Back to Journals » Patient Preference and Adherence » Volume 16
Preferences for Patients with Type 2 Diabetes Mellitus for Medications in Shandong Province, China: A Discrete Choice Experiment
Authors Lv Y ![]() , Ren R, Tang C, Song K, Li S
, Ren R, Tang C, Song K, Li S ![]() , Wang H
, Wang H ![]()
Received 31 March 2022
Accepted for publication 10 August 2022
Published 25 August 2022 Volume 2022:16 Pages 2335—2344
DOI https://doi.org/10.2147/PPA.S367985
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Naifeng Liu
Yuyu Lv,1,2 Ru Ren,1– 3 Chengxiang Tang,4 Kuimeng Song,5 Shunping Li,1– 3 Haipeng Wang1,2
1Center for Health Management and Policy Research, School of Public Health, Cheeloo College of Medicine, Shandong University, Jinan, People’s Republic of China; 2NHC Key Laboratory of Health Economics and Policy Research (Shandong University), Jinan, People’s Republic of China; 3Center for Health Preference Research, Shandong University, Jinan, People’s Republic of China; 4Macquarie University Centre for the Health Economy, Macquarie University Business School & Australian Institute of Health Innovation, Macquarie University, Sydney, NSW, Australia; 5School of Health Care Security, Shandong First Medical University & Shandong Academy of Medical Sciences, Jinan, People’s Republic of China
Correspondence: Shunping Li; Haipeng Wang, Centre for Health Management and Policy Research, Wenhua Xi Road 44, Jinan, Shandong Province, 250012, People’s Republic of China, Tel +86-131-8893-4998, +86-186-6899-6362, Email [email protected]; [email protected]
Purpose: To evaluate preferences for medications among patients with type 2 diabetes mellitus (T2DM) from urban community health stations or rural village clinics in Shandong province, China.
Methods: We use a discrete choice experiment (DCE) to measure the medication preferences. Each patient completed six DCE choice sets. The attributes for the DCE questionnaire include mode of administration, out-of-pocket medication cost per month, fasting blood glucose control effect and frequency of hypoglycemia events. The conditional logit model (Clogit) and mixed logit model (MXL) were used to evaluate choice data.
Results: A total of 887 patients with T2DM completed the survey. The mean age of participants was 64 years, 36.42% experienced complications, and the mean duration of diabetes was about 8 years. Overall, patients’ ideal medication would not have hypoglycemia events, provide normal fasting glucose levels, have oral medication three times a day and lower monthly medication cost. Patients prioritized the frequency of hypoglycemia events (β=15.055, P < 0.01) and were willing to spend CNY 393.10 per month to avoid hypoglycemia events. For patients with higher educational levels and with longer diagnosis time, the effect of fasting blood glucose was more relevant than all other outcomes.
Conclusion: This study provides information on T2DM patients’ preference for medications. Our results suggest that clinical doctors should present patients with a variety of pharmaceutical characteristics and include their preference into medication decision, which will improve patient adherence and health outcomes.
Keywords: type 2 diabetes mellitus, patients’ preference, medication, discrete choice experiment
Introduction
Diabetes mellitus is a chronic metabolic disorder characterized by a long disease course and being prone to a variety of serious complications that significantly impact patients’ quality of life.1 According to the International Diabetes Federation (IDF), the prevalence of diabetes is 10.5% among adults aged 20–79 years globally in 2021. While China has the largest number of people at risk of diabetes, it is estimated the adults with diabetes will reach to 164 million by 2030.2 However, the rate of treatment and control remained at a consistently low level from 2013 to 2018, patients generally have poor medication adherence.3
Type 2 diabetes mellitus (T2DM) accounts for more than 90% of diabetes cases in China.2 Almost all patients with T2DM should take medications for the rest of their lives, as they are critical in lowering glycaemic levels, postponing complications and improving patients’ survival conditions.4 Typically, patients with T2DM are treated with metformin hydrochloride or some injectable drugs such as insulin.5,6 There are multiple medications available to keep their blood glucose levels under control, which vary in efficacy and side effect. Along with the doctor’s guidance, it is necessary to understand the patients’ preferences for medications, since this will involve patients in shared decision-making.
Evidence of patients’ preference for medications offers the potential for shared decision-making in clinical practice, where physicians and patients make decisions together based on individual patient factors and multiple options for T2DM treatment. This will help patients fully understand their condition, reduce concerns about treatment options and improve medication adherence.7 Meanwhile, it will facilitate the transformation of medical decision-making from the traditional “physician-led” to “patient-physician shared decision-making” and better realize “patient-centered” health care services.8,9
So far, there are Stated Preference (SP) and Revealed Preference (RP) methods to measure preferences.10 SP is used to analyze the results of respondents’ choices under the hypothetical scenarios. RP utilizes the observed real-world behavior data.11 Due to the fact that health is not a “typical” market with established pricing mechanisms,12 the discrete choice experiment (DCE) is an SP approach that is more commonly used in healthcare preference studies.13 In recent years, DCE has been conducted in the study of T2DM in a number of developed countries,14–18 but these studies do not adequately represent the general situation in China. To date, there are comparatively few empirical studies in China.19,20 Only one study examined the treatment preferences of patients with T2DM in hospitals, with an emphasis on overall diabetes health management,20 whereas the objective of our study is to assess patient preferences in urban community health stations or rural village clinics, focusing on medications. Therefore, this study will assist doctors in understanding the actual and daily preferences of patients following discharge from hospitals and in developing tailored medication plans.
