Back to Journals » Patient Preference and Adherence » Volume 20
Preferences of Patients and Cardiologists Regarding Pacemaker Characteristics in Spain: A Discrete Choice Experiment
Authors García Fernández FJ ![]() , Fidalgo Andrés ML, Álvarez Orozco M, Comellas M, Viciano Delibano E
, Fidalgo Andrés ML, Álvarez Orozco M, Comellas M, Viciano Delibano E ![]() , Ruiz Mateas F
, Ruiz Mateas F
Received 20 October 2025
Accepted for publication 28 January 2026
Published 20 February 2026 Volume 2026:20 575656
DOI https://doi.org/10.2147/PPA.S575656
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Francisco Javier García Fernández,1,* María Luisa Fidalgo Andrés,2,* María Álvarez Orozco,3,* Marta Comellas,4,* Elena Viciano Delibano,4,* Francisco Ruiz Mateas5,*
1Arrhythmia Unit, University Hospital Complex of Burgos (CAUBU), Burgos, Spain; 2Arrhythmia Unit, University Hospital Complex of León (CAULE), León, Spain; 3Medtronic Iberica S.A., Madrid, Spain; 4Outcomes’ 10 (a ProductLife Group Company), Castellón, Spain; 5Department of Cardiology, Costa del Sol University Hospital, Marbella, Spain
*These authors contributed equally to this work
Correspondence: Francisco Ruiz Mateas, Department of Cardiology, Hospital Universitario Costa del Sol, Marbella, 29603, Spain, Email [email protected]
Purpose: A better understanding of the preferences of patients and cardiologists for pacemaker characteristics is essential for advancing patient-centered care. We therefore aimed to identify and quantify the preference that patients and cardiologists assign to specific characteristics.
Patients and Methods: We conducted an observational, cross-sectional, descriptive study based on a discrete choice experiment (DCE). The design was informed by a literature review, a patient focus group, and a scientific committee.
Results: A total of 42 patients (66.7% male, mean [SD] age 64.2 [12.1] years) and 42 cardiologists (64.3% male, mean age 47.3 [9.3] years) participated in the study. For both patients (P) and cardiologists (C), the most important characteristics of pacemakers (higher relative importance, RI) are MRI compatibility (P: 28.1%; C: 25.1%) and battery longevity (P: 22.6%; C: 23.8%). The type of follow-up is more highly valued by cardiologists than by patients (P: 10.2%; C: 21.1%), whereas pacemaker size is prioritized by patients (P: 19.1%; C: 7.7%). From the cardiologists’ perspective, safety (12-month post-implantation infection rate: 19.39%) and technical aspects such as conduction system pacing (CSP) (15.14%), algorithms for minimizing unnecessary right ventricular stimulation (9.43%), and programming modes (9.11%) are also important decision drivers.
Conclusion: MRI compatibility and battery longevity are key factors for both patients and cardiologists in decision-making. Patients also prioritize generator size and replacement processes, while cardiologists additionally focus on safety (infection rates) and technical aspects (CSP and algorithms to reduce unnecessary right ventricular stimulation).
Plain Language Summary: Pacemakers help control abnormal heart rhythms. These devices differ in several features, and both patients and cardiologists may value them differently.
This study explored which pacemaker characteristics are most important to patients and cardiologists. Forty-two patients with pacemakers and forty-two cardiologists participated in a survey that asked them to choose between different device options.
Both groups agreed that MRI compatibility (being safe for magnetic resonance scans) and battery longevity were the most valued characteristics. Patients gave greater importance to the size of the device, preferring smaller generators, while cardiologists placed more value on how follow-up is performed after implantation.
Cardiologists also emphasized safety, such as lowering infection risk after the procedure, and technical aspects, including conduction system pacing and algorithms that help reduce unnecessary right ventricular stimulation.
Overall, the study shows that patients and cardiologists share similar priorities regarding MRI compatibility and battery life, but differ in their focus on other features. Recognizing these differences can help improve communication and support shared decision-making when selecting a pacemaker, ensuring that treatment choices better reflect what matters most to patients.
Keywords: pacemaker, preferences, discrete choice experiment
Introduction
Cardiovascular diseases are the leading cause of morbidity and mortality worldwide, including disorders of the cardiac conduction system that result in bradyarrhythmias and require permanent cardiac pacing.1–3 Implantable pacemakers (PM) are an effective treatment for these conditions and have been shown to improve survival and health-related quality of life (HRQoL).4–7 Accordingly, PM implantation rates remains high across several European countries,8 with the Spanish Pacemaker Registry reporting an implantation rate of 891 units per million population in 2023.9
Advances in PM technology have transformed cardiac pacing, evolving from simple single-lead devices (conventional PM) to more sophisticated systems with distinct technical characteristics, such as stimulation modes, sensing capabilities, and implantation approaches.10–14 Among these, leadless pacemakers (LLPM) represent a major innovation, offering potential advantages over conventional transvenous PMs in certain clinical scenarios,15–18 particularly for patients with limited vascular access and high risk of infection.19–24 These devices reduce the complications associated with conventional PM implantation, largely related to the implantation technique, the electrode, and the generator pocket.7,25
Although the benefits of different types of PMs in improving HRQoL and survival are well stablished, data on how patients and cardiologists value specific PM characteristics remain limited. Understanding these preferences could facilitate the implementation of shared decision-making, a fundamental pillar of patient-centered medicine,26,27 especially in cardiology, where therapeutic options available are diverse and complex. Capturing and comparing these preferences provides valuable insight into real-world decision-making and potential mismatches between patient and clinician perspectives. Moreover, patient preferences are increasingly recognized as relevant inputs for clinical guidelines, health technology assessment and healthcare decision-making, supporting more informed and patient-centered decision-making processes.28–30
The aim of this study was to identify and quantify patients’ and cardiologists’ preferences for PM characteristics.
Materials and Methods
This was a cross-sectional study employing a discrete choice experiment (DCE), led by a scientific committee (SC) consisting of three cardiologists (FJGF, MLFA, FRM) with extensive experience in PM implantation.
Population
Patients aged ≥18 years implanted with a PM (conventional or leadless) for at least 12 months were eligible for inclusion. Cardiologists were eligible if they had at least 1 year of experience in the implantation and/or follow-up of conventional PM and LLPM, were actively involved in cardiac pacing, electrophysiology, or arrhythmia units within the Spanish public healthcare system, and had ongoing clinical activity in device implantation. Operator experience was further characterized by years of practice and annual procedural volume.
To obtain a heterogeneous patient sample, participants were identified and invited to take part in the study through the Spanish patient advocacy group CardioAlianza, and recruited during routine clinical practice by the 3 cardiologists serving on the SC.
The SC also identified and invited cardiologists to participate in the study.
According to the rule of thumb proposed by Johnson and Orme,31–33 a minimum sample size of 42 participants was estimated.
Discrete Choice Experiment
A DCE is a conjoint analysis technique that enables the identification and analysis of participants’ preferences regarding a treatment, intervention, or health product in a relatively straightforward manner,34–36 and simulates the process of choosing a treatment or medical device. This is achieved by presenting participants with a series of hypothetical scenarios (choice sets) comprising 2 or more alternatives. These alternatives are derived from the combination of different attributes (or characteristics) of the treatments or health products, along with the respective levels (or values) that each attribute can assume. Participants are then required to select their preferred option from the choice set.34,37 The DCE in this study was conducted following the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) good practice recommendations for conjoint analysis in healthcare.34
To design the choice sets, a literature review was performed and a focus group was held with patients. The literature review in international databases (PubMed/Medline) identified the characteristics (attributes and levels) that describe pacemakers. The information obtained was supplemented with a review of the technical documentation of these devices. A focus group with patients who had undergone pacemaker implantation was subsequently organized to determine which pacemaker characteristics were considered most relevant. The patients who participated in the focus group were identified and invited to participate through CardioAlianza. The SC reviewed and confirmed the attributes and levels identified in the literature and the patient focus group.
