Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Preoperative Anemia and Iron Deficiency Screening, Evaluation and Management: Barrier Identification and Implementation Strategy Mapping
Authors Delaforce A ![]() , Duff J
, Duff J ![]() , Munday J
, Munday J ![]() , Hardy J
, Hardy J ![]()
Received 2 October 2020
Accepted for publication 4 November 2020
Published 1 December 2020 Volume 2020:13 Pages 1759—1770
DOI https://doi.org/10.2147/JMDH.S282308
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Alana Delaforce,1,2 Jed Duff,1,3 Judy Munday,3,4 Janet Hardy2
1School of Nursing and Midwifery, The University of Newcastle, Callaghan, NSW, Australia; 2Mater Health Services, South Brisbane, QLD 4101, Australia; 3School of Nursing/Centre for Healthcare Transformation, Queensland University of Technology, Kelvin Grove, QLD, Australia; 4School of Nursing, The University of Agder, Kristiansand, Norway
Correspondence: Alana Delaforce Email [email protected]
Introduction and aims: Patients undergoing major surgery risk significant blood loss and transfusion, which increases substantially if they have pre-existing anemia. Preoperative Anemia and Iron Deficiency Screening, Evaluation and Management Pathways (PAIDSEM-P) outline recommended blood tests and treatment to optimize patients before surgery. Documented success using PAIDSEM-P to reduce transfusions and improve patient outcomes exists, but the reporting quality of such studies is suboptimal. It remains unclear what implementation strategies best support the implementation of PAIDSEM-P.
Method: Maximum variation, purposive sampling was used to recruit a total of 15 participants, including a range of health professionals and patients for semi-structured interviews. Data analysis utilized a deductive approach informed by the Consolidated Framework for Implementation Research (CFIR) for barrier identification and the Expert Recommendations for Implementing Change (ERIC) for reporting recommended implementation strategies. A modified version of the Action, Actor, Context, Target and Time (AACTT) framework assisted with conceptualisation and targeted strategy selection.
Results: The analysis revealed five barriers: access to knowledge and information, patient needs and resources, knowledge and beliefs about the intervention, available resources, and networks and communications, which had strong ERIC recommendations, including conduct educational meetings, develop educational materials, distribute educational materials, obtain and use patients/consumers family feedback, involve patients/consumers/family members, conduct a local needs assessment, access new funding, promote network weaving, and organize clinician implementation team meetings.
Conclusions: Mapping the barriers and strategies using the ERIC framework on the basis of individual actor categories proved to be useful in identifying a pragmatic number of implementation strategies that may help in supporting the utilisation of the PAIDSEM-P and other evidence-based healthcare implementation problems more broadly.
Keywords: patient blood management, preoperative anemia screening, Consolidated Framework for Implementing Research, Expert Recommendations for Implementing Change, qualitative
Plain Language Summary
Patients having major surgery can lose a significant amount of blood and require a transfusion. However, transfusions carry risks including increased rate of infection, length of stay in hospital and sustaining a venous thromboembolism. Transfusions can sometimes be avoided by preparing patients for surgery. Presurgical screening that checks hemoglobin levels and iron stores helps to identify patients who will benefit from treatment or management to ensure they are optimized before their procedure. A previous systematic review undertaken by the authors revealed that implementation of these checks is highly variable, and it is difficult to work out why some facilities do not succeed, as the barriers to embedding this into practice are explained using different terminology or not at all in the current evidence base. This paper builds on that review and aims to demonstrate the benefit of using a common language to communicate barriers and identify strategies suggested in the literature to be effective. It provides a blueprint for implementation in one facility, that may be generalizable to others who wish to use the same methodological approach as the one deployed in this study.
