S586241
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Martin Kallab, Sarah Hinterberger, Sophie Schneider, Olivia Murauer, Julius Schöllhorn, Matthias Bolz, Clemens A Strohmaier, Anna-Sophie Reisinger
Department of Ophthalmology and Optometry, Kepler University Hospital, Johannes Kepler University, Linz, OÖ, Austria
Correspondence: Anna-Sophie Reisinger, Department of Ophthalmology and Optometry, Kepler University Hospital Linz, Johannes Kepler University, Altenberger Strasse 69, Linz, OÖ, 4040, Austria, Tel +43 5 768083-1050, Fax +43 5 768083-1822, Email [email protected]
Purpose: Conjunctival properties are known to influence the fate of glaucoma filtration surgeries but are hard to quantify in clinical practice. Therefore, the aim of this study was to investigate the predictive potential of anterior segment optical coherence tomography angiography (AS-OCTA) measured preoperative surgical site vessel density (SSVD) for secondary intervention and intraocular pressure (IOP) after Preserflo Microshunt implantation (PMI). Moreover, association of clinical preoperative conjunctival hyperemia grading (HG) with secondary intervention, SSVD and IOP was assessed.
Methods: In 23 open angle glaucoma patients, preoperative AS-OCTA measured SSVD and slit lamp photography-based HG were assessed. After PMI had been performed, patients were clinically followed for 6 months and secondary interventions as well as topical medications (MEDs) were recorded. The predictive value of SSVD and HG for secondary interventions was assessed using logistic regression modelling and their correlation with each other and with IOP was tested.
Results: Secondary interventions were performed in 3 of 23 patients. SSVD (p = 0.0339, area under the receiver operating characteristics curve (AUROC): 0.8167) but not HG (p = 0.7719, AUROC: 0.5750) was predictive for secondary interventions until 6 months after primary surgery. No correlations between SSVD/HG and IOP at any timepoint were detected (p > 0.05 for all timepoints). The number and type of preoperative MEDs were not predictive for secondary interventions and were not correlated with SSVD or HG (p > 0.05 for all analyses).
Conclusion: In this exploratory study preoperative AS-OCTA measured SSVD, but not clinical HG was a promising biomarker with predictive potential for surgical success of PMI. Confirmation of results in large scale studies is necessary and interventional trials are needed to evaluate whether vessel density based clinical decision making enhances clinical outcomes after filtration surgery.
Keywords: anterior segment optical coherence tomography angiography, vessel density, surgical success, Preserflo Microshunt
Introduction
Intraocular pressure (IOP) is still the only modifiable risk factor for glaucoma. When conservative IOP lowering strategies do not sufficiently slow or prevent disease progression or are not tolerated, surgical IOP lowering is performed. Current bleb-forming approaches (ie, Trabeculectomy (TE),1 Preserflo Microshunt implantation (PMI),2,3 and Xen Gel implantation (XGI))4,5 are highly dependent on proper filtration bleb function and IOP increase secondary to bleb fibrosis is one of the most common postoperative complications.6 In these cases secondary interventions (ie, needling, open revision) are performed to reestablish filtration properties.
Recently, bleb vessel density evaluation using anterior segment optical coherence tomography angiography (AS-OCTA) has been successfully utilized to discover early postoperative biomarkers for future surgical success/IOP, both after TE7–9 and PMI.10
While comparable preoperative AS-OCTA based biomarkers are scarce for TE11 and lacking for PMI, it is, however, well-known that preoperative conjunctival properties also largely influence the outcome of filtration surgeries.12 Specifically, ocular surface disease (OSD), which is – in the context of glaucoma – often caused or deteriorated by topical IOP lowering therapy itself or adjuvant preservatives (eg, benzalkonium chloride), is known to be a risk factor for bleb failure.12–16 In the last decades, therefore, extensive research has been conducted to characterize preoperative conjunctival changes down to the microscopic (high goblet cell density,17 low dendritic cell density18), and molecular level (MUC5AC+19) that are associated with surgical success. However, clinically readily-usable biomarkers predicting surgical success are scarce and AS-OCTA imaging offers potential to close this diagnostic gap.
Therefore, as a preoperative application of our previously published postoperative AS-OCTA findings,10 the aim of this study was to investigate the predictive potential of AS-OCTA measured preoperative surgical site vessel density (SSVD) for secondary intervention after PMI. Moreover, clinical conjunctival hyperemia grading (HG) and its association with both SSVD and secondary interventions was assessed.
Materials and Methods
Study Design and Patient Selection
Approval for this single-center study was obtained from the Ethic Committee of the Johannes Kepler University (EC-No.: B-142-17). Before study inclusion, written informed consent was given by every patient. We adhered to the tenets of the Declaration of Helsinki during all study-related procedures.
Criteria for inclusion to the study were a diagnosis of open-angle glaucoma (primary open-angle glaucoma, pseudoexfoliation glaucoma or pigment dispersion glaucoma) and indication for PMI. Indication for surgery was defined as: maximal tolerated IOP-reducing medical therapy AND uncontrolled IOP > 21 mmHg and/or visual field (VF) progression as tested using the 30–2 SITA fast algorithm of Humphrey Field Analyzer II 750 (Carl Zeiss Meditec Inc., Dublin, CA, USA) and/or progressive retinal nerve fiber layer thickness reduction as measured using Spectralis OCT (Heidelberg Engineering, Heidelberg, Germany). Exclusion criteria were secondary glaucomas (except the named), angle closure glaucoma and previous filtration surgery.
Preoperative Therapeutic Regimen, Limbal Marking, Slit Lamp Photography and AS-OCTA Imaging
Once scheduled for surgery, patients were switched to preservative-free (PF) topical therapy and Monodex® (dexamethasone) topical steroids were prescribed 10 days before surgery four times daily, according to our clinical standard.
