Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Predictors of Mortality Among Children with Confirmed and Suspected Cases of COVID-19 in East Java, Indonesia
Authors Efendi F ![]() , Haryanto J, Has EMM, Makhfudli M
, Haryanto J, Has EMM, Makhfudli M ![]() , Indarwati R, Kuswanto H, Wahyuhadi J, Farabi MJA, Ho KHM
, Indarwati R, Kuswanto H, Wahyuhadi J, Farabi MJA, Ho KHM ![]() , Susanti IA
, Susanti IA ![]()
Received 6 October 2022
Accepted for publication 24 January 2023
Published 7 February 2023 Volume 2023:16 Pages 355—362
DOI https://doi.org/10.2147/JMDH.S391917
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ferry Efendi,1 Joni Haryanto,1 Eka Mishbahatul Mar’ah Has,1 Makhfudli Makhfudli,1 Retno Indarwati,1 Heri Kuswanto,2 Joni Wahyuhadi,3,4 Makhyan Jibril Al Farabi,4,5 Ken Hok Man Ho,6 Ika Adelia Susanti7
1Faculty of Nursing, Universitas Airlangga, Surabaya, Indonesia; 2Department of Statistics, Institut Teknologi Sepuluh Nopember, Surabaya, Indonesia; 3Department of Neurosurgery, Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia; 4Dr. Soetomo General Hospital, Surabaya, Indonesia; 5Department of Cardiology and Vascular Medicine, Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia; 6Nethersole School of Nursing, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, Hong Kong; 7Faculty of Health Science, Universitas dr. Soebandi, Jember, Indonesia
Correspondence: Ferry Efendi, Email [email protected]
Introduction: Coronavirus disease 2019 (COVID-19) increases rapidly and causes mortality in all groups, including children. However, the predictive risk factors of mortality among children remain inconclusive. This study aimed to analyse the predictors related to mortality among children with COVID-19.
Methods: Secondary data analysis was conducted using provincial COVID-19 data from April 2020 to May 2021. We selected 6441 children under age 18 to be included in this study. Chi-square and binary logistic regression were used to evaluate the predictors of mortality in children with COVID-19.
Results: This study showed that the prevalence of children who died COVID-19 was 2.7%. Age, case definition, treatment status, severity of illness, and travel history had a significant relationship with survival status in children with COVID-19. As the increasing age, the risk of death with COVID-19 will decrease [AOR=0.94; CI 95%=0.91– 0.97]. Otherwise, suspected status [AOR=2.12; 95% CI=1.48– 3.04], hospitalization with ventilators [AOR=22.25; 95% CI=5.73– 86.42], severe illness [AOR=46.76; 95% CI=21.69– 100.80], and travel history [AOR=1.78; 95% CI=1.22– 2.60] were significantly related with an increased risk of death in children with COVID-19.
Discussion: Severe illness in children was the strongest predictor of mortality. Disease prevention and health promotion programs are the key to preventing hospitalizations in children and decreasing the mortality rate.
Keywords: child health, COVID-19, child mortality
Introduction
Coronavirus disease 2019 (COVID-19) poses a major risk of mortality worldwide.1 Since COVID-19 was declared a worldwide pandemic by the World Health Organization in March 2020, the number of reported cases, deaths, and affected countries has continuously increased.2 By June 2020, global reports of COVID-19 recorded 10 million cases and 503,862 deaths, with several countries categorized as having community transmission.3 At the same time, Indonesia also reported a total of 55,092 confirmed cases, the third country in Southeast Asia with the highest number of confirmed cases.3 Most provinces in the Java region reported an increase in cases and deaths.4 The East Java Province became the first province in Indonesia, with the highest number of cases reaching 11,823 by June 2020.5 The COVID-19-related fatality rate in East Java continues to increase, reaching 7.44%.6,7 Moreover, based on data from online hospital applications, the East Java Provincial Health Office announced that the bed occupation rate (BOR) in East Java reached more than 80% and was categorized as a red zone area.8 This fact requires special attention in overcoming the COVID-19 pandemic and reducing the number of confirmed cases and COVID-related deaths in East Java Province.9
The COVID-19 data update in East Java was conducted by the COVID-19 task force and reported through online systems such as websites, mass media, and government accounts.10,11 Although the trend of COVID-19 cases shows fluctuating data, the overall number cases in East Java have increased.6 Each region implements strict health protocols to manage the outbreak of a small number of cases to reduce the likelihood of a larger number of cases. Public health protection is provided through several strategies: health promotion, early detection, physical and social restrictions, coughing and sneezing etiquette, self-isolation, and quarantine.12 However, these efforts have not significantly reduced the number of COVID-19 cases in East Java.
