Back to Journals » Orthopedic Research and Reviews » Volume 12
Preoperative Planning and the Use of Free Available Software for Sagittal Plane Corrective Osteotomies of the Lumbar Spine in Ankylosing Spondylitis
Authors van Royen BJ ![]()
Received 11 August 2020
Accepted for publication 5 November 2020
Published 17 November 2020 Volume 2020:12 Pages 171—182
DOI https://doi.org/10.2147/ORR.S275860
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Barend J van Royen
Department of Orthopaedic Surgery, Amsterdam UMC, Vrije Universiteit and University of Amsterdam, Amsterdam Movement Sciences, Amsterdam, the Netherlands
Correspondence: Barend J van Royen
Department of Orthopaedic Surgery Amsterdam UMC, Vrije Universiteit and University of Amsterdam, Amsterdam Movement Sciences, Meibergdreef 9, 1105 AZ, Amsterdam, the Netherlands
Tel +31 20 56 62672
Fax +31 20 56 69117
Email [email protected]
Background: Ankylosing spondylitis (AS) may cause a severe rigid thoracolumbar kyphotic deformity (TLKD) that leads to considerable disturbances of posture and spinal balance. In few patients, a corrective osteotomy of the lumbar spine may be considered. Preoperative planning of a lumbar osteotomy for correction of a severe TLKD due to AS is important to correct patient’s sagittal balance and view angle. There is a need for accurate preoperative planning that can be used easily in daily practice.
Methods: The basic biomechanical and mathematical principles of preoperative planning for correction of a TLKD due to AS are described. A search was performed for free available computer programs that can be used for pre-operative planning of spinal osteotomies in AS. Finally, the use of these computer programs is illustrated and described.
Results: Sagittal balance is measured on a standing lateral full-length radiograph of the spine. The assessment of the pelvic parameters (PI, PT, SS) in conjunction with sagittal vertical axis (SVA) and chin-brow-to-vertical angle (CBVA) provides a comprehensive picture of the sagittal spinal alignment and compensatory mechanisms of the patient. The relation between the level of lumbar osteotomy and the amount of correction needed can be calculated with different elementary trigonometric equations. Two free available computer programs, ASKyphoplan and Surgimap, are illustrated and described that can be used for pre-operative planning of spinal osteotomies in AS.
Conclusion: Preoperative planning of the lumbar osteotomy in AS involves assessment of the combined effect of location of the osteotomy, amount of bone resection, SVA, CBVA, and pelvic parameters. Two free available computer programs, ASKyphoplan and Surgimap, are easy to use in clinical practice to predict postoperative sagittal balance of lumbar osteotomies in patients with severe TLKD due to AS.
Keywords: preoperative planning, lumbar osteotomy, ankylosing spondylitis, computer programs, kyphosis
Introduction
Ankylosing spondylitis (AS), or axial spondyloarthritis (axSpA), is a chronic inflammatory disease that primarily affects the spine and sacroiliac joints, causing pain, stiffness, and a progressive severe rigid thoracolumbar kyphotic deformity (TLKD). The TLKD can be so extreme that the patient cannot sit, stand, or lie in comfort. In severe cases, patients may be unable to look above the level of the horizon, causing problems in daily activities, like communication, participating in traffic, and getting something above their head. Additionally, patients with a severe TLKD may show intestinal and respiratory problems of various degrees as a result of compression by the rib margin on the abdominal viscera and secondary decreased diaphragmatic respiration on which these patients often depend.
In few patients, a corrective osteotomy of the lumbar spine may be considered to correct the postural balance and view angle. These osteotomies proved to be advantageous for numerous patients.1 However, occasional complications and poor results have diminished their acceptance by rheumatologists and orthopaedic surgeons. This is not surprising, since up to now there were many unsolved questions regarding posture and balance in patients with AS, and there were no standardized methods for assessing the severity of the spinal sagittal deformity. In addition, no accurate preoperative planning, including the degree of correction required, nor knowledge of the level to operate on, was available.
Over the past two decades, however, both the surgical technique and knowledge of preoperative assessment of the fixed sagittal deformity of the spine in AS have undergone significant evolution.2 The TLKD is best corrected by a lordosing osteotomy in the lumbar spine, where the capacious spinal canal reduces the risk of perioperative injury to the cauda equine. In addition, the overall correction is greatest when the intervention is performed at the lowest possible level of the lumbar spine. Thoracic osteotomy is not preferred as the primary osteotomy because of the vulnerability of the narrow, midthoracic spinal cord to perioperative injury. Besides, the thoracic correction is limited by ankylosis of the costovertebral joints. Many surgical techniques have been described to correct the lumbar spine in AS.1 Currently, a closing wedge osteotomy (CWO), or pedicle subtraction osteotomy (PSO), of the lumbar spine has been recognized as the preferred surgical technique used to restore the thoracolumbar kyphosis, sagittal balance and view angle in patients with AS. This procedure has been used in clinical practice for more than 70 years, and its value in correcting the spinal deformity in AS has been well established.1,3–5 The biomechanical advantages of a CWO or PSO technique have been recently demonstrated through cadaveric tests6,7 and computer-based models.8 In addition, the understanding of the sagittal deformity and subsequence the importance of adequate preoperative deformity planning in AS has been recognized. First, the significance of the effect of the lower extremities in balance control.9 Second, the introduction of the pelvic parameters, including the pelvic incidence (PI), pelvic tilt (PT) and sacral slope (SS), in addition to the measurement of the sagittal vertical axis (SVA) for the assessment of sagittal plane deformities,10,11 and third, the effect of a lumbar osteotomy on the correction of the view angle as measured by the chin-brow-to-vertical angle (CBVA).12–14
The focus of surgical correction of spinal deformity in AS has shifted to not only restoring kyphosis but also re-establishing sagittal balance, placing the pelvis in a neutral position and restore normal range of movement in the hip joints, and correction of the view angle (Figure 1). Careful assessment of the sagittal alignment, spinal parameters, are fundamental for surgical planning and effective pre-operative patient counselling in patients with TLKD caused by AS.