At the day of surgery limbal marking of the targeted site of PMI was performed. Afterwards photographs of the surgical site were taken using a standard slit lamp photography setup and 10x slit lamp magnification. Finally, AS-OCTA measurements (PLEX Elite 9000; Carl Zeiss Meditec, Dublin, CA, USA) were performed at the surgical site.
Preserflo Microshunt Implantation
PMI surgical technique and medical device specifications (Santen Pharmaceutical, Osaka, Japan) have been published elsewhere.2,3 In short, the PM is made from poly(styrene-block-isobutylene-block-styrene) (SIBS), which is highly biocompatible and bioinert, and the medical device has the following basic dimensions: length: 8.5 mm, outer diameter: 350 µm, inner diameter: 70 µm.
Mitomycin C (MMC) augmented PM implantation in the supero-temporal or supero-nasal quadrant was performed under subtenon or general anesthesia. After dissection of the conjunctiva, three sponges soaked with 0.02% MMC were applied for 3 minutes. Then, the scleral pocket and tunnel to the anterior chamber were created before the PM was placed in the tunnel and introduced into the anterior chamber until the fins were securely placed inside the scleral pocket. Finally, the implant was flushed with balanced saline solution and flow was visualized. Interrupted, resorbable sutures were used for conjunctival wound closure.
Postoperative Treatment and Examinations
Following our clinical standard, Ofloxa-Vision® sine (Ofloxacin) PF antibiotic eye drops for 1 week and dexamethasone eye drops tapered over 12 weeks were prescribed postoperatively. One (POW1), 2 (POW2) and 4 week(s) (POW4), as well as 2 (POM2), 3 (POM3) and 6 months (POM6) after surgery, slit-lamp examinations and IOP measurements were performed. Number and type of IOP lowering medications (MEDs) and necessity as well as type of secondary interventions (needling, open revision, glaucoma drainage device (GDD)) were recorded. A secondary intervention was offered according to a predefined protocol as used in a previous study:10 If postoperative IOP exceeded the target pressure as preoperatively defined according to the guidelines of the European Glaucoma Society20 and no bleb or a scarred bleb was clinically visible. Depending on fulfilment of the endpoint “secondary intervention” patients were allocated to one of the two outcome groups.
AS-OCTA Scan Acquisition and Image Analysis
All AS-OCTA images were acquired using the PLEX Elite 9000 OCTA in combination with a 10 dpt anterior segment add-on lens. Basic principles of AS-OCTA image processing and surgical site vessel density (SSVD) calculation were similar to an already published protocol.10 Figure 1 shows image post-processing in a representative case with subsequent secondary intervention (Figure 1A–C) and in a patient without secondary intervention (Figure 1D–F). The current approach differed as follows: The distal end of the limbal marking was located in the best suited corresponding structural AS-OCT B-scan, and the Y-axis overlay was placed at the corresponding A-Scan location. The resulting cross-hair overlay was automatically translated to the full thickness AS-OCTA slab (Figure 1A and D). The distal end of the limbal marking was used as a reference location for all images. Images were exported to Fijii ImageJ21 for all further processing. Motion artifacts were removed using a fast-Fourier transform (FFT) bandpass filter as published previously10,22 before an obliquely rotated elliptical region of interest (400 x 800 px diameter) was placed between the X- and Y-axis of the cross-hair overlay (Figure 1B and E). It was, thus, positioned in the area of the future surgical site. Binarization using the Otsu algorithm23 and vessel density calculation were performed as previously published (Figure 1C and F).10
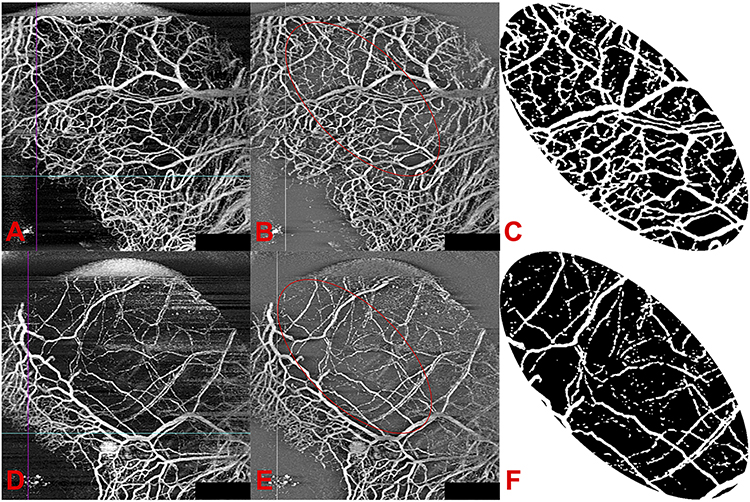 |
Figure 1 AS-OCTA-Image processing workflow. (A–C) Representative OCTA-image and processing steps of a patient with subsequent secondary intervention. (D–F) Representative OCTA-image and processing steps of a patient without secondary intervention. OCTA-Images with XY-axis overlay (turquois horizontal/violet vertical line, placed at distal end of limbal marking) were exported to ImageJ (A and D) where motion artefacts were removed by a fast-Fourier transform bandpass filter and an oblique elliptical ROI (red ellipse) was placed between the XY-axis overlay (grey horizontal/white vertical line, (B and E)) before the ROI was binarized using Otsu thresholding algorithm (C and F) to calculate surgical site vessel density. |
Clinical Hyperemia Grading
According to a five-step grading scale,24 conjunctival hyperemia was graded by one experienced glaucoma consultant (A-S.R) blinded to the patients’ group assignment. Figure 2 shows representative slit lamp images of one patient with subsequent secondary intervention (Figure 2 left) and of another patient without secondary intervention (Figure 2 right) in the upper row and the corresponding binarized AS-OCTA image in the lower row.