Several studies have been conducted on COVID-19 to assess treatment-related risk factors and the clinical features of COVID-19 have become clearer in identifying the virus that causes COVID-19 and acute respiratory syndrome coronavirus 2 (SARS-CoV-2).13–16 The impact of COVID-19 on patients is clinically complex; outcomes may range from asymptomatic respiratory failure to death.17 In a pandemic, community resilience must be considered, especially for vulnerable groups.18 A previous study showed that the elderly were the most vulnerable population at risk, especially those with heart disease, respiratory disease, diabetes, or other autoimmune diseases.19 Although children appear to have milder symptoms and a better prognosis than adults,15,20,21 the number of cases in children is growing rapidly.22 It may also contribute to community transmission.23 Moreover, the potential harm caused by COVID-19 in children remains largely unknown, especially in neonates and infants.24 Previous studies have shown that several factors contribute to the fatality rate of children, such as those age ≥ 10 years, severe illness, poor oxygen ratio, and chronic underlying disease.25–27 Although several studies have analysed the predictors of mortality, most of the studies have focused on adults and the elderly, leading to difficulty in generalization. In this context, this study aimed to examine predictors of mortality among patients with COVID-19, especially in children.
Materials and Methods
Data Source
This study was a secondary data study using provincial COVID-19 data in Indonesia particularly in East Java province. The children dataset used for this study contains information about children aged less than 18 years and their health data related to COVID-19. East Java province COVID-19 platform pooled all of data from April 2020 to May 2021 through an online platform. The researcher applied for dataset access permission the East Java COVID-19 task force to obtain research data. The data were obtained from all health facilities in East Java that served all cities or regency within East Java province. Each health facilities were obliged to report all the cases to the data platform.
Subjects
This study involved paediatric patients with COVID-19 in East Java. The purposive sampling method was used to select a sample of 6441 children. The sampling technique allows selected respondents in population to be included in sampling due to certain criteria. The inclusion criteria in this study were children aged less than 18 years, either outpatient or inpatient. The definition of children following the guideline from the Government of Indonesia.28
Variables
The dependent variable in this study was survival status, namely, alive and dead. The time point started from the first-time admission to the health facilities until they discharged (dead or alive). Alive and dead is the current status when conducting data collection in May 2021 on health care status in outpatient and inpatient patients. Independent variables included sex, case definition, treatment status, severity of illness, travel history, and exposure to a person with a suspected/confirmed case of COVID-19. Sex was divided into two categories: male and female. In this study, the case definition category is divided into confirmed and suspected. Confirmed cases can be defined as positive cases of COVID-19 infection as evidenced by polymerase chain reaction (PCR) tests. Meanwhile, suspected cases were defined as cases that showed COVID-19-like symptoms with inconclusive results using PCR or any other type of testing.12 Treatment status was divided into three categories: non-hospitalized (isolation), hospitalized, and hospitalized with a ventilator. The severity of illness was divided into mild, medium, and severe based on reference to the Decree of the Minister of Health of the Republic of Indonesia. Mild symptoms include fever, cough, fatigue, anorexia, shortness of breath, myalgias, or other unspecified symptoms without evidence of viral pneumonia or without hypoxia. Moderate symptoms are characterized by the presence of clinical signs of pneumonia (fever, cough, shortness of breath, rapid breathing) without signs of severe pneumonia. Meanwhile, severe symptoms are characterized by clinical signs of pneumonia coupled with a respiratory rate > 30 x/minute or severe respiratory distress.29 Travelling history and exposure to a person with a suspected/confirmed case of COVID-19 was divided into two categories: yes and no.
