")
Back to Journals » Patient Preference and Adherence » Volume 17
Predictors of Medical Care Delay or Avoidance Among Chinese Adults During the COVID-19 Pandemic
Received 23 August 2023
Accepted for publication 2 November 2023
Published 22 November 2023 Volume 2023:17 Pages 3067—3080
DOI https://doi.org/10.2147/PPA.S436794
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Lili Kang,1 Changle Li,1 Huifeng Du2
1School of Health Management, Fujian Medical University, Fuzhou, People’s Republic of China; 2School of Health Management, Inner Mongolia Medical University, Hohhot, People’s Republic of China
Correspondence: Huifeng Du, School of Health Management, Inner Mongolia Medical University, Chilechuan Dairy Development Zone, Hohhot, 010110, People’s Republic of China, Email [email protected]
Purpose: Medical care delay or avoidance increases morbidity and mortality risk and is costly for the national healthcare system. The objective of this study was to identify factors associated with medical care delay or avoidance among Chinese adults during the COVID-19 pandemic.
Materials and Methods: A cross-sectional analysis was conducted using data from the 2020 China Family Panel Study (CFPS). The CFPS was conducted from July to December 2020 during the COVID-19 pandemic. The final sample included 4369 adults. A logistic regression model was employed to identify the factors associated with medical care delay or avoidance.
Results: The empirical results indicate that regardless of rural-urban residence, older adults and adults with chronic conditions were less likely to delay or avoid medical care during the pandemic. However, individuals who had completed more than three years of college showed a higher likelihood of delaying or avoiding medical care. In urban areas, larger family sizes, greater general trust in physicians, and higher provider structural quality were associated with a decreased probability of delaying or avoiding medical care during the pandemic. In contrast, employed adults were more likely to delay or avoid medical care. In rural areas, current smokers were more likely to delay or avoid medical care during the pandemic.
Conclusion: This study has identified several factors affecting medical care delay or avoidance, some of which are amenable to policy changes. Policymakers can help improve the utilization of health facilities and patient health outcomes by implementing a series of reforms.
Keywords: delay or avoidance behavior, medical care, COVID-19 pandemic, China
Introduction
People often delay or avoid medical visits even when they suspect they should go.1 36.0% of American adults, 10.9% of French adults, and 40.4% of Chinese breast cancer patients delayed or avoided doctor visits they had deemed necessary before the coronavirus disease 2019 (COVID-19) pandemic.2–4 During the COVID-19 pandemic, COVID-19-related factors such as stay-at-home orders, physical distancing measures, and fears of COVID-19 within hospitals have prompted people to delay or avoid seeking medical care.5,6 Figure 1 shows the proportion of medical care delay or avoidance before and during the COVID-19 pandemic in China. Medical care delay or avoidance has been observed to increase during pandemics. Nevertheless, the factors that may influence medical care delay or avoidance among Chinese adults during the COVID-19 pandemic are not well understood.
 |
Figure 1 Medical care delay or avoidance according to the severity of self-reported physical symptoms before and during the COVID-19 pandemic. Note: Data were from the 2018 and 2020 China Family Panel Studies.7 |
At the individual level, medical care delay or avoidance may increase morbidity and mortality risk associated with underlying, preventable, and treatable medical conditions and contribute to excess mortality, including deaths related to COVID-19 directly or indirectly.8,9 In addition, medical care delay or avoidance can extend hospital stays, use more medications, and visit high-frequency emergency departments, and may generate higher medical expenditures in the long run.2,10,11 At the societal level, medical care delay or avoidance is costly for the national healthcare system.12
Medical care avoidance is defined as the act of keeping away from medical care that is thought to cause mental or physical distress.1,13 Medical care delay is often combined with avoidance, which incorporates a temporal element (postponing medical care until a later time) into the definition of medical care avoidance.13 Medical care delay or avoidance can also occur due to barriers, including financial limitations, time constraints, and lack of access to a medical care provider.1,13,14 Delay or avoidance of medical care can occur at any point using preventive healthcare, treatment seeking, and treatment adherence.1,13 A review of the literature implies that many factors affect medical care delay or avoidance, including the following three categories of variables: individual-level socioeconomic status and demographic characteristics, personal barriers, and institution-related care avoidance factors.