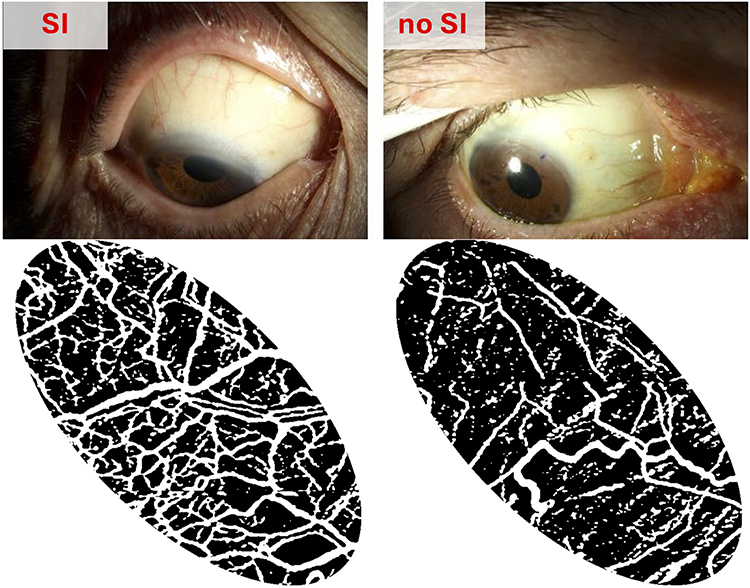 |
Figure 2 Slit-lamp photographs for clinical conjunctival hyperemia grading and corresponding binarized AS-OCTA image for vessel density calculation. Left: representative images of a patient with subsequent secondary intervention. Right: representative images of a patient without secondary intervention. Abbreviation: SI, secondary intervention. |
Statistical Analysis
All values were presented as means ± standard deviation (SD) unless otherwise indicated. Logistic regression modelling was used to evaluate the predictive value of SSVD for the dependent dichotomic variable (“secondary intervention” no “secondary intervention”). A likelihood-ratio test was used to evaluate the significance of the independent variable. Moreover, receiver operating characteristics (ROC) curves, areas under the receiver operating characteristics curves (AUROC) and odds ratios (ORs), together with 95% confidence intervals of AUROCs and ORs were presented. The chi squared trend test was additionally used to analyse whether distribution of the categorial variable “conjunctival hyperemia” is different between the two outcome groups. Pearson bivariate correlation was used to evaluate associations of continuous and categorial variables. No formal sample size calculation was performed due to the exploratory nature of this study and the lack of prior studies on SSVD upon PMI. We, nevertheless, estimated that a similar sample size as in a previous analysis of our group on postoperative bleb vessel density after PMI10 (n = 23) would be sufficient. Prism 10 (GraphPad Software, Boston, MA, USA) was used for statistical testing and graph production.
Results
Study Subjects, Secondary Interventions and Baseline Characteristics
Twenty-five patients with POAG were included in this study. Two patients were excluded from the final analysis: One patient did not complete the study due to withdrawal of consent and in one patient no preoperative AS-OCTA could be performed due to insufficient compliance. Baseline characteristics of the whole cohort and stratified by necessity for secondary intervention (SI) are displayed in Table 1.
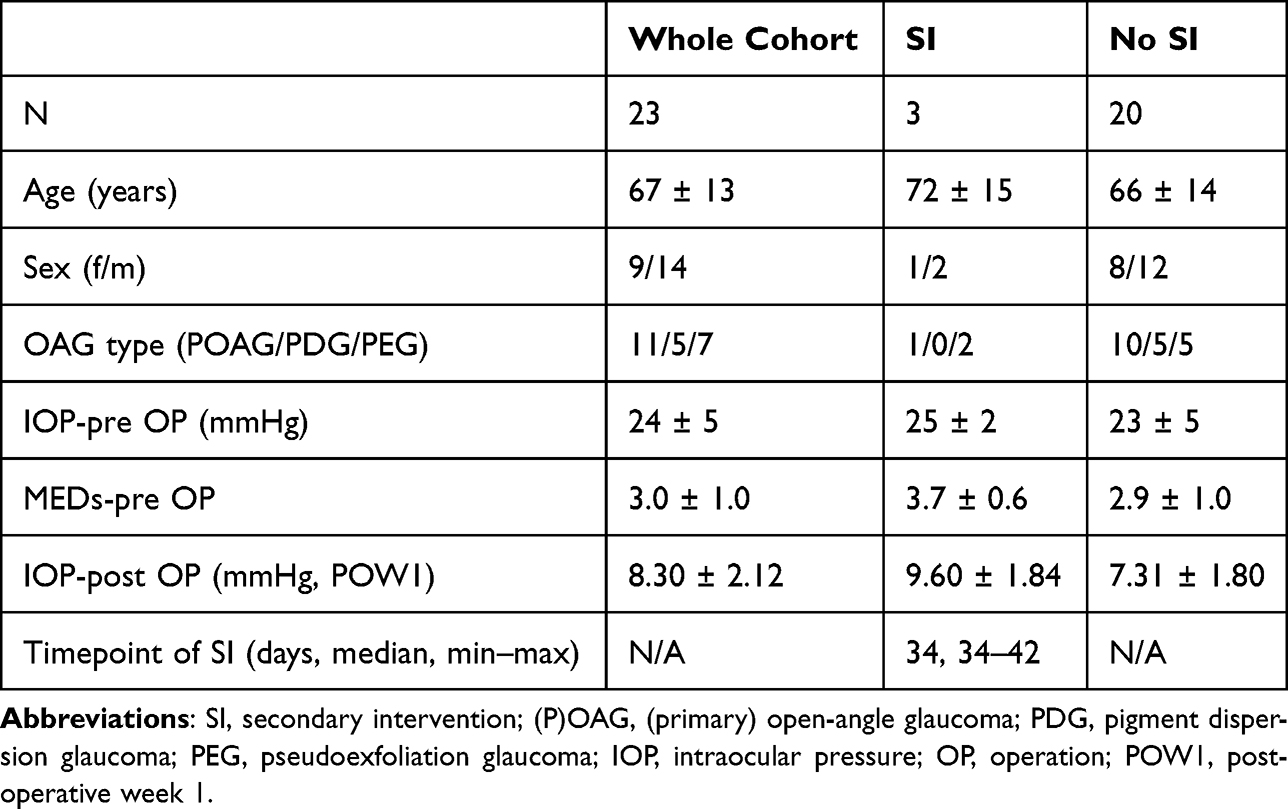 |
Table 1 Baseline characteristics |
Postoperative Course of IOP/MEDs and Necessity for Secondary Intervention