Data Analysis
SPSS version 25 was used for data analysis in this study. The data that were obtained were analysed using chi-square and logistic regression to examine the determinants of survival status in children with COVID-19. To determine the strength of the relationship between the dependent and independent variables, it was assessed using an odds ratio and 95% confidence interval (CI) (p<0.05). We adjusted for any variables known to be associated with the independent variables. All the missing data were excluded from this analysis.
Ethical Approval
The datasets used in this study are available upon request after all individual-level identification variables were removed. It was not possible to identify the residence of any of the subjects. Therefore, ethical approval was not required for the study. This study confirmed that informed consent was obtained from all participants and performed according to the Declarations of Helsinki ethical principles for medical research involving human subjects.30
Results
Out of 6441 children, 3496 children with COVID-19 in East Java were male (54.3%) and categorized as having a suspected case of COVID-19 (65.4%). Based on treatment status, as of 60% children were hospitalized (60.0%) and a few were hospitalized with a ventilator (1.2%). Higher percentage of the children with COVID-19 had mild cases (86.4%), no travel history (58.8%) and were exposed to a person with a suspected/confirmed case of COVID-19 (63.2%) (Table 1). Table 1 also describes a bivariate analysis of the survival status of paediatric patients with COVID-19, with 177 children (2.7%) dead and 6246 children (97.3%) alive. From the analysis results, several factors related to mortality among children with COVID-19 including treatment, severity of illness, and travel history.