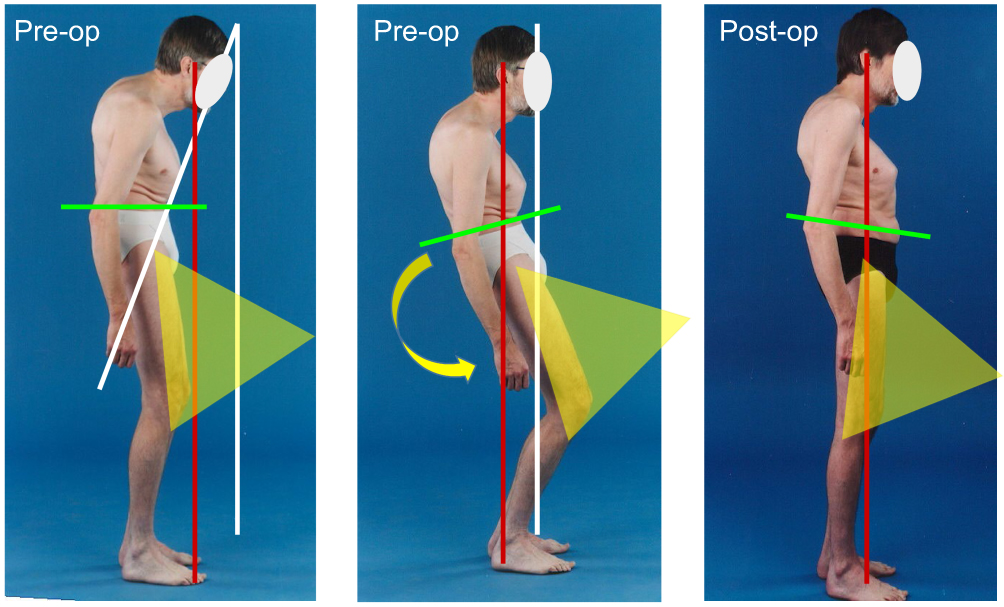 |
Figure 1 The aims of surgery in AS are to restore the patients’ ability to see ahead to the horizon, to restore the balance of the spine, to place the pelvis in a neutral position and restore normal range of movement in the hip joints. |
The aim of this article is to describe the basic biomechanics of preoperative planning for correction of a TLKD due to AS and to incorporate mathematical methods described in the past and to describe the current free available computer programs of deformity planning that can be used in daily practice.
Methods
The basic biomechanical and mathematical principles of preoperative planning for correction of a TLKD due to AS are described. Parameters are discussed that assess sagittal balance, view angle and the position of pelvis and the lower extremities. Mathematical methods used in the past are described and a search was performed for free available computer programs that can be used for pre-operative planning of spinal osteotomies in AS. Finally, the use of these computer programs is illustrated and described.
Biomechanical Principles of Preoperative Planning
A normal sagittal balance in upright position is acquired when a biomechanical plumb line from the collective center of mass (COM) of trunk, head, upper extremities and any external weight, intersects the connective axis between the femoral heads and the supporting area of the feet. By standing and walking in balanced spinal alignment, a minimal use of muscular energy is necessary. Unfortunately, it is very difficult to locate exactly the COM in an individual patient with a TLKD due to AS. The exact position of the COM depends on the distribution of mass and thus on the shape of the spine, the distribution of fat, muscles and bowels, and the position of head and arms. In clinical practice, it is not feasible to determine the exact position of the COM in patients with AS.
Therefore, in clinical practice, sagittal balance is measured on a standing lateral full-length radiograph of the spine. In normal standing upright balance, the sagittal plane curves of the spine tend to balance the patient in such a way that the head, trunk, and pelvis are lined up vertically by segmental mobility of the spine, the position of the pelvis, and the position of the hip joints.15,16 However, patients with AS lack vertebral segmental compensation due to a complete ankylosed spine. In order to compensate for the downward view angle and the sagittal unbalance, the patient’s only option is a backward rotation of the pelvis with maximal extension of the hips, which is accompanied by flexion of the knees and ankles.9 This results in a fatiguing standing position with high muscular stress especially of the upper and lower muscles of the legs.
Sagittal balance on a lateral full-spine radiograph is defined by the sagittal vertical axis (SVA) and measured by the horizontal distance between the posterior edge of the sacral endplate and the plumb line from C7. But, measurements of the sagittal SVA in patients with a severe TLKD are insufficient for adequate assessment of sagittal balance in AS. In order to compensate for the severe TLKD and the sagittal unbalance in AS, the SVA is influenced by backward rotation of the pelvis with maximal extension of the hips and flexion of the knees and ankles. In addition, SVA translations during standing radiographic analysis were found to depend on small changes of the angles of the hip, knee, and ankle joints in a model with a fixed spine due to ankylosing spondylitis.9 This indicates that measurements of the sagittal SVA alone is insufficient for complete appreciation of sagittal plane deformities in AS.
Recent studies have shown that the pelvis plays a critical role in regulating spinal alignment and compensating for spinal malalignment. The assessment of the three basic pelvic parameters, including pelvic incidence (PI), sacral slope (SS) and pelvic tilt (PT), in conjunction with SVA provides a more comprehensive picture of the sagittal spinal alignment.10,11 The three basic pelvic parameters show a geometrical relationship where PI is equal to the sum of PT and SS. PI reflects the individual and constant morphological parameter. PT and SS are positional or compensatory mechanisms which are employed to maintain functional sagittal balance. As the COM, and therefore the SVA, shifts anteriorly in patients with a severe TLKD due to AS, the pelvis tends to retrovert as a compensatory mechanism, thereby decreasing SS and increasing PT in an attempt to maintain sagittal balance.
While spinal balance is related to the relative position of the SVA, view angle is related to the sagittal curvature. Functional restoration of the view angle is the most important reason for surgical intervention in AS patients.13,14,17,18 Currently, the most common way to measure the view angle is the assessment of the chin-brow to vertical angle (CBVA). The CBVA, is a non-invasive measurement of the TLKD and can be measured clinically, or on a photograph, or on a radiograph that includes the cranium in standing lateral position. The CBVA is defined as the angle between a line drawn through the chin and the brow to the vertical.12–14 Optimal CBVA for sagittal view angle in ankylosing spondylitis kyphosis has been shown to be between 10 and 20 degrees.12
The relation between the level of osteotomy in the lumbar spine and the amount of correction needed in patients with AS has been discussed extensively. A more caudal osteotomy level leads to a greater amount of correction of balance; however, the correction of CBVA is independent of the level of osteotomy3,14,19 (Figure 2).