Introduction
Patients undergoing major surgery, and who lose more than 500mls of blood, are at risk of becoming anemic postoperatively and requiring a blood transfusion.1 Blood transfusions are not without risk and can increase the chance of infection, venous thromboembolism and increased length of stay (in a surgical setting).2–4 Due to these risks, mitigation strategies are necessary to ensure patients are optimized before surgery and to help avoid blood transfusions.1 Patient Blood Management (PBM) guidelines outline recommended preoperative screening tests and treatment pathways for optimization.5–8 The tests ascertain if the patient has anemia (iron or non-iron related) and if present, recommends treatment including iron supplementation or further investigation to determine the underlying cause of anemia.1
To date, many facilities have experienced varying success in implementing Preoperative Anemia and Iron Deficiency Screening, Evaluation and Management Pathways (PAIDSEM-P), and there is no conclusive, context-specific, evidence to suggest the most effective way to mitigate reported barriers.9 Implementation frameworks and tools exist that can help identify barriers, conceptualize the actions needed from key stakeholders, and suggest implementation strategies.10 This paper uses the Consolidated Framework for Implementation Research (CFIR) for barrier identification, the Actor, Action, Context, Target and Time (AACTT) framework for conceptualizing actors and actions, and the Expert Recommendations for Implementing Change (ERIC) framework for implementation strategy selection.11
The CFIR consists of five domains (intervention characteristics, inner setting, outer setting, individual characteristics and process) and 39 constructs that were devised over multiple Delphi rounds by implementation experts to develop a taxonomy for common implementation barriers.11 It can be used at multiple phases of implementation and facilitates multi-level analysis (including individual, organizational, environment and process).11 The AACTT is designed to assist with mapping each person involved in the delivery of an intervention, specifying the action they are required to perform, the context in which it needs to be undertaken, to whom the action is targeted at, and the time frame required to carry it out.12 The modified AACTT framework is used in this study to conceptualize actor categories and defined actions they need to perform when using the PAIDSEM-P.12
Identified CFIR barriers can then be linked to mitigation strategies using the ERIC framework.13 The recommended strategies are categorized by strength, depending on the level of consensus provided by implementation experts as to the effectiveness of strategies in barrier mitigation.13 Strength is divided into three categories: weak (less than 20% consensus), moderate (20–49% consensus) and strong (50% or greater consensus).13 In a previous review, we ascertained CFIR coded barriers related to PBM implementation as reported in the broader context and compared strategies used by health facilities with those suggested in the ERIC framework.9 The review confirmed the common utilization of the implementation strategies, but there was no relationship noted between barriers identified, strategies and improvement outcomes.9
This paper used qualitative methods to identify the most common barriers to implementing PAIDSEM-P locally, conceptualized on an individual “actor” basis, and the most strongly recommended strategies to address the barriers comparedagainst existing evidence.
Materials and Methods
Aim
This study aimed to identify the barriers to implementing PAIDSEM-P, conceptualize the actions required of individuals, select suitable strategies to assist with implementation and compare them with existing evidence.
Design
Using a qualitative approach, we sought the perspectives of both health professionals who may influence the introduction, and operationalization of the PAIDSEM-P, and patients who had undergone surgery, to help identify barriers to the uptake of recommended screening and treatment.
Setting
The setting of this study is a large, metropolitan, tertiary referral hospital that provides services for both public and privately insured patients over a wide range of specialties. Approximately 1400 major surgeries (eligible for the PAIDSEM-P) are undertaken in the public service, and 1900 in the private service annually. Preoperative screening processes, in general, are not standardized, and the adoption of the PAIDSEM-P for both public and private patients has yet to be commenced.14
Participants and Recruitment
We used purposive, maximum variation sampling to gain perspectives across a breadth of healthcare professionals and patients.15 This sampling method was chosen as it was not the intention of the study to seek data saturation, but to conduct interviews until a clear understanding of barriers were gathered.16 Health professional recruitment occurred by direct, personal email invitation, and postoperative patients were directly recruited by the first author (AD) on the surgical ward. AD liaised with nursing staff to determine potential patients for participation who met the criteria of having undergone major surgery, were 18 years of age and over, and were able to provide informed consent. We sought health professionals with experience in prescribing, administering, supplying or governing the provision of blood and blood products. Before each interview, participants provided informed, written consent. Full ethical approval from the hospital Human Research Ethics Committee (HREC), and administrative approval from the university HREC (reference: AM/MML/47826) was obtained.
Data Collection
Semi-structured interviews were informed by the CFIR framework. Interview questions were iteratively adapted based on emerging, preliminary findings. After each interview, AD completed a diary reflecting on interview responses, and discussed results with JD and JM to ensure reflexivity, transparency and agreement with the direction of future interviews. All interviews were conducted in a private and quiet area in the hospital, at the participants’ convenience, by one member of the research team (AD), who had pre-existing professional relationships with all health care professional participants. The interviews were recorded, transcribed and de-identified. Basic demographic data collected at the time of the interview included role and years of experience.
