Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
Predictors of postoperative outcomes in infants with low birth weight undergoing congenital heart surgery: a retrospective observational study
Authors Lu C ![]() , Yu L, Wei J, Chen J, Zhuang J, Wang S
, Yu L, Wei J, Chen J, Zhuang J, Wang S ![]()
Received 20 February 2019
Accepted for publication 27 May 2019
Published 9 July 2019 Volume 2019:15 Pages 851—860
DOI https://doi.org/10.2147/TCRM.S206147
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor De Yun Wang
Chao Lu,1,* Lina Yu,2,* Jinfeng Wei,1 Jimei Chen,3 Jian Zhuang,3 Sheng Wang1
1Department of Anesthesiology, Guangdong Cardiovascular Institute, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangzhou, People’s Republic of China; 2Department of Anesthesiology, The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China; 3Department of Cardiac Surgery, Guangdong Cardiovascular Institute, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Background: Despite improvements in neonatal cardiac surgery and postoperative care, hospitalized death for infants with low birth weight remains high.
Objective: This study sought to identify predictors of postoperative outcomes in low-birth-weight infants undergoing congenital heart surgery and establish nomograms to predict postoperative intensive-care unit (ICU) stay.
Methods: From June 2009 to June 2018, a retrospective review of 114 infants with low birth weight (≤2.5 kg) undergoing congenital heart surgery was conducted at Guangdong Provincial People’s Hospital. Purely surgical ligation of patent ductus arteriosus was excluded from this study. A total of 26 clinical variables were chosen for univariate, multivariate, and Cox regression analysis, and 14 variables were analyzed as predictors of postoperative outcomes. Nomograms were established to predict risk of postoperative cardiac ICU (CICU) stay, postoperative neonatal ICU (NICU) stay, and total ICU length of stay in infants with cardiac diseases.
Results: Two variables were independent predictors in multiple logistic regression analysis of hospitalized death: operation weight and Society of Thoracic Surgeons–European Association for Cardio-Thoracic Surgery (STAT) risk categories. Six variables were independent predictors in the Cox model of postoperative ICU length of stay, including sex, prematurity, birth weight, preoperative stay time in NICU, diagnostic classification, and STAT risk categories. We calculated concordance-index values to estimate the discriminative ability of models of risk of postoperative CICU stay, postoperative NICU stay, and total ICU length of stay, with values of 0.758 (95% CI 0.696–0.820), 0.604 (95% CI 0.525–0.682), and 0.716 (95% CI 0.657–0.776), which indicated the possibility of true-positive results.
Conclusion: Our findings might help clinicians predict postoperative outcomes and optimize therapeutic strategies.
Keywords: low birth weight, congenital heart disease, neonatal cardiac surgery, outcome prognosis, predictive tools, nomogram
Introduction
The term “low birth weight” (LBW) denotes infants born weighing ≤2.5 kilograms, which includes those born preterm or small for gestational age.1 The probability of cardiovascular malformation in preterm infants is double that of those born at term.2 Infants with congenital heart disease have a high probability (8%–23%) of LBW, and vary in specific cardiac malformation.2–4 While waiting for weight gain over the weeks, these infants are at greater risk of pulmonary infection, gastrointestinal ischemia, anemia, hypoxic ischemic encephalopathy, and myocardial dysplasia.5
Despite improvements in surgical techniques, extracorporeal circulation, and intensive care over the last few decades, many cardiac centers have reported increased mortality rates of LBW infants with cardiac surgery — 10%–24%.6–8 However, risk factors of LBW infants with cardiac surgery are still controversial, and there is no effective prediction system at present.9 Furthermore, few researchers have paid attention to the impact of LBW on postoperative hospital stay.
The aim of this study was to investigate risk factors related to postoperative outcomes in LBW infants undergoing congenital heart surgery and establish nomograms that will predict postoperative intensive-care unit (ICU) length of stay.
Methods
Study design and patient population
This study was conducted in accordance with the Declaration of Helsinki and was also approved by the Medical Ethics Committee of Guangdong Provincial People’s Hospital. Patient consent to review their medical records was not required, as this was an observational retrospective study that did not infringe upon the interests or rights of the patients. All data were strictly confidential. After acquiring institutional review board approval and permission to waive consent, the electronic medical records of 114 LBW infants undergoing congenital heart surgery from January 2009 to January 2018 were conducted. This article followed the STROBE checklist for observational studies. As a heart center of southern China, the quantity of our cardiac surgery has increased steadily every year, reaching 5,619 cases in 2017, over 100 of which were neonatal heart operations. The neonatal cardiac intensive-care section is staffed with highly trained neonatal cardiac intensive-care cardiologists and nurses, neonatal respiratory therapists, and neonatal nutritionists. Purely surgical ligation of patent ductus arteriosus was excluded from this study.