Methods
DCE is based on the random utility theory, where respondents will choose the option with the greatest utility in given scenarios.21 In DCE, participants are generally expected to trade off in a serious of scenarios, which combine different attributes and levels.13,22 These scenarios refer to medication options consisting of different efficacy and side effects in this study. Patient preferences depend on the level values of these attributes. In addition, researchers can use DCE to estimate respondents’ willingness to pay (WTP) and relative importance for attributes.23 In this study, the DCE was designed and analyzed according to the checklists and good research practices that were conducted by the International Society for Pharmacoeconomics and Outcomes Research (ISPOR).11
Attributes and Levels
Determining attributes and levels is such a significant step in DCE research.24 First of all, we selected 6 attributes through literatures,25–32 included mode of administration, frequency of medication, out-of-pocket medication cost per month, fasting blood glucose control effect, frequency of hypoglycemia events and weight gain per year. Then, we invited 2 experienced clinical doctors in diabetes treatment and 5 patients with T2DM to conduct in-depth interviews. They were asked to rank those 6 possible attributes from the most to the least importance. According to ranking results, the weight gain per year attribute was removed, because they all considered it not significant for medication choices. In addition, we also consulted three experts in the field of DCE, they suggested that the frequency of medication could be combined into the mode of administration. The levels for each of these attributes incorporated a range of possible T2DM medication outcomes. These levels were mainly based on literature, current practice and expert reviews. After a few modifications, the final 4 attributes and corresponding levels are shown in Table 1.
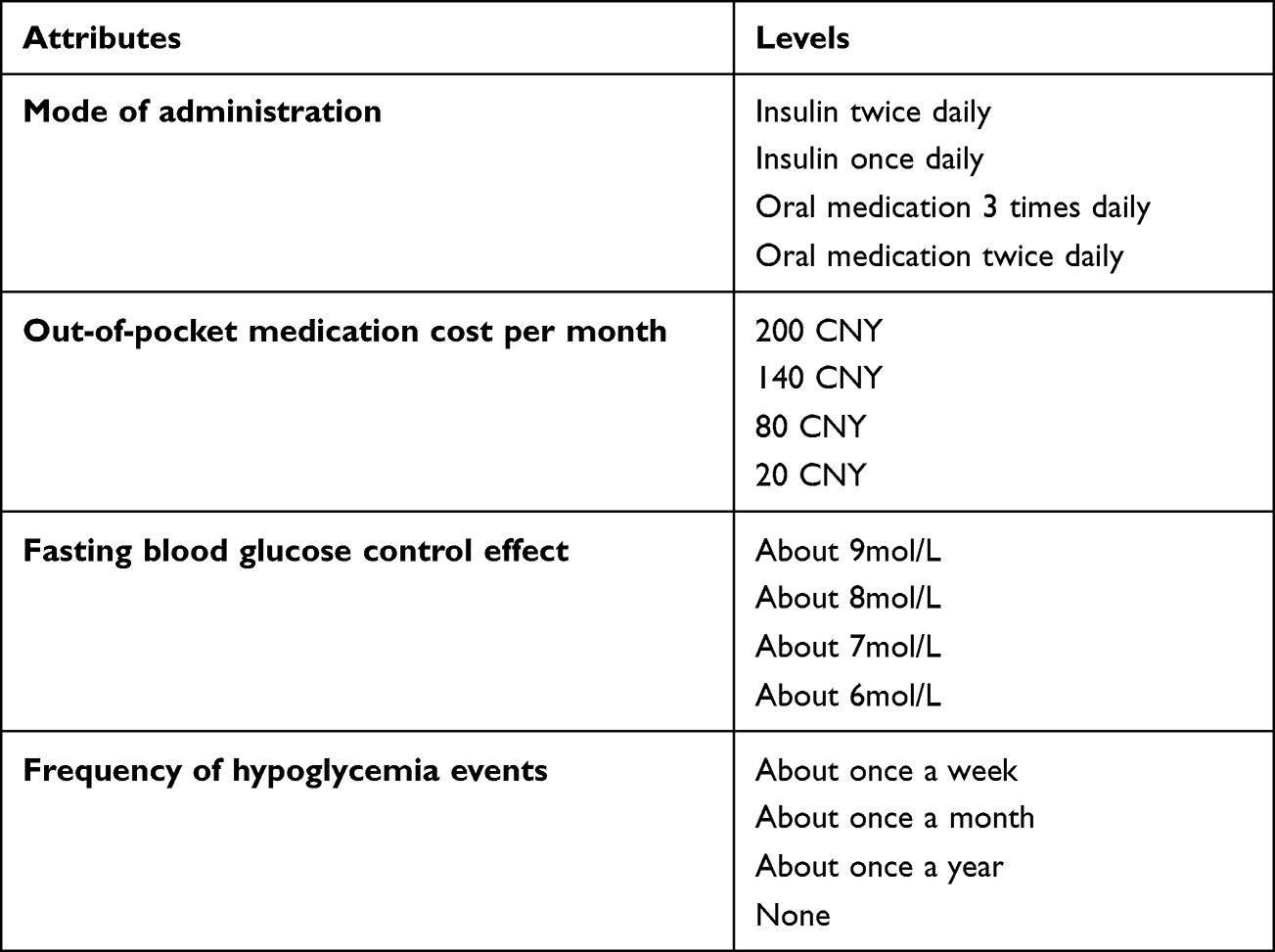 |
Table 1 Attributes and Levels for Discrete Choice Experiment (DCE) Choice Questions |
DCE Design
In this study, we used Ngene software (ChoiceMetrics, Sydney, Australia) to create an orthogonal design.33 The design generated 10 choice sets that further divided into 2 blocks to reduce the response burden of respondents. In addition to using the Ngene software, we also manually added one choice task for each block. This additional choice task was used to test internal consistency,13 in which 1 of 2 alternatives was strictly better than the other for all attributes (but 1) with clear preference. For mode of administration, we used the same level in both medication options. Each respondent was randomly assigned one of the 2 blocks that required 6 DCE questions. We chose to use forced-choice tasks between 2 medication profiles in which respondents indicated which medication they would prefer to take. This setup is usual and considered good research practice in health field.11 An example of DCE question is shown in Table 2.