Since some of the characteristics included in the scenarios were highly technical and likely to be difficult for patients to understand, it was decided to create two separate DCEs: one for both patients and cardiologists (DCE 1), and another exclusively for cardiologists (DCE 2). The language used in the DCE addressed to patients was adapted to enhance their understanding. Efforts were made to simplify complex terminology and ensure that the choice set and instructions were clear and comprehensible.
Table 1 shows the attributes and levels included in DCE 1 and DCE 2. A common attribute (absence/presence of leads) was included in both DCEs to jointly analyze the preferences of cardiologists. This repeated attribute was intentionally included to allow joint estimation of preferences across DCE blocks and to facilitate comparison of trade-offs under different attribute combinations, in accordance with standard DCE methodology.34,38
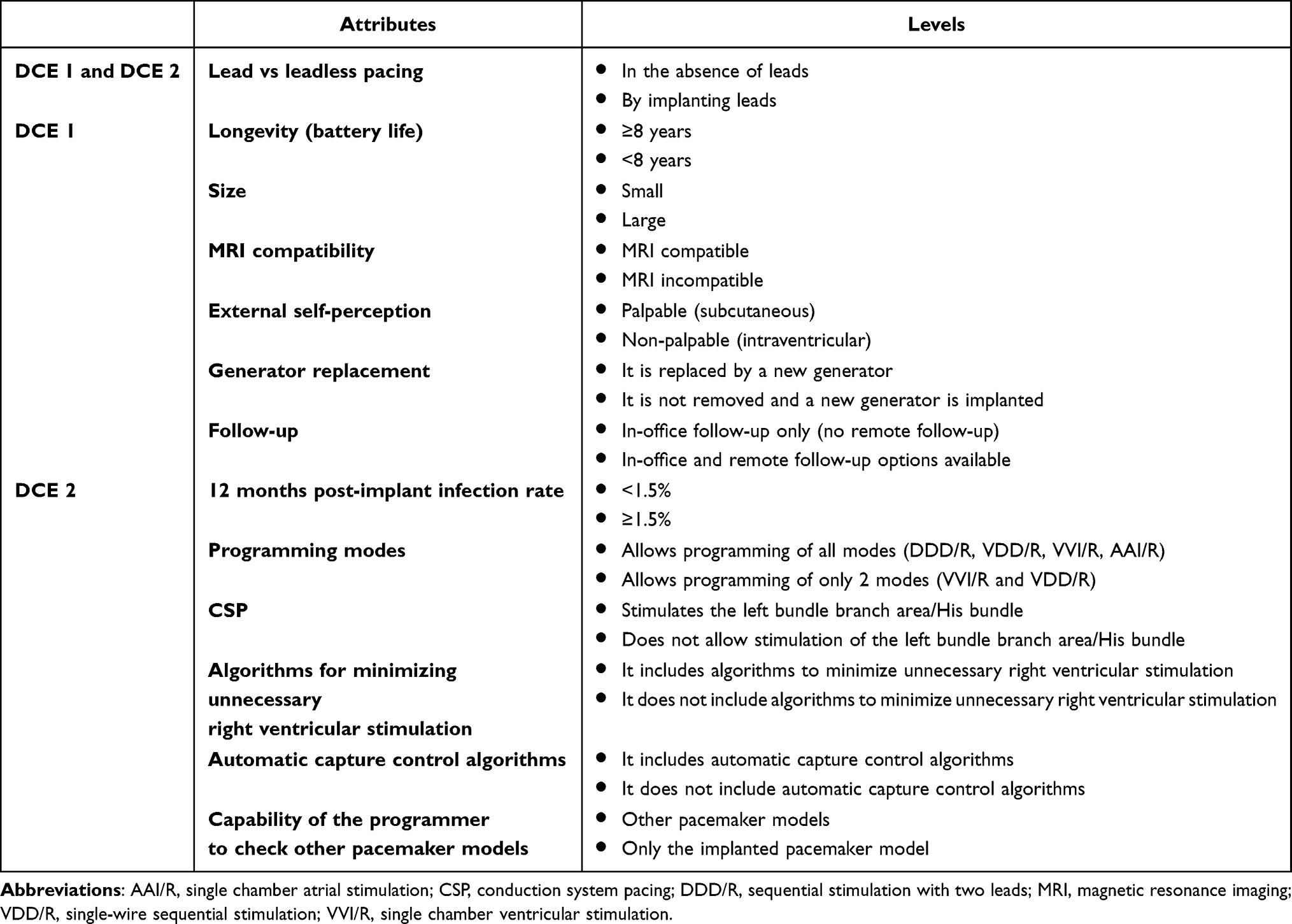 |
Table 1 Attributes and Levels Included in DCE 1 (Addressed to Patients and Cardiologists) and DCE 2 (Addressed to Cardiologists) |
To construct the different choice sets, the attributes and levels were combined following ISPOR guidelines,34 ensuring their orthogonality and balance. The orthogonal design guarantees that all attribute levels vary independently, while the balance design ensures that each attribute level occurs the same number of times. A total of 12 pairs of choice sets were obtained for each DCE (Table 2).
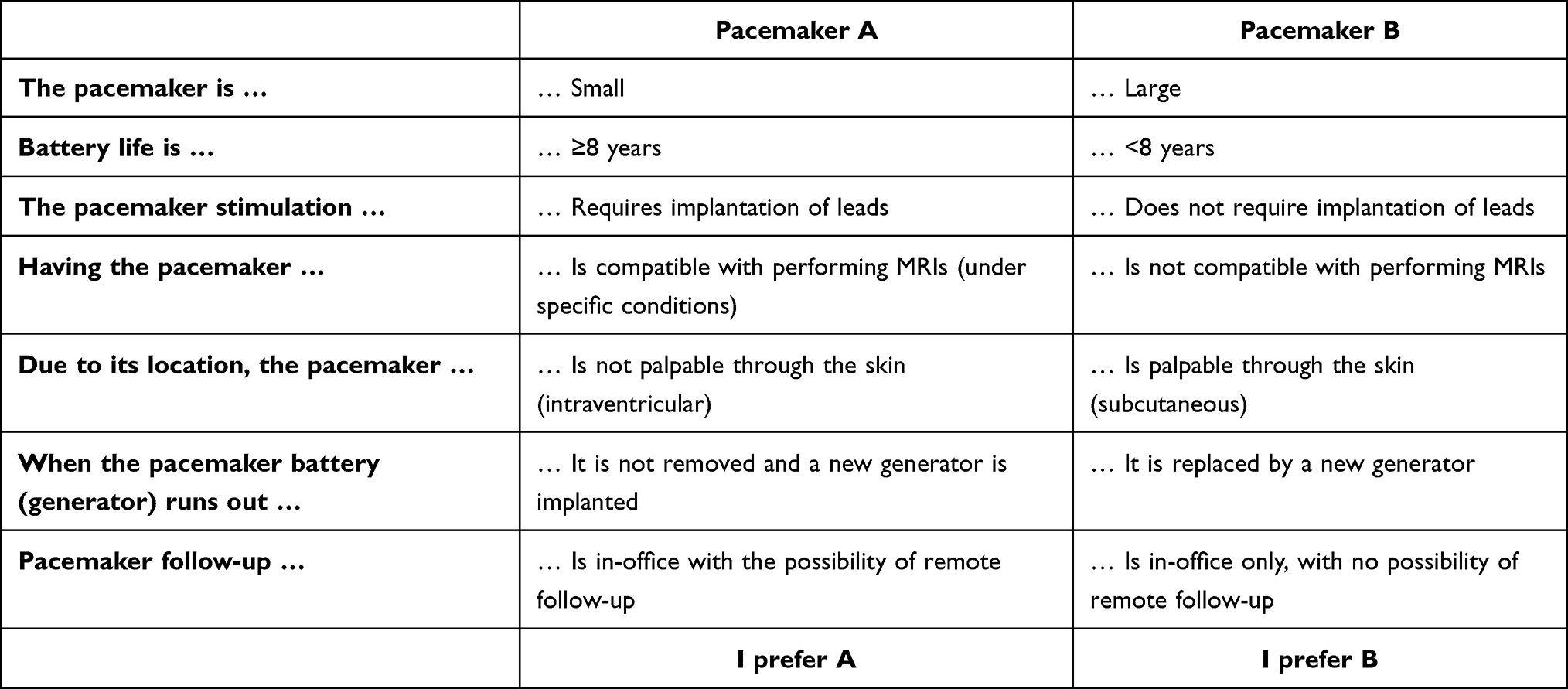 |
Table 2 Example of Choice Set in the DCE 1 Addressed to the Cardiologists |
To ensure that all participants included in the analysis had fully understood the methodology, a choice set with a dominant scenario, depicting the desired levels or characteristics of each PM attribute (Table S1) was also presented along with the rest of the choice sets. Participants were required to respond correctly to this scenario to proceed with the study.