In the whole cohort, IOP was 8.26 ± 2.70, 8.39 ± 2.57, 12.61 ± 8.31, 12.13 ± 5.50, 12.50 ± 6.97 and 12.68 ± 3.76 mmHg 1, 2 and 4 week(s) as well as 2, 3 and 6 months after surgery, respectively. IOPs at the respective timepoints were 8.40 ± 2.85, 8.2 ± 2.85, 9.85 ± 2.78, 10.60 ± 2.72, 10.60 ± 3.35 and 12.15 ± 3.45 mmHg in the “no SI” outcome group and 7.34 ± 1.15, 9.67 ± 1.53, 31.00 ± 10.15, 22.34 ± 9.07, 31.50 ± 3.54 and 18.00 ± 2.83 mmHg in the “SI” outcome group. Apart from one patient at POM6, in whom one MED was initiated, there was no necessity for MEDs in the “no SI” group. In the “SI” group, however, median MEDs count was zero at POW1–4, three at POM2 and POM3 and two at POM6. The time course of IOPs in the two outcome groups is visualized in Figure 3, with black dots representing IOPs in the “no SI” group and red squares representing IOPs in the “SI” group.
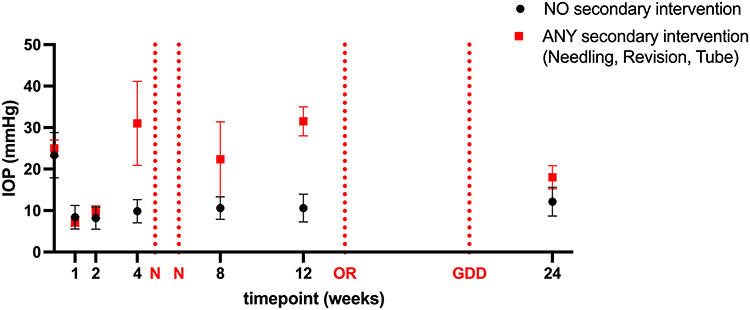 |
Figure 3 Time course of intraocular pressure (IOP) in the two outcome groups. IOPs are presented as mean ± SD. Abbreviations: N, needling; OR, open revision; GDD, glaucoma drainage device. |
In three patients, secondary interventions (three needlings, one open revision, one GDD implantation) were performed during the 6 months follow-up.
In all three patients, the first secondary intervention was a needling, which was performed 34 days (two patients) or 42 days (one patient) after primary surgery. One of the three patients refused further surgery after one unsuccessful needling, in one patient subsequent open revision was performed and in the third patient a GDD implantation (Ahmed valve) was performed. These events are highlighted in Figure 3 with dotted red lines and marked with N (needling), OR (open revision) and GDD (glaucoma drainage device, ie, Ahmed valve).
Association of Preoperative SSVD and HG with Secondary Interventions
Logistic regression modelling revealed that preoperative SSVD was associated with necessity of secondary interventions until 6 months after primary surgery (likelihood-ratio test p-value = 0.0337, OR (95% CI) = 1.193 (1.013–1.524)) and AUROC (95% CI) was 0.8167 (0.5409–1) (Figure 4 left plot). Preoperative HG was, however, not predictive for secondary interventions (likelihood-ratio test p-value = 0.7719, OR (95% CI) = 1.306 (0.1672–8.123), chi squared test for trend p-value = 0.7711, AUROC (95% CI) = 0.5750 (0.2545–0.8955), Figure 4 right plot). Please note that ORs for SSVD and HG are not directly comparable as units are different.
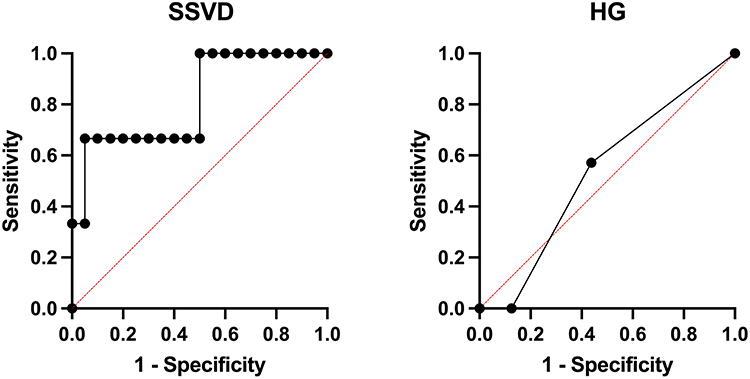 |
Figure 4 Receiver operating characteristics curves for preoperative surgical site vessel density (SSVD) and clinical hyperemia grading (HG). |
Correlation of Preoperative Vascularity Parameters and Their Correlation with Postoperative IOP
Preoperative SSVD and clinical HG did not correlate significantly (r = 0.377, p = 0.075). No significant correlations could be found for preoperative SSVD or clinical HG and IOP at any timepoint or parameter (r between −0.259 and 0.276, p >0.05 for all timepoints). Correlations with IOP are summarized in Table 2.
