")
Back to Journals » Patient Preference and Adherence » Volume 17
Preferences for Health Care and Its Determinants Among Mentally Ill Patients of the West Shoa Zone Community, Oromia, Ethiopia
Received 2 November 2022
Accepted for publication 25 February 2023
Published 7 March 2023 Volume 2023:17 Pages 557—570
DOI https://doi.org/10.2147/PPA.S393903
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Getachew Adela Kasa,1 Mirgissa Kaba2
1School of Public Health, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 2Department of Preventive Medicine, School of Public Health, College of Health Science, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Getachew Adela Kasa, School of Public Health, St. Paul’s Hospital Millennium Medical College, PO Box 1271, Gulele Sub-City, Addis Ababa, Ethiopia, Tel +251919292590 ; +2514793932709, Fax +251112-78-85-92, Email [email protected]
Background: Over 9 million people die from mental diseases each year, making them the second highest cause of mortality and the primary cause of disability worldwide.
Objective: To explore the preferences for health care and its determinants among mentally ill patients in the West Shoa Zone Community in Oromia, Ethiopia, from July 11–September 20, 2022.
Methods: The preference for health care and its determinants among mentally ill patients in the West Shoa Zone community were explored using an ethnographical study. Purposefully, a total of 16 FGD participants and 10 unstructured interview subjects, who had pertinent experiences and perspectives, were carefully selected from the urban and district levels. Data was collected utilizing two approaches in a triangulated manner and then coded, findings were contextualized, and a thematic plot was developed for thematic analysis.
Results: In this study, in response to the questions, three main findings were thematized according to the causes, and six sub-themes were framed under the themes according to the preferences for treatment among mentally ill patients. The themes that emerged from the data were; 1. Supernatural causes, 2. Traditional non-spiritual beliefs and practices; and 3. Medico-surgical problems. The majority of the participants responded that residents preferred religious spiritualists the most (46%), followed by traditional counselors (Wabeka) (19%), traditional spiritualists (15%), institutional care (12%), herbalists (4%), and psychologists (4%).
Conclusions and Recommendations: In this study, the most commonly perceived causes of mental illnesses were bad spirits, devilish activity, and engaging in actions that violated social norms and regulations. Religious spiritualists were the study’s first choice for mental health care. This study advises collaboration and a shared strategy between health care professionals and traditional and religious stakeholders.
Keywords: mental illness, traditional healer, cultures, preferences
Introduction
Over 276 million years of life with a disability-adjusted life expectancy and over 9 million deaths per year are accounted for by mental diseases, which are also the second biggest cause of mortality globally.1 They are present in 10% of adult populations worldwide at any given time. Young adults, who are the most productive age group in the population, are most affected by mental health issues.2 We use the term “mental illnesses” to refer to all diagnosable mental diseases that are characterized by changes in cognition, emotion, or behavior (or some combination of these), as well as distress and/or diminished functioning.3 People with mental illnesses are typically viewed as lazy, worthless, stupid, dangerous to be around, violent, always in need of supervision, under the control of demons, suffering from divine punishment, unpredictable, unreliable, irresponsible, without consciousness, unfit for marriage and childrearing, unable to work, and getting sicker and sicker as they age.2 According to a study conducted in India, the frequency of mental diseases varies across the nation from 10 to 370 per 1000 people, with females experiencing rates that are roughly 20–25% higher.2 According to reports, 15% of children and 18% of adults in Ethiopia suffer from mental diseases. Only in the rural regions of Ethiopia do mental illnesses account for 11% of all disorders.4
There are various myths regarding the causes of mental illness.5 The stigma associated with mental illness makes many individuals feel guilty and discourages them from getting care. This is exacerbated by myths and misconceptions about the condition.2 Non-Western countries, like Ethiopia, typically adhere to traditional and religious perspectives to explain the etiology of mental illness, while Western cultures typically follow the biological paradigm of disease conceptualization and treatment.4 The most frequently cited causes of mental illness were stress, genetics, and bad childhood experiences.6 Bad parenting, air pollution, loss of semen, poor diet, past sin, the curse of God, and the evil eye are also some of the important myths related to its causation.2 It was evident that many people in Uganda think that witchcraft, curses, and demonic or ancestral spirits cause mental illness. Most interviewees responded that in Ugandan society, mental diseases were seen as “spiritual” illnesses, the product of “evil powers”, or both.7 According to a study on Ethiopian perceptions of mental disease, excessive concern and thinking, poverty, the death of a family member, and poisoning are all causes of mental illness.8
In developing countries, age, gender, marital status, family size, parity, education level, and other physical, socioeconomic, cultural, and political determinants are just a few examples of the variables that are frequently linked to and used to evaluate health-preferring behaviors and the healthcare system.9 People are known to be reluctant to seek professional care because of things like the fear of being labeled as having a mental illness, mistrust of the system, and a lack of faith in medical personnel.7 The decision to seek assistance also seems to be influenced by the person’s sense of the illness’ severity, with those who do so feeling more driven to do so.7 Innovations are emerging to provide accessible, affordable, and acceptable prevention, care, and treatment services to the different communities affected by mental health challenges, as mental illness is acknowledged as a worldwide burden.1 Prior research revealed that just 32% of people use community intervention facilities globally, which covers any sort of care for patients with mental illnesses seeking mental health interventions outside of hospitals. This is despite an increase in mental diseases.10 In rural regions, cultural customs and beliefs can cause delays in self-care, home cures, and consultations with traditional healers.9 Additionally, where one chooses to get assistance is considered to depend on what is thought to be the illness’s underlying cause. Due to the widespread belief that mental disease is caused by supernatural factors, a sizable proportion of those who have mental health issues initially favor and subsequently seek out the services of traditional healers.7 As a result, traditional healers find themselves shouldering a large burden of care for patients with mental health problems.7
Ethiopians are frequently drawn to traditional medicine for a variety of reasons, including greater cultural acceptance, comparatively lower costs, accessibility, availability, shared social norms, and beliefs about the causes, effects, and course of illness. As a result, in Ethiopia, those who need assistance with mental health symptoms must mostly turn to family, friends, and traditional healers.4 When individuals are brought to the few places providing westernized mental health care, it is often after exhausting other traditional and religious alternatives.4 Mental disorders continue to increase, and these disorders remain poorly understood, mostly in developing countries.10 In undeveloped countries, only 36% of those with mental illnesses have insurance coverage, compared to >92% in wealthy countries.10
Healthcare in Ethiopia is provided by self-care, traditional therapy, private and public health facilities, a mixed system, and a complex composition of health care systems. Literature on perceptions of particular mental illnesses and healthcare preferences in Ethiopia is scarce. Due to the dearth of studies in this field, it is clear that more research is needed into the various facets of mental disorders in our nation. This burden has prompted us to investigate the most significant aspect of health care preferences in order to bridge the gap between traditional and modern therapies.
Research questions include four conceptual domains
Domain 1: What do populations know about mental health problem?
Domain 2: What do they think about the possible causes?
Domain 3: Where do people prefer to go or to be treated when they develop mental problems?
Domains 4: Why do they prefer it (based on Domains 3)?