Data Analysis
The CFIR was used to code interview responses to enable barrier identification.11 During coding, a pilot sampling approach was used: 20% of the transcripts were coded by multiple authors (AD, JD & JM).17 After evidence of good agreement with coded data (over 80%), one author (AD) coded the remaining interviews. Following coding, data were provided to the two other authors for perusal before analysis to ensure credibility. Consensus discussions resolved any coding disagreements. After finalization of coding, one author (AD) organized the data by the “actor” category as suggested by the AACTT framework and then identified the most common barriers mentioned by participants in each category.12 After allocating participants to actor categories, we devised the action they contributed to the PAIDSEM-P. The data were then forwarded to participants to provide an opportunity for them to review their answers, confirm that identified barriers were reflective of their concerns and that actions allocated to their actor category were correct, to ensure trustworthiness (Figure 1). Following this, mapping to determine appropriate ERIC strategies occurred.13 During the barrier and strategy mapping, only the strongest suggested ERIC strategies (over 50% expert agreement for effectiveness) for each actor barrier were included in our recommendations to avoid losing context.13
 |
Figure 1 Data analysis process overview. |
Results
Demographics of Included Participants
A total of 15 people participated in the interviews, including 13 multidisciplinary health professionals and two patients (one receiving care in the private hospital and one in the public hospital). One person in each of the following categories was interviewed: anesthetist, surgeon/surgical residents/preadmissions medical team, ward physicians/clinical hematologists, pathology/blood bank, laboratory hematologist, pre-admission/private practice nurses, clinical governance/quality staff. We recruited two of each of the following categories: ward nurses, executive directors and patients. There were five males and seven females across the multidisciplinary group, and the years of experience in professional role ranged from 2 to 39 years. Both patients were female.
CFIR Domains and Barrier Constructs (Directed Content Analysis)
Four of five CFIR domains had commonly mentioned barriers, namely the outer setting, inner setting, characteristics of individuals and process. Ten CFIR barrier constructs represented those most frequently mentioned across the interviews (Table 1). A more detailed content analysis is available in Supplementary text S1.
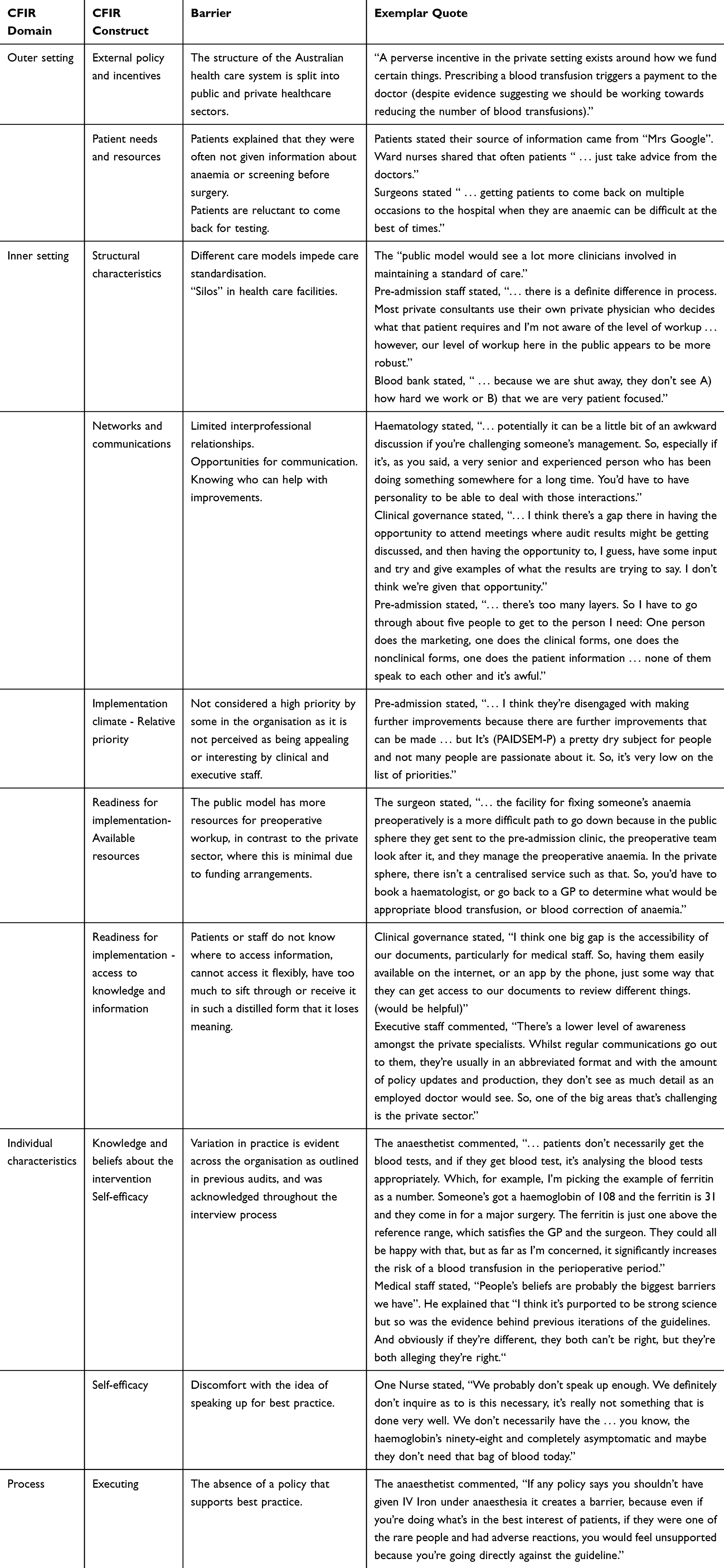 |
Table 1 Summarised Results of Identified Barrier by CFIR Domain and Construct |
ERIC Barrier and Strategy Mapping Analysis
Only 5 of the 10 identified barriers had strongly recommended implementation strategies (with ≥50% expert endorsement for the strategy) including access to knowledge and information, available resources, knowledge and beliefs about the intervention, networks and communications, patient needs and resources. For these five barriers, nine implementation strategies are strongly recommended according to the ERIC tool including; conduct educational meetings, develop educational materials, distribute educational materials, access new funding, promote network weaving, organize clinician implementation team meetings, obtain and use patients/consumers/family feedback, involve patients/consumers/family members and conduct a local needs assessment (Table 2).
 |
Table 2 Actor, Action, Barriers and Recommended Strategies |
Discussion
To the authors’ knowledge, this study is the first to identify barriers to the implementation of PAIDSEM-P using rigorous implementation methodology. The analysis revealed ten common barriers, five of which had nine strongly recommended implementation strategies. The utilization of these strategies should lead to an effective change in practice. Inclusion of the modified AACTT framework facilitated pragmatic and context-specific conceptualization and data analysis.