The choice sets included in the DCE 1 and DCE 2 were reviewed by the study SC to ensure their plausibility for the participants and to avoid implausible combinations in the experimental design.34,38 Additionally, the choice sets were presented to 3 patients to verify that the attributes and levels included in the scenarios, as well as the language used, were understandable and that they could easily complete the required exercise.
An electronic questionnaire was developed to present the choice sets to participants. This questionnaire also collected patient sociodemographic, clinical and care characteristics, including age, sex, permanent address, level of education, dependence on a PM, and the date of PM implantation. The following variables were collected from cardiologists: age, sex, institutional affiliation and scope of practice (public, private, or mixed healthcare), years of experience in the implantation of conventional PMs and LLPMs, and the approximate number of implants performed in the last year.
Because DCE1 and DCE2 included different sets of accompanying attributes, the relative importance and statistical significance of a given attribute may vary across DCEs, reflecting context-dependent preferences and trade-offs rather than inconsistency in responses.
Statistical Analysis
The choices made by participants (patients and cardiologists) in each scenario were analyzed to obtain the partial utility values of each level of the attributes using a mixed logit regression model for patients. In this model, the participant’s choice in each scenario was the dependent variable, while the attribute levels were treated as independent variables. The attributes are the characteristics of the PM (such as battery duration, size, or magnetic resonance imaging [MRI] compatibility), and the levels are the specific options within each attribute (eg, a PM with a battery life of 5 years versus one with 10 years). Unlike conditional logit models, the mixed logit model accounts for preference heterogeneity across individuals, allowing the estimation of preferences at the individual level.39,40 However, the mixed logit model did not converge for the cardiologist sample, likely due to the combination of sample size and model complexity. Therefore, a conditional logit model was employed to estimate average preferences for cardiologists. Owing to the use of different model specifications, direct statistical comparison of utility coefficients between patients and cardiologists was not performed. Instead, the maximum utility values of each attribute were used to establish their relative importance (RI), reflecting the importance of each attribute relative to the others.41,42 Statistics of centrality and dispersion were calculated for each RI.
The statistical analysis was performed using STATA v.14. For all statistical tests, a p-value <0.05 was considered significant. Quantitative variables were described using centrality and dispersion statistics (mean, standard deviation [SD], quartiles, minimum and maximum), while qualitative variables were described with relative and absolute frequencies.
Student’s t-test (or the equivalent non-parametric test in the case of non-normal distribution of the variables) was used to establish the differences in the preferences (RI) assigned by cardiologists and patients.
Compliance with Ethical Guidelines
The study was conducted in accordance with the Declaration of Helsinki and followed International Council for Harmonisation Good Clinical Practice guidelines. The study was evaluated and approved by the Clinical Research Ethics Committee of the Hospital Puerta de Hierro de Madrid, Spain (code 07/23).
All patients provided written informed consent.
Results
Sociodemographic and Clinical Characteristics
A total of 42 patients (66.7% male; mean [SD] age 64.2 [12.1] years; 40.5% with higher education; 73.8% with PM dependency), and 42 cardiologists (64.3% male; mean [SD] age 47.3 [9.3] years; 61.0% working in public healthcare only; mean [SD] 16.8 [9.4] years performing conventional PM implantation and mean [SD] 6.7 [8.1] years performing LLPM; with a mean [SD] of 115 [69.2] PMs implanted last year) met the inclusion criteria, responded correctly to the dominant scenario, and completed the electronic questionnaire (Table 3).
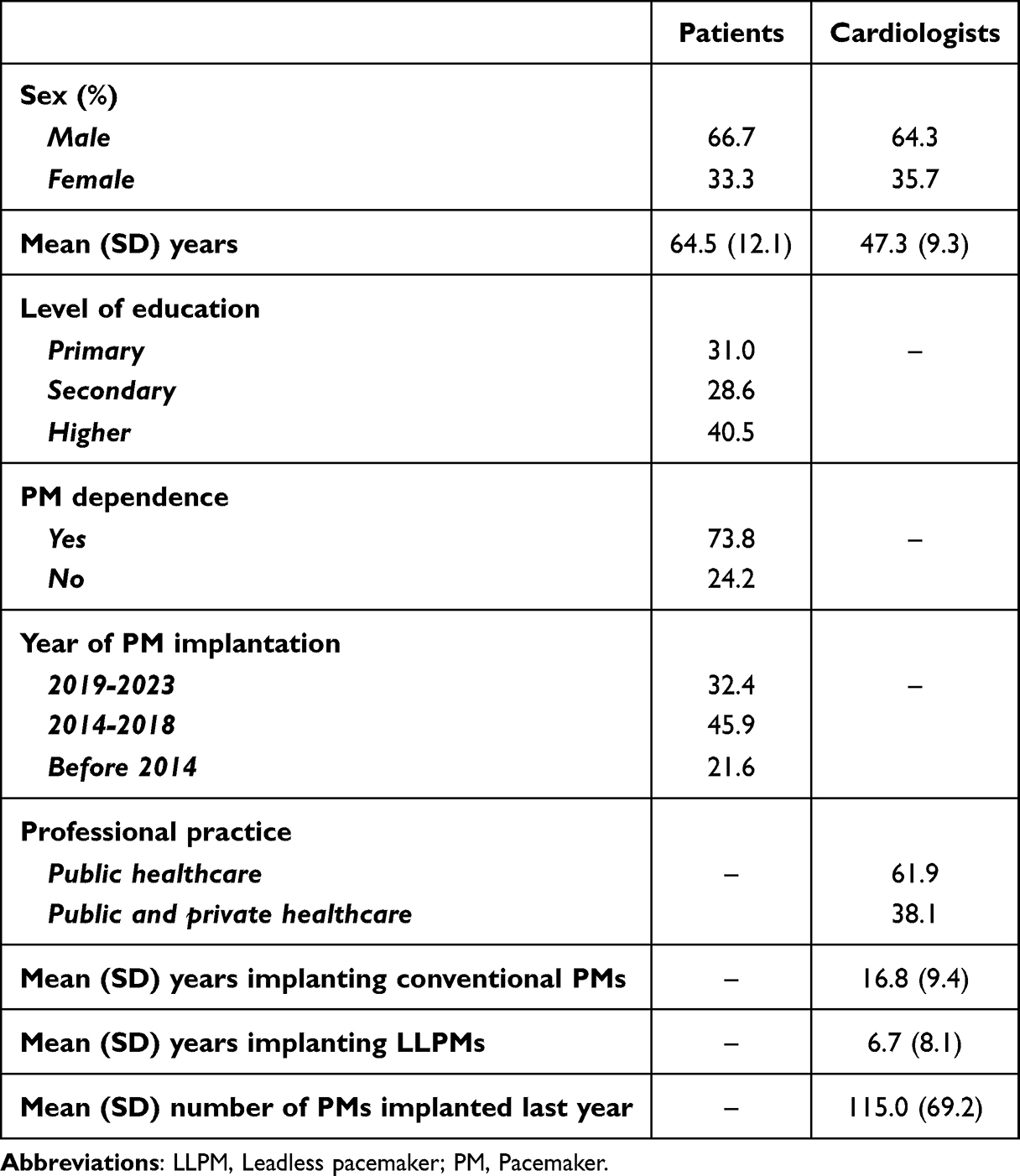 |
Table 3 Characteristics of Patients and Cardiologists |
Patients’ and Cardiologist’ Preferences
Partial Utilities
Partial utilities reflect the importance of an attribute level against a reference level.34 A negative coefficient indicates a lower preference for the level compared to the reference level.