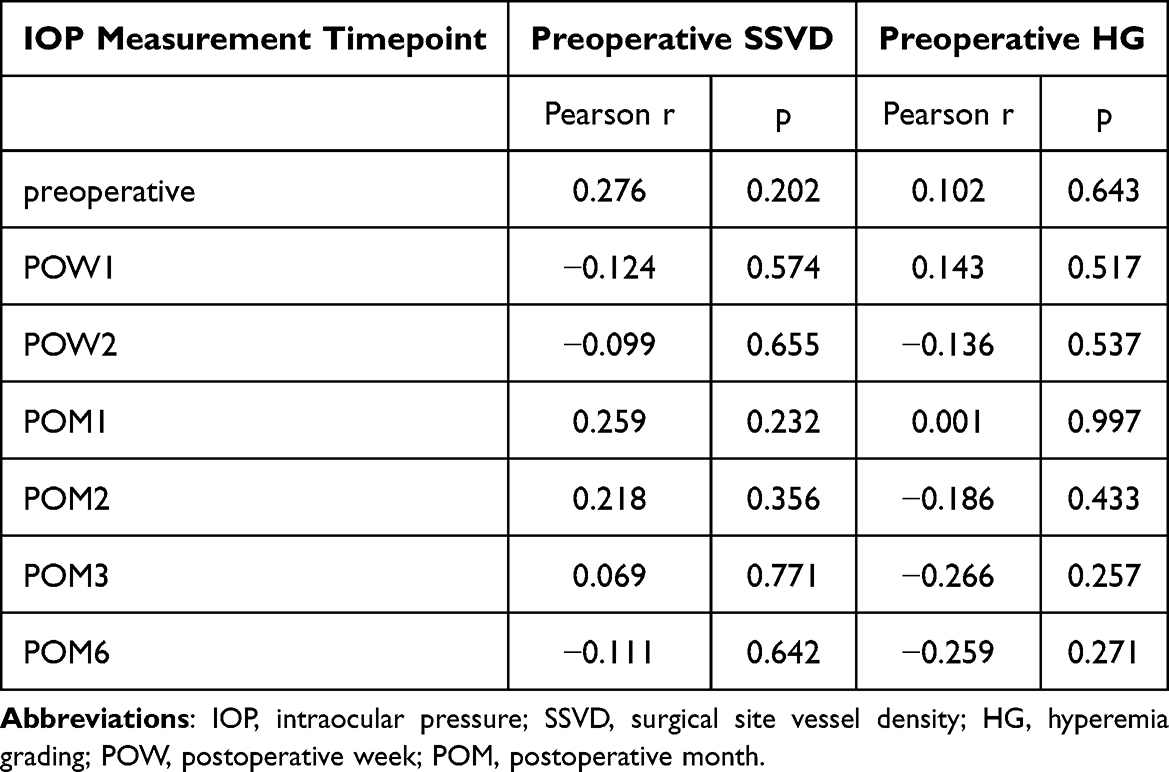 |
Table 2 Correlations of preoperative SSVD or preoperative HG with IOP |
Association of Preoperative MEDs with Secondary Interventions and Preoperative Vascularity Parameters
The number of preoperative MEDs was borderline not predictive for the necessity of secondary interventions (logistic regression LHR-test p-value = 0.079, OR (95% CI) = 6.510 (0.8473–156.5), AUROC (95% CI) = 0.767 (0.4878–1.000)) and it did not correlate with preoperative SSVD or clinical HG (SSVD: r = 0.183, p = 0.402; HG: r = 0.040, p = 0.857). Also, no type of preoperative MED was predictive for necessity for secondary intervention (Fisher’s exact test p-values between 0.538 and 0.999) and none of the types correlated with SSVD/HG (PGA: r = 0.223/0.031, p = 0.307/0.888, BB: r = 0.114/0.139, p = 0.603/0.528, CAI: r = 0.056/0.060, p = 0.801/0.786, AA: r = 0.110/−0.012, p = 0.618/0.957).
Discussion
In this exploratory, prospective, longitudinal study, preoperative surgical site vessel density but not clinical hyperemia grading was found to be a promising biomarker with predictive potential for secondary intervention until 6 months after PMI. No significant correlation was identified between the two preoperative vascularity parameters, and also no correlation to IOP at any timepoint was found.
IOP drop and time course of postoperative IOP as well as number of necessary secondary interventions were compatible with already published data for PMI.25,26
We are aware of two prior AS-OCT studies27,28 and one AS-OCTA study11 evaluating conjunctival properties prior to TE. To the best of our knowledge our study is, however, the first to evaluate preoperative AS-OCTA based biomarkers for their ability to predict surgical outcome after PMI. Mastropasqua et al, using structural AS-OCT, found reduced preoperative stromal, epithelial and full conjunctival thickness to be lower as well as hyperreflectivity to be higher upon surgical failure,27 while Agnifili et al, using a multivariable machine learning-based approach (conventional statistical methods did not identify significant predictors), found increased stromal thickness, higher reflectivity and younger age to be the most important predictors for failure.28 The authors stated that differences in topical therapy may cause the conflicting results,28 as conjunctival thickness seems to also be dependent on substance class specific properties of topical MEDs (eg, stromal atrophy due to prostaglandin analogues).28,29 Therefore, reduced generalizability of this structural thickness parameter may limit its potential as a predictive biomarker.