The conceptual framework that describes the determinants and care preferences of mental illnesses is explained in Figure 1 in the annex.
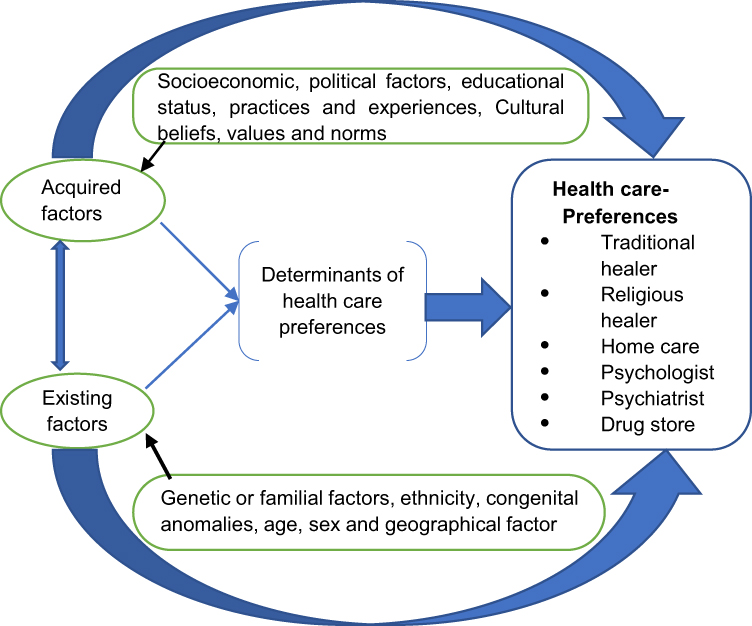 |
Figure 1 Framework for Preferences of Healthcare and Its Determinants among Mentally Ill Patients of the West Shoa Zone Community, Oromia, Ethiopia, July 2022. |
Materials and Methods
Study Setting
The study was carried out in the West Shoa Zone, which is one of the twenty-one (21) zones found in the Oromia region of Ethiopia. With a projected total population of 2,869,314 people, the Zone is administratively divided into 529 rural and 55 urban kebeles and 1 town administration. At the time of the survey, there were about 598 medical facilities in the zone.
Study Population and Period
Community representatives were drawn and recruited from one district and one urban residence. The rural area was the district of Jeldu, which is 121 kilometers West of Addis Ababa. The urban town is Ambo, which is 112 kilometers West of Addis Ababa. The study was conducted from July 11 through September 20, 2022.
Research Design and Recruitment of Participants
How cultural norms, values, or cultures influence people’s preferences for mental health concerns was explored using an ethnographic study. Participants were carefully selected among community members who were deemed to have a thorough comprehension of the subject under study.
Data Collection Methods
To better understand the complex social phenomenon of preferences for healthcare and its determinants among mentally ill patients, three gender-specific focus group discussions (FGDs) with sixteen (16) participants were conducted. In addition to that, in-depth interviews with five participants from families directly affected by mental illnesses and five community key informants were also carried out. Mental health stakeholders also took part in this interview. A total of ten interviews, drawn from one district and one urban settlement, were conducted for this interview. For data collection, two techniques were triangulated. Along with other stakeholders, religious leaders and traditional healers were also interviewed about how and where they and their patients obtain mental health care. FGDs were conducted with some relatively homogenous participant groups that were formed separately for males and females.
Members were collected from different occupations in order to elicit participant opinions, record the conversation and interactions between these participants in relation to specific topics, and capture a range of viewpoints within these groups. For the FGDs, a community health center served as the location. Each FGD featured an average of eight participants. The total number of subjects who gave data saturation was twenty-two (22); however, data collection was extended for an additional four participants. Key informant interviews were conducted with those interviewees who had either direct or indirect exposure to the mental illness episode in the year prior. A focus group discussion lasted on average for roughly 40 minutes. Every member of the group had an opportunity to speak and express their ideas. The discussions were conducted in A/Oromo, the local tongue of each venue, and audio recorded before being translated into English. The questionnaires were written in English, then translated and given out in A/Oromo. Verbatim notes from the FGDs were transcribed in order to provide a record of what was said. The participants were chosen in a two-step process, with participants drawn from the community as well as institutions such as school officials, and they represented the majority of the affected age and social groups. As guides and checklists for FGD were being created, opinions and reflections were being recorded.
Data Quality Assurance and Trustworthiness
In order to guarantee the accuracy and integrity of the results, the main researcher conducted the interview and was open and honest about any prior assumptions about the study and any knowledge of potential bias. Even though we were aware of some of the care choices of mentally ill patients, the participants were assured that the researchers were not engaged in picking or rating health care preferences or plans. The comments made by the participants needed to be honest. The consistency of the data was regularly examined during the data collection process. The co-investigator, who did not participate in the focus groups, also confirmed the interpretation and translation of the data. To assure validity and reliability, the triangulation approach was performed. Members of the research team who served as multiple observers reviewed the study. It was successful in giving a thorough description of the data. The second research team analyzed the analytical process to maintain consistency and looked at whether the study’s conclusions might be applied to different scenarios.
Data Analysis
The process of data analysis began with data gathering and was closely related to the end analysis. All of the materials were verbatim transcribed once the interviews had been collected, and they were then translated from their native language to English. The research assistant double-checked all transcriptions and translations for accuracy and completeness of data before moving on to the next round of interviews. From the interviews, all the data relevant to each theme was taken. The 30 pages of interviews were translated from A/Oromo, the original language of the interviewees, into “English” by a bilingual assistant. The data was coded, the conclusions were contextualized, and then they were categorized in a way that was appropriate for the topic in order to identify themes and enable the inductive detection of patterns. These topics were then further developed, leading to the creation of the final theme for the thematic analysis. The options for treating mental illnesses in the community were then examined using a theme analysis. The study team looked over and summarized the data to ensure the objectivity of the results. An inductive thematic approach that started with the raw data was used to generate sub-themes and overall themes.
Results
Participant Demographics
Twenty-six (26) community representatives, ranging in age from twenty (20) to fifty five (55), took part in the study. Twelve (12) women and fourteen (14) men made up the group. Five (5) of the interviewees had a history of mental illness in their families. Twenty-six (26) participants included two (2) young adults and twenty-four (24) older persons. The participants’ average age was 37.92 years. Seven (7) participants were employed by the government, three (3) were business owners, seven (7) were farmers, and the remaining participants worked for themselves. On Table 1 and Table 2 below, the participant profiles are displayed.
