Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 12
Predictors of Partial Immunization Among Children Aged 12–23 Months in Yirga Cheffe District, South Ethiopia – A Community-Based Unmatched Case-Control Study
Authors Nenko G, Addisu Y, Eifa A, Ketema W ![]()
Received 24 June 2021
Accepted for publication 4 August 2021
Published 8 August 2021 Volume 2021:12 Pages 395—404
DOI https://doi.org/10.2147/PHMT.S326319
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Getachew Nenko,1 Yohannes Addisu,1 Aberash Eifa,2 Worku Ketema3
1School of Public Health, College of Health Sciences, Dilla University, Dilla, Gedio, Ethiopia; 2Department of Midwifery, College of Health Sciences, Hawassa University, Hawassa, Sidama, Ethiopia; 3Department of Pediatrics and Child Health, College of Health Sciences, Hawassa University, Hawassa, Sidama, Ethiopia
Correspondence: Worku Ketema
Department of Pediatrics and Child Health, College of Health Sciences, Hawassa University, Hawassa, Sidama, Ethiopia
Tel +251 933207095
Email [email protected]
Background: Universal age-specific immunization is one of the areas where preventive public health policy has become successful. Despite the increase in global immunization coverage, however, many children around the world, especially in developing countries, are still left unvaccinated. The study aimed at assessing the determinants of partial immunization among children 12– 23 months of age in Yirga Cheffe, Gedeo, Ethiopia.
Methodology: A community-based unmatched case-control study design was conducted. Using a simple random sampling technique, 328 samples (164 cases and 164 controls) were selected. Index case was defined as a child aged 12 to 23 months who missed at least one dose of vaccine from the scheduled dose. The odds ratio (OR) and 95% confidence interval (CI) were used to calculate the association, and the level of significance was set at p 0.05.
The Result: The study showed that 40% of children were fully vaccinated, and the prevalence of those with partial vaccination was 46%. The likelihood of having incomplete vaccination was 45% higher in children whose mothers had no antenatal coverage (ANC) visit during pregnancy [OR=0.55, (95% CI; 0.297, 1.035)]. Lack of knowledge about the schedule of the vaccination has negatively affected the success of full vaccination (OR=2.3; 95% CI=1.01, 5.56).
Conclusion: The study revealed that significant numbers of children are not fully vaccinated. Despite appreciable efforts by the Federal Ministry of Health to improve complete immunization coverage, there are still bottlenecks that need to be tackled in enhancing coverage. We recommend the expansion of ANC and providing education on vaccination schedule and importance to minimize the burden of partial vaccinations and its sequelae.
Keywords: partial immunization, 12– 23 month children, Yirgacheffe
Introduction
Immunization obviates about 2 to 3 million deaths every year in all age groups from diphtheria, tetanus, pertussis, and measles globally. By expanding the universal vaccination coverage, yet more than one and a half million deaths might be circumvented.1–3
Nations are implementing immunization program and in most developing countries, children under five years old are immunized with the standard World Health Organization (WHO) recommended vaccines that protect against ten vaccine-preventable diseases like Tuberculosis, Diphtheria, Tetanus (including neonatal tetanus through immunization of mothers), Pertussis (Whooping cough), Poliomyelitis, Measles, Liver disease due to hepatitis B virus, and Meningitis and Pneumonia associated with Haemophilus influenzae bacteria and Rota virus-associated gastro-enteritis. These strategies are averting more than two and half million child deaths yearly.2–5
Since the inception of the Expanded Program on Immunization in Ethiopia, 1980, the main poem was attaining 100% immunization coverage of all children under two years old by 1990. However, in 1986, the coverage target was reorganized to 75%, and the target age group was changed to under one year in accordance with the global immunization target considerations of the child exposure time to natural infection.5–8
Only 24% of children in the age of 12–23 months in Ethiopia have completed their vaccination as per the schedule in 2011, which showed slight improvement than the previous report (19%) in 2005, yet below the Health Sector Development Program (HSDP) IV target, which was supposed to be 66% and 90% national coverage and 80% in every district with all vaccines by 2020.4,9 The immunization coverage had regional discrepancies, like up to 78.5% in Addis Ababa, 69.9% in South Ethiopia, a region of our study place, and 41.3% in the Afar region.2,4,7
In Ethiopia, strategies for increasing immunization coverage and defaulter tracing have been comprehensively studied and described in the literature. The coverage has negatively influenced by low access to immunization services, inadequate awareness of mothers’ or immediate caregivers, and missed opportunities are major factors contributing to incomplete child immunization.4,6,10,11
Many health institutions attempt to improve immunization coverage through strengthening Antenatal Coverage (ANC) and Postnatal Care (PNC) services, and promoting institutional delivery, enhancement on the benefits of vaccination, and reducing the incidences of missed opportunities.1,2,7,11
The studies conducted earlier were mostly parts of coverage evaluation surveys which might have a greater chance of recall bias. Conducting this study will minimize this research gap and draw attention to the factors that may be associated with incomplete childhood immunization and will generate data which will be applicable for averting the problems associated with incomplete immunization, and enhancing the coverage. Hence, this study was aimed at identifying factors associated with partial immunization among children 12–23 months of age in Yirga Cheffe, South Ethiopia.