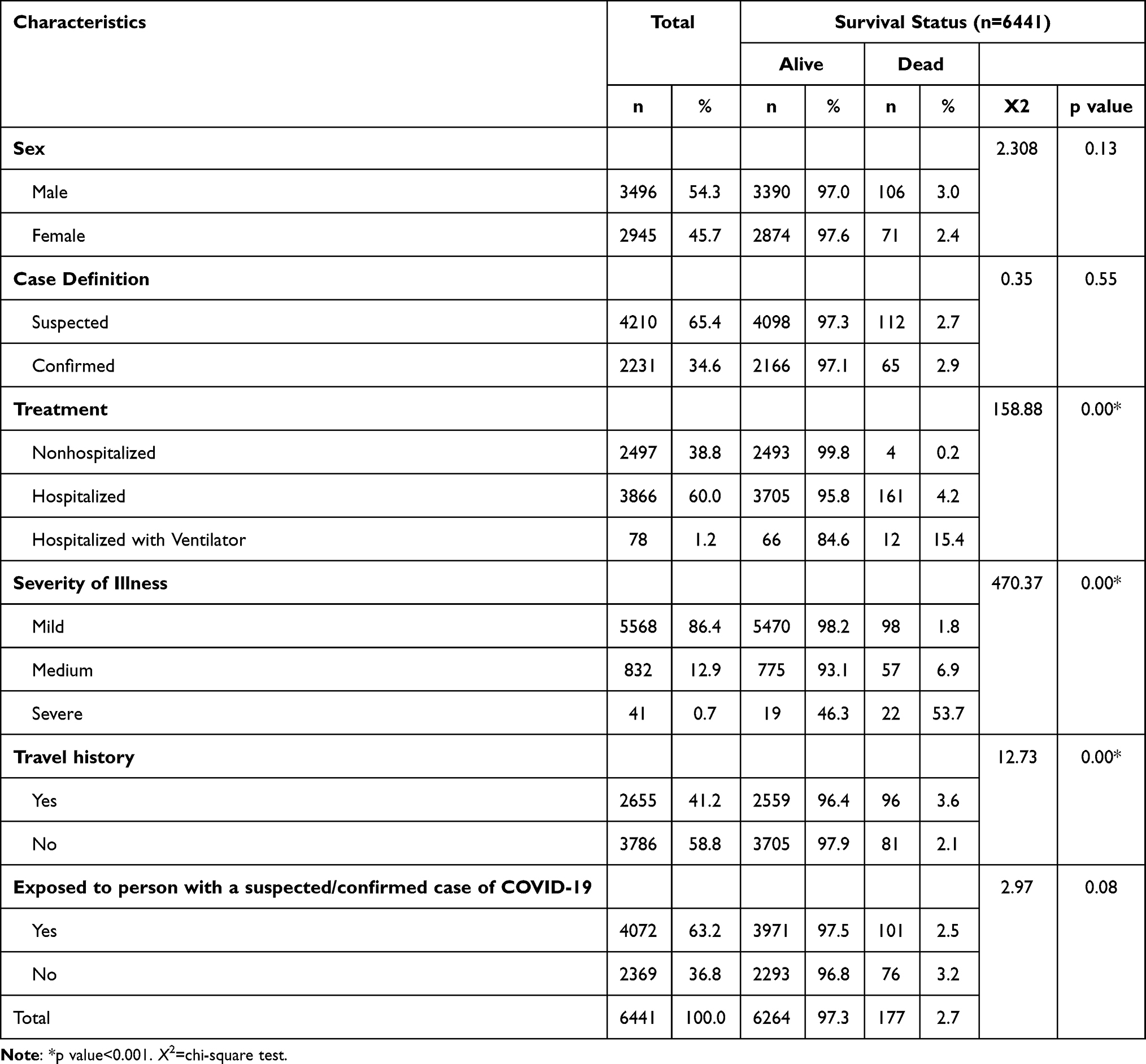 |
Table 1 Sociodemographic Data of Patients with COVID-19 (n=6441) |
In a multivariate analysis using logistic regression, it was found that age, case definition, treatment status, severity of illness, and travel history had a significant relationship with survival status in children with COVID-19 in East Java. Based on the analysis results, as the child’s age increases, the risk of death will decrease by 0.94 times [AOR=0.94; 95% CI=0.91–0.97]. Children with a suspected case of COVID-19 have a higher risk of death than children with a confirmed case of COVID-19 [AOR=2.12; 95% CI=1.48–3.04]. Meanwhile, children hospitalized with ventilators had the highest risk of death, reaching 22 times that of isolated children [AOR=22.25; 95% CI=5.73–86.42]. The survival status of children with severe cases was 47 times more likely to die than those with mild cases [AOR=46.76; 95% CI=22.69–100.80]. The risk of death in children increased almost twice in children with a travel history compared to children without a history of travel [AOR=1.78; 95% CI=1.22–2.60] (Table 2).
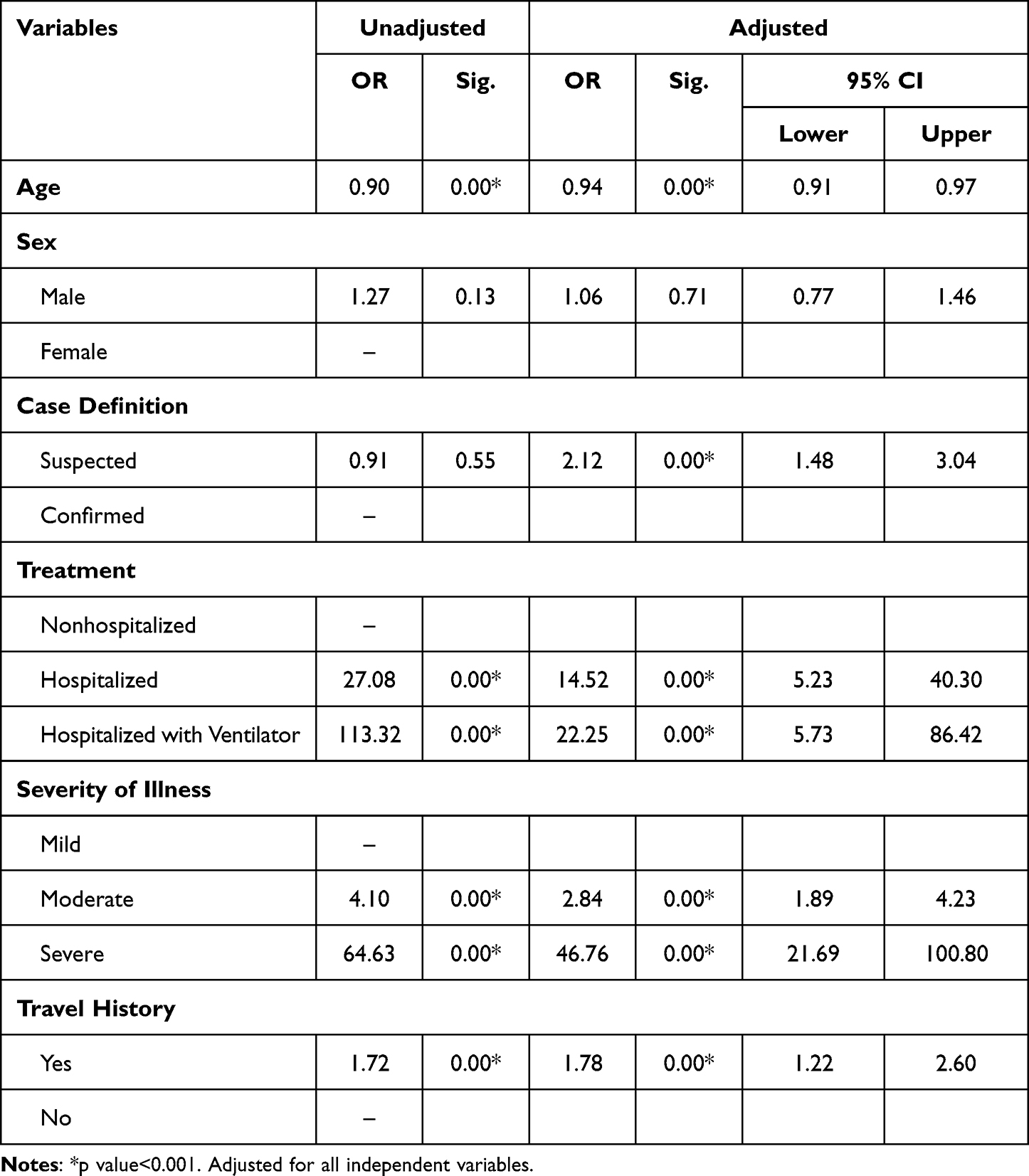 |
Table 2 Multivariate Analysis of Survival Status in Children with COVID-19 (n=6441) |
Discussion
The results showed several factors related to mortality among children with COVID-19 in East Java. As the child’s age increases, they are less likely to die of COVID-19. This result is in line with a previous study showing that the most significant proportion of severe and critical cases in children under one year of age was higher than that in older children, reaching 10.6%.31 The authors argue that the health facilities in East Java do not support the most significant number of critical cases in children under one year of age. This increases the