Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Predictors of Complication Risk Perception and Impact on Self-Management Behavior in Young and Middle-Aged Patients with Type 2 Diabetes: A Latent Profile Analysis
Received 3 October 2025
Accepted for publication 18 November 2025
Published 2 December 2025 Volume 2025:18 Pages 4399—4410
DOI https://doi.org/10.2147/DMSO.S570673
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ernesto Maddaloni
Yuting Zhang,1 Xueqin Jin2
1School of Medicine, Jiangsu University, Zhenjiang, Jiangsu Province, People’s Republic of China; 2Department of Nursing, Kunshan Hospital Affiliated to Jiangsu University, Suzhou, Jiangsu Province, People’s Republic of China
Correspondence: Xueqin Jin, Department of Nursing, Kunshan Hospital Affiliated to Jiangsu University, Suzhou, Jiangsu Province, People’s Republic of China, Email [email protected]
Aim: To explore latent categories of complication risk perception in young and middle-aged patients with T2DM, and to examine their relationship with self-management behavior.
Methods: A cross-sectional study was conducted between September 2024 and March 2025, involving 316 young and middle-aged patients with type 2 diabetes mellitus from the endocrinology department of a tertiary hospital in Jiangsu Province, China. Data were collected via a general information questionnaire, the Diabetes Risk Perception Scale, and the Diabetes Self-Management Behavior Scale. Latent profile analysis identified distinct complication risk perception groups, while logistic regression was performed to identify factors influencing different categories. Self-management Behavior scores were compared across subgroups.
Results: Complication risk perception in young and middle-aged patients with T2DM was divided into three latent categories: the Low Risk Perception-Optimism Bias Group (43.7%, n=138), the Overall Medium Risk Perception Group (42.1%, n=133), and the High Risk Perception-Worry Group (14.2%, n=45). Logistic regression indicated that education level, employment status, disease duration, complications, and the occurrence of hypoglycemia within a week were all significantly associated with the risk perception categories (p < 0.05). Significant differences in self-management behavior scores were observed among the different risk perception categories (p < 0.05). Specifically, patients in the High Risk Perception-Worry Group attained the highest total score (M = 2.54, SD = 0.56), while those in the Low Risk Perception-Optimism Bias Group scored the lowest (M = 2.02, SD = 1.12).
Conclusion: Three latent categories of complication risk perception were identified in young and middle-aged patients with T2DM, and their self-management behaviors differed significantly across these categories. Clinicians should provide targeted interventions based on the risk characteristics of each category to improve self-management behaviors.
Keywords: young and middle‐aged, type 2 diabetes, risk perception, self-management behavior, latent profile analysis
Introduction
Diabetes mellitus (DM) is a prevalent metabolic disorder characterized by insufficient insulin secretion or impaired insulin action, resulting in protracted hyperglycemia within the body.1 DM is a major public health challenge. Its high incidence and multiple complications have significantly increased the global burden of disease.2 Currently, China has the world’s largest diabetes population. According to statistics,3 as of 2019, the prevalence rate of diabetes in China was 11.9%, whereas it was 12.4% based on the ADA 2010 standard. Among these cases, over 90% are patients with type 2 diabetes mellitus (T2DM).4 Research indicates that in 2021, approximately 1.4 million individuals in China succumbed to complications associated with T2DM.5 Moreover, the financial burden of diabetes treatment is rising steadily. China is also the country with the highest cost of diabetes treatment after the United States, and it is expected to increase to $460 billion by 2030.6 Overall, the spread of T2DM not only poses a serious threat to patients’ health but also exerts tremendous pressure on the global health system and the economy. Adults under 60 years old account for approximately 59% of patients with T2DM,7 and young and middle-aged individuals (aged 18–59 years) have become the fastest-growing group in terms of T2DM prevalence.8 Compared with the general population, those who develop T2DM before age 40 have a 3.72-fold higher risk of death, a greater risk of diabetes-related complications, and worse blood sugar control.9
Although T2DM poses a significant threat to health, particularly among young and middle-aged individuals, effective self-management of the condition can significantly improve health outcomes.10 Self-management is a strategy that uses inner strength to change behavior, reducing negative actions and increasing positive ones.11 Diabetes self-management is not only fundamental for patients to control their condition but also a key factor in preventing diabetic complications and improving quality of life. It mainly includes medication adherence, physical activity, diet and weight management, and blood glucose monitoring.12 Yet young and middle-aged patients often demonstrate suboptimal self-management behaviors due to high work and life pressures and heavy psychological burdens.13
Studies show that the perception of complication risk is one of the key factors influencing diabetic patients’ self-management behaviors.14 Risk perception is defined as individuals’ subjective experiences and feelings regarding potential harm to their health and associated risk factors.15 Extremely low or high risk perception can adversely affect patients’ physical and mental health. Therefore, guiding young and middle-aged patients with T2DM to maintain an appropriate level of risk perception is essential for improving their self-management behaviors.
However, most existing studies assess risk perception level only by the overall scale score, thereby ignoring individual differences.16,17 Latent profile analysis (LPA), a relatively novel statistical method,18 reveals individual differences in multiple variables through data-driven methods, which can accurately classify groups and avoid subjective bias. Compared with traditional methods, LPA provides more detailed and flexible population classification, which helps to provide scientific support for personalized intervention programs.
Currently, relatively few studies have applied LPA to examine risk perception in young and middle-aged patients with T2DM, especially regarding self-management behaviors. Therefore, this study aims to explore the latent categories of complication risk perception in young and middle-aged patients with T2DM using LPA and to analyze differences in self-management behaviors among these categories, thereby providing a reference for precise interventions.
Methods
Study Design
A cross-sectional study incorporating latent profile analysis.