Methodology
Study Area and Period
This study was carried out in Yirga Cheffe district which is situated about 130 Km to the Southern segment from the Capital city (Hawassa). Yirga Cheffe district is highly populous among six districts found in Gedeo Zone with the population size of 271,000. There are 31 Community Health Posts and 8 health centers in the district. There is one newly constructed primary hospital in Yirga Cheffe tow.
Study period was from December 1 to 31, 2017.
Study Design
A community-based unmatched case-control study was used.
Study Population
Our study populations were Children 12–23 months of age residing in Yirga Cheffe and who fulfill the inclusion criteria.
Sampling Units
The sampling units in our study were Households in 10 randomly selected districts.
Study Units
Children 12–23 months of age who are not fully immunized for age as per the national guideline (index cases), and who are fully immunized (reference cases) and mothers’/caretakers’ in the selected households.
Eligibility Criteria
Inclusion Criteria
Households with at least one alive child 12–23 months of age were eligible for the study. In case of two or more children, the youngest child by age will be selected and in case of twin both children will be included in the study. Children who never got vaccination will be also included in the study.
Exclusion Criteria
Children whose mother or immediate care taker was not present during the study were excluded from the study.
Sample Size Determination
The EPI INFOTM software version 3.04 was used for sample size determination.
Proportion of caretakers, 76% and 52% for index cases and reference cases, respectively (from the study conducted by Mohammed H, and Atomsa A. in Oromia Regional State in 2010).12 5% significance level, power of 80%, 95% confidence interval, 1:1 ratio of index case to reference cases, least extreme Odd Ratio (OR) to be detected was 2.0, and 10% non-response rate. The estimated final sample size was 332 (166 index cases and 166 reference cases).
Sampling Technique
9 rural and one Kebeles were randomly selected by simple random sampling after 10 Kebeles were stratified. Index Case and reference cases were determined after initially conducting census. Initially, census was conducted to determine index cases and reference cases. The calculated total sample size was shared to each Kebeles according to the sample size proportion.
Variables
Dependent Variable
Incomplete immunization among children 12–23 months of age.
Independent Variables
- Socio demographic characteristics of mothers/caretakers and children
- Knowledge of mothers/immediate caretakers about immunization.
- ANC visit.
- PNC visit
- Reasons for not immunizing
Data Collection Instrument
The Ethiopia Demographic and Health Survey (EDHS 2011) and other previous similar literature were used for the development of questionnaire with some modification.9
The tools had parts like socio-demographic variables, questions related to maternal and child health services, knowledge of the mothers about vaccination, immunization status of children, reasons for defaulting and not immunizing the child.
Data Collection Procedure
The immunization card and mothers’/immediate caretakers verbal reactions were used for the data collection, and the mothers’/immediate caretakers were asked for the availability of child’s immunization card. Then accordingly, the data collectors proceed for the collection based on the sources. Priority was given for the review of immunization card first and then the mother if no information is available. Specifically, the dose number that has been given and vaccine administration route were sought from the card and other information from the mother.
Training of Data Collectors
Data were collected by 10 clinical nurses and data collection process was being supervised by 5 public health officers who were hired from Wonago Health Centre. The data collectors and supervisors were briefed for two days on the main aim of the study, important techniques on how to approach the study units and time management.
Data Quality Management
The questionnaire was pre-tested on 17 children who were not selected for the study prior to data collection, and minor amendments were made on the flow of the questionnaire.
Data Processing and Analysis
After being checked for discrepancies and completeness, data were processed to EPI-Info 11, and then transferred to SPSS version 24.0 for analysis. Associated factors were identified by binary logistic regression model, and variables having P values less than or equal to 0.25 was further analyzed in to multivariate logistic regression so that confounding effects could be controlled.
Bivariate and multivariate Logistic regression models were used to identify factors that affected partial vaccination. The strength of association was used to look for the strength of association at 95% confidence interval. We set the level of statistical significance at p < 0.05.
Operational Definition
The following operational definitions were used:
Index cases (Cases); children 12–23 months of age who are not fully immunized for age as per the national guideline.
Reference cases (Controls); Children 12–23 months of age who are fully immunized.
Defaulter
If the child missed at least one of the recommended vaccines, he/she was considered as defaulter.