For patients (Table 4), all attributes were statistically significant, except for those involving leads or leadless pacing and self-perception, indicating that they are important when choosing a PM. All partial utilities were negative, so the preferred levels are the reference levels [ref]: small size, duration ≥8 years, LLPM, MRI compatibility, no external perception of the device, possibility of generator replacement by the time elective replacement is indicated, and availability of both types of follow-up (in-office and remote).
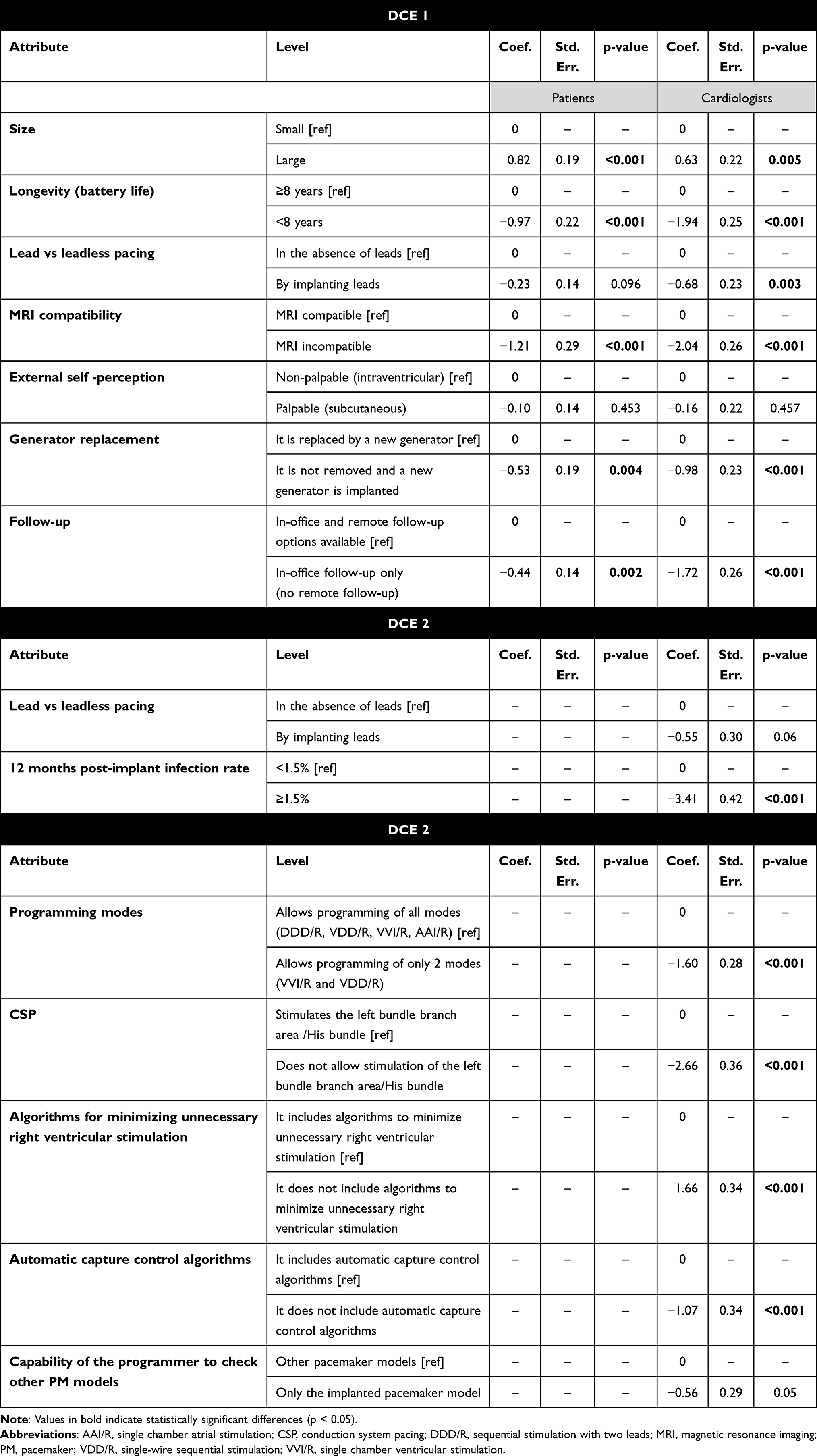 |
Table 4 Patients’ and Cardiologists’ Partial Utilities (DCE 1 and DCE 2) |
Similarly, for cardiologists (Table 4), all attributes, except for external self-perception, were statistically significant and therefore considered drivers of decision making. Likewise, all utilities were negative, so the preferred levels are reference levels.
The partial utilities showed that all the presented technical characteristics, except for the capability of the programmer to check other PM models and lead vs leadless pacing, were relevant for the decision (Table 4). In this case, the reference levels were also the preferred ones: leadless pacing, 12-month post-implantation infection rate of <1.5%, allows programming of all modes, CSP, inclusion of algorithms to minimize unnecessary right ventricular stimulation, inclusion of automatic capture control algorithms, and the compatibility of the programmer with other PM models.
Relative Importance
The RI assigned to each attribute enables the characteristics of the PM to be ranked and establishes the importance of each attribute compared to the rest.
For both patients (P) and cardiologists (C) (Figure 1), the most relevant characteristics of PMs (higher RI) were MRI compatibility (P: 28.1%; C: 25.1%) and battery longevity (P: 22.6%; C: 23.8%). In third place, cardiologists assigned greater importance to the type of follow-up (21.1%), whereas patients considered PM size a more valuable characteristic (P: 19.1%). Finally, leadless pacing and external self-perception were the least prioritized characteristics by both doctors and patients (P: 2.4%; C: 2.0%).
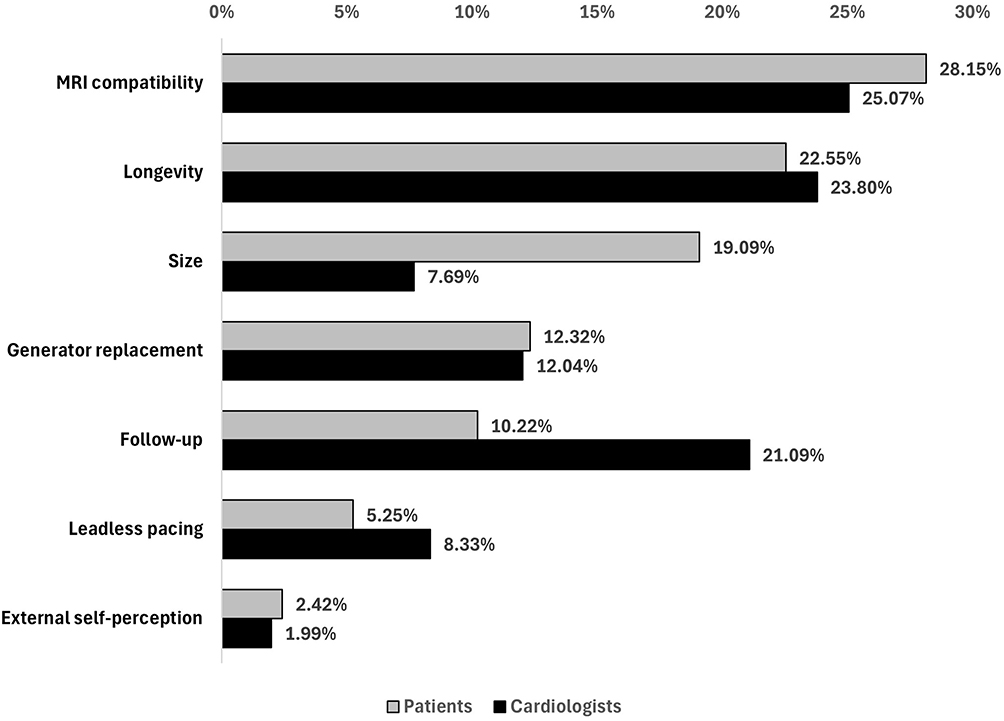 |
Figure 1 Relative importance given by patients and cardiologists (DCE1). |
When all the characteristics of the PMs were considered (including those technical features of DCE 2), the most important and therefore decision drivers from the cardiologists’ perspective were: 12-month post-implantation infection rate (19.39%), CSP (15.14%), MRI compatibility (9.44%), algorithms for minimizing unnecessary right ventricular stimulation (9.43%), programming modes (9.11%), and battery longevity (8.96%) (Figure 2).