The study revealed that external policy and incentives have a significant impact on the ability of health care facilities to deliver standardized care. Currently, external government and private health funding policy do not support the judicious use of blood products or encourage optimization to avoid usage, which is the intent of the PAIDSEM-P. This sentiment has been shared in a quasi-experimental before and after the study by Morgan and colleagues who acknowledge that private prescribers, in particular, have far greater autonomy than those in the public sector.18 In the context of patient blood management, it may be implied that private prescribers can use as much blood as they like (and are reimbursed for it), but the appropriateness of that utilization is reflected on the organization. The latter has little power to influence the individual practitioner.19
Despite the absence of a strongly recommended implementation strategy to mitigate external policy and incentives, one step towards addressing this issue would be to remove reimbursement for prescribers (alter incentive and allowance structures) attached to provision of blood, which may influence the uptake of optimization to prevent transfusions. One strategy with weak expert endorsement, but which the literature suggests is effective, is to involve executive boards and alter incentive allowance structures.20 This strategy has been helpful, as demonstrated by previous studies, to champion support for blood management programs more broadly.20,21 Abbett et al implemented a financial incentive attached to the reduction in utilization of blood products overall and found a reduction of 14.3% in transfusions considered to be given outside of guidelines.20 Others have also demonstrated, through a quasi-experimental before and after study, a reduction of 43% in units of blood per patient discharged using a PBM program that was supported and championed by the hospital executive.21
It was identified that patient needs related to blood management are currently unmet in the local setting, as no specific information regarding preoperative anemia is provided for patients. It was found that neither prescribers nor patients currently receive structured education. Obtaining patient feedback and involving them is a strongly recommended implementation strategy to address this barrier. A multidimensional framework by Carman et al outlines different levels of patient inclusion and considers that it can range from consultation, involvement or partnership and shared leadership.22 In the context of PBM literature, the inclusion of patients in intervention development has tended to be tokenistic, with consumer consultation and feedback usually only sought after the development of an intervention (for example, patient information or policy).23,24 Liao et al shared this sentiment and undertook a qualitative study of health professionals and patients perceptions of informed consent,24 seeking to understand how patients perceive current resources available to them that provide information on risks, and how they would prefer to receive that information.24 Interestingly, they found a similar trend to our study where patients tended to rely upon, and trust, doctors recommendations, as they feel too overwhelmed to make informed decisions.24 The study also found that patients felt a verbal and individualized conversation between the prescribing clinician and the patient is more valuable than written materials, which they would prefer to have as a source of reference, to read in their own time.24