Complete Immunization
Complete immunization will be considered if the child took all the recommended vaccines including BCG (Bacillus Calmette–Guerin), OPV (Oral Polio Vaccine, Pentavalent), IPV (Inactivated polio vaccine), PCV (Pneumococcal Vaccine), Rota virus vaccine, and measles vaccine by the age of 12–23 months.
Knowledge of the Schedule of Vaccine
If mothers’/immediate care givers’ knows the schedule of at least two vaccine series were considered as knowledgeable.
Maternal knowledge towards the schedule of vaccination was assessed by asking the schedule of at least four vaccines series. A score of “1” was given if the mothers/care takers respond the given questions correctly and “0” if not. The sum and the mean of each response was computed and dichotomized into good and poor knowledge. If respondents scored below the mean, he/she was labeled as having poor knowledge and if the respondents scored above the mean, he/she was labeled as good knowledge.
Ethical Consideration
Before data collection, support letter was secured from Dilla University, Research, Dissemination and Community Services Directorate Office to be submitted to Yirga Cheffe district and town health office for consent. The Institutional Review Board of Dilla University College of Health Science had approved the consent process, and accordingly verbal consent was obtained from mothers/immediate caregivers prior to data collection. The names of the study participants were not included in the questionnaire for confidentiality.
Results
Socio-Demographic Characteristics of the Respondents
The analysis involved 328 children aged 12–23 months residing in the identified study area. The response rate of 164 index cases and 164 reference cases was 98.8%.
Males made up 99 (60.4%) of the 164 child index cases, while females made up 75 (45.7%). Males constituted 56.1% of the reference cases. The mean and standard deviation were 9.72 months and 3.56, respectively. The majority of the children among the index cases and reference cases lie in the age group of 12–23 months, where they accounted for 88.4% and 76.2%, respectively. In both the index case and reference cases groups, 54% of mothers or caregivers were between the ages of 15 and 24. The most important Sociodemographic variables for most mothers in the study unit were Gedio ethnicity, Protestant religion, and living in a rural area.
Mothers of index cases and reference cases who had attended primary school education were 37.2% and 25%, respectively, and 48.2% of mothers of index cases and 53.1% of reference cases children have no education at all, but secondary and higher educational status of mothers of both groups accounted below 15%. In both index cases and reference cases, the primary caregivers were housewives (56%), but government employees accounted for only 7.3% of index cases and 6.1% of reference cases. The median monthly family income of index cases and reference cases was 400 Ethiopian Birr (ETB) (16 United States Dollar (USD) and 450 (18 USD)), respectively, Table S1.
Mothers’ index cases having only a single child within the family members were 15.2%, which accounted for 14% for reference cases and 2 to 4 children alive within the family members for index cases and reference cases were 66.5% and 59.8%, respectively, but five or more alive children within the family members presented for index cases were 18.3% and 26.2% for reference cases. Concerning the birth order of a child, being born first was 16.5% for index cases and 54.3% for reference cases and being second to fourth in the family was 56.1% for index cases and 31.7% for reference cases, but being fifth and above in the family accounted for 27.4% of index cases and 14% of reference cases. Mothers or immediate caregivers with five or fewer children accounted for 31.7% of index case children, 61.6% of reference cases children, but five or more family members accounted for 68.3% of index case children and 238.4% of reference cases children.
Maternal and Child Health Services Utilization and Related Factors
Of the immediate caretakers who vaccinated their children, 15.9% of index cases and 92% of reference cases mothers did not postpone the vaccination schedule. The majority of reasons (70.3%) for postponed vaccination schedule mentioned by mothers/immediate caretakers of children were missing date of appointment but maternal or child illness and social engagement of mothers/immediate caretakers were reasons mentioned by 26.8% partially vaccinated and 69.2% of fully vaccinated children. The immediate caretakers of the index case children (43.6%) and reference case children (56.4%) had attended the ANC follow up during their pregnancy, but 64% of the reference cases immediate caretakers reported a post-natal care (PNC) visit during their last pregnancy (Table 1).
