Back to Journals » Risk Management and Healthcare Policy » Volume 16
Predictors of Compassion Satisfaction, Compassion Fatigue, and Burnout Among Nursing Professionals in a Medical City in Saudi Arabia
Authors Alreshidi SM ![]() , Rayani AM
, Rayani AM ![]()
Received 10 November 2023
Accepted for publication 20 December 2023
Published 22 December 2023 Volume 2023:16 Pages 2883—2892
DOI https://doi.org/10.2147/RMHP.S430082
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Salman M Alreshidi,* Ahmad M Rayani*
Community and Psychiatric Mental Health Nursing Department, King Saud University, Riyadh City, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Salman M Alreshidi, Community and Psychiatric Mental Health Nursing Department, College of Nursing, King Saud University, P.O. Box 12372, Riyadh, Saudi Arabia, Email [email protected]
Purpose: The present study aims to evaluate compassion satisfaction (CS), compassion fatigue (CF), and burnout levels in a population of nurses employed at medical city in Riyadh City, Saudi Arabia.
Patients and Methods: A self-report survey was employed to gather data from 300 nurses at the selected medical city in Riyadh. The survey incorporated a demographic inquiry along with the utilization of the Professional Quality of Life Scale version 5 (ProQOL 5). The ProQOL scale is one of the most widely used measures of CS, CF, and burnout. The ProQOL scale assesses multiple domains of work experiences (ie CS, CF, and burnout). This survey was disseminated through email channels, and it garnered participation from 177 nurses, culminating in a response rate of 59%.
Results: The study’s findings reveal that nurses displayed average mean levels of CS, CF, and burnout. Interestingly, the participants aged 18– 56 reported higher levels of burnout, particularly those in the age groups of 18– 25, 26– 35, and 36– 56. Moreover, those with under 10 years’ experience exhibited higher degrees of burnout and less CS compared to their more experienced counterparts. Additionally, nurses with professional qualifications demonstrated better scores on CS, CF, and burnout compared to those without such qualifications.
Conclusion: The experience of CF and CS among nurses appears to be influenced by multiple variables, such as length of experience, age, and professional qualifications. Nurses in certain age groups and with less experience are more prone to experiencing burnout, while having professional qualifications seems to protect against adverse outcomes to some extent.
Keywords: compassion satisfaction, compassion fatigue, burnout, survey, Saudi, nurses
Introduction
Nursing is commonly recognize as being a stressful occupation due to the need to manage the complexities of patient care and complex operational settings. Nurses are subjected to emotional and physical demands and lack support on a structural and social level. Nursing professionals often experience a myriad of mental and physical health issues (including sleep disorders, depression, relationship problems, diminished empathy, grief, anxiety, and physical complaints) as a consequence of the demands and stress associated with their roles.1–3
The term Compassion Fatigue (CF) is used to refer to the adverse emotional outcomes associated with being exposed to the psychological and physical anguish of patients in the context of self-care practices.4 Due the inherent complexities of their occupation, nurses often suffer the indirect trauma of CF, when patients suffer.4 CF can arise if a carer is exposed to the traumatic experiences of their patients on an ongoing basis.5 Todaro-Franceschi4 frames CF as a direct outcome of the relationships nurses have with their patients. Stamm5 Indications of CF may encompass disassociation and depersonalization from extensive symptoms of anxiety, sleep disturbances, persistent recollection of distressing episodes, and a deliberate effort to steer clear of any triggers associated with those distressing occurrences (p. 5). The concept of CF is often employed interchangeably with secondary trauma, which is more commonly known as secondary traumatic stress (STS).3 Frequently, nurses grappling with CF find it challenging to sustain emotional involvement with their patients, even though they openly express their enduring passion for their profession.6
At first, CF was commonly employed as a synonym for burnout. Nevertheless, contemporary literature has drawn a clear distinction between the two.4 In the nursing context, CF is specifically linked to the nurse-patient relationship, whereas burnout encompasses a broader spectrum of a nurse’s discontent with various aspects of their profession, including factors such as compensation, organizational culture, nursing specialization, and their interactions with patients.4,7 Hooper et al1 describe how “Symptoms of burnout include fatigue, illness, disillusionment, cynicism, anger, difficulties sleeping, and a sense of helplessness/hopelessness” (p. 422). A nurse suffering from burnout might appear detached and disconnected from their work from an outsider’s perspective. Yet it is more often a sense of powerlessness to change their situation, rather than disconnection.4 CF tends to manifest rapidly and abate relatively quickly, whereas burnout develops gradually and takes a longer time to alleviate.8 Simultaneously, the nursing profession in Saudi Arabia faces numerous challenges as a result of burnout, and nurses’ intentions to leave.9–11 Moreover, in Saudi Arabia studies show high percentages of prevalence of burnout among healthcare providers (38–82.3%) and show high levels of burnout especially among nurses.12–14
