")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Prenatal Diagnosis of Congenital Heart Disease and Voluntary Termination of Pregnancy: A Population-Based Study in Qingdao, China
Authors Lu X, Li G, Wu Q, Ni W, Pan S, Xing Q
Received 15 November 2023
Accepted for publication 11 January 2024
Published 20 January 2024 Volume 2024:17 Pages 205—212
DOI https://doi.org/10.2147/RMHP.S447493
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Xuning Lu,1,2 Guoju Li,1 Qin Wu,1 Wei Ni,1 Silin Pan,1 Quansheng Xing1
1Heart Center, Qingdao Women and Children’s Hospital, Shandong University, Qingdao, Shandong Province, People’s Republic of China; 2Heart Center, Dalian Municipal Women and Children’s Medical Center (Group), Dalian, Liaoning Province, People’s Republic of China
Correspondence: Quansheng Xing, Heart Center, Qingdao Women and Children’s Hospital, Shandong University, 217 Liaoyang West Road, Qingdao, Shandong Province, 266034, People’s Republic of China, Tel +86 136 0642 6893, Fax +86 532 8285 7650, Email [email protected]
Objective: The outcomes of fetuses with isolated congenital heart disease (CHD) diagnosed prenatally have not been investigated in a population-based study in China. This population-based study aimed to evaluate the rate of voluntary termination of pregnancy after the prenatal diagnosis of isolated CHD in Qingdao, China.
Methods: This was a population-based retrospective study in which data were collected from all pregnant women in Qingdao (eastern China) from August 2018 to July 2020; fetal data, maternal data and data on pregnancy outcomes were extracted from medical records regarding prenatal diagnosis of CHD. The inclusion criteria were as follows: pregnant women or their husbands who had a household registration in Qingdao and who underwent regular prenatal screening in Qingdao. The exclusion criterion was the failure to sign an informed consent form. Counseling for all parents of fetuses with CHD was provided by a multidisciplinary team of experienced pediatric cardiologists, obstetricians, geneticists, etc. According to the type and severity of CHD, the pregnancy termination rate was analyzed.
Results: Among the 126,843 pregnant women, 1299 fetuses with a prenatal diagnosis of CHD were included in the study. Among the included fetuses, 1075 were diagnosed with isolated CHD, and the overall pregnancy termination rate was 22.8%. Termination rates varied according to the complexity of CHD (low complexity vs moderate complexity, P=0.000; low complexity vs high complexity, P=0.000; moderate complexity vs high complexity, P=0.000), with rates of 6.0% for low complexity, 54.2% for moderate complexity, and 99.1% for high complexity. The decision to terminate the pregnancy in cases of isolated CHD was unrelated to maternal age (P=0.091) but was related to gestational age (p=0.000).
Conclusion: In Qingdao, 99.1% of parents whose fetuses were diagnosed with isolated high-complexity CHD chose to voluntarily terminate the pregnancy. The pregnancy termination rate increased with increasing complexity of prenatally diagnosed CHD.
Plain Language Summary: In our study population, with the popularity of prenatal diagnosis, complex congenital heart disease will disappear, because 99.1% of parents whose fetuses were diagnosed with isolated high-complexity congenital heart disease chose voluntary pregnancy termination.
Keywords: congenital heart defect, fetal echocardiography, prenatal diagnosis, termination of pregnancy
Introduction
Congenital heart disease (CHD) is a gross structural abnormality of the heart or intrathoracic great vessels that may have functional significance.1 CHD is the most common birth defect, the incidence of which ranges from 0.6% to 0.7%, and it accounts for 30–50% of infant deaths caused by birth defects.2–7 In China, approximately 150,000 to 200,000 children with CHD are born every year.8 In recent years, with advances in fetal echocardiography, the prenatal diagnosis of CHD has shown a spectrum similar to that seen in the diagnosis of postnatal disease, and the prenatal diagnosis of CHD in early pregnancy has increased. On the one hand, prenatal diagnosis can be useful in optimizing perinatal management; on the other hand, it provides opportunities for prenatal counseling and is helpful for parents in deciding whether to terminate the pregnancy.9–13 Studies have shown that parents’ decisions regarding termination of pregnancy (TOP) are influenced not only by the severity of CHD and the gestational age at the time of diagnosis but also by society, religion and culture.14,15 The purpose of this population-based study was to clarify the rate of voluntary TOP given a prenatal diagnosis of isolated CHD.