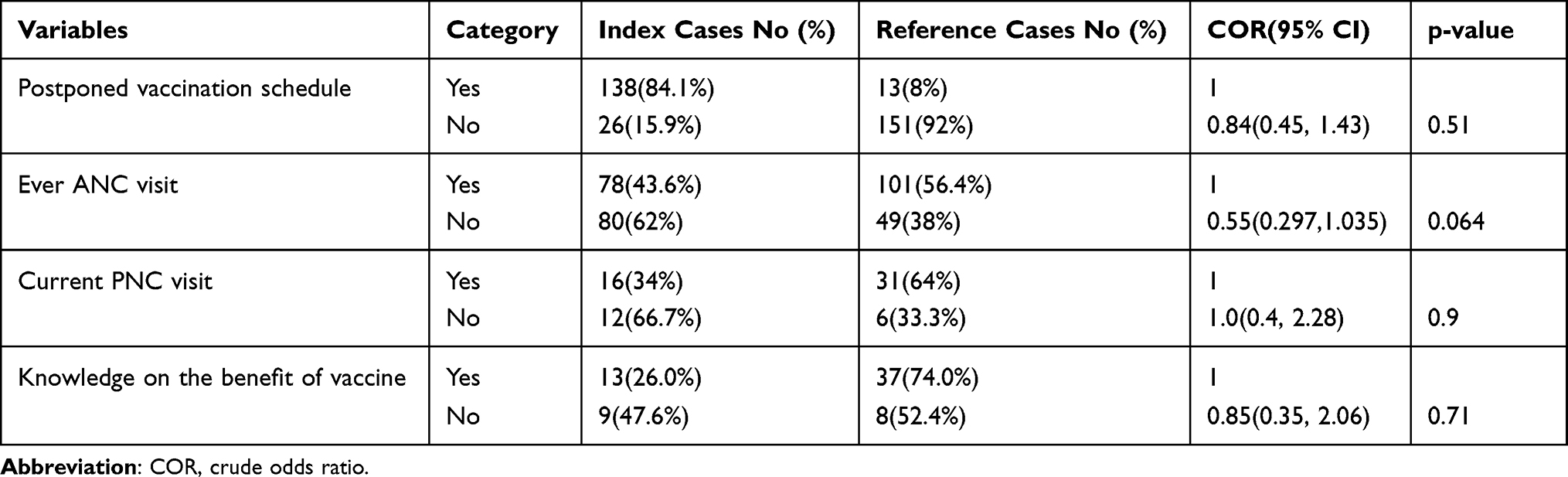 |
Table 1 Bivariate Analysis of Maternal and Child Health Services Utilization and Related Factors in Yirga Cheffe District, South Ethiopia, August 2017 |
Knowledge of Mother’s or Immediate Caretakers About Immunization and Related Factors
From the total mothers/immediate caretakers interviewed, 62.2% of mothers of index cases and 82.3% of reference cases children know about immunization. Among those mothers who were knowledgeable about immunization, the vast majority of mothers of children (91.6%) knew the measles vaccine, but 61.9% and 58.3% of reference cases mothers knew the BCG and the Polio vaccines, respectively. Only 39.7% of mothers in the index case and reference cases knew about immunization, while 60.3% of mothers in the reference cases knew the schedule for at least two types of vaccines (BCG and measles).
Almost 60% of mothers with index case children and 42.4% of mothers with reference cases children are aware of at least two new vaccines (Rota Virus Vaccines and PCV). The proportion of reference cases mothers who knew newly added vaccines, Rota Virus Vaccine (72%) and PCV (75.8%) was almost the same but only 36% mothers of index case children and 64% of reference cases children were aware of vaccines for the prevention of hepatitis virus. The newly inactivated poliomyelitis vaccine (IPV) was unfamiliar to all of the immediate caregivers.
Among the mothers/immediate caretakers of index cases, children (26%) and reference cases (74%) knew the benefit of immunization, and 60.5% believed in its usefulness for the prevention of infectious diseases. Health professionals were the most common source of information about the vaccine’s benefits for mothers of index cases (38.5%) and the reference cases (59.5%) (Table S2).
Factors Related to Immunization Service Delivery
Apart from vaccination, caregivers can take their children to the health facility for other reasons, such as medical illness remedies, which were observed in this study in 39.6% and 60.4% of the index case and reference cases, respectively. This was one of the good opportunities which can be effectively used by healthcare professionals to assess the immunization status of the children and intervene accordingly (Table 2).