CF and burnout are not predetermined outcomes of a nursing career. On the contrary, Compassion Satisfaction (CS) symbolizes the sense of fulfillment that nurses experience when they excel in their professional roles.5 Nurses who experience high levels of CS derive greater job satisfaction because they perceive themselves as more effective in providing care to their patients.5 CS acts as a safeguard, counterbalancing the adverse impacts of burnout and CF. The pleasure derived from caring for patients serves to inoculate a nurse against the adverse variables that lead to CF and burnout.1,15 Satisfaction is achieved through the capacity to ease a patient’s discomfort without becoming overcome by emotional responses.1 Moreover, nurses with elevated CS scores have been found to be more successful with the separation between their personal and work lives.8
Although there is ongoing debate in the literature regarding the precise definitions and applications of CF, burnout, and CS, the fundamental framework remains intact. Nursing is a profession that can be emotionally and physically draining, and it has the potential to make nurses experience feelings of hopelessness and devaluation. Nevertheless, there are nurses who confront patient suffering on a daily basis and still find fulfillment in their work.4
The objective of this study was to investigate the levels of CS, CF, and burnout among all nurses employed at Medical City in Riyadh City. A recent review of the existing literature indicates that nurses often encounter elevated levels of CF and burnout when they work extended shifts and put in more than full-time hours.3,8,16 Our research aligns with these findings. Furthermore, studies have demonstrated that nurses with greater years of experience typically exhibit higher levels of CS and lower rates of CF.6,17 The literature review revealed that previous studies did not specifically explore the role of certification in conjunction with CF, CS, and burnout among nurses. Our study fills this gap in the existing literature. Additionally, our research contributes to the ongoing discourse in the literature concerning the correlation between nursing specialties and CF, CS, and burnout. The primary objectives of our study were (a) to determine the prevalence of CS, CF, and burnout among nurses, and (b) to investigate how various work-related and demographic factors impact the development of CS, CF, and burnout in nurses.
Literature Review
Compassion and the desire to provide care for others are often the driving forces that draw individuals into helping professions. However, an intense level of empathy for those going through crises and traumatic experiences can make one susceptible to CF and burnout. The repercussions of CF experienced by nurses encompass a rise in staff resignations and absenteeism, a decline in the quality of patient care and safety, reduced patient satisfaction, and challenges in staff recruitment and retention.18 CF can be a leading factor in nurses choosing to exit the profession, and it has a substantial impact on their personal lives. Individuals experiencing CF may exhibit symptoms such as irritability, detachment, reduced tolerance, feelings of sadness, depression, and a noticeable lack of compassion and empathy towards their patients.1
CF and burnout are not one-size-fits-all experiences in the nursing field. Each nurse encounters CF and burnout differently. The patient population with whom a nurse interacts can significantly influence the degree of CF, CS, and burnout they may undergo. Kolthoff and Hickman6 CF can manifest in nurses who work with older populations, as these patient groups often contend with more complex medical issues and higher mortality rates compared to younger patients. Moreover, a study revealed that working with pediatric patients diagnosed with severe or terminal conditions was a significant factor contributing to the development of CF in nursing.19 Specialization within the nursing profession can also influence a nurse’s CS. For instance, one study indicated that ICU nurses are more prone to experiencing reduced levels of CS compared to nurses in other specialties.20
Numerous studies have underscored the significance of nurses’ experience levels as a determining factor in CS, CF, and burnout. A specific study highlighted the role of inexperience among nurses, attributing it to their feelings of inadequacy and helplessness, ultimately contributing to CF.8 Additionally, research found that nurses with fewer than 10 years of experience exhibited lower levels of CS compared to those with over a decade of experience.17 In another investigation conducted by Kolthoff and Hickman,6 it was revealed that nurses with less than a year of experience were more prone to CF when compared to their counterparts with more than a year of experience with the same patient population.
In a separate study by Berger, Polivka19 it was noted that pediatric nurses with 4–10 years of experience were at a heightened risk of burnout, while nurses exhibited the highest levels of CS when they possessed over two decades of experience and were above the age of 40. The study by Kolthoff and Hickman6 also linked the vulnerability of inexperienced nurses to their failure to establish a peer support network or potentially to neglecting activities that could provide them with the necessary energy to attend to their patients’ needs.