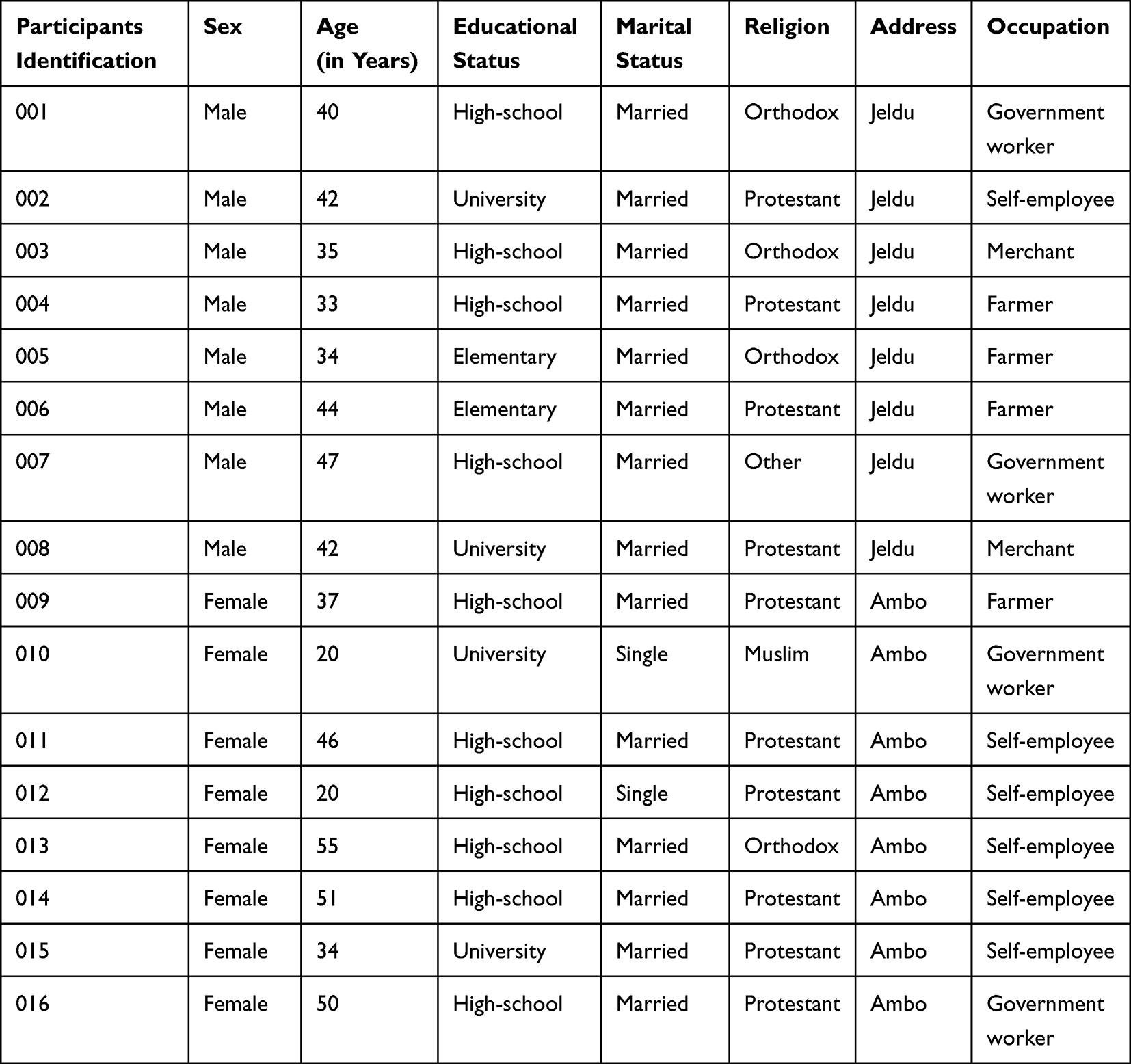 |
Table 1 Focus Group Discussion Participant’s Demographics in the West Shoa Community, Oromia Region, Ethiopia, July 2022 |
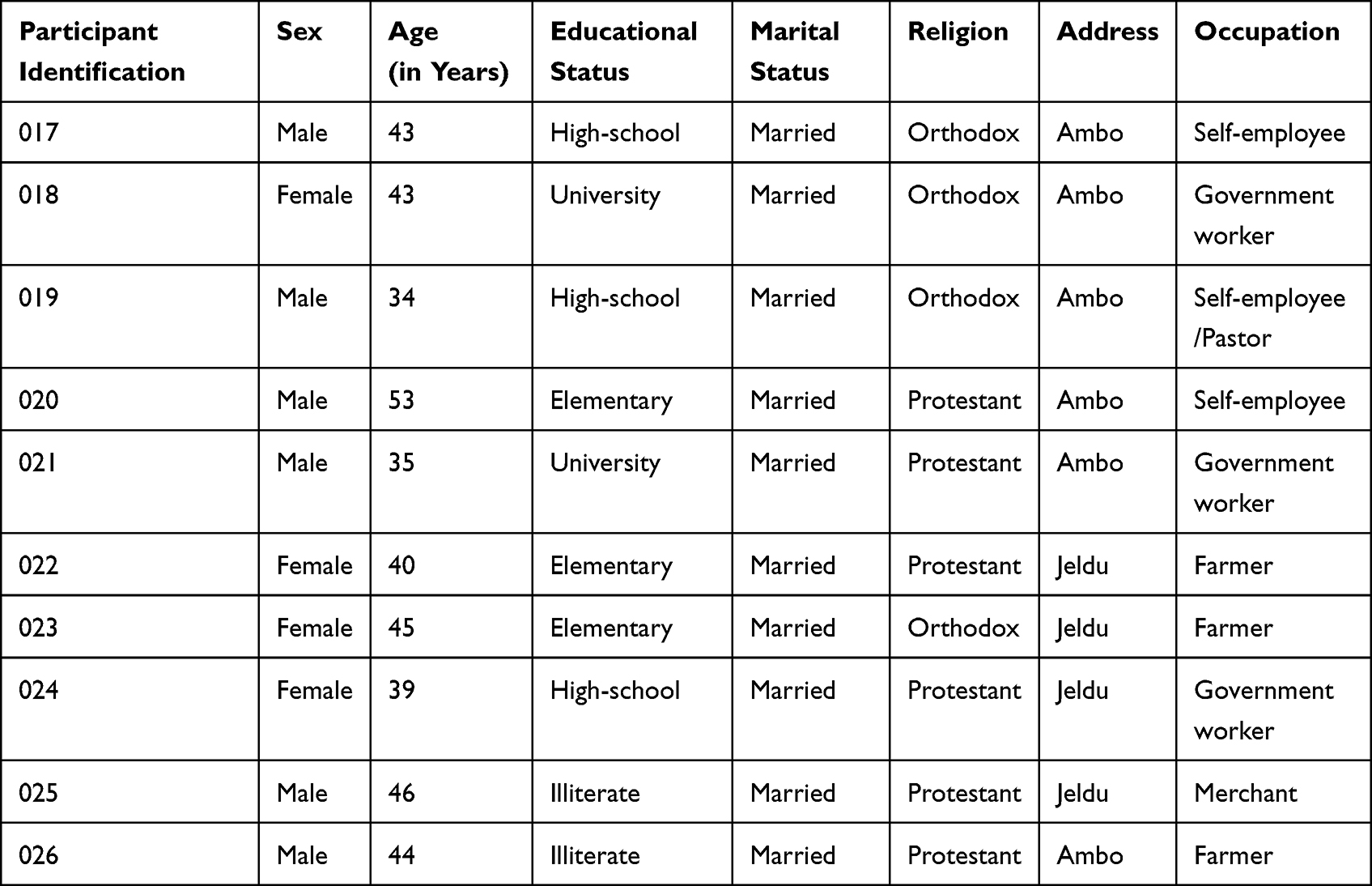 |
Table 2 Participant’s Demographics from Face-to-Face Individual Interviews in the West Shoa Zone Community, Oromia Region, Ethiopia, June 2022 |
Beliefs of Participants About Mental Illnesses
The community members who were chosen to participate have shared a variety of views on the causes of mental illness as well as their preferred approaches to treating individuals who are afflicted with mental illnesses. Participants stated that the community’s perception of mental diseases and their causes, along with socioeconomic status and educational level, affects how people affected are handled. There were no differences in the conclusions or arguments between the two approaches (FGD vs KII/IDI). Most of the participants agreed that someone might be diagnosed with mental illness if they display unusual behaviors that are different from what they were previously doing. The behaviors listed as unusual includes; aggression, strange behavior, irresponsibility, inability to marry and raise children, inability to work, affecting rich people, becoming increasingly ill throughout life, walking around naked, begging, wandering aimlessly, talking to themselves, self-neglect, and destructive behavior. According to the results, participants’ answers to questions about what constitutes mental illness, its origins, preferred forms of treatment, and the variables affecting those decisions show that there are many parallels and few differences.