Structural characteristics provide a significant barrier due to the different care models and organizational structures. Staff admitted preoperative workup appears to be more robust in the public model (although this does not yet include routine preoperative anemia and iron deficiency screening), and that standardization of care into the private that mirrors this approach might help optimize preoperative care and reduce variation. Consideration is required to ensure that the intervention is tailored to the specific model of care. The ERIC recommends assessing the readiness for change by identifying barriers and facilitators.13 One study in the context of PBM implementation utilized the strategy of developing a formal blueprint resulting in a 25% reduction in transfusions.25 An additional study that has demonstrated the positive impact of using a formalized implementation planning process pioneered the first system-wide PBM project in Western Australia.26 Their group showed a 10% decrease in the use of blood products, despite an increase in hospital activity between 2008 and 2012.26 While they were not specific in their pre-implementation assessment, this points positively towards the impact that this strategy can have on increasing the chance of intervention uptake.25
Relative priority was mentioned as an issue because some participants stated that clinicians and executives found the subject of PAIDSEM-P not to be a priority. The ERIC recommends the conduct of local consensus discussions, including the formation of working parties. Albinarrate et al established a multidisciplinary team to determine consensus on best practice before rolling out their PBM program, which included preoperative anemia screening and treatment and demonstrated a positive effect.27 They achieved a decrease of 21.6% in transfusion reduction within the orthopedic service, although compliance with preoperative anemia pathways influence on change, specifically, was not reported.27
Networks and communications were described as a barrier by patients and health professionals. Patients mentioned the difficulty they would sometimes have in getting through to speak to their treating physician, and health professionals were unsure of whom to contact to initiate change. The ERIC suggests the promotion of network weaving and organization of clinician implementation team meetings. One study that relied heavily on clinician meetings, including an off-site summit, managed to reduce transfusion per patient discharged by 43% in their before and after, quasi-experimental research.21
Available resources were evident as an issue due to the difference in funding models, including time and resources given to health professionals to thoroughly assess patients preoperatively. The ERIC strongly suggests that accessing new funding can mitigate this issue. In this setting, an increase in available resources is required to enhance the availability of staff to review tests and increased work up in the private sector. Provision of these resources will be necessary to facilitate optimal screening and treatment. One of the first major PBM programs, globally, originated in Western Australia and had substantial support from public sector government funding.28 They obtained funding to cover dedicated preoperative PBM assessment nurses who ensured all patients received the necessary workup.28 While this study did not report specific compliance with preoperative anemia screening, it formed part of their program, and they achieved a reduction in transfused elective patients from 22.5% to just over 2% across 8 years.28
Access to knowledge and information is currently an issue because there is no standardized pathway, and any resources available that are hospital-specific and might help support good clinical decision-making are only available on the hospital intranet. It was suggested during interviews that making information and support tools available remotely to health professionals and patients would help improve access and awareness of the benefits of PAIDSEM-P. The strongly recommended strategy is the conduct of educational meetings, in addition to the development and distribution of educational materials to address this barrier. An education package, alongside audit, has been demonstrated to increase the rate of pre-transfusion testing from 87% to 93%.29 Again, there was no direct reporting of compliance to preoperative screening, but the broad impact of this intervention on blood utilization was positive.