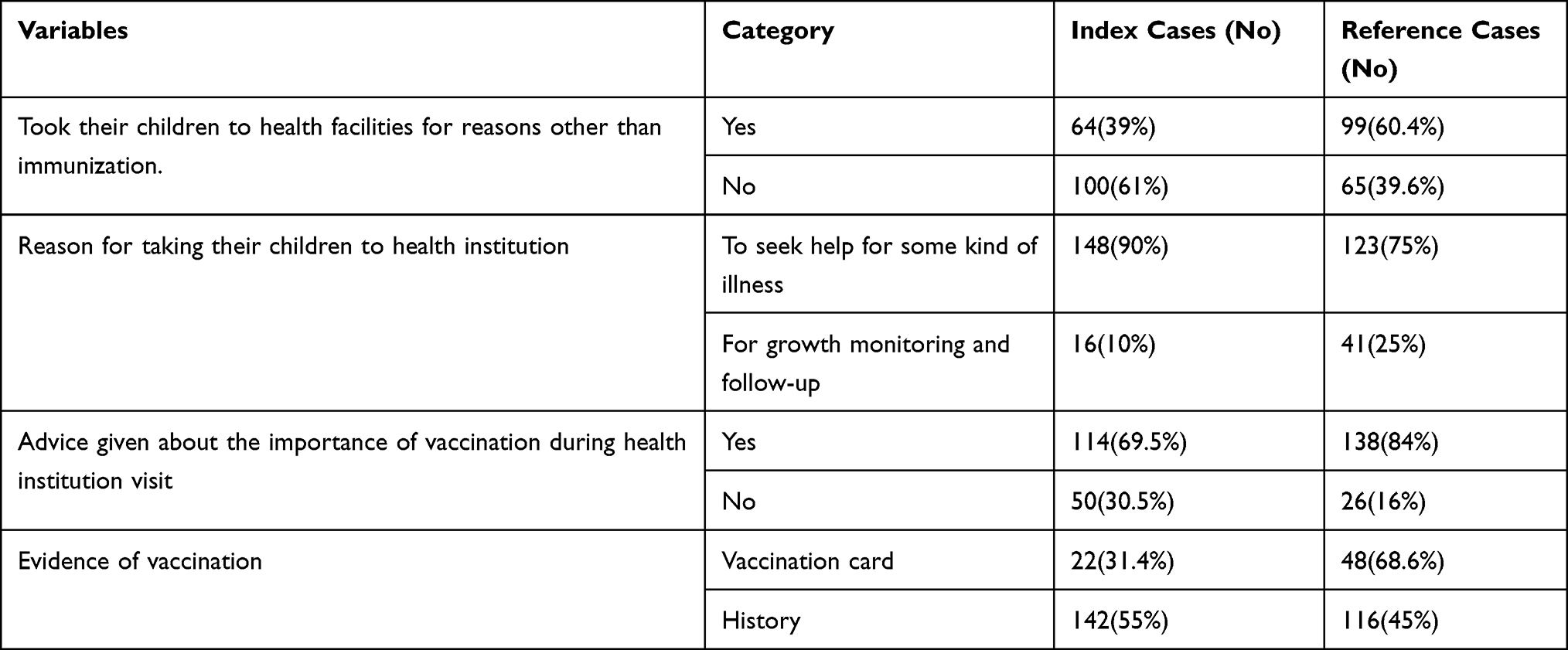 |
Table 2 Immunization Service Delivery of Respondents in Yirga Cheffe District, South Ethiopia, August 2017 |
Immunization Status of Children
About 40% of the children had taken all the recommended immunizations, but 46% of the children were partially immunized. Besides, in our survey, 14% of children were left unvaccinated. Inconvenient vaccination times and a lack of awareness about the importance of vaccination were cited as reasons for incomplete vaccination by nearly half of those polled, but only 17.3% of mothers/immediate caregivers cited a lack of vaccine supplies on the date of appointment and a lack of personnel at the health facility as reasons for incomplete vaccination.
Predictors of Childhood Immunization Status
Factors like maternal age, educational status of mothers, household monthly income, and family size significantly influenced the default to complete vaccination at a p – value of ≤ 0.25 in the bivariate analysis. Whereas maternal age, educational status of mothers, household monthly income, family size, maternal ANC visit, and knowledge of the schedule of vaccine statistically affected the default to full vaccination in multivariable analysis at a p-value of ≤ 0.05 (Table 3).
 |
Table 3 Bivariate Analysis of Socio-Demographic Characteristics of the Respondents Related to Incomplete Child Immunization in Yirga Cheffe District, South Ethiopiaz, August 2017 |
Independent Predictors of Incomplete Immunization
After adjusting for other variables, maternal age, educational status of mothers, household monthly income, and family size maintained their statistical significance.
The odds of incomplete vaccination among younger mothers were 0.308 as compared to older mothers with the default rate of 69% (OR=0.308; 95% CI=0.13, 0.75). The study also depicted that higher literacy was one of the tools where vaccination performance had been improved, like children of care takers who had secondary education [OR=0.45, (95% CI: 0.13, 1.52)] and higher [OR=0.42, (95% CI: 0.20, 1.19)] by literacy level were 55% and 58% lower default rate to complete immunization, respectively, as equated to children of care takers who had any formal education. Monthly family income had a direct association with the completeness of vaccination, with an 83% lower default rate in the monthly income of 500–1000 as compared to less than 500 ETB, [OR=0.17 (95% CI; 0 0/05, 0.68)]. The status of full immunization has been greatly affected by the number of family sizes, and accordingly, having five or more family members was supposed to have a double default rate as compared to those who had less than five family members. [OR = 2.17 (95% CI [1.26, 3.79])]. The likelihood of having incomplete vaccination was 45% higher in children whose mothers had no ANC visit during pregnancy [OR=0.55, (95% CI; 0.297, 1.035)].