Individual-level socioeconomic status and demographic characteristics affecting medical care delay or avoidance include age, gender, educational attainment, employment status, income level, and health insurance status. The findings are mixed on how age, gender, and educational attainment affect medical care delay or avoidance. For example, Sulku et al, Reisinger et al, and Splinter et al found that the probability of delaying or avoiding medical care increases as age increases.15–17 However, Kannan et al, Ratnapradipa et al, and Spleen et al reported the opposite.2,11,18 Reisinger et al and Spleen et al found that men are more likely to delay or avoid medical care.16,18 These two population-based cross-sectional studies were conducted in the USA. In contrast, Sulku et al, Splinter et al, and Karim et al reported that women are more likely to delay or avoid medical care.15,17,19 These three population-based cross-sectional studies were conducted in Turkey, the Netherlands, and Bangladesh. Hwang et al, Farina and Ailshire, and Zhong et al showed that higher educational attainment is positively associated with medical care delay or avoidance.20–22 However, Splinter et al and Needham et al found that lower educational attainment is more likely to be associated with medical care delay or avoidance.17,23
The effects of income level, health insurance status, and employment status on medical care delay or avoidance were found to be similar across several studies. Ratnapradipa et al, Jatrana and Crampton, and Vilhjalmsson found that lower income is positively associated with medical care delay or avoidance.11,24,25 Gertz et al, Reisinger et al, Wisk and Witt, and Mollborn et al reported that individuals without health insurance are more likely to delay or avoid medical care.9,16,26,27 Reisinger et al and Pharr et al found that unemployed or retired people are less likely to delay or avoid medical care.16,28
Personal barriers associated with medical care delay or avoidance include emotions (anxiety, fear, denial, worry), attitude, financial or resource limitations, health beliefs, lack of knowledge, lack of support, language barriers, perception of risk, transportation, stigma or embarrassment of illness, and time constraints.13 For example, Hwang et al reported that higher levels of fear of COVID-19 show increased odds of delaying or avoiding medical care.20 Wisk and Witt found that people with high family financial burdens are more likely to delay or avoid medical care.26 Kannan and Veazie showed that low health self-efficacy is positively associated with medical care delay or avoidance.2 Tipirneni et al found that higher health insurance literacy is associated with a lower likelihood of delaying or avoiding medical care.29 Reisinger et al reported that people without social support are more likely to delay or avoid medical care.16 Sulku et al found that people who feel severe pain are less likely to delay or avoid medical care.15 During the COVID-19, social distancing and lockdowns turned many patients to online forums, where various forms of lay expertise were mobilized to cope with disease and illness,30 pushing some patients away from credentialed experts.
Institution-related care avoidance factors are found to be associated with medical care delay or avoidance, including attitude and knowledge of the provider, distrust of providers, lack of access to a provider, and lack of user-friendly service hours. For example, Kannan and Veazie reported that fear or dislike of medical treatment and time is positively associated with medical care delay or avoidance.2 Spleen et al found that rural residents who reported lower levels of trust in physicians are more likely to delay or avoid medical care.18 Lack of trust in medical professionals brought on by the dismissal of experiences of those suffering from the complications of COVID-19 or Long COVID,31 as well as instances of bribery of medical professionals by patients.32,33 Arnetz et al showed that a negative patient healthcare experience had a higher probability of delaying or avoiding medical care.34
Since the launch of the new health reform of 2009, the Chinese government has made considerable investments to strengthen the provision of primary care and extend healthcare coverage. However, people continue to delay or avoid medical care. Delay or avoidance behavior and factors affecting medical care delay or avoidance have implications for government policies related to types of investments that will be most effective in improving the utilization of health facilities and patient health outcomes. However, little is known about delay or avoidance behavior during emergency situations in China, and this study is an attempt to understand delay or avoidance behavior in rural and urban areas of China and to identify factors associated with medical care delay or avoidance among Chinese adults during the COVID-19 pandemic.
Methods and Materials
Theoretical Model
The current study employed the Behavioral Model of Health Services Use (BMHSU), initially developed by Andersen.35 In the BMHSU model, the individual’s use of health services (delay or avoidance of health services) is a function of his or her predisposition characteristics to use healthcare, enable or impede use, and his or her need for health services. Figure 2 presents the theoretical model of this study. Each part of the model can be an independent contribution to delaying or avoiding medical care. More importantly, the model presents an explanatory process or causal ordering.31 Predisposing characteristics can be measured by socio-economic and demographic characteristics. Demographic factors suggest the probability that an individual needs medical care, and socio-economic characteristics express an individual’s ability to deal with presenting problems. Therefore, Predisposing characteristics can influence an individual’s subsequent perceptions of need and delay or avoidance of medical care. Enabling resources emphasize the resources available to an individual for using medical care. Perceived need refers to an individual’s own judgment about his or her health status and need for medical care, and evaluated need means health personnel’s judgment, which directly influences an individual’s delay or avoidance of medical care.35,36
 |
Figure 2 The theoretical model of this study. |
Participants
The database used in this study was obtained from the 2020 China Family Panel Studies (CFPS) conducted from July to December 2020 during the COVID-19 pandemic. The CFPS is a general-purpose, nationally representative, longitudinal survey conducted by the Institute of Social Science Survey of Peking University. The survey sample was drawn from twenty-five provinces and their administrative equivalents; thus, it represents 95% of the total population in mainland China. A multistage probability proportional to size (PPS) sampling method was used for the survey. More details about the sampling design are available from Xie and Lu.37 The CFPS used multi-module designs for questionnaires, including household information, family income, family assets, demographic background, educational history, schooling, language use, marriage, subjective measurements, health status and physical functioning, mental health, work, retirement, and pension, etc.38
Due to the COVID-19 pandemic, the CFPS primarily conducted telephone interviews, and 89% of respondents were interviewed by telephone.39 The CFPS respondents are reinterviewed every two years, with the first wave occurring in 2010. The 2020 CFPS had a total sample of 28,530 individuals. From the full sample, only the adults (16 years old or older) who reported feeling any physical discomfort in the past two weeks prior to the survey interview were selected (5830 adults). Figure 1 shows the proportion of medical care delay or avoidance according to the severity of self-reported physical symptoms during the COVID-19 pandemic. The proportion of medical care delay or avoidance was as high as 51.5% among adults with mild physical symptoms. Adults with mild physical symptoms reported low perceived need to seek medical care, often because they expected their illness or symptoms to improve over time.1 Most of them choose self-treatment or no treatment at all. Therefore, this study excluded adults with the severity of self-reported physical symptoms as mild (1260 adults). After all missing data were eliminated (201 adults), the final sample consisted of 4369 adults.
