Back to Journals » Risk Management and Healthcare Policy » Volume 16
Preferences on Policy Options for Ensuring the Financial Sustainability of Healthcare Services in the Kingdom of Saudi Arabia
Authors Huraysi NA, Kattan WM ![]() , Alqurashi MA, Fadel BA, Al-Hanawi MK
, Alqurashi MA, Fadel BA, Al-Hanawi MK ![]()
Received 29 March 2023
Accepted for publication 3 June 2023
Published 12 June 2023 Volume 2023:16 Pages 1033—1047
DOI https://doi.org/10.2147/RMHP.S414823
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Najwa Ali Huraysi,1,2 Waleed M Kattan,1 Mohamed A Alqurashi,1 Bodour Ayman Fadel,1 Mohammed Khaled Al-Hanawi1,3
1Department of Health Services and Hospital Administration, Faculty of Economics and Administration, King Abdulaziz University, Jeddah, Saudi Arabia; 2Human Resources Planning Department, King Abdulaziz Hospital, Makkah, Saudi Arabia; 3Health Economics Research Group, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Mohammed Khaled Al-Hanawi, Tel +966 556522222, Email [email protected]
Background: Escalating global health expenditures pose a threat to healthcare financing sustainability, requiring the exploration of alternative financing policies and resource allocation strategies to curb their adverse effects. The aim of this study was to gather insight into the preferences of healthcare workers, including physicians, nurses, allied healthcare professionals, and healthcare administrators, as well as academics in the field of healthcare management and health sciences in Saudi universities, regarding policy options that can secure the financial sustainability of healthcare services in Saudi Arabia.
Methods: A cross-sectional research design was employed, and data were collected through an online self-administered survey from August 2022 to December 2022 in Saudi Arabia. The survey garnered responses from 513 participants hailing from all 13 administrative regions in Saudi Arabia. Analyses were performed using non-parametric statistical tests, specifically the two-sample Mann–Whitney U-test and Kruskal–Wallis test, to determine the statistical significance of differences in the policy ranking and policy feasibility options.
Results: The study findings reveal a consensus among stakeholders on the most and least preferred policies. All stakeholders expressed opposition to financing healthcare by diverting resources from defence, social protection, and education, while they favoured policies that entail imposing penalties on health-related issues such as waste management and pollution. Nevertheless, variations among stakeholders were evident in regard to the rankings for specific policies, particularly between healthcare workers and academics. Moreover, the results highlight that tax-based policies are the most feasible approach to generating healthcare funds, despite ranking lower in terms of preferred policies.
Conclusion: This study provides a framework for understanding stakeholder preferences on healthcare financing sustainability by ranking 26 policy options according to stakeholder groups. The appropriate mixture of financing mechanisms should be informed by evidence-based and data-driven approaches that consider relevant stakeholder preferences.
Keywords: healthcare financing, healthcare policy, preferences, Saudi Arabia, sustainability
Introduction
Access to quality healthcare is an essential human right and is closely linked to an individual’s economic progress and productivity.1 The United Nations Sustainable Development Goals (SDGs) prioritize universal health coverage (UHC) as a key policy objective. This is particularly relevant to SDG 3.8, which emphasizes the importance of improving access to high-quality healthcare services and safeguarding individuals from catastrophic healthcare expenses.2,3 Universal health coverage is an ambitious goal that aims to enhance the availability, affordability, and quality of healthcare services.3 In recent years, there has been widespread international support for UHC, especially since publication of the 2010 World Health Report. Universal health coverage, characterized by population coverage, service coverage, and cost-sharing, is crucial in tackling disparities in healthcare provision and promoting equity.4
Despite global efforts to attain UHC, the persistent rise in healthcare spending poses a significant challenge. In some cases, healthcare expenditures surpass 10% of the country’s gross domestic product.5 The growing demands for healthcare due to aging populations, a surge in chronic diseases, increased patient demands, and the high cost of new medical technologies, are common to all societies.6–9 Sustainability has become a critical concern in healthcare in the 21st-century, it referring to the lasting capacity of healthcare systems to maintain their functions and viability over time.10 Financial sustainability in healthcare involves securing and managing sufficient financial resources to cover operational costs and provide high-quality healthcare services consistently in the long term.11 The concern of such sustainability has prompted apprehension about funding options such as resource reallocation, fundraising, or service rationing.12 As such, policymakers need to react appropriately to enable countries to meet their UHC targets through either generating more revenue or reallocating resources from other sectors to finance the soaring healthcare budgets.13,14
The successful implementation of UHC and the effectiveness of selected policy options require broad stakeholder involvement and support; therefore, the policy preferences of key stakeholders in health financing must be examined when setting health priorities. Consequently, understanding whether stakeholders have unified or different preferences on how to finance healthcare remains key to the success of healthcare financing reforms. This issue has received inadequate attention in the healthcare financing literature to date and has not yet been investigated in the context of the Arabian Gulf region. Exploring such preferences is particularly crucial for the Kingdom of Saudi Arabia (KSA) where the healthcare system accounts for a significant portion of the national budget.