Lack of knowledge about the schedule of the vaccination has negatively affected the success of full vaccination (OR=2.3; 95% CI=1.01, 5.56) (Table 4).
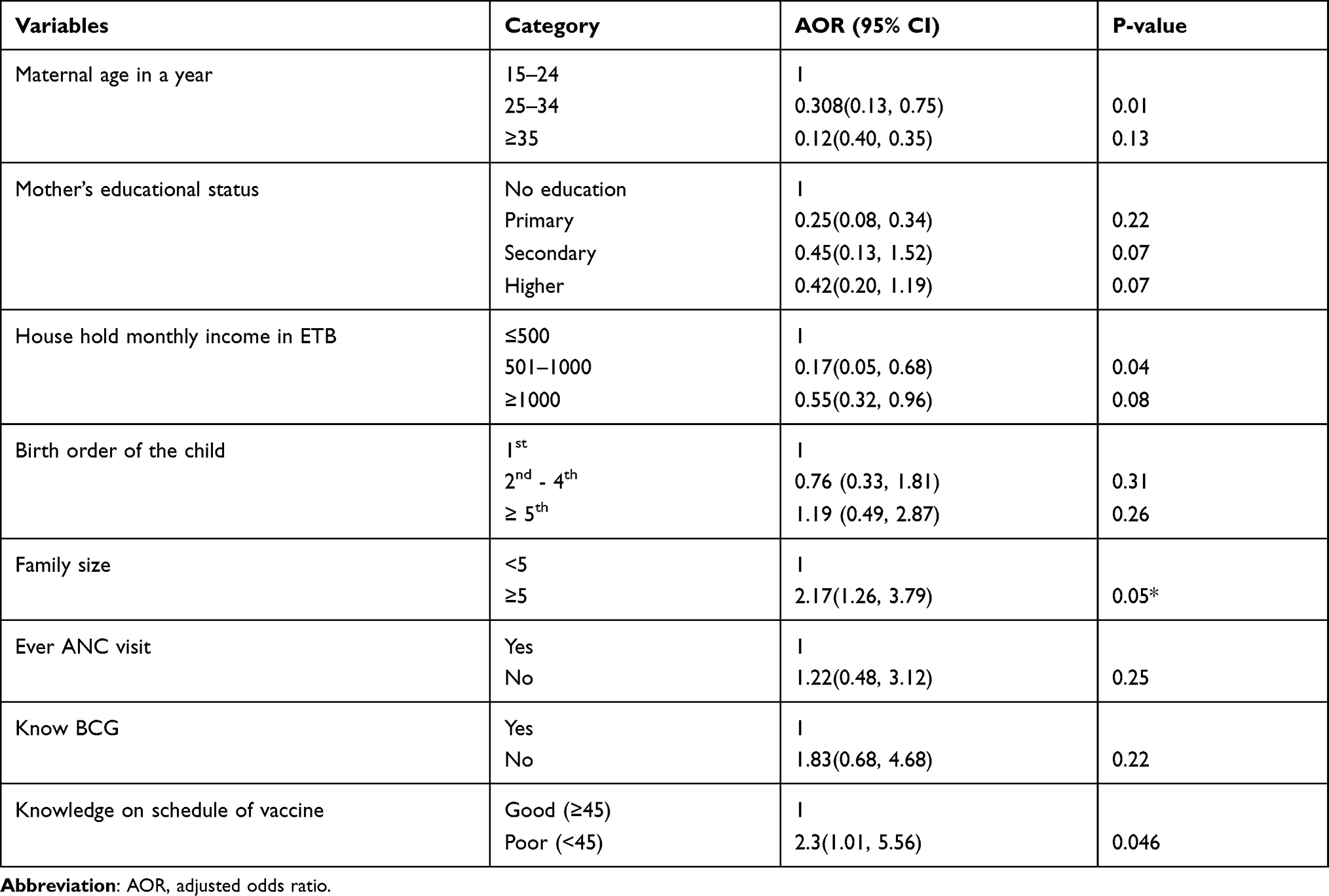 |
Table 4 Multivariate Analysis of Determinants of Incomplete Childhood Immunization Status in Yirga Cheffe District, South Ethiopia, August 2017 |
Discussion
Despite having access to vaccination services every month at the outreach and on a daily basis at the facilities, approximately 46% of the children were not fully vaccinated. Our study revealed a greater proportion of the dropout rate than the study done in Kenya (22.6%).13 But, it was close to the study done in the Wonago district (42%).6 The result was also greater than that of the national EPI cluster survey result (35.6%)5 and invariably nearer to the Ethiopian DHS 2016 survey result, 45%.4 According to the earlier report in 2011 Ethiopian DHS, only 24% of children ages 12–23 months were fully vaccinated.9 This shows there is an improvement in vaccination coverage from year to year, below the target though. The discrepancies among the aforementioned studies are probably due to selection bias, sample size differences, time of studies done, and socioeconomic factors.6,8,10,13,14
Index Case children had a 76% of BCG vaccination rate, which was lower than that of the study carried out in Arbegona (90%) and higher than the Ethiopian DHS 2016 survey (69%), but nearly comparable with the study undertaken in Wonago (73.5%).2,4,6 The measles vaccination rate, 22.6%, was found to be higher than the result of research done in Arbegona (10%) and Wonago (17%) but less than half of the survey done by Ethiopian DHS (54%).2,4,6 This might be because of the Sociodemographic differences among the study areas.6,15–17
Of the strong predictors of incomplete immunizations, the child’s age was one. In the present study, the majority of reference cases children age between 10 and 12 months were fully immunized when compared to older children in comparison to other studies which was comparable with a study done in East Gojjam Zone.11 The trend that younger child getting more attention than the older one might justify this. It could also be because of the current attention given by the Government in immunization coverage.2,4,8,18,19
Families’ traditional male child preferences may result in more male children being vaccinated than their female counterparts. Presumably, traditional society had the habit of keeping females at home rather than taking them to a health facility.6,11–13,17,19
When compared to elderly caregivers, younger mothers have a higher default rate for their children. Our study showed that the age of the caretakers significantly affects health service utilization, ie, the older the mother, the better the utilization of vaccination services. The findings are consistent with case-control study conducted by Nigussie in Arbegona district.2 The reason could be that the elderly/mothers are more aware of the importance of healthcare services and may pay close attention to their children’s immunization status. It could also be because of job-related factors. That is, young mothers are busy earning money.1,4,6,11,12