Measures
Dependent Variable
Medical care delay or avoidance was set as a binary variable, indicating the decision to avoid visiting a doctor (or not) among the adults who reported moderate or serious physical symptoms in the past two weeks. The CFPS question that represents this variable is: “Have you seen a doctor within the past two weeks?”. Response options are yes or no. If the adult reported “no”, the respondent was categorized as delaying or avoiding medical care.
Independent Variables
General trust in physicians:
In the CFPS, each adult was asked, “Considering everything together, how much do you trust physicians in China? Please answer by picking a number between 0 and 10, where 0 stands for not at all and 10 for completely” (An 11-point Likert scale). For the analysis, we have categorized reported levels of general trust in physicians into three groups: low level of trust (0–3), medium level of trust (4–6), and high level of trust (7–10).
Perceived quality of care:
The present study measured the perceived quality of care from provider competence and structural quality. Provider competence was set as a dummy variable equaling one if the adults answered “very good” and 0 otherwise. The question in the CFPS that collected information on provider competence is: “How would you evaluate the knowledge, expertise, skills, and abilities of the health care provider that you visit most often?”. Provider structural quality was also set as a dummy variable that equaled one if the adults who answered “very satisfied” and 0 otherwise, based on a question that asks: “Are you satisfied with the condition of the health care facility that you visit most often (such as the adequacy of facilities, equipment, staff, and drug, qualifications of physicians and nurses, administrative structures, and convenient transportation)?”.
The analysis also considered the following three categories of variables to explain medical care delay or avoidance. (1) Predisposing factors: gender, age, educational attainment, marital status, employment status, place of residence, and locations of respondents. (2) Enabling factors: insurance status, household income, family size, and GDP. (3) Need factors: in addition to general trust in physicians, provider competence, and provider structural quality, other need factors included in the analysis were self-rated health, chronic conditions, current smoking, regular drinking, and patient experience (a proxy indicator for primary care visits). The definitions of the variables are provided in Table 1.
 |
Table 1 Definitions of Variables Used in the Empirical Analysis of Avoiding Medical Visits (2020 China Family Panel Study) |
Statistical Analysis
Bivariate analyses were used to examine differences between adults who consulted a doctor (seeking health care) and those who did not consult a doctor (medical care delay or avoidance) when they felt physical discomfort during the COVID-19 pandemic. Statistical significance between groups was assessed through Pearson’s chi-square test for categorical variables and two-sample t-tests for continuous variables.
This study used a logistic regression model to identify factors associated with medical care delay or avoidance. This model is based on a latent regression and is defined as follows:

where x' is a vector of independent variables, including predisposing, enabling, and need factors; β is the coefficient vector; and y* is an unobserved latent variable linked to the observed dichotomous response of medical care delay or avoidance (MCDA). We assume that ε has mean zero and has a standardized logistic with variance  . Our observation is
. Our observation is


where  indicates that the individual delay or avoid medical care.
indicates that the individual delay or avoid medical care.





The logistic regression model was estimated using maximum likelihood estimation.40 Since the health care delivery and health insurance systems differ between urban and rural areas, the logistic regression model was used to analyze factors affecting medical care delay or avoidance stratified by urban-rural residence, which should help avoid potential bias created by differences between urban and rural health systems. The results are presented as odds ratios (ORs) and 95% confidence intervals (CIs). All statistical analyses were conducted employing Stata Version 17 (Stata Corp, College Station, TX).
Results
General Characteristics of Subjects
Table 1 shows the characteristics of the study sample. The sample size was 4369, with 41.79% of adults being male and 51.41% completing at least a middle school education. The average age of adults was approximately 52 years. Among those who reported moderate or serious physical symptoms, the proportion of medical care delay or avoidance was 31.84%. About 59% of adults reported a high level of trust in physicians. The proportion of adults who reported provider competence being very good was 14.05%. Approximately 10% of adults reported satisfaction with provider structural quality in 2020.
Bivariate Analyses of Medical Care Delay or Avoidance
Table 2 reports predisposing, enabling, and need factors by medical care delay or avoidance. The descriptive analysis implies that gender, primary care, and provider competence did not significantly relate to medical care delay or avoidance. Other variables, however, are related to medical care delay or avoidance as a group. These include age, educational attainment, marital status, medical insurance coverage, family size, place of residence, household income, employment status, self-rated health status, chronic conditions, current smoking, regular drinking, general trust in physicians, provider structural quality, locations of respondents, and GDP.