The KSA is a high-income country in the Arabian Gulf region spanning an area of approximately 2,150,000 km2. As one of the largest producers and exporters of oil globally, the revenue generated is utilized to finance various expenditures, including healthcare.7,15 Similar to many countries in the region, the KSA provides healthcare in public health facilities free of charge to its citizen, which leads to many inherent issues such as overuse of services and increasing numbers of unnecessary referrals.16–18 The government has prioritized healthcare in the country, with the Ministry of Health (MOH) operating approximately 60% of hospitals and primary healthcare centres. The healthcare infrastructure in Saudi Arabia was relatively weak and resource-scarce prior to 1925; however, significant improvements have been made in recent decades in terms of the quality and quantity of healthcare services.7 Modernization of the hospital infrastructure has resulted in improved health statistics such as an increase in life expectancy from 66 to 74.9 years between 1983 and 2017, and a decline in the infant mortality rate from 52 to 6.3 per 1000 live births.19
However, the KSA’s healthcare system confronts challenges stemming from demographic changes, an aging population, rising costs, and evolving disease patterns, which have led to increased demand and healthcare expenditure.7 Moreover, cultural shifts caused by rapid economic growth and globalization have contributed to an elevated disease burden, especially non-communicable diseases (NCDs) caused by unhealthy lifestyles and behaviours. The escalating healthcare expenditure, combined with an unpredictable oil market, is exerting mounting pressure on the public sector healthcare system in the KSA, raising doubts about its sustainability in the long term.20 As the healthcare system in the KSA accounts for a significant portion of the national budget, exploring alternative financing options has now become necessary in ensuring the financial sustainability of healthcare services in the country.
Numerous studies have examined the increasing healthcare expenses over recent decades, but their focus has primarily been on the effects of out-of-pocket expenses on health and health inequalities,21–24 and there is a lack of studies directly exploring various policy options for healthcare funding in the related literature. Additionally, the sustainability of existing funding modalities for healthcare remains an under-researched area. It is evident that countries such as the KSA cannot sustain their healthcare expenses due to an overreliance on revenues from natural resources for healthcare financing and the provision of free-of-charge healthcare services. This highlights the unique context of the KSA, preventing the application of related results from studies on the topic in the European context.25 Therefore, there is a need to investigate alternative policy options and examine the most acceptable way to raise funds by soliciting stakeholder preferences on potential funding methods. Moreover, since the KSA has a similar culture and religion to other countries in the Arabian Gulf region, these results could be applicable to the entire region.
In this study, an online cross-sectional survey was conducted to determine the policy preferences of healthcare workers (including physicians, nurses, allied healthcare professionals, and healthcare administrators) and academics in the field of healthcare management and health sciences in Saudi universities towards ensuring the financial sustainability of healthcare services in the KSA. Based on the survey responses, we ranked 26 policy options according to their overall sum score mean, revealing the levels of stakeholder preference for these policies. This study’s main significance lies in the ability to elicit preferences from stakeholder groups, which can help reduce the gap between preferences and actual policy practice. Therefore, it is essential to examine stakeholder policy options preferences to ensure implementing the most appropriate mix of policies to achieve the goal of ensuring the healthcare system’s financial sustainability.
Materials and Methods
Survey
This study used data with permission from a cross-sectional online validated survey25 that was conducted in the KSA from August 2022 to December 2022. The survey contained four sections. The first section included a set of questions related to the participants’ socio-demographic characteristics. The second section consisted of questions related to the participants’ levels of agreement or disagreement with a series of statements related to the policy options using a five-point Likert scale. On this scale, response options ranged from 1 to 5, where 1 indicated strongly disagree and 5 indicated strongly agree. In contrast to Tordrup et al,25 who presented 21 policy options, this study expanded upon their work by introducing an additional 5 options specifically tailored to align with the context of the Saudi healthcare system. All 26 policy options were ranked according to the mean of the overall sum score; policies with a higher sum score were more preferred than those with a lower sum score. The policy options included increasing the revenue base for healthcare through raising taxes on income, reducing the cost of provided services through decreasing the purchase of expensive technology, implementing market-based mechanisms such as the privatization of some healthcare components, reallocating resources from other areas of public spending, subsidizing healthy living, and supporting preventive health services. In the third section, the participants were asked to rank the 26 policy options and select the top five most feasible options. The fourth section asked the respondents if they have any suggestions for future funding of healthcare services in KSA.
The reliability of the study tool was assessed using Cronbach’s alpha coefficient. Nunally & Bernstein26 consider a Cronbach’s alpha value of 0.7 or higher to be an indicator of adequate reliability; we found a Cronbach’s alpha value of 0.812 for our survey instrument, indicating good internal reliability. Further, the structure of the questionnaire was validated by calculating the correlation between the coefficient of the axis items and the total degree for all items of this axis using the Pearson correlation coefficient (r). All correlation coefficients were statistically significant at the level of P<0.01, ranging from r = 0.323 to r = 0.573.
Sample
The sample comprised 513 individuals in senior key healthcare industry roles, including physicians, nurses, other allied healthcare professionals, healthcare administrators, and academics in the fields of healthcare management and health sciences in Saudi universities. Although other stakeholders, including individuals from professional associations, political leadership, and community members, are equally significant for policymaking and implementation, this study has focused on the senior key healthcare industry stakeholders due to time and access constraints. Assessing the preferences of these stakeholders was justified from the fact that individuals in these roles will likely have a deeper and more comprehensive understanding of the current situation relating to the healthcare system in the KSA. The sampling frame was obtained from the databases of Saudi universities and the healthcare sector. Although data on the overall population of healthcare workers in Saudi Arabia is accessible, specific information regarding academicians is lacking. As a result, the study aimed to gather responses from a wide range of individuals without setting a predefined size of the target population in the country. The survey was administered through a snowball sampling technique, in which initial email and WhatsApp messages were sent to few targeted respondents who then forward the message to others related to the target group. Following the distribution of the survey information to all potential participants, a total of 556 individuals responded to the questionnaire. After excluding 43 respondents who did not respond to all questions and/or excluded responding to a variable of interest to this study, the final sample included in the analysis consisted of 513 participants.
