Back to Journals » Advances in Medical Education and Practice » Volume 6
Predictors of self-reported academic performance among undergraduate medical students of Hawassa University, Ethiopia
Authors Gedefaw A ![]() , Tilahun B
, Tilahun B ![]() , Asefa A
, Asefa A
Received 3 December 2014
Accepted for publication 14 February 2015
Published 9 April 2015 Volume 2015:6 Pages 305—315
DOI https://doi.org/10.2147/AMEP.S78604
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Md Anwarul Azim Majumder
Abel Gedefaw,1 Birkneh Tilahun,2 Anteneh Asefa3
1Department of Gynecology and Obstetrics, 2Department of Pediatrics and Child Health, 3School of Public and Environmental Health, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia
Background: This study was conducted to identify predictors of self-reported academic performance in undergraduate medical students at Hawassa University.
Methods: An analytical cross-sectional study involving 592 undergraduate medical students was conducted in November 2012. The academic performance of the study subjects was measured by self-reported cumulative grade point average (GPA) using a self-administered questionnaire. Data were entered and analyzed using Statistical Package for the Social Sciences version 16 software. Pearson's bivariate correlations, multiple linear regression, and multiple logistic regression were used to identify predictors of academic performance.
Results: The self-reported academic performance of students had been decreasing as the academic years progressed, with the highest and lowest performance being in the premedicine (mean GPA 3.47) and clinical I (mean GPA 2.71) years, respectively. One hundred and fifty-eight (26.7%) of the participants had ever been delayed, 37 (6.2%) had ever re-sat for examination, and two (0.3%) had ever been warned due to academic failure. The overall variation in self-reported academic performance of the students was 32.8%. Participant age alone explained 21.9% of the variation. On the other hand, university entrance examination results, substance use at university, and medicine as first choice by students were identified as predictors of variation in self-reported academic performance, accounting for 6.9%, 2.7%, and <1% of the variation, respectively. Students who had never used tobacco, alcohol, or khat after starting university were twice as likely to score a self-reported cumulative GPA above 3.0 (adjusted odds ratio 1.95, 95% confidence interval 1.25–3.02) and less likely to be delayed, have to re-sit an examination, or be warned (adjusted odds ratio 0.47, 95% confidence interval 0.29–0.77).
Conclusion: Only 32.8% of the variation in self-reported academic performance was explained by the studied variables. Hence, efficacious mechanisms should be designed to combat the intervenable determinants of self-reported academic performance, like substance use and a low medical school entrance examination result. Further studies should also be undertaken to gain a better understanding of other unstudied determinants, like personality, learning style, cognitive ability, and the system used for academic evaluation.
Keywords: predictors, academic performance, medical students, Ethiopia
Introduction
Academic performance is a key component of medical education that is used by governing bodies like ministries of education and health and universities to assess whether a medical graduate is sufficiently competent and fit to practice medicine.1,2 It is also used to identify students who are displaying the appropriate level of competence, to enable students to ascertain their own academic progress, and to predict the future performance of students.1,3 The purpose of medical education is to ensure that students meet the ethical, clinical, technical, and scientific standards expected of a good physician.4 Therefore, academic performance of medical students should be evaluated continuously.5
In developed countries, various studies have revealed that a number of factors affect the academic performance of undergraduate medical students. Prior academic achievement, such as medical school entrance examination result,6,7 cognitive ability,8,9 personality,10,11 learning style,12 and stress at medical school8 were among the identified factors. There is a scarcity of scientific evidence on determinants of academic performance among medical students in developing countries like Ethiopia. However, studies done on substance use among university students found that use of substances like khat and cigarettes negatively affected academic performance.13,14
Khat is a stimulant drug derived from a shrub (Catha edulis) found in Eastern Africa and Southern Arabia. Leaves of the khat shrub are held in the cheek or chewed as gum, and release their stimulants cathinone and cathine. These chemicals are structurally similar to amphetamine and have a similar stimulant effect on the brain and body.15
Ethiopia, one of the developing countries in Eastern Africa, suffers from a shortage of health professionals, particularly physicians. According to the 2011/2012 report of the Federal Ministry of Health, the physician to population ratio was 1:28,847.16 This figure is far below the international standard recommendation of 1:10,000.17 Recently, the Ministry of Education, as well as the Ministry of Health, in Ethiopia aimed to increase the number of physicians by opening new medical schools to increase the number of medical students.18,19 Despite the increased intake of medical students each year, the number of students graduating from these schools is still not as high as needed, largely due to a high attrition rate. Attrition is of concern, because it is a waste not only of the students’ time, effort, and money, but also for medical academic institutions and the government.20
As it is normal for some students in an educational institution to perform well while others do poorly, even after receiving the same services, researchers are curious to know what makes some students perform poorly. The findings of the current study would help in assisting policy-makers and implementers to come up with policies and strategies that can be employed to improve academic performance, in addition to generating evidence about predictors of self-reported academic performance among medical students in Ethiopia. Hence, this study aimed at identifying the predictors of academic performance in undergraduate medical students.
Materials and methods
This study was conducted among undergraduate medical students of Hawassa University (HU, a public university established in 1999) in Hawassa City, the capital city of the Southern Nations Nationalities and People’s Region of Ethiopia. The university has a total of five campuses. It is one of the 32 public universities in Ethiopia, and is engaged in the provision of all-round education, research, and training.