 |
Table 2 Differences Between Avoiding Medical Visits and Non- Avoiding Medical Visits According to Predisposing, Enabling, and Need Characteristics |
Logistic Regression Analysis on Medical Care Delay or Avoidance
The results of the logistic regression are reported in Table 3. The results imply that the probability of delaying or avoiding medical care decreased as age increased, although the odds ratio is close to 1 (OR=0.99, 95% CI: 0.99–1.00). Higher educational attainment had a positive association with medical care delay or avoidance. For example, compared to illiterate or semi-literate adults, adults who graduated from middle school were more likely to delay or avoid medical care (OR=1.31, 95% CI: 1.06–1.61). High school completion showed an increased probability of delaying or avoiding medical care compared to those who were illiterate or semi-literate (OR=1.30, 95% CI: 1.00–1.68). Compared to illiterate or semi-literate adults, completing more than three years of college showed increased odds of delaying or avoiding medical care (OR=1.72, 95% CI: 1.28–2.31). Family size was negatively associated with medical care delay or avoidance (OR=0.96, 95% CI: 0.92–0.99). Urban residents reported a higher likelihood of delaying or avoiding medical care compared to rural residents (OR=1.25, 95% CI: 1.09–1.45). Employed adults showed a higher likelihood of delaying or avoiding medical care (OR=1.18, 95% CI: 1.01–1.38). Adults with chronic conditions were less likely to delay or avoid medical care (OR=0.37, 95% CI: 0.31–0.43). Adults who reported higher levels of trust in physicians were less likely to delay or avoid medical care (OR=0.71, 95% CI: 0.55–0.90; OR=0.71, 95% CI: 0.56–0.89). Adults who lived in the east, central, and west regions show decreased odds of delaying or avoiding medical care compared to those who lived in the northeast region (OR=0.59, 95% CI: 0.46–0.76; OR=0.47, 95% CI: 0.37–0.61; OR=0.46, 95% CI: 0.36–0.57).
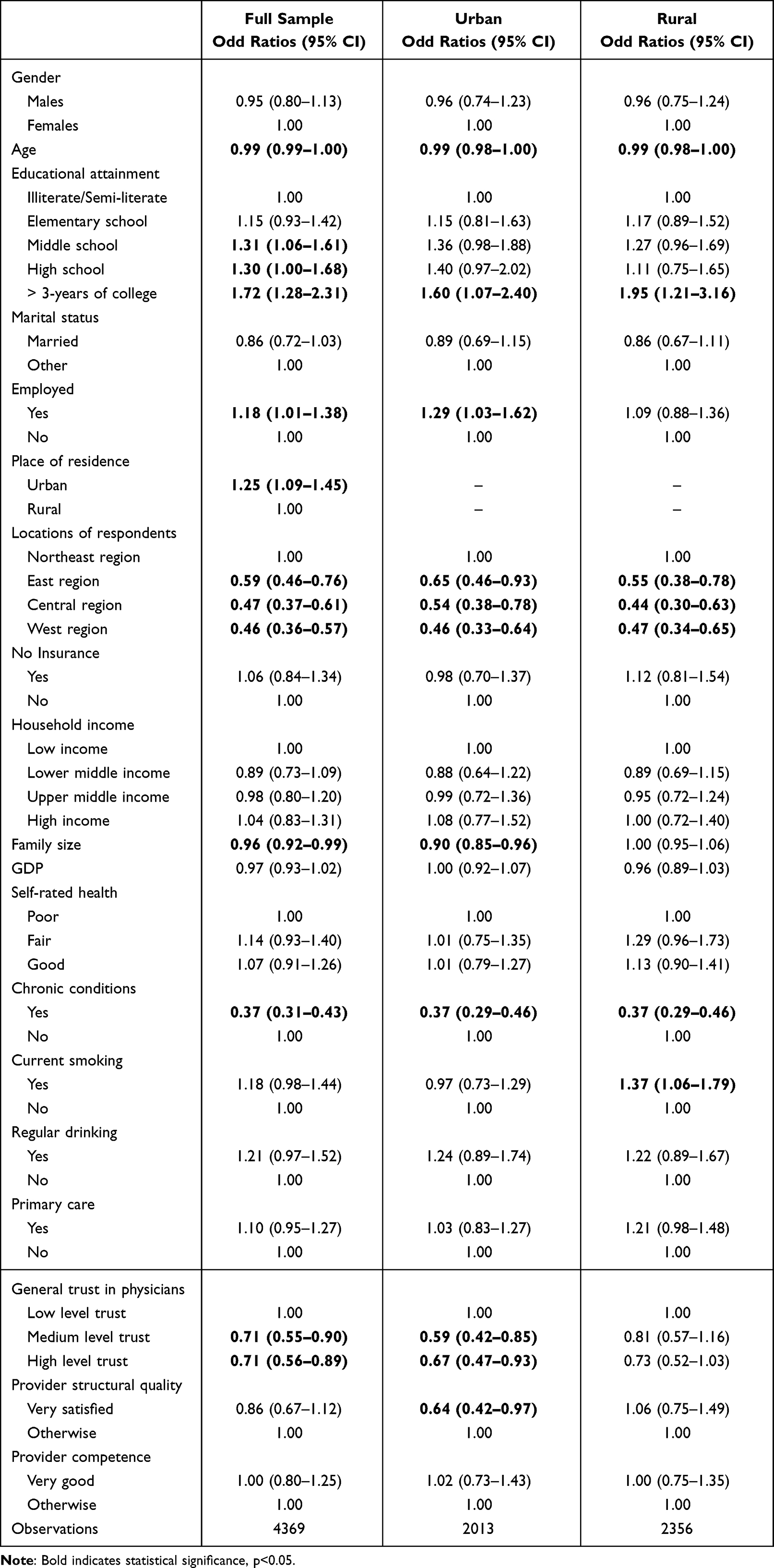 |
Table 3 Logistic Regression Analysis on Avoiding Medical Visits |
Regardless of rural-urban residence, the probability of delaying or avoiding medical care decreased with age increased (OR=0.99, 95% CI: 0.98–1.00). Compared to illiterate or semi-literate adults, completion of more than three years of college showed increased odds of delaying or avoiding medical care in both rural and urban areas (OR=1.60, 95% CI: 1.07–2.40; OR=1.95, 95% CI: 1.21–3.16). Adults with chronic conditions showed a lower probability of delaying or avoiding medical care in both rural and urban areas (OR=0.37, 95% CI: 0.29–0.46; OR=0.37, 95% CI: 0.29–0.46). In both rural and urban areas, adults who lived in the east, central, and west regions were less likely to delay or avoid medical care compared to those who lived in the northeast region.