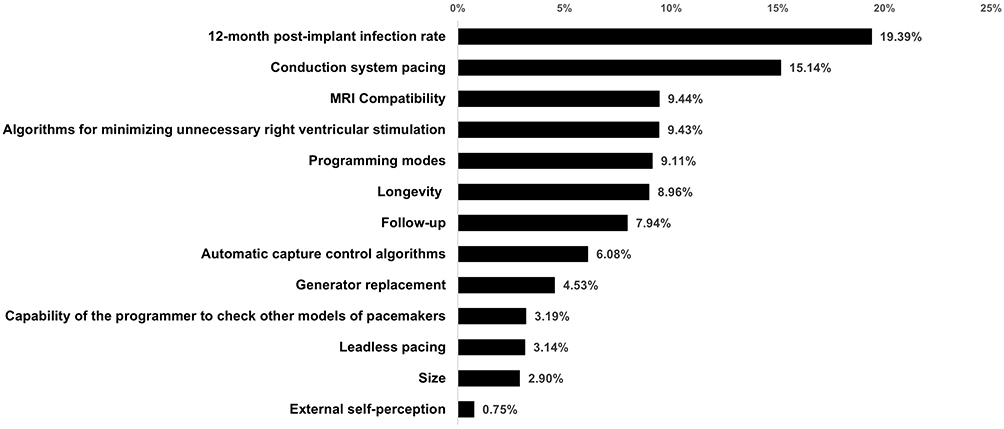 |
Figure 2 Relative importance of cardiologists (DCE2). |
Discussion
Current guidelines for the management of patients with cardiovascular diseases recommend that clinicians should engage eligible patients in shared decision‐making,29,30 particularly when it comes to selecting the type of stimulation (pacing or resynchronization), programming type, and addressing patient needs during cardiac device placement.30 A key component of patient-centered care is involving patients in decision-making, which ensures that treatment decisions align with patients’ values and needs.26 Therefore, understanding their preferences is crucial for the successful implementation of this approach.
This study provides information on the preferences of patients and cardiologists for PM characteristics. This preference data may facilitate shared decision-making, since most of the attributes included in DCEs significantly predicted choice and were important to this process. Additionally, the information gathered in this study could be highly useful in defining the clinical development strategy of new devices, potentially helping to create devices that reflect the preferences of both patients and cardiologists.
A total of 42 patients and 42 cardiologists participated in the study. The characteristics of the patient sample were broadly comparable to those reported in the 2023 National Pacemaker Registry published by the Heart Rhythm Association of the Spanish Society of Cardiology.9 However, patients included in our study were substantially younger (64.5 vs 77.8 years) than those reported in the registry.9 This age difference likely reflects a selection effect inherent to preference-based studies using self-administered electronic questionnaires and cognitively demanding DCE, which may limit participation among older or more frail patients. This limitation may affect the generalizability of the findings but does not compromise the internal validity of the estimated preference structures. In contrast, the data show that the cardiologists involved have extensive experience in PM implantation and follow-up.
Although different surveys have explored patient preferences on topics related to cardiac implantable electronic devices (such as discharge timing after implantation,43 their experiences with PM home follow-up,44,45 preferences for PM removal,46,47 and removable over non-removable LLPMs and conventional PMs48), no prior studies have examined the perspective of both patients and cardiologists on the specific elements of PMs. To our knowledge, this is the first study evaluating the preferences of both patients and cardiologists for PM characteristics.
The study results show that, for both groups, MRI compatibility and longer longevity of the PMs (≥8 years) are the main decision drivers.
MRI is considered the gold standard imaging technique for a wide range of cardiac and non-cardiac diseases, and it is estimated that about 50%-75% of patients with PMs will need an MRI during their lifetime. While having a PM was previously considered an absolute contraindication for MRI, significant advances in PM device technology have made it possible to overcome this challenge.49–51
Regarding battery longevity, a recent systematic review52 showed that one of the most common complications in patients with a PM was early battery depletion (a battery that fails before the manufacturer’s specified lifespan), which affected between 0.8%53 to 5.5%54 of patients. However, the improvements made to PMs have enhanced performance in this regard. A recent study has reported that real-world data on longevity exceeds manufacturer predictions, with a median virtual battery life reaching up to 16 years.55
The type of follow-up is also an aspect valued by both cardiologists and patients. Previous evidence from semi-structured interviews with patients and clinicians shows that, although there are concerns about the limited understanding of how remote follow-up and alerts work, patients and clinicians generally have confidence in the technology and remote monitoring.44 Furthermore, in line with our findings, a patient survey indicated that patients prefer remote follow-up, citing benefits such as reduced travel time and receiving actionable alerts.45 Remote monitoring has also been shown to reduce hospitalizations and healthcare resource use,56–59 and to provide clinical benefits, including longer battery life and better survival rates.56,60
From the patients’ perspective, the size of the PM is also a decision driver. Reducing the generator size has been one of the key goals pursued in advancing PM technology.61 Over the years, smaller PMs have been developed to offer several benefits, including improved patient comfort, reduced risk of complications, and easier implantation, especially in patients with smaller or more challenging anatomies.61
Analysis of cardiologists’ preferences for technical characteristics (DCE 2) showed that cardiologists assigned the highest RI to infections at 12 months post-implantation, followed by CSP, MRI compatibility, and algorithms for minimization of right ventricular stimulation. The higher preference for fewer infections is further supported by the established association between infections and increased morbidity and mortality.62
The risk of infection may be influenced by several elements, including technical factors (generator size, number of interventions), patient factors (comorbidities like diabetes mellitus, heart failure, chronic kidney disease, and other transient conditions), periprocedural factors, and the implantation approach.63–65 LLPMs have a lower infection rate than conventional PMs, mainly due to the absence of a subcutaneous pocket and leads and reduced skin and glove contact, as well as differences in size, external self-perception, and device material.65
These preferences are consistent with current trends in pacing strategies, which increasingly favor dual-chamber systems and physiologic pacing approaches. Recent evidence indicates that dual-chamber pacing is associated with improved myocardial performance and better clinical outcomes compared with single-chamber pacing, and that conduction system pacing, including left bundle branch pacing, provides significant clinical and long term benefits and is increasingly considered part of standard of care.66,67
Cardiologists’ preferences for CSP aligns with its proven general feasibility and safety,68–74 along with its advantages such as reduced interventricular dyssynchrony, preventing PM-induced cardiomyopathy,75 and its safety in patients with cardiac amyloidosis.76 Algorithms to minimize right ventricular pacing can reduce the risk of permanent atrial fibrillation and cardiovascular hospitalization in patients requiring anti-bradycardia therapies, without an increased risk of adverse symptoms.77 Different algorithms, such as the Ventricular Pace Suppression algorithm and the Intrinsic Rhythm Support plus algorithm, have proven to be safe and effective in reducing unnecessary ventricular pacing in patients with symptomatic sinus node dysfunction.78 These considerations support the significant value placed by cardiologists on the algorithms to reduce unnecessary right ventricular pacing.
Our findings are partially consistent with previous preference studies,48 evaluating patient preferences for features associated with leadless versus conventional transvenous pacemakers. While prior studies have highlighted the relevance of leadless systems from the patient perspective, particularly in relation to perceived safety and comfort, our results suggest that both patients and cardiologists place greater emphasis on specific device outcomes and characteristics-such as MRI compatibility, battery longevity, and infection risk-rather than on device type alone. Differences across studies may be related to variations in study design, healthcare setting, and population characteristics. Nevertheless, the consistent prioritization of safety- and outcome-related attributes across studies suggests the presence of common perceptions that transcend individual healthcare systems.