 |
Table 2 An Example of a Discrete Choice Question (Translated Version) |
Sampling
This study used multistage sampling method. First, we selected 3 prefectures to represent the east (Qingdao), middle (Weifang) and western (Liaocheng) Shandong province according to the geographical location and economic development level. Second, in each prefecture we selected 3 urban districts and 3 rural towns. Third, 3 communities from each district and 3 villages from each town were randomly selected. Eventually, a total of 27 communities and 27 villages were selected as the sample areas. Respondents were eligible if they were above 18 years old, had T2DM diagnosed by physician and were incorporated into the management of basic public health services.
The sample size differed among the DCE studies due to the different number of attribute and level, subgroup analysis and experimental design.34,35 The rules of thumb proposed by Orme B. suggested that we could use the formula (N>500c/(t*a)) to dictate the sample size, where “c” is the number of analysis cells, “t” equals to the number of choice tasks and “a” refers to the number of alternatives.36 When analyzing the main effects, “c” is the largest number of levels of all attributes. Accordingly, our study should be more than 333 participants (500*4/(1*6)). To meet the requirements of the subgroup analysis and improve the credibility of the study results, we decided to appropriately increase the number of samples based on the minimum sample size and the total sample size should be not less than 800. In practice, a total of 887 people participated in this study, of which 885 (99.8%) answered at least one DCE question.
Data Collection
In addition to DCE questions, participants’ socio-demographic characteristics and clinical history were also collected. Prior to data collection from August to September 2019, we conducted a pilot with patients with T2DM in the community (N = 30) to assess the comprehensibility and validity of the experiments. This was deemed appropriate on the basis of pilot results. Considering the age of the participants and the quality of answering, the survey was collected by means of paper-based and one-to-one interviews in community health service centers or village clinics. A gift worth 10 to 20 CNY was used to encourage each respondent to pay attention to the choice tasks.
Data Analysis
The data were double-entered using EpiData version 3.1 and all statistical analyses were operated with STATA 15.1 (StataCorp LP, College Station, TX, USA). All attributes were set as dummy-coded categorical variable in the beginning, but in the mixed logit model (MXL) and the calculation of WTP, cost was specified as a continuous variable. The socio-demographic and clinical data were used for a descriptive analysis, such as Chi-square tests and Student’s t-tests. The conditional logit model (Clogit) and the MXL were used to analyze the data of discrete choice experiment to derive the influence of the medication attributes on the medication selection and the relative importance for patients with T2DM. The coefficients of models indicated relative importance basing on reference levels. The higher the coefficient is, the more attention participants attach to it. Finally, we also conducted the subgroup analyses to understand different population preference heterogeneity, respondents were grouped by age (≤60 or >60 years), education level (illiteracy, primary school, middle school or high school and above), duration of diabetes (<5, 5–10 or >10 years) and complications (yes or no). In later analysis, results were also analyzed by respondent region (rural or city) and gender (male or female).
Results
Participants
Of the participants who answered at least one DCE question, 829 (93.50%) respondents were included in the final main effect analysis due to passing the internal consistency test, indicating most of the participants seriously participated in the survey. There were no significant differences in socio-demographic characteristics between those who failed the test and those who passed, excluding the region and the education levels. For more information, see Table 3. The mean age of the remaining 829 respondents was 64 years old. Most of the respondents were married (89.85%) and had an education level of Middle school or below (83.82%). More than half were female (66.74%) and came from urban (55.37%). In addition, the mean duration of diabetes was about 8 years, and 36.42% of patients had complications.