Materials and Methods
We conducted a population-based cohort study to collect data from all pregnant women registered in the Qingdao Women’s and Children’s Health Center system from August 2018 to July 2020 in Qingdao, a city on China’s east coast with a population of 10.25 million people. The inclusion criteria were as follows: pregnant women or their husbands had a household registration in Qingdao and who underwent regular prenatal screening in Qingdao. The exclusion criterion was the failure to sign an informed consent form. The system established in 2018 includes all relevant institutions in the maternal and child health management network and is jointly managed by the Qingdao Municipal Center for Birth Defect Control and Qingdao Women and Children’s Hospital. The system covers all pregnant women in the Qingdao area, includes the results of regular health examinations and prepregnancy and delivery data, and uses ID numbers as the unique identifiers of pregnant women with data in the database. If a fetus is diagnosed with CHD, a multidisciplinary team informs the family, provides medical advice, and discusses the clinical significance of the diagnosis, including possible neurologic sequelae and heart malformations. The team consists of experienced gynecologists, pediatric cardiologists, geneticists, and specialists in fetal medicine. In this article, fetal data, maternal data and data on pregnancy outcomes were extracted for fetuses diagnosed with CHD, and we focused on the analysis of the termination or continuation of pregnancy for fetuses diagnosed with isolated CHD.
We classified all cases of CHD into 9 phenotypes: septal defects (phenotype 1), conotruncal defects (phenotype 2), left ventricle outflow tract obstruction (LVOTO, phenotype 3), right ventricle outflow tract obstruction (RVOTO, phenotype 4), atrioventricular septal defects (AVSDs, phenotype 5), anomalous pulmonary venous return (APVR, phenotype 6), univentricular heart or isomerism (phenotype 7), vascular rings (phenotype 8), and cardiac tumors (phenotype 9). In addition, according to the guidelines of the American Heart Association and the American College of Cardiology published in 2018, all patients with isolated CHD diagnosed during the fetal period were divided into three groups, namely, low complexity, moderate complexity and high complexity,16 to analyze the change in the TOP rate among the groups. In the case of multiple related cardiac malformations, the pathology that had the greatest impact on prognosis in terms of the requirement for major surgery was used for classification.
A P value < 0.01 was considered to indicate statistical significance, and SPSS statistics version 19.0 (SPSS, Inc., Chicago, IL) was used for statistical analysis. The difference between the women who decided to terminate their pregnancies and those who decided to continue their pregnancies was evaluated by an unmatched t-test and Fisher’s exact test or the χ2 test if appropriate. Descriptive statistics are expressed as the mean, percentage, range and frequency. The main outcome was the TOP due to fetal CHD.
This study was approved by the Ethics Committee of Qingdao Women’s and Children’s Hospital, and written informed consent was obtained from the patients before selection. The study protocol adhered to the ethical guidelines of the Declaration of Helsinki.
Results
Overall, a total of 139,472 pregnant women were registered in the system. Among these women, 126,843 underwent obstetrical ultrasound; however, 1243 had multiple fetuses, and 8639 had fetuses with no follow-up data available and were therefore excluded from this study. A total of 1299 fetuses diagnosed with CHD were ultimately included in the study, and the distribution is shown in Figure 1. Details for the following are shown in Table 1: septal defects accounted for 73.3% of the cases, including atrial septal defects (ASDs) and ventricular septal defects (VSDs); conotruncal defects accounted for 9.8% of the cases, including transposition of the great arteries (TGA), double-outlet right ventricle (DORV), and tetralogy of Fallot (TOF); LVOTO accounted for 4.3% of the cases, including coarctation of aorta (CoA), hypoplastic left heart syndrome (HLHS), and interrupted aortic arch (IAA); RVOTO accounted for 5.0% of the cases, including hypoplastic right heart syndrome (HRHS), pulmonary atresia (PA), and the Ebstein anomaly; AVSDs accounted for 3.0% of the cases; APVR accounted for 0.8% of the cases, including partial or total APVR; univentricular heart or isomerism accounted for 1.6% of the cases; vascular rings accounted for 1.7% of the cases; and cardiac tumors accounted for 0.5% of the cases.