Importantly, although leadless pacemakers are associated with lower infection rates,79 cardiologists did not prioritize the device type (leadless vs conventional) as an isolated attribute. This finding likely reflects the fact that clinicians prioritize infection risk as a clinical outcome rather than as a surrogate for a specific device category. In routine practice, infection risk is multifactorial and influenced not only by lead presence, but also by patient comorbidities, implantation technique, procedural volume, and follow-up strategies. Consequently, cardiologists may focus on minimizing infection risk regardless of the pacing technology used, which may explain this apparent discrepancy.
Additionally, having access to all programming modes could be highly beneficial for patients in specific situations, such as during cardiac rehabilitation programs involving physical exercise. For example, the rate responsive function (RRF) of the PM programming mode plays a crucial role in patients’ exercise capacity, as patients with RRF activated demonstrated superior functional capacity.80
Study Limitations
This study has limitations, some of which are inherent to its design. Although the DCE is the recommended method for assessing the preferences of patients and healthcare professionals for the characteristics of a treatment or medical device, there is always a risk of a mismatch between the stated and revealed preferences,34,81 and therefore the choices made by patients or cardiologists in real life may differ from those made in the DCE. Furthermore, although the use of self-administered electronic questionnaires ensures that the sample number required to respond to the main study objective is reached, the accuracy of the data provided by the participants cannot be verified.82 In addition, this methodology has an inherent selection bias caused by the fact that the answers will only be provided by those patients and cardiologists willing to participate in the study, whose opinions could differ from those who refuse to participate.82 Limitations may also arise in the selection of attributes and/or levels; the DCE may not include potentially relevant attributes, or the selection of levels within an attribute may not be appropriate. To minimize this potential bias, the SC members and patient focus group reviewed and verified the relevance of the attributes and levels included in the DCE. Finally, this study was conducted exclusively in Spain within the context of the Spanish public healthcare system. As healthcare organization, clinical practice patterns, and cultural factors may influence preferences, the generalizability of these findings to other countries and healthcare settings may be limited.
Conclusion
The information provided by this study enables the identification and quantification of patients’ and cardiologists’ preferences for the characteristics of PMs. For both groups, MRI compatibility and battery longevity emerged as key drivers in the decision-making process. Additionally, patients attach relevance to other aspects such as the generator size and its replacement process. In contrast, cardiologists place significant importance on aspects related to the type of follow-up and other safety and technical considerations such as the 12-month post-implantation infection rate, conduction system pacing, and algorithms to reduce unnecessary ventricular stimulation.
Considering the broad range of PMs currently available, information on patients’ and cardiologists’ preferences may promote and facilitate shared decision-making. Moreover, this knowledge may guide the development of new devices that reflect these preferences, ensuring that innovations meet the needs and expectations of both patients and cardiologists.
Acknowledgments
The authors would like to thank all the patients and healthcare professionals who participated in this study for their valuable time and contribution.
Funding
This project was funded by Medtronic Ibérica S.A.
Disclosure
F.J.G.F. reports that the study was supported by Medtronic, with no personal payments received, and has received consulting fees from Medtronic and Boston Scientific, as well as honoraria from Biotronik.M.L.F.A. and F.R.M. report that the study was supported by Medtronic, with no direct payment received, and have received consulting fees from Medtronic. M.C. and E.V.D. report that the study was supported by Medtronic Ibérica S.A. through a contract with Outcomes’10, their employing institution, which also received consulting fees from Medtronic for services related to the study. M.A.O. is a full-time employee of Medtronic Ibérica S.A. The authors report no other conflicts of interest in this work.
References
1. Roth GA, Johnson C, Abajobir A, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70(1):1–14. doi:10.1016/j.jacc.2017.04.052
2. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
3. Desai DS, Hajouli S. Arrhythmias. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025.
4. Chaudhary MH, Dev S, Kumari A, et al. Holistic approaches to arrhythmia management: combining medication, ablation, and device interventions. Cureus. 2023;15(9):e45958. doi:10.7759/cureus.45958
5. Nagpal AK, Pundkar A, Singh A, et al. Cardiac arrhythmias and their management: an in-depth review of current practices and emerging therapies. Cureus. 2024;16(8):e66549.
6. Defaye P, Biffi M, El-Chami M, et al. Cardiac pacing and lead devices management: 25 years of research at EP Europace journal. Europace. 2023;25(8). doi:10.1093/europace/euad202
7. Cosgun MS, Cosgun C. Predictors of shoulder limitations and disability in patients with cardiac implantable electronic devices: importance of device size. Pacing Clin Electrophysiol. 2021;44(12):1979–1986. doi:10.1111/pace.14378
8. Timmis A, Aboyans V, Vardas P, et al. European society of cardiology: the 2023 atlas of cardiovascular disease statistics. Eur Heart J. 2024;45(38):4019–4062. doi:10.1093/eurheartj/ehae466
9. Molina-Lerma M, Cózar-León R, García-Fernández FJ, et al. Spanish pacemaker registry. 21st official report of heart rhythm association of the spanish society of cardiology (2023). Rev Esp Cardiol. 2024;77(11):947–956. doi:10.1016/j.recesp.2024.07.010
10. Agarwal S, Shinde RK. Smart pacemaker: a review. Cureus. 2022;14(10):e30027. doi:10.7759/cureus.30027
11. Piemontese GP, Toniolo S, Biffi M, et al. Bridging the future of cardiac stimulation: physiologic or leadless pacing? Rev Cardiovasc Med. 2022;23(3):107. doi:10.31083/j.rcm2303107
12. Sperzel J, Hamm C, Hain A. Nanostim-leadless pacemaker. Herzschrittmacherther Elektrophysiol. 2018;29(4):327–333. doi:10.1007/s00399-018-0598-3
13. Cohen MI, Thurber C. The history of cardiac pacing in the young and a look to the future. Curr Opin Pediatr. 2022;34(5):476–483. doi:10.1097/MOP.0000000000001160
14. Della Rocca DG, Gianni C, Di Biase L, et al. Leadless pacemakers: state of the art and future perspectives. Card Electrophysiol Clin. 2018;10(1):17–29. doi:10.1016/j.ccep.2017.11.003
15. El-Chami MF, Bockstedt L, Longacre C, et al. Leadless vs. transvenous single-chamber ventricular pacing in the Micra CED study: 2-year follow-up. Eur Heart J. 2022;43(12):1207–1215. doi:10.1093/eurheartj/ehab767
16. Crossley GH, Piccini JP, Longacre C, et al. Leadless versus transvenous single-chamber ventricular pacemakers: 3 year follow-up of the micra CED study. J Cardiovasc Electrophysiol. 2023;34(4):1015–1023. doi:10.1111/jce.15863
17. El-Chami MF, Higuera L, Longacre C, et al. Two-year outcomes of micra AV leadless pacemakers in the micra AV CED study. Europace. 2024;26(11):euae273. doi:10.1093/europace/euae273
18. Crossley GH, Longacre C, Higuera L, et al. Outcomes of patients implanted with an atrioventricular synchronous leadless ventricular pacemaker in the medicare population. Heart Rhythm. 2024;21(1):66–73. doi:10.1016/j.hrthm.2023.09.017
19. El-Chami MF, Clementy N, Garweg C, et al. Leadless pacemaker implantation in hemodialysis patients: experience with the micra transcatheter pacemaker. JACC Clin Electrophysiol. 2019;5(2):162–170. doi:10.1016/j.jacep.2018.12.008