Participants
We recruited young and middle-aged patients with T2DM from the endocrinology department of a tertiary hospital in Jiangsu Province, China, between September 2024 and March 2025. Inclusion criteria were as follows: (1) patients who met the diagnosis criteria of T2DM; (2) age 18–59 years; (3) clear consciousness, normal communication ability, and provision of informed consent for voluntary participation. Exclusion criteria were as follows: (1) presence of severe diabetic complications or other serious organic conditions, end-stage renal disease requiring dialysis, amputation, disabling stroke, or a recent myocardial infarction (within the past 6 months); (2) history of mental illness. (3) participating in other studies, to mitigate potential biases from prior interventions or data collection. Although previous research suggested that the minimum sample size for LPA is 250,19 based on a crude sample size estimation (5–10 times the number of variables, with 26 independent variables in this study) and allowing for a 10% invalid response rate, a minimum of 163 samples was required.
Instruments
General Information Questionnaire
Based on a literature review and team discussions, the researchers designed a data collection tool consisting of two parts: general demographic information and disease-related information. The general demographic information includes age, gender, body mass index (BMI), smoking status, education level, marital status, payment method, region, and employment status. The disease-related information includes family history of diabetes, disease duration, fasting blood glucose, glycated hemoglobin, treatment methods, occurrence of hypoglycemia within a week, presence of complications, and other diseases.
Diabetes Risk Perception Scale (PPS-DM)
The Diabetes Risk Perception Scale (PPS-DM) was developed by Walker et al20 in 2007 and translated into Chinese by Ma et al21 in 2022. It evaluates a patient’s perceived risk of diabetes complications. The scale consists of 23 items across 5 dimensions: personal control (3 items), worry (2 items), optimism bias (2 items), personal disease risk (9 items), and relative environmental risk (7 items). A 4-point Likert scale is used, with responses from “completely disagree/almost no risk” (1 point) to “completely agree/high risk” (4 points). Higher total scores indicate higher risk perception. In this study, the Cronbach’s α for the scale was 0.917, which reflects excellent internal consistency.
Scale of Diabetes Self-Care Activities (SDSCA)
The Scale of Diabetes Self-Care Activities (SDSCA) was developed by Toobert et al22 in 2000 and translated into Chinese by Hua and Zhu23 in 2014. It assesses patients’ self-management behaviors over the past week. The scale contains 11 items in four domains: diet (5 items), exercise (2 items), blood glucose monitoring (2 items), and foot care (2 items). Higher scores indicate better self-management. The total score is 28; a score above 23 signifies good self-management, 17–23 is considered average, and below 17 is poor. In this study, the Cronbach’s αcoefficient of the scale in this study was 0.902, indicating that the scale has good internal consistency.
Data Collection
Before the survey, researchers provided standardized instructions explaining the purpose of the study. After obtaining written informed consent, participants were given detailed guidance on how to complete the questionnaires, including precautions, and were asked to answer independently based on their actual situations. Questionnaires were collected and checked on site; if any responses were unclear, patients were promptly queried for clarification. In this study, 330 questionnaires were distributed, 14 were deemed invalid, and 316 valid questionnaires were ultimately collected, yielding an effective response rate of 95.8%.
Data Analysis
In this study, Mplus 8.0 was used for latent profile analysis, and the number of latent categories determined according to RPS-DM scores was used as the observation index. Model fit was evaluated with multiple indices: Akaike information criterion (AIC), Bayesian information criterion (BIC), and adjusted BIC (aBIC). For these criteria, smaller values indicate better model fit. Entropy values range from 0 to 1, with values closer to 1 indicating more accurate latent class classification. The Lo-Mendell–Rubin test (LMR) and the bootstrap likelihood ratio test (BLRT) were used to compare model solutions; if both p-values were significant (p < 0.05), the K-class model was considered a significantly better fit than the (K-1)-class model.
Data analysis was performed using SPSS 25.0. Categorical variables were expressed as frequencies and percentages, and continuous variables as mean and standard deviations (SD). Group differences were examined using the chi-square test for categorical variables and one-way analysis of variance (ANOVA) for continuous variables. The factors influencing latent category membership were analyzed by a multivariate logistic regression model, with a significance level of p<0.05.
Ethics
This research was conducted in accordance with the Declaration of Helsinki, and written approval was obtained from Kunshan Hospital Affiliated to Jiangsu University Ethics Committee (2024-03-045-H00-K01). Informed consent was obtained from all individual participants included in the study. Participants were provided with detailed information regarding the study’s purpose, procedures, potential risks and benefits, and confidentiality measures. Written consent forms were signed by all participants before their involvement in the research.
Results
Latent Profile Analysis of Complication Risk Perception in Young and Middle-Aged Patients with T2DM
In this study, the scores of the five dimensions of the risk perception scale were analyzed, and a total of four latent profile models were fitted. The fit indices of each model are shown in Table 1. As the number of categories increased from 1 to 4, AIC, BIC, and aBIC values all decreased. Although the four-class model had the highest entropy, its LMR test result was not significant (p > 0.05). Therefore, the three-class model was selected as the optimal solution based on a comprehensive evaluation of the indices. Using this three-class model, the latent profile for each of the three risk perception categories was characterized (Figure 1). Class 1 included 45 patients (14.2%). The risk perception level of this group was higher than that of the other two groups, and their “worry” dimension score was significantly higher than the other dimensions. This group was thus labeled the “High Risk Perception-Worry Group”. Class 2 included 133 patients (42.1%). The scores of all dimensions in this group were moderate, so it was labeled the “Overall Medium Risk Perception Group”. Class 3 included 138 patients (43.7%). This group had the lowest overall risk perception level but a notably high score in the “optimism bias” dimension, so it was labeled the “Low Risk Perception-Optimism Bias Group”. The scores of complication risk perception in the three categories from high to low are as follows: the High Risk Perception-Worry Group (M = 2.54, SD = 0.56), the Overall Medium Risk Perception Group (M = 2.25, SD = 0.83), and the Low Risk Perception-Optimism Bias Group (M = 2.02, SD = 1.12).