Knowledge and beliefs about the intervention were evident as a barrier where staff could not correctly define PBM guidelines or provide correct parameters for hemoglobin ranges. They stated that there is a high variation in the knowledge levels amongst health professionals concerning PAIDSEM-P and PBM. Nursing staff noted a lack of coverage within their university curricula and relied on knowledge gained through their graduate nurse program from allocated mentors. Nursing staff are expected to complete mandatory online education on PBM, which includes exploration of the importance of investigating anemia correctly before deciding on treatment. However, it is only context-specific, and a ward nurse, who is still potentially responsible for the preoperative care of a patient, may not see the patient blood management module as relevant to them. The ERIC recommends the conduct of educational meetings to address this barrier. A 43% reduction in perioperative transfusions has been demonstrated following the implementation of a PAIDSEM-P, and one aspect of achieving this reduction included ensuring continual staff education on the importance of adherence to the hospital guideline.30
Self-efficacy is a barrier as some health professionals felt they were capable of providing best-practice care but did not feel supported by policy and procedure. This is recognized as a pervasive issue, particularly concerning guideline dissemination and prevention of autonomy through organizational barriers has been found to impact the uptake of PBM.31 A before and after survey study that measured the beliefs of physicians before and after the implementation of a locally developed PBM programme made allowances for individualized clinical decision-making and found that there was an increase in the belief that preoperative anemia adversely affected patient morbidity and mortality from 25% to 37%.31 While there are currently no strong ERIC recommendations for this barrier, perhaps ensuring that policy and procedure are written with allowances for clinicians to make truly evidence-based decisions based on their experience, patient preference and guidelines would help in addressing it.13,32
Recommendations for Future Practice
This paper demonstrates an approach that can be used to identify a pragmatic number of barriers on the basis of the actor category and strategies that may be overcome to address them. This method should be applicable more broadly to other evidence-based health implementation problems and requires testing to evaluate the effectiveness of the approach.
Strengths and Limitations
Using the CFIR framework to identify barriers was most helpful in this study, particularly since the modified AACTT framework was used to conceptualize what actions were required at the individual stakeholder level. Further research that identifies which strategies are most effective at mitigating barriers will help strengthen guidance provided by these tools.
Further, the focus of this study was on prioritizing common barriers, to maximize the chance of initial implementation attempts. Less common barriers may need exploring if the results of this study are not effective in achieving an improvement in the implementation of PADISEM-P.
Any potential limitation due to the pilot coding process adapted was offset by utilizing a rigorous checking process with all participants to ensure that the strongest barriers were summarized from their responses. In addition, employing consensus during a pilot coding phase involving three investigators, before coding of all interviews.
Conclusion
This study has revealed ten barriers, including five with strong recommendations. These five barriers (access to knowledge and information, available resources, knowledge and beliefs about the intervention, networks and communications, patient needs and resources) should be addressed using nine implementation strategies: conduct educational meetings, develop educational materials, distribute educational materials, access new funding, promote network weaving, organize clinician implementation team meetings, obtain and use patients/consumers/family feedback, involve patients/consumers/family members and conduct a local needs assessment. Mapping the barriers and strategies using the ERIC framework on the basis of individual actor categories proved to be useful in identifying a pragmatic number of implementation strategies that may help in supporting the utilization of the PAIDSEM-P. The approach used in this study provides a pragmatic method for approaching other evidence-based healthcare implementation problems and requires testing.
Abbreviations
AACTT, Actor Action Context Time Target framework; CFIR, Consolidated Framework for Implementation Research; ERIC, Expert Recommendations for Implementing Change; PAIDSEM-P, preoperative anemia and iron deficiency screening, evaluation and management pathway/s; PBM, patient blood management.
Data Sharing Statement
All data generated or analysed during this study are available in the published article and the attached file.
Ethics Approval and Informed Consent
Low-risk ethical approval was gained from the hospital and the University of Newcastle Human Research Ethics Committees (HREC). Written informed consent was gained from participants, prior to participation in the study. It was emphasized that participation was voluntary, and all participants were informed that they could withdraw from the study up until their data were de-identified (which was specified as five business days from completion of data collection). Data will be stored for at least 15 years, as per the Australian Code for the Responsible Conduct of Research.33 No hard copy data collected for this study will be retained in its original form. Any hard copy data were destroyed via the hospital confidential waste system after being scanned and stored on the hospital’s secure drive in a password-protected file. All other electronic data have been stored in this manner also.
Consent for Publication
All participants were given an opportunity to review the preliminary results and edit their answers before the publication of the study.
Acknowledgments
AD gratefully acknowledges assistance received from the Australian Government Research Training Program Scholarship. AD also thanks all study participants for giving their time and assistance with this important project.