Data collection
We recorded characteristics of all patients from the electronic medical record systemas follows. The preoperative section comprised sex, prematurity (yes/no), gestational age, birth weight, age at operation, operation weight, preoperative concurrent diseases, preoperative ventilation (yes/no), preoperative pulmonary overcirculation (yes/no), preoperative stay in neonatal ICU (NICU), emergency operation (yes/no), diagnostic classification, and Society of Thoracic Surgeons–European Association for Cardio-Thoracic Surgery (STAT risk categories). The intraoperative section comprised cardiopulmonary bypass (CPB) time, clamp time, deep hypothermic circulatory arrest (DHCA) (yes/no), DHCA time, and delayed sternal closure (yes/no). The postoperative section comprised trachea reintubation (yes/no), unplanned reoperation (yes/no), postoperative complications, postoperative ventilation time, postoperative stay in cardiac ICU (CICU), postoperative time in NICU, total ICU length of stay, hospitalized death (yes/no), and death cause.
STAT risk categories were based on the definition established by O’Brien et al,10 and diagnostic classification was characterized as compound deformity, univentricular deformity, biventricular deformity, and macrovascular deformity. Preoperative pulmonary overcirculation was mainly diagnosed with chest radiography. Researchers and research assistants were trained and responsible for quality control of data acquisition and entry.
Statistical analysis
Catagorical data are expressed as proportions, and quantitive data as medians and ranges. Data were classified as characteristics before, at, and after surgery. Catagrical outcomes were regressed with a logistic model, in all independent variables that achieved a significance level of 20% in univariate analysis were included in a multivariate logistic regression model and examined by stepwise backward elimination. Likelihood-ratio tests were used to select variables in the multivariate model and check the goodness of fit. Quantitive outcomes were analysed with the Cox proportional-hazard model and examined by stepwise backward elimination with the Akaike information criterion (AIC). Models were validated by calibration plots and discrimination plot (C-index). Statistical analyses were conducted with R version 3.4.1. P<0.05 was considered statistically significant for all modeling.
Construction and calibration of nomograms