 |
Table 1 The Fit Indices of Four Latent Profile Models |
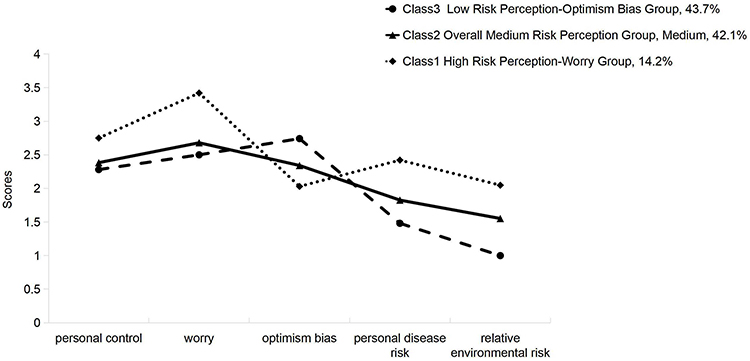 |
Figure 1 Latent profiles of complication risk perception. |
General Characteristics of Young and Middle-Aged Patients with T2DM
Among the 316 young and middle-aged patients with T2DM, 156 (49.4%) were 18–44 years old and 160 (50.6%) were 45–59 years old. The majority were male (63.6%), non-smokers (60.8%), married (83.9%), employed (70.9%), town residents (55.4%), and those who use the national medical insurance payment method (87.0%). However, those with a bachelor’s degree or above account for only 9.2%. In terms of disease-related conditions, the majority of patients had a family history of diabetes (53.8%), concurrent other diseases (60.4%), diabetes duration less than 5 years (55.1%), and glycated hemoglobin not up to standard (91.1%). Regarding complications, the majority of patients had none (76.3%), while the remainder had only non-severe complications (23.7%), such as mild peripheral neuropathy, non-proliferative retinopathy, or microalbuminuria. The predominant treatment was oral hypoglycemic drugs combined with insulin (52.2%). It should be noted that the study participants were recruited from a tertiary hospital, which may account for the observed high frequency of insulin therapy. Other general characteristics of the participants are presented in Table 2.
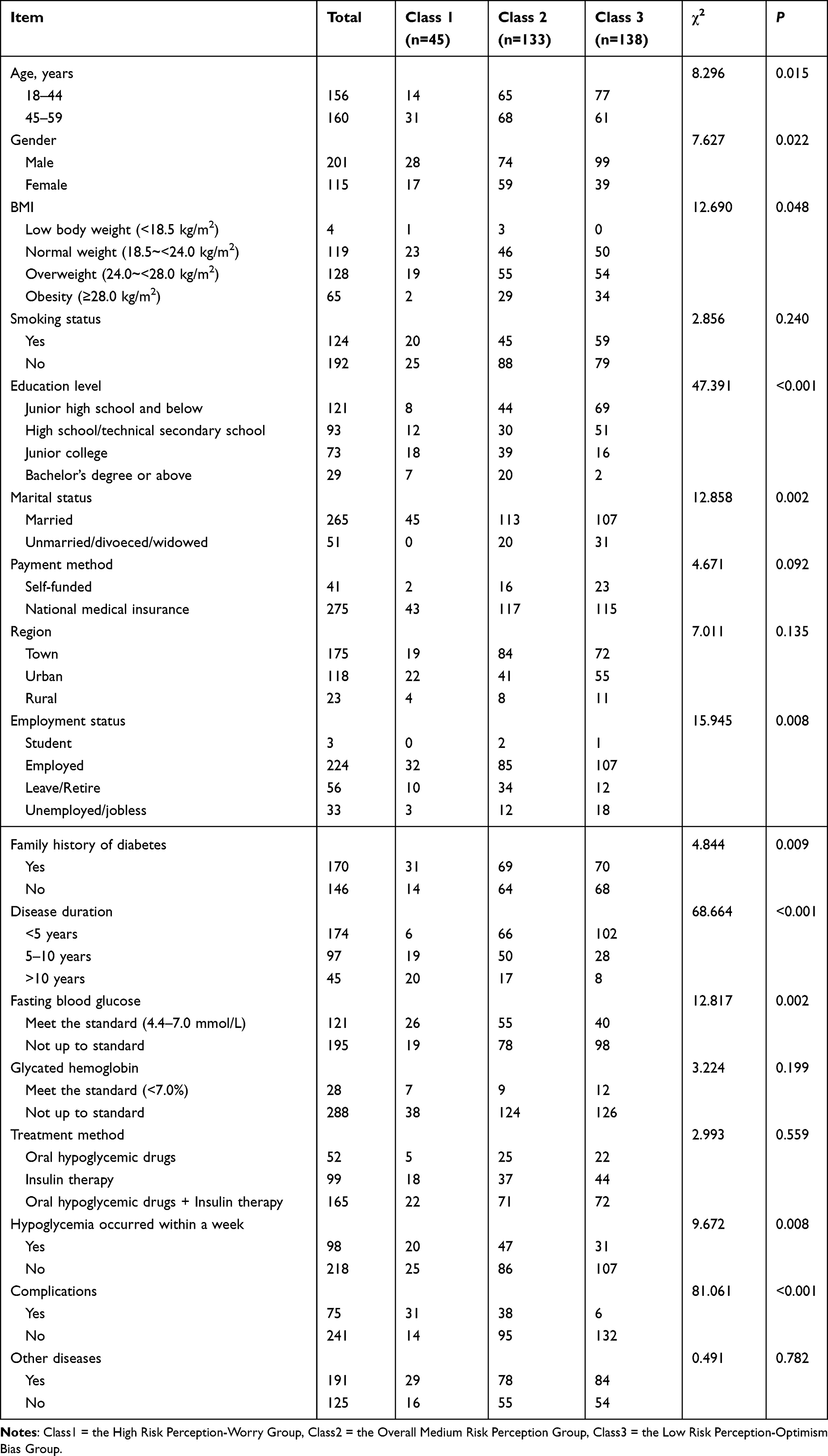 |
Table 2 Comparison of General Demographic Characteristics of Different Potential Categories in Young and Middle-Aged Patients with T2DM |
Comparison of Self-Management Behaviors in Young and Middle-Aged Patients with T2DM Across Different Risk Perception Categories
The self-management behavior scores for the three risk perception categories are presented in Table 3. Analysis of variance was used for inter-category comparison. The results showed that the self-management behaviors of different categories of risk perception were statistically significant (p<0.01). The least significant difference method (LSD-t) was utilized for further pairwise comparisons. The results suggested statistically significant differences in the total scores and dimensions of self-management behaviors across the three categories (p<0.05). Specifically, the High Risk Perception-Worry Group had the highest scores in diet, exercise, blood glucose monitoring, and foot care, the Overall Medium Risk Perception Group had intermediate scores, and the Low Risk Perception-Optimism Bias Group had the lowest scores.