In urban areas, larger family sizes decreased the probability of delaying or avoiding medical care (OR=0.90, 95% CI: 0.85–0.96). Employed adults were more likely to delay or avoid medical care in urban areas (OR=1.29, 95% CI: 1.03–1.62). Urban adults who reported higher levels of trust in physicians had a lower probability of delaying or avoiding medical care (OR=0.59, 95% CI: 0.42–0.85; OR=0.67, 95% CI: 0.47–0.93). Urban adults who reported being very satisfied with the provider structural quality were less likely to delay or avoid medical care (OR=0.64, 95% CI: 0.42–0.97). In rural areas, adults who currently smoke tobacco products reported increased odds of delaying or avoiding medical care (OR=1.37, 95% CI: 1.06–1.79).
Discussion
The present study examined the factors associated with medical care delay or avoidance among Chinese adults during the COVID-19 pandemic. The results indicate that approximately 32% of Chinese adults delay or avoid medical care during the pandemic. Our finding is consistent with research conducted during the pandemic from both Australia (32.9%) and Hong Kong SAR (30.4%).41,42 There are some countries, however, where medical care delay or avoidance is relatively high (the USA (40.9%) and Portugal (44.0%)) or low (the Netherlands (20.2%) and South Korea (4.0%)).8,17,20,43 The delay or avoidance behavior in different countries may have been affected by varying access to medical care, health insurance coverage, health system performance, and various individual-level predisposing, enabling, and need characteristics. Since medical care delay or avoidance may increase morbidity and mortality risk and generate higher medical expenditures in the long run, addressing the medical care delay or avoidance issue should significantly impact individuals’ health outcomes and health system efficiency. Therefore, identifying the factors associated with delaying or avoiding medical care will help policymakers gain a deeper understanding of the issue of medical care delay or avoidance.
Regardless of rural-urban residence, the probability of delaying or avoiding medical care decreased with age increased during the COVID-19 pandemic. The result is consistent with other findings in the literature.2,11,18 The Grossman model emphasizes that people inherit an initial health stock that depreciates with age and can be increased by investment.44 Older adults who often have complex medical needs belong to a particularly vulnerable and high-risk population.22 The complex medical needs of older adults make them particularly vulnerable and high-risk to the negative health consequences of medical care delay or avoidance.45 Therefore, older adults seek medical care services more promptly than their younger counterparts when uncertain about their physical symptoms’ severity.46 We found that adults with chronic conditions were less likely to delay or avoid medical care during the COVID-19 pandemic. People with chronic conditions are similar to older adults and have complex care needs, especially those with multiple chronic conditions.47 We also found that completing more than three years of college showed increased odds of delaying or avoiding medical care during the COVID-19 pandemic. This finding is in line with previous research.20–22 Educational attainment is an indicator of socioeconomic status (SES), and higher SES may also be associated with better knowledge about the relative quality of services offered through primary and upper levels facilities. Patients with better educational status in China prefer tertiary hospitals that represent the most advanced level of service provided in China.48 However, long waiting times for registration to see a doctor is problematic in tertiary hospitals.49 Moreover, the amount of outpatient registration per day has been reduced to mitigate the risk of COVID-19 spread, which leads to a longer wait time.50
In both rural and urban areas, adults who lived in the east, central, and west regions were less likely to delay or avoid medical care compared to those who lived in the northeast region. The medical care delay or avoidance across regions may have been influenced by variations in primary healthcare center (PHC) accessibility. For example, northeastern provinces show more inequalities in PHC accessibility, while less inequalities in southwestern and south-central provinces.51 We found that urban residents reported a higher likelihood of delaying or avoiding medical care compared to rural residents. Rural residents often rely on primary care facilities in the area due to the difficulty of accessing alternative healthcare providers. Because of the “one village, one village clinic” principle in China, most village clinic doctors and villagers live in the social environment of acquaintances in the same village.52 Frequent contact and long-term relationships decrease the probability of delaying or avoiding medical care.53 In addition, urban residents are less likely to trust physicians compared to rural residents, which may hinder access to medical care.54 In rural areas, current smokers were more likely to delay or avoid medical care during the COVID-19 pandemic. Current smokers are more risk tolerant and may more willingly bear disease risk. A higher willingness to bear risk increases the probability of delaying or avoiding medical care.55
In urban areas, larger family sizes decreased the probability of delaying or avoiding medical care. The bigger family sizes increase the likelihood that patients receive support from their family members. Family support plays an essential protective role in delaying or avoiding medical care.56 Employed adults were more likely to delay or avoid medical care in urban areas. Additional paid sick leave or additional benefits during the COVID-19 pandemic is not universally available to Chinese employees. Those without paid sick leave are more likely to delay or avoid medical care.57 Moreover, time constraints may delay employed adults from seeking medical care services.1 Urban adults who reported higher levels of trust in physicians had a lower probability of delaying or avoiding medical care. High general trust in physicians is associated with effective physician-patient communication, higher patient satisfaction, and good continuity of care.27 Moreover, patient experiences with past visits to healthcare providers are the proximate causes of trust in physicians.54 Those factors are associated with a decreased probability of delaying or avoiding medical care. Urban adults who reported being very satisfied with the provider structural quality were less likely to delay or avoid medical care. This result is not unexpected - high provider structural quality is associated with lower organizational barriers such as adequacy of facilities, qualifications of physicians, and convenient transportation.