Perioperative deaths were deleted in the nomograms to predict risk for postoperative CICU stay, postoperative NICU stay, and total ICU length of stay in infants with cardiac diseases. Based on the results obtained from the Cox proportional-hazard model, nomograms were established to predict risk of postoperative outcomes using the R package. A score was assigned to identified factors according to their regression coefficients, which will be convenient for clinical usage. We calculated the C-index to estimate the discriminative ability of models of risk. The maximum value of the C-index is 1, referring to perfect discrimination, whereas 0 refers to no discrimination ability.11
Results
Patient characteristics
From January 2009 to January 2018, 185 LBW infants undergoing congenital heart surgery were included. Of these, 71 infants with purely surgical ligation of patent ductus arteriosus were removed. Therefore, our final comparative study comprised 114 infants, and patient characteristics (before, at, and after surgery) are shown in Table S1. Diagnosis, operation,and mortality of the infants are shown in Table 1. A total of 24 cases died during hospitalization, the overall mortality rate was 21.1%, of which four cases died during operation, 12 cases died early after operation (72 hrs), and 3 cases had treatment ceased.
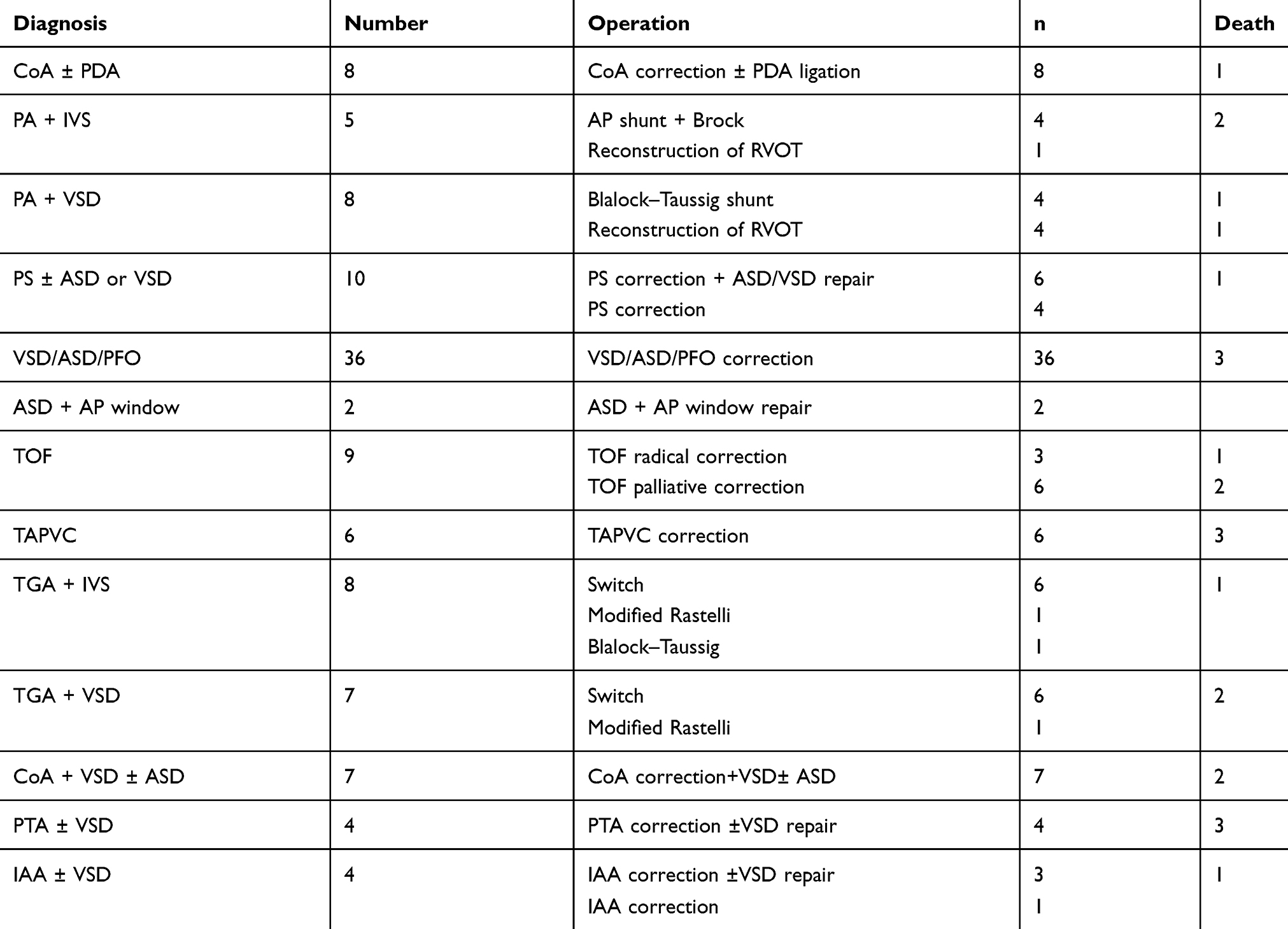 |
Table 1 Diagnosis, operation, and mortality of 114 infants |
Univariate and multivariate logistic analysis of hospitalized death
Ten risk factors were found to show significant differences in the univariate analysis of hospitalized death (Table 2). When these factors were further entered into the multivariate logistic model checked by the likelihood-ratio test, only two were independent predictors in multiple logistic regression analysis (Table 3: operation weight (OR 0.17, 95% CI 0.03–0.85; P=0.031) and STAT risk categories (OR 1.97, 95% CI 1.21–3.22; P=0.006).
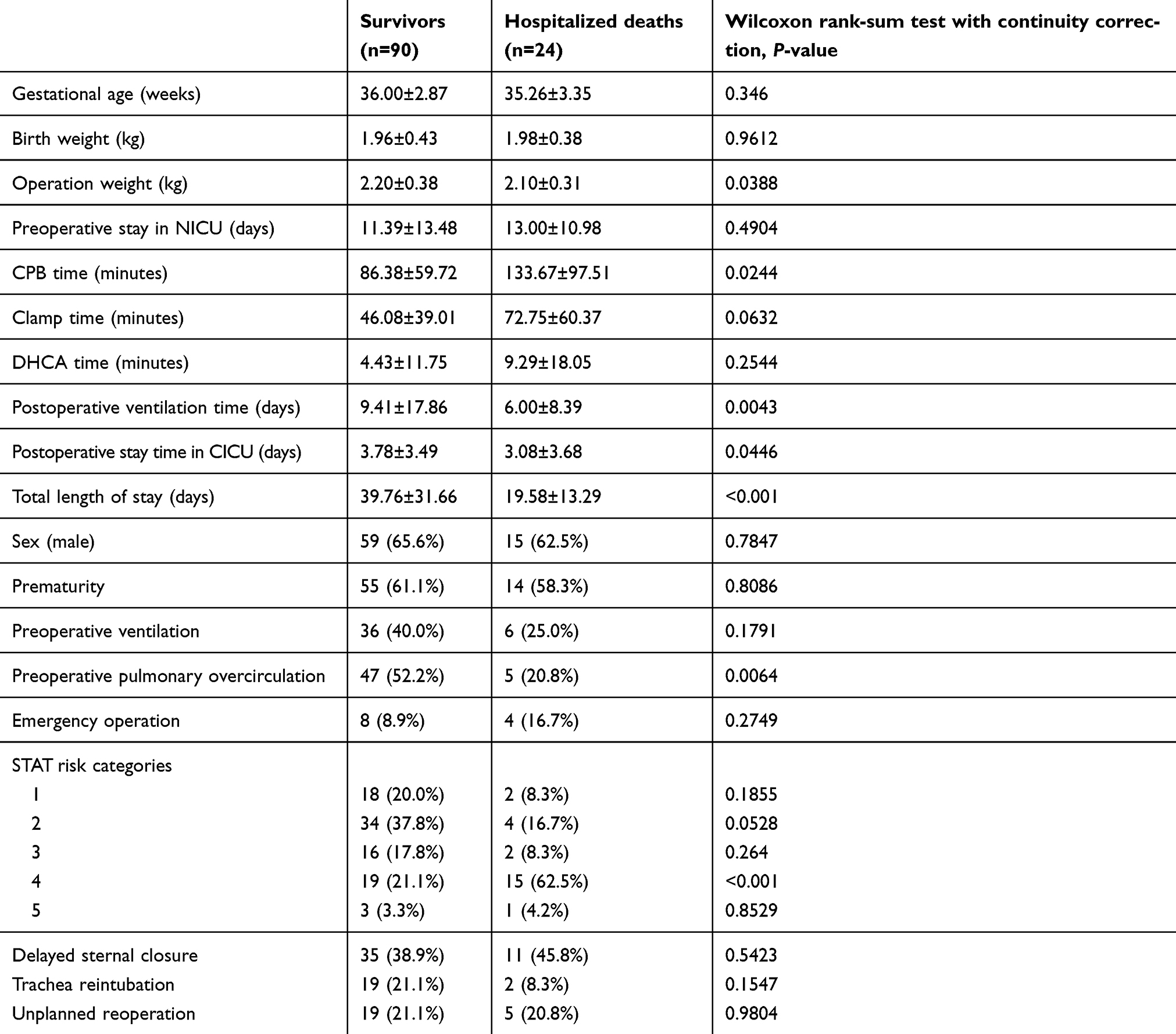 |
Table 2 Univariate risk analysis for hospitalized death in low-birth-weight infants |
 |
Table 3 Multivariate logistic analysis for hospitalized death in low-birth-weight infants |
Cox proportional-hazard model
Perioperative deaths were deleted in the Cox proportional-hazard model. Quantitive outcomes (postoperative CICU/NICU stay, total ICU length of stay) were fitted to the model and covariates selected by stepwise backward elimination with the AIC (Table S2). Five variables were independent predictors in the Cox model for postoperative CICU stay: sex, prematurity, preoperative stay in NICU, diagnostic classification, and STAT risk categories. Two variables were independent predictors in the Cox model for postoperative NICU stay: gestational age and STAT risk categories. Three variables were independent predictors in the Cox model for total ICU length of stay: birth weight, preoperative stay in the NICU, and STAT risk categories.