Statistical Analysis
Demographic variables were summarized as frequencies and percentages according to the different professions. The distribution of Likert-item responses between the subgroups of interest was assessed using the non-parametric two-sample Mann–Whitney U-test and Kruskal–Wallis test as appropriate. Parametric statistics rely on assumptions regarding the distribution of the population and are suitable for data that follows a normal distribution. On the other hand, non-parametric statistics do not depend on such assumptions and are applicable to any continuous data, using ranks of data values instead.27 Given the characteristics of the data, the study opted for non-parametric alternatives, specifically the Mann–Whitney U-test and Kruskal–Wallis test, as they are better suited for analysis. The U-test was used to evaluate the differences in opinion and preferences between two groups, specifically by comparing the academics and healthcare workers. The Kruskal–Wallis test was used to evaluate the differences in opinion among multiple groups, specifically by comparing the academics, physicians, nurses, allied healthcare professionals, and health administrators. This enabled establishing any differences in the practical and theoretical viewpoints among various stakeholders and experts. All statistical analyses were conducted using SPSS version 24.
Ethical Considerations
All procedures performed in this study involving human participants complied with the institutional and/or national research committee ethical standards and the 1964 Helsinki Declaration, and subsequent amendments, or equivalent ethical standards. The study was designed and conducted in accordance with the ethical principles established by King Abdulaziz University. In addition to King Abdulaziz University’s ethical approval, the study has also received ethical approval from the MOH in the KSA (Institutional Review Board number: H-02-K-076-0722-769). Online informed consent to participate was obtained from all respondents who participated in the study.
Results
Descriptive Statistics
Table 1 presents the sample characteristics from the 513 respondents. Out of the total participants, 275 (53.6%) were male. Approximately 42% of the respondents were in the age group of 30–39 years, whereas only 8.2% were in the age group of 50 years and older. More than half of the respondents had a university degree and 28.7% had achieved postgraduate degree. The government sector represented 82.1% of the total sample respondents and over one-third of the respondents (37.3%) had professional experience of more than 10 years. Among all survey respondents, 24.2% reported a profession as academic staff and the remaining 75.8% of the sample was split between the several healthcare-industry worker groups.
 |
Table 1 Description of the Study Population Characteristics (n = 513) |
Preferences on Policy Options