Formal training of medical professionals at HU began in 2003 with the opening of the College of Medicine and Health Sciences (CMHS) and its tertiary teaching hospital, ie, Hawassa University Referral Hospital. At the time of the study, the college had an annual acceptance of 150–200 medical students. Medical students are admitted to the school as per the national criteria set by the Federal Ministry of Education, which are mainly based on students’ performance in the Ethiopian National Higher Education Entrance Examinations.21
New medical students joining the CMHS at HU initially attend general courses for 6 months in the premedical training program before embarking on the preclinical academic years, ie, preclinical I (year 1) and preclinical II (year 2). All medical students completing preclinical and clinical training, ie, clinical I (year 3) and clinical II (year 4), are required to successfully pass through a 1-year internship program in order to graduate. In general, the duration of undergraduate medical training has a curriculum of 5.5 years. Until the end of 2013, the medical school has graduated more than 340 general medical practitioners.
The curriculum of the medical school during the study period includes the basic medical courses in the preclinical years (years 1 and 2) while the clinical courses are usually covered in the subsequent three years (clinical I, II, and internship). The student evaluation system includes written examinations, oral examinations, individual and group assignments, practical examinations, and progressive assessment. Students are expected to score at least 60% to pass each course. Students who fail to achieve 60% in the basic and clinical courses need to repeat the course or re-sit an examination based on individual academic records.
The grading system of the school is based on the fixed scale system of HU with 85%–100% (A), 80%–84.9% (B+), 70%–79.9% (B), 65%–69.9% (C+), 60%–64.9% (C), 55%–59.9% (D+), 50%–54.9% (D), and less than 50% (F). According to the system, A has a score of 4.0 whereas B+, B, C+, C, D, and F have scores of 3.5, 3.0, 2.5, 2.0, 1.0, and 0, respectively. Accordingly, the maximum and the minimum cumulative grade point average (GPA) a medical student can achieve will be 4.0 and 0, respectively.
Study design and participants
This analytical cross-sectional study, which used a quantitative data collection method, involved all medical students who had at least one semester GPA (year 1 to internship program) at the CMHS. Medical students who did not have at least one semester GPA were excluded.
Variables
The dependent variable (academic performance) was measured by students’ self-reported cumulative GPA for the current academic year.22 The independent variables were: prior academic performance (university entrance examination result and type of high school), sociodemographic characteristics (age, sex, maternal educational level, paternal educational level, original background, and allowance per month), personal characteristics (choice of medicine as first interest, substance use before and after joining university, history of academic withdrawal, duration of study at university, usual number of sleeping hours per day, estimated length of time spent on extracurricular activities, and missing academic activities).23
Academic performance was dichotomized into good and low based on the mean cumulative GPA and/or presence of academic delays, experience of re-sitting examinations, and academic warnings.24,25
Substance use in this study represented the use of at least one of chewing khat, smoking cigarettes, or alcohol use in the 30 days preceding the study period.
Data collection and analysis
A self-administered, pretested, structured questionnaire prepared in English was used for data collection, since English is the medium of instruction in all higher education institutions in Ethiopia. Most of the questions were close-ended with precoded responses, and mainly grouped into sociodemographic characteristics, earlier school performance and characteristics, behavioral characteristics, and academic performance and GPA in each academic year. The questionnaire was developed by the authors after reviewing the relevant literature on the subject. Based on their training background, students were divided into two main categories: preclinical (years 1 and 2) and clinical (years 3 and 4 and internship). To minimize the non-response rate, data were collected for each batch of students immediately after they finished written examinations or after bedside teaching; the data collection was conducted in lecture halls. Data collectors as well as the supervisors were trained assistant lecturers from other campuses at HU. Instructions on how to complete the questionnaire correctly, particularly on how to follow skip patterns, was given to the study subjects before embarking on completing the questionnaire. After the questionnaires were collected back from the students, the supervisors checked all questionnaires for completeness.
Data were entered, cleaned, and analyzed using Statistical Package for the Social Sciences version 16 software (SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to summarize and present the data. To determine the relationship between self-reported academic performance and the different independent variables, bivariate Pearson’s correlation analysis was done three times (for total participants, and for preclinical, and clinical student subcategories). Multiple linear regression was used to estimate the cumulative and individual effects of each independent variable as well as to control confounding effects.
To explain the variability of the outcome variable according to the explanatory variables and identify the effects of confounding, three multiple linear regression analyses were constructed for total participants, clinical, and preclinical students. Out of the 20 explanatory variables, we used a backward selection procedure to test several combinations of these variables and used a model that gives us the largest adjusted R2 and the smallest standard error. Regression diagnostics were done for the fitness of model. The correlation between each of the explanatory variables was less than 0.7, and the variance inflation factor was ≤5. Moreover, linearity and other assumptions were guided under the umbrella of central limit theory because the sample size was very large.
For the logistic regression models, a P-value <0.2 was taken as a cut-off point for selecting variables to enter into the multiple logistic regression model. A probability value of <0.05 was considered to be statistically significant.
Ethical considerations
Ethical approval was obtained from the institutional review board at CMHS. Further, permission letters were presented to all responsible units in the CMHS to seek permission to engage in data collection. Participation of the students was on a voluntary basis. Written informed consent was obtained after the purpose of the study was explained to the students in their specific subcategories. Identifiers of the study participants were not recorded anywhere on the questionnaire, and appropriate measures (adequate spacing between individuals during completion of the questionnaires, recruiting data collectors, and supervisors from other campuses) were taken to ensure confidentiality of information.