Authors’ Information
AD is a Registered Nurse with a background in perioperative settings. She holds a BN, GCertPeriopN, MN and is working towards completion of a PhD. She has prior experience in conducting interviews and has undergone training in qualitative data collection methods. Currently, she works as a Quality Coordinator overseeing the Blood Management and Apheresis portfolio at Mater Hospital. As a result, AD has a pre-existing working relationship with all interview participants, and conversations about the project occur on an ongoing basis. Participants were made fully aware that the interview data collected would form part of a PhD for publication. Informed consent was obtained from all participants, and it was stressed that confidentiality of responses would be maintained. This review has been undertaken with the intent of inclusion in the AD’s Doctor of Philosophy Thesis.
JD is a Professor of Nursing, jointly employed by the Queensland University of Technology and The Royal Women’s and Children's Hospital, Brisbane.
JM is a Lecturer in Nursing, jointly employed by the Queensland University of Technology and the University of Adger in Norway.
JH is a Professor in the University of Queensland school of medicine and is the Director of Palliative and Supportive Care at the Mater Hospital Brisbane.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
AD gratefully acknowledges the financial support received from the University of Newcastle that assisted with transcription costs. AD also gratefully acknowledges the support received from the Mater Foundation.
Disclosure
The authors declare they have no competing interests.
References
1. Munting KE, Klein AA. Optimisation of pre-operative anaemia in patients before elective major surgery - why, who, when and how? Anaesthesia. 2019;74(Suppl 1):49–57.
2. Carson JL, Triulzi DJ, Ness PM. Indications for and adverse effects of red-cell transfusion. N Engl J Med. 2017;377(13):1261–1272. doi:10.1056/NEJMra1612789
3. Goel R, Patel EU, Cushing MM, et al. Association of perioperative red blood cell transfusions with venous thromboembolism in a North American registry. JAMA Surg. 2018;153(9):826–833. doi:10.1001/jamasurg.2018.1565
4. Faulds J, Whately-Smith C, Clarke K. Transfusion requirement and length of stay of anaemic surgical patients associated with a patient blood management service: a single-centre retrospective study. Transfus Med. 2019;29(5):311–318. doi:10.1111/tme.12617
5. National Blood Authority, National Health Medical Research Council. Patient Blood Management Guidelines: Module 2 - Perioperative. Canberra, ACT: National Blood Authority; 2012.
6. Vaglio S, Gentili S, Marano G, et al. The italian regulatory guidelines for the implementation of patient blood management. Blood Transfus. 2017;15(4):325–328.
7. Meybohm P, Froessler B, Goodnough LT, et al. “Simplified International Recommendations for the Implementation of Patient Blood Management” (SIR4PBM). Perioper Med (Lond). 2017;6:5. doi:10.1186/s13741-017-0061-8
8. Gammon HM, Waters JH, Watt A, Loeb JM, Donini-Lenhoff A. Developing performance measures for patient blood management. Transfusion. 2011;51(11):2500–2509. doi:10.1111/j.1537-2995.2011.03406.x
9. Delaforce A, Duff J, Munday J, Hardy J. Overcoming barriers to evidence-based patient blood management: a restricted review. Implement Sci. 2020;15(1):6. doi:10.1186/s13012-020-0965-4
10. Damschroder LJ. Clarity out of chaos: use of theory in implementation research. Psychiatry Res. 2020;283:112461. doi:10.1016/j.psychres.2019.06.036
11. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4(1):50. doi:10.1186/1748-5908-4-50
12. Presseau J, McCleary N, Lorencatto F, Patey AM, Grimshaw JM, Francis JJ. Action, actor, context, target, time (AACTT): a framework for specifying behaviour. Implement Sci. 2019;14(1):102. doi:10.1186/s13012-019-0951-x
13. Waltz TJ, Powell BJ, Fernandez ME, Abadie B, Damschroder LJ. Choosing implementation strategies to address contextual barriers: diversity in recommendations and future directions. Implement Sci. 2019;14(1):42.
