Back to Journals » Patient Preference and Adherence » Volume 19
Preferences for Non-Pharmacological Traditional Chinese Medicine in Cancer Care: A Mixed-Methods Systematic Review
Authors Chen YX ![]() , Zhou Y
, Zhou Y ![]() , Zhang XL, He WY, Ye Q, Xu M
, Zhang XL, He WY, Ye Q, Xu M ![]()
Received 16 September 2025
Accepted for publication 4 December 2025
Published 16 December 2025 Volume 2025:19 Pages 4091—4105
DOI https://doi.org/10.2147/PPA.S567999
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Ying-Xiang Chen,1,* You Zhou,1,* Xiao-Lan Zhang,1 Wen-Yan He,2 Qin Ye,1 Min Xu1
1Department of Nursing, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, Zhejiang, People’s Republic of China; 2Oncology Department, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Min Xu, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), No. 54, Post Road, Shangcheng District, Hangzhou, People’s Republic of China, Email [email protected]
Background: Non-pharmacological therapies in traditional Chinese medicine (TCM) are gradually gaining popularity. However, there has been no systematic understanding about cancer patients’ preferences regarding these treatments.
Objective: This review aims to clarify cancer patients’ preferences for these therapies and the factors influencing them through systematic integration of evidence.
Methods: A systematic search was conducted among eight databases. The time period spanned from the inception of each database to April 7, 2025. The Mixed Methods Assessment Tool was employed to assess the quality of the studies that met inclusion criteria. The JBI Convergent Synthesis Method was used to transform the extracted quantitative data into qualitative data that was then synthesized with qualitative data. A socio-ecological model was applied to group factors that influence TCM choices.
Results: A total of 27 studies were included in this review, consisting of 13 quantitative and 14 qualitative studies. The factors that might affect cancer patients’ preferences in favor of TCM non-pharmacological therapies are multifaceted, covering every level that exists within the socio-ecological model, including the individual (belief and past experiences), interpersonal (professional recommendations and family), healthcare system (service accessibility and cost), society (cultural origins and resources), and governmental (insurance and standards). The PROSPERO registration was dated April 6, 2025 (Registration Number: CRD420251026914).
Conclusion: Patients’ preference for TCM non-pharmacological therapies is driven by cultural affinity and interpersonal care needs rather than objective clinical evidence. This reminds us that while respecting patient preferences is essential for achieving patient-centered care, we must also adhere to evidence-based science to ensure safety and effectiveness. Future research should prioritize non-pharmacological therapies other than acupuncture (eg, massage, qigong) to bridge the evidence gap regarding their safety and efficacy. One limitation of this review lies in the overemphasis on acupuncture among cited studies and the cultural homogeneity.
Keywords: cancer, traditional chinese medicine, non-pharmacological therapies, preferences, influencing factors, mixed-methods study, systematic review
Introduction
Cancer has become a major health issue that demands international attention due to a growing incidence and death rate. Though there has been tremendous progress in the treatment of cancer due to modern medicine, the side-effects of such treatments tend to produce adverse results in terms of the physical and psychological well-being of the patients.1 Therefore, cancer patients urgently seek strategies beyond extending survival to alleviate symptoms and enhance overall well-being.2
In this context, there has been a growing trend among people to use Complementary and Alternative Medicine (CAM). The average use rate among patients with cancer has been found to be 35.9%.3,4 Within these groups, Non-Pharmacologic Therapies derived from Traditional Chinese Medicine (TCM), such as acupuncture, moxibustion, tuina, cupping, and dietary therapy, have recently gained widespread research interest.5 Recent evidence6–9 has suggested that these treatments possess potential as adjuvants to improve mood and alleviate side effects to improve quality of life.10,11 Not surprisingly, with these treatments increasingly brought within mainstream oncology practices, cancer patients are increasingly choosing them.
Modern medicine promotes patient-centered practices that mandate consideration of patients’ values, preferences, and needs in all medical choices. This addresses significant needs in improving adherence to treatments, patient satisfaction, and ultimately outcomes.12,13 Yet, with the present trend on the non-pharmacologic application of TCM treatments, there is still a lack of systematic insight into patient preferences and factors that specifically impact decisions. Clearly there are still significant research gaps in the current evidence base. First, most research has focused on single therapies such as acupuncture, while little is known about patients’ preferences, acceptance, and influencing factors regarding other common therapies like massage, dietary therapy, and qigong.14,15 Second, existing studies employ relatively limited methodologies, predominantly quantitative cross-sectional surveys16,17 or qualitative in-depth interviews.18–20 Quantitative studies help reveal prevalence rates and associated factors of preferences but struggle to delve into the complex motivations and personal experiences driving these preferences. Conversely, while qualitative studies offer rich, in-depth insights, their findings have limited generalizability. Therefore, to comprehensively integrate the strengths of both types of evidence, there is an urgent need for mixed methods systematic reviews (MMSRs).21,22
To systematically analyze these complex influencing factors, this review adopted the Socio-ecological Model as its theoretical framework.23 The socio-ecological model combines levels such as the individual level, interpersonal level, healthcare system level, social level, and the policy level to form an integral understanding about how these preferences are shaped. To our knowledge, while existing systematic reviews have examined TCM efficacy or utilization rates, there remains a lack of MMSRs systematically synthesizing cancer patients’ preferences for TCM non-pharmacological therapies and their influencing factors. Therefore, this review aims to comprehensively analyze quantitative and qualitative evidence in this field through MMSRs, utilizing the socio-ecological model to construct an integrated analytical framework and fill this research gap.
Methods
Study Design
This review utilizes the Joanna Briggs Institute (JBI) mixed methods systematic reviews reporting specifications for reporting. This systematic review was registered with PROSPERO on April 2025 (CRD420251026914) and reported under the PRISMA 2020 statement.
Search Strategy
A search strategy employing the expertise of a librarian in systematic reviewing helped in planning the search. The search included a total of eight databases, PubMed, CINAHL, Embase, ProQuest, PsycINFO, Web of Science, Wan Fang Data, and China National Knowledge Infrastructure. The search dates ranged from the database inception to the final search date of April 7, 2025.