Nomogram model
Based on the results obtained from multiple logistic regression and the Cox model, nomograms were established to predict risk of postoperative stay in the CICU and NICU and total ICU length of stay of LBW patients born with cardiac diseases (Figures 1–3). We calculated C-index values to estimate the discriminative ability of models of risk of postoperative stay in the CICU and NICU and total ICU length of stay — 0.758 (95% CI 0.696–0.820), 0.604 (95% CI 0.525–0.682), and 0.716 (95% CI 0.657–0.776), respectively — which indicated the possibility of true-positive results. AIC values for postoperative stay in the CICU and NICU and total ICU length of stay were 610.8, 600.1, and 577.5.
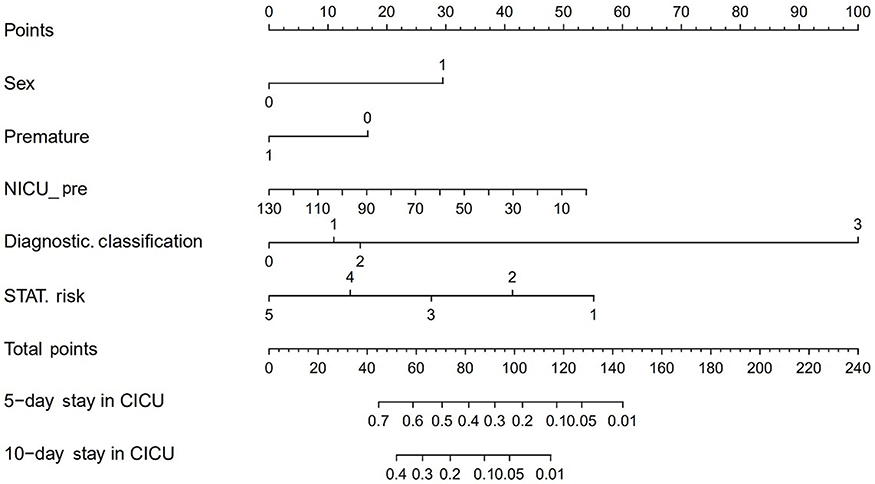 |
Figure 1 Nomogram prediction of postoperative stay time in CICU.Abbreviations: STAT, Society of Thoracic Surgeons–European Association for Cardio-Thoracic Surgery; NICU, neonatal intensive-care unit; CICU, cardiac ICU. |
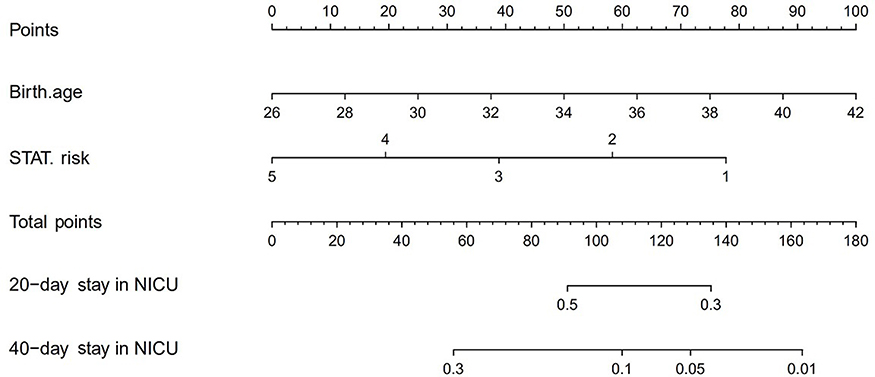 |
Figure 2 Nomogram prediction of postoperative stay time in NICU.Abbreviations: STAT, Society of Thoracic Surgeons–European Association for Cardio-Thoracic Surgery; NICU, neonatal intensive-care unit |
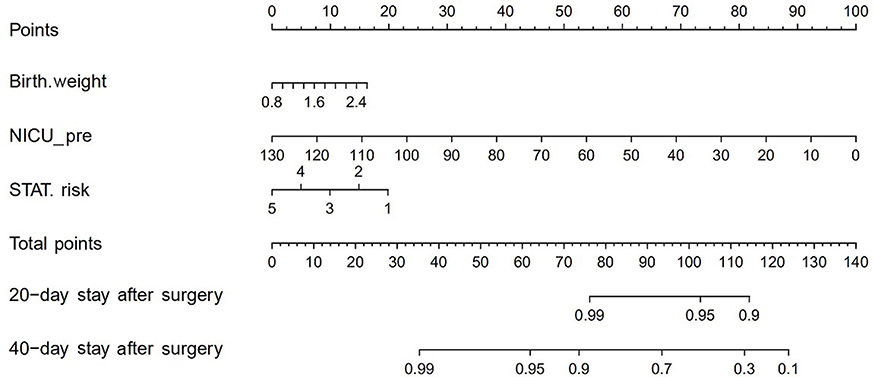 |
Figure 3 Nomogram prediction of total ICU length of stay.Notes: Premature — 0 = no, 1 = yes; diagnostic classification — 0 = compound deformity, 1 = univentricular deformity, 2 = biventricular deformity, 3 = macrovascular deformity. Abbreviations: Pre, preoperative; ICU, intensive-care unit; NICU, neonatal ICU; STAT, Society of Thoracic Surgeons–European Association for Cardio-Thoracic Surgery. |
Discussion
Despite good outcomes for many infants, great challenges remain in improving outcomes in LBW infants with congenital heart disease.12 Postoperative outcomes depend not only on surgical techniques but also on many other factors, such as anesthesia, intensive care and patient-specific characteristics.13 Therefore, prognostic estimation and perioperative management of infants undergoing congenital cardiac surgery are critical for patients’ health and prognosis.
A recent study from Westmead Children’s Hospital in Australia reported that low operation weight remained associated with high mortality rates.14 Analysis of the Society of Thoracic Surgeons Congenital Heart Surgery database from 32 participating centers reached a similar conclusion.12 Consistently with previous studies, we found that low operation weight was a significant risk factor for mortality in LBW infants with congenital heart disease, which stresses the importance of understanding the certain danger. The Society of Thoracic Surgeons database indicated that lower weight consistently raised the risk of mortality after risk classification.12 Our data confirmed the verification of STAT risk categories as these applied to the Chinese population, and indicated a strong relationship between STAT risk categories and postoperative mortality.