Table 2 presents the ranking of policy options for ensuring the financial sustainability of healthcare services in the KSA. All 26 policy options were ranked according to their overall sum score mean by respondents. Policies with a higher sum score are those that were more preferred by the respondents than those with a lower sum score. The top 10 preferred policies included imposing a tax on the environmental phenomena that cause the spread of diseases; imposing fees on waste management to penalize entities that violate waste disposal policies to reduce pollution; rewards for eating healthy food both at home and in the workplace; using traffic regulations violation revenue from fines to finance healthcare services; developing a policy forcing contracted medical technology companies to take back their devices at the end of their lifespan and replace them with newer devices at a lower cost to encourage the circular economy; set a policy for deducting an annual percentage from health insurance companies in case the beneficiaries are not benefitting from service to finance healthcare; limiting electives, through prioritizing access for those with chronic diseases and reducing less essential procedures such as cosmetic surgery; using part of the healthcare budget to subsidize gym subscriptions; increasing the role of private sector participation in the healthcare sector through expanding service provision and financing; and introducing additional excise taxes on tobacco products.
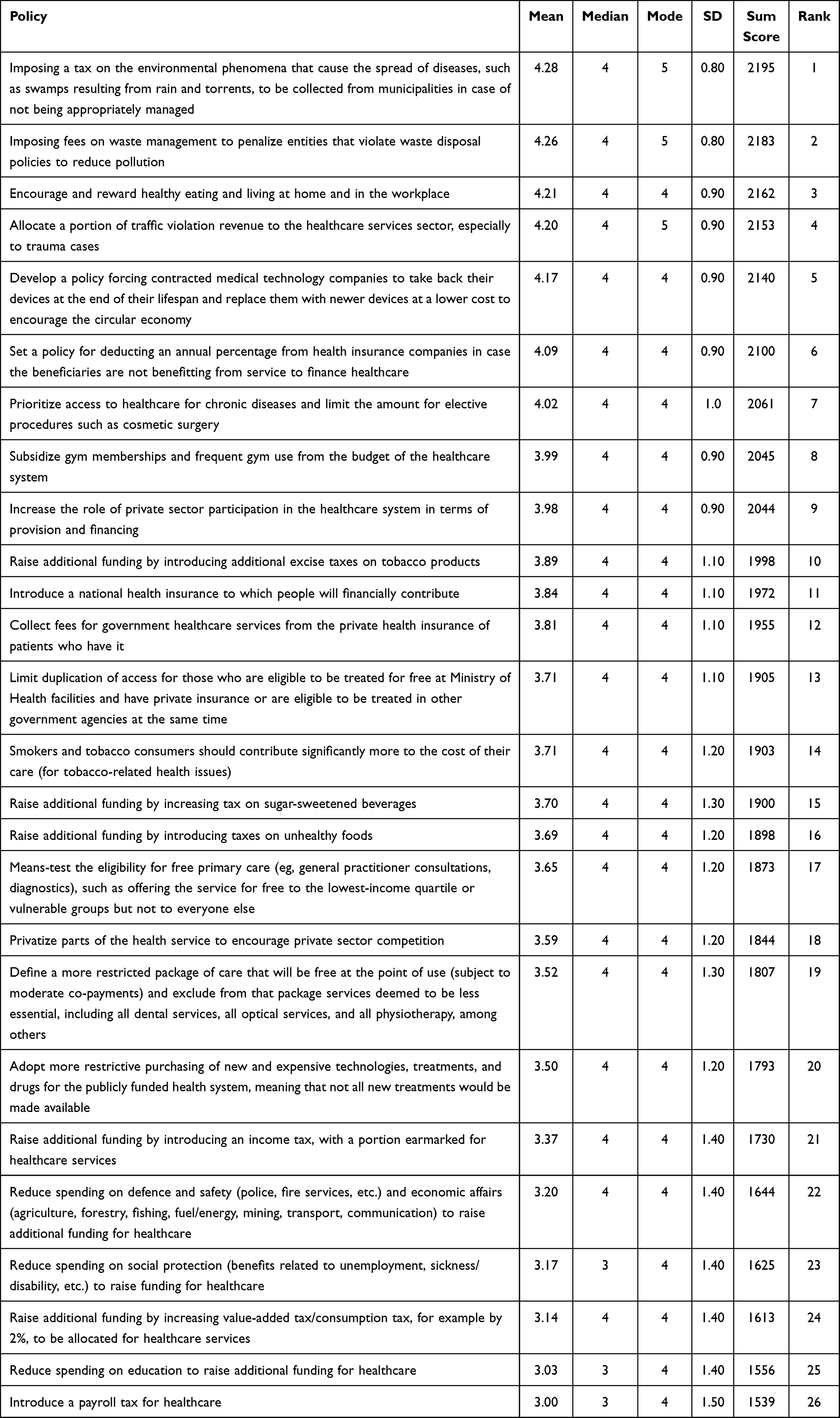 |
Table 2 Overall Ranking of Policy Options |
The bottom five policies listed in Table 2 reflect the options that were the least preferred by the respondents. These policies included financing healthcare by diverting resources from defence, social protection, and education; financing healthcare using increased value-added tax (VAT) income; and introducing a payroll tax to finance healthcare.
Divergence of Preferences on Policy Options
Table 3 presents the outcomes of the relative preferences of policy options among the academics, physicians, nurses, allied healthcare professionals, and healthcare administrators. There were significant differences in the preferences on all except four policy options among the five groups. The exceptions in which all stakeholder groups agreed were imposing a tax on the environmental phenomena that cause the spread of diseases, such as swamps resulting from rain and torrents, to be collected from municipalities in case of not being appropriately managed; imposing fees on waste management to penalize entities that violate waste disposal policies to reduce pollution; encourage and reward healthy eating and living at home and in the workplace; and develop a policy forcing contracted medical technology companies to take back their devices at the end of their lifespan and replace them with newer devices at a lower cost to encourage the circular economy. All of these policy options were ranked among the top five for all groups. Moreover, although there was a significant difference in the specific scores on policy options among all groups for the five lowest-scoring policy options, all groups ranked them as least preferred (between rank 22 and 26).
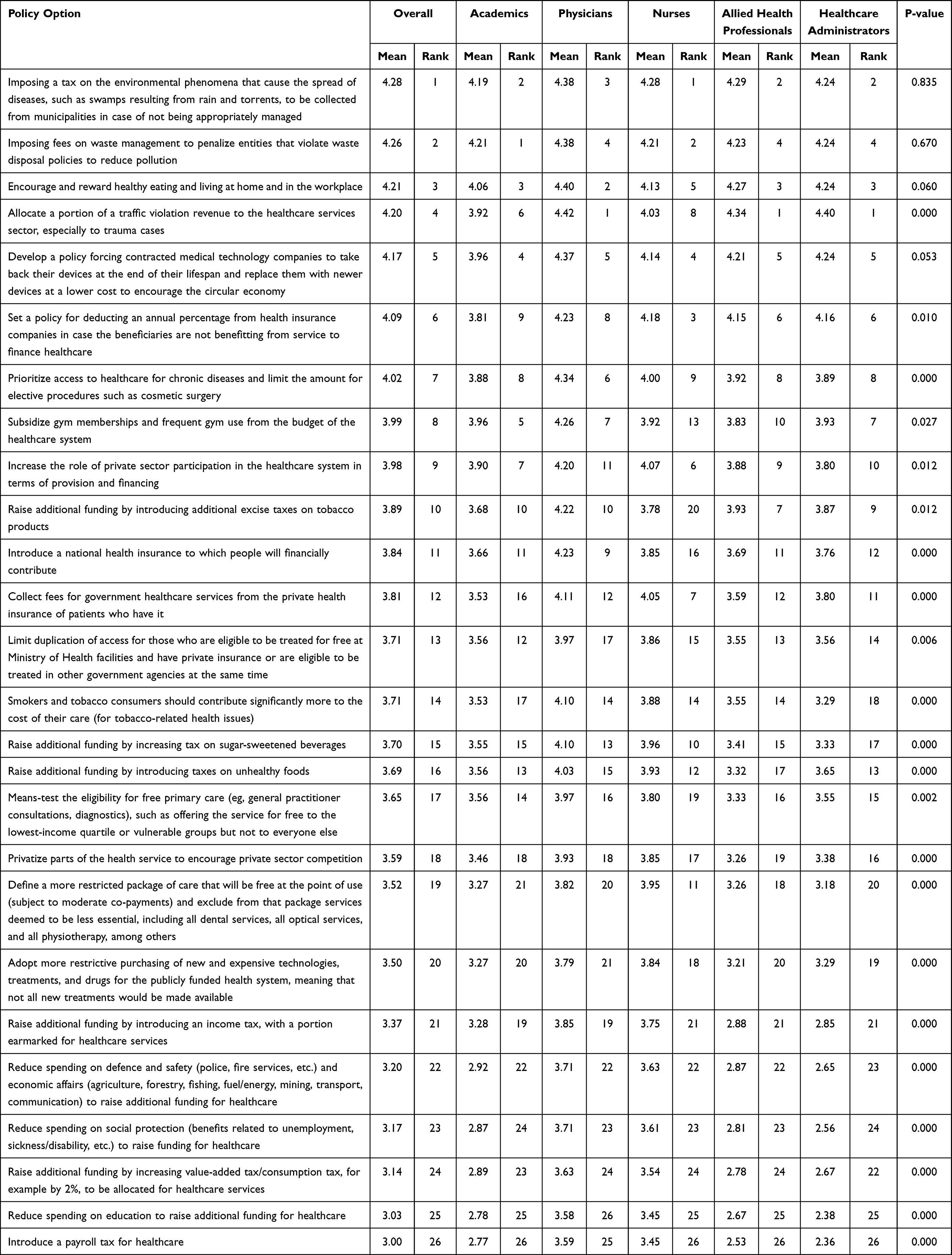 |
Table 3 Differences in Preferences on Policy Options Among Academics, Physicians, Nurses, Allied Healthcare Professionals, and Healthcare Administrators |