Results
During the study period, a total of 770 undergraduate medical students were registered in the medical school. However, 150 students were in their premedical study period so were excluded from the study as they did not have any GPA. Of the 620 students invited, 610 participated in the study, giving a response rate of 98.4%. Questionnaires from only 592 students were used for the study; questionnaires for 18 students were discarded because of incomplete responses.
Of the total number of respondents, 36.3% were in the preclinical years, and the remaining 63.7% were in the clinical years. More than three-quarters (79.9%) of the participants were male, and the mean age of the participants was 22.16±1.85 years. Participants reported an average monthly allowance of 19.8±14.7 USD; males reported a smaller allowance than females (17.5 USD versus 29 USD, respectively, P<0.0001, Table 1).
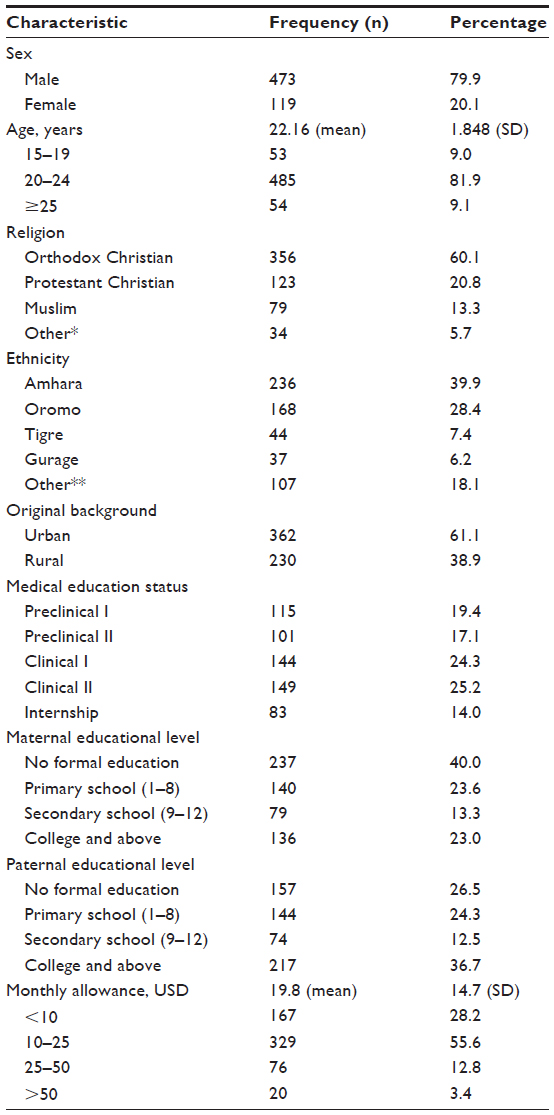 | Table 1 Sociodemographic characteristics of undergraduate medical students at College of Medicine and Health Sciences, Hawassa University, November 2012 |
With regards to preuniversity history, more than three quarters (77.9%) of participants completed their high school education at a government school and the average self-reported university entrance examination result was 72%±3.97%. There was a statistically significant difference between the mean entrance examination results of male and female students (72.4% versus 71.2%, respectively, P=0.009). Of the total number of participants, only 33 (5.6%) had ever used any substance before starting university, while about a quarter (24.2%) used any substances during the data collection period. Khat was the most commonly used substance, followed by alcohol and cigarette smoking. When substance use was disaggregated by academic year, the proportion of substance users increased with increment in academic year. The students’ mean lengths of time usually spent studying, sleeping, and on extracurricular activities in 24 hours were 7.9±2.8, 6.96±1.22, and 3.2±1.74, respectively, Table 2).
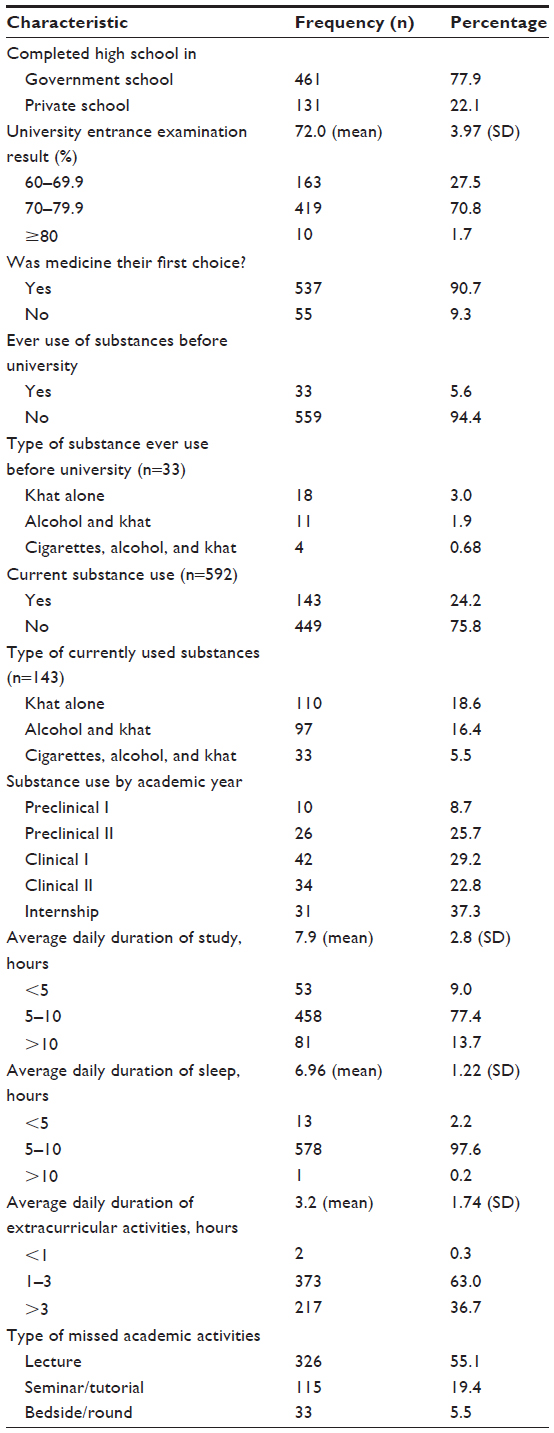 | Table 2 Former high school background and behavioral characteristics of undergraduate medical students at College of Medicine and Health Sciences, Hawassa University, November 2012 |
Forty-seven participants (7.9%) had been in medical school for more than 6 years. Self-reported academic performance had been decreasing as the academic years progressed, with the highest and lowest performance being in premedicine (mean GPA 3.47) and clinical I medicine (mean GPA 2.71), respectively. The mean current self-reported cumulative GPA of the participants was 3.08±0.38; more than half (61.7%) of the students had a cumulative GPA ≥3.0, and there was no difference in cumulative GPA between female and male students (3.08 and 3.09, P=0.804). However, there was a statistically significant difference in cumulative GPA between clinical and preclinical students (2.95 and 3.31, P=0.000, Table 3).