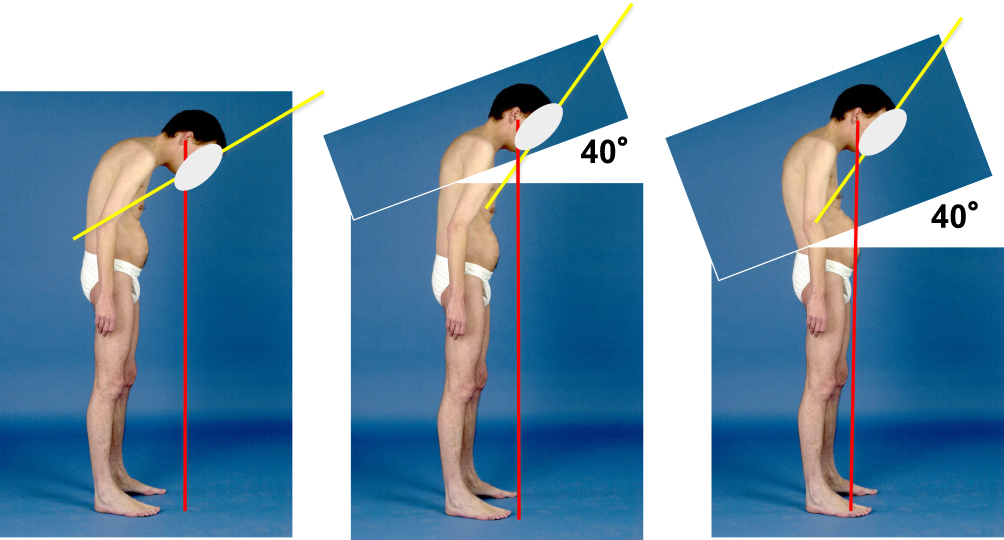 |
Figure 2 The effect of a spinal osteotomy on the correction of the horizontal gaze, measured by the chin-brow-to-vertical angle (CBVA), is equal to the osteotomy angle, irrespective of the osteotomy level. However, the effect of a spinal osteotomy on the sagittal balance of the spine depends on both the osteotomy angle and the level of osteotomy simultaneously. The correction of the sagittal balance is maximal when the intervention is performed at the lowest possible level of the lumbar spine. |
Recently, it has been shown that the amount of SVA correction and correction of the pelvic tilt (PT) not only depends on the level of osteotomy but also on the ratio of closure (RoC) within the vertebral body.20 The RoC is defined by the percentage of the upper part closure (truncal closure) divided by the percentage of the lower part (pelvis closure) of the resected vertebral body, and thereby creating a vector inside the wedge resection. A CWO, or PSO, therefore, can be performed in a truncal dominant correction (eg 60/40), proportional correction (50/50), or pelvic dominant correction (eg 40/60). A pelvic dominant correction resulted in more correction of the SVA and less correction of the PT.20
History of Pre-Operative Planning of Spinal Osteotomies in AS
In the past, there was no biomechanical and mathematical preoperative planning technique available, nor knowledge of the level to operate on. The classical method includes a radiograph trace and cut-out method. In addition, deformity planning at that time had been performed with rule-of-the-thumb methods.3 Preoperative clinical analysis of the TLKD in AS was done as follows: the horizontal gaze was corrected to as close to normal as possible by asking the standing patient to bend the knees with the hip joints extended. The lumbar osteotomy angle was estimated by dividing the knee angle into halves. In daily practice, however, the surgeon strived for maximal correction within the anatomical limitations of the vertebral body.3 However, aiming for maximal correction achievable obviously create the risk of over-correction.21 Kim et al in 2002 classified his results by three types of correction: balanced correction, over correction, and under correction.4 However, since in AS the spine is a rigid beam of bone, an osteotomy can be planned with elementary trigonometric equations. Several methods of preoperative planning have been described to predict the effect of a spinal osteotomy on the correction of the sagittal balance and view angle in AS.
Van Royen et al in 2000 described a biomechanical and mathematical method that considered the compensation mechanism of the pelvis, the planned correction angle, the level of osteotomy and the effect of the osteotomy on the correction of the SVA and CBVA.14 It was assumed that the normal SS defines the neutral position of the pelvis. The mean normal SS is approximately 40 degrees. Hence, if the sacral endplate is corrected to 40 degrees with the horizontal, it means that the pelvic retroversion has been corrected. This method is not a really individualized because the SS was defined at the same angle for every patient. However, individualization is possible by adjusting the SS. When the pelvis is placed per an aimed SS, the uncompensated SVA for the individual patient can be calculated. The combined use of the SVA, CBVA and SS as biomechanical parameters gives information on the level of osteotomy and the amount of lumbar correction in relation to both the SVA and the CBVA. Unfortunately, the mathematical equations promoted are not easily used in daily practice.
Ondra et al in 2006 described a simple mathematical measurement, by using the tangent function, to predict the correction needed from a CWO or PSO to achieve optimal sagittal spinal alignment postoperatively.22 This mathematical method, however, only included the correction of the rigid spine and did not account for the level of osteotomy and the position of the pelvis.
Kim et al in 2006 proposed a formula based on the sagittal Cobb angle, recommending that the difference between lumbar lordosis (LL) and thoracic kyphosis (TK) should be more than 20 degrees (ie, LL > TK + 20 degrees).23 TK was measured using the Cobb angle between T5–T12 and LL was measured between T12 and S1. This approach, however, did not include the position of the pelvis and the level of osteotomy.
Min et al in 2007 described a planning method using the whole body kyphosis angle (WBKA) measured on a preoperative clinical photographs at the level of the umbilicus, to calculate clinically the amount of correction needed.17 In addition, the thoracic kyphosis, lumbar lordosis, total spinal kyphosis, and the sacral slope (SS) were measured on the standing whole spine radiographs. This approach included the CBVA and tight angle correction but did not take into account the level of surgery and pelvic parameters, and thus fails to predict the extra correction needed on patients with decreased SS or increased PT.
Rose et al in 2009 modified the above mentioned Kim’s formula, adding pelvic parameters, and concluded that PI and TK can predict the LL necessary to correct sagittal balance with the formula PI + TK + LL < 45 degrees.24 However, since the SS or PT correction needed were not included in this formula, patients with high PT (or low SS) could be undercorrected based on this formula. In addition, the level of osteotomy was not included in the formula.
Schwab et al in 2009 proposed the formula LL = PI ± 9 degrees.10,25 They noted that this formula was only applicable to patients with decreased LL, but relative normal thoracic kyphosis, since this formula also fails to predict the extra correction needed on patients with decreased SS or increased PT.
Le Huec et al in 2011 proposed a mathematical method named FBI (Full Balance Integrated), that is based on a global analysis of the full body balance, to calculate the amount of correction needed for a given patient.26 The correction angle is calculated by the formula: FBI angle of correction = C7TA + FOA + PTCA, where C7TA is the angle of C7 translation, FOA is the angle of femur obliquity, and PTCA is pelvic tilt compensation angle. This technique again was difficult to use in daily practice and did not include the level of osteotomy.
For patients with hyper kyphosis and retroversion of the pelvis, Lafage et al in 2011 proposed two separate formulas to predict postoperative PT and SVA.27 The predicted PT is dependent on LL and PI, and is calculated by: PT = 1.14 + 0.71 x PI – 0.52 x (Maximal lumbar lordosis LL) –0.19 x (Maximal thoracic kyphosis TK). The post-operated SVA is predicted by another formula: SVA = –52.87 + 5.90 x PI –5.13 x (Maximal LL) –4.45 x PT – 2.09 x (Maximal TK) + 0.566 x (Age). Despite the inclusion of spinopelvic parameters and the interesting integration of patient age into the calculation, the promoted mathematical equations are not easily used in daily practice for surgical planning for correction of spinal sagittal malalignment.