Policymakers can help improve the utilization of health facilities and patient health outcomes by implementing a series of reforms. This study has identified several factors affecting medical care delay or avoidance, some of which are amenable to policy changes. First, more providers and resources should be offered to meet the vulnerable and high-risk population’s needs for medical care services. Second, the Chinese government may consider improving the quality of primary care and referral systems in community health centers to attract educated people. Third, primary care should deliver screening programs to rural smokers. Fourth, night and holiday medical care services should be provided to employed persons. Last, the Chinese government should focus on the physician-patient relationship performance and improve general trust in physicians.
Limitations
Even though the present study employed a national survey to analyze factors affecting delay or avoidance behavior among Chinese adults during the COVID-19 pandemic, several limitations should be mentioned. First, this was a cross-sectional study based on the 2020 CFPS. It has limitations in proving causality that could use longitudinal study designs. Second, medical care delay or avoidance is a single-item self-report medical care utilization question, and there are no follow-up questions to understand the reasons of medical care delay or avoidance. Third, limitations of all self-reported data exist, such as recall bias and unreliability of responses under pressure. Last, the current study excluded adults with the severity of self-reported physical symptoms as mild and only concerned with severe cases and emergency situations. Further studies should be performed to extend a general model of all patients.
Conclusion
This study aimed to identify factors associated with medical care delay or avoidance among Chinese adults during the COVID-19 pandemic. The results indicate that approximately 32% of Chinese adults delay or avoid medical care during the COVID-19 pandemic. Moreover, urban residents reported a higher likelihood of delaying or avoiding medical care than rural residents. The empirical findings suggested that regardless of rural-urban residence, older adults and adults with chronic conditions were less likely to delay or avoid medical care during the pandemic. However, completing more than three years of college showed increased odds of delaying or avoiding medical care. In urban areas, larger family sizes, high general trust in physicians, and high provider structural quality decreased the probability of delaying or avoiding medical care during the pandemic. In contrast, employed adults were more likely to delay or avoid medical care. In rural areas, current smokers were more likely to delay or avoid medical care during the pandemic. These results can be used to design policy reforms to improve the utilization of health facilities and patient health outcomes.
Ethics Approval
Ethical approval was issued by the Peking University Biomedical Ethics Review Committee (IRB00001052-14010), and all respondents signed an informed consent form before the study was initiated. The study was conducted in accordance with the regulations and ethics followed in compliance with the Declaration of Helsinki.
Funding
This research was funded by the Inner Mongolia Autonomous Region Natural Science Fund (2022MS07001).
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Taber JM, Leyva B, Persoskie A. Why do people avoid medical care? A qualitative study using national data. J Gen Intern Med. 2015;30(3):290–297. doi:10.1007/s11606-014-3089-1
2. Kannan VD, Veazie PJ. Predictors of avoiding medical care and reasons for avoidance behavior. Med Care. 2014;52(4):336–345. doi:10.1097/MLR.0000000000000100
3. Rivenbark JG, Ichou M. Discrimination in healthcare as a barrier to care: experiences of socially disadvantaged populations in France from a nationally representative survey. BMC Public Health. 2020;20(1):31. doi:10.1186/s12889-019-8124-z
4. Li YL, Qin YC, Tang LY, et al. Patient and care delays of breast cancer in China. Cancer Res Treat. 2019;51(3):1098–1106. doi:10.4143/crt.2018.386
5. Xiao H, Dai X, Wagenaar BH, et al. The impact of the COVID-19 pandemic on health services utilization in China: time-series analyses for 2016–2020. Lancet Reg Health West Pac. 2021;2021(9):100122. doi:10.1016/j.lanwpc.2021.100122
6. Yang Y, Le KJ, Liang C, et al. Changes in inpatient admissions before and during COVID-19 outbreak in a large tertiary hospital in Shanghai. Ann Transl Med. 2022;10(8):469. doi:10.21037/atm-22-1594
7. Peking University Open Research Data Platform. China family panel Studies(CFPS). Available from: https://opendata.pku.edu.cn/dataverse/CFPS;jsessionid=aa6862c1c0a7aedce5d017ef9913.