The search strategy consisted of three main concepts: (1) cancer patients, (2) non-pharmacological therapies in TCM, and (3) patient preferences. For all concepts, a combination of subject headings as well as free-text terms was used. Therapy-related terms were also used in relation to therapy in order to include concepts such as acupuncture, moxibustion, tuina massage, cupping, qigong, as well as dietary therapy. The search terms were designed for PubMed at first, but later adjusted for syntax as well as subject headings of other search databases. The full search strategy for PubMed as well as other search databases is presented in Supplementary 1. Detailed Search Strategy. In an attempt to include even more studies which could be of potential interest, we manually reviewed for possible inclusion as references all articles which met inclusion criteria as well as systematic reviews in our searches.
Inclusion and Exclusion Criteria
As this review focuses on exploring patient preferences rather than comparing the effectiveness of interventions, we used the Population, Phenomenon of Interest, and Context (PICo) framework to define the eligibility criteria.
Studies were included if they met the following criteria. The population (P) consisted of patients of any age diagnosed with any type or stage of cancer. The phenomenon of interest (I) was the preferences, attitudes, choices, utilization, acceptance, willingness, and influencing factors related to TCM non-pharmacological therapies. For this review, TCM non-pharmacological therapies were defined as interventions rooted in TCM theory that do not involve the ingestion of substances, such as acupuncture, acupressure, moxibustion, cupping, tuina (massage), dietary therapy (as a guided intervention), and mind-body practices like Qigong and Tai Chi. Patient preference is a qualitative or quantitative assessment of the relative desirability or acceptability of a particular alternative or choice.21 The context (Co) included any clinical or community setting in any country where cancer treatment, rehabilitation, or symptom management occurs. All quantitative, qualitative, and mixed-methods study designs were eligible.
Studies were excluded if they: (1) focused exclusively on pharmacological TCM therapies (eg, herbal medicine); (2) only evaluated the clinical effectiveness of a therapy without addressing patient preferences or influencing factors; (3) were not published in English or Chinese; (4) were duplicate publications; or (5) had unavailable full texts or incomplete data from which key information could not be extracted.
Study Selection
All retrieved records were imported into EndNote X9 for duplicate removal. Subsequently, two reviewers (YXC and YZ) independently screened the titles and abstracts of the remaining records against the eligibility criteria. The full texts of potentially relevant articles were then retrieved for a second-stage screening, which was also conducted independently by the same two reviewers. Any disagreements at either stage were resolved through discussion and consensus, with a third reviewer (MX) acting as an arbiter if needed.
Assessment of Methodological Quality
A Mixed Methods Appraisal Tool (MMAT) was used to determine the quality of incorporated quantitative, qualitative, and mixed studies. The criteria for evaluating quantitative, qualitative, and mixed studies included five statements, which needed to be answered in either “yes,” “no,” or “unclear.” Prior to using the criteria of the MMAT, two screening questions needed to be answered, and only after responding affirmatively could further review of certain criteria be undertaken, which depended upon their study type.24 Scores are represented as a percentage. Two researchers independently assessed the quality of the included literature based on the MMAT evaluation criteria, and in cases of disagreement, a consensus was achieved through discussion with a third member of the subject group.
Data Extraction
The data extraction portion adhered rigorously to the standardized process established by the Joanna Briggs Institute for the extraction of both quantitative and qualitative data. The JBI standard data extraction procedure to obtain quantitative and qualitative data.25 Extracts comprised the author, country, year, phenomenon of interest, study population, study design type, and factors affecting patient preference. For mixed-methods studies, we extracted data to classify them as quantitative or qualitative.
Data Transformation
Extracts comprised the author, country, year, phenomenon of interest, study population, study design type, and factors affecting patient preference. For mixed-methods studies, we extracted data to classify them as quantitative or qualitative.25 Therefore, after extraction, quantitative information from quantitative studies is converted into qualitative information such as themes, categories, or descriptions. For example, when investigating whether perceived need affects Chinese cancer survivors’ willingness to use TCM for survivorship care,26 higher levels of perceived need (OR: 1.33, 95% CI: 1.14–1.56), especially in the domains of nutrition and symptoms, were positively associated with a greater willingness to use TCM techniques for survivorship care. Translated into qualitative information, “High levels of perceived need were a facilitator of the use of TCM techniques for survival care.”
Data Synthesis and Integration
Analysis and integration were conducted following the convergent integration technique as advised by the JBI Center for Evidence-Based Health Care Mixed-Methods Systems Evaluation Guide in three stages: (1) Two researchers independently extracted both quantitative and qualitative data. (2) They qualitatively transformed the extracted quantitative data. (3) They integrated the qualitative results derived from the quantitative data with the qualitative data obtained from the qualitative study, coded the data according to pertinent themes, and synthesized, discussed, and revised iteratively with subject matter experts to ensure that the themes accurately represent the findings of the information.
Based on the Social Ecological Model,23 we categorized the factors affecting individual preference behavior into five levels, arranged from proximal to distal: individual level, interpersonal level, healthcare system level, societal level, and public policy level. Materials were classified and consolidated based on these five kinds of criteria.
Findings
Study Inclusion Criteria
The initial database search yielded a total of 3026 records. After removing 1,065 duplicates, 1,961 records remained for title and abstract screening. During this stage, 1,705 records were excluded as they were clearly irrelevant to the research topic. This left 256 articles for full-text review. In addition, 12 records were identified through citation searching. Of the 268 reports sought for retrieval, 19 could not be retrieved. The remaining 249 full-text articles were assessed for eligibility. From these, 222 were excluded for various reasons, with the most common being that they did not address patient preferences or influencing factors (n=155). Ultimately, 27 studies met all inclusion criteria and were included in the systematic review. The detailed process of study selection is illustrated in the PRISMA 2020 flow diagram (Figure 1).
 |
Figure 1 PRISMA flowchart. |
Methodological Quality
All of the 27 included studies passed the screening process using the MMAT quality appraisal tool. For the quality of the 14 included qualitative studies, in general, they appeared to be of good quality. A total of 13 of the studies received a rating of yes for all of the quality criteria. Only one study27 received a rating of no for criteria 1.4 (support for interpretation of results by data) and criteria 1.5 (lack of consistency between data, analysis, and results). For the remaining 13 quantitative studies, in general, they appeared to vary in terms of methodology, including poor methodology. The most common problems occurred in criterion 3.1 (representative sample), where a total of 8studies (61.5%) received a rating of no, signifying that they did not have a representative sample of their target population. The secondary issue is where criterion 3.5 (whether interventions were implemented as intended) also received an unclear rating for a total of 8 studies (61.5%). Only three of the quantitative studies28–30 received a rating of yes for all criteria. The quality scores for inclusion in this review ranged from a total of 40% to a total of 100%. Nonetheless, none of the studies for this review shall be eliminated to be more comprehensive of all information yielded by this review. Quality Assessment of Qualitative research and Quantitative research is in Supplementary 3.1 and 3.2.