Themes and Sub-Themes Identified from the Study
In response to the questions, the study’s results listed six sub-themes that were framed under the themes in accordance with the preferences of treatment, along with three primary findings that were thematically structured according to the reasons. These topics linked the concepts of community perceptions of mental disease, perceived causes, care preferences, and factors influencing those choices in patients who are mentally ill. The subjects that emerged from the data are broken down into sub-themes in Table 3 below.
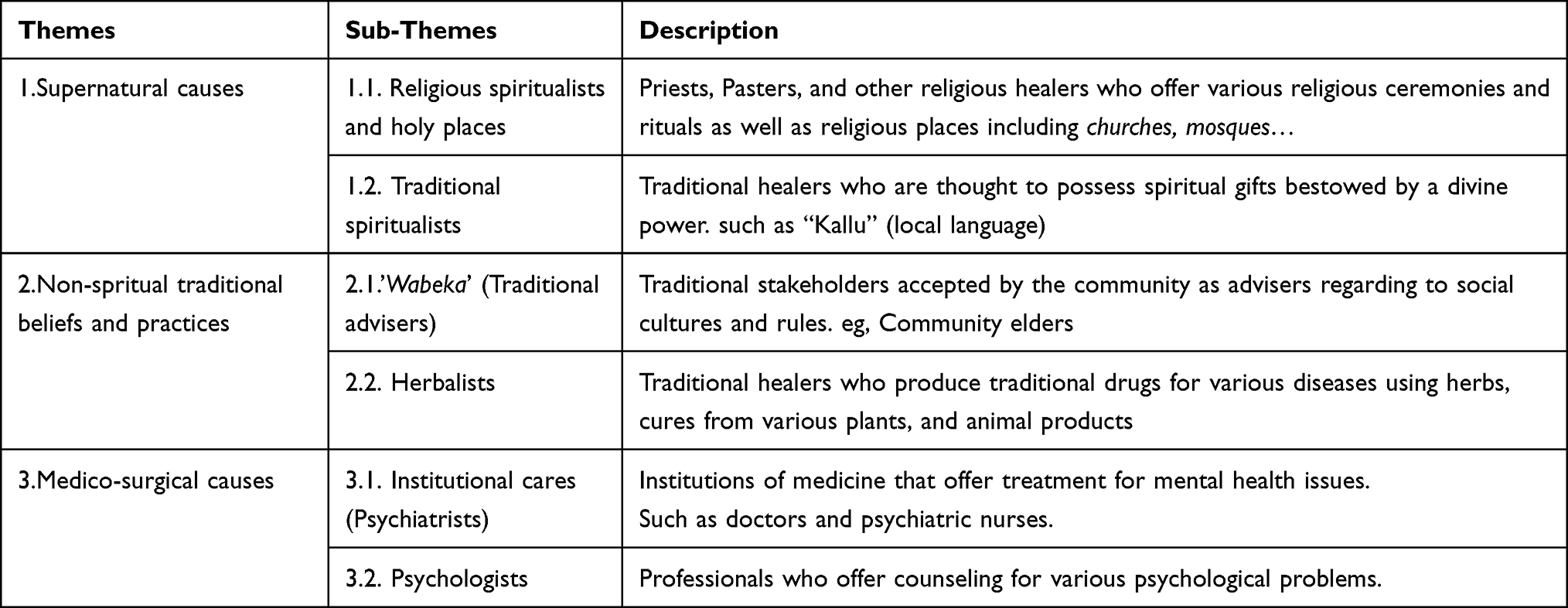 |
Table 3 Themes and Sub-Themes with Descriptions, West Shoa Zone Community, Oromia Region, Ethiopia, July 2022 |
Supernatural Causes
1.1. According to the study’s findings, the majority of those who took part in focus group discussions and in-person interviews (61%) agreed that the majority of people in the West Shewa Zone community thought that mental illness was more of a spiritual issue than a disease. This calls for the healing power of the divine, or of God. As a result, when they or a member of their family was diagnosed with a mental illness, they frequently turned to supernatural treatments as a last resort. The two sub-themes that fall under this theme are; 1. Religious spiritualists, and holy places; 2. Traditional spiritualists.
Religious Spiritualists and Holy Places
The vast majority of participants agreed that the devil’s work and bad spirits are both involved in mental illness as a problem. When someone breaks God’s rules and refuses to obey him, God may punish that person for their actions. They also highlighted two more ways that a person may be exposed to the devil and bad spirits. God might do this by sending them a wicked spirit, which can result in mental health problems. The second argument was that if someone loses God’s protection because they act in a way that goes against the morality of their faith as taught by religious preachers, they are then open to the devil, which can interfere with their capacity to think clearly. One participant exclaimed that
Living against God’s law, engaging in evil deeds, and disobeying his commands and his teachings all of this, as communicated by religious preachers, can lead to mental illness. (FGDs-Farmer, 33 Years old, rural)
The participants were also told,
We won’t have mental health problems if we conduct our lives in close accordance with God’s commands and have faith in him to guide us through all of life’s difficulties.