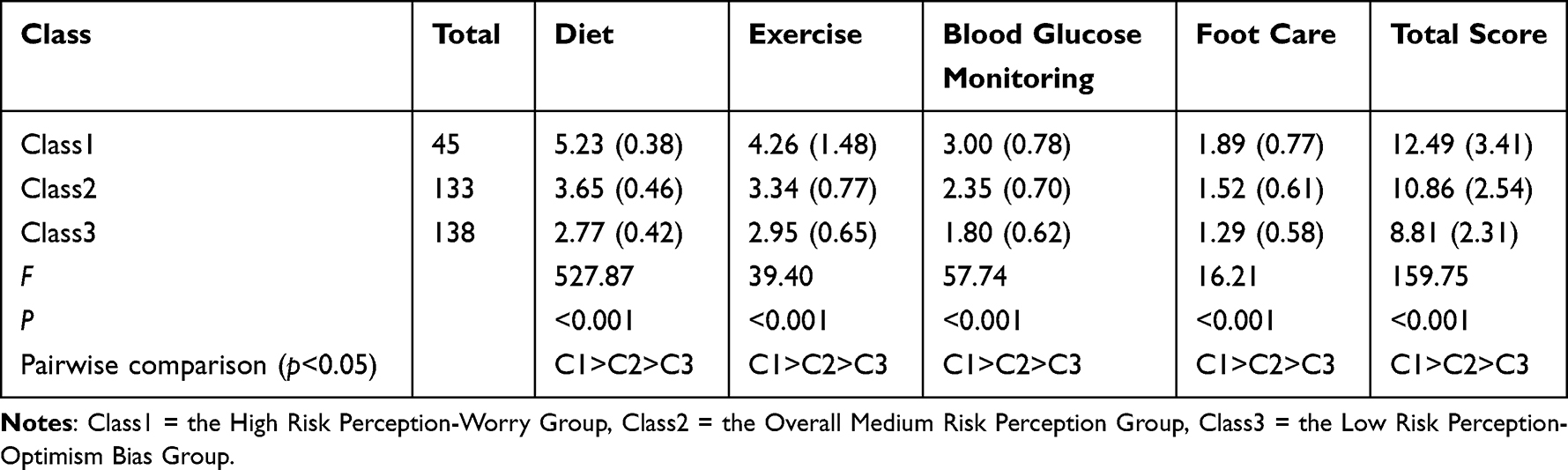 |
Table 3 Comparison of Self-Management Ability Scores Among Young and Middle-Aged Patients with T2DM in Different Categories |
Univariate Analysis of Factors Associated with Risk Perception Categories in Young and Middle-Aged Patients with T2DM
In comparing general characteristics across the different latent risk perception categories, there were no statistically significant differences in variables such as smoking status, region, HbA1c, treatment methods, or presence of other diseases (p>0.05). Table 2 highlights the variables that showed statistically significant differences between categories.
Multivariate Analysis of Factors Influencing Risk Perception Categories in Young and Middle-Aged Patients with T2DM
A multivariate logistic regression was performed with the risk perception category (latent class) as the dependent variable and the factors showing significant differences in univariate analysis as independent variables. The “High Risk Perception-Worry Group” was set as the reference category, and the coding of independent variables is shown in Table 4.
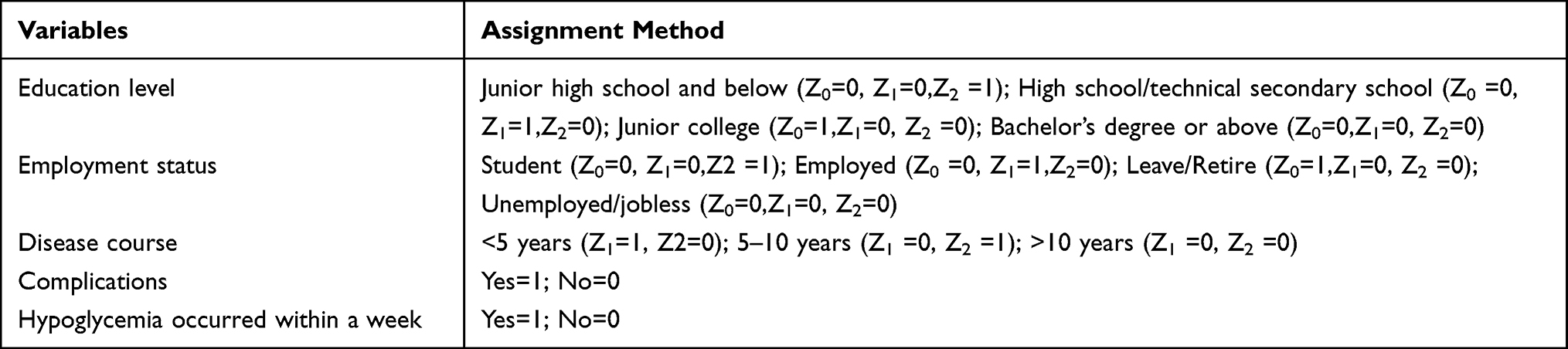 |
Table 4 Variable Assignment Methods |
The regression results indicated that compared with the High Risk Perception-Worry Group, patients with a junior high school education and below (OR=5.825, 95% CI=1.920–17.651), those who were employed (OR=2.833, 95% CI=1.542–8.877), and those with a disease duration of <5 years (OR=3.405, 95% CI=1.650–9.454) were more likely to belong to the Low Risk Perception-Optimism Bias Group, while patients with existing diabetic complications (OR=0.612, 95% CI=0.421–0.936) were less likely to belong to the Low Risk Perception-Optimism Bias Group. Compared with the High Risk Perception-Worry Group, patients with existing diabetic complications (OR=0.797, 95% CI=0.639–0.994) or who had experienced hypoglycemia in the past week (OR=0.256, 95% CI=0.082–0.968) were less likely to belong to the Overall Medium Risk Perception Group. There were no statistically significant differences in age, gender, BMI, family history of diabetes, payment method, marital status, or fasting blood glucose among the three risk perception categories (p>0.05), as shown in Table 5.