Characteristics of the Included Studies
This systematic review encompassed 27 studies.14–20,26–45 The research was published from 2007 to 2024 and originated from seven nations. The predominant cancer type was breast cancer, supplemented by various tumor types, including lung cancer and hematological malignancies. Fourteen studies19,20,27,31–35,37,39,41,42,44,45 analyzed qualitative content from four countries, with China having the highest number of publications (n=8).19,20,27,31,32,35,37,45 Research methods included 10 qualitative descriptive studies,27,31–34,37,39,41,44,45 2 phenomenological studies,19,20 and 2 grounded theory studies.35,42 Thirteen studies14–18,26,28–30,36,38,40,43 analyzed quantitative content from five countries, with most originating from the United States (n=4)14,16,17,28 and China (n=5).15,18,26,38,43 These comprised 12 cross-sectional studies15–18,26,28–30,36,38,40,43 and one longitudinal study.14 The phenomena examined primarily included patient preferences, usage, attitudes, acceptance, willingness to use, and influencing factors related to non-pharmacological TCM therapies, particularly acupuncture. The key characteristics of these studies are summarized in Tables 1 and 2.
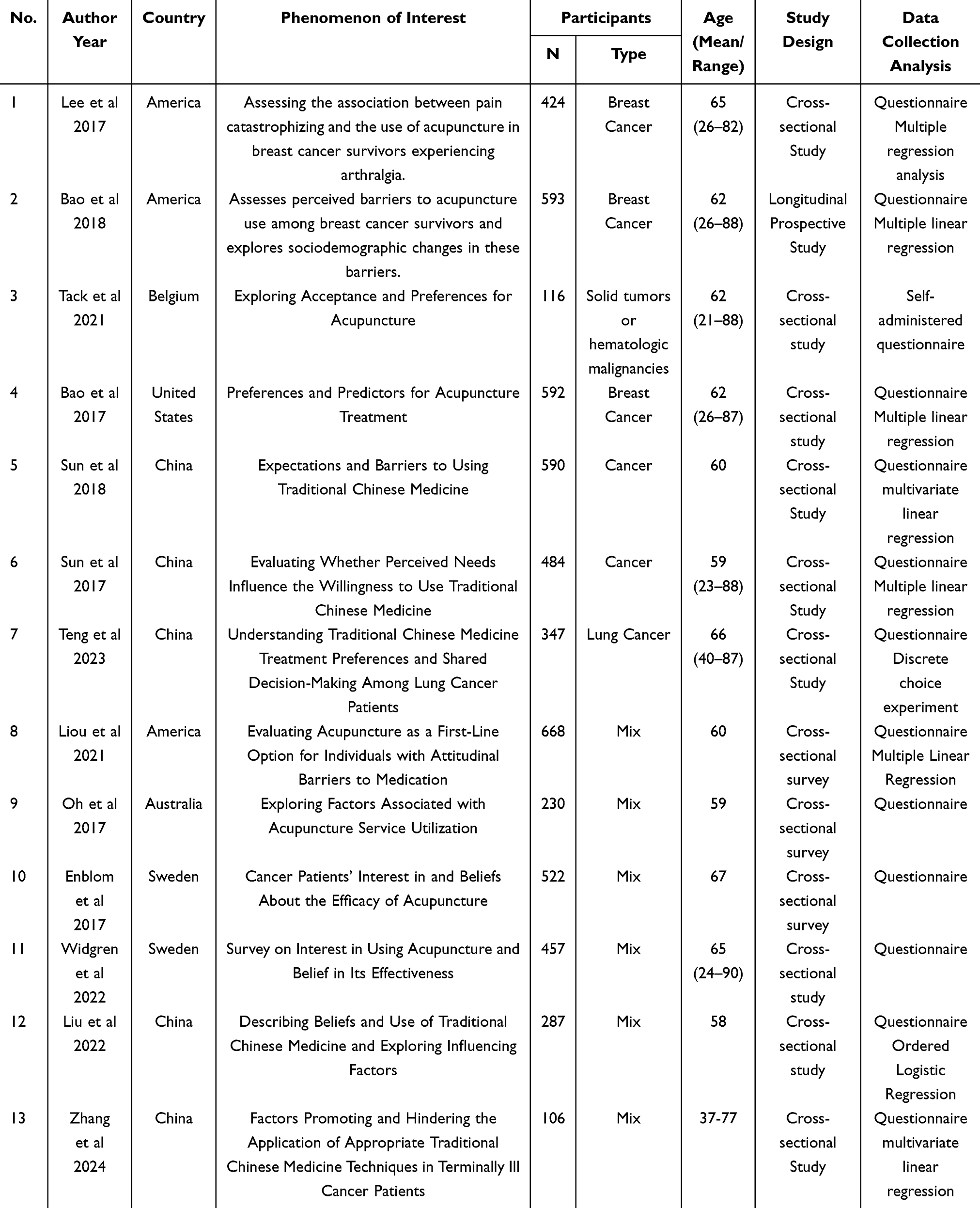 |
Table 1 Characteristics Included in Quantitative Research (N=13) |
 |
Table 2 Characteristics Included in Qualitative Studies (N=14) |
Integrated findings
The process of data synthesis and integration is detailed in Supplementary 2. Figure 2 presents a visual representation of the socio-ecological model illustrating factors influencing cancer patients’ preferences for TCM non-pharmacological therapies.