However, they asserted that the absence of God or the Holy Spirit, which results in disturbance and mental disease, is connected to depression, a lack of compassion for others, sadness, and aggressiveness. One of the participants as explained this:
If we violate God’s laws. if we commit evil acts that cause harm to another person, God will take h- is holy spirit from us, and we will experience signs of mental illness as a result, (KII-Self-employee/ Paster, 34 yrs., urban)
The occurrence of mental disease because of the bad people who resided in the neighborhood was the other topic to which participants responded. The terms “Buda [evil eye]”, “Tenkuay [wizard or witchcraft]”, and “Jinni [evil spirit]” are used to describe these people. The majority of our community (46%) favors spiritual (religious) healers as a result, according to many respondents who made this statement. One participant added, “Our community thought that since mental illness is a spiritual disorder linked to evil spirits and the devil’s activities, we obtain help and healing from Almighty God, who is capable of accomplishing anything and has answers for all issues”. The opposing party responded by saying, “Because of their beliefs regarding mental illness and its causes related to spirit, our community preferred religious settings and spiritual healing associated with religious rituals and duties as a first source for seeking care for mental ailments”. Another participant added, “Our community visits holy sites in order to be cleansed from this person’s immoral deeds and subsequently from mental health issues”. Participants believe that leading moral lives and adhering to God’s rules can give us a spirit of serenity and contentment that protects against disease and other health problems. As a result, the majority of communities do not go to places like medical institutions for treatment of mental health problems or disorders. They favor religious institutions and spiritual healers instead, since mental disease is brought on by evil spirits who cannot be seen by laboratory or other advanced investigations. One of the respondents (KII- Self-employee, 43 yrs., urban) as explained this
The best location for mental illness patients to receive care is by praying to God for assistance bec-ause anything is possible for him because he knows everything. The majority of our community pre-ffers sacred locations, and this is what I personally believe and accept.
In a similar vein, the other participant stated that:
…That individual can be healed from his or her mental disorder if he or she regrets his or her sin, re- pents, and seeks forgiveness, returns and lives according to religious teaching, seeking the face of God. (FGDs: 35-year-old rural merchant)
In addition, they prefer religious areas for a variety of reasons, including: they receive religious knowledge, counseling, and other supports; they frequently pray and fast in an effort to benefit their soul; and similar things. This was clarified by one of the participants as follows: “...in addition to that, they prefer religious areas for a variety of reasons, including that they receive religious knowledge, counseling, and other supports”. The further participant stated, “Except for those connected to meal, drink, or bed services, among other things, we are not charged for the religious services we get. Otherwise, we can receive free services from places of worship”. The participants explained for why they thought that their community’s viewpoint affected how they preferred to treat mental illnesses. The overwhelming majority of participants agree that the community prefers sacred places to seek mental health treatment. One of the attendees mentioned the other components of religious healing as being spiritual healers, sometimes known as prayers or men of God. In order to obtain sin forgiveness and so be relieved from the symptoms of mental health issues, a segment of the population also chose to go to such people for prayer and aid from a religious person. At churches, people look for priests, prophets, evangelists, pastors, and other spiritual healers: One of the participants (KII-Government worker, 43 yrs., urban) gave the following explanation:
Being free from sin and living in God’s spirit brought us serenity and contentment. Therefore, the majority of our people turn to churches, ‘Gedam [abbeys]’, ‘Tsebel [holy water]’, and religious fi- gures who are thought to have tremendous healing powers.
Traditional Spiritualists
However, society also thought that giving up ancestor worship, which parents and grandparents had taught and experienced themselves, was a component of mental illness because it went against cultural norms, values, and beliefs. This can result in a family or ancestor’s curse making the members or their siblings mentally ill. According to 15% of participants, the greatest choice for treating the mental disease that is associated with this condition is spiritual (traditional) healing. Those traditional spiritualists are referred to by the people as “Kallu” or “Abba Ayyaanaa”. The term “Kallu” is used to refer to traditional spiritualists who are regarded as having spiritual gifts. The community has been exposed to a variety of traditions in this instance, such as delivering the traditional gifts known as “Casa” and “Darara” to “Kallu”. These gifts include items like salt, clothing, cereal, lambs, grass, and others. To accomplish their objectives, they are given spiritual instructions and direction from “Kallu”. They will build a relationship with the ancestor spirit and be able to heal from mental illness if they heed these instructions and advice and repeat the ancestral worship or sacrifices of their parents or grandparents that they had previously ceased. One of the participants gave the following explanation:
It is a problem of living experiences that contradict spiritual rules and principles, so adjusting ones-elf is necessary with these spiritual rules and continuing what our parents and grandparents have been doing, including; regular and timely worship and sacrifices can provide healing from mental problems. (KII- ‘A-Gadaa, 53 years old, urban)
Despite the fact that everyone in the community agrees on the underlying causes, some people may choose to get treatment somewhere else. The majority of the population, as previously mentioned, agreed with one individual who asserted, “Mental disease is an issue of wicked spirits”. However, while some people prefer traditional spiritualists, the majority of people prefer religious spiritualists. One of the participants stated:
Traditional spiritualists have the power and gift to banish demonic spirits like ‘Setana [the devil],’ ‘Buda [the evil eye],’ and ‘Jinni [the evil spirit],’ which are responsible for impaired mental functions. (FGDs-self-employee, 42 yrs., rural)
Non-Spiritual Traditional Beliefs and Practices
“Wabeka [Traditional Advisers]”
As I said above, the reasons why certain members of the community choose one over the other are tied to how people think about mental illness and its causes. The participants discussed how a segment of the community believed that mental illness was a problem that could be brought on by excluding oneself from communal living practices, flouting social values and norms, and displaying disrespect for the sociocultural characteristics of the community, such as disrespecting elders or acting in an abnormal or unusual way in the community. This results in “Abarsa [curses]”, as they are known in the local language. Therefore, in those communities, the preferred healthcare professionals for mental health issues are traditional stakeholders or advisers, also called “Wabeka” in the local language. Following the spiritual (religious) healers, “Wabeka [Traditional Advisers]” is the second most frequently mentioned site by 19% of participants for locating care for mental illness in the neighborhood. There is some similarity between “Kallu” and “Wabeka”, however, “Wabeka” is more concerned with guiding the community toward the standards, values, and customs of the community than “Kallu” is, and its services are more focused on advising. “Kallu” is more concerned with spiritual gifts and powers. As a result, they influence society to reflect its traditions and ideas. Even religious people revere “Wabeka”, as opposed to “Kallu”. One respondent (FGDs, a government worker, 40 years old, rural) stated the belief of those in the community regarding the etiology of mental diseases who favor “Wabeka” as follows:
Mental illness is a problem that can arise when people show disrespect to elders who have more re-spect in the community, as well as if someone does something illegal in the community against cult- ure, beliefs, and religions.
The second reason “Wabeka” was preferred was that the community also thought that mental illness had arisen because of what is known as “Mora” in the local language. The participants claim that this is an act carried out by one person against another because they are envious of their friend or neighbor’s success, whether it be in terms of riches, education, or having more authority or standing in the community. As a result, the community believes that meeting with and receiving advice from “Wabeka” is the preferred setting for seeking treatment for mental illness. However, others believe that religious places are preferred for “Mora” in order to lessen its action. One of the participants described this as follows:
They believe that ‘mora’ (an incantation or sorcery) is one of the factors contributing to mental illn-ess. Then they suggest that ‘Wabeka,’ the traditional stakeholder in our community, is the solution. The greatest method of treating mental illness is to follow the advice of pertinent people of the com- munity. (FGDs, Farmer, 37 years old, urban)
Herbalist
Herbalists are expert traditional medical practitioners who can create herbal treatments for a wide range of ailments, including mental health conditions. Participants shared that traditional healers create traditional medicines using herbs, various plant remedies (such as garlic, ginger, ginseng, echinacea, and feverfew), and animal products (organs or parts of animals). A small percentage of participants (4%) mentioned that some community members also seek out traditional healers for mental illness therapy if they believe their condition is the result of evil individuals who are out to get them. According to one of the participants, the community also turned to traditional medicine for reasons mentioned as follows:“... it is easy to receive the traditional treatment and the administration is equally straightforward and for a short length of time”.