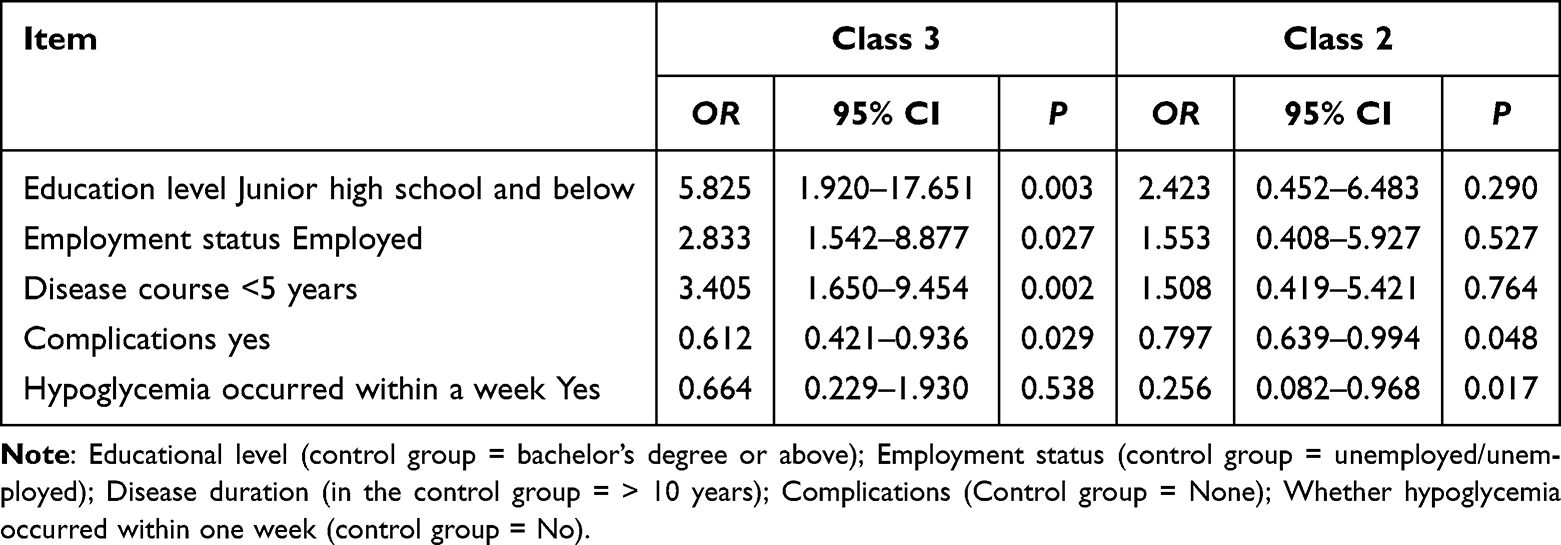 |
Table 5 Multivariate Logistic Regression Analysis of Potential Categories of Complication Risk Perception in Young and Middle-Aged Patients with T2DM |
Discussion
Characteristics of Latent Risk Perception Categories in Young and Middle-Aged Patients with T2DM
Using latent profile analysis, this study identified three latent risk perception categories among young and middle-aged patients with T2DM: the Low Risk Perception-Optimism Bias Group, the Overall Medium Risk Perception Group, and the High Risk Perception-Worry Group. This finding indicates the presence of group heterogeneity in complication risk perception.
Specifically, the Low Risk Perception-Optimism Bias Group comprised 43.7% of the patients, making it the largest subgroup. Based on the existing literature, this finding is consistent with previous research indicating that a considerable proportion of young and middle-aged patients with T2DM have insufficient perception of complication risk.24 Patients in this group scored higher on the “optimism bias” dimension than on other dimensions, indicating a tendency toward blindly optimistic attitudes in the face of their disease. In contrast, their scores on the “personal disease risk” and “relative environmental risk” dimensions were relatively low, suggesting insufficient awareness of diabetes risk factors and personal disease risk. A global survey reveals that 10% of patients with T2DM are not aware of cardiovascular diseases and their risk factors, and approximately 17% of respondents reported that healthcare workers have never discussed the correlation between the two with patients.25 Therefore, the early identification of this important subgroup has a significant impact on clinical practice.
The Overall Medium Risk Perception Group comprised 42.1% of patients. The average score for each item in this group was intermediate relative to the other groups. These patients recognized the existence of risks to some extent, but their scores were not high, lower than the results of previous research.26 This indicates that the patients’ risk knowledge source channel is single, and perception is incomplete. Although patients have received fragmented health education, it is difficult to establish a complete risk perception framework. It can be seen from this that the current health education model has structural deficiencies in the risk transmission of diabetic complications, which may weaken patients’ awareness of early warning and prevention and control behaviors regarding diabetic complications.
The High Risk Perception-Worry Group represented 14.2% of patients, and its risk perception was the highest among the groups. Notably, the “worry” dimension score was the highest in this group, indicating that these patients maintained a high level of concern about the potential threats of diabetes, but there might be psychological barriers. This perception of high risk can provide patients with a certain degree of confidence and motivation in self-management, but excessive anxiety may backfire.27 Therefore, in clinical work, it is recommended to incorporate psychological distress related to diabetes into routine screening, thereby enhancing the accuracy of their risk perception.
Differences in Self-Management Behavior Levels Among Young and Middle-Aged Patients with T2DM with Different Categories of Complication Risk Perception
Diabetes self-management is not only a core component of treatment but also the foundation for achieving long-term health and improved quality of life.28 The results of this study confirmed that self-management behavior levels differed significantly among young and middle-aged patients with T2DM across the different risk perception categories. These findings underscore the crucial relationship between complication risk perception and self-management behaviors, especially in young and middle-aged patients with T2DM.