 |
Figure 2 A Socio-Ecological Model of Factors Influencing Cancer Patients’ Preferences for TCM Non-Pharmacological Therapies. |
Individual Factors
Demographic Characteristics
Numerous studies14–18,26,28–30,32,36,38,40,43 demonstrated relationships among age, gender, literacy, race, employment status, and cultural background with preferences and usage patterns. Research indicates that younger individuals (under 60 years),17 females,38 patients of particular ethnicities (such as Caucasians),17 and those with a cultural affiliation to TCM (eg, from Taiwan)32 may exhibit a greater propensity to engage in specific non-pharmacological therapies within TCM, such as acupuncture. The correlation between literacy and preference has yielded inconsistent findings across several investigations.15,17,38
Disease-Related Factors
The disease stage26,38,40,43 and the patient’s symptom experience16,28,40,41,44 are significant determinants affecting demand. Patients at various stages of sickness possess distinct expectations about TCM. Patients in the early stages typically employ TCM to avert recurrence or metastasis, whilst those in the late stages concentrate on enhancing their health with TCM.32 Patients pursuing TCM primarily aim to alleviate treatment-related side effects, such as chemotherapy-induced fatigue, sleep disturbances, and joint pain, as well as discomfort stemming from the disease itself, including pain, gastrointestinal issues, and peripheral numbness.14,16,17,26,28,30,32,33,36,40–42,44 The extent of symptom perception significantly affects need, as patients with diminished symptom awareness or elevated tolerance are likely to have reduced need.18,19,26,35
Psychological and Emotional Factors
Individuals exhibiting elevated levels of stress, anxiety, sadness, and significant weariness are more inclined to contemplate non-pharmacological interventions utilizing TCM.19,33,41,44 The psychological trauma associated with a cancer diagnosis, such as denial and depressive symptoms, significantly drives patients to pursue additional treatment from TCM.25 Patients’ need for a sense of control over their own health is closely related to seeking non-pharmacological treatments in TCM.30,32,33,35,42
Perceptions, Beliefs and Attitudes
Overall perceptions of TCM, trust,17–20,28,30–35,37,38,41–45 perceived usefulness,15,19,20,26,29,32,35,36,39,40,45 perceived safety,18,45 and perceived ease of use18,45 were important contributing factors. Conversely, lack of knowledge about TCM,20,43 doubts about its scientific evidence,14,34,43 and concerns about the side effects of Western medicine14,32,34,36,40 also influence choice. Patients’ expectations of treatment outcomes are also critical.17,27,37,40
Experience and Knowledge
Prior experience of use30–35,38,41,42,44,45 and knowledge related to non-pharmacological therapies of TCM14,18,19,27,31,34,38 will influence patients’ choices. Individuals’ previous experience of using TCM techniques with good results will enhance patients’ trust and propensity to choose TCM.41 However, insufficient knowledge of the indications for specific TCM non-pharmacological therapies (eg, lack of knowledge that acupuncture can treat insomnia) can affect their utilization.18
Personal Preferences and Fears
Patient preferences and concerns critically shape the selection of treatment modalities. Apprehension regarding pain, for instance with acupuncture,14,27,33,41 typically steers patients towards less painful or less stimulating alternatives such as moxibustion or gentle acupuncture.27 Accordingly, therapies that are easy to perform, suitable for home practice (eg, dietary therapy, acupressure), and are non-invasive or painless (eg, auricular acupressure) demonstrate particular popularity among patients.27
Interpersonal Relationships
Factors at the interpersonal level include influences from healthcare professionals, family members, friends, and other patients.
Influence From Healthcare Professionals
The recommendations, information dissemination, professionalism, communication abilities, and compassionate demeanor of healthcare professionals, including practitioners of Chinese medicine, Western medicine, and nursing staff, significantly influence patient selection.27,30–33,36,38,41,42 A robust doctor–patient relationship fosters confidence.33,39
Influence From the Family
Emotional support, encouragement, and acknowledgment from family members,32,33,36,41,42,44 endorsements from relatives and friends (eg, derived from their previous triumphs),42 and familial customs regarding TCM utilization42,45 are significant enabling elements. The collective involvement of family members can also augment motivation.42
Influence From Friends and Other Patients
Peer advice (friends, other patients), experience sharing,33,36,44 perceptions of social support networks,18,19,35,41,45 and community encouragement (eg, online and offline support groups)41 can affect patients’ decision-making willingness.
Health System Factors
The service delivery model of a healthcare organization, its capacity to integrate resources, and its promotional and instructional initiatives collectively shape the organizational environment that affects patients’ preferences in choice.
Accessibility of Healthcare Facilities
This encompasses temporal accessibility (prolonged waiting periods, frequent and time-intensive follow-up appointments, rigid scheduling),14,27,29,32,34,35,40 economic accessibility (elevated costs, inadequate health insurance coverage),14,15,20,27,28,33–35,39,41–43 and geographic accessibility (availability of facilities, ease of distribution).14,19,27,32,33,35,37,40–44 Services that are complimentary or insured considerably enhance the propensity to utilize them.
Service Content and Quality
The provision of requisite TCM non-pharmacological therapies by the healthcare organization,28,29 the quality of service (including counseling quality, professionalism, and therapists’ communication skills),14,33 and the advocacy of the technology by healthcare professionals32 all impact the decision-making process.
Therapeutic Environment
Comfort, privacy28,34,37,39,42 and familiarity33,41,42 of the environment influence patient preferences.
Integration and Collaboration in Healthcare Organizations
The extent of integration between Chinese and Western medicine services (eg, concurrent provision within an organization, incorporation into standard procedures) directly influences the accessibility of combined care for cancer patients; however, inadequate collaboration between the two medical systems remains a prevalent issue.32,33
Healthcare Organization Promotion and Education
Information dissemination at the organization level (eg, health talks, promotional materials)28,33,41 influences patient awareness and acceptance.
Social Factors
The cultural atmosphere of the community as well as the distribution of resources together influence patients’ choice of non-pharmacological therapies in TCM.
Cultural and Social Norms
The community’s distinct cultural background influences identification and trust for TCM, particularly in the interpretation of its fundamental principles (eg, contrasting “regulating” and “consolidating” in Eastern viewpoints with TCM’s perception in Western cultures).17,18,28,31,32,37,44 The general atmosphere of acceptance among the community is pivotal.19,29,30,33,45 Media coverage, public image, and levels of understanding further shape attitudes towards TCM.30,33 The extent of TCM’s incorporation into the community’s healthcare system and daily life influences its acceptance.31,37 It is conclusively recognized that acceptance levels for TCM varied significantly across various cultural contexts.19,28,31,33,39
Community Resources and Accessibility
The number, distribution, cost and inclusion of TCM services in the community27,29,37,39,42 are key at the practice level. For example, the popularity of community-based TCM clinics in Taiwan has improved accessibility,37 while inadequate clinic distribution and promotion of specific services (eg, group acupuncture) have limited patient choice.39
Policy Level
The macro-policy environment, especially in terms of health insurance coverage, industry regulation, research support and health system integration, has a decisive impact on the adoption of non-pharmacological therapies in TCM.