Medico-Surgical Causes
Institutional Care
Few participants (12%) mentioned the reasons that force the community to go to hospitals for mental health care. Lack of assistance from traditional or religious institutions, mental illnesses linked to long-term medical conditions, eating or drinking poisonous substances, and mental health problems caused by trauma such as RTA, head injuries, excessive bleeding, or an aneurysm were among them. One of the participants mentioned that,
People go straight to health treatment in this circumstance since they know the source of mental illness is recognized and that it is unrelated to any foul spirits or other allegedly traditional or spiritual factors.
Participants were also made aware of additional issues that prevent the community from receiving mental health care from medical facilities. Two participants mentioned it as follows:
One of the participants said,
One factor that prevents our patients from receiving medical care is the cost of medical care, and many treatments for mental health issues are not offered by hospitals but must be ordered from private pharmacies instead. (KII-School Director, 35 years in the city)
According to the second participant:
Most patients seeking treatment at hospitals, including the Amanuel hospital, find it difficult to make significant progress, and most of them discontinue taking their prescribed drugs. Other problems in- clude the adverse effects of the drugs recommended for mental illness, the lengthening of the app- ointment time as more drugs are taken, and the insufficient concern shown and given at this. (FGDs-Rural 42-year Merchant)
Psychologist
Only 4% of participants brought up the fact that some community groups, particularly those with better education levels and stable economic standing, choose psychological consultations for mental health difficulties as their final point. These community members more often link mental illnesses than spiritual factors to stress and depression. One of the participants noted, “If excessive stress, depression, drug or alcohol abuse, persistent and excessive alcohol use, or substance abuses are factors in the development of a mental disorder, psychologists are consulted”. “Some other factors that call for psychologists include mental disease associated with love, loss of loved ones, work-related stress, overthinking, losing our possessions, or mental illness due to psychological traumas like rape and kidnapping”. Professional guidance is therefore necessary rather than traditional or spiritual treatments for these disorders. A participant gave the following explanation: “People in that community believe that education is a gift from God as well, not only learning, and thus we must put their beliefs into practice”. One of the participants said, “Career is a skill that someone would learn via training. Humans are creatures of talent and knowledge”. Participants did note that the community does not have a good understanding of this profession, and even if it were needed, it would be difficult to access. The general descriptions of themes, sub-themes, and health care preferences for mental illnesses that emerged from the data are described in Table 4 below.
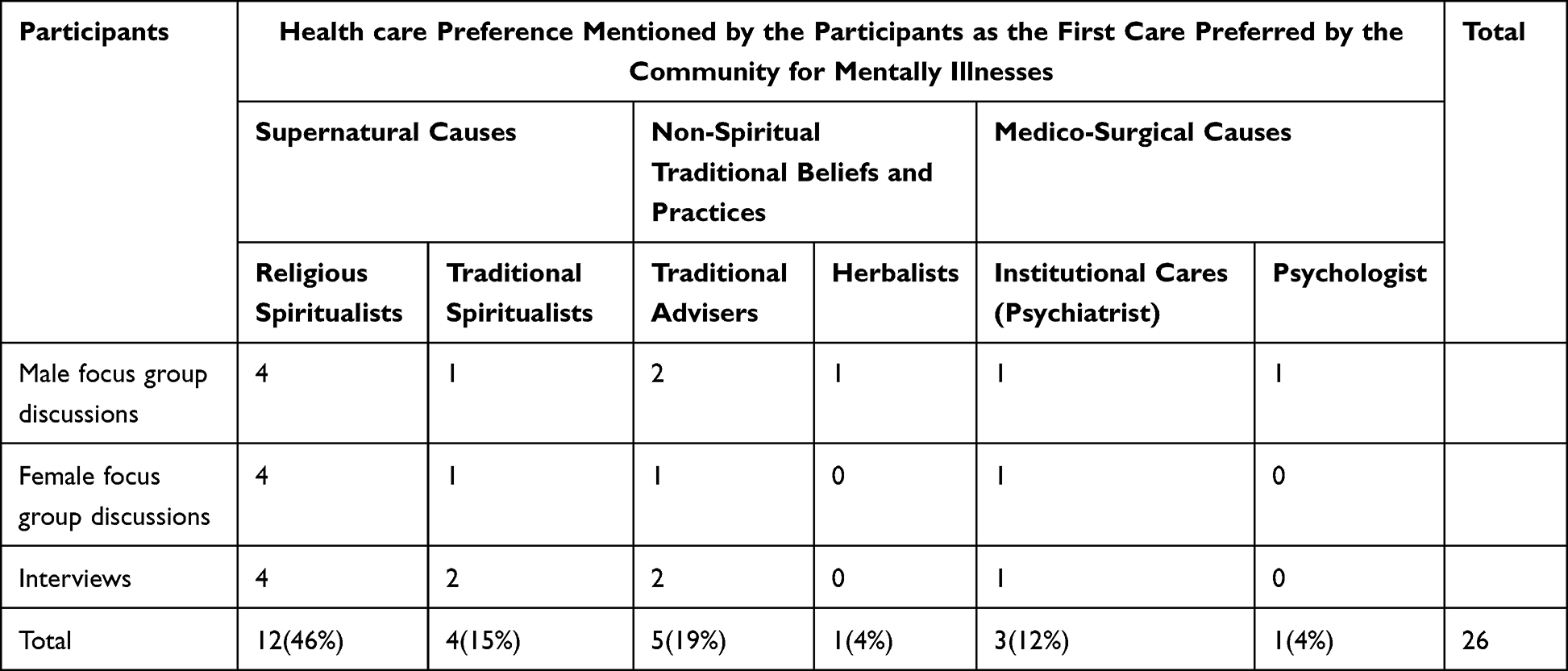 |
Table 4 Themes, Sub-Themes, and Health Care Preferences of Mentally Ill Patients, West Shoa Zone Community, Oromia Region, Ethiopia, July 2022 |
Finally, participants noted that, as was indicated in earlier discussions, a range of factors affect people’s preferences for treatment of mental health conditions. Age, education, financial condition, the pre-existing social and cultural framework of the community, attitudes toward professional care, and perceptions of mental illness were among the factors most frequently mentioned by participants.
Discussion
This is a type of qualitative research design used to investigate the influence of society’s norms, values, or cultures on people’s preferences for receiving treatment for mental health issues. This ethnographic study reveals specific treatment choices for mental illnesses within the West Shoa Community in Ethiopia’s Oromia Region. The findings of this study are connected to community beliefs about mental illness, perceived causes, and community preferences for health care for mental diseases in a specified study location, as well as factors that influence these preferences. The community participants in this study were asked about their choices for health treatment when they or a member of their family became ill. There are typically three central themes identified based on the causes of mental illnesses. This include; 1. Supernatural causes; 2. Non-spiritual traditional beliefs and practices; and 3. Medico-surgical difficulties.