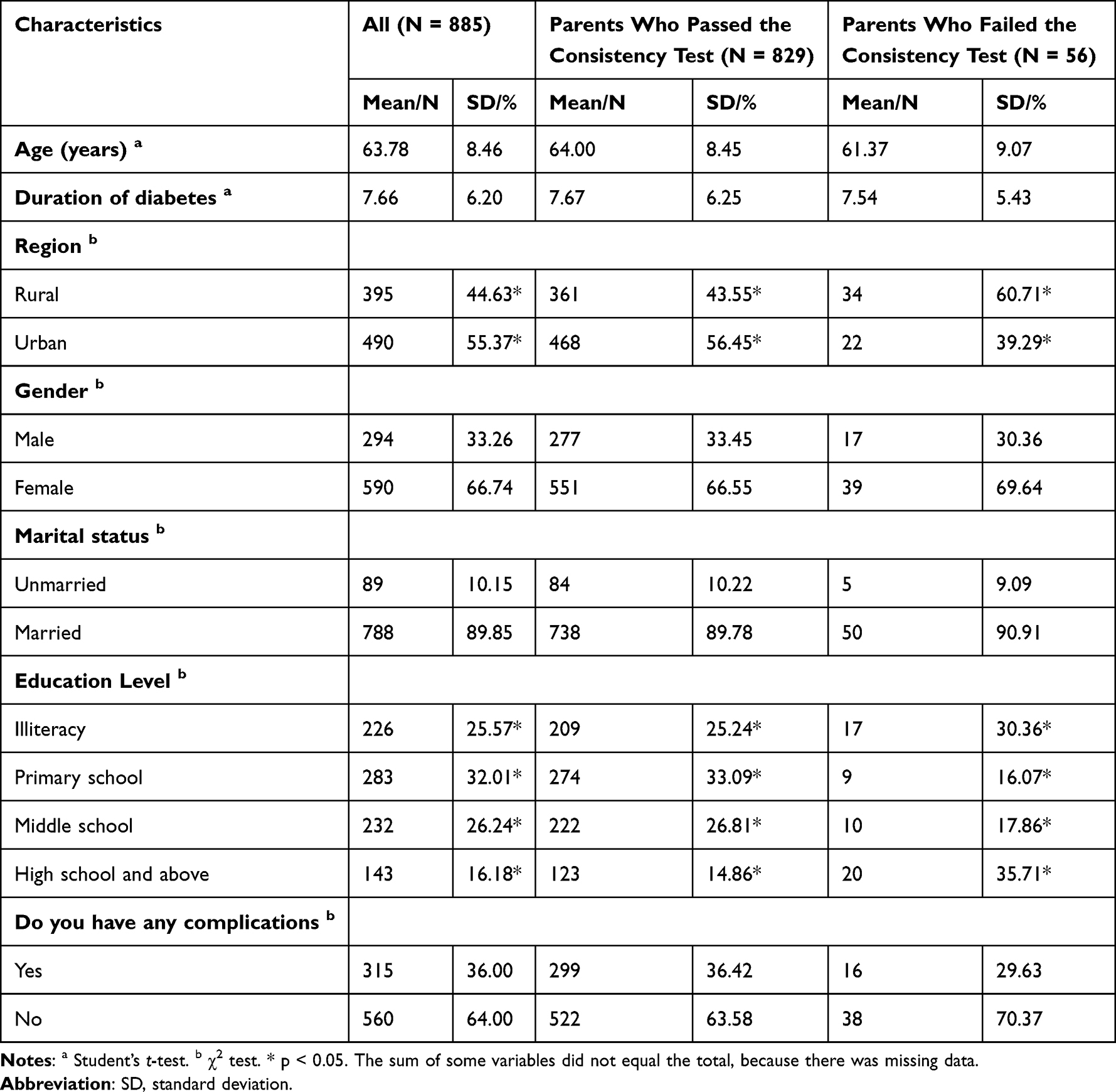 |
Table 3 Self-Reported Sociodemographic Characteristics and Clinical Characteristics |
DCE Main Effect results
Clogit was used for sensitivity analysis. There were also no significant differences in preferences between the full sample and the respondents who passed the consistency test (More details please see Supplemental Tables 1 and 2). However, considering adequate sample size, the DCE results were based on the parents who passed the consistency test. According to the log likelihood, Akaike information criterion (AIC) and Bayesian information (BIC) value,35,37 the MXL model was more appropriate than Clogit and the MXL estimates are reported in Table 4.