Song et al in 201328 modified this method for calculating the angle required for spinal osteotomy in AS after the introduction of the pelvic parameter concept, adding PI and PT to the sacral end plate angle or SS. They promoted a decrease of the PT to the individual’s normal value, instead of increasing the SS to the normal position. The individual normal PT was defined according to preoperative PI, which was given by the mathematical equation: PT = 0.37 × PI – 7. In addition, they defined the plumb line of the hilus pulmonis, instead of the C7 plumb line, as the gravity SVA. The osteotomy angle was planned and calculated at the apex vertebra of the sagittal deformity by the angle between the hilus pulmonis and the calculated individual PT.
Free Available Computer Programs for Pre-Operative Planning of Spinal Osteotomies in AS
For adequate pre-operative surgical planning of a lumbar osteotomy in AS, the global sagittal kyphosis, biomechanical aspects, mathematical equations and all compensation mechanism have to be taken into account. Unfortunately, all aforementioned biomechanical principles and mathematical equations used to predict postoperative sagittal balance and view angle (PT, SVA and CBVA) are not easy to use in daily practice. Though the use of computer-based techniques for planning corrective spinal osteotomies in AS will simplify this task. Despite some commercially available add-on planning software packages that can be used in combination with a local picture archiving and communication (PACS) system, for example “spineEOS software” or “Sectra Orthopaedic Package”, there is a need for independent and free available planning software. Currently, there are two free available computer programs available, ASKyphoplan and Surgimap, for pre-operative planning of spinal osteotomies in AS. Both computer programs include the position of the pelvis in the pre-operative planning to predict postoperative sagittal balance of spinal osteotomies in these patients.
ASKyphoplan
ASKyphoplan29 is a free available computer program (www.askyphoplan.com) that was first described and published in 2007. It analyses and visualizes the planning procedure for sagittal plane corrective osteotomies of the lumbar spine in AS based on the mathematical principles published in 2000 by Van Royen et al.14 The program is developed only for deformity planning in patients with a fixed spine due to AS. The relationship between the planned correction angle, level of osteotomy and sagittal balance defined by the SVA are coupled into the program. In addition, the effect of the osteotomy on the correction of the view angle (CBVA) in degrees is recorded. The procedure of this basic, but user-friendly, sagittal alignment tool has been described in detail.29 After uploading a lateral full-spine radiograph, five consecutive steps are followed: “Calibration”, “Draw”, “Set SEA”, “Calculate”, and “Report”.
Calibration: This is used to convert pixels into millimeters. Two marks are placed on the grid of the film that define the distance in millimeters for calibration. The computer then calibrate distances on a scanned radiographic film.
Draw: This creates a coordinate system. The posterior superior corner of the sacrum (PSCS), and the actual (compensated) sacral end plate angle (SEA) or SS can be drawn on the radiograph. The center of body C7 is marked, and the compensated plumb line from C7 appears in millimeters.
Set SEA (or SS): This will rotate and project the radiograph onto the coordinate system with the SEA (SS) at the desired angle. In healthy patients, the SS makes an angle of approximately 40 degrees with the horizon on a standing lateral radiographic projection. With the normal SS of 40 degrees, the hip joints are in the zero position. Thus allowing for small compensatory movements of the pelvis.
Calculate: The computer program calculates and visualizes the relationship between the correction angle, location of the osteotomy, and the sagittal balance. Using the “visibility” bar, the virtual post-operative radiograph can be visualized (Figure 3). By varying the level of the osteotomy and correction angle, its effect on the SVA and CBVA can be visualized and tested until desired parameters are obtained.
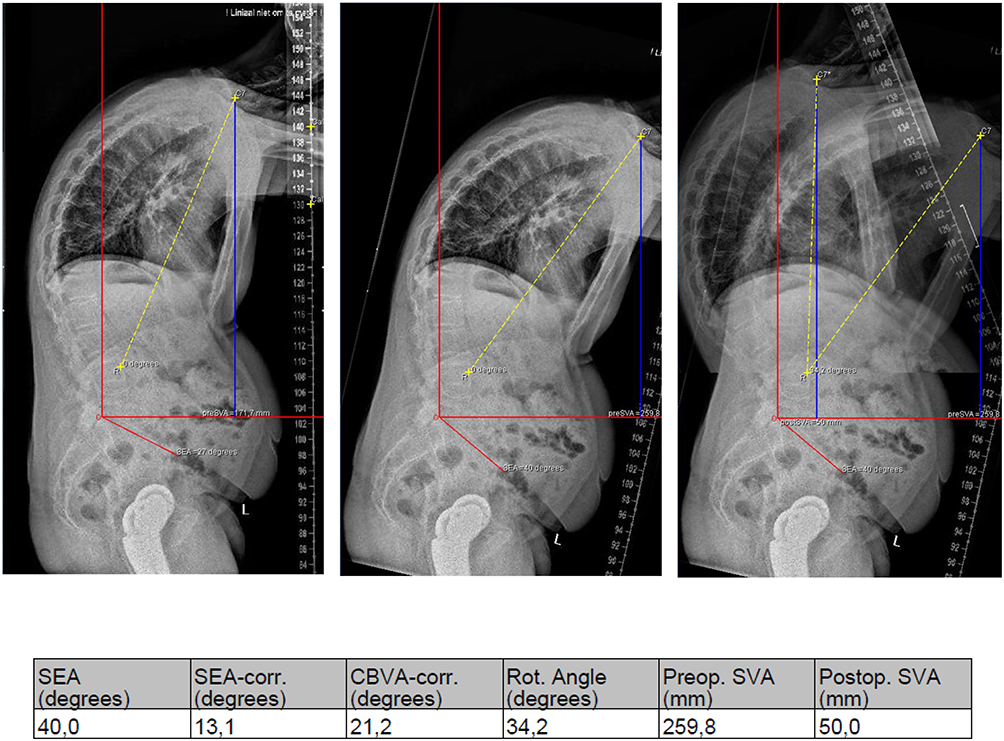 |
Figure 3 Pre-operative and post-planning images of the ASKyphoplan software. Preoperative ASKyphoplan report showing a preoperative SEA (SS) of 27° and SVA of 172 mm. Rotation of the radiograph onto the coordinate system with the SEA at 40° results in an SVA (SEA 40) of 261 mm. A 34° osteotomy at L4 predicts the postoperative SVA (SEA 40) of 50 mm. The predicted CBVA correction is 21°. |
Report: The preoperative deformity planning, calculation and visualization of the osteotomy can be saved as a PDF file for documentation.
Alterations for the normal SEA or SS from 40 degrees can be applied individually according to the pelvic parameters and their geometrical relationship (PI = PT + SS). The effectiveness of preoperative planning with this software in the restoration of balance and view in AS patients has been described.30 The ease of use, the visualization of the osteotomy and the inclusion of the effect of the osteotomy on the correction of both the CBVA and SVA are the main advantages of this computational program. In addition, since the final report is only saved as a local PDF file, and data are not saved in any database, there is no need for additional provisions and requirements related to the processing and saving of personal data of patients according to the General Data Protection Regulation (GDPR). However, one of the major shortcomings of this program is that it did not account for the pelvic parameters. The concept of these basic pelvic parameters and their geometrical relationship were not available at the time of publication of the underlying mathematical principles. However, the basic principle of including the position of the pelvis into account by correcting for the individual’s SEA or SS, is the same (PI = PT + SS).