The majority of participants’ responses indicated that someone could be diagnosed with mental illness if they display unusual behaviors that differ from what they used to do. The unusual behaviors described by the participants includes; walking around naked, begging, aimlessly wandering, talking to themselves, self-neglect, destructiveness, being lazy, unintelligent, worthless, stupid, unsafe to be with, always needing supervision, having depression, having a lack of tolerance, being impatient, and acting aggressively to others. Some of the symptoms listed in the study conducted on the Somali migrants in the USA were said to be similar. Participants in this study described mental illness primarily in terms of observable behaviors, such as: lack thereof, someone who does not know what they are talking about or where they are going, talking incoherently, talking to people who are not present, talking too loudly, or saying nothing when a response would have been appropriate. This is similar to how participants in our study described mental illness.11 Most interviewees claimed that the community did not regard mental health concerns as medical conditions that needed to be treated, but rather as spiritual difficulties or illnesses connected to the devil. This result is in line with that of an Indian cross-sectional study, which found that 31.6% of rural inhabitants and 50% of urban residents had the same opinion.2
More than half of the participants in this poll said that supernatural causes, such as the devil’s interference because of participating in wicked or immoral behavior or missing God’s protection, were
the primary causes of mental diseases. Participants claimed that breaking God’s commandments, performing evil activities, and disregarding his commands as revealed through religious preachers could lead to mental illness. As a result, the community began to notice odd behaviors that are indicative of mental health problems. The results of the survey done in the USA ran counter to this conclusion. Many participants in the USA study compared mental illness to intellectual and developmental prowess because they believed that mental disease was related to one’s mental prowess. In other words, those who struggled with their mental health tended to be less bright and to have developmental disabilities.12 The results of our investigation do not agree with the conclusions of the Indian study. The difficulties rose in the Indian study, such as decreased sex desire (23.7% rural, 18% urban), loss of vaginal secretion or semen (33.9% rural, 8.6% urban, and 1.3% professionals), and air pollution (51.5% rural, 11.5% urban, and 5.2% professionals) were not taken into account in this study. The consistency of our findings with a qualitative research conducted in Addis Ababa and Asella, Ethiopia, is another instance.2,8
Our findings also clarified how the other participants perceived how individuals known as “Buda” (the evil eye), “Tenkuay” (wizard or witchcraft), and “Jinni” (the evil spirit) are to blame for mental illness. Those people are viewed as either having divine power or serving as the devil’s wrathful agents. The community also believed that abandoning ancestral worship, which your parents and grandparents had instilled in you and which they had practiced themselves, was a source of mental illness because it went against conventional norms, values, and beliefs. These results are also consistent with earlier research done in Addis Ababa and Asella, Ethiopia.8 The participants also discussed how social exclusion, disregarding social values and norms, and disrespecting sociocultural aspects of the community, such as disrespecting elders or engaging in abnormal, out-of-The-ordinary behaviors in the community, are problems that might arise as a result of the other perceived causes of mental illnesses. The study on Somali refugees in the USA also disputed this finding. Most of the participants agreed that the most frequent reason given for mental illness was the loss of a family member who had experienced trauma, an untimely death, or both.11 Few study participants agreed that: medical conditions, consuming poisonous foods or beverages, traumatic events like car accidents, head injuries, excessive bleeding, excessive thinking, economic stress, loss of a loved one, worrying excessively or developing obsessive fears, as well as substance or drug abuse, can also be considered as causes of mental health issues.
These results are at odds with research from Rwanda and a comparative cross-sectional quantitative community-based survey conducted in Eastern Ethiopia’s Harari Region, which discovered that the participants’ most frequent references to these believed causes were in the studies’ respective countries.10,13
According to this study, the community’s perceptions of mental diseases and their causes influence how those people want to be treated. The majority of participants (46%) reported that religious spiritualists and religious rituals are their top choice of health care preferences, followed by traditional advisers, or “Wabeka”, according to the study’s findings on preferences for mental illness care. This outcome is also consistent with the research Amy Tiberi and Waganesh A. Zeleke conducted in Ethiopia.4 However, it conflicted with a study conducted in Addis Ababa and Asella by Nicole M. Monteiroa and Shyngle Kolawole Balogun, which found a combination of modern and traditional therapy to be the most effective treatment for mental disease.8 Participants claimed that religious rituals and spiritualists are the most efficient means of driving off evil spirits, which is beneficial for those with mental health problems.
The study also revealed that, the second most often cited alternative care preference, cited by 19% of participants, is “Wabeka [traditional advisor]”. With the exception of a few minor commonalities with “Kalu”, such members are seen differently because of their knowledge and experiences as community consultants and as almost non-spiritual people. They were admired and embraced even by religious people. As was already established, participants cited curses as the second causal agent for actions that excluded them from community living, such as insulting elders and acting strangely or unusually in public. As a result, if the community believed that these factors contributed to mental illnesses, they would consult traditional counselors, or “Wabeka”, for advice and directives before acting on what they said to recover from mental illnesses. The third most preferred method of care, according to participants, is traditional spiritualism (15%). The people as “Kallu” or “Abba Ayyaanaa” refer to those traditional spiritualists. The term “Kallu” refers to traditional spiritualists who seen as having spiritual gifts. These are usually preferred if the mental diseases’ purported cause is linked to giving up ancestor devotion. In this case, the society has been exposed to a variety of traditions, such as the tradition of frequently giving gifts. These findings are also in the same vein as the previous studies conducted by Amy Tiberi and Waganesh A. Zeleke in Ethiopia.4
Some community groups (12%), notably those with higher education levels and stable economic standing, have been described as preferring institutional care for mental illness. Psychiatrists’ counseling and the use of mental health drugs are part of this care. Participants in this case agreed that when mental health issues are closely linked to physical ailments and other diseases with known concrete causes, such as trauma, those institutions should be in charge of providing care for the community’s mental health issues rather than spiritual or traditional healers. This finding was also supported by the study done in china; that is, individuals exposed to and influenced by Western norms and practices held more positive attitudes toward seeking professional help and actually used more mental health services.14 Additionally, if they are unable to find improvement in traditional and religious settings, they eventually turn to institutions. This outcome is consistent with a prior study carried out in Eastern Ethiopia, the Harari Region, Addis Ababa, and Asella.8,13 Lastly, a small number of participants raised the issue of how some community groups, who are also educated and have good incomes, prefer psychological consultations (4%) for mental health problems. Those participants explained that mental illnesses related to excessive stress, depression, substance abuse, drug abuse, chronic and excessive alcohol consumption, mental illnesses related to love, losing his or her love, work overload, overthinking, and losing property need psychological consultations. The remaining 4% of people look for traditional healers who make their medicines from scratch using a variety of herbs, plant-based remedies, and animal extracts.