Table 4 presents the outcomes of the relative preferences of policy options between the academics and healthcare workers considered as a single, pooled group. The preferences for several policy options appeared to differ between the two groups. For example, the academics ranked limiting electives and priority for people with chronic illness as number 8, whereas the healthcare workers ranked the same policy as number 7 (P=0.022), meaning that healthcare workers prefer increasing resources from healthcare spending to chronic illnesses while reducing expenditures on less-essential electives such as cosmetic surgery more than the academic staff. Moreover, the academics ranked increasing the role of private sector participation in the healthcare system in terms of provision and financing as number 9, whereas healthcare workers ranked the same policy as number 8 (P=0.019), indicating that healthcare workers prefer encouraging the participation of the private sector in the provision and financing of healthcare services more than the academics. Additionally, the healthcare workers and academic staff also differed in terms of their viewpoints on the reduction in social spending to raise funding for healthcare (P˂.001). The academics ranked this option as number 24, whereas the healthcare workers ranked it slightly higher at number 23. Thus, while both groups are reluctant to reduce social spending to raise additional funding for healthcare, the academics are more reluctant to adopt this option relative to the healthcare workers.
 |
Table 4 Differences in Preferences on Policy Options Between Academics and Healthcare Workers |
Feasibility of Policy Options
Respondents were asked to select five policies and rank them according to what they perceived to be the most feasible package for implementation within the Saudi healthcare system. Table 5 presents the top five policy options ranked by the participants: increased tax on cigarettes; introducing an income tax, with a portion earmarked for healthcare services; the allocation of traffic violations penalty revenue to healthcare, particularly to trauma cases; increasing VAT/consumption tax, for example by 2%, to be allocated for healthcare services; and increasing tax on sugar-sweetened beverages.
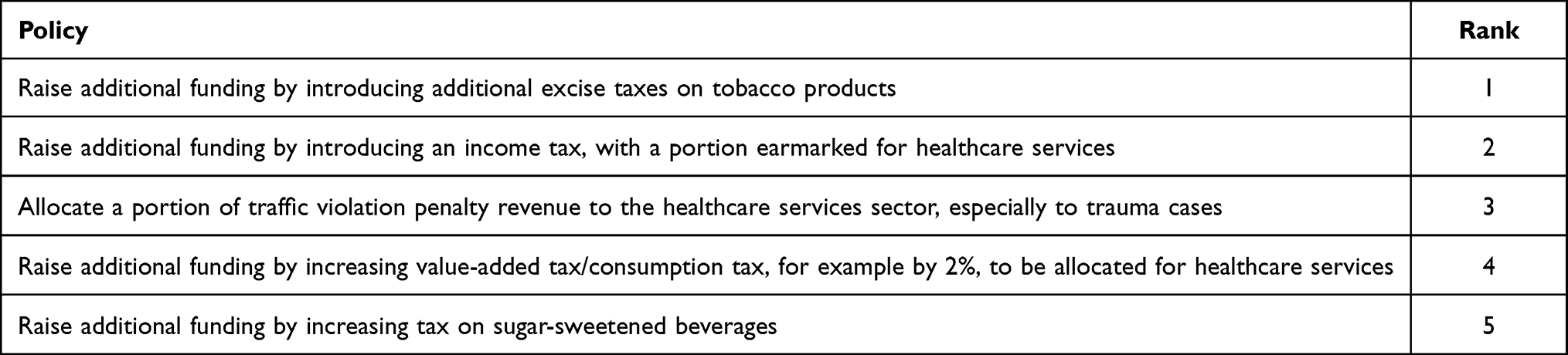 |
Table 5 Overall Ranking of Feasible Policy Options |
Discussion
This study conducted an online cross-sectional survey to elicit preferences on policy options for ensuring the financial sustainability of healthcare services in the KSA by soliciting views from healthcare workers (including physicians, nurses, allied healthcare professionals, and healthcare administrators) and academics in the fields of healthcare management and health sciences in Saudi universities. Using non-parametric two-sample Mann–Whitney U-test and Kruskal–Wallis test, the 26 policy options were ranked according to their overall sum score mean by respondents, revealing the levels of stakeholder preference for these policies. Apart from eliciting preferences from stakeholder groups that will be essential for policy implementation, this study presents the first attempt in the KSA to examine healthcare sustainability issues in line with funding options from a stakeholder perspective.