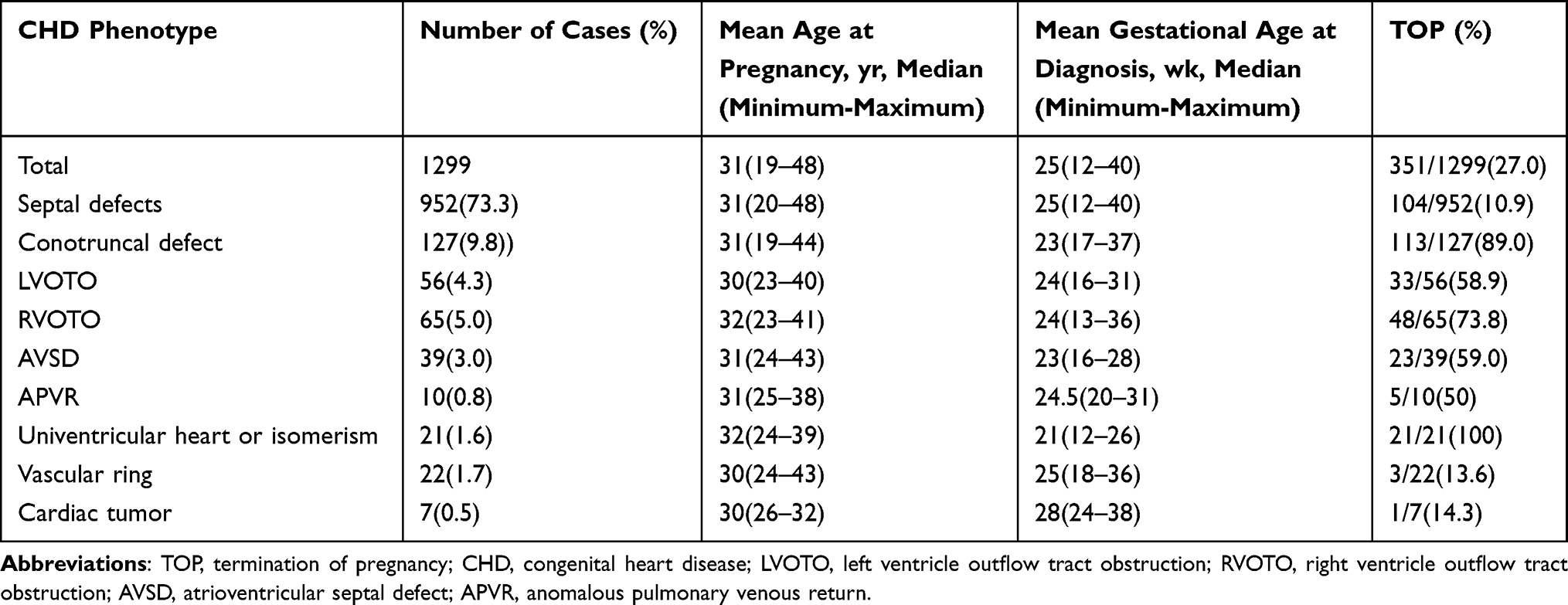 |
Table 1 Characteristics and Number of Pregnancies Terminated for Each CHD Phenotype |
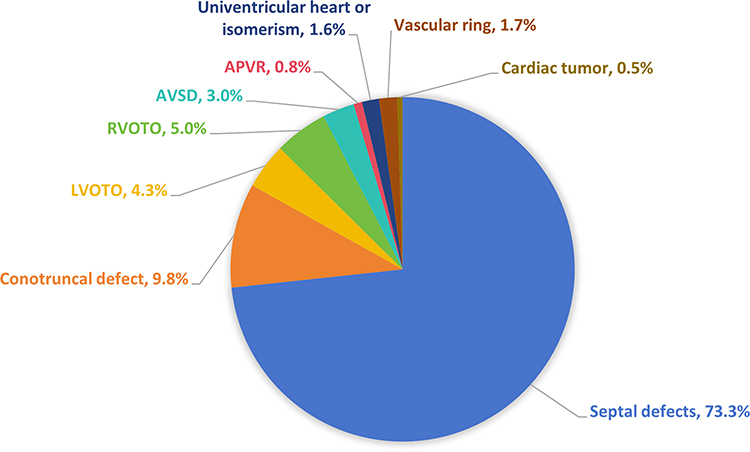 |
Figure 1 The distribution of CHD in our study. Abbreviations: CHD, congenital heart defect; LVOTO, left ventricle outflow tract obstruction; RVOTO, right ventricle outflow tract obstruction; AVSD, atrioventricular septal defect; APVR, anomalous pulmonary venous return. |
The median maternal age of the 1299 women was 31 (19–48) years, and the median gestational age at CHD diagnosis was 25 (12–40) weeks. A total of 1075 of the 1299 (82.8%) fetuses were diagnosed with isolated CHD, and 224 of the 1299 (17.2%) fetuses with CHD were diagnosed with CHD combined with other extracardiac malformations, other genetic pathologies, or chromosomal abnormalities. The percentage of pregnancies terminated according to the type of CHD is shown in Figure 2. The percentage pregnancies terminated was 22.8% (245 of 1075) in the isolated CHD group, while in the group with CHD combined with other extracardiac malformations, other genetic pathologies or chromosomal abnormalities, the percentage was 47.3% (106 of 224). The difference between the two groups was significant (P=0.000) (Table 2).