As far as we know, length of ICU stay, a principal indicator of medical quality, has a great impact on admission policy, surgical arrangement, and costs. Identification of risk factors influencing ICU hospitalization after cardiac surgery can not only provide reliable risk adjustment for administrative data but also enhance overall quality. Recently, several factors have been identifed as risk factors of prolonged ICU stay, such as gestational age, operation weight, preoperative ventilation, single-ventricle anomalies, STAT risk categories, CPB time, clamp time, and postoperative complications.15–19 Consistently with Pagowska-Klimek’s study, we have not found a close relationship between DHCA time and total postoperative ICU length of stay.16 Our study confirmed the usefulness of STAT risk categories as means of predicting postoperative CICU stay, NICU stay, and total ICU length of stay, which was consistent with Brown et al.18 CPB time is now well recognized as a risk factor associated with ICU length of stay in both children and adults.20,21 However, our study found that CPB time was not an independent predictor of postoperative ICU stay in LBW infants. We identified sex as an independent predictor of postoperative CICU stay, largely due to differences in STAT risk categories between the sexes.
LBW infants often suffer from severe morbidity of prematurity and intrauterine growth restriction.5 The latter raises rates of respiratory distress syndrome and bronchopulmonary dysplasia in premature babies.22,23 Also, LBW infants with congenital heart disease tend to be critically ill and their condition complicated by noncardiac malformation. Over the past few decades, numerous single-center studies have documented increased morbidity and mortality correlated with cardiac surgery in LBW infants.7–9 However, few studies have focused on the impact of LBW on postoperative length of hospitalization. As these LBW infants with varied adverse risk factors start to have advanced survival, the morbidity burden would be aggravated with a commensurate rise in the length of hospitalization. Our study showed that gestational age, birth weight, and STAT risk categories were significant predictors in postoperative NICU stay and total length of ICU stay. Nevertheless, further larger studies are needed to validate the impact of LBW on postoperative length of hospitalization.