In addition to specialization and years of experience, the literature highlights the potential influence of extended shifts and overtime on CF. Nursing has a history of 12-hour shifts and overtime work.3,8 Several studies discovered that nurses working more hours per week were at a higher risk of experiencing elevated levels of CF compared to those working 40 hours or less.3,8
The literature underscores the non-uniform impact of CS, CF, and burnout on nurses, with variables such as specialty, patient population, and years of experience influencing their levels of these phenomena.8,19,20 Consequently, strategies to mitigate CS, CF, and burnout cannot be universally applied to all nurses. It is imperative to explore all potential contributing factors comprehensively to ensure effective responses. However, while the literature has provided valuable insights into the conditions leading to CF, CS, and burnout, some consistent issues arise concerning the homogeneity of the study samples. The demographics of the participants in these studies were often fairly uniform, with a significant majority identifying as Caucasian or White when asked to specify their race.6,19 Moreover, many studies did not even inquire about the racial identity of their respondents.8,17,20,21 This lack of diversity within the samples represents a missed opportunity to investigate the potential impact of systemic racial biases, both in society and within healthcare systems, on CF, CS, and burnout. Understanding the factors contributing to CF, CS, and burnout is essential for providing optimal support to nurses and enhancing their capacity to find fulfillment in their careers, ultimately reducing nurse turnover and increasing patient satisfaction.
Conceptual Framework
Several significant frameworks have played a pivotal role in shaping research endeavors related to CF, CS, and burnout. Notable among these are Watson’s theory of human caring and Maslow’s hierarchy of needs.22 However, the stress process model stands out as one of the most crucial theoretical frameworks that has greatly informed this area of study.23 The stress process model illustrates CF as an outcome arising from the innate empathy of caregivers, coupled with their exposure to the traumatic experiences of their patients. Building upon this model, Stamm24 further integrated it into the development of the Professional Quality of Life (ProQOL) scale.24 The CS–CF model presented in this context represents a theoretical path analysis, elucidating the positive outcomes of CS and the negative outcomes of CF that can emerge from assisting individuals affected by traumatic stress.2
Stamm24 proposed the ProQOL framework in order to explain the consequences of working as a “helper” to traumatized individuals. The term “helper” refers to nurses, trauma therapists, psychologists, social workers, and other professionals who have been trained to work with traumatized victims. In this framework, two broad overarching concepts, CF and CS, are used to explain the work realities of caregivers. This framework divides CF symptoms into two categories: job burnout and STS. Stamm24 defines burnout as persistent feelings of hopelessness and exhaustion that impair one’s ability to perform effectively at work. Burnout symptoms include “emotional exhaustion”, “depersonalization”, and “personal accomplishment”, and dissatisfied with one’s job. Workers suffering from STS are said to be “preoccupied with thoughts of people they have helped”. Caregivers describe “emotional exhaustion”, “depersonalization”, and “infected” “by the trauma of others”. Fear, difficulty sleeping, intrusive images, and avoidance of traumatic narratives are all symptoms of STS. Stamm believes that STS and burnout are two separate but related concepts: “[they] both measure negative affect but are clearly different; the burnout scale does not address fear while the secondary traumatic stress does” (pp. 13–14). (See Figure 1 for graphical depictions of ProQOL model).
 |
Figure 1 ProQOL Model: Burnout and Secondary Traumatic Stress are distinct but correlated factors in Compassion Fatigue. |
In designing this study, we used Stamm24 model as a guiding framework to understand the interactions between CS, CF, and burnout in nurses. The underlying prediction is that both individual and organizational factors impact and result in CS, CF, and burnout in nurses. In line with the literature, we identified several variables of interest, such as weekly work hours, specialty, years of experience, and possession of a certification in a specialty. The dependent variables included CS, CF, and burnout. Additionally, we collected demographic data.
Materials and Methods
Sampling and Demographics
This cross-sectional and descriptive study employed a one-time survey conducted at a specific point in time between July and August 2023 that targeted nurses at medical city in Riyadh City. The healthcare provider concerned operated medical city with 1,200 licensed beds and multiple specialist provisions. The questionnaire was distributed to all RNs within the medical city, excluding technicians and licensed practical nurses. A sample size estimation was not conducted before the participants were recruited. Out of the 300 nurses initially contacted to participate in the study, 177 completed the survey, representing 59%. The sample size was 177.