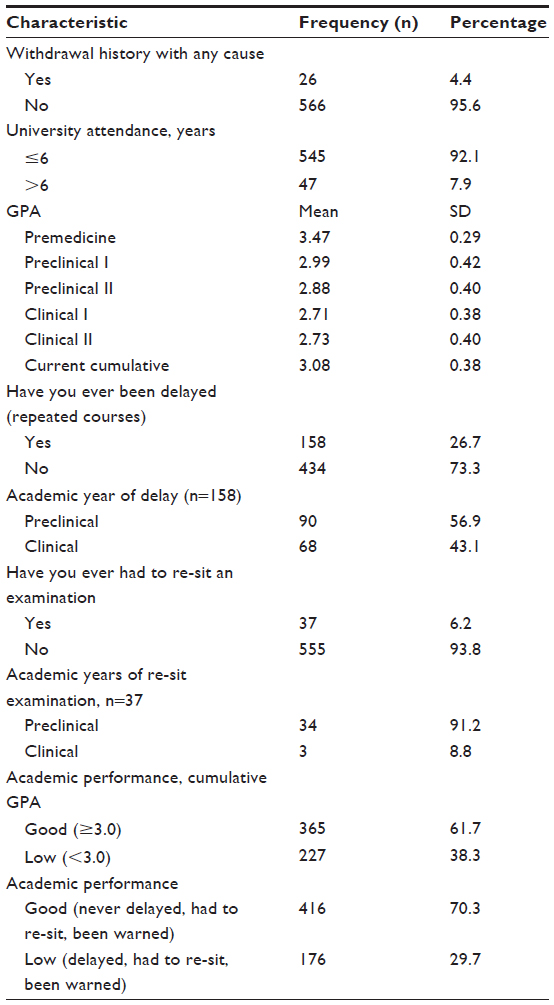 | Table 3 Patterns of academic performance among undergraduate medical students at College of Medicine and Health Sciences, Hawassa University, November 2012 |
More than a quarter of the participants (26.7%) had ever been delayed (needed to repeat a course) in their time as medical students, but few (6.2%) had needed to re-sit an examination. Self-reported academic performance was good for 61.7% of the students (cumulative GPA ≥3.0). Low academic performance (delay, re-sit, and/or warning) was reported by 29.7% of the students (Table 3).
According to the bivariate Pearson’s correlation analysis, seven of the independent variables had a significant correlation with self-reported academic performance. Age (r=−0.469, P=0.000), university entrance examination results (r=0.356, P=0.000), substance use at university (r=−0.219, P=0.000), and missing of bedside/round sessions (r=−0.398, P=0.000) were moderately correlated, and history of withdrawal from academic activity (r=0.094, P=0.022), missing lectures (r=0.111, P=0.007), and missing seminars/tutorials (r=0.147, P=0.000) were weakly correlated.
Similar correlation analyses were done for subgroups (clinical and preclinical years): age (r=−0.540, P=0.00), university entrance examination results (r=0.390, P=0.00), substance use at university (r=0.261, P=0.000), missing lectures (r=0.168, P=0.001) and missing seminars/tutorials (r=−0.091, P=0.020) had a statistically significant correlation with academic performance among the preclinical students. Only three variables, ie, history of withdrawal from academic activity (r=0.18, P=0.036), university entrance examination results (r=0.240, P=0.000), and medicine as first choice (r=−0.139, P=0.035) had a statistically significant correlation with academic performance in the clinical years.