To the best of our knowledge, no accurate prediction model specific for LBW infants with cardiac surgery exists. In the present study, we examined risk factors associated with postoperative outcomes and established nomograms to estimate the risk of postoperative length of hospitalization in LBW infants with cardiac surgery. Each factor included in the nomograms was attributed a risk score, and integration of these risk scores can provide potential incidence of postoperative length of hospitalization. Moreover, the nomograms that we have established had good discrimination ability and good concordance-index values in the present series.
Limitations
Several limitations have to be admitted in our study. First, it was a retrospective single-center study with a limited number of cases. Collecting and analyzing Chinese major cardiac multiinstitutional data set of LBW patients is thus an essential part of our plan, and will be the subject of communication in the future. Second, there was a lack of long-term postdischarge follow-up to predict long-term mortality and morbidity. Finally, while the nomograms indicated good efficacy to predict postoperative outcomes in our hospital, they may not apply to other patient populations. External validation of the nomograms in a multicenter database is thus necessary. Despite these limitations, our study has developed nomograms that will effectively predict postoperative outcomes for LBW infants undergoing congenital heart surgery.
Conclusion
Our novel nomogram predictions are tools that provide risk adjustment for administrative data that might help clinicians predict postoperative outcomes and optimize therapeutic strategies. Further studies with large samples are encouraged to ensure their application in multiple institutions.
Abbreviation list
PDA, patent ductus arteriosus; CoA, coarctation of aorta; ASD, atrial septal defect; VSD, ventricular septal defect; PFO, patent foramen ovale; TOF, tetralogy of Fallot; TAPVC, total anomalous pulmonary venous drainage; TGA, (complete) transposition of great arteries; IVS, interventricular septum; PA, pulmonary atresia; PS, pulmonary artery stenosis; PTA, permanent trunk of artery; IAA, interruption of aortic arch, AP, aortopulmonary, LBW, low birth weight, IGUR, intrauterine growth restriction, STAT, Society of Thoracic Surgeons–European Association for Cardio-Thoracic Surgery; ICU, intensive-care unit; NICU, neonatal ICU; CICU, cardiac ICU; CPB, cardiopulmonary bypass; DHCA, deep hypothermic circulatory arrest.
Availability of data and material
All data supporting our findings will be shared on request. Contact Sheng Wang via [email protected].
Ethics approval and consent to participate
The Institutional Review Committee of Guangdong Provincial People’s Hospital approved this study, and all investigations were conducted in accordance with ethical research principles. Patient consent was not required.
Acknowledgment
We would like to thank Shanghai Ruihui Biotech for data processing and management.
Author contributions
SW, JZ, LY, and CL designed the study. CL, LY, SW, JZ, and JW gathered the data. JC, SW, JZ, LY, and CL analyzed the data. CL, LY, JW, JC, JZ, and SW wrote the manuscript and agree to be responsible for its contents. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work
Disclosure
JZ received funding from Guangdong Project of Science and Technology (2017A070701013 and 2017B090904034). SW received funding from the Natural Science Foundation of Guangdong Province (2018A030313535). The authors report no other conflicts of interest in this work.
References
1. Rosenberg A. The IUGR newborn. Semin Perinatol. 2008;32:219–224. doi:10.1053/j.semperi.2007.11.003
2. Tanner K, Sabrine N, Wren C. Cardiovascular malformations among preterm infants. Pediatrics. 2005;116:833–838. doi:10.1542/peds.2004-2446
3. Kramer HH, Trampisch HJ, Rammos S, et al. Birth weight of children with congenital heart disease. Eur J Pediatr. 1990;149:752–757.
4. Rosenthal GL, Wilson PD, Permutt T, et al. Birth weight and cardiovascular malformations: a population-based study. The Baltimore-Washington infant study. Am J Epidemiol. 1991;133:1273–1281. doi:10.1093/oxfordjournals.aje.a115839
5. Williams GD, Cohen RS. Perioperative management of low birth weight infants for open-heart surgery. Paediatr Anaesth. 2011;21:538–553. doi:10.1111/j.1460-9592.2011.03529.x
6. Ades AM, Dominguez TE, Nicolson SC, et al. Morbidity and mortality after surgery for congenital cardiac disease in the infant born with low weight. Cardiol Young. 2010;20:8–17. doi:10.1017/S1047951109991909
7. Seo DM, Park JJ, Yun TJ, et al. The outcome of open heart surgery for congenital heart disease in infants with low body weight less than 2500 g. Pediatr Cardiol. 2011;32:578–584. doi:10.1007/s00246-011-9910-2
8. Chang AC, Hanley FL, Lock JE, et al. Management and outcome of low birth weight neonates with congenital heart disease. J Pediatr. 1994;124:461–466.