The mother’s level of literacy influences the child’s immunization status, and the more they educate, the more likely children are to be vaccinated, even though the chances of incomplete immunization were higher in those educated to secondary and above, 55% and 58%, respectively, compared to children born to caretakers who had no education. This result is less than the findings from Ethiopian DHS 2016 survey results, which is about 31% of children whose mothers/immediate caretakers have no formal education complete the recommended vaccination series compared with more than (72%) of index cases with the caretakers being educated to more than the secondary level of education.4 This may be due to the influence of maternal education which helps to increase awareness on the utilization of vaccination services.3,11,17–19
Maternal occupation was not statistically associated with full immunization status in our survey, but this is in contrast to a study from Thailand15 and Yirgalem town8 which found that being a professional government employee for mothers was a significant predictor of childhood immunization status. This might be due to the fact that the majority of the respondents in our survey were housewife. Household monthly income is related to the status of complete childhood vaccination, as found in the Wonago study.6 In this study, there is no significant relationship between parity, birth order, and immunization status of the children. Mothers with five or more children, on the other hand, have a higher chance of having fewer children than mothers with fewer than five children. This could be due to being preoccupied with caring for a large number of children, as well as the state of the economy.3,4,10,13,15,19
Like the research done in the East Gojjam zone,11 low parity was associated with a greater chance of being completely vaccinated, which revealed that children of mothers with lower parity were more likely to be fully immunized. This finding could be correlated to a study carried out in Southwestern Ethiopia19 that revealed children from families with more than one under-five child were less likely to be completely immunized. This is probably because of self-caring in older children and also being in the nursery at an older age will give more freedom for the mother to care for her younger child comfortably.2,11,17–19
Children whose mothers attended antenatal clinics had a lower risk of not being fully immunized. As observed in the study, the ANC has positively affected the completeness of childhood vaccinations, like a study done in the East Gojjam Zone.11 The more you talk to a doctor, the more you’ll learn about the benefits of full vaccinations. Because PNC is not widely used, it will have no effect on the status of full vaccinations, such as the ANC. Still, PNC is one of the opportunities to discuss with the caregiver the importance of full vaccination.2,4,6,7,11,14,17,19
This study revealed that, the more the mother is knowledgeable about the vaccination schedule, the more likely her child will be fully vaccinated (p-value < 0.046). This is consistent with a study conducted in the Wonago district6 which found that children of mothers who remembered the vaccination schedule were three times more likely to be vaccinated than children whose mothers did not remember the due date of vaccination [OR = 3 (95% CI: 1.4, 6.3)]. This highlights the importance of providing health education to mothers/care givers whenever possible, particularly during the ANC follow up. It also involves assigning us duty to look for better methods of reminding them of the vaccination schedule.