As increased vascularity is known to be a common feature of inflammation ultimately leading to (susceptibility for) fibrosis and bleb failure,30,31 objective and reproducible biomarkers of vascularity, as assessed in our current study, may be a promising approach. In this context it should be mentioned that preoperative surgical site vessel density was independent of the number and type of topical MEDs in our analysis. Similarly to our results for PMI, Hayek et al found preoperative conjunctival vessel density to be predictive for needling necessity 1 and 6 months after TE.11 Divergent to our results after PMI, Hayek et al11 also found a correlation between preoperative vessel density and pre- and postoperative IOP. We speculate, that one reason for the discrepancy could be differences in included types of glaucoma (OAG vs OAG/ACG/angle-recession glaucoma) as the isolated effect of preoperative conjunctival status on filtration surgery success might be variable. Moreover, also device/procedure specific reasons could play a role in this finding: In fact, although this was previously shown to hold true for TE,7 we did not observe any correlations to postoperative IOPs at any timepoint either in a previously published longitudinal study, in which we found 2 and 4 week’s bleb vessel density to be predictive for secondary interventions until 12 months after PMI.10 Finally, we believe that missing correlation after needling timepoints can be related to successful IOP-lowering following the procedure.
Applicability of objective AS-OCTA preoperative vascularity biomarkers across different types of filtration surgeries as seen for surgical site vessel density in this study is in line with previous data on predictive AS-OCTA based biomarkers of the postoperative phase for surgical success. Indeed, it was shown that postoperative bleb vessel density is both predictive for surgical success after TE7–9 and PMI,10 while this was the case for commonly used structural bleb parameters (bleb wall thickness, total bleb height) only after TE32,33 and not after PMI.34
Lacking predictive value of preoperative hyperemia grading may be attributable to its subjective nature and reduced observability of deeper structures which limit the applicability of clinical grading scores for filtration surgery.35,36 In contrast, AS-OCTA serves as an objective tool to quantify whole tissue vascularity integrating intravascular flow information of both conjunctival and (epi)scleral layers. Concerning the contribution of deeper layers, Luo et al – upon cross-sectional postoperative AS-OCTA based bleb evaluation after TE – identified vessel density in the Tenon’s rather than in superficial bleb layers to be positively correlated with IOP, while vessel densities in all layers were lower in successful blebs.37 This information is, however, hard to interpret as little is known on a potentially differential (patho)physiological role of blood vessels in different bleb layers. One can only speculate that blood vessels in different layers could either have positive or negative effects.
Our current study has several strengths. First of all, the longitudinal design with prospective inclusion of patients should be mentioned. This allowed us to follow patients longitudinally to evaluate the predictive value of preoperative parameters and minimize selection bias on a subject level.
Secondly, by preoperative limbal marking of the surgical site clock hour we ensured AS-OCTA image acquisition took place in the correct region and by defining a standardized ROI location as well as shape/size we increased comparability between study subjects.
Thirdly, motion artefacts are a crucial issue to be dealt with in AS-OCTA, as motion-tracking is not as readily available as in posterior segment OCTA. We, therefore, used a FFT bandpass filter during image postprocessing to reduce their influence on vessel density calculation.
Fourthly, as in our previous study, which evaluated the predictive value of postoperative AS-OCTA measured bleb vessel density for surgical success after PMI,10 we – again – decided against an IOP-based surgical success definition due to various reasons. First of all, although the WGA has published recommendations on IOP-based endpoint definitions, they acknowledge that there is no single IOP value suitable as a universal endpoint and, therefore, advocate for presentation of results using various cut-offs.38 In studies on AS-OCT/A based conjunctival/bleb parameters this is, however, rarely done, leading to a myriad of studies that are poorly comparable. Moreover, we wanted to prevent individual misclassification as surgical failure, only due to exceedance of an arbitrary IOP cut-off. Finally, we believe that this endpoint is well-suited to be used in interventional clinical trials. Such trials are needed to confirm the predictive value of AS-OCT(A) based parameters around filtration surgeries. Furthermore, patients would be allocated to intensified or loosened follow-up schemes based on their AS-OCT(A) biomarkers and these schemes would be compared to standard care. We acknowledge that selection of “necessity for secondary intervention” as endpoint poses a certain risk for subjectivity if precise decision-making criteria for secondary intervention are lacking. We, therefore, meticulously monitored adherence to the above-mentioned predefined decision protocol upon decision-making to offer secondary intervention.
This study has some limitations that warrant discussion. First of all, obviously, the rather small sample-size of 23 analyzed patients should be mentioned. To partly compensate for that we aimed at a homogenous study cohort by including filtration-surgery naïve primary open-angle, pseudoexfoliation and pigment dispersion glaucoma patients only. Moreover, we present significant results, which is indicative of a sufficient sample size to detect effects. We, however, acknowledge that – considering the sample size – borderline results need to be interpreted with caution. Finally, the small number of only three events renders results from logistic regression analysis fragile. Although statistically significant, they should, therefore, be interpreted with the necessary caution due to a certain risk of model overfitting.
Secondly, we decided against separated, depth-resolved analyses but analyzed full-thickness slabs instead. This was mainly due to a lack of readily available segmentation algorithms that are easily implemented in clinical workflows elsewhere, which would hinder generalizability. We balanced these considerations against the possible gain of novel (patho)physiological insights but decided in favor of the simpler protocol.
Additionally, due to the exploratory nature of this analysis, assessment of SSVD was performed by only one author (MK) experienced in quantitative AS-OCTA analysis and no formal analysis of intra- and inter-observer variability was performed. While we regard the risk of marked variability as low due to the above-mentioned standardized and objective workflow, intra- and interclass correlation coefficients of SSVD should be assessed in future large-scale studies.
Finally, as an observational study, this investigation cannot answer the question of whether AS-OCTA-measured vessel density-based decision making (eg, higher antifibrotic concentration in high vessel density cases, looser follow-up intervals, or lower antifibrotic concentration in low vessel density cases) enhances surgical success and/or reduces rate of complications and, therefore, larger scale interventional trials are needed.