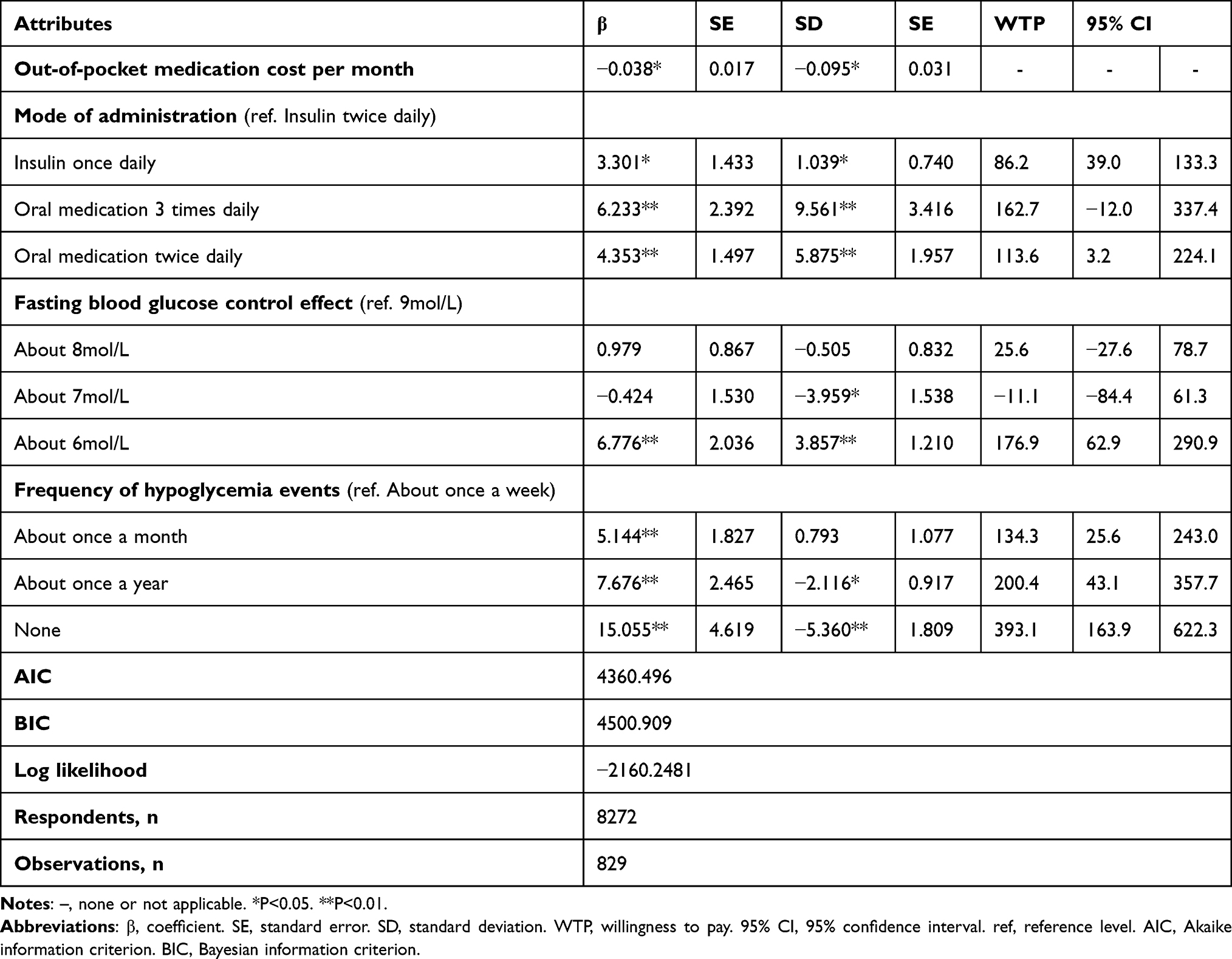 |
Table 4 Mixed Logit Model Results (N = 829) |
MXL results show that all attributes we selected were statistically significant. Patients with T2DM strongly prefered not to have hypoglycemia events compared with having hypoglycemia events about once a week (β=15.055, P<0.01). Patients also expressed a preference to control fasting blood glucose effect to about 6 mol/L compared with to about 9mol/L (β=6.776, P<0.01), as well as oral medication 3 times daily over insulin twice daily (β=6.233, P<0.01). The negative coefficient of the medication costs per month attribute indicated that a cheaper medication option would be preferred. As presented in Table 4, the statistically significant SD of some attributes indicated that there was preference heterogeneity among patients with T2DM.
Willingness to Pay
The willingness to pay estimates for the analysis sample (N = 829) are reported in Table 4. We found an obvious preference among respondents regarding the frequency of hypoglycemia events, patients with T2DM are willing to, respectively, pay CNY 393.10 and 258.80 (this is calculated by 393.10–134.30) per month for not having hypoglycemia events rather than having hypoglycemia events about once a week and once a month. Compared to controlling fasting blood glucose level to 9 mol/L, patients with T2DM were willing to pay CNY 176.90 to improve the normal level (about 6 mol/L). If the mode of administration was changed from insulin twice daily to oral medication 2 times daily, patients were willing to pay CNY 113.60 per month.
Subgroup Analysis
In subgroup analyses (by gender, age, education, region, duration of diabetes and complications), variation in ranking of attributes was observed, but frequency of hypoglycemia events was the most important factor in most subgroups. Complication subgroup results were not significantly different from the overall analysis sample. Young, rural and male patients have consistent preferences and they pay more attention to the mode of administration. Patients with higher educational levels and with longer diagnosis time consider fasting blood glucose control effect more important. For more details, please see Supplemental Table 3.
Discussion
This study used DCE methodology to investigate four key factors in determining patients’ preferences for T2DM medications in China. Among all attributes, the frequency of hypoglycemia events had the largest effect on medication choice. We found that patients with T2DM focus on reducing the frequency of hypoglycemia events. This result was consistent with a previous study conducted in the UK.16 What is more, the finding that patients were willing to pay more on average for medications associated with a lower frequency of hypoglycemia events means that they trade costs and benefits of medications. Hypoglycemia is a serious complication that can lead to physical discomfort such as dizziness, convulsions and even life-threatening in severe cases.38 Risk factors for hypoglycemia include age, use of multiple medications and associated comorbidity.1 The patients in this survey are at high risk of hypoglycemia, most of them have been educated about hypoglycemia during medications, especially those treated with insulin, they are aware of the dangers of hypoglycemia. Therefore, we suggest that doctors should set individual blood glucose targets and avoid strict glycaemic control to prevent hypoglycemia. At the same time, patients should be told not to fear excessively and improve their self-management ability.