Health Insurance and Reimbursement Policies
Health insurance coverage, rates, and amounts14,32,33,35,36,39,42 are crucial for economic accessibility, and reimbursement policies differ markedly among countries and regions.15,41
Industry Standardization and Quality Regulation
The soundness of operational rules,32,35,39 practitioner credentials (eg, acupuncturists),32,35,39 and the adverse reaction monitoring and reporting system19 of TCM services influences patients’ belief in the safety and efficacy of TCM. The absence of standardized protocols and stringent regulations32,39 may engender patient skepticism over the quality and safety of services, such as the danger of infection associated with acupuncture, hence influencing their willingness to utilize these services.
Scientific Research Funding and Promotion of Results
The level and direction of funding for TCM research by the government or related organizations, as well as the publication, dissemination, and public popularization of research results,19,32,34,36,40 all affect the scientific validity and social acceptance of non-pharmacological therapies in TCM. The lack of sufficient research investment and effective dissemination of results29,31,32,34 has resulted in insufficient evidence-based medicine for TCM, limiting its standardized application in clinical practice and widespread acceptance by patients.
Discussion
Key Findings
This mixed-methods systematic review represents the first synthesis of evidence regarding cancer patients’ preferences for TCM non-pharmacological therapies. Our core finding is that patient preferences do not equate to the objective clinical efficacy of these therapies. A key contribution of this review is revealing that the factors driving patient choice are multidimensional and profoundly influenced by cultural context, emotional needs, and systemic barriers.
Evidence shows that the key to TCM acceptance is more about cultural affinity and social expectations rather than objective evidence.19,29,30,33,45 This cultural perspective seems to take shape in highly divergent regional settings. In areas that are heavily immersed in TCM culture, such as mainland China, Hong Kong, and Taiwan, there is an intrinsic cultural affinity and trust with TCM among the patients. In this context, TCM has come to be understood as traditional wisdom about regulating the body and strengthening the foundation, acting as an integral aid during the recovery stages.15,32,38 As demonstrated by multiple studies included in this review, this concept has been reinforced within China’s mainstream healthcare system: TCM is not an alternative medicine, but rather a medical system that is equally valued alongside Western medicine and receives policy support.46 In stark contrast to such settings within Western cultural milieus, as made evident in research studies conducted within the United States, Australia, and Canada that are represented within this review, due to TCM standing as an alternative form of medicine, it occupies a different cultural construct within these settings.33,42 The evidence shows that, within these areas, there are paramount considerations among patients and medical personnel concerned about a lack of scientific evidence in conjunction with concerns about efficacy and safety. For example, there has been evidence suggesting that some patients prefer treatments with acupuncture as an option due to concerns surrounding the side effects posed by Western pain relievers.17 In other words, within either cultural identity within Eastern culture milieus or due to evidence gaps within Western cultural milieus, there has been evidence within this review that patient preference choices are instead impacted by these settings rather than standard governed purely within the considerations of efficacy.
Second, this cultural preference finds more pronounced expression on the interpersonal process level. Patient preferences for TCM mainly represent a strong preference for interpersonal care with higher touch.33,39 In fact, this finding offers an alternative explanation to the “placebo effect” often associated with TCM, suggesting that the benefits are driven more by contextual factors (eg, interpersonal care) than by the placebo effect alone. The reason is that within the standardized highly efficient diagnostic-therapeutic process within modern oncology, there tends to be an absence of individual care. In TCM diagnostic models, more time is allotted and more interpersonal communication is possible. Multiple systematic reviews47,48 confirm that physician empathy not only enhances patient satisfaction but also leads to objective improvements in clinical outcomes, such as reduced pain, anxiety, and glycated hemoglobin levels. A qualitative study49 comparing responders and non-responders to acupuncture provides direct evidence: responders reported perceiving practitioner empathy, which fostered trust and led to more active adherence to lifestyle and dietary recommendations. Non-responders, lacking this trust connection, experienced persistent anxiety about treatment safety.
Notwithstanding the above-mentioned significant preference stemming from cultural and emotional considerations, there has been a fundamental conflict arising from the mismatch between patients’ strong preference and the existence of high-quality clinical evidence. Indeed, the area of CAM has been defined by the existence of a fundamental conflict between the widespread use and the lack of evidence represented by the absence of high-quality randomized controlled trials (RCT). The great majority of articles compiled in this review are concerned with acupuncture. Other approaches such as tuina massage, nutritional therapy, and qigong are involved in a lack of studies on preference and display weaker evidence with respect to the safety and efficacy these approaches display. The conflict represented by the mismatching between the patient’s strong preference and the lack of evidence is pushing patients to make decisions based on cultural considerations rather than safety and efficacy. Oncologists face the dilemma of proposing integrated medicine to patients with the lack of evidence-based recommendation. Furthermore, TCM non-pharmacological therapies are thwarted in accessing mainstream medicine due to the lack of evidence represented by RCTs accepted by modern medicine.