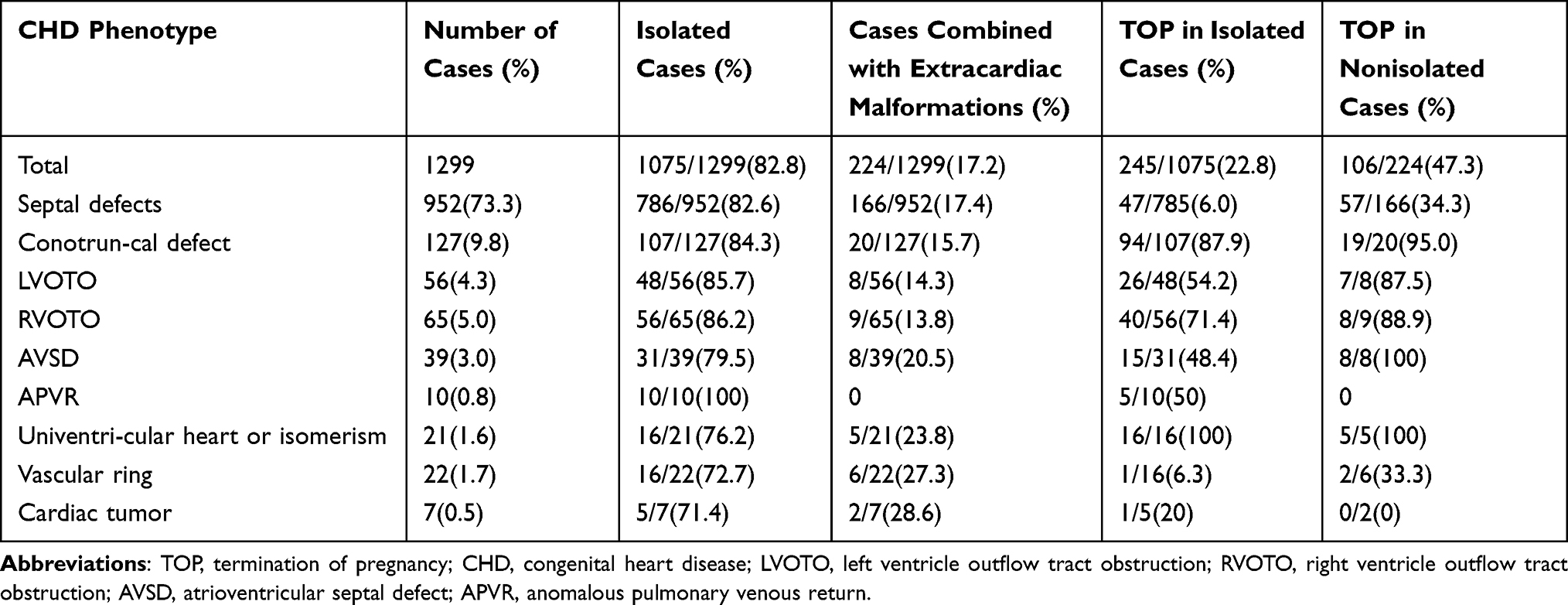 |
Table 2 Characteristics and Number of Pregnancies Terminated for Each CHD Phenotype in Fetuses with Isolated CHD vs CHD Combined Extracardiac Malformations |
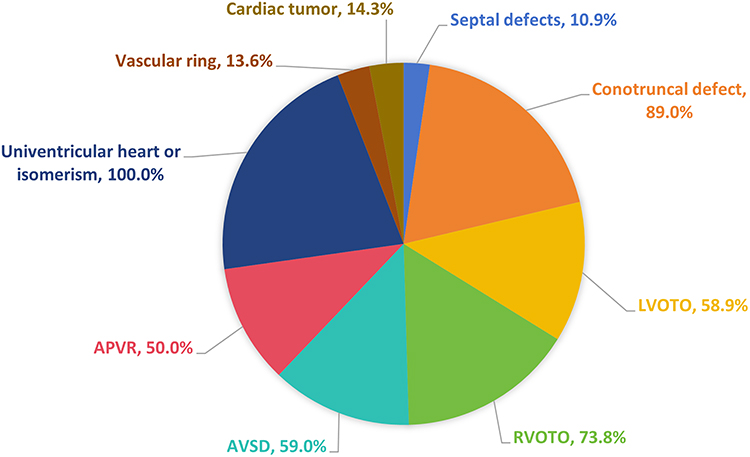 |
Figure 2 The TOP rate according to the type of CHD. Abbreviations: CHD, congenital heart defect; LVOTO, left ventricle outflow tract obstruction; RVOTO, right ventricle outflow tract obstruction; AVSD, atrioventricular septal defect; APVR, anomalous pulmonary venous return; TOP, termination of pregnancy. |
As shown in Table 2, Group 1 included 139 cases of ASDs and 813 cases of VSDs, and the TOP rate among women whose fetuses were diagnosed with isolated CHD was 6.0%; Group 2 included 33 cases of TGA, 68 cases of TOF, 25 cases of DORV, and 1 case of double-outlet light ventricle (DOLV), and the TOP rate among women whose fetuses were diagnosed with isolated CHD was 87.9%; Group 3 included 9 cases of HLHS, 40 cases of CoA, 4 cases of IAA, and 3 cases of mitral atresia (MA), and the TOP rate among women whose fetuses were diagnosed with isolated CHD was 54.2%; Group 4 included 6 cases of HRHS, 5 cases of the Ebstein anomaly, 22 cases of PS, 28 cases of PA, and 4 cases of tricuspid atresia (TA), and the TOP rate among women whose fetuses were diagnosed with isolated CHD was 71.4%. In Group 5, the TOP rate among women whose fetuses were diagnosed with isolated AVSD was 48.4% Group 6 included 10 cases of total anomalous pulmonary venous return (TAPVR), and the TOP rate among women whose fetuses were diagnosed