20. Lancellotti P, Gach O, Marechal P, et al. Micra® leadless pacemaker. Rev Med Liege. 2019;74(S1):S104–s8.
21. Limite LR, Baratto F, Mantica M, et al. Leadless pacemakers: results of a survey from implanter centers in the Lombardy region. G Ital Cardiol. 2022;23(2):120–127. doi:10.1714/3735.37214
22. Martínez-Sande JL, García-Seara J, Rodríguez-Mañero M, et al. The micra leadless transcatheter pacemaker. implantation and mid-term follow-up results in a single center. Rev Esp Cardiol. 2017;70(4):275–281. doi:10.1016/j.recesp.2016.09.011
23. Reynolds D, Duray GZ, Omar R, et al. A leadless intracardiac transcatheter pacing system. N Engl J Med. 2016;374(6):533–541. doi:10.1056/NEJMoa1511643
24. Boveda S, Higuera L, Longacre C, et al. Two-year outcomes of leadless vs. transvenous single-chamber ventricular pacemaker in high-risk subgroups. Europace. 2023;25(3):1041–1050. doi:10.1093/europace/euad016
25. Modi Atig A, Alhamad YI, Alanizi FS, et al. Retrospective study of post-operative infections in implantable cardiac devices in a cardiac tertiary care center. Ann Saudi Med. 2022;42(1):58–63. doi:10.5144/0256-4947.2022.58
26. Barry MJ, Edgman-Levitan S. Shared decision making--pinnacle of patient-centered care. N Engl J Med. 2012;366(9):780–781. doi:10.1056/NEJMp1109283
27. Charles C, Gafni A, Whelan T. Decision-making in the physician-patient encounter: revisiting the shared treatment decision-making model. Soc Sci Med. 1999;49(5):651–661.
28. Centers for Medicare and Medicaid Services. Decision memo for implantable cardioverter defibrillators (CAG‐00157R4). Available from: https://www.cms.gov/medicare-coverage-database/details/nca-decision-memo.aspx?NCAId=288.
29. Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: executive summary: a report of the American college of cardiology/American heart association task force on clinical practice guidelines and the heart rhythm society. Heart Rhythm. 2018;15(10):e190–e252. doi:10.1016/j.hrthm.2017.10.035
30. Glikson M, Nielsen JC, Kronborg MB, et al. 2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy: developed by the task force on cardiac pacing and cardiac resynchronization therapy of the European society of cardiology (ESC) with the special contribution of the European heart rhythm association (EHRA). Rev Esp Cardiol. 2022;75(5):430. doi:10.1016/j.rec.2022.04.004
31. de Bekker-Grob EW, Donkers B, Jonker MF, et al. Sample size requirements for discrete-choice experiments in healthcare: a practical guide. Patient. 2015;8(5):373–384. doi:10.1007/s40271-015-0118-z
32. Johnson R, Orme B. Getting the most from CBC: Sequim: Sawtooth Software Research Paper Series, Sawtooth Software; 2003.
33. Orme B. Sample size issues for conjoint analysis. In: Wis M, editor. Getting Started with Conjoint Analysis: Strategies for Product Design and Pricing Researc.
34. Bridges JF, Hauber AB, Marshall D, et al. Conjoint analysis applications in health--a checklist: a report of the ISPOR good research practices for conjoint analysis task force. Value Health. 2011;14(4):403–413. doi:10.1016/j.jval.2010.11.013
35. Cochran WG. Sampling Techniques.
36. Shanahan M, Larance B, Nielsen S, et al. A protocol for a discrete choice experiment: understanding patient medicine preferences for managing chronic non-cancer pain. BMJ Open. 2019;9(8):e027153. doi:10.1136/bmjopen-2018-027153
37. Hincapie AL, Penm J, Burns CF. Factors associated with patient preferences for disease-modifying therapies in multiple sclerosis. J Manag Care Spec Pharm. 2017;23(8):822–830. doi:10.18553/jmcp.2017.23.8.822
38. Reed Johnson F, Lancsar E, Marshall D, et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR conjoint analysis experimental design good research practices task force. Value Health. 2013;16(1):3–13. doi:10.1016/j.jval.2012.08.2223
39. Benning TM, Kimman ML, Dirksen CD, et al. Combining individual-level discrete choice experiment estimates and costs to inform health care management decisions about customized care: the case of follow-up strategies after breast cancer treatment. Value Health. 2012;15(5):680–689. doi:10.1016/j.jval.2012.04.007
40. Train K. Discrete Choice Methods with Simulation. Cambridge University Press; 2022.
41. Mangham LJ, Hanson K, McPake B. How to do (or not to do). Designing a discrete choice experiment for application in a low-income country. Health Policy Plan. 2009;24(2):151–158. doi:10.1093/heapol/czn047
42. Trapero-Bertran M, Rodríguez-Martín B, López-Bastida J. What attributes should be included in a discrete choice experiment related to health technologies? A systematic literature review. PLoS One. 2019;14(7):e0219905. doi:10.1371/journal.pone.0219905
43. Naraparaju V, Almnajam M, Joseph L, et al. A survey on patient preferences towards CIED implantation. Indian Pacing Electrophysiol J. 2021;21(4):227–231. doi:10.1016/j.ipej.2021.04.004
44. Fraiche AM, Matlock DD, Gabriel W, et al. Patient and provider perspectives on remote monitoring of pacemakers and implantable cardioverter-defibrillators. Am J Cardiol. 2021;149:42–46. doi:10.1016/j.amjcard.2021.03.023
45. Shurlock J, Brown S, Dayer M, et al. Rapid roll out of a pacemaker home monitoring programme: a patient perspective. Heart Lung Circ. 2023;32(6):726–734. doi:10.1016/j.hlc.2023.03.015
46. Portig I, Karaaslan E, Hofacker E, et al. Patients’ perspective on termination of pacemaker therapy-A cross-sectional anonymous survey among patients carrying a pacemaker in Germany. Healthcare. 2023;11(21). doi:10.3390/healthcare11212896
47. Portig I, Hofacker E, Sommer P, et al. Cardiologists’ perspective on termination of pacemaker therapy-an anonymous survey among cardiologists in Germany. Clin Res Cardiol. 2024. doi:10.1007/s00392-024-02525-z
48. Reed SD, Yang JC, Wallace MJ, et al. Patient preferences for features associated with leadless versus conventional transvenous cardiac pacemakers. Circ Cardiovasc Qual Outcomes. 2024;17(12):e011168. doi:10.1161/CIRCOUTCOMES.124.011168
49. Gillam MH, Inacio MCS, Pratt NL, et al. Magnetic resonance imaging in people with cardiac implantable electronic devices: a population based cohort study. Heart Lung Circ. 2018;27(6):748–751. doi:10.1016/j.hlc.2017.09.004
50. Minaskeian N, Hajnal SP, Liu MB, et al. Safety of magnetic resonance imaging in patients with cardiac implantable electronic devices with generator and lead(s) brand mismatch. J Appl Clin Med Phys. 2022;23(3):e13520. doi:10.1002/acm2.13520
51. Rowe MK, Shanahan L. Cardiac implantable electronic devices: an update. Aust J Gen Pract. 2024;53(7):430–435. doi:10.31128/AJGP-05-23-6847
52. Sugiharto F, Asmara AD, Sari WP, et al. Types of complications and associated factors in patients undergoing permanent cardiac pacemaker implantation: a systematic review. J Multidiscip Healthc. 2025;18:83–100. doi:10.2147/JMDH.S489600
53. Markos S, Nasir M, Ahmed M, et al. Assessment of trend, indication, complications, and outcomes of pacemaker implantation in adult patients at tertiary hospital of Ethiopia: retrospective follow up study. Int J Gen Med. 2024;17:93–103. doi:10.2147/IJGM.S448135
54. Nasir M, Dejene K, Bedru M, et al. Predictors of complications and mortality among patients undergoing pacemaker implantation in resource-limited settings: a 10-year retrospective follow-up study. BMC Cardiovasc Disord. 2024;24(1):400. doi:10.1186/s12872-024-04068-7