The identified independent variables explained 32.8% of the variation in academic performance (R2=0.328, P=0.000). Four variables (participant age, substance use at university, university entrance examination results, and medicine as first choice), accounted for the statistically significant variation in self-reported academic performance. Multiple linear regression analyses for subgroups revealed that the aforementioned independent variables explained 30.1% and 14.7% of the variation in self-reported academic performance for preclinical and clinical year students, respectively (Table 4).
 | Table 4 Bivariate correlation between independent variables and academic performance among undergraduate medical students at College of Medicine and Health Sciences, Hawassa University, November 2012 |
Stepwise multiple linear regression analysis was also done for all the participants. Participant age alone explained 21.9% of the variation in self-reported academic performance. University entrance examination results, substance use at university, and medicine as first choice explained 6.9%, 2.7%, and <1% of variation in academic performance, respectively. Considering type of substance used versus academic performance, the mean cumulative GPA of substance users was found to be less than that of non-users (alcohol, 2.96 versus 3.12, P=0.000; khat, 2.91 versus 3.12, P=0.000; cigarettes, 2.90 versus 3.12, P=0.007).
To express the strength of relationship in a more interpretable way, bivariate and multivariate logistic regressions were done. Students who have never used any substances at university were twice as likely to have scored a self-reported cumulative GPA of 3.0 and above (adjusted odds ratio [AOR] 1.95, 95% confidence interval [CI] 1.25–3.02) and less likely to have been delayed, to have had to re-sit, and/or be warned (AOR 0.47, 95% CI 0.29–0.77) than their counterparts. Those students whose university entrance examination result was 66%–70% (AOR 3.05, 95% CI 1.25–7.47) and 71%–75% (AOR 3.81, 95% CI 1.91–4.29) were more likely to have scored a self-reported cumulative GPA of 3.0 and above than students whose entrance examination result was ≤65% (Table 6). When the predictive validity of university entrance examination results as a predictor of self-reported academic performance was tested using a receiver operating characteristic curve, the point of the curve that was closer to the left upper quadrant of the x-y axis yielded a sensitivity of 0.61 and 1 – specificity of 0.33. The threshold point that minimizes the trade-off between the sensitivity and specificity of the university entrance examination result was at 72.25%. The area under the receiver operating characteristic curve was found to be 0.68 (95% CI 0.64–0.73). Although the university entrance examination result was associated with the student’s self-reported academic performance, an area of 0.68 under the receiver operating characteristic curve implies that the university entrance examination result was poor in setting the threshold for a dependent variable, in this case self-reported academic performance. We also noted an association between participant age and academic performance, with the odds of having a self-reported cumulative GPA ≥3.0 being 70% less for students aged older than 22 years (AOR 0.30, 95% CI 0.20–0.44) when compared with their younger counterparts (Table 5).
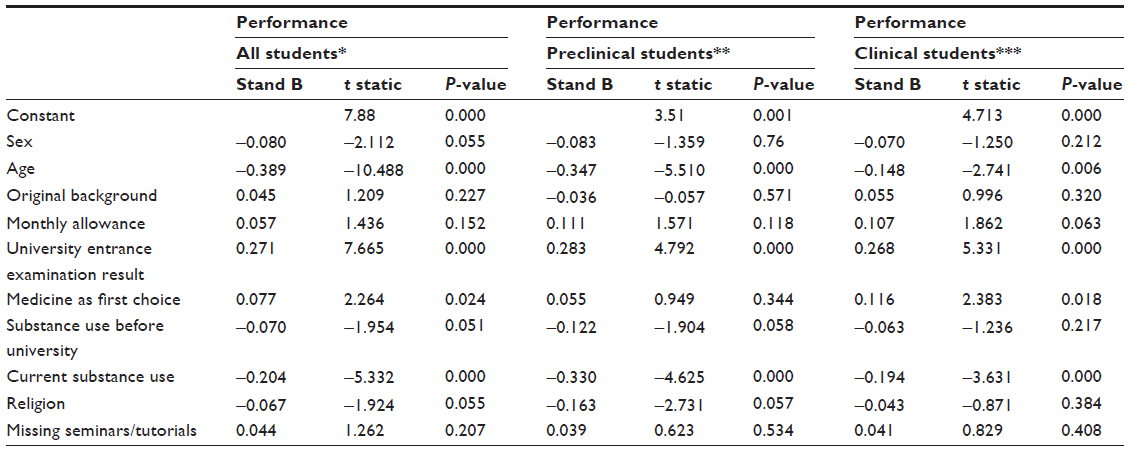 | Table 5 Results of multiple linear regression analysis of academic performance among undergraduate medical students at College of Medicine and Health Sciences, Hawassa University, November 2012 |