with isolated TAPVR was 50%. In Group 7, the TOP rate among women whose fetuses were diagnosed with isolated univentricular heart or isomerism was 100%. Group 8 included 2 cases of double aortic arch (DAA), 18 cases of right aortic arch with left ligamentum (RAA-LD), and 2 cases of pulmonary artery sling (PAS), and the TOP rate among women whose fetuses were diagnosed with isolated vascular ring corresponded to the one case of PAS. In Group 9, 7 cardiac tumors were presumed to be rhabdomyomas, of which 4 were in the left ventricle, 2 were in the right ventricle, and 1 involved both ventricles, and TOP was performed.
As shown in Table 3, the TOP rate among women whose fetuses were diagnosed with isolated CHD was 6.0% in the low-complexity group, 54.2% in the moderate-complexity group and 99.1% in the high-complexity group. There was a significant difference in the TOP rate among women whose fetuses were diagnosed with isolated CHD between the low-complexity group and the moderate-complexity group (P=0.000) or the high-complexity group (P=0.000), and there was a significant difference between the moderate-complexity group and the high-complexity group (P=0.000). In addition, in terms of maternal age and gestational age, there was a significant difference between women who continued their pregnancies and those who chose TOP (P=0.009, P=0.000). However, after excluding factors related to CHD combined with extracardiac malformations, we detected no significant difference in maternal age of women whose fetuses were diagnosed with isolated CHD (P=0.091).