Conclusions
In conclusion, in this exploratory analysis, preoperative surgical site vessel density was predictive for secondary intervention until 6 months after PMI, while no such pattern could be found for preoperative clinical hyperemia grading. No correlation with IOP at any timepoint was found for surgical site vessel density or hyperemia grading. This study adds to the body of evidence that AS-OCTA measured vessel density could be a promising predictor for surgical success of filtration surgery, with flexible applicability, both with respect to the timepoint relative to surgery (preoperatively and early postoperative phase) and the type of surgery (TE and PMI). Larger studies are necessary to confirm our promising finding and interventional trials are needed to evaluate whether vessel density-based clinical decision making enhances clinical outcomes after filtration surgery.
Data Sharing Statement
The data presented in this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Approval for this single-center study was obtained from the Ethic Committee of the Johannes Kepler University (EC-No.: B-142-17). We adhered to the tenets of the Declaration of Helsinki during all study-related procedures. Before study inclusion, written informed consent was given by every patient.
Acknowledgments
Supported by Johannes Kepler University Open Access Publishing Fund and the Federal State Upper Austria.
Funding
No funding was received for this study.
Disclosure
M.K.: AbbVie (Honorarium). C.A.S.: Elios Vision (Research Support, Honorarium, Travel Support), Bausch&Lomb (Honorarium), AbbVie (Honorarium), Santen (Honorarium), Zeiss (Honorarium), Thea Pharma (Honorarium). The other authors have no competing interests to declare for this work.
References
1. Cairns JE. Trabeculectomy. Preliminary report of a new method. Am J Ophthalmol. 1968;66(4):673–10. doi:10.1016/0002-9394(68)91288-9
2. Pinchuk L, Riss I, Batlle JF, et al. The development of a micro-shunt made from poly(styrene-block-isobutylene-block-styrene) to treat glaucoma. J Biomed Mater Res B Appl Biomater. 2017;105(1):211–221. doi:10.1002/jbm.b.33525
3. Pinchuk L, Riss I, Batlle JF, et al. The use of poly(styrene-block-isobutylene-block-styrene) as a microshunt to treat glaucoma. Regen Biomater. 2016;3(2):137–142. doi:10.1093/rb/rbw005
4. Lewis RA. Ab interno approach to the subconjunctival space using a collagen glaucoma stent. J Cataract Refract Surg. 2014;40(8):1301–1306. doi:10.1016/j.jcrs.2014.01.032
5. Schlenker MB, Gulamhusein H, Conrad-Hengerer I, et al. Efficacy, safety, and risk factors for failure of standalone ab interno gelatin microstent implantation versus standalone trabeculectomy. Ophthalmology. 2017;124(11):1579–1588. doi:10.1016/j.ophtha.2017.05.004
6. Marolo P, Reibaldi M, Fallico M, et al. Reintervention rate in glaucoma filtering surgery: a systematic review and meta-analysis. Eur J Ophthalmol. 2022;32(5):2515–2531. doi:10.1177/11206721221093828
7. Yin X, Cai Q, Song R, He X, Lu P. Relationship between filtering bleb vascularization and surgical outcomes after trabeculectomy: an optical coherence tomography angiography study. Graefes Arch Clin Exp Ophthalmol. 2018;256(12):2399–2405. doi:10.1007/s00417-018-4136-0
8. Seo JH, Lee Y, Shin JH, Kim YA, Park KH. Comparison of conjunctival vascularity changes using optical coherence tomography angiography after trabeculectomy and phacotrabeculectomy. Graefes Arch Clin Exp Ophthalmol. 2019;257(10):2239–2255. doi:10.1007/s00417-019-04412-0
9. Seo JH, Kim YA, Park KH, Lee Y. Evaluation of functional filtering bleb using optical coherence tomography angiography. Transl Vis Sci Technol. 2019;8(3):14. doi:10.1167/tvst.8.3.14
10. Schneider S, Kallab M, Murauer O, et al. Bleb vessel density as a predictive factor for surgical revisions after Preserflo Microshunt implantation. Acta Ophthalmol. 2024;102(5):e797–e804. doi:10.1111/aos.16642
11. Hayek S, Labbe A, Brasnu E, Hamard P, Baudouin C. Optical coherence tomography angiography evaluation of conjunctival vessels during filtering surgery. Transl Vis Sci Technol. 2019;8(4):4. doi:10.1167/tvst.8.4.4
12. Agnifili L, Sacchi M, Figus M, et al. Preparing the ocular surface for glaucoma filtration surgery: an unmet clinical need. Acta Ophthalmol. 2022;100(7):740–751. doi:10.1111/aos.15098
13. Broadway DC, Grierson I, O’Brien C, Hitchings RA. Adverse effects of topical antiglaucoma medication. I. The conjunctival cell profile. Arch Ophthalmol Chic IL 1960. 1994;112(11):1437–1445. doi:10.1001/archopht.1994.01090230051020
14. Broadway DC, Grierson I, O’Brien C, Hitchings RA. Adverse effects of topical antiglaucoma medication. II. The outcome of filtration surgery. Arch Ophthalmol Chic IL 1960. 1994;112(11):1446–1454. doi:10.1001/archopht.1994.01090230060021
15. Boimer C, Birt CM. Preservative exposure and surgical outcomes in glaucoma patients: the PESO study. J Glaucoma. 2013;22(9):730–735. doi:10.1097/IJG.0b013e31825af67d
16. Chamard C, Larrieu S, Baudouin C, Bron A, Villain M, Daien V. Preservative-free versus preserved glaucoma eye drops and occurrence of glaucoma surgery. A retrospective study based on the French national health insurance information system, 2008-2016. Acta Ophthalmol. 2020;98(7):e876–e881. doi:10.1111/aos.14410
17. Gwynn DR, Stewart WC, Pitts RA, McMillan TA, Hennis HL. Conjunctival structure and cell counts and the results of filtering surgery. Am J Ophthalmol. 1993;116(4):464–468. doi:10.1016/s0002-9394(14)71405-9
18. Mastropasqua R, Fasanella V, Brescia L, et al. In vivo confocal imaging of the conjunctiva as a predictive tool for the glaucoma filtration surgery outcome. Invest Ophthalmol Vis Sci. 2017;58(6):BIO114–BIO120. doi:10.1167/iovs.17-21795
19. Agnifili L, Fasanella V, Mastropasqua R, et al. In vivo goblet cell density as a potential indicator of glaucoma filtration surgery outcome. Invest Ophthalmol Vis Sci. 2016;57(7):2928–2935. doi:10.1167/iovs.16-19257
20. European Glaucoma Society. European glaucoma society terminology and guidelines for glaucoma, 5th edition. Br J Ophthalmol. 2021;105(Suppl 1):1–169. doi:10.1136/bjophthalmol-2021-egsguidelines
21. Schindelin J, Arganda-Carreras I, Frise E, et al. Fiji: an open-source platform for biological-image analysis. Nat Methods. 2012;9(7):676–682. doi:10.1038/nmeth.2019
22. Gan J, Sng CCA, Ke M, et al. Anterior segment optical coherence tomography angiography following trabecular bypass minimally invasive glaucoma surgery. Front Med. 2022;9:830678. doi:10.3389/FMED.2022.830678