risk of death in younger children than that in older children. At first, neonates and infants were not prioritized in the first wave of the pandemic. In 2020, the government focused on the elderly group, and the capacity for paediatric care was limited.32 This statement was also supported by data from online hospital applications that reported that the number of beds in the Neonatal Intensive Care Unit (NICU) and Paediatric Intensive Care Unit (PICU) in East Java were very limited in 2020.8 Furthermore, these results can be used as supporting data to identify indicators of mortality in high-risk patients with COVID-19, such as the risk associated with the child’s age.
Case definition was significantly related to the survival status in children with COVID-19. Children with suspected status have a 2.12 higher risk of death than children with confirmed status. This study is similar to previous research in which there were more suspected cases in children than confirmed cases, reaching 65.9%.33 A patients with a confirmed case of COVID-19 showed clinical signs and symptoms compared with patients with a suspected case.34 Patients with a confirmed case, by definition, may experience severe symptoms such as difficulty breathing, loss of speech/mobility, confusion, and chest pain.19 Based on this definition, the signs and symptoms and illness severity cause patients with confirmed cases of COVID-19 to have an increased risk of mortality. Although the clinical manifestations of children with COVID-19 are generally less severe than those of adults, they are more susceptible to infection.33 We also assume that children with confirmed status have rapid treatment and intervention compared with suspected cases. Thus, it can increase the risk of mortality among children with suspected cases.