8. Czeisler MÉ, Marynak K, Clarke KEN, et al. Delay or avoidance of medical care because of COVID-19-related concerns - United States. MMWR Morb Mortal Wkly Rep. 2020;69(36):1250–1257. doi:10.15585/mmwr.mm6936a4
9. Gertz AH, Pollack CC, Schultheiss MD, Brownstein JS. Delayed medical care and underlying health in the United States during the COVID-19 pandemic: a cross-sectional study. Prev Med Rep. 2022;28:101882. doi:10.1016/j.pmedr.2022.101882
10. Kraft AD, Quimbo SA, Solon O, Shimkhada R, Florentino J, Peabody JW. The health and cost impact of care delay and the experimental impact of insurance on reducing delays. J Pediatr. 2009;155(2):281–5.e1. doi:10.1016/j.jpeds.2009.02.035
11. Ratnapradipa KL, Jadhav S, Kabayundo J, Wang H, Smith LC. Factors associated with delaying medical care: cross-sectional study of Nebraska adults. BMC Health Serv Res. 2023;23(1):118. doi:10.1186/s12913-023-09140-0
12. Jaffee KD, Shires DA, Stroumsa D. Discrimination and delayed health care among transgender women and men: implications for improving medical education and health care delivery. Med Care. 2016;54(11):1010–1016. doi:10.1097/MLR.0000000000000583
13. Byrne SK. Healthcare avoidance: a critical review. Holist Nurs Pract. 2008;22(5):280–292. doi:10.1097/01.HNP.0000334921.31433.c6
14. Islam MI, Freeman J, Chadwick V, Martiniuk A. Healthcare avoidance before and during the COVID-19 pandemic among Australian youth: a longitudinal study. Healthcare. 2022;10(7):1261. doi:10.3390/healthcare10071261
15. Sulku SN, Tokatlioglu Y, Cosar K. Determinants of health care avoidance and avoidance reasons in Turkey. J Public Health. 2023;31(5):817–829. doi:10.1007/s10389-021-01577-z
16. Reisinger MW, Moss M, Clark BJ. Is lack of social support associated with a delay in seeking medical care? A cross-sectional study of Minnesota and Tennessee residents using data from the behavioral risk factor surveillance system. BMJ Open. 2018;8(7):e018139. doi:10.1136/bmjopen-2017-018139
17. Splinter MJ, Velek P, Ikram MK, et al. Prevalence and determinants of healthcare avoidance during the COVID-19 pandemic: a population-based cross-sectional study. PLoS Med. 2021;18(11):e1003854. doi:10.1371/journal.pmed.1003854
18. Spleen AM, Lengerich EJ, Camacho FT, Vanderpool RC. Health care avoidance among rural populations: results from a nationally representative survey. J Rural Health. 2014;30(1):79–88. doi:10.1111/jrh.12032
19. Karim F, Islam MA, Chowdhury AM, Johansson E, Diwan VK. Gender differences in delays in diagnosis and treatment of tuberculosis. Health Policy Plan. 2007;22(5):329–334. doi:10.1093/heapol/czm026
20. Hwang J, Kim WH, Heo J. An association between individual’s risk perceptions and delayed or foregone healthcare services during the COVID-19 pandemic in Korea. BMC Health Serv Res. 2023;23(1):850. doi:10.1186/s12913-023-09807-8
21. Farina MP, Ailshire JA. Sociodemographic and health status differences in delaying medical care during the COVID-19 pandemic among older adults: findings from the health and retirement study. BMC Public Health. 2022;22(1):1720. doi:10.1186/s12889-022-14118-4
22. Zhong S, Huisingh-Scheetz M, Huang ES. Delayed medical care and its perceived health impact among US older adults during the COVID-19 pandemic. J Am Geriatr Soc. 2022;70(6):1620–1628. doi:10.1111/jgs.17805
23. Needham DM, Foster SD, Tomlinson G, Godfrey-Faussett P. Socio-economic, gender and health services factors affecting diagnostic delay for tuberculosis patients in urban Zambia. Trop Med Int Health. 2001;6(4):256–259. doi:10.1046/j.1365-3156.2001.00709
24. Jatrana S, Crampton P. Primary health care in New Zealand: who has access? Health Policy. 2009;93(1):1–10. doi:10.1016/j.healthpol.2009.05.006
25. Vilhjalmsson R. Family income and insufficient medical care: a prospective study of alternative explanations. Scand J Public Health. 2021;49(8):875–883. doi:10.1177/1403494820944096
26. Wisk LE, Witt WP. Predictors of delayed or forgone needed health care for families with children. Pediatrics. 2012;130(6):1027–1037. doi:10.1542/peds.2012-0668
27. Mollborn S, Stepanikova I, Cook KS. Delayed care and unmet needs among health care system users: when does fiduciary trust in a physician matter? Health Serv Res. 2005;40(6):1898–1917. doi:10.1111/j.1475-6773.2005.00457.x
28. Pharr JR, Moonie S, Bungum TJ. The impact of unemployment on mental and physical health, access to health care and health risk behaviors. Int Sch Res. 2012;2012:483432. doi:10.5402/2012/483432
29. Tipirneni R, Politi MC, Kullgren JT, Kieffer EC, Goold SD, Scherer AM. Association between health insurance literacy and avoidance of health care services owing to cost. JAMA Netw Open. 2018;1(7):e184796. doi:10.1001/jamanetworkopen.2018.4796
30. Au L, Eyal G. Whose advice is credible? Claiming lay expertise in a Covid-19 online community. Qual Sociol. 2022;45(1):31–61. doi:10.1007/s11133-021-09492-1
31. Au L, Capotescu C, Eyal G, Finestone G. Long covid and medical gaslighting: dismissal, delayed diagnosis, and deferred treatment. SSM Qual Res Health. 2022;2:100167. doi:10.1016/j.ssmqr.2022.100167
32. Sc CC, Yao Z. A market of distrust: toward a cultural sociology of unofficial exchanges between patients and doctors in China. Theor Soc. 2018;47(6):737–772. doi:10.1007/s11186-018-09332-2
33. Guo W, Xu B. Dignity in red envelopes: disreputable exchange and cultural reproduction of inequality in informal medical payment. Soc Psychol Q. 2022;85(1):23–43. doi:10.1177/01902725211044815
34. Arnetz BB, Goetz C, vanSchagen J, Baer W, Smith S, Arnetz JE. Patient-reported factors associated with avoidance of in-person care during the COVID-19 pandemic: results from a national survey. PLoS One. 2022;17(8):e0272609. doi:10.1371/journal.pone.0272609
35. Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav. 1995;36(1):1–10. doi:10.2307/2137284
36. Babitsch B, Gohl D, von Lengerke T. Re-revisiting andersen’s behavioral model of health services use: a systematic review of studies from 1998–2011. Psychosoc Med. 2012;9:11. doi:10.3205/psm000089
37. Xie Y, Lu P. The sampling design of the China family panel studies (CFPS). Chin J Sociol. 2015;1(4):471–484. doi:10.1177/2057150X15614535
38. Xie Y, Hu JW. An Introduction to the China Family Panel Studies (CFPS). Chin Sociol Rev. 2014;47:3–29. doi:10.2753/CSA2162-0555470101
39. Institute of Social Science Survey of Peking University. Progress report of CFPS 2020. Available from: https://www.isss.pku.edu.cn/cfps/en/news/news1/1355152.htm.