Surgimap
Surgimap Spine software (www.surgimap.com) is a free available planning software and has been introduced in 2013.31 Surgimap includes the pelvic parameters, in addition to other parameters of sagittal balance, to determine the location and the size of osteotomy. Currently, Surgimap is the most common used computer planning program for both research and clinical practice, and offers regular free updates. This program offers many utilities for different measurements and surgical planning, and can also be used for surgical planning in patients with a fixed sagittal TLKD due to AS by using the specialized sagittal alignment tool.32,33 The practical use and validation has been published recently.31 Following uploading a lateral full-spine radiograph, three planning steps are to be performed.
Measure: On the first “Measure” page, the radiographic image has to be calibrated so the lengths of measurements can be calculated.
Sagittal alignment wizard: Within the ‘measuring tools’ page, the sagittal alignment wizard (“SA spine”) is used to achieve a full evaluation of the sagittal plane including the pelvic parameters by identification of the femoral heads with two adjustable circles and four vertebral end plates (superior S1, superior L1, superior T1, and inferior C2).
Wedge osteotomy wizard: Finally, within the ‘surgical tools’ page the wedge osteotomy wizard “wedge” can be used to create a wedge-shaped resection of a vertebral body. The application of a simulation will remove a portion of the image in a wedge shape and visualize the surgical correction of the radiograph and reports the virtual pelvic parameters and SVA. The results can be saved in the database of the program (Figure 4). The effect of both the level of osteotomy and the effect of the ratio of closure (RoC) on the spinal balance (SVA and PT) by using the “vector” inside the angle of resection can be visualized.20 By adjusting the level of osteotomy and/or the vector, variable correction of the SVA and PT can be tested until desired parameters are obtained. The results can then be saved in the database of the program (Figure 4).
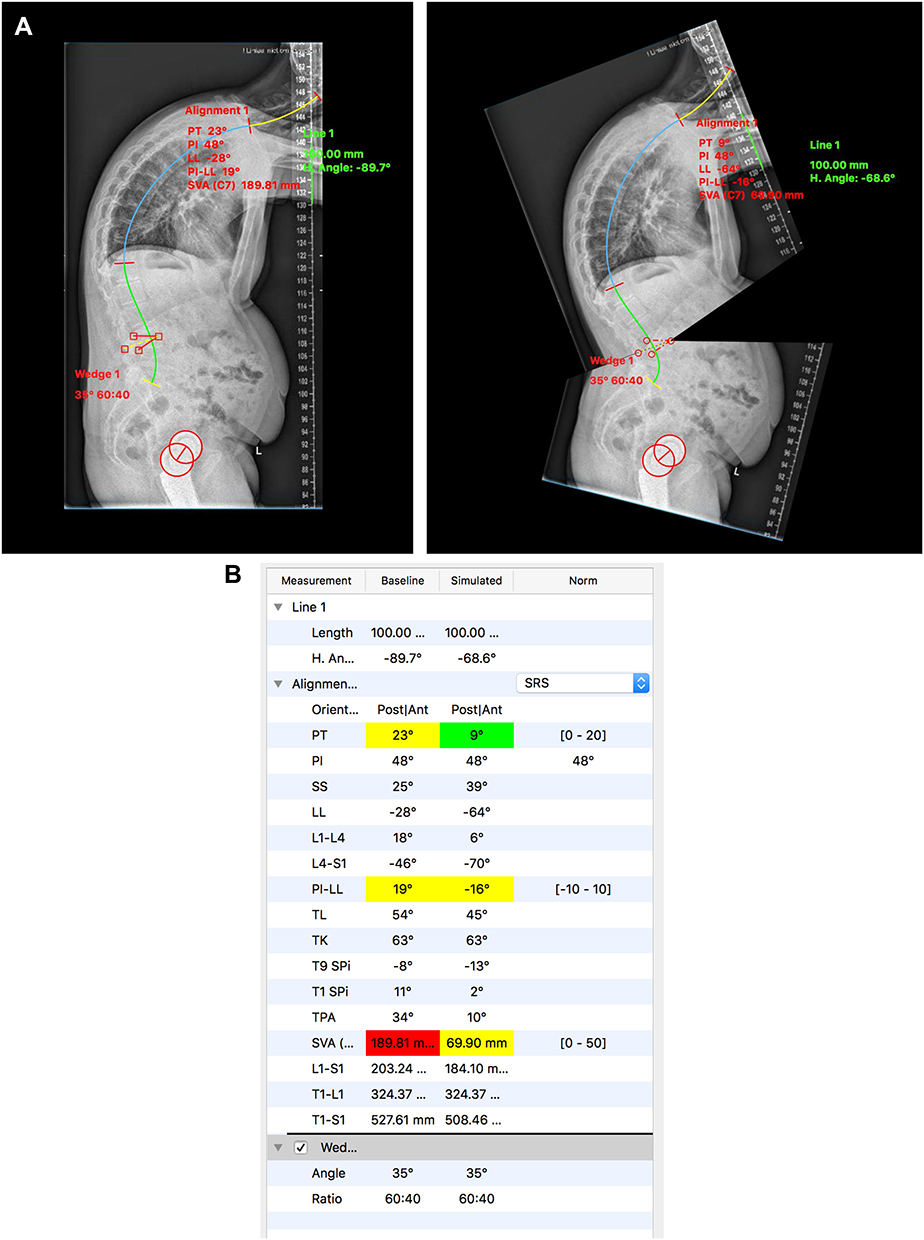 |
Figure 4 (A) Pre-operative and post-planning images of the Surgimap software. (B) Surgimap report showing pelvic parameters: PI = 48°, PT = 23°, SS = 25°, and SVA = 190 mm. A 35° osteotomy (with RoC 60/40) at L4 predicts the postoperative SVA of 70 mm, SS = 39°, and PT = 8°. |
Surgimap also allows for rotation of the image as with ASKyphoplan until desired postoperative PT is reached. The steps are then similar, and the only difference is that the ratio line, or vector, within the “wedge” tool should be aligned with the lower resection line of the osteotomy (ratio set to 100%). Surgimap is a user-friendly sagittal alignment planning software; however, the underlying biomechanical and mathematical principles are not presented. In addition, the simultaneous effect of the osteotomy on the correction of the CBVA is not generated. Since data are saved in the Surgimap database, provisions and requirements related to the processing and saving of patient’s data according to the GDPR should be taken into account.