In our study, the High Risk Perception-Worry Group achieved the highest self-management behavior scores, the Overall Medium Risk Perception Group had intermediate scores, and the Low Risk Perception-Optimism Bias Group had the lowest scores. This pattern suggests that risk perception may directly or indirectly affect patients’ self-management behaviors.29 An appropriate level of risk perception can increase patients’ attention to their health status and promote active engagement in self-monitoring and management. The health belief model (HBM) suggests that while some patients recognize the importance of self-management, they may struggle to maintain healthy behaviors over time due to a lack of motivation or self-efficacy, possibly leading to declining behavioral compliance.30 Therefore, in clinical practice, healthcare providers should incorporate risk education on diabetic complications into the core content of diabetes management and adopt problem-oriented teaching methods, such as scenario simulation and case guidance, which could enhance patients’ glycemic control and behavioral outcomes.31 By integrating multi-disciplinary teams such as nutrition and psychology, personalized intervention plans can be formulated.32 At the same time, regularly checking patients’ self-monitoring records allows for the timely provision of specific praise and data feedback, which encourages patients to recognize their progress and enhance their self-confidence. Additionally, for emotional cognitive biases, the psychological resilience training model can be drawn upon. Through mindfulness intervention and stress management courses, patients’ emotional regulation abilities can be enhanced, promoting the transformation of healthy behaviors. Nonetheless, research linking risk perception and self-management behavior remains limited. Future studies should further explore how to determine an “appropriate” risk perception threshold and identify a balance that encourages effective self-management without inducing excessive anxiety.
Factors Influencing Latent Risk Perception Profiles in Young and Middle-Aged Patients with T2DM
Patients with an education level of junior high school and below were about 5 times more likely to be classified into the Low Risk Perception-Optimism Bias Group than into the High Risk Perception-Worry Group. Consistent with this finding, other studies have shown that education level is negatively correlated with risk perception of patients; that is, the lower the patient’s level of education, the lower their complication risk perception tends to be.33 Patients with limited formal education often have restricted access to health information and a shallow understanding of diabetes and its complications, which may lead them to underestimate the disease’s severity and its potential risks.34 Therefore, healthcare providers should offer personalized health education programs tailored to different education levels—especially for patients with less education—to use visual aids such as pictures and videos, which can be utilized to help patients understand the concept, complications, and management methods of diabetes more intuitively.35
This study also found that patients with a disease duration of less than 5 years were more likely to be classified into the Low Risk Perception-Optimism Bias Group, consistent with previous findings.36 This may be because patients with shorter disease duration have less illness experience and thus a lower risk perception. Most individuals diagnosed at a younger age or early stage have not yet encountered obvious complications or treatment difficulties, and they are not fully aware of diabetes’s long-term harms. In addition, lacking the chronic health stress that accumulates over a longer disease course and receiving insufficient health education can lead these patients to underestimate the seriousness of diabetes.37 Therefore, educational interventions for this population are particularly critical. Clinicians should employ personalized communication strategies tailored to patients’ needs and preferences during risk communication, to improve their accurate understanding of diabetes complications risk and to foster more effective self-management.
Notably, employment status was another important predictor of belonging to the Low Risk Perception-Optimism Bias Group among young and middle-aged patients with T2DM. Employed young and middle-aged patients were more likely to be classified into the Low Risk Perception-Optimism Bias Group. This finding is consistent with existing research literature, which shows that compared with elderly patients, middle-aged and young patients tend to focus more on career development and financial pressures, leaving insufficient time and energy for their health, resulting in an insufficient understanding of the severity of the disease.38 Therefore, healthcare providers should attach importance to building and optimizing family and social support systems for this group of people. Meanwhile, they can develop a home diabetes care application platform based on digital technology to help them better balance work and diabetes self-management in daily life.39
This study found that most patients with existing diabetic complications fell into the High Risk Perception-Worry Group. This is supported by previous research, which indicates that personal experience of diabetic foot ulcers made patients more aware of their health risks.40 These patients accordingly become more concerned about future health problems. This finding suggests that healthcare providers should implement differentiated health education strategies in practice. For patients with low risk perception, experiential education about complications can be used to increase their awareness of diabetes’s potential hazards. By demonstrating the actual consequences of diabetes complications, such education helps patients more intuitively understand the risks of diabetes and thereby enhances their health management behaviors.41 For patients already experiencing diabetes complications, although they have high health awareness, they may develop excessive worry and anxiety about their health. Medical staff should attach importance to patients’ benefit experience, strengthen the education on diabetes complications, reshape disease cognition, and help patients better accept and cope with the disease.
This study found that compared to the Overall Medium Risk Perception Group, patients who had experienced hypoglycemia within the past week were more likely to belong to the High Risk Perception-Worry Group. This may be because hypoglycemic episodes are often accompanied by distress and potentially serious consequences,42 making patients more vigilant and concerned about managing their condition. However, previous studies have shown that an excessive fear of hypoglycemia can hinder blood sugar control and negatively affect patients’ quality of life.43 It is recommended that healthcare providers strengthen patients’ ability to recognize and handle hypoglycemia through timely interventions and education, thereby improving their confidence and the effectiveness of self-management.
Limitations
This study has several limitations. First, we selected patients from a single tertiary hospital in Jiangsu Province, China, which may limit the generalizability of our findings due to potential sample bias. Second, the study was cross-sectional, so it could not capture dynamic changes over time. Future studies could employ a latent class growth model to more comprehensively examine the trajectories of relevant variables over time. Third, we acknowledge that the observed association between risk perception profiles and disease duration may be influenced by confounding, as longer exposure to the disease could independently heighten risk awareness. Finally, our data were self-reported, which introduces the possibility of social desirability bias and recall bias, potentially affecting the accuracy and objectivity of the results. Future research should consider combining objective measures (such as direct behavioral observations) with self-reports to obtain a more comprehensive understanding of self-management behaviors and risk perceptions in young and middle-aged patients with T2DM.