Based on the results of this research, treatment factors were found to be significantly related to survival in children with COVID-19. Children who were hospitalized on a ventilator had 22 times higher risk of death than isolated children. This finding is consistent with studies conducted in Saudi Arabia showing that patients on mechanical ventilators (MVs) experience a high risk of death from COVID-19.35 Additionally, another study showed that the risk of death in patients admitted to the intensive care unit was high among hospitalized patients with COVID-19.36 Children and paediatric patients who required intensive care and those who died had different comorbidities with hydronephrosis, leukaemia, and intussusception.37 This demonstrated that comorbidities might be one of the factors contributing to the survival status of patients with COVID-19, but our data did not analyse this issue. The survival probability among patients with COVID-19 is also associated with the length of hospital stay (LOS), in which the first 14 days of hospitalization have a higher survival probability than patients treated for 30 days.35 Hospitalized children had a higher prevalence of symptoms, namely, fever, respiratory and gastrointestinal symptoms, and relatively lower haemoglobin and neutrophil levels.38 Based on this finding, we think this remains important to assess symptoms in children with COVID-19 to determine indications for hospitalization and ventilator use to increase survival probability.
The present study demonstrated that the survival status of children was associated with the severity of illness. Children with severe cases were 47 times more likely to die than those with mild cases. This study is in line with previous research conducted in China showing that the severity of illness in the nonsurvival group was higher than that in the survivor group.39 The mortality rate among patients with critical and severe cases increased to 17.6%. Decreases in arterial partial pressure of oxygen (PaO2) and the fraction of inspired oxygen (FiO2) were detected among nonsurviving patients with COVID-19, which mainly caused acute lung injury and death, especially in severely ill patients.39 Another study also showed that severe COVID-19 causes approximately 20% of hospitalizations and causes acute respiratory distress syndrome (ARDS) and viral sepsis.40 We suspect that although children have a risk of mild disease severity, infants and children with congenital (pre-existing) illnesses and various comorbidities, such as malignancy, could be a precipitating factor for increased disease severity, requiring ICU care, as described by previous studies.37,41 This illustrates the urgent need for an early warning system to monitor the progression of COVID-19 in children.
The last factor related to the risk of death in children was travel history. Children with a travel history were more likely to die than children without a travel history. This finding is consistent with a previous study showing that the major risk factors for COVID-19 in children were related to having close contact with family members with COVID-19, travel history, and living in endemic areas.37 A travel history is related to community mobility which has been believed to contribute to the increase of COVID-19 transmission.42 We also suspected that community mobility among children increases the risk of COVID-19 exposure, which increases children’s vulnerability to severe illness and death.
Limitations
Some limitations were identified in this study. First, the data were secondary and contained only certain variables. Therefore, researcher only select the available variables within the dataset. Second, the results of this study do not imply causality. Further the data were not reported the possibility of bias on the testing site and the cause of dead of the children. Despite these limitations, this study contributes to informing determinant factors of mortality among children with confirmed and suspected cases of COVID-19 in a specific population.
Conclusion
Mortality among children with COVID-19 was determined by several factors, including age, suspected status, hospitalization with ventilators, severe illness, and travel history. The key to reducing the risk of COVID-19-related mortality among children remains at the clinical and community levels. The promotion and prevention strategy should be deployed massively to reduce the risk of transmission at the community level. While at the clinical setting, resources should be utilized to prevent children getting severe condition. Therefore, initiatives to improve patient management like supportive care including provision of respiratory support, nutrition support, and family support at the clinical level should be implemented and prevention strategies within the community should also be improved. At the community level, health education through face-to-face or virtual can be implemented to give supportive care and monitor the health status of children.