9. Kalfa D, Krishnamurthy G, Duchon J, et al. Outcomes of cardiac surgery in patients weighing ≤2.5 kg: affect of patient-dependent and -independent variables. J Thorac Cardiovasc Surg. 2014;148:2499–2506. doi:10.1016/j.jtcvs.2014.07.031
10. O’Brien SM, Clarke DR, Jacobs JP, et al. An empirically based tool for analyzing mortality associated with congenital heart surgery. J Thorac Cardiovasc Surg. 2009;138:1139–1153. doi:10.1016/j.jtcvs.2009.03.071
11. Montero PH, Yu C, Palmer FL, et al. Nomograms for preoperative prediction of prognosis in patients with oral cavity squamous cell carcinoma. Cancer. 2014;120:214–221. doi:10.1002/cncr.28407
12. Curzon CL, Milford-Beland S, Li JS, et al. Cardiac surgery in infants with low birth weight is associated with increased mortality: analysis of the society of thoracic surgeons congenital heart database. J Thorac Cardiovasc Surg. 2008;135:546–551. doi:10.1016/j.jtcvs.2007.09.068
13. Dimmick S, Walker K, Badawi N, et al. Outcomes following surgery for congenital heart disease in low-birthweight infants. J Paediatr Child Health. 2007;43:370–375. doi:10.1111/j.1440-1754.2007.01082.x
14. Padley JR, Cole AD, Pye VE, et al. Five-year analysis of operative mortality and neonatal outcomes in congenital heart disease. Heart Lung Circ. 2011;20:460–467. doi:10.1016/j.hlc.2011.03.009
15. Mori M, McCracken C, Maher K, et al. Outcomes of neonates requiring prolonged stay in the intensive care unit after surgical repair of congenital heart disease. J Thorac Cardiovasc Surg. 2016;152:720–727. doi:10.1016/j.jtcvs.2016.04.040
16. Pagowska-Klimek I, Pychynska-Pokorska M, Krajewski W, et al. Predictors of long intensive care unit stay following cardiac surgery in children. Eur J Cardiothorac Surg. 2011;40:179–184. doi:10.1016/j.ejcts.2010.11.038