Conclusions
This study used latent profile analysis to classify young and middle-aged patients with T2DM into different complication risk perception categories and examined the relationship between these categories and self-management behaviors. We identified three distinct latent categories of risk perception: the Low Risk Perception-Optimistic Bias Group, the Overall Medium Risk Perception Group, and the High Risk Perception-Worry Group. Each category exhibited different self-management behaviors. Our findings underscore that complication risk perception can positively influence self-management behaviors in young and middle-aged patients with T2DM. Therefore, our study sheds light on the diverse risk profiles among patients, which underscores the necessity of personalized approaches in diabetes care. Future research could focus on creating practical tools or guidelines that would allow healthcare providers to deliver risk communication and interventions tailored to the characteristics of distinct risk subgroups, with the ultimate goal of improving patients’ risk perception and self-management behaviors.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author.
Ethical Conduct of Research
At the outset, written approval was obtained from Kunshan Hospital Affiliated to Jiangsu University Non-Invasive Ethics Committee (2024-03-045-H00-K01), Kunshan Hospital Affiliated to Jiangsu University Chief Physician, and Endocrinology Department to conduct the study.
Acknowledgments
We thank all the participants for their corporation. Special thanks to our supervisor—Xueqin Jin for the funding and support, as well as the efforts and contributions made by the research team throughout the study. The study was supported by the Medical Discipline Project of Suzhou [number SZFCXK202106].
Author Contributions
Conceptualization: Yuting Zhang, Xueqin Jin; Methodology: Yuting Zhang, Xueqin Jin; Data collection and data analysis: Yuting Zhang; Writing-original draft: Yuting Zhang; Writing-review & editing:Yuting Zhang, Xueqin Jin; Supervision: Xueqin Jin; Funding acquisition: Xueqin Jin. All authors gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Disclosure
The authors have no conflicts of interest to report.
References
1. American Diabetes Association. Introduction: standards of Medical Care in Diabetes—2022. Diabetes Care. 2022;45(Supplement_1):S1–S2. doi:10.2337/dc22-Sint.
2. Blair Y, Wessells H, Pop-Busui R, et al. Urologic complications in diabetes. J Diabet Complicat. 2022;36(10):108288. doi:10.1016/j.jdiacomp.2022.108288
3. Wang L, Peng W, Zhao Z, et al. Prevalence and Treatment of Diabetes in China, 2013-2018. JAMA. 2021;326(24):2498. doi:10.1001/jama.2021.22208
4. Wu X, Liu X, Liao W, et al. Prevalence and characteristics of alcohol consumption and risk of type 2 diabetes mellitus in rural China. BMC Public Health. 2021;21(1):1644. doi:10.1186/s12889-021-11681-0
5. Zhu D, Zhou D, Li N, Han B. Predicting Diabetes and Estimating Its Economic Burden in China Using Autoregressive Integrated Moving Average Model. Int J Public Health. 2022;66:1604449. doi:10.3389/ijph.2021.1604449
6. Liu J, Liu M, Chai Z, et al. Projected rapid growth in diabetes disease burden and economic burden in China: a spatio-temporal study from 2020 to 2030. Lancet Regional Health - Western Pacific. 2023;33:100700. doi:10.1016/j.lanwpc.2023.100700
7. Xu Y, Lu J, Li M, et al. Diabetes in China part 1: epidemiology and risk factors. Lancet Public Health. 2024;9(12):e1089–e1097. doi:10.1016/S2468-2667(24)00250-0
8. Zhang Y, Luk AOY, Chow E, et al. High risk of conversion to diabetes in first-degree relatives of individuals with young-onset type 2 diabetes: a 12-year follow-up analysis. Diabet Med. 2017;34(12):1701–1709. doi:10.1111/dme.13516
9. Lin B, Coleman RL, Bragg F, et al. Younger-onset compared with later-onset type 2 diabetes: an analysis of the UK Prospective Diabetes Study (UKPDS) with up to 30 years of follow-up (UKPDS 92). Lancet Diabetes Endocrinol. 2024;12(12):904–914. doi:10.1016/S2213-8587(24)00242-0
10. Polsook R, Aungsuroch Y, Thontham A. The effect of self‐management intervention among type 2 diabetes: a systematic review and meta‐analysis. Worldviews Ev Based Nurs. 2024;21(1):59–67. doi:10.1111/wvn.12688
11. Lorig KR, Holman HR. Self-management education: history, definition, outcomes, and mechanisms. Ann Behav Med. 2003;26(1):1–7. doi:10.1207/S15324796ABM2601_01
12. Luo X, Liu T, Yuan X, et al. Factors Influencing Self-Management in Chinese Adults with Type 2 Diabetes: a Systematic Review and Meta-Analysis. IJERPH. 2015;12(9):11304–11327. doi:10.3390/ijerph120911304
13. Sato M, Yamazaki Y. Work‐related factors associated with self‐care and psychological health among people with type 2 diabetes in Japan. Nursing & Health Sciences. 2012;14(4):520–527. doi:10.1111/j.1442-2018.2012.00729.x
14. Vaja I, Umeh KF, Abayomi JC, et al. A grounded theory of type 2 diabetes prevention and risk perception. British J Health Psychol. 2021;26(3):789–806. doi:10.1111/bjhp.12503
15. Ferrer RA, Klein WM. Risk perceptions and health behavior. Current Opinion in Psychology. 2015;5:85–89. doi:10.1016/j.copsyc.2015.03.012
16. Liang F, Ye Y, Peng L, et al. Study on the status quo and influencing factors of risk perception of cardiovascular disease in high-risk populations. Military Nursing. 2024;41(11):49–52. doi:10.3969/j.issn.2097-1826.2024.11.012
17. Li L, Kou T, Wang X, et al. A study on the correlation between shared decision-making and risk perception in type 2 diabetes patients. Mod Preventive Med. 2025;52(1):97–102. doi:10.20043/j.cnki.MPM.202407370