Data Sharing Statement
The datasets analysed during the current study available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Universitas Airlangga, Surabaya, Indonesia through “Hibah Riset Mandat Top Tier” (Top Tier Mandate Research Grant) grant number [768/UN3.15/PT/2021].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Odd D, Stoianova S, Williams T, et al. Child mortality in England during the COVID-19 pandemic. Arch Dis Child. 2021;107(3):e22.
2. World Health Organization. WHO director-general’s opening remarks at the media briefing on COVID-19-11 march 2020. WHO Dir Gen Speeches. 2020;2020:4.
3. World Health Organization. Coronavirus disease (COVID-19) situation report – 162 30 June 2020. WHO. 2020;8(1):3–8.
4. World Health Organization. Coronavirus Disease 2019 (COVID-19) situation report - 60; 2021.
5. Satgas COVID-19. Map of Distribution of COVID-19 Covid19 (Peta Sebaran COVID-19 Covid19); 2020.
6. Pemprov Jatim. East Java COVID-19 distribution map (Peta Sebaran COVID-19 Jatim); 2019.
7. Kemenkes RI. Info on emerging infections of the ministry of health of the republic of Indonesia: special info on COVID-19 (Info Infeksi emerging kementerian kesehatan republik Indonesia: info khusus COVID-19) ;2022.
8. Aplikasi RS Online. An overview of the COVID-19 Bed Occupation Rate (BOR) in East Java (Gambaran BOR COVID-19 di Jawa Timur); 2021.
9. Mastuti S, Aji TN, Liana C Covid-19 disaster mitigation policy in surabaya in pressing positive increasing numbers. In:
10. Pemerintah Provinsi Jawa Timur. East Java Responds to COVID-19 (Jatim Tanggap COVID-19). Pemerintah Provinsi Jawa Timur; 2021.
11. Pemprov Jatim. East java responds to COVID-19 (Jatim Tanggap COVID-19); 2021.
12. Kemenkes RI. Guidelines for prevention and control of coronavirus disease (COVID-19) (Pedoman Pencegahan dan Pengendalian Coronavirus Disease (COVID-19)); 2020:1–214.
13. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi:10.1016/S0140-6736(20)30566-3
14. Epidemiology Team. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19)—China, 2020. China CDC Wkly. 2020;2(8):113.
15. Ludvigsson JF. Systematic review of COVID‐19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. 2020;109(6):1088–1095. doi:10.1111/apa.15270
16. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
17. Siegel RM, Mallow PJ. The Impact of COVID-19 on Vulnerable Populations and Implications for Children and Health Care Policy. Clin Pediatr. 2021;60(2):93–98. doi:10.1177/0009922820973018
18. Saleem H, Rahman J, Aslam N, Murtazaliev S, Khan S. Coronavirus disease 2019 (COVID-19) in children: vulnerable or spared? A systematic review. Cureus. 2020;12:5.
19. World Health Organization. Coronavirus disease (COVID-19). World Health Organization; 2021.
20. Shekerdemian LS, Mahmood NR, Wolfe KK, et al. Characteristics and outcomes of children with coronavirus disease 2019 (COVID-19) infection admitted to US and Canadian pediatric intensive care units. JAMA Pediatr. 2020;174(9):868–873. doi:10.1001/jamapediatrics.2020.1948
21. Ding Y, Yan H, Guo W. Clinical characteristics of children with COVID-19: a meta-analysis. Front Pediatr. 2020;8:431. doi:10.3389/fped.2020.00431
22. Ma H, Hu J, Tian J, et al. A single-center, retrospective study of COVID-19 features in children: a descriptive investigation. BMC Med. 2020;18(1):1–11. doi:10.1186/s12916-020-01596-9