Data Collection Procedure
Before data collection commenced, we sought approval from the King Saud University institutional review boards for the medical city (IRB no. 23-708). The questionnaire was then sent via email to 300 nursing staff working at the relevant medical institutions. The communication included a study summary, a clause stating that clicking on the link to the survey implies consent, primary researcher contact details, and the survey link. The questionnaire incorporated the ProQOL 5 scale and demographic questions. To boost the response rate, two weeks after the initial email, the participants received a follow-up email. The privacy and anonymity of the participants was maintained throughout the research by ensuring that no information that could identify the respondents was linked to the survey responses. Each participant signed an online informed consent form after reading the investigation’s purpose statement. This research followed the guidelines outlined in the Helsinki Declaration. A set of demographic elements devised by the research team, these demographic questions gathered concerning the nurses’ education level, years of experience, hours worked per week, specialty, certification status, age, and gender.
Instrument
The tool employed in this study consisted of the Arabic version of the ProQOL 5.25 The ProQOL 5 applied in this research was a 30-item self-administered tool containing three subscales, CS, CF, and Burnout, of which items 1, 4, 15, 17, and 29 were reverse-scored. Every subscale had 10 questions and used five-point Likert scale response set ranging from 1 = never to 5 = very often. The ProQOL 5 results for each subscale indicated the respondents’ levels of CS, CF, and Burnout. Each subscale’s scores ranged from 10 to 50. A CS score of 22 or below signified low levels of CS, a score of 23–41 denoted average levels of CS, and a CS score of 42 and above suggested high levels of CS. For CF and Burnout, a score of 22 or lower indicated low levels of CF and Burnout, a score of 23–41 signified average levels of CF and Burnout, and a score of 42 and above implied high levels of CF and Burnout.25
Stamm24 established the construct validity and reliability of the ProQOL scale. Utilizing analyses of both convergent and discriminant validity, it was convincingly demonstrated that each of the scales within the ProQOL measures unique and separate constructs. Each individual subscale operates independently, and therefore, it is not advisable to aggregate the scores from these subscales into a single composite score. Moreover, the results of psychometric assessments affirmed the robust internal consistency of the ProQOL’s three subscales, characterized by Cronbach’s α reliability coefficients ranging from 0.84 to 0.90. In the context of this specific study, the Cronbach’s α for the Arabic version of ProQOL 5 were as follows: 0.68 for the overall scale, 0.88 for the CS subscale, 0.85 for the CF subscale, and 0.76 for the Burnout subscale.
Data Analysis
The data collected from the ProQOL 5 survey underwent analysis using the Statistical Package for the Social Sciences (SPSS) version 28.0. Initially, univariate analyses were conducted on both the demographic variables and the ProQOL 5 subscales to construct a comprehensive profile of the study participants. Subsequently, bivariable analyses were performed to explore potential associations between predictor and outcome variables. Furthermore, a series of statistical tests, including Pearson’s correlation coefficient, t-tests, and one-way analysis of variance (ANOVA), were carried out to investigate the relationships between predictor variables such as weekly working hours, nursing specialty, years of experience, and the presence of certification, and their impact on CS, CF, and burnout. Prior to the analysis, two of the independent variables, weekly hours and nursing specialty, were subjected to recoding. Specifically, the predictor variable of weekly hours, which was initially treated as an interval variable, was recategorized into a categorical variable.
The recoded weekly hours variable comprised three categories: 35 hours or less per week, 36–40 hours per week, and 41 or more hours per week. The categories for nursing specialty included (a) critical care, (b) surgical services, (c) emergency department, (d) inpatient noncritical, and (e) pediatrics. Post hoc tests Tukey HSD and LSD were conducted once the statistically significant results between the groups were identified.
Results
Demographic Characteristics
The study included 177 nurses from medical city in Riyadh City. The mean age of the participants was 30.34, with a 5.90 standard deviation. On average, the participants had 6 years of professional nursing experience. Most of the respondents (53.7%) were female, indicating a slightly higher representation of women in the study. Regarding educational attainment, a significant ratio of the participants were educated to the held bachelor’s level in nursing. A little over 10% had an associate degree, while 6.2% and 1.1% mentioned holding a master’s or PhD, respectively.
The participants’ nursing specializations were uniformly distributed across various groups. Notably, 19.8% of participants and 41% of nurses employed in inpatient noncritical services reported providing surgical services. Additionally, 15.3% of nurses mentioned working in both emergency rooms and critical care units. A smaller proportion (7.9%) of interviewees reported employment in the field of pediatrics, which was less common. The vast majority of nurses (59.9%) reported working at least 41 hours per week. A smaller percentage (5.6%) indicated working 35 hours a week or less, while 34.5% reported working 36 to 40 hours a week. The demographics of the nurses who participated are summarized in Table 1.