The findings of this study indicate that stakeholder preferences are influenced by ideological principles and the level of involvement with the healthcare system in the KSA. Across all stakeholder groups, the top five preferred policy options for ensuring financial sustainability of healthcare services were: implementing a tax on environmental factors that contribute to the spread of diseases, levying fees on waste management to penalize entities that violate waste disposal policies and reduce pollution, incentivizing healthy eating at home and in the workplace, utilizing revenue from traffic violation fines to fund healthcare services, and mandating medical technology companies to take back their devices at the end of their lifespan and replace them with newer, more affordable models to promote a circular economy. The convergence of stakeholder opinions on specific policies is consistent with previous research in stakeholder analysis.12,25
The preference for taxes on environmental phenomena and fees on waste management, in addition to generating revenue, is likely due to stakeholders’ efforts to reduce the overall burden of disease by addressing the root causes. These measures have the potential to both raise revenue and decrease the incidence of disease, which is appealing to healthcare workers and academics alike. Stakeholders also tend to favour policies that prioritize equity, fairness, and ethical considerations;4,12 as such, taxes and fees on environmental and waste management issues are viewed as attractive to all stakeholders. Furthermore, stakeholders are likely to support these options as they do not directly affect the public, but rather target companies and organizations that are deemed responsible for these issues and are therefore seen as justified in paying such taxes and fees.
The inclusion of rewards for healthy eating habits, both at home and in the workplace, among the top preferred policy options is not surprising, given the shift in disease epidemiology from predominantly communicable diseases to NCDs, as the largest lifestyle health problem currently facing the KSA.28 In the KSA, the rise of NCDs is attributed to unhealthy lifestyles and behaviours resulting from rapid economic growth and globalization.29 NCDs are responsible for approximately 41 million deaths per year, accounting for 71% of all deaths worldwide.30 In light of these statistics, it is understandable that the policy option to incentivize healthy behaviours received unanimous support from stakeholders who possess knowledge and experience in dealing with NCD cases. Such rewards can promote healthy lifestyles, which can in turn help reduce the prevalence of NCDs as the population ages and healthcare expenses continue to rise.
Given the strain on the healthcare system in the KSA, stakeholders are likely to support policies that increase funding for the sector and reduce healthcare expenses without compromising equity, access, or quality. This explains why all stakeholder groups rated the use of revenue from traffic regulations violation fines to finance healthcare services among their top five preferred policy options, which would generate additional revenue. At present, approximately $7 billion of medical costs and property is wasted annually in the KSA due to road accidents.31 Therefore, the proposed allocation of some resources from road traffic violation fines to healthcare could reduce the financial burden brought about by road accident casualties. Additionally, stakeholders highly value a policy that would compel medical technology companies to take back their devices at the end of their lifespan and replace them with newer devices at a lower cost, thus promoting the circular economy. Advancements in healthcare technology have contributed to rising healthcare costs,11,32 and since technology is continually improving, this consensus would significantly reduce healthcare expenses associated with technological advancement.
Similar to the findings of Tordrup et al,25 this study demonstrates that all stakeholder groups share common policies that they least prefer, although the specific policies differ according to the group. The policies that healthcare workers and academics least prefer include financing healthcare by diverting resources from defence, social protection, and education; financing healthcare through increased VAT; and introducing a payroll tax to finance healthcare. Stakeholders are unwilling to divert resources from other critical sectors, given the long-term correlation between the performance of these sectors and the health of the population.6 Diverting resources may compromise the socio-economic demographics of a country and be in opposition to notions of equity and fairness.33,34 Additionally, stakeholders showed a low preference for tax-related policies because they consider the detrimental effects of taxes on disposable income and economic growth.35 These policies would increase the burden on taxpayers, leading to a decline in consumption and private sector activity, which could result in protracted economic challenges. Stakeholders’ low preferences for these policies reflect their concerns about maintaining equity, access, and quality in healthcare without compromising other critical sectors and the overall economy.
The results of the study revealed a notable discrepancy in policy preferences among academics, physicians, nurses, allied healthcare professionals, and healthcare administrators, aside from the top four preferred policies. For instance, nurses ranked the introduction of additional excise taxes on tobacco products as their least preferred option (ranked at 20) compared to other stakeholders (with an average rank of 10). Aikins et al36 reported that people prefer higher taxes on alcohol and tobacco, as their consumption contributes to the increasing burden of NCDs. However, nurses, who directly deal with tobacco-addicted patients, may show empathy to the patients and oppose such policies to avoid overburdening them. Nurses also ranked the policy to allocate a portion of traffic violation revenue to healthcare services, particularly to trauma cases, as one of their least preferred options (ranked at 8), while academics (ranked at 6) and other professionals (ranked at 1) preferred this option. Nurses may prefer that the allocation be made generally rather than earmarked for specific trauma cases to help more patients. This is in line with the study by Bourke et al,37 who found that severity of a disease is not a sufficient justification for special preferential funding according to the surveyed public in the United Kingdom.
The policy preferences of nurses also differed significantly from those of other healthcare professionals, as indicated by their rankings. Nurses ranked the policy to deduct an annual percentage from health insurance companies in case beneficiaries are not receiving services as their third most preferred policy, while other professionals ranked this option in eighth or ninth position. In addition, nurses preferred a more restricted package of care, excluding fewer essential services such as dental, optical, and physiotherapy, as their eleventh most preferred policy, while other professionals ranked it as their twentieth most preferred policy. Nurses’ preferences suggest that they prioritize maximizing the number of patients receiving treatment and believe that insurance companies should pay back unused premiums. Ejughemre38 contends that there should be regulation of the private sector’s efforts to finance healthcare, which is consistent with this finding.