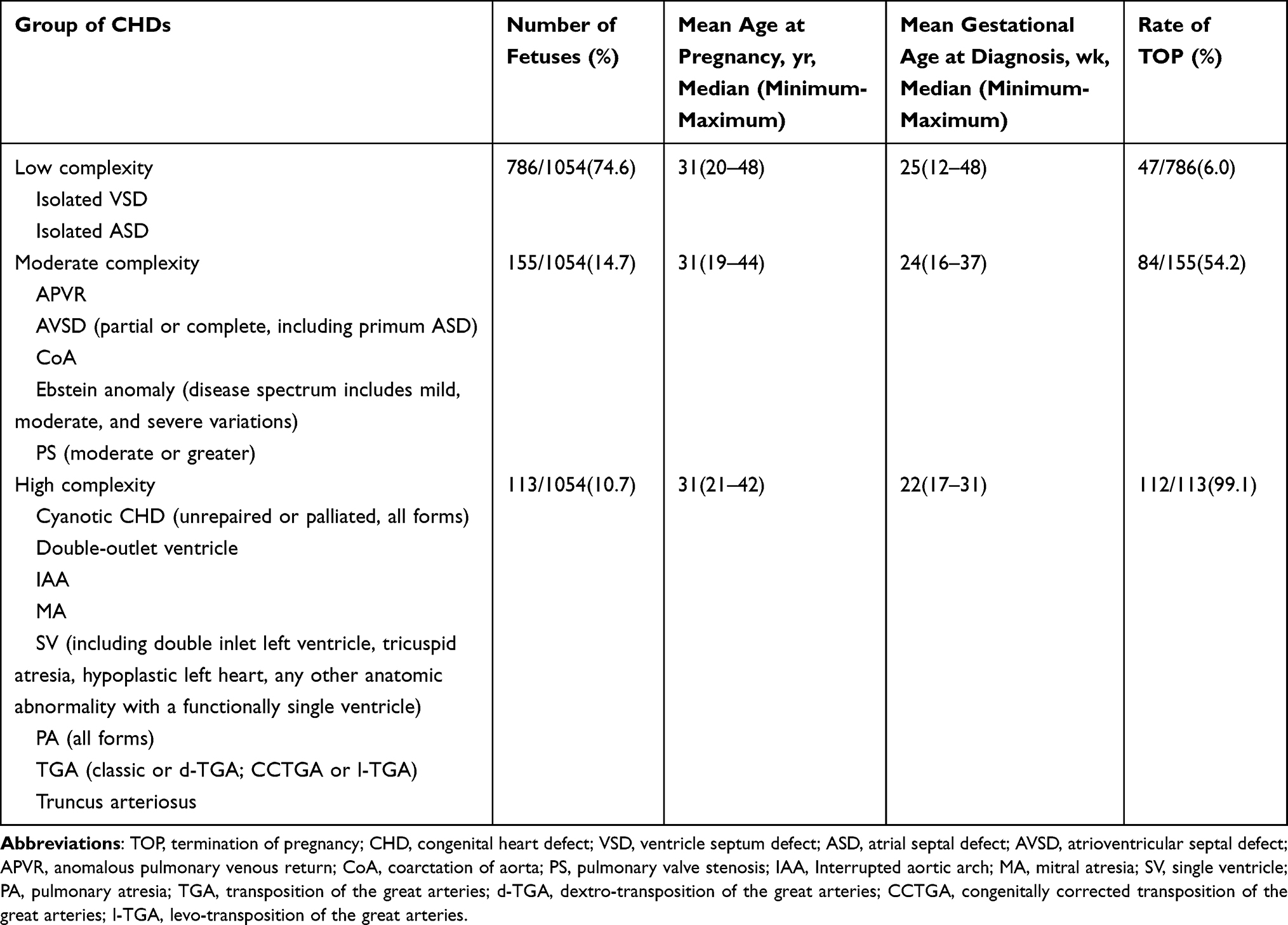 |
Table 3 TOP Rate in Each Group of Fetuses with Isolated CHD According to the American Heart Association and American College of Cardiology Guidelines16 |
Discussion
Principal Findings
In our population, the incidence of TOP increased with increasing complexity of prenatally diagnosed CHD. The TOP rate among women whose fetuses were diagnosed with isolated CHD was 6.0% in the low-complexity group, 54.2% in the moderate-complexity group and 99.1% in the high-complexity group.