The theoretical insight within this research is about displaying the dynamic processes among various levels within the socio-ecological model. From the results, it is clear that these patient preferences must overcome various practical obstacles to be successfully executed. Policy-level aspects such as health insurance coverage are critical in this case. The economic strain is widespread; even within the Chinese healthcare system, cumulative TCM expenses are felt to be significant by the patients. Notably, such an issue does not necessarily result in the dismissal of Western medicine. A survey was conducted among Chinese-Americans with rheumatology within the United States. The paradoxical result found there showed that patients following TCM had greater adherence to Western prescription drugs. The rationale suggests that the Healthy Adherer Effect might be active among patients who prefer TCM. These might be more actively concerned with managing their medical conditions.50 However, lack of communication might present potential dangers within these integrated Chinese and Western medical approaches. A study among Hong Kong patients found that 61% are concerned that Western doctors might oppose them if these patients disagreed about concealing TCM use.51
Strengths and Limitations
The primary strengths of this review are: (1) The application of mixed-methods systematic review with the integration of the extensive quantitative study results with the in-depth results of qualitative research. This systematic review method offers an extensive and in-depth insight into the preferences of cancer patients with respect to TCM non-pharmacological treatments and the extensive underlying causes and experiences. (2) Adherence to JBI MMSR guidelines and PRISMA statement in performing the extensive searches of various databases, critically screening the retrieved literature, evaluating the quality, and synthesizing the results to ensure that the review has scientific rigor and validity. (3) The integration of influencing factors using a socio-ecological model. The analytical contribution of this review lies in its pioneering application of this framework to the domain of TCM preferences. By synthesizing vast, dispersed qualitative and quantitative data, it constructs a systematic understanding of how preferences are formed and interact—transcending a mere descriptive enumeration of factors. (4) Innovation and application to practice. This review addresses the issue that there has been no systematic review on this issue so far. The results are of great references to break through personalized treatments in cancer care and to establish integrated medical models that optimize the use of resources and medical health policies.
In addition, this review also has several limitations of its own, including: (1) The search criteria for this review include only Chinese and English language publications, which may cause bias in this review because only two languages are being used in this search process. (2) A review of previous literature shows that more emphasis has been placed upon assessing preferences for treatments using acupuncture, which to date has been addressed by relatively few studies, including tuina massage, dietary therapy, auricular therapy, as well as qigong, which also fall into TCM category of non-pharmacological therapies. (3) Although studies from multiple countries were included, those originating from regions with deep roots in TCM culture accounted for a disproportionately high proportion. This suggests that the findings of this review may reflect preferences driven by cultural affinity rather than universal health needs. The generalizability of these results to other cultural contexts requires careful consideration.
Implications for Practice and Future Research
The results of this research carry important implications in terms of practicing and further research. Practicing implications include the need to change from reactive to proactive and patient-centered integration within healthcare settings. The current research highlights that patient preferences are deeply impacted by both individual and interpersonal predictors. As such, structured preference assessments can be mainstreamed within oncology settings. In these assessments, instead of focusing on whether patients want TCM or not, there needs to be further research on the underlying drivers. For example, assessments need to identify whether patients are looking to alleviate symptoms or reduce anxieties, while pointing to concerns about expenses and pain. These analyses will allow oncology settings to ensure that there is personalized evidence-based recommendation, like recommending equal evidence-based Acupressure or Auriculotherapy to patients with needles phobias. Additionally, to improve upon the poor integration within current healthcare settings and the need to personally integrate oncology settings in terms of coordination and stress among patients, there needs to be standardized interdisciplinary referral and communication mechanisms within oncology settings. These include establishing an approved internal list of TCM non-pharmacological practitioners such as Acupuncturists and Tuina practitioners with clear referral criteria and accompanying feedback questionnaires. These ensure that oncology physicians are fully updated about the use and outcome of other treatments within complementary therapies.
At the level of future research, the observation that patient preferences are widespread but lack high-quality evidence highlighted by this review encourages researchers to move ahead immediately in two distinct areas. Firstly, focusing on efficacy validation research, our analysis illustrates that current research is overwhelmingly focused on acupuncture; meanwhile, treatments that are actually preferred by patients, like massage, nutritional therapy, and qi gong, are underserved by the lack of high-quality evidence.52 Therefore, future research resources (such as research grants) should strategically establish dedicated programs to prioritize funding for studies on the efficacy and safety of these therapies, which is fundamental to addressing barriers to clinical integration. Secondly, at the level of implementation science,53 evidence of therapeutic efficacy alone is insufficient to overcome the clinical integration barriers identified in this review. Future research must explore how to safely and effectively integrate these therapies into routine oncology care. As such, research must develop and validate tailored cancer-specific patient decision aids;54 implement intervention studies to evaluate the impact of TCM Evidence Literacy and Communication Skills training modules on providers’ knowledge and attitudes. To address patient-reported accessibility barriers, design studies to test different service models. For example, evaluate the practical effectiveness of integrating non-pharmacological TCM therapies into group rehabilitation programs or developing telemedicine-based apps for self-administered acupressure or qigong guidance in improving patient adherence, quality of life, and cost-effectiveness.
Conclusions
The implications of this research are that there are complex preferences among cancer patients with regard to non-pharmacological treatments that are employed in TCM. Furthermore, these preferences are shaped by various considerations that cut across the entire spectrum from the personal to macro-level considerations. Understanding and respecting patient preferences is a crucial step toward achieving patient-centered cancer care. However, this review also reveals that these preferences are heavily influenced by cultural affinity and the need for personalized care, often not grounded in rigorous scientific evidence. Future clinical practice, policy development, and scientific research must collaborate to strike a balance between respecting patients’ cultural needs and upholding evidence-based science. This requires optimizing services, refining regulations, and prioritizing research to address gaps in safety and efficacy. Ultimately, this approach will enable more cancer patients to benefit from safe and effective TCM non-pharmacological therapies.
Acknowledgments
The authors thanked all.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This review was funded by the Zhejiang Province Science and Technology Plan Project (Grant Number:2023C03165).
Disclosure
The authors declare no competing interests in this work.
References
1. Mogavero MP, DelRosso LM, Fanfulla F, Bruni O, Ferri R. Sleep disorders and cancer: state of the art and future perspectives. Sleep Med Rev. 2021;56:101409. doi:10.1016/j.smrv.2020.101409
2. Kwon JH, Lee SC, Lee MA, et al. Behaviors and attitudes toward the use of complementary and alternative medicine among Korean cancer patients. Cancer Res Treat. 2019;51(3):851–860. doi:10.4143/crt.2019.137
3. Zhang XW, Hou WB, Pu FL, et al. Acupuncture for cancer-related conditions: an overview of systematic reviews. Phytomedicine. 2022;106:154430. doi:10.1016/j.phymed.2022.154430
4. Krejbich P, Birringer M. The self-administered use of complementary and alternative medicine (CAM) supplements and antioxidants in cancer therapy and the critical role of Nrf-2-A systematic review. Antioxidants. 2022;11(11). doi:10.3390/antiox11112149
5. Lin JY, Meng HT, Wang Y, et al. Analysis of annual evidence from clinical studies on non-pharmacological therapies in traditional chinese medicine (2023). J Tianjin Univer Tradit Chin Med. 2025;44(01):59–64.