Academics ranked subsidizing gym memberships and frequent gym use from the healthcare system’s budget in sixth position, whereas healthcare workers ranked this option in ninth position. Healthcare professionals understand that being healthy involves more than simply exercising at the gym, including factors such as a healthy diet. As a result, any policy that aims to reduce healthcare funding is likely to meet resistance from healthcare workers. However, healthcare workers ranked the option that smokers and tobacco consumers should contribute significantly more to the cost of their care (for tobacco-related health issues) higher (at 13) than academics (at 17), who rarely encounter tobacco-related cases. The same is true for the policy of increasing tax on sugar-sweetened beverages to generate additional funding, which healthcare workers ranked at 14 while academics ranked lower at 16. Healthcare workers appear to prioritize solutions that do not disproportionately affect specific population groups.
According to the results, the top five feasible policies are as follows: increasing taxes on cigarettes; introducing an income tax with a portion earmarked for healthcare services; allocating a portion of the traffic violation penalty revenue to healthcare, particularly for trauma cases; increasing VAT or consumption tax by two percentage points and allocating it for healthcare services; and increasing taxes on sugar-sweetened beverages. All stakeholders concur that policies related to implementing different types of taxes are feasible and more straightforward to implement. However, some stakeholders have concerns regarding the diverse impact these policies would have on the economy, people’s welfare, and the excess burden. Therefore, while these policies may be practical, they may not necessarily be desirable.
This study has some limitations. Specifically, the data were analysed using non-parametric statistical tests such as the two-sample Mann–Whitney U-test and Kruskal–Wallis test, and the policy options were ranked based on their overall sum score mean by the respondents. However, as pointed out by Wiseman,39 different methods of aggregation can result in different preference rankings. Therefore, the results should be interpreted in the context of the specific technique used. The sample size included a large number of health practitioners relative to the academic staff. Therefore, full sample results could be influenced by the preferences of the larger group. Nevertheless, the healthcare workers group is diverse with several subgroups that should reduce the degree of preference monopoly. Additionally, due to access constraints, the study was unable to incorporate other stakeholders, such as individuals from professional associations, political leadership, and community members. Future studies may consider including these stakeholders to capture their preferences and insights. Finally, since the sampling procedure was a snowball sampling technique, there is a chance of the professionals referring the survey to their like-minded colleagues, which would induce non-randomness of the sample. Future research should therefore consider using physical interviews and random selection of the respondents. Furthermore, this study should be replicated in other similar countries in the Arabian Gulf to ascertain external validity through comparison of results.
Conclusions
This study provides a framework for understanding stakeholder preferences on healthcare financing sustainability, ranking 26 policy options according to stakeholder groups. To ensure that healthcare policies align with stakeholder preferences, governments must take these preferences into account when formulating policies. When designing healthcare financing systems, governments should carefully consider factors such as whether the funding system promotes progressiveness or horizontal equity, whether it leads to redistribution, and its effects on healthcare coverage, access, and the broader economy. Additionally, policymakers must carefully guide policy-making processes that involve private sector actors to ensure strategies that support the achievement of UHC and the sustainability of healthcare finances. Countries must plan for the long-term implementation and sustainable financing of UHC by considering total resource requirements. The appropriate mix of financing mechanisms should be informed by evidence-based and data-driven approaches that consider relevant stakeholder preferences.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available due to privacy and confidentiality agreements as well as other restrictions but are available from the corresponding author (MKA) on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Kennedy EM. Health care as a basic human right: moving from lip service to reality. Harv Hum Rts J. 2009;22:165.
2. UN. United Nations: transforming our world: the 2030 agenda for sustainable development; 2015. Available from: https://sdgs.un.org/2030agenda.
3. The World Bank.Universal health coverage; 2023. Available from: https://www.worldbank.org/en/topic/universalhealthcoverage.
4. Oraro-Lawrence T, Wyss K. Policy levers and priority-setting in universal health coverage: a qualitative analysis of healthcare financing agenda setting in Kenya. BMC Health Serv Res. 2020;20:1–11. doi:10.1186/s12913-020-5041-x
5. Hartwig J. What drives health care expenditure?—Baumol’s model of ‘unbalanced growth’revisited. J Health Econ. 2008;27(3):603–623. doi:10.1016/j.jhealeco.2007.05.006
6. Dixon A. Are medical savings accounts a viable option for funding health care? Croat Med J. 2002;43(4):408–416.
7. Al-Hanawi MK, Alsharqi O, Almazrou S, Vaidya K. Healthcare finance in the Kingdom of Saudi Arabia: a qualitative study of householders’ attitudes. Appl Health Econ Health Policy. 2018;16:55–64. doi:10.1007/s40258-017-0353-7
8. Horton S, Sullivan R, Flanigan J, et al. Delivering modern, high-quality, affordable pathology and laboratory medicine to low-income and middle-income countries: a call to action. Lancet. 2018;391(10133):1953–1964.
9. Bloom DE, Khoury A, Subbaraman R. The promise and peril of universal health care. Science. 2018;361(6404):eaat9644. doi:10.1126/science.aat9644
10. Folke C, Carpenter S, Elmqvist T, Gunderson L, Holling CS, Walker B. Resilience and sustainable development: building adaptive capacity in a world of transformations. AMBIO. 2002;31(5):437–440. doi:10.1579/0044-7447-31.5.437
11. Lim J. Sustainable health care financing: the Singapore experience. Global Policy. 2017;8:103–109. doi:10.1111/1758-5899.12247
12. MacLeod TE, Harris AH, Mahal A. Stated and revealed preferences for funding new high-cost cancer drugs: a critical review of the evidence from patients, the public and payers. Patient Centered Outcom Res. 2016;9:201–222. doi:10.1007/s40271-015-0139-7
13. Mathauer I, Torres LV, Kutzin J, Jakab M, Hanson K. Pooling financial resources for universal health coverage: options for reform. Bull World Health Organ. 2020;98(2):132. doi:10.2471/BLT.19.234153
14. Mathauer I, Koch K, Zita S, et al. Revenue-raising potential for universal health coverage in Benin, Mali, Mozambique and Togo. Bull World Health Organ. 2019;97(9):620. doi:10.2471/BLT.18.222638
15. Al-Hanawi MK, Mwale ML, Kamninga TM. The effects of health insurance on health-seeking behaviour: evidence from the kingdom of Saudi Arabia. Risk Manag Healthc Policy. 2020;595–607. doi:10.2147/RMHP.S257381
16. Al-Amoudi SM. Health empowerment and health rights in Saudi Arabia. Saudi Med J. 2017;38(8):785. doi:10.15537/smj.2017.8.19832