55. Carretta DM, Tomasi L, Tondo C, et al. Leadless micra pacemakers: estimating long-term longevity. A real word data analysis. Int J Cardiol. 2025;426:133062. doi:10.1016/j.ijcard.2025.133062
56. Lopez-Villegas A, Leal-Costa C, Perez-Heredia M, et al. Knowledge update on the economic evaluation of pacemaker telemonitoring systems. Int J Environ Res Public Health. 2021;18(22):12120. doi:10.3390/ijerph182212120
57. Piccini JP, Mittal S, Snell J, et al. Impact of remote monitoring on clinical events and associated health care utilization: a nationwide assessment. Heart Rhythm. 2016;13(12):2279–2286. doi:10.1016/j.hrthm.2016.08.024
58. Ricci RP, Morichelli L, D’Onofrio A, et al. Manpower and outpatient clinic workload for remote monitoring of patients with cardiac implantable electronic devices: data from the HomeGuide Registry. J Cardiovasc Electrophysiol. 2014;25(11):1216–1223. doi:10.1111/jce.12482
59. García-Fernández FJ, Osca Asensi J, Romero R, et al. Safety and efficiency of a common and simplified protocol for pacemaker and defibrillator surveillance based on remote monitoring only: a long-term randomized trial (RM-ALONE). Eur Heart J. 2019;40(23):1837–1846. doi:10.1093/eurheartj/ehz067
60. Varma N, Piccini JP, Snell J, et al. The relationship between level of adherence to automatic wireless remote monitoring and survival in pacemaker and defibrillator patients. J Am Coll Cardiol. 2015;65(24):2601–2610. doi:10.1016/j.jacc.2015.04.033
61. Cingolani E, Goldhaber JI, Marbán E. Next-generation pacemakers: from small devices to biological pacemakers. Nat Rev Cardiol. 2018;15(3):139–150. doi:10.1038/nrcardio.2017.165
62. Modi V, Shah K, Ferraro B, et al. Cardiac implantable electronic device implantation and device-related infection. Europace. 2023;25(9). doi:10.1093/europace/euad208
63. Bielick CG, Arnold CJ, Chu VH. Cardiovascular implantable electronic device infections: a contemporary review. Infect Dis Clin North Am. 2024;38(4):673–691. doi:10.1016/j.idc.2024.07.004
64. Han HC, Hawkins NM, Pearman CM, et al. Epidemiology of cardiac implantable electronic device infections: incidence and risk factors. Europace. 2021;23(23 Suppl 4):iv3–iv10. doi:10.1093/europace/euab042
65. El-Chami MF, Bonner M, Holbrook R, et al. Leadless pacemakers reduce risk of device-related infection: review of the potential mechanisms. Heart Rhythm. 2020;17(8):1393–1397. doi:10.1016/j.hrthm.2020.03.019
66. Mohan B, Batta A. Dual-chamber pacing confers better myocardial performance and improves clinical outcomes compared to single-chamber pacing. World J Cardiol. 2024;16(11):626–631. doi:10.4330/wjc.v16.i11.626
67. Batta A, Hatwal J. Left bundle branch pacing set to outshine biventricular pacing for cardiac resynchronization therapy? World J Cardiol. 2024;16(4):186–190. doi:10.4330/wjc.v16.i4.186
68. Keene D, Arnold AD, Jastrzębski M, et al. His bundle pacing, learning curve, procedure characteristics, safety, and feasibility: insights from a large international observational study. J Cardiovasc Electrophysiol. 2019;30(10):1984–1993. doi:10.1111/jce.14064
69. Padala SK, Master VM, Terricabras M, et al. Initial experience, safety, and feasibility of left bundle branch area pacing: a multicenter prospective study. JACC Clin Electrophysiol. 2020;6(14):1773–1782. doi:10.1016/j.jacep.2020.07.004
70. Saleiro C, Sousa PA, Nogueira C, et al. His bundle pacing and left bundle branch area pacing: feasibility and safety. Rev Port Cardiol. 2023;42(8):683–691. doi:10.1016/j.repc.2022.10.013
71. Sharma PS, Dandamudi G, Naperkowski A, et al. Permanent His-bundle pacing is feasible, safe, and superior to right ventricular pacing in routine clinical practice. Heart Rhythm. 2015;12(2):305–312. doi:10.1016/j.hrthm.2014.10.021
72. Su L, Wang S, Wu S, et al. Long-term safety and feasibility of left bundle branch pacing in a large single-center study. Circ Arrhythm Electrophysiol. 2021;14(2):e009261. doi:10.1161/CIRCEP.120.009261
73. Vijayaraman P, Subzposh FA, Naperkowski A, et al. Prospective evaluation of feasibility and electrophysiologic and echocardiographic characteristics of left bundle branch area pacing. Heart Rhythm. 2019;16(12):1774–1782. doi:10.1016/j.hrthm.2019.05.011
74. Zanon F, Ellenbogen KA, Dandamudi G, et al. Permanent His-bundle pacing: a systematic literature review and meta-analysis. Europace. 2018;20(11):1819–1826. doi:10.1093/europace/euy058
75. Tokavanich N, Prasitlumkum N, Mongkonsritragoon W, et al. A network meta-analysis and systematic review of change in QRS duration after left bundle branch pacing, His bundle pacing, biventricular pacing, or right ventricular pacing in patients requiring permanent pacemaker. Sci Rep. 2021;11(1):12200. doi:10.1038/s41598-021-91610-8
76. Pham-Trung C, Veloza-Urrea D, Segura-Domínguez M, et al. Feasibility and safety of left bundle branch area pacing in cardiac amyloidosis. A single center experience. Pacing Clin Electrophysiol. 2024;47(1):149–155. doi:10.1111/pace.14894
77. Mei DA, Imberti JF, Vitolo M, et al. Systematic review and meta-analysis on the impact on outcomes of device algorithms for minimizing right ventricular pacing. Europace. 2024;26(8). doi:10.1093/europace/euae212
78. Hwang J, Han S, Park HS, et al. Evaluation of ventricular pacing suppression algorithms in dual chamber pacemaker: results of “LEADER” study. J Arrhythm. 2024;40(4):965–974. doi:10.1002/joa3.13117
79. Oliveira VMR, Rivera A, Oliveira IC, et al. The effectiveness and safety of leadless pacemakers: an updated meta-analysis. Current Cardiology Reports. 2024;26(8):789–799. doi:10.1007/s11886-024-02079-6
80. Caloian B, Sitar-Taut AV, Gusetu GN, et al. The influence of cardiac pacemaker programming modes on exercise capacity. Vivo. 2018;32(2):419–424.
81. Viney R, Lancsar E, Louviere J. Discrete choice experiments to measure consumer preferences for health and healthcare. Expert Rev Pharmacoecon Outcomes Res. 2002;2(4):319–326. doi:10.1586/14737167.2.4.319
82. Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. PLoS Med. 2007;4(10):e297. doi:10.1371/journal.pmed.0040297
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Preferences in the Design and Delivery of Neurodevelopmental Follow-Up Care for Children: A Systematic Review of Discrete Choice Experiments
Sharma P, Kularatna S, Abell B, Eagleson K, Vo LK, Halahakone U, Senanayake S, McPhail SM
Patient Preference and Adherence 2023, 17:2325-2341
Published Date: 19 September 2023
Medical Personnel Behavior Preferences for Providing mHealth Service in China: A Discrete Choice Experiment
Jiang S, Xiong M, Rao X, Liang J, Zhu X, Fu H, Chen J, Wang C
Risk Management and Healthcare Policy 2023, 16:2405-2418
Published Date: 10 November 2023
Preferences for Physical Examination Service in Community Health Service Center in China: A Discrete Choice Experiment
Sun H, Li F, Xu Y, Qi Q, Du Y
Patient Preference and Adherence 2024, 18:39-51
Published Date: 6 January 2024
Patients’ and Relatives’ Preferences for Outpatient and Day Care Services Within End-of-Life Care in Germany – A Discrete Choice Experiment
Apolinarski B, de Jong L, Herbst FA, Huperz C, Röwer HAA, Schneider N, Damm K, Stiel S
Patient Preference and Adherence 2024, 18:519-529
Published Date: 29 February 2024
An Empirical Comparison of Discrete Choice Experiment and Best-Worst Scaling to Estimate Patient Preferences in Infertility Treatment in China
Chen J, Qian X, Su D, Gong J, Shang J, Zhang L, Li X
Patient Preference and Adherence 2025, 19:869-882
Published Date: 30 March 2025