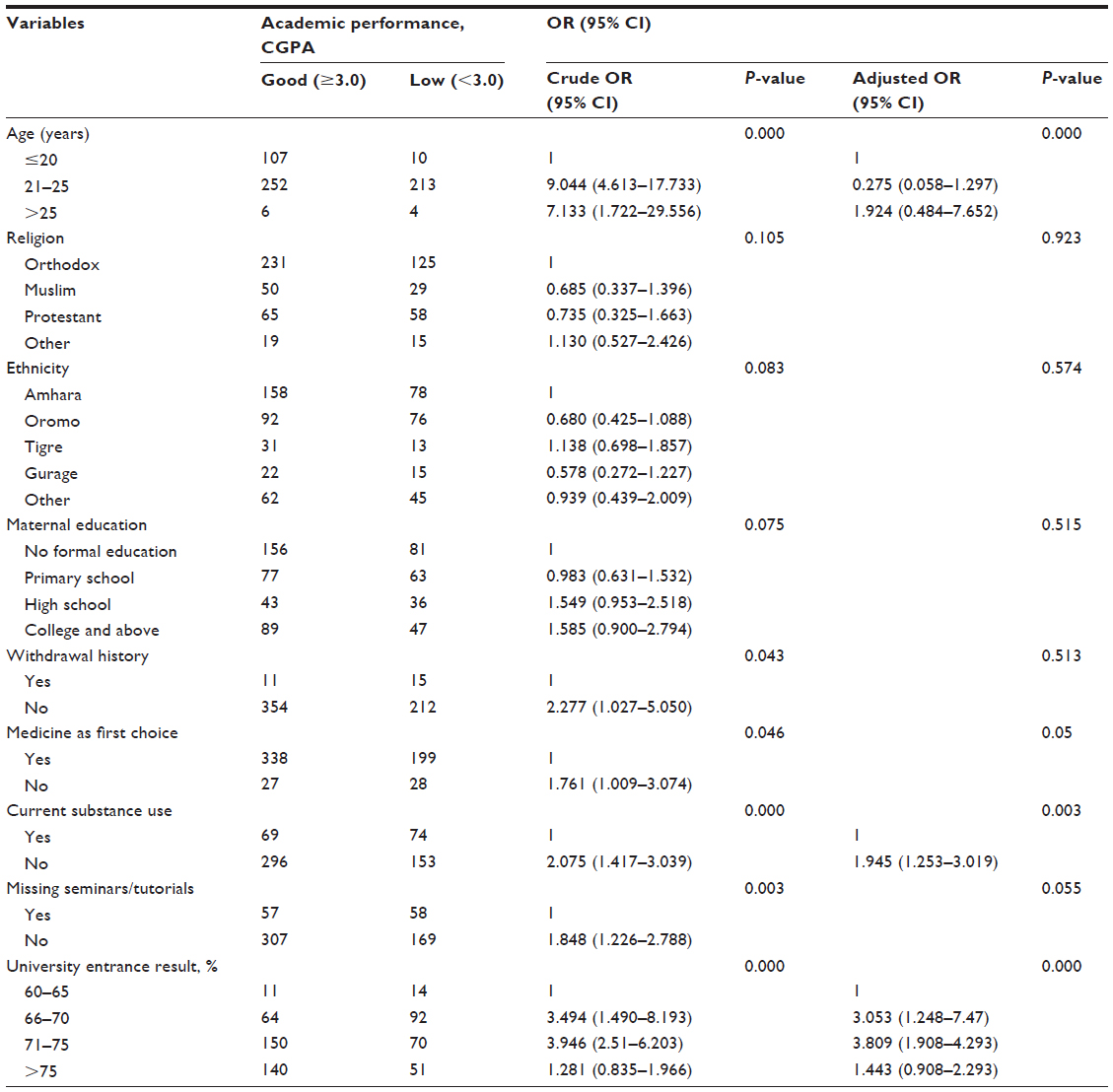 | Table 6 Binary and multiple logistic regression analysis of academic performance based on CGPA average as a dichotomous variable, College of Medicine and Health Sciences, Hawassa University, November 2012 |
Discussion
In the present study, we evaluated the correlation of different independent variables with self-reported academic performance. Self-reporting may affect the quality of study data, even though appropriate measures are taken during data collection to assess actual performance. To minimize this problem, an appropriate explanation was given to the participants on the importance of reporting their actual academic performance, and the data collection tool was pretested on paramedical students. More than three quarters of the participants were male (79.9%) which is consistent with the male predominance found in other studies done in higher institutions in Ethiopia.13,26–28 This indicates that female involvement in higher institutions is still low, despite continuing recruitment efforts.
In the current study, self-reported academic performance was higher among premedicine students. This is consistent with the findings of a study of freshmen at Jimma University where medical students had the lowest dismissal rate.29 Although the definition of low academic performance in medical students varies in the literature, two studies done in the USA of 1st-year medical students found low academic performance rates of 11.4% and 14%,24,25 which are by far lower than the low academic performance level found in the current study.
The identified explanatory variables accounted for only 32.8% of the variation in self-reported academic performance for the total study population, indicating that approximately 70% of the variation in academic performance had to be explained by determinants not assessed in this study. Subgroup analysis showed that these variables explained only 30.1% and 14.7% of the variation in academic performance for preclinical and clinical year students, respectively. This finding suggests that the variables chosen are poorer predictors of self-reported academic performance for students in the clinical years than for students in the preclinical years. This could be due to a difference in the teaching–learning and evaluation system between the two categories of students.
Participant age was one of the predictors of self-reported academic performance in this study. Student age alone accounted for 21.9% of the variation in academic performance, with academic performance decreasing as age increased. After controlling for other variables, for every 1-year increment in age, the cumulative GPA decreased by 0.389. However, the effect of student age on performance at medical school is a controversial issue. Older students in several studies did less well in scientific reasoning and tended to be graded with lower scores at the beginning of their courses, basically in the 1st year of their medical studies.30–32 However, recent studies show that older and more mature medical students performed better than their younger counterparts.33,34
Student age warrants very careful attention when interpreting the findings of the current study, given that this was at the point of data collection not the age of entry to medical school. It is very difficult to conclude that older students are performing less well than their younger counterparts, because being older could be due to academic delay, a longer time spent at medical school, or a difference in the nature of the academic years rather than age alone.