40. Greene WH. Econometric Analysis. Pearson Education India; 2003.
41. Czeisler MÉ, Kennedy JL, Wiley JF, et al. Delay or avoidance of routine, urgent and emergency medical care due to concerns about COVID-19 in a region with low COVID-19 prevalence: Victoria, Australia. Respirology. 2021;26(7):707–712. doi:10.1111/resp.14094
42. Hung KK, Walline JH, Chan EYY, et al. Health Service Utilization in Hong Kong During the COVID-19 Pandemic - A cross-sectional public survey. Int J Health Policy Manag. 2022;11(4):508–513. doi:10.34172/ijhpm.2020.183
43. Soares P, Leite A, Esteves S, et al. Factors associated with the patient’s decision to avoid healthcare during the COVID-19 pandemic. Int J Environ Res Public Health. 2021;18(24):13239. doi:10.3390/ijerph182413239
44. Grossman M. On the concept of health capital and the demand for health. J Polit Econ. 1972;80(2):223–255. doi:10.1086/259880
45. Leyva B, Taber JM, Trivedi AN. Medical care avoidance among older adults. J Appl Gerontol. 2020;39(1):74–85. doi:10.1177/0733464817747415
46. Ryan CJ, Zerwic JJ. Perceptions of symptoms of myocardial infarction related to health care seeking behaviors in the elderly. J Cardiovasc Nurs. 2003;18(3):184–196. doi:10.1097/00005082-200307000-00004
47. Peters VJT, Meijboom BR, Bunt JEH, et al. Providing person-centered care for patients with complex healthcare needs: a qualitative study. PLoS One. 2020;15(11):e0242418. doi:10.1371/journal.pone.0242418
48. Li C, Chen Z, Khan MM. Bypassing primary care facilities: health-seeking behavior of middle age and older adults in China. BMC Health Serv Res. 2021;21(1):895. doi:10.1186/s12913-021-06908-0
49. Cao W, Wan Y, Tu H, et al. A web-based appointment system to reduce waiting for outpatients: a retrospective study. BMC Health Serv Res. 2011;11(1):318. doi:10.1186/1472-6963-11-318
50. Chen X, Deng W, Zhou W, et al. Understanding the experiences of patients with cancers in hospitals during COVID-19 pandemic in China: a qualitative research study. Nurs Open. 2022;9(1):358–366. doi:10.1002/nop2.1073
51. Jia P, Wang Y, Yang M, et al. Inequalities of spatial primary healthcare accessibility in China. Soc Sci Med. 2022;314:115458. doi:10.1016/j.socscimed.2022.115458
52. Liu J, Yin H, Zheng T, et al. Primary health institutions preference by hypertensive patients: effect of distance, trust and quality of management in the rural Heilongjiang province of China. BMC Health Serv Res. 2019;19(1):852. doi:10.1186/s12913-019-4465-7
53. Green CA, Johnson KM, Yarborough BJ. Seeking, delaying, and avoiding routine health care services: patient perspectives. Am J Health Promot. 2014;28(5):286–293. doi:10.4278/ajhp.120702-QUAL-318
54. Li C, Khan MM. Public trust in physicians: empirical analysis of patient-related factors affecting trust in physicians in China. BMC Prim Care. 2022;23(1):217. doi:10.1186/s12875-022-01832-6
55. Li C, Sun J. The impact of current smoking, regular drinking, and physical inactivity on health care-seeking behavior in China. BMC Health Serv Res. 2022;22(1):52. doi:10.1186/s12913-022-07462-z
56. Montagni I, Langlois E, Koman J, Petropoulos M, Tzourio C. Avoidance and delay of medical care in the young: an interdisciplinary mixed-methods study. Young. 2018;26(5):505–524. doi:10.1177/1103308817734474
57. DeRigne L, Stoddard-Dare P, Quinn L. Workers without paid sick leave less likely to take time off for illness or injury compared to those with paid sick leave. Health Affairs. 2016;35(3):520–527. doi:10.1377/hlthaff.2015.0965
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.