Case Example
A 43-year-old man with bilateral THR and a 20-year history of AS complicated by a progressive TLKD with a clinical CBVA of 50 degrees is indicated for lumbar osteotomy. Pre-operative planning is performed by using both the ASKyphoplan software (Figure 3) and the Surgimap software (Figure 4).
By using ASKyphoplan, the standard full-length lateral radiograph of the whole spine showed a pre-operative compensated SVA of 172 mm and a sacral slope (SEA) of 27 degrees. Rotation of the radiograph onto the coordinate system with the SEA at 40 degrees resulted in a pre-operative uncompensated SVA of 261 mm. Aiming for an SVA 50 mm anterior to the posterior superior corner of the sacral endplate, a correction angle of 34 degrees at level L4 was required. In addition, a 34-degree correction at L4 would correct the CBVA by 21 degrees (Figure 3). By using Surgimap, the standard full-length lateral radiograph of the whole spine showed a pre-operative compensated SVA of 190 mm, PI of 48 degrees, SS of 25 degrees and PT of 23 degrees. Simulating a 35-degree correction at L4 with an RoC 60/40, the SS would correct to 39 degree, the PT to 8 degree, and the postoperative SVA to 70 mm (Figure 4).
By using both software programs for this case, similar amount of correction, level of osteotomy and final sagittal balance (SVA) were calculated (Table 1). The ASKyphoplan lacks direct information of the pelvic parameters but also gives information about the view angle (CBVA) correction, and Surgimap gives direct information of the pelvic parameters in the planning software. Interestingly, the Surgimap program showed an automatic SS correction to nearly 40 degrees; however, the underlying mathematical principles were not reported.
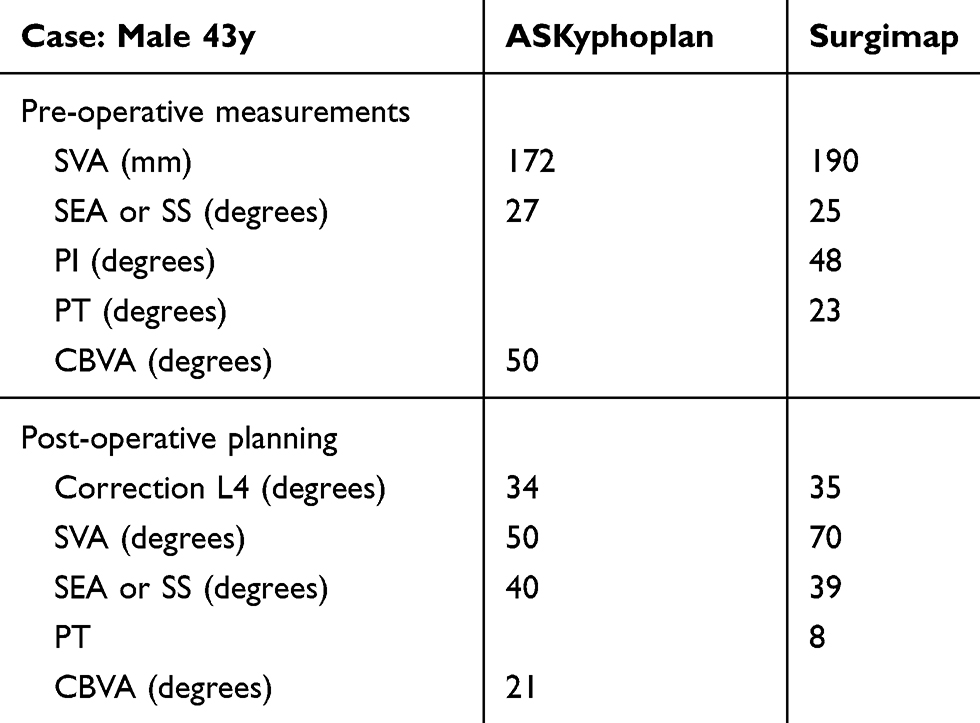 |
Table 1 Parameters of Interest of the as Case Presentation Measured and Planned by the Two Free Available Software Programs ASKyphoplan and Surgimap |
Discussion
Preoperative planning of the lumbar osteotomy in patients with severe TLKD due to AS involves assessment of the combined effect of location of the osteotomy, amount of bone resection, SVA, CBVA, and pelvic parameters. Both software programs, ASKyphoplan and Surgimap, are easy to use in clinical practice to predict postoperative sagittal balance of lumbar osteotomies in these patients. However, the acquired correction during lumbar spine surgery, the effect of secondary hip arthritis on balance control and the sequence of surgical treatment in AS patients with both a severe TLKD that requires spinal osteotomy and secondary hip arthritis that requires a THR should be discussed.
Surgical Correction of the Planned Osteotomy
The surgical procedure of the CWO, including positioning of the patient, anesthesia and surgical technique is described earlier.1,3–5 Intraoperatively, the amount of correction at the desired vertebra is assessed by using the image intensifier. During the closure procedure of the osteotomy, lateral images of the lumbar spine from the image intensifier can be sent to the local picture archiving and communication system (PACS) at regular times. The acquired correction during surgery can be estimated by measuring the Cobb’s angle in degrees between the upper and lower endplate of the vertebra operated on using the “measuring angle” tool displayed on the digital system, until the required correction angle is achieved.29
The Hip-Spine Dilemma and Pre-Operative Planning in Ankylosing Spondylitis
Owing to the ankylosis of the spine, only the mobile joints of the hips, knees, and ankle joints can compensate for the sagittal displacement of the trunk COM in AS. Therefore, range of motion (ROM) at the hip was thought to be important for control of sagittal balance in patients with TLKD due to AS. Studies have shown that the hip joints are less involved in balance control than previous thought, and that they have limited ability to compensate for the anterior shift of the COM.9,34 Posterior rotation of the pelvis may result in a large correction of both the sagittal alignment of the spine and view angle. However, it places the pelvic acetabulum out of the neutral position, and the femoral heads in maximal extension. Thus, further extension of the hip joints is limited in the posterior rotated pelvis. As patients need some spare hip extension for dynamic balance control, they are not able to fully extend the hip joints during standing and walking.