Results for What is Known
In this study, there were significant differences in maternal age and gestational age between women who continued their pregnancies and those who chose TOP. However, there was no significant difference in maternal age among women whose fetuses were diagnosed with isolated CHD. In terms of the complexity of CHD, with increasing complexity, the TOP rate among women whose fetuses were diagnosed with isolated CHD increased significantly, and there was a significant difference between the low-complexity group and the moderate-complexity group or high-complexity group. These results are consistent with previous studies.17
Clinical and Research Implications
In Qingdao, a total of 99.1% of parents whose fetuses were diagnosed with isolated high-complexity CHD chose voluntary TOP; when parents are told that their fetus has CHD, their feelings and thoughts about whether to terminate or continue pregnancy are greatly impacted. Therefore, the process of consultation and notification has become particularly important. In this process, doctors should not only pay attention to the disease itself but also pay attention to parents’ emotional and psychological changes. The inclusion of a psychiatrist in this process should be considered. In addition, prenatal diagnosis of CHD can reduce the mortality of critical and complex CHD and improve the prognosis.18,19 This study showed that prenatal diagnosis of CHD greatly contributes to voluntary TOP, and how to best use such prenatal diagnosis is worthy of further study.
Strengths and Limitations
To our knowledge, this is the first population-based study on the intrauterine diagnosis of CHD in China; it focused on the decision that parents must make regarding whether to terminate or continue the pregnancy. Second, the research team was composed of experienced pediatric cardiologists, obstetric experts, specialists in fetal medicine and genetic experts. After prenatal diagnosis of CHD, the same team plays a key role in providing information and consultative support for the couple.
In this study, the TOP rate among women whose fetuses were diagnosed with isolated CHD was 6% in the low-complexity group, 54.2% in the moderate-complexity group and 99.1% in the high-complexity group. These results may be related to the following considerations. First, the traditional concept guiding Chinese parents is the desire to have a healthy child. Parents are very frightened when they learn that their child has a congenital heart defect. Although cardiac surgery technologies are currently very mature, parents still choose to terminate the pregnancy. Second, in China, prenatal diagnosis of CHD is reported step by step, and when parents come to a tertiary medical center, they may have already been informed that their fetus has CHD and received inappropriate counseling. Third, the cognitive dissonance associated with a diagnosis of CHD is considerable, especially given the related therapeutic effects and costs of CHD treatment. At present, CHD-related treatment technology is very mature, and the mortality rate is significantly lower than before. However, in China, most of the treatment costs associated with CHD are borne by the government. There is obvious dissonance in people’s cognition regarding these two aspects.
This study has several limitations. First, the duration of the study was approximately 2 years. In future work, we will continue to collect data and evaluate the rate of voluntary TOP given the prenatal diagnosis of isolated CHD and its effect on the disease spectrum. Second, the vast majority of patients in this study were of Chinese ancestry, and we were unable to study the influence of race on pregnancy decisions. Third, the loss of follow-up data may have had an impact on the observed TOP rate.
Conclusion
The rate of voluntary TOP after the prenatal diagnosis of CHD increases significantly with increasing CHD complexity. However, in our study population, the voluntary TOP rate was 6% for low-complexity CHD and nearly 100% for high-complexity CHD. In addition, the rate of voluntary TOP with univentricular heart or isomerism was 100%.
Acknowledgments
The authors would like to thank all the doctors, nurses, and patients who participated in the study.
Funding
This work is supported by the National Natural Science Foundation of China (NSFC) [Grant numbers 81770315, 82071583], the Taishan Scholars Program, and the China Postdoctoral Science Foundation Funded Project [Grant number 2019M662307].