17. Almasabi M. An overview of health system in Saudi Arabia. Res J Med Sci. 2013;7(3):70–74.
18. Walston S, Al-Harbi Y, Al-Omar B. The changing face of healthcare in Saudi Arabia. Ann Saudi Med. 2008;28(4):243–250. doi:10.5144/0256-4947.2008.243
19. Al-Hanawi MK, Khan SA, Al-Borie HM. Healthcare human resource development in Saudi Arabia: emerging challenges and opportunities—a critical review. Public Health Rev. 2019;40:1–16. doi:10.1186/s40985-019-0112-4
20. Alkhamis AA. Critical analysis and review of the literature on healthcare privatization and its association with access to medical care in Saudi Arabia. J Infect Public Health. 2017;10(3):258–268. doi:10.1016/j.jiph.2017.02.014
21. Mwale ML, Mchenga M, Chirwa GC. A spatial analysis of out-of-pocket payments for healthcare in Malawi. Health Policy Plan. 2022;37(1):65–72. doi:10.1093/heapol/czab090
22. Rahman M, Islam M, Hossain F, Alam A, Jung J, Akter S. Forgone healthcare and financial burden due to out-of-pocket payments in Bangladesh: a multilevel analysis. Health Econ Rev. 2022;12(1):1–11. doi:10.1186/s13561-021-00348-6
23. Al-Hanawi MK. Decomposition of inequalities in out-of-pocket health expenditure burden in Saudi Arabia. Soc Sci Med. 2021;286:114322. doi:10.1016/j.socscimed.2021.114322
24. Sinha RK, Chatterjee K, Nair N, Tripathy PK. Determinants of out-of-pocket and catastrophic health expenditure: a cross-sectional study. Br J Med Med Res. 2016;11(8):1. doi:10.9734/BJMMR/2016/21470
25. Tordrup D, Angelis A, Kanavos P. Preferences on policy options for ensuring the financial sustainability of health care services in the future: results of a stakeholder survey. Appl Health Econ Health Policy. 2013;11:639–652. doi:10.1007/s40258-013-0056-7
26. Nunally JC, Bernstein IH. Psychometric Theory. New York: McGraw-Hill; 1978.
27. Ali Z, Bhaskar SB. Basic statistical tools in research and data analysis. Indian J Anaesth. 2016;60(9):662. doi:10.4103/0019-5049.190623
28. Algabbani A, Alqahtani A, BinDhim N. Prevalence and determinants of non-communicable diseases in Saudi Arabia. Food Drug Regulat Sci J. 2019;2(2):1–10.
29. Al-Hanawi MK. Socioeconomic determinants and inequalities in the prevalence of non-communicable diseases in Saudi Arabia. Int J Equity Health. 2021;20(1):1–13. doi:10.1186/s12939-021-01510-6
30. World Health Organization. Noncommunicable diseases: key facts 2022; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases.
31. Alghnam S, Alkelya M, Alfraidy M, Al-Bedah K, Albabtain IT, Alshenqeety O. Outcomes of road traffic injuries before and after the implementation of a camera ticketing system: a retrospective study from a large trauma center in Saudi Arabia. Ann Saudi Med. 2017;37(1):1–9. doi:10.5144/0256-4947.2017.1
32. Gapenski L. Healthcare Finance: An Introduction to Accounting and Financial Management. Washington: Health Administration Press; 2012.
33. Creese AL. User charges for health care: a review of recent experience. Health Policy Plan. 1991;6(4):309–319. doi:10.1093/heapol/6.4.309
34. Lu H, Burge P, Sussex J. Measuring public preferences between health and social care funding options. J Choice Model. 2021;38:100266. doi:10.1016/j.jocm.2020.100266
35. Stoilova D. Tax structure and economic growth: evidence from the European Union. Contad Adm. 2017;62(3):1041–1057. doi:10.1016/j.cya.2017.04.006
36. Aikins M, Tabong PT-N, Salari P, Tediosi F, Asenso-Boadi FM, Akweongo P. Positioning the National Health Insurance for financial sustainability and Universal Health Coverage in Ghana: a qualitative study among key stakeholders. PLoS One. 2021;16(6):e0253109. doi:10.1371/journal.pone.0253109
37. Bourke SM, Plumpton CO, Hughes DA. Societal preferences for funding orphan drugs in the United Kingdom: an application of person trade-off and discrete choice experiment methods. Value Health. 2018;21(5):538–546. doi:10.1016/j.jval.2017.12.026
38. Ejughemre UJ. Accelerated reforms in healthcare financing: the need to scale up private sector participation in Nigeria. Int J Health Policy Manag. 2014;2(1):13. doi:10.15171/ijhpm.2014.04
39. Wiseman V. Aggregating public preferences for healthcare: putting theory into practice. Appl Health Econ Health Policy. 2004;3:171–179. doi:10.2165/00148365-200403030-00008
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.