In addition, AS may lead to limitations in range of motion (ROM) of the hip joints due to secondary arthritis.35 Symptomatic unilateral or bilateral hip arthritis and ankyloses have been reported in 30–50% of AS patients.36 Total hip arthroplasty replacement (THR) is very successful in these patients.37,38 However, a relative high rate of complications, such as infection, dislocation, and heterotopic ossification, and early mechanical failure of the implant in the short to midterm have been reported.39,40
The sequence of surgical treatment in AS patients with secondary hip arthritis that requires a THR, and a severe TLKD that requires spinal osteotomy is debated. Traditionally, THR was recommended before the osteotomy of the spine was considered,3,38,39 because it was felt that compensation by a mobile hip may improve the sagittal balance and obviate the need for a spinal osteotomy. Also, a THR was considered a less morbid procedure than a spinal osteotomy. However, Zheng et al recently suggested that a spinal osteotomy should be performed before THR.41 They argued that patients with a severe TLKD have high potential risk for dislocation of the prosthesis, and that pre-operative and post-operative management of THR is safer if a spinal osteotomy had been performed first. Finally, the positioning of the patient during hip surgery, and anatomical placement of the acetabular and femoral component has been shown to be less difficult following spinal osteotomy resulting in a better outcome.40–42
Conclusion
Deformity correction in patients with a severe TLKD due to AS by a lumbar osteotomy is very successful in improving sagittal balance and view angle. Preoperative assessment of the TLKD in AS involves measurement of the pelvic parameters, the SVA, the CBVA, and an understanding of the effect of the lower limbs on maintaining sagittal balance. Planning the lumbar osteotomy involves assessment of the effect of the location of the osteotomy and the amount of bone resection in a CWO on correction of these parameters. Both software programs, ASKyphoplan and Surgimap, are free available, user-friendly, and can be used for planning sagittal plane corrective osteotomies of the spine in clinical practice. These software programs help visualize the effect of the location of the osteotomy and the amount of wedge resection on the sagittal balance and view angle of the individual patient with a severe TLKD due to AS. However, the use of these clinical and biomechanical parameters of interest in the current free available software programs for sagittal plane corrective osteotomies of the lumbar spine in AS, has been presented here for a single case. There is a need for prospective studies to evaluate and compare the effectiveness of preoperative planning with the use of computer software programs in the restoration of balance and view angle in patients treated with lumbar osteotomy in AS.
Abbreviations
AS, ankylosing spondylitis; axSpA, axial spondyloarthritis; CBVA, chin-brow-to-vertical angle; COM, center of mass; CWO, closing wedge osteotomy; FBI, full balance integrated; GDPR, General Data Protection Regulation; LL, lumbar lordosis; PACS, picture archiving and communication system; PI, pelvic incidence; PSCS, posterior superior corner of the sacrum; PSO, pedicle subtraction osteotomy; PT, pelvic tilt; RoC, ratio of closure; ROM, range of motion; SEA, sacral endplate angle (=SS); SS, sacral slope (=SEA); SVA, sagittal vertical axis; THR, total hip replacement; TK, thoracic kyphosis; TLKD, thoracolumbar kyphotic deformity; WBKA, whole body kyphosis angle.
Data Sharing Statement
Not applicable.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Consent for publication is obtained from patients in Figure 1 and Figure 2.
Funding
There is no funding to report.
Disclosure
The author is among the developers and owners of ASKyphoplan software, with no financial benefit and reports no other potential conflicts of interest for this work.
References
1. Van Royen BJ, De Gast A. Lumbar osteotomy for correction of thoracolumbar kyphotic deformity in ankylosing spondylitis. A structured review of three methods of treatment. Ann Rheum Dis. 1999;58(7):399–406. doi:10.1136/ard.58.7.399
2. Koller H, Koller J, Mayer M, Hempfing A, Hitzl W. Osteotomies in ankylosing spondylitis: where, how many, and how much? Eur Spine J. 2018;27(Suppl S1):70–100. doi:10.1007/s00586-017-5421-z
3. van Royen BJ, Slot GH. Closing-wedge posterior osteotomy for ankylosing spondylitis. Partial corporectomy and transpedicular fixation in 22 cases. J Bone Joint Surg Br. 1995;77-B(1):117–121. doi:10.1302/0301-620X.77B1.7822367
4. Kim KT, Suk KS, Cho YJ, Hong GP, Park BJ. Clinical outcome results of pedicle subtraction osteotomy in ankylosing spondylitis with kyphotic deformity. Spine. 2002;27(6):612–618. doi:10.1097/00007632-200203150-00010
5. Bridwell KH, Lewis SJ, Rinella A, Lenke LG, Baldus C, Blanke K. Pedicle subtraction osteotomy for the treatment of fixed sagittal imbalance. Surgical technique. J Bone Joint Surg Am. 2004;86(Suppl 1):44–50. doi:10.2106/00004623-200403001-00007
6. La Barbera L, Brayda-Bruno M, Liebsch C, et al. Biomechanical advantages of supplemental accessory and satellite rods with and without interbody cages implantation for the stabilization of pedicle subtraction osteotomy. Eur Spine J. 2018;27(9):2357–2366. doi:10.1007/s00586-018-5623-z
7. La Barbera L, Wilke HJ, Liebsch C, et al. Biomechanical in vitro comparison between anterior column realignment and pedicle subtraction osteotomy for severe sagittal imbalance correction. Eur Spine J. 2020;29(1):36–44. doi:10.1007/s00586-019-06087-x
8. Luca A, Ottardi C, Sasso M, et al. Instrumentation failure following pedicle subtraction osteotomy: the role of rod material, diameter, and multi-rod constructs. Eur Spine J. 2017;26(3):764–770. doi:10.1007/s00586-016-4859-8
9. Bot SD, Caspers M, Van Royen BJ, Toussaint HM, Kingma I. Biomechanical analysis of posture in patients with spinal kyphosis due to ankylosing spondylitis: a pilot study. Rheumatology (Oxford, England). 1999;38(5):441–443. doi:10.1093/rheumatology/38.5.441
10. Schwab F, Lafage V, Patel A, Farcy JP. Sagittal plane considerations and the pelvis in the adult patient. Spine. 2009;34(17):1828–1833. doi:10.1097/BRS.0b013e3181a13c08
11. Legaye J, Duval-Beaupere G, Hecquet J, Marty C. Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J. 1998;7(2):99–103. doi:10.1007/s005860050038
12. Song K, Su X, Zhang Y, et al. Optimal chin-brow vertical angle for sagittal visual fields in ankylosing spondylitis kyphosis. Eur Spine J. 2016;25(8):2596–2604. doi:10.1007/s00586-016-4588-z
13. Suk KS, Kim KT, Lee SH, Kim JM. Significance of chin-brow vertical angle in correction of kyphotic deformity of ankylosing spondylitis patients. Spine. 2003;28(17):2001–2005.
14. Van Royen BJ, De Gast A, Smit TH. Deformity planning for sagittal plane corrective osteotomies of the spine in ankylosing spondylitis. Eur Spine J. 2000;9(6):492–498. doi:10.1007/s005860000183
15. Ames CP, Smith JS, Scheer JK, et al. Impact of spinopelvic alignment on decision making in deformity surgery in adults: a review. J Neurosurg Spine. 2012;16(6):547–564. doi:10.3171/2012.2.SPINE11320
16. Gelb DE, Lenke LG, Bridwell KH, Blanke K, McEnery KW. An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine. 1995;20(12):1351–1358. doi:10.1097/00007632-199520120-00005
17. Min K, Hahn F, Leonardi M. Lumbar spinal osteotomy for kyphosis in ankylosing spondylitis: the significance of the whole body kyphosis angle. J Spinal Disord Tech. 2007;20(2):149–153. doi:10.1097/01.bsd.0000211252.67576.d9
18. Halm H, Metz-Stavenhagen P, Zielke K. Results of surgical correction of kyphotic deformities of the spine in ankylosing spondylitis on the basis of the modified arthritis impact measurement scales. Spine. 1995;20(14):1612–1619.