Limitations
We tried to find vaccination data from vaccination cards, but not all women had vaccination cards for their children. Mothers’/immediate care-takers’ recall bias may affect their children’s immunization status, as well as over-reporting of vaccine doses due to complacency, without the ability to check the information. As such, we did not rely on mothers’ verbal reports, which are subject to recall bias, and the cases and controls were misclassified. The other point is, this study did not explore the factors associated with a high dropout rate between initial and subsequent doses of routine vaccinations. We, hence, recommend the findings in this paperwork should carefully be interpreted.
Conclusion
The study revealed that incomplete vaccination is still in excess of the tolerable level. The reasons given by mothers for the vaccination schedule being postponed/omitted include a missed appointment date, maternal social engagement, and maternal/child illness. As a result, intensive health education and work on the identified core problems are required to improve complete immunization coverage. We especially recommend the expansion of ANC, and providing education on vaccination schedule and importance to minimize the burden of partial vaccinations and its sequelae.
Data Sharing Statement
All data are available without restriction.
Ethics
This study was executed in compliance with Helsinki Declaration.
Acknowledgments
We acknowledge all individuals who contributed to the accomplishment of this paperwork, especially Dilla University, Hawassa University, and Pharma Health Science College (Hawassa branch).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There was no funding agency for this paper.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Abdulraheem JA, Oladipo A. Reasons for incomplete vaccination and factors for missed opportunities among rural Nigerian children. J Public Health Epidemiol. 2011;3(4):194–203.
2. Abel Nigussie WK, Assegid S, Hagan AK. Factors associated with incomplete childhood immunization in Arbegona district, southern Ethiopia: a case – control study. BMC Public Health. 2016;16(27):1–5.
3. Harris JBG-DM, Eggers R, Brown DW, Sodha SV. Global routine vaccination coverag. BMC Public Health. 2014;63(46):1055–1058.
4. Federal Ministry of Health AAE. Central Statistical Agency, Ethiopia Demographic and Health Survey. 2016:3–11
5. Federal ministry of Health (FMOH) E. EPI Cluster Sampling Coverage Survey. 2006:3–6
6. Tadesse HDA, Wolde M. Predictors of defaulting from completion of child immunization in South Ethiopia, A case-control study. BMC Public Health. 2009;9(150). doi:10.1186/1471-2458-9-150
7. Federal Ministry Of Health E. Ethiopian National Expanded Program on Immunization. Comprehensive Multi-Year Plan 2016 – 2020.; 2015.
8. Mesfin M. Incomplete vaccination and associated factors among children aged 12-23 months in Yirgalem Town, South Ethiopia. BMC Public Health. 2015;1–7.
9. Federal Ministry Of Health E. Ethiopia Demographic and Health Survey. Central Statistical Agency; 2011.
10. Federal ministry of Health (FMOH) E. National Expanded Program on Immunization. 2015:2–3
11. Yenit MKAS, Abrha H. Factors associated with incomplete childhood vaccination among children 12-23 months of age in Machakel Woreda, East Gojjam Zone: a case control study. J Pregnancy Child Health. 2015;2(4):180.
12. Atomsa HMA. Assessment of child immunization coverage and associated factors. BMC Public Health. 2010.
13. Moses NKDC, Amina I, Salome C, et al.Immunization coverage and risk factors for failure to immunize within the Expanded Program on Immunization in Kenya after introduction of new Haemophilus influenza type b and hepatitis b virus antigens. BMC Public Health. 2006;6:132.
14. Orenstein WADR, Rodewald LE. Immunizations in the United States: success, structure and stress. Health Affairs (Millwood). 2005;24(3):599–610. doi:10.1377/hlthaff.24.3.599
15. Sein Lei Than OL, Mongkolchati A. Determinants of incomplete immunization among hill tribe children aged under two years in Myanmar, Thailand. Journal of Public Health Dev. 2016;14(2):17–28.
16. Simons EFM, Fricks J, Wannemuehler K, et al. Assessment of the 2010 global measles mortality reduction goal: results from a model of surveillance data. The Lancet. 2012;379(9832):2173–2178. doi:10.1016/S0140-6736(12)60522-4
17. Lfred Douba NALB, Attoh-Toure H, Bangaman Akani C, et al. An analysis of risk factors for incomplete immunization for children in côte d’ivoire: examination of 1998-1999 and 2011-2012 demographic and health survey. Health Sci Dis. 2016;17(1):1–7.
18. Gianluca R, Patrizio P, Rodrigue MB, et al. Vaccine coverage and determinants of incomplete vaccination in children aged 12–23 months in Dschang, West Region, and Cameroon: a cross-sectional survey during a polio outbreak. RBMC Public Health. 2015;15:630.
19. Yohannis Dibaba Wado MFA, Hindin MJ. Childhood vaccination in rural Southwestern Ethiopia: the nexus with demographic factors and women’s autonomy. Pan Afr Med J. 2014;1(9):3–4.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.