17. Alsoufi B, McCracken C, Ehrlich A, et al. Single ventricle palliation in low weight patients is associated with worse early and midterm outcomes. Ann Thorac Surg. 2015;99:668–676. doi:10.1016/j.athoracsur.2014.09.036
18. Brown KL, Ridout DA, Goldman AP, et al. Risk factors for long intensive care unit stay after cardiopulmonary bypass in children. Crit Care Med. 2003;31:28–33. doi:10.1097/01.CCM.0000046068.19048.86
19. Polito A, Patorno E, Costello JM, et al. Perioperative factors associated with prolonged mechanical ventilation after complex congenital heart surgery. Pediatr Crit Care Med. 2011;12:122–126. doi:10.1097/PCC.0b013e3181e912bd
20. Gillespie M, Kuijpers M, Van Rossem M, et al. Determinants of intensive care unit length of stay for infants undergoing cardiac surgery. Congenit Heart Dis. 2006;1:152–160. doi:10.1111/j.1747-0803.2006.00027.x
21. Atoui R, Ma F, Langlois Y, et al. Risk factors for prolonged stay in the intensive care unit and on the ward after cardiac surgery. J Card Surg. 2008;23:99–106. doi:10.1111/j.1540-8191.2007.00564.x
22. Tommiska V, Heinonen K, Lehtonen L, et al. No improvement in outcome of nationwide extremely low birth weight infant populations between 1996–1997 and 1999–2000. Pediatrics. 2007;119:29–36. doi:10.1542/peds.2006-1472
23. McIntire DD, Bloom SL, Casey BM, et al. Birth weight in relation to morbidity and mortality among newborn infants. N Engl J Med. 1999;340:1234–1238. doi:10.1056/NEJM199904223401603
Supplementary material
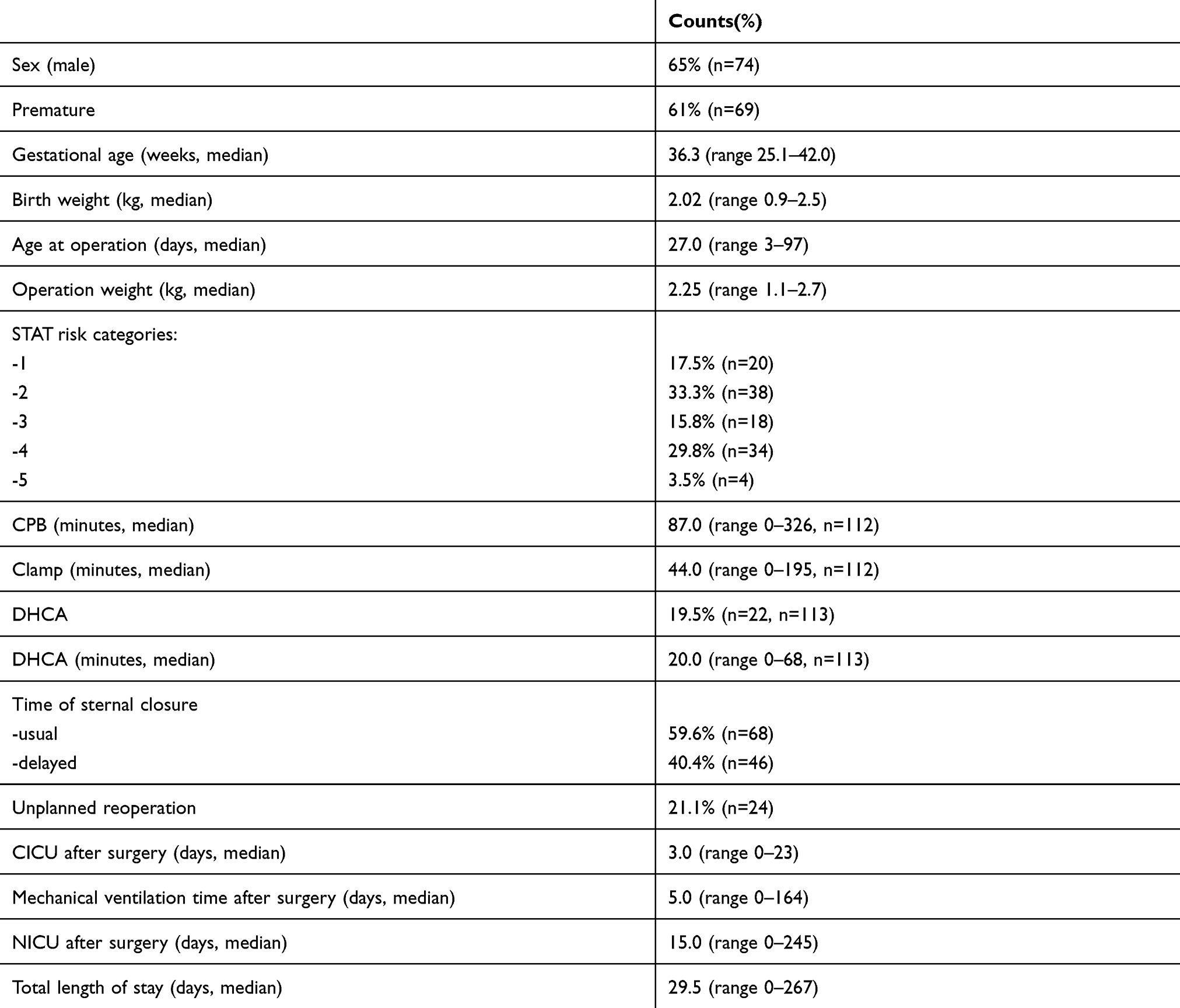 |
Table S1 Patient characteristics of 114 infants undergoing congenital heart surgery |
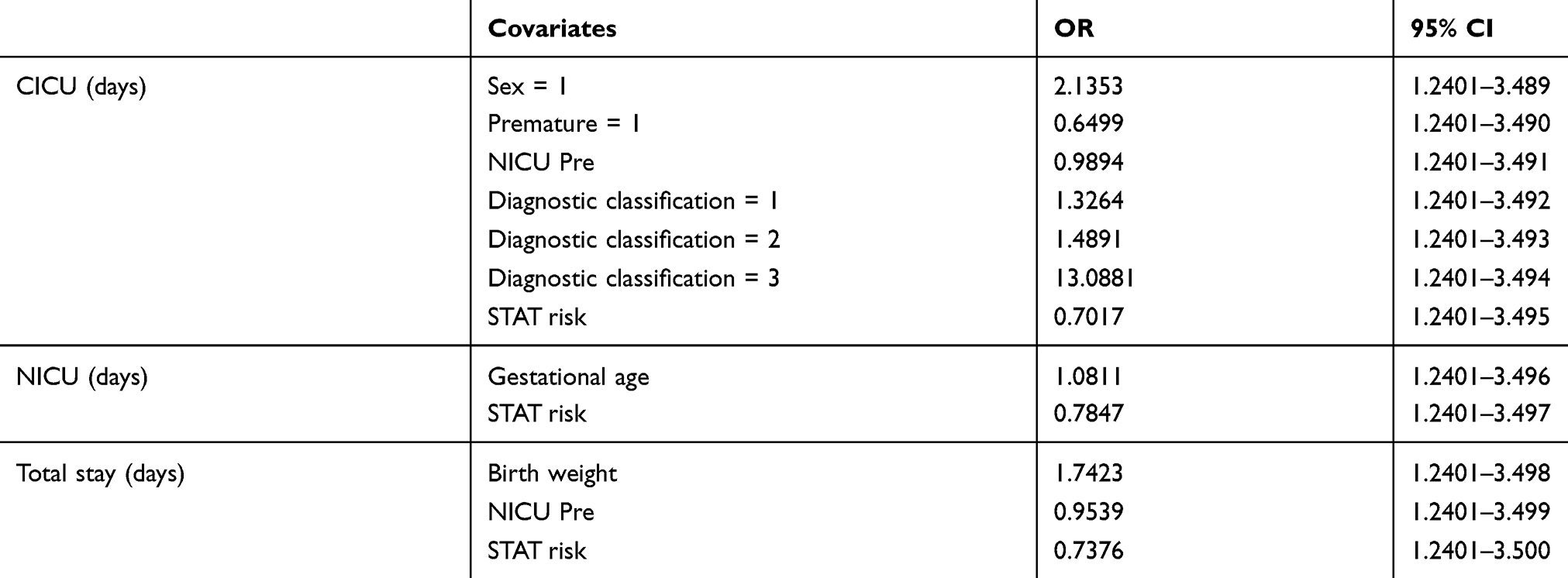 |
Table S2 Cox proportional-hazard model of quantitive outcomes |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.