Whether the blood glucose level can be effectively controlled is the main factor affecting the medication choice of patients. A previous study conducted in the US indicated that participants valued reductions in A1c levels and were willing to pay more for it.39 Our study also found that fasting blood glucose control effect remains an important factor for medication choice among patients with T2DM. There were two levels of this attribute (control fasting blood glucose effect to about 8 mol/L and 7 mol/L) that were not statistically significant, and the possible reason was that the patients have low awareness of blood sugar control, and they may not even know what a normal glycaemic level is.40
Out-of-pocket costs were relatively less important than the frequency of hypoglycemia events and the blood glucose level for patients in their medication choice. However, several previously published studies demonstrated that cost had the greatest impact on choice.41 This may be because the cost offered in those studies was difficult to affordable to patients ($25, $200). In addition, the attributes and levels set in the previous study are different from those in this study and cannot be directly compared. According to the negative coefficient of the cost attribute, we can know that patients preferred to accept cheaper drugs. This finding might be because that the mean age of respondents was 64 years old who were beyond the working age, many of whom had no financial resources and lacked the ability to pay. Meanwhile, Chinese government is trying to relieve the financial burden of patients’ medications. The 2019 government work report clearly pointed out that outpatient drugs for diabetes can be included in the medical insurance reimbursement, which can be reimbursed by more than 50%. We believe that patients’ needs for low prices will be gradually satisfied.
However, patients with T2DM in our study were less concerned about the mode of administration. That is probably because the average duration of diabetes with T2DM was 8 years, patients had formed medication habits. For medication frequency, patients prefered having oral medication 3 times daily over twice daily, this finding deserved our attention. But this may have something to do with the local three-meal daily diet, which makes it easier for patients to remember when they took their medication. Patients prefer to take oral medicine rather than insulin because they generally believe that insulin injection is troublesome and prone to addiction.42 This fear of insulin injection will lead to inadequate glycaemic administration, progression of complications of diabetes and suboptimal clinical outcomes.43 In the medication of diabetes, clinical physicians should strengthen communication with patients, timely detect patients’ wrong cognition of insulin injection and give intervention to improve their medication adherence.
Patients’ preference for medications can directly reflect patient needs and subjective feelings. In the process of T2DM diagnosis and treatment, clinical doctors could consider evidences on patients’ preference heterogeneity for medications and make tailored treatment plans, which will improve medication adherence and doctor–patient relationship. Although many clinical guidelines give recommendations on the selection of glucose-lowering drugs for different patients, there is a lack of information on patients’ preference for medications. It is recommended that clinical guidelines should be formulated with more integration of clinical efficacy and patient preferences, so as to better realize patient-centered healthcare services and effectively improve the health outcomes of patients with T2DM.
There are some limitations in our study. First, the relative importance of attributes can only be explained in the scope of attributes and levels used in this study, which is not promotional for other literatures even though the same study theme. Second, the sample size calculation approach used in this study is relatively simple. The results may not be strictly accurate or reliable. Future DCE research should use sophisticated methods to obtain a more accurate sample size. Third, although our study provided some important conclusions on the stated behavior of patients with T2DM, the sample of this study may not represent the patients with T2DM in other provinces of China and other countries, which potentially limited the generalizability of the results. Finally, the external validity of the study could not be tested. Stated preferences may not be consistent with actual choices. For example, patients usually consider the opinions of family members when they make medication choices, rather than making their own trade-offs. However, we are also trying to narrow the gap between the hypothetical scenario and the real world by double-checking attributes and levels.
Conclusion
This DCE study provides evidence on patients’ preference for medications. The frequency of hypoglycemia events was the most important attribute that affect patients’ medication choices. A medication with controlling fasting blood glucose to normal level would be more preferred, while out-of-pocket medication cost per month and mode of administration had little impact on patients’ decisions. Doctors should understand patients’ thought and design individualized medication plans, it will effectively improve patients’ adherence and clinical outcomes. In addition, patients should be encouraged to participate in the process of diabetes prevention and control program.
Abbreviations
WTP, willingness to pay; T2DM, type 2 diabetes mellitus; DCE, discrete choice experiment; Clogit, conditional logit model; MXL, mixed logit model; SP, Stated Preference; RP, Revealed Preference; ISPOR, International Society for Pharmacoeconomics and Outcomes Research; AIC, Akaike information criterion; BIC, Bayesian information.
Data Sharing Statement
The dataset can be available through the corresponding author on reasonable request.
Ethics
All respondents provided written informed consent ahead of enrolment and all responses were anonymous. This study was approved by the ethics committee of the School of Healthcare Management, Shandong University, China (ID: ECSHCMSDU20170401). The study complied with the guidelines outlined in the Declaration of Helsinki.