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
References
1. Mitchell SC, Korones SB, Berendes HW. Congenital heart disease in 56,109 births. Incidence and natural history. Circulation. 1971;43:323–332. doi:10.1161/01.cir.43.3.323
2. Dolk H, Loane M, Garne E; European Surveillance of Congenital Anomalies (EUROCAT) Working Group. Congenital heart defects in Europe: prevalence and perinatal mortality, 2000 to 2005. Circulation. 2011;123(8):841–849. doi:10.1161/CIRCULATIONAHA.110.958405
3. Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39(12):1890–1900. doi:10.1016/s0735-1097(02)01886-7
4. Van der linde D, Konings EE, Slager MA, et al. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol. 2011;58:2241–2247. doi:10.1016/j.jacc.2011.08.025
5. Harris KW, Brelsford KM, Kavanaugh-McHugh A, Clayton EW. Uncertainty of prenatally diagnosed congenital heart disease: a qualitative study. JAMA Netw Open. 2020;3(5):Article e204082. doi:10.1001/jamanetworkopen.2020.4082
6. Pradat P, Francannet C, Harris JA, Robert E. The epidemiology of cardiovascular defects, part I: a study based on data from three large registries of congenital malformations. Pediatr Cardiol. 2003;24(3):195–221. doi:10.1007/s00246-002-9401-6.2003
7. Tegnander E, Williams W, Johansen OJ, Blaas HG, Eik-Nes SH. Prenatal detection of heart defects in a non-selected population of 30,149 fetuses: detection rates and outcome. Ultrasound Obstet Gynecol. 2006;27(3):252–265. doi:10.1002/uog.2710
8. Cawsey MJ, Noble S, Cross-Sudworth F, et al. Feasibility of pulse oximetry screening for critical congenital heart defects in homebirths. Arch Dis Child Fetal Neonatal Ed. 2016;101(4):349–351. doi:10.1136/archdischild-2015-309936
9. Bull C, Assoc BPC. Current and potential impact of fetal diagnosis on prevalence and spectrum of serious congenital heart disease at term in the UK. Lancet. 1999;354:1242–1247. doi:10.1016/S0140-6736(99)01167-8
10. Huang H, Cai M, Wang Y, Liang B, Lin N, Liangpu X. SNP array as a tool for prenatal diagnosis of congenital heart disease screened by echocardiography: implications for precision assessment of fetal prognosis. Risk Manag Healthc Policy. 2021;14:345–355. doi:10.2147/RMHP.S286001
11. McAuliffe FM, Trines J, Nield LE, Chitayat D, Jaeggi E, Hornberger LK. Early fetal echocardiography: a reliable prenatal diagnosis tool. Am J Obstet Gynecol. 2005;193:1253–1259. doi:10.1016/j.ajog.2005.05.086
12. Khoshnood B, De Vigan C, Vodovar V, et al. Trends in prenatal diagnosis, pregnancy termination, and perinatal mortality of newborns with congenital heart disease in France, 1983–2000: a population-based evaluation. Pediatrics. 2005;115(1):95–101. doi:10.1542/peds.2004-0516
13. Carlsson T, Bergman G, Wadensten B, Mattsson E. Experiences of informational needs and received information following a prenatal diagnosis of congenital heart defect. Prenat Diagn. 2016;36(6):515–522. doi:10.1002/pd.4815
14. Tararbit K, Lelong N, Jouannic JM, Goffinet F, Khoshnood B. Is the probability of prenatal diagnosis or termination of pregnancy different for fetuses with congenital anomalies conceived following assisted reproductive techniques? A population-based evaluation of fetuses with congenital heart defects. BJOG. 2015;122(7):924–931. doi:10.1111/1471-0528.13345
15. Chenni N, Lacroze V, Pouet C, Fraisse A, Kreitmann B, Gamerre M. Fetal heart disease and interruption of pregnancy: factors influencing the parental decision-making process. Prenat Diagn. 2012;32(2):168–172. doi:10.1002/pd.2923
16. Stout KK, Daniels CJ, Aboulhosn JA, et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease: executive summary: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. Circulation. 2019;139:e637–e697. doi:10.1161/CIR.0000000000000602
17. Montaguti E, Balducci A, Perolo A, et al. Prenatal diagnosis of congenital heart defects and voluntary termination of pregnancy. Am J Obstet Gynecol. 2020;2(4):100207. doi:10.1016/j.ajogmf.2020.100207
18. Tworetzky W, McElhinney DB, Reddy VM, Brook MM, Hanley FL, Silverman NH. Improved surgical outcome after fetal diagnosis of hypoplastic left heart syndrome. Circulation. 2001;103(9):1269–1273. doi:10.1161/01.CIR.103.9.1269
19. Van Velzen CL, Haak MC, Reijnders G, et al. Prenatal detection of transposition of the great arteries reduces mortality and morbidity. Ultrasound Obstet Gynecol. 2015;45(3):320–325. doi:10.1002/uog.14689
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.