14. Delaforce A, Moore D, Duff J, Munday J, Hardy J. Assessing transfusion practice in elective surgical patients: a baseline audit. ISBT Sci Series. 2019;14(4):415–422. doi:10.1111/voxs.12496
15. Palinkas LA, Horwitz SM, Green CA, Wisdom JP, Duan N, Hoagwood K. Purposeful sampling for qualitative data collection and analysis in mixed method implementation research. Adm Policy Ment Health. 2015;42(5):533–544. doi:10.1007/s10488-013-0528-y
16. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
17. Pluddemann A, Aronson JK, Onakpoya I, Heneghan C, Mahtani KR. Redefining rapid reviews: a flexible framework for restricted systematic reviews. BMJ Evid Based Med. 2018;23(6):201–203. doi:10.1136/bmjebm-2018-110990
18. Morgan PN, Coleman PL, Martinez-Garduno CM, Gunaratne AW, McInnes E, Middleton S. Implementation of a patient blood management program in an Australian private hospital orthopedic unit. J Blood Med. 2018;9:83–90. doi:10.2147/JBM.S157571
19. Duckett SJ. Living in the parallel universe in Australia: public Medicare and private hospitals. Cmaj. 2005;173(7):745–747. doi:10.1503/cmaj.051011
20. Abbett SK, Kaufman RM, Gustafson M, Greenberg JO. Multifaceted approach to reducing unnecessary red blood cell utilization. Healthc (Amst). 2015;3(2):67–73. doi:10.1016/j.hjdsi.2014.07.003
21. Oliver JC, Griffin RL, Hannon T, Marques MB. The success of our patient blood management program depended on an institution-wide change in transfusion practices. Transfusion. 2014;54(10 Pt 2):2617–2624. doi:10.1111/trf.12536
22. Carman KL, Dardess P, Maurer M, et al. Patient and family engagement: a framework for understanding the elements and developing interventions and policies. Health Aff (Millwood). 2013;32(2):223–231. doi:10.1377/hlthaff.2012.1133
23. Flores CJ, Sethna F, Stephens B, et al. Improving patient blood management in obstetrics: snapshots of a practice improvement partnership. BMJ Qual Improv Rep. 2017;6:1. doi:10.1136/bmjquality-2017-000009
24. Liao A, Burgess M, Barritt-Eyles R, Trompf L, Crispin P. Perceptions on consumer information in transfusion. A qualitative study of consumers and prescribers. Vox Sang. 2020;n/a(n/a).
25. Brevig J, McDonald J, Zelinka ES, Gallagher T, Jin R, Grunkemeier GL. Blood transfusion reduction in cardiac surgery: multidisciplinary approach at a Community Hospital. Ann Thorac Surg. 2009;87(2):532–539. doi:10.1016/j.athoracsur.2008.10.044
26. Farmer SL, Towler SC, Leahy MF, Hofmann A. Drivers for change: Western Australia Patient Blood Management Program (WA PBMP), World Health Assembly (WHA) and Advisory Committee on Blood Safety and Availability (ACBSA). Best Pract Res Clin Anaesthesiol. 2013;27(1):43–58. doi:10.1016/j.bpa.2012.12.007
27. Albinarrate A, Lopez-Picado A, Oiartzabal I, Lopez-Ariznabarreta C, Molano J, Barrachina B. Assessment of the introduction of a blood management program in orthopaedic surgery. Rev Esp Anestesiol Reanim. 2015;62(8):443–449. doi:10.1016/j.redar.2014.09.004
28. Gallagher T, Leahy MF, Darby S, et al. Assembling a state-wide patient blood management program as a standard of care: the Western Australian experience. ISBT Sci Series. 2017;12(3):365–374. doi:10.1111/voxs.12350
29. Garrioch M, Sandbach J, Pirie E, Morrison A, Todd A, Green R. Reducing red cell transfusion by audit, education and a new guideline in a large teaching hospital. Transfus Med. 2004;14(1):25–31. doi:10.1111/j.0958-7578.2004.00476.x
30. Mallett SV, Armstrong M. Point-of-care monitoring of haemostasis. Anaesthesia. 2015;70(Suppl 1):
31. Fischer DP, Zacharowski KD, Müller MM, et al. Patient blood management implementation strategies and their effect on physicians’ risk perception, clinical knowledge and perioperative practice - the Frankfurt experience. Transfusion Med Hemother. 2015;42(2):91–97. doi:10.1159/000380868
32. Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ (Clinical Research Ed). 1996;312(7023):71–72. doi:10.1136/bmj.312.7023.71
33. National Health and Medical Research Council ARC, Universities Australia. Australian Code for the Responsible Conduct of Research. Canberra: Australian Government; 2007.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.