19. Roussouly P, Nnadi C. Sagittal plane deformity: an overview of interpretation and management. Eur Spine J. 2010;19(11):1824–1836. doi:10.1007/s00586-010-1476-9
20. Diebo BG, Lafage R, Ames CP, et al. Ratio of lumbar 3-column osteotomy closure: patient-specific deformity characteristics and level of resection impact correction of truncal versus pelvic compensation. Eur Spine J. 2016;25(8):2480–2487. doi:10.1007/s00586-016-4533-1
21. Sengupta DK, Khazim R, Grevitt MP, Webb JK. Flexion osteotomy of the cervical spine: a new technique for correction of iatrogenic extension deformity in ankylosing spondylitis. Spine. 2001;26(9):1068–1072. doi:10.1097/00007632-200105010-00016
22. Ondra SL, Marzouk S, Koski T, Silva F, Salehi S. Mathematical calculation of pedicle subtraction osteotomy size to allow precision correction of fixed sagittal deformity. Spine. 2006;31(25):E973–979. doi:10.1097/01.brs.0000247950.02886.e5
23. Kim YJ, Bridwell KH, Lenke LG, Rhim S, Cheh G. An analysis of sagittal spinal alignment following long adult lumbar instrumentation and fusion to L5 or S1: can we predict ideal lumbar lordosis? Spine. 2006;31(20):2343–2352. doi:10.1097/01.brs.0000238970.67552.f5
24. Rose PS, Bridwell KH, Lenke LG, et al. Role of pelvic incidence, thoracic kyphosis, and patient factors on sagittal plane correction following pedicle subtraction osteotomy. Spine. 2009;34(8):785–791. doi:10.1097/BRS.0b013e31819d0c86
25. Schwab F, Patel A, Ungar B, Farcy JP, Lafage V. Adult spinal deformity-postoperative standing imbalance: how much can you tolerate? An overview of key parameters in assessing alignment and planning corrective surgery. Spine. 2010;35(25):2224–2231. doi:10.1097/BRS.0b013e3181ee6bd4
26. Le Huec JC, Leijssen P, Duarte M, Aunoble S. Thoracolumbar imbalance analysis for osteotomy planification using a new method: FBI technique. Eur Spine J. 2011;20(Suppl S5):669–680. doi:10.1007/s00586-011-1935-y
27. Lafage V, Schwab F, Vira S, Patel A, Ungar B, Farcy JP. Spino-pelvic parameters after surgery can be predicted: a preliminary formula and validation of standing alignment. Spine. 2011;36(13):1037–1045. doi:10.1097/BRS.0b013e3181eb9469
28. Song K, Zheng G, Zhang Y, Zhang X, Mao K, Wang Y. A new method for calculating the exact angle required for spinal osteotomy. Spine. 2013;38(10):E616–620. doi:10.1097/BRS.0b013e31828b3299
29. van Royen BJ, Scheerder FJ, Jansen E, Smit TH. ASKyphoplan: a program for deformity planning in ankylosing spondylitis. Eur Spine J. 2007;16(9):1445–1449. doi:10.1007/s00586-007-0371-5
30. Pigge RR, Scheerder FJ, Smit TH, Mullender MG, van Royen BJ. Effectiveness of preoperative planning in the restoration of balance and view in ankylosing spondylitis. Neurosurg Focus. 2008;24(1):E7. doi:10.3171/FOC/2008/24/1/E7
31. Lafage R, Ferrero E, Henry JK, et al. Validation of a new computer-assisted tool to measure spino-pelvic parameters. Spine J. 2015;15(12):2493–2502. doi:10.1016/j.spinee.2015.08.067
32. Hu W, Yu J, Liu H, et al. Osteotomy in ankylosing spondylitis, a prospective case series with minimum 2 year follow-up. PLoS One. 2016;11(12):e0167792. doi:10.1371/journal.pone.0167792
33. Park YS, Kim HS, Baek SW, Oh JH. Preoperative computer-based simulations for the correction of kyphotic deformities in ankylosing spondylitis patients. Spine J. 2014;14(10):2420–2424. doi:10.1016/j.spinee.2014.02.022
34. Del Din S, Carraro E, Sawacha Z, et al. Impaired gait in ankylosing spondylitis. Med Biol Eng Comput. 2011;49(7):801–809. doi:10.1007/s11517-010-0731-x
35. Braun J, van den Berg R, Baraliakos X, et al. 2010 update of the ASAS/EULAR recommendations for the management of ankylosing spondylitis. Ann Rheum Dis. 2011;70(6):896–904. doi:10.1136/ard.2011.151027
36. Sochart DH, Porter ML. Long-term results of total hip replacement in young patients who had ankylosing spondylitis. Eighteen to thirty-year results with survivorship analysis. J Bone Joint Surg Am. 1997;79(8):1181–1189. doi:10.2106/00004623-199708000-00010
37. Joshi AB, Markovic L, Hardinge K, Murphy JC. Total hip arthroplasty in ankylosing spondylitis: an analysis of 181 hips. J Arthroplasty. 2002;17(4):427–433. doi:10.1054/arth.2002.32170
38. Bhan S, Eachempati KK, Malhotra R. Primary cementless total hip arthroplasty for bony ankylosis in patients with ankylosing spondylitis. J Arthroplasty. 2008;23(6):859–866. doi:10.1016/j.arth.2007.07.014
39. Tang WM, Chiu KY. Primary total hip arthroplasty in patients with ankylosing spondylitis. J Arthroplasty. 2000;15(1):52–58. doi:10.1016/S0883-5403(00)91155-0
40. Blizzard DJ, Penrose CT, Sheets CZ, Seyler TM, Bolognesi MP, Brown CR. Ankylosing spondylitis increases perioperative and postoperative complications after total hip arthroplasty. J Arthroplasty. 2017;32(8):2474–2479. doi:10.1016/j.arth.2017.03.041
41. Zheng GQ, Zhang YG, Chen JY, Wang Y. Decision making regarding spinal osteotomy and total hip replacement for ankylosing spondylitis: experience with 28 patients. Bone Joint J. 2014;96-b(3):360–365.
42. Hu J, Qian B-P, Qiu Y, et al. Can acetabular orientation be restored by lumbar pedicle subtraction osteotomy in ankylosing spondylitis patients with thoracolumbar kyphosis? Eur Spine J. 2017;26(7):1826–1832. doi:10.1007/s00586-016-4709-8
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.