Acknowledgments
The authors sincerely thank all the patients who took part in the study. We are also grateful to the research staff who conducted and supported the project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research work was funded by the Natural Science Foundation of Shandong Province of China (ZR2016GQ02) and the National Key R&D Program of China (2020YFC2006505).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chinese Diabetes Society [homepage on the Internet]. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition). Available from: http://rs.yiigle.com/CN115399202004/1315489.htm.
2. International Diabetes Federation [homepage on the Internet]. IDF Diabetes Atlas, 10th edn. Available from: https://www.diabetesatlas.org.
3. Wang L, Peng W, Zhao Z, et al. Prevalence and Treatment of Diabetes in China, 2013-2018. JAMA. 2021;326(24):2498–2506. doi:10.1001/jama.2021.22208
4. Sundaram M, Kavookjian J, Patrick JH. Health-related quality of life and quality of life in type 2 diabetes. Patient. 2009;2(2):121–133. doi:10.2165/01312067-200902020-00008
5. Shurrab NT, Arafa E-SA. Metformin: a review of its therapeutic efficacy and adverse effects. Obesity Med. 2020;17:100186. doi:10.1016/j.obmed.2020.100186
6. Home P, Riddle M, Cefalu WT. et al. Insulin therapy in people with type 2 diabetes: opportunities and challenges? Diabetes Care. 2014;37(6):1499–1508. doi:10.2337/dc13-2743
7. Mueck KM, Leal IM, Wan CC, et al. Shared decision-making during surgical consultation for gallstones at a safety-net hospital. Surgery. 2018;163(4):680–686. doi:10.1016/j.surg.2017.10.043. Epub 2017 Dec 6
8. Fraenkel L, Nowell WB, Michel G, Wiedmeyer C. Preference phenotypes to facilitate shared decision-making in rheumatoid arthritis. Ann Rheum Dis. 2018;77(5):678–683. doi:10.1136/annrheumdis-2017-212407
9. Vercellini P, Frattaruolo MP, Rosati R, et al. Medical treatment or surgery for colorectal endometriosis? Results of a shared decision-making approach. Human Reproduction. 2018;33(2):202–211. doi:10.1093/humrep/dex364
10. Bridges J, Onukwugha E, Johnson F, Hauber A. Patient preference methods—a patient centered evaluation paradigm. ISPOR Connections. 2007;13(6):4–7.
11. Bridges JF, Hauber AB, Marshall D, et al. Conjoint analysis applications in health—a checklist: a report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health. 2011;14(4):403–413. doi:10.1016/j.jval.2010.11.013
12. Rakotonarivo OS, Schaafsma M, Hockley N. A systematic review of the reliability and validity of discrete choice experiments in valuing non-market environmental goods. J Environ Manage. 2016;183:98–109. doi:10.1016/j.jenvman.2016.08.032
13. Soekhai V, de Bekker-Grob EW, Ellis AR, Vass CM. Discrete choice experiments in health economics: past, present and future. Pharmacoeconomics. 2019;37(2):201–226. doi:10.1007/s40273-018-0734-2
14. Janssen EM, Hauber AB, Bridges JFP. Conducting a Discrete-Choice Experiment Study Following Recommendations for Good Research Practices: an Application for Eliciting Patient Preferences for Diabetes Treatments. Value Health. 2018;21(1):59–68. doi:10.1016/j.jval.2017.07.001
15. Igarashi A, Bekker Hansen B, Langer J, et al. Preference for Oral and Injectable GLP-1 RA Therapy Profiles in Japanese Patients with Type 2 Diabetes: a Discrete Choice Experiment. Adv Ther. 2021;38(1):721–738. doi:10.1007/s12325-020-01561-1
16. Gelhorn HL, Stringer SM, Brooks A, et al. Preferences for medication attributes among patients with type 2 diabetes mellitus in the UK. Diabetes Obes Metab. 2013;15(9):802–809. doi:10.1111/dom.12091
17. Muhlbacher A, Bethge S. What matters in type 2 diabetes mellitus oral treatment? A discrete choice experiment to evaluate patient preferences. Eur J Health Econ. 2016;17(9):1125–1140. doi:10.1007/s10198-015-0750-5
18. Muhlbacher AC, Sadler A, Juhnke C. Personalized diabetes management: what do patients with diabetes mellitus prefer? A discrete choice experiment. Eur J Health Econ. 2021;22(3):425–443. doi:10.1007/s10198-021-01264-6
19. Wang X, Song K, Zhu P, Valentijn P, Huang Y, Birch S. How do type 2 diabetes patients value urban integrated primary care in China? Results of a discrete choice experiment. Int J Environ Res Public Health. 2020;17(1):117. doi:10.3390/ijerph17010117
20. Huang Y, Huang Q, Xu A, Lu M, Xi X. Patient preferences for diabetes treatment among people with type 2 diabetes mellitus in China: a discrete choice experiment. Front Public Health. 2021;2424. doi:10.3389/fpubh.2021.782964
21. de Bekker‐Grob EW, Ryan M, Gerard K. Discrete choice experiments in health economics: a review of the literature. Health Econ. 2012;21(2):145–172. doi:10.1007/s40273-014-0170-x