Participants noted as a conclusion that despite the presence of numerous health care systems in the neighborhood, the population’s preference for care is affected by a variety of circumstances. The majority of participants listed age, educational level, economic standing, the preexisting social and cultural system of the community, community beliefs regarding mental illness, and attitude toward professional care as determining factors of care preference for mentally ill patients. Other factors included community beliefs regarding mental illness and attitudes toward professional care. The majority of participants from the district residence claimed that cultural norms, beliefs, and values commonly influence how much reliance communities place on traditional and religious healers as well as self-care or at-home care. The study found that, in addition to the characteristics already mentioned, perceptions of the source of mental illness have been connected to preferences for receiving care.
Strengths and Limitations of the Study
This study’s reliance on community stakeholders and their families, who make up the bulk of participants rather than individuals with mental illnesses, places it at a disadvantage. The study period was too short for this ethnographic study to be considered fully engaged in the community, which was another negative. The study’s originality in this field of study is its benefit because there has not been prior research on this subject. Another aspect of this study is the consideration of maximal variation to elicit a range of opinions and the triangulation of several data collection methods.
Conclusions and Recommendations
According to the study’s findings, the majority of people in the research area considered mental illnesses to be spiritual problems that needed to be treated via religious rituals and obligations rather than by seeking medical care. According to this survey, those societies’ most frequent perceptions of the causes were evil spirits, demonic activities, and engaging in behaviors that were against social norms and laws. Religious spiritualists were shown to be the most favored caregivers for mental illness in the study area, followed by traditional counselors (known as “Wabeka”, traditional spiritualists, and institutional treatment. The factors that were most commonly mentioned as determining the preferences for health care among mentally ill patients were their educational level, financial situation, and the pre-existing social and cultural framework of the society. This study suggests collaboration and a shared strategy between health care professionals, traditional and religious stakeholders to emphasize their services in addressing mental health issues. As evidenced in this study, traditional and religious practices and beliefs are deeply ingrained in the community. A link or referral system between traditional and modern care should also be developed, as well as improving community health insurance, expanding access to low-cost mental health services at neighboring medical institutions, and more. Due to the fact that the study’s scope was limited to our nation, more research is required in order to better understand how the community views mental diseases and to raise community understanding of their causes and available treatments. Our understanding of the phenomenon of mental health care preferences among people who have lived outside the study region will also be advanced by this research.
Abbreviations
DALYs, Disability-adjusted life years; FGDs, Focus Groups Discussions; KIs-Key Informants; LLC, Low Level Countries; PP, Patient Preferences; PTSD, Post-traumatic stress disorder; SPHMMC, Saint Paul’s Hospital Millennium Medical College; SSI, Semi-structured Interviews; WHOs, World Health Organization’s.
Data Sharing Statement
The authors will freely share the raw data that underlies the results of this article.
Ethical Issue
The district government representatives were informed about the study and given formal authorization. The SPHMMC Ethical Committee formally approved the research protocol. The study objectives were conveyed to community representatives and other notables before community members were interviewed, and their consent was obtained. Additionally, everyone who took part gave his or her consent to be interviewed. Each participant provided both written and verbal informed consent, which included permission to publish his or her anonymous comments. All paper copies and computer-based data were maintained in a secure location with the PI, and the forms did not include any names. To protect the participants’ confidentiality, no identifiable personal information was published in this report. The Declaration of Helsinki served as the foundation for this investigation.
Consent for Publication
The participants agreed to the publication of their opinions and gave their formally written consent.
Acknowledgment
We thank Saint Paul’s Hospital Millennium Medical College (SPHMMC) for giving us the chance to conduct this study in conjunction with them and for their ongoing support as we worked on the thesis. Additionally, we would like to thank the research assistants who assisted us, particularly Mr. Takele Gezahegn (MPH, Coordinator, Research and Publication Office), who has been supporting and encouraging us.
Author Contributions
Mr. Getachew Adela Kasa made direct and important contributions that had a big impact on the study’s concept, design, data collection, analysis, and interpretation. Dr. Mirgissa Kaba, M.D., contributed significantly to the work that was reported, notably by heavily revising and analyzing the article. In general all authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there is no conflicts of interest in this work.
References
1. Larsen A, Tele A, Kumar M. Mental health service preferences of patients and providers: a scoping review of conjoint analysis and discrete choice experiments from global public health literature over the last 20 years (1999–2019). BMC Health Serv Res. 2021;21(1):1–13. doi:10.1186/s12913-021-06499-w
2. Kishore J, Gupta A, Jiloha RC, Bantman P. Myths, beliefs and perceptions about mental disorders and health-seeking behavior in Delhi, India. Indian J Psychiatry. 2011;53(4):324–329. doi:10.4103/0019-5545.91906
3. Grob GN, Grob GN. Defining ‘mental illness’ in mental health policy. Health Aff. 2006;25:737–749. doi:10.1377/hlthaff.25.3.737
4. Hughes TL, Quinn C, Tiberi A, Zeleke WA. Developing a framework to increase access to mental health services for children with special needs in Ethiopia. Front Sociol. 2020;5:1–6. doi:10.3389/fsoc.2020.583931
5. Szasz T. The myth of mental illness. Am Psychol. 1960;15(2):113–118. doi:10.1037/h0046535
6. Dogra N. Defining Mental Health and Mental Illness. CRC Press; 2014:2009.
7. Nsereko JR, Kizza D, Kigozi F, et al. Stakeholder’s perceptions of help-seeking behaviour among people with mental health problems in Uganda _ international journal of mental health systems _ Full Text. Int J Ment Health Syst. 2011;5:1–9. doi:10.1186/1752-4458-5-1
8. Monteiro NM, Balogun SK. International journal of culture and perceptions of mental illness in Ethiopia: a profile of attitudes, beliefs and practices among community members, healthcare workers and traditional healers. Int J Cult Ment Health. 2013;37–41. doi:10.1080/17542863.2013.784344
9. Shaikh BT, Haran D, Hatcher J. Where do they go, whom do they consult, and why? Health-Seeking behaviors in the northern areas of Pakistan. Qual Health Res. 2008;18(6):747–755. doi:10.1177/1049732308317220
10. Muhorakeye O, Biracyaza E. Exploring barriers to mental health services utilization at kabutare district hospital of rwanda: perspectives from patients. Front Psychol. 2021;12:638377. doi:10.3389/fpsyg.2021.638377
11. Bettmann JE, Penney D, Clarkson Freeman P, Lecy N. Somali refugees’ perceptions of mental illness. Soc Work Health Care. 2015;54(8):738–757. doi:10.1080/00981389.2015.1046578
12. Harris J, Crumb L, Crowe A, McKinney J. African Americans’ perceptions of mental illness and preferences for treatment. J Couns Pract. 2020;11(1):1–33. doi:10.22229/afa1112020
13. Gari H, Mulugeta G, Tesfaye D, Fitsum W, Assefa T. Prevalence and determinants of common mental illness among adult residents of Harari regional state, Eastern Ethiopia. Pan Afr Med J Conf Proc. 2017;8688:1–16. doi:10.11604/pamj.2017.28.262.12508
14. Chen SX, Mak WWS. Seeking professional help: Etiology beliefs about mental illness across cultures. J Couns Psychol. 2008;55(4):442–450. doi:10.1037/a0012898
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.