In the current study, as university entrance examination result of participants increased by one mark, their cumulative GPA increased by 0.271. Other researchers have demonstrated a similar predictive validity of academic performance prior to entry into medical school.7,35 A study done on school leaving examination results in New Zealand showed that these were predictive of GPA at medical school, especially in the preclinical years; however, only 16% of the variance in GPA at medical school was explained by previous academic performance.36 Studies done in the USA and the UK also found that previous academic achievement is a stronger predictor of preclinical academic performance than clinical academic performance, and that its predictive value decreased as students progressed through the academic years.37,38 This is because prior academic achievement demonstrates that the student has a minimum level of competence and the basic knowledge on which to build and integrate new knowledge.39
In the current study, khat, a central nervous system stimulant,40,41 was the most commonly used substance at university. Similar rates of khat use have been found in other studies in Ethiopian high schools (18.4%),27 universities (19.6%),28 and medical schools (14%–33.1%).13,24
There was a significant difference in mean self-reported cumulative GPA between substance users and non-users. Substance use alone explained 2.7% of the variation in self-reported academic performance, and students who were not substance users were twice as likely to self-report a cumulative GPA ≥3.0 and less likely to be delayed, have to re-sit, or be warned than their counterparts. This finding is consistent with the findings of a study conducted among medical and health officer students at Jimma University.13 Similar studies in Ethiopia14 and Saudi Arabia42 found that chewing khat is a risk factor for frequent absenteeism from class and poor academic performance in students. A recent study done in the same study area also found that absenteeism was higher among substance users,43 indicating that substance use has a negative influence on academic performance, perhaps as a result of the waste of valuable time and energy spent chewing khat, absenteeism from class, and lack of concentration during class due to insomnia.
This study has several limitations. It used self-administered questionnaires and instruments, so the reliability of the data could be questioned since bias might have been introduced, resulting in underreporting or overreporting. Further, there could have been some recall bias in students’ self-reported GPAs. We recommend future studies designed with appropriate ethical considerations taken into account in order to be able to use students’ academic records to assess their academic performance. The cross-sectional design of our study is also a limitation, because the presented associations lack cause-effect relationship. However, we included a representative sample of all undergraduate medical students from year 1 to internship, with a large sample size and a high response rate. Thus, it is possible to generalize the results internally for all medical students at HU. However, generalizability to medical students attending other medical schools might be limited.
Conclusion
The factors investigated in this study explained only 32.8% of variation in academic performance. Other factors known to influence academic performance, such as student motivation, personality, evaluation system, and learning style, should be studied in the future. It would be important to pay extra attention to students with a lower entrance examination result, substance users, and older students, particularly during the clinical years. More education to promote awareness of the harmful effects of substance use in medical schools is needed.
Acknowledgments
We are grateful to the Hawassa University’s College of Medicine and Health Sciences and the Johns Hopkins University Technical Support for the Ethiopian HIV/AIDS Initiative for their technical and financial support during this study. We would also like to thank all the medical students who participated in this study for their commitment.
Author contributions
AG conceived the research idea; AG and AA wrote the proposal; AG and AA were involved in data collection; and AG and BT analyzed the data and wrote the draft manuscript. AG, AA, and BT critically reviewed and edited the manuscript for intellectual content. All authors reviewed and approved the final manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Amin Z, Yap Seng C, Eng HE. Practical guide to medical student assessment. London, UK: World Scientific; 2006. Available from: http://www.eduv.hums.ac.ir/edc/evaluation/test_analysis/useful_files/EBOOKS/Practical_Guide_to_Medical_student_Assessment.pdf. Accessed February 17, 2015. | |
Kuper A, Reeves S, Albert M, Hodges BD. Assessment: do we need to broaden our methodological horizons? Med Educ. 2007;41:1121–1123. | |
Shumway JM, Harden RM; Association for Medical Education in Europe. AMEE Guide No 25. The assessment of learning outcomes for the competent and reflective physician. Med Teach. 2003;25:569–584. | |
Macpherson C, Kenny N. Professionalism and the basic sciences: an untapped resource. Med Educ. 2008;42:183–188. | |
Andrich D. A framework relating outcomes based education and the taxonomy of educational objectives. Studies in Educational Evaluation. 2002;28:35–59. | |
Kreiter CD, Kreiter Y. A validity generalization perspective on the ability of undergraduate GPA and the Medical College Admission Test to predict important outcomes. Teach Learn Med. 2007;19:95–100. | |
Powis D, Bore M, Munro D, Lumsden MA. Development of the Personal Qualities Assessment as a tool for selecting medical students. Journal of Adult and Continuing Education. 2005;11:3–14. | |
Petrides KV, Chamorro-Premuzic T, Frederickson N, Furnham A. Explaining individual differences in scholastic behaviour and achievement. Br J Educ Psychol. 2005;75:239–255. | |