23. Otsu N. A threshold selection method from gray-level histograms.
24. Wei S, Wang Y, Shi F, Sun S, Li X. Developing a deep learning model to evaluate bulbar conjunctival injection with color anterior segment photographs. J Clin Med. 2023;12(2):715. doi:10.3390/jcm12020715
25. Beckers HJM, Aptel F, Webers CAB, et al. Safety and effectiveness of the PRESERFLO(R) MicroShunt in primary open-angle glaucoma: results from a 2-year multicenter study. Ophthalmol Glaucoma. 2022;5(2):195–209. doi:10.1016/j.ogla.2021.07.008
26. Baker ND, Barnebey HS, Moster MR, et al. Ab-Externo MicroShunt versus trabeculectomy in primary open-angle glaucoma: one-year results from a 2-year randomized, multicenter study. Ophthalmology. 2021;128(12):1710–1721. doi:10.1016/j.ophtha.2021.05.023
27. Mastropasqua L, Brescia L, Oddone F, et al. Conjunctival thickness as a predictive imaging biomarker for the glaucoma filtration surgery outcome: an optical coherence tomography study. Clin Exp Ophthalmol. 2020;48(9):1192–1200. doi:10.1111/ceo.13857
28. Agnifili L, Figus M, Porreca A, et al. A machine learning approach to predict the glaucoma filtration surgery outcome. Sci Rep. 2023;13(1):18157. doi:10.1038/s41598-023-44659-6
29. Tekin S, Seven E, Batur M. Evaluation of antiglaucomatous drops on conjunctival thickness in patients with primary open-angle glaucoma. J Ocul Pharmacol Ther. 2019;35(4):216–222. doi:10.1089/jop.2018.0124
30. Amadeu T, Braune A, Mandarim-de-Lacerda C, Porto LC, Desmoulière A, Costa A. Vascularization pattern in hypertrophic scars and keloids: a stereological analysis. Pathol Res Pract. 2003;199(7):469–473. doi:10.1078/0344-0338-00447
31. Nadella V, Mohanty A, Sharma L, et al. Inhibitors of apoptosis protein antagonists (Smac mimetic compounds) control polarization of macrophages during microbial challenge and sterile inflammatory responses. Front Immunol. 2017;8:1792. doi:10.3389/fimmu.2017.01792
32. Waibel S, Spoerl E, Furashova O, Pillunat LE, Pillunat KR. Bleb morphology after Mitomycin-C augmented trabeculectomy: comparison between clinical evaluation and anterior segment optical coherence tomography. J Glaucoma. 2019;28(5):447–451. doi:10.1097/IJG.0000000000001206
33. Narita A, Morizane Y, Miyake T, Seguchi J, Baba T, Shiraga F. Characteristics of early filtering blebs that predict successful trabeculectomy identified via three-dimensional anterior segment optical coherence tomography. Br J Ophthalmol. 2018;102(6):796–801. doi:10.1136/bjophthalmol-2017-310707
34. Ibarz Barbera M, Hernandez-Verdejo JL, Bragard J, et al. Bleb geometry and morphology after Preserflo Microshunt surgery: risk factors for surgical failure. PLoS One. 2023;18(6):e0286884. doi:10.1371/journal.pone.0286884
35. Hoffmann EM, Herzog D, Wasielica-Poslednik J, Butsch C, Schuster AK. Bleb grading by photographs versus bleb grading by slit-lamp examination. Acta Ophthalmol. 2020;98(5):e607–e610. doi:10.1111/aos.14335
36. Wells AP, Ashraff NN, Hall RC, Purdie G. Comparison of two clinical Bleb grading systems. Ophthalmology. 2006;113(1):77–83. doi:10.1016/j.ophtha.2005.06.037
37. Luo M, Zhu Y, Xiao H, et al. Characteristic assessment of angiographies at different depths with AS-OCTA: implication for functions of post-trabeculectomy filtering bleb. J Clin Med. 2022;11(6):1661. doi:10.3390/jcm11061661
38. Shaarawy T, Grehn F. Guidelines on design and reporting of glaucoma surgical trials. Kugler Publications; 2009.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.