22. Vass C, Gray E, Payne K. Discrete choice experiments of pharmacy services: a systematic review. Int J Clin Pharm. 2016;38(3):620–630. doi:10.1007/s11096-015-0221-1
23. Hauber AB, González JM, Groothuis-Oudshoorn CG, et al. Statistical methods for the analysis of discrete choice experiments: a report of the ISPOR conjoint analysis good research practices task force. Value Health. 2016;19(4):300–315. doi:10.1016/j.jval.2016.05.002
24. Coast J, Al‐Janabi H, Sutton EJ, et al. Using qualitative methods for attribute development for discrete choice experiments: issues and recommendations. Health Econ. 2012;21(6):730–741. doi:10.1002/hec.1739
25. Mansfield C, Sikirica MV, Pugh A, et al. Patient Preferences for Attributes of Type 2 Diabetes Mellitus Medications in Germany and Spain: an Online Discrete-Choice Experiment Survey. Diabetes Ther. 2017;8(6):1365–1378. doi:10.1007/s13300-017-0326-8
26. Guimaraes C, Marra CA, Gill S, et al. A discrete choice experiment evaluation of patients’ preferences for different risk, benefit, and delivery attributes of insulin therapy for diabetes management. Patient Prefer Adherence. 2010;4:433–440. doi:10.2147/PPA.S14217
27. Jendle J, Torffvit O, Ridderstrale M, Ericsson A, Nilsen B, Bogelund M. Willingness to pay for diabetes drug therapy in type 2 diabetes patients: based on LEAD clinical programme results. J Med Econ. 2012;15(Suppl 2):1–5. doi:10.3111/13696998.2012.703633
28. Hauber AB, Mohamed AF, Johnson FR, Falvey H. Treatment preferences and medication adherence of people with Type 2 diabetes using oral glucose-lowering agents. Diabet Med. 2009;26(4):416–424. doi:10.1111/j.1464-5491.2009.02696.x
29. Aristides M, Weston AR, FitzGerald P, Le Reun C, Maniadakis N. Patient preference and willingness-to-pay for Humalog Mix25 relative to Humulin 30/70: a multicountry application of a discrete choice experiment. Value Health. 2004;7(4):442–454. doi:10.1111/j.1524-4733.2004.74007.x
30. Hauber AB, Han S, Yang JC, et al. Effect of pill burden on dosing preferences, willingness to pay, and likely adherence among patients with type 2 diabetes. Patient Prefer Adherence. 2013;7:937–949. doi:10.2147/PPA.S43465
31. Rydén A, Chen S, Flood E, Romero B, Grandy S. Discrete choice experiment attribute selection using a multinational interview study: treatment features important to patients with type 2 diabetes mellitus. Patient. 2017;10(4):475–487. doi:10.1007/s40271-017-0225-0
32. Morillas C, Feliciano R, Catalina PF, et al. Patients’ and physicians’ preferences for type 2 diabetes mellitus treatments in Spain and Portugal: a discrete choice experiment. Patient Prefer Adherence. 2015;9:1443–1458. doi:10.2147/PPA.S88022
33. Johnson FR, Lancsar E, Marshall D, et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR conjoint analysis experimental design good research practices task force. Value Health. 2013;16(1):3–13. doi:10.1016/j.jval.2012.08.2223
34. Green PE, Srinivasan V. Conjoint analysis in consumer research: issues and outlook. J Consumer Res. 1978;5(2):103–123. doi:10.1086/208721
35. Lancsar E, Louviere J. Conducting discrete choice experiments to inform healthcare decision making: a user's guide. Pharmacoeconomics. 2008;26(8):661-677. doi:10.2165/00019053-200826080-00004
36. Orme B. Sample size issues for conjoint analysis studies. Sequim. 1998;1:215.
37. Hensher DA. Accounting for scale heterogeneity within and between pooled data sources. Transportation Res Part A. 2012;46(3):480–486. doi:10.1016/j.tra.2011.11.007
38. Tourkmani AM, Alharbi TJ, Rsheed AMB, et al. Hypoglycemia in Type 2 Diabetes Mellitus patients: a review article. Diabetes Metab Syndrome. 2018;12(5):791–794. doi:10.1016/j.dsx.2018.04.004
39. Janssen EM, Longo DR, Bardsley JK, Bridges JF. Education and patient preferences for treating type 2 diabetes: a stratified discrete-choice experiment. Patient Prefer Adherence. 2017;11:1729–1736. doi:10.2147/PPA.S139471
40. Tang J, Gao L. Illness perceptions among patients with type 2 diabetes mellitus: a cross-sectional study. Int J Nurs Pract. 2020;26(5):e12801. doi:10.1111/ijn.12801
41. Hauber AB, Tunceli K, Yang JC, et al. A survey of patient preferences for oral antihyperglycemic therapy in patients with type 2 diabetes mellitus. Diabetes Ther. 2015;6(1):75–84. doi:10.1007/s13300-015-0094-2
42. Mirahmadizadeh A, Delam H, Seif M, Banihashemi SA, Tabatabaee H. Factors affecting insulin compliance in patients with type 2 diabetes in South Iran, 2017: we are faced with insulin phobia. Iran J Med Sci. 2019;44(3):204.
43. Fu AZ, Qiu Y, Radican L. Impact of fear of insulin or fear of injection on treatment outcomes of patients with diabetes. Curr Med Res Opin. 2009;25(6):1413–1420. doi:10.1185/03007990902905724
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.