Oswald FL, Schmitt N, Kim BH, Ramsay LJ, Gillespie MA. Developing a Biodata measure and situational judgement inventory as predictors of college student performance. J Appl Psychol. 2004;89:187–207. | |
Lumsden MA, Bore M, Millar K, Jack R, Powis D. Assessment of personal qualities in relation to admission to medical school. Med Educ. 2005;39:258–265. | |
Cassidy S, Eachus P. Learning style, academic belief systems, self report student proficiency and academic achievement in higher education. Educ Psychol. 2000;20:307–322. | |
McManus IC, Richards P, Winder BC, Sproston KA. Clinical experience, performance in final examinations, and learning style in medical students: prospective study. BMJ. 2004;316:345–350. | |
Kalayu M, Andualem M, Yeshigeta G. Effect of substance use on academic achievement of health officer. Ethiop J Health Sci. 2009;19:155–163. | |
Ayana A, Mekonen Z. Khat (Catha edulis Forsk) chewing, sociodemographic description and its effect on academic performance, Jimma University students. Ethiop Med J. 2004;42:125–136. | |
Widler P, Mathys K, Brenneisen R, Kalix P, Fisch H. Pharmacodynamics and pharmacokinetics of khat: a controlled study. Clin Pharmacol Ther. 1994;55:556–562. | |
Ministry of Health. Health and Health-Related Indicators. Addis Ababa, Ethiopia: Federal Democratic Republic of Ethiopia Ministry of Health; 2011. | |
World Health Organization. Working Together for Health: The World Health Report. Geneva, Switzerland: World Health Organization; 2006. | |
Ministry of Health. Health Sector Strategic Plan (HSDP-III). Addis Ababa, Ethiopia: Health Sector Strategic Plan (HSDP-III); 2005. Available from: http://can-mnch.ca/wp-content/uploads/2013/09/Ethiopia-Health-Sector-Development-PlanHSDP-III.pdf. Accessed February 17, 2015. | |
Ministry of Health. Health and Health Related Indicators. Addis Ababa, Ethiopia: Federal Democratic Republic of Ethiopia Ministry of Health; 2008. | |
Grover PL, Smith DU. Academic anxiety, locus of control, and achievement in medical school. J Med Educ. 1981;56:727–736. | |
Federal Ministry of Education. Placement of students to university medical schools, and appeals. 2013. Available from: http://info.moe.gov.et/nimeia.shtml. Accessed February 6, 2015. | |
McDonough CM, Horgan A, Codd MB, Casey PR. Gender differences in the results of the final medical examination at University College Dublin. Med Educ. 2000;34:30–34. | |
Ferguson E, James D, Madeley L. Factors associated with success in medical school: systematic review of the literature. BMJ. 2002;324:952–957. | |
Terry DS, Carol LE. A holistic review of the medical school admission process: examining correlates of academic underperformance. Med Educ Online. 2014;19:22919. Available from: http://dx.doi.org/10.3402/meo.v19.22919. Accessed February 17, 2015. | |
Durning SJ, Cohen DL, Cruess D, McManigle JM, MacDonald R. Does student promotions committee appearance predict below-average performance during internship? A seven-year study. Teach Learn Med. 2008;20:643–650. | |
Deressa W, Azazh A. Substance use and its predictors among undergraduate medical students of Addis Ababa University in Ethiopia. BMC Public Health. 2011;11:660. | |
Binyam N. Substance use among high school students in Dire Dawa, Ethiopia. Harar Bulletin of Health Sciences. 2012;2:42–49. | |
Yeshalem M. Khat chewing and its associated factor among college students in Bahir Dar Town, Ethiopia. Science Journal of Public Health. 2013;1:209–214. | |
Asmamaw A, Getachew K. Student related determinants of the first semester academic status: the case of 2006/7 first year students at some selected faculties of Jimma University. Ethiop J Educ Sci. 2011;7:19–37. | |
Aldous C, Leeder S, Price J, Sefton A, Teubner J. A selection test for Australian graduate-entry medical schools. Med J Aust. 1997;166:247–250. | |
Huff K, Fang D. When are students most at risk of encountering academic difficulty? A study of the 1992 matriculants to US medical schools. Acad Med. 1999;74:454–460. | |
Kay L, Pearson S, Rolfe I. The influence of admission variables on first year medical school performance: a study from Newcastle University, Australia. Med Educ. 2002;36:154–159. | |
Rolfe I, Pearson S, Powis D, Smith A. Time for a review of admission to medical school? Lancet. 1995;346:1329–1333. | |
James D, Chilvers C. Academic and non-academic predictors of success on the Nottingham undergraduate medical course 1970–1995. Med Educ. 2001;35:1056–1064. | |
McManus IC, Powis DA, Wakeford R, Ferguson E, James D, Richards P. Intellectual aptitude tests and A levels for selecting UK school leaver entrants for medical school. BMJ. 2005;331:555–559. | |
Collins JP, White GR, Kennedy JA. Entry to medical school – an audit of traditional selection requirements. Med Educ. 1995;29:22–28. | |
Powis D, Hamilton J, McManus IC. Widening access by changing the criteria for selecting medical students. Teaching and Teacher Education. 2007;23:1235–1245. | |
McManus IC, Richards P, Winder B, Sproston KA. Clinical experience, performance in final examinations and learning style in medical students: a prospective study. BMJ. 1998;316:345–350. | |
Roth P, BeVier C, Schipmann J, Switzer F. Meta-analyzing the relationship between grades and job performance. J Appl Psychol. 1996;81:548–556. | |
Ezekiel G. Khat in the Horn of Africa: historical perspectives and current trends. J Ethnopharmacol. 2010;132:607–114. | |
Alles GA, Fairchild D, Jensen M. Chemical pharmacology of Catha edulis. J Med Pharm Chem. 1986;3:323–352. | |
Alsanosy RM, Mahfouz MS, Gaffar AM. Khat chewing among students of higher education in Jazan region, Saudi Arabia: prevalence, pattern, and related factors. Biomed Res Int. 2013;2013:487232. | |
Desalegn AA, Berhan A, Berhan Y. Absenteeism among medical and health science undergraduate students at Hawassa University, Ethiopia. BMC Med Educ. 2014;14:81. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.