6. Zhang X, Qiu H, Li C, Cai P, Qi F. The positive role of traditional Chinese medicine as an adjunctive therapy for cancer. Biosci Trends. 2021;15(5):283–298. doi:10.5582/bst.2021.01318
7. Choi TY, Ang L, Jun JH, Alraek T, Lee MS. Acupuncture and moxibustion for cancer-related fatigue: an overview of systematic reviews and meta-analysis. Cancers. 2022;14(10). doi:10.3390/cancers14102347
8. Cheung DST, Xu X, Smith R, et al. Invasive or noninvasive? A systematic review and network meta-analysis of acupuncture and acupressure to treat sleep disturbance in cancer patients. Worldviews Evid Based Nurs. 2023;20(3):202–211. doi:10.1111/wvn.12617
9. Holanda da da Cunha G, Lima Ramalho AK, Dantas MB, et al. Auriculotherapy for people with sleep disorders: a systematic review. Complement Ther Clin Pract. 2025;59:101976. doi:10.1016/j.ctcp.2025.101976
10. Kim JS, Kwon JH, Rha SY, et al. Status of using complementary and alternative medicine among patients with cancer in Korea: an online survey of online cancer support groups (KCSG PC21-20). Cancer Res Treat. 2023;55(2):442–451. doi:10.4143/crt.2022.1483
11. Teo I, Chow M, Chaudhry I, Malhotra C, Ozdemir S, Finkelstein EA. Complementary and alternative medicine use in the last year of life: the COMPASS cancer cohort study. J Pain Symptom Manage. 2025;69(4):e257–e264. doi:10.1016/j.jpainsymman.2024.12.022
12. Rockenbauch K, Schildmann J. Shared decision making (SDM): a systematic survey of terminology use and concepts. Gesundheitswesen. 2011;73(7):399–408. doi:10.1055/s-0030-1262870
13. Schoefs E, Vermeire S, Ferrante M, et al. What are the unmet needs and most relevant treatment outcomes according to patients with inflammatory bowel disease? A qualitative patient preference study. J Crohns Colitis. 2023;17(3):379–388. doi:10.1093/ecco-jcc/jjac145
14. Bao T, Li Q, DeRito JL, Seluzicki C, Im EO, Mao J. Barriers to acupuncture use among breast cancer survivors: a cross-sectional analysis. Integr Cancer Ther. 2018;17(3):854–859. doi:10.1177/1534735418754309
15. Teng Y, Wei Y, Chen Y, et al. Patient preferences and shared decision making for the traditional Chinese medicine treatment of lung cancer: a discrete choice experiment study. Integr Med Res. 2023;12(3):100969. doi:10.1016/j.imr.2023.100969
16. Lee I, Garland SN, DeMichele A, Farrar JT, Im EO, Mao JJ. A cross-sectional survey of pain catastrophising and acupuncture use among breast cancer survivors. Acupunct Med. 2017;35(1):38–43. doi:10.1136/acupmed-2016-011056
17. Bao T, Li SQ, Dearing JL, et al. Acupuncture versus medication for pain management: a cross-sectional study of breast cancer survivors. Acupunct Med. 2018;36(2):80–87. doi:10.1136/acupmed-2017-011435
18. Zhang S. A qualitative study on the facilitating and hindering factors for the application of Chinese medicine appropriate technology in terminal tumor patients. J Chin Med Management. 2024;32(19):37–39. doi:10.16690/j.cnki.1007-9203.2024.19.039
19. Li XM, Yang L, Du J, et al. A qualitative study on the dietary therapy needs of cancer-caused fatigue patients with traditional Chinese medicine. Bright Chin Med. 2023;38(01):22–26.
20. Yin DQ, Yu XQ. A qualitative study of malignant tumor chemotherapy patients’ experience of Chinese medicine nursing techniques. Qilu Nursing J. 2017;23(09):65–68.
21. Harden A, Thomas J, Cargo M, et al. Cochrane qualitative and implementation methods group guidance series-paper 5: methods for integrating qualitative and implementation evidence within intervention effectiveness reviews. J Clin Epidemiol. 2018;97:70–78. doi:10.1016/j.jclinepi.2017.11.029
22. Bian W, Chen YL, Liao JM, et al. Introduction to mixed-methods research system evaluation. Chinese J of Evidence-Based Med. 2019;19(04):498–503.