23. World Health Organization. COVID-19 disease in children and adolescents. World Health Organization; 2021:1–10.
24. De Rose DU, Piersigilli F, Ronchetti MP, et al. Novel Coronavirus disease (COVID-19) in newborns and infants: what we know so far. Ital J Pediatr. 2020;46(1):56. doi:10.1186/s13052-020-0820-x
25. Dewi R, Kaswandani N, Karyanti MR, et al. Mortality in children with positive SARS-CoV-2 polymerase chain reaction test: lessons learned from a tertiary referral hospital in Indonesia. Int J Infect Dis. 2021;107:78–85. doi:10.1016/J.IJID.2021.04.019
26. Leoni MLG, Lombardelli L, Colombi D, et al. Prediction of 28-day mortality in critically ill patients with COVID-19: development and internal validation of a clinical prediction model. PLoS One. 2021;16(7):e0254550. doi:10.1371/journal.pone.0254550
27. Kim W, Han JM, Lee KE. Predictors of mortality in patients with COVID-19: a systematic review and meta-analysis. Korean J Clin Pharm. 2020;30(3):169–176. doi:10.24304/kjcp.2020.30.3.169
28. GoI. Undang-Undang Republik Indonesia Nomor 23 Tahun 2002 Tentang Perlindungan Anak. Sekretariat Negara; 2002.
29. Kepmenkes RI. Decree of the minister of health of the republic of Indonesia number HK.01.07/Menkes/5671/2021 concerning clinical management of corona virus disease 2019 (Covid-19) in Health Service Facilities (Keputusan Menteri Kesehatan Republik Indonesia Nomor HK. Tentang Managemen Klinis COVID-19 di Fasilitas Layanan Kesehatan; 2021.
30. WMA General Assembly. WMA declarations of Helsinki - ethical principles for medical research involving human subjects. Brazil: WMA General Assembly; 2013:1975.
31. Dong Y, Mo XI, Hu Y, et al. Epidemiological characteristics of 2143 pediatric patients with 2019 coronavirus disease in China. Pediatrics. 2020;145. doi:10.1542/peds.2020-0702
32. Kemenkes RI. Avoid the elderly from covid-19 (Hindarkan Lansia dari Covid-19). Pusat Analisis Determinan Kesehatan Kementerian Kesehatan Republik Indonesia 2020.
33. Dong Y, Mo X, Hu Y, et al. Epidemiology of COVID-19 among children in China. Pediatrics. 2020;145:6.
34. World Health Organization. Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease is Suspected: Interim Guidance, 13 March 2020. World Health Organization; 2020.
35. Khan AA, AlRuthia Y, Balkhi B, et al. Survival and estimation of direct medical costs of hospitalized COVID-19 patients in the Kingdom of Saudi Arabia. Int J Environ Res Public Health. 2020;17(20):7458. doi:10.3390/ijerph17207458
36. Abate SM, Checkol YA, Mantedafro B, Basu B. Prevalence and risk factors of mortality among hospitalized patients with COVID-19: a systematic review and meta-analysis. Bull World Heal Organ. 2020;2020:10.
37. Alsohime F, Temsah MH, Al-Nemri AM, Somily AM, Al-Subaie S. COVID-19 infection prevalence in pediatric population: etiology, clinical presentation, and outcome. J Infect Public Health. 2020;13:1791–1796. doi:10.1016/j.jiph.2020.10.008
38. Parcha V, Booker KS, Kalra R, et al. A retrospective cohort study of 12,306 pediatric COVID-19 patients in the United States. Sci Rep. 2021;11(1):1–10. doi:10.1038/s41598-021-89553-1
39. Zhang XB, Hu L, Ming Q, et al. Risk factors for mortality of coronavirus disease-2019 (COVID-19) patients in two centers of Hubei province, China: a retrospective analysis. PLoS One. 2021;16(1):e0246030. doi:10.1371/journal.pone.0246030
40. Prescott HC, Girard TD. Recovery from severe COVID-19: leveraging the lessons of survival from sepsis. JAMA. 2020;324(8):739–740. doi:10.1001/jama.2020.14103
41. Dhochak N, Singhal T, Kabra SK, Lodha R. Pathophysiology of COVID-19: why children fare better than Adults? Indian J Pediatr. 2020;87(7):537–546. doi:10.1007/s12098-020-03322-y
42. Nouvellet P, Bhatia S, Cori A, et al. Reduction in mobility and COVID-19 transmission. Nat Commun. 2021;12(1):1–9. doi:10.1038/s41467-021-21358-2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.