18. Yin K, Peng J, Zhang J. The application of latent profile analysis in organizational behavior research. Adv Psychol Sci. 2020;28(7):1056–1070. doi:10.3724/SP.J.1042.2020.01056
19. Tein J-Y, Coxe S, Cham H. Statistical Power to Detect the Correct Number of Classes in Latent Profile Analysis. Struct Equ Modeling. 2013;20(4):640–657. doi:10.1080/10705511.2013.824781
20. Walker EA, Caban A, Schechter CB, et al. Measuring Comparative Risk Perceptions in an Urban Minority Population. Diabetes Educ. 2007;33(1):103–110. doi:10.1177/0145721706298198
21. Ma H, Niu M, Li F, et al. Chinese version of the risk perception survey for diabetes mellitus and its reliability and validity testing. J Nurses Training. 2022;37(9):769–773. doi:10.16821/j.cnki.hsjx.2022.09.001
22. Toobert DJ, Hampson SE, Glasgow RE. The summary of diabetes self-care activities measure: results from 7 studies and a revised scale. Diabetes Care. 2000;23(7):943–950. doi:10.2337/diacare.23.7.943
23. Hua L, Zhu W. Reliability and validity validation of the Chinese version of the Diabetes Self-Management Behavior Scale. J Nursing Chin People’s Liberation Army. 2014;31(16):5–8. doi:10.3969/j.issn.1008-9993.2014.16.002
24. Gu Y, Chen Y, Tang Q, et al. Study on the status quo and influencing factors of complication risk perception in elderly diabetics in nursing institutions. J Nursing. 2023;38(19):105–108. doi:10.3870/j.issn.1001-4152.2023.19.105
25. Saeedi P, Karuranga S, Hammond L, et al. Cardiovascular diseases and risk factors knowledge and awareness in people with type 2 diabetes mellitus: a global evaluation. Diab Res Clin Pract. 2020;165:108194. doi:10.1016/j.diabres.2020.108194
26. Calvin D, Quinn L, Dancy B, et al. African Americans’ Perception of Risk for Diabetes Complications. Diabetes Educ. 2011;37(5):689–698. doi:10.1177/0145721711416258
27. Zhu Y, Xu H, Ding D, et al. Resourcefulness as a mediator in the relationship between self-perceived burden and depression among the young and middle-aged stroke patients: a cross-sectional study. Heliyon. 2023;9(8):e18908. doi:10.1016/j.heliyon.2023.e18908
28. Davis J, Fischl AH, Beck J, et al. National Standards for Diabetes Self-Management Education and Support. Diabetes Care. 2022;45(2):484–494. doi:10.2337/dc21-2396
29. Chen Z, Li Y, Wu F. Research progress on the correlation of complication risk perception in type 2 diabetes patients. Chin J Modern Nurs. 2024;30(23):3216–3220. doi:10.3760/cma.j.cn115682-20231125-02232
30. Jiang X, Jiang H, Li M, et al. The Mediating Role of Self‐Efficacy in Shaping Self‐Management Behaviors Among Adults With Type 2 Diabetes. Worldviews Ev Based Nurs. 2019;16(2):151–160. doi:10.1111/wvn.12354
31. Yuan X, Wang F, Fish AF, et al. Effect of case management on glycemic control and behavioral outcomes for Chinese people with type 2 diabetes: a 2-year study. Patient Educ Couns. 2016;99(8):1382–1388. doi:10.1016/j.pec.2016.03.010
32. Levengood TW, Peng Y, Xiong KZ, et al. Team-Based Care to Improve Diabetes Management: a Community Guide Meta-analysis. Am J Preventive Med. 2019;57(1):e17–e26. doi:10.1016/j.amepre.2019.02.005
33. Li F, Gao Y, Xu Q, et al. Correlation between risk perception and self-management level of young and middle-aged patients with type 2 diabetes mellitus. Nursing Research. 2023;37(4):590–595. doi:10.12102/j.issn.1009-6493.2023.04.005
34. Skrine Jeffers K, Cadogan M, Heilemann MV, Phillips LR. Assessing Informal and Formal Diabetes Knowledge in African American Older Adults With Uncontrolled Diabetes. J Gerontol Nurs. 2019;45(2):35–41. doi:10.3928/00989134-20190111-06
35. Baptista DR, Wiens A, Pontarolo R, et al. The chronic care model for type 2 diabetes: a systematic review. Diabetol Metab Syndr. 2016;8(1):7. doi:10.1186/s13098-015-0119-z
36. Zhang H, Tian X, Li Q, et al. Analysis of situation and influencing factors of perceived risk of recurrence in middle-aged and elderly stroke patients. J Nurses Training. 2025;40(9):897–902. doi:10.16821/j.cnki.hsjx.2025.09.001
37. Guo Z, Fu Y, Wang X, et al. The impact of perception bias for cardiovascular disease risk on physical activity and dietary habits. Int J Nurs Sci. 2024;11(5):505–512. doi:10.1016/j.ijnss.2024.10.011
38. Cai P, Liang Y, Wang J, et al. Analysis of the trajectory of dietary behavior compliance and influencing factors in young and middle-aged patients with type 2 diabetes. Chin J Nurs. 2024;59(13):1592–1599. doi:10.3761/j.issn.0254-1769.2024.13.009
39. Mehraeen E, Noori T, Nazeri Z, et al. Identifying features of a mobile-based application for self-care of people living with T2DM. Diab Res Clin Pract. 2021;171:108544. doi:10.1016/j.diabres.2020.108544
40. Mogre V, Johnson NA, Tzelepis F, Paul C. Attitudes towards, facilitators and barriers to the provision of diabetes self-care support: a qualitative study among healthcare providers in Ghana. Diabetes Metab Syndr. 2019;13(3):1745–1751. doi:10.1016/j.dsx.2019.03.041
41. Yan J, Qiu H, Jia Y, et al. Application of simulated experience-based complication health education in young and middle-aged patients with newly diagnosed type 2 diabetes. J Nurs. 2021;28(5):75–78. doi:10.16460/j.issn1008-9969.2021.05.075
42. Amiel SA, Amiel SA. The consequences of hypoglycaemia. Diabetologia. 2021;64(5):963–970. doi:10.1007/s00125-020-05366-3
43. Wu C, Wang W, Cheng S, et al. The relationship between components of hypoglycemia worries and avoiding hypoglycemia behavior in type 2 diabetes mellitus with hypoglycemia: a network analysis. BMC Psychiatry. 2023;23(1):204. doi:10.1186/s12888-023-04698-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.