23. Stokols D. Translating social ecological theory into guidelines for community health promotion. Am J Health Promot. 1996;10(4):282–298. doi:10.4278/0890-1171-10.4.282
24. Hong QN, Gonzalez-Reyes A, Pluye P. Improving the usefulness of a tool for appraising the quality of qualitative, quantitative and mixed methods studies, the Mixed Methods Appraisal Tool (MMAT). J Eval Clin Pract. 2018;24(3):459–467. doi:10.1111/jep.12884
25. Stern C, Lizarondo L, Carrier J, et al. Methodological guidance for the conduct of mixed methods systematic reviews. JBI Evid Implement. 2021;19(2):120–129. doi:10.1097/xeb.0000000000000282
26. Sun L, Yang Y, Vertosick E, Jo S, Sun G, Mao JJ. Do perceived needs affect willingness to use traditional Chinese medicine for survivorship care among Chinese cancer survivors? A cross-sectional survey. J Glob Oncol. 2017;3(6):692–700. doi:10.1200/jgo.2016.007955
27. Dongsheng B, Guo Y, Chen B, et al. A survey study on insomnia perceptions and acupuncture treatment preferences of breast cancer survivors based on the in-depth interview method. Chinese Acupuncture. 2024;44(09):1023–1028. doi:10.13703/j.0255-2930.20231207-0001
28. Tack L, Lefebvre T, Blieck V, et al. Acupuncture as a complementary therapy for cancer care: acceptability and preferences of patients and informal caregivers. Article. JAMS J Acupuncture Meridian Studies. 2021;14(2):67–74. doi:10.51507/j.jams.2021.14.2.67
29. Enblom A. Patients’ and physiotherapists’ belief in and use of acupuncture for cancer-related symptoms. Acupunct Med. 2017;35(4):251–258. doi:10.1136/acupmed-2015-011007
30. Widgren Y, Fransson P, Efverman A. Acupuncture in patients undergoing cancer therapy: their interest and belief in acupuncture is high, but few are using it. Integr Cancer Ther. 2022;21:15347354221077277. doi:10.1177/15347354221077277
31. Chan HY, Chui YY, Chan CW, et al. Exploring the influence of Traditional Chinese Medicine on self-care among Chinese cancer patients. Eur J Oncol Nurs. 2014;18(5):445–451. doi:10.1016/j.ejon.2014.05.005
32. Chen K-W, Chung K-P, Hsu C-H. The intention of utilization and experience toward traditional Chinese medicine among breast cancer patients in the early and late stages: a qualitative study. BMC Complement Med Therap. 2023;23(1):1–10. doi:10.1186/s12906-023-04054-0
33. Ee C, Singleton AC, de Manincor M, et al. A qualitative study exploring feasibility and acceptability of acupuncture, yoga, and mindfulness meditation for managing weight after breast cancer. Integr Cancer Ther. 2022;21:15347354221099540. doi:10.1177/15347354221099540
34. Garland SN, Eriksen W, Song S, et al. Factors that shape preference for acupuncture or cognitive behavioral therapy for the treatment of insomnia in cancer patients. Support Care Cancer. 2018;26(7):2407–2415. doi:10.1007/s00520-018-4086-4
35. Hung YL, Leung SS, Chiu SP, et al. Perceptions about traditional Chinese medicine use among Chinese breast cancer survivors: a qualitative study. Cancer Med. 2023;12(2):1997–2007. doi:10.1002/cam4.5046
36. Liou KT, Trevino KM, Meghani SH, et al. Fear of analgesic side effects predicts preference for acupuncture: a cross-sectional study of cancer patients with pain in the USA. Support Care Cancer. 2021;29(1):427–435. doi:10.1007/s00520-020-05504-y
37. Liu CH, Tang WR, Wang HM, Lee KC. Cancer patients’ experience of combined treatment with conventional and traditional Chinese medicine: a biopsychosocial phenomenon. Cancer Nurs. 2011;34(6):495–502. doi:10.1097/NCC.0b013e31820d4da9
38. Liu J, Sun Y, Liu S, He J. Belief in and use of traditional Chinese medicine in Chinese patients with cancer receiving outpatient care. Eur J Int Med. 2022;58:102221. doi:10.1016/j.eujim.2022.102221
39. Oberoi D, Reed EN, Piedalue KA, Landmann J, Carlson LE. Exploring patient experiences and acceptability of group vs. individual acupuncture for Cancer-related pain: a qualitative study. BMC Complement Med Ther. 2022;22(1):155. doi:10.1186/s12906-022-03600-6
40. Oh B, Eade T, Kneebone A, et al. Factors affecting whether or not cancer patients consider using acupuncture. Acupunct Med. 2017;35(2):107–113. doi:10.1136/acupmed-2016-011115
41. Peter M, Joy B, Jacqueline F, Jennifer FJ, Alexander M. Receiving or not receiving acupuncture in a trial: the experience of participants recovering from breast cancer treatment. Complement Ther Clin Pract. 2014;20(4):291–296. doi:10.1016/j.ctcp.2014.10.002
42. Porter D, Cochrane S, Zhu X. Current usage of traditional Chinese medicine for breast Cancer-A narrative approach to the experiences of women with breast cancer in Australia-A pilot study. Medicines. 2017;4(2). doi:10.3390/medicines4020020
43. Sun L, Mao JJ, Vertosick E, Seluzicki C, Yang Y. Evaluating cancer patients’ expectations and barriers toward Traditional Chinese Medicine Utilization in China: a patient-support group-based cross-sectional survey. Integr Cancer Ther. 2018;17(3):885–893. doi:10.1177/1534735418777117
44. Walker G, de Valois B, Davies R, Young T, Maher J. Ear acupuncture for hot flushes--the perceptions of women with breast cancer. Complement Ther Clin Pract. 2007;13(4):250–257. doi:10.1016/j.ctcp.2007.06.003
45. Sheng X, Huang B, Lin G, et al. A qualitative study on the facilitating factors for oncology patients’ acceptance of Chinese medicine nursing appropriate technology. China Medical Guide. 2024;22(10):5–8. doi:10.15912/j.issn.1671-8194.2024.10.002
46. Wang JW, Yang ZQ, Liu C, et al. Cancer survivors’ perspectives and experience on western medicine and traditional Chinese medicine treatment and rehabilitation: a qualitative study. Patient Prefer Adherence. 2015;9:9–16. doi:10.2147/ppa.S76617
47. Howick J, Moscrop A, Mebius A, et al. Effects of empathic and positive communication in healthcare consultations: a systematic review and meta-analysis. J R Soc Med. 2018;111(7):240–252. doi:10.1177/0141076818769477
48. Derksen F, Bensing J, Lagro-Janssen A. Effectiveness of empathy in general practice: a systematic review. Br J Gen Pract. 2013;63(606):e76–84. doi:10.3399/bjgp13X660814
49. Ho RST, Ho FF, Adams J, et al. Patients’ perceptions on non-specific effects of acupuncture: qualitative comparison between responders and non-responders. Integr Med Res. 2022;11(1):100771. doi:10.1016/j.imr.2021.100771
50. Sun K, Szymonifka J, Tian H, Chang Y, Leng JC, Mandl LA. Is use of traditional Chinese medicine associated with non‐adherence to prescribed western rheumatic medications among Chinese‐American patients? A cross‐sectional survey. Arthritis Care Research. 2019;2019.
51. Lam YC, Cheng CW, Peng H, Law CK, Huang X, Bian Z. Cancer patients’ attitudes towards Chinese medicine: a Hong Kong survey. Chin Med. 2009;4:25. doi:10.1186/1749-8546-4-25
52. Vickers AJ, Vertosick EA, Lewith G, et al. Acupuncture for chronic pain: update of an individual patient data meta-analysis. J Pain. 2018;19(5):455–474. doi:10.1016/j.jpain.2017.11.005
53. Proctor E, Silmere H, Raghavan R, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health. 2011;38(2):65–76. doi:10.1007/s10488-010-0319-7
54. Stacey D, Légaré F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;4(4):Cd001431. doi:10.1002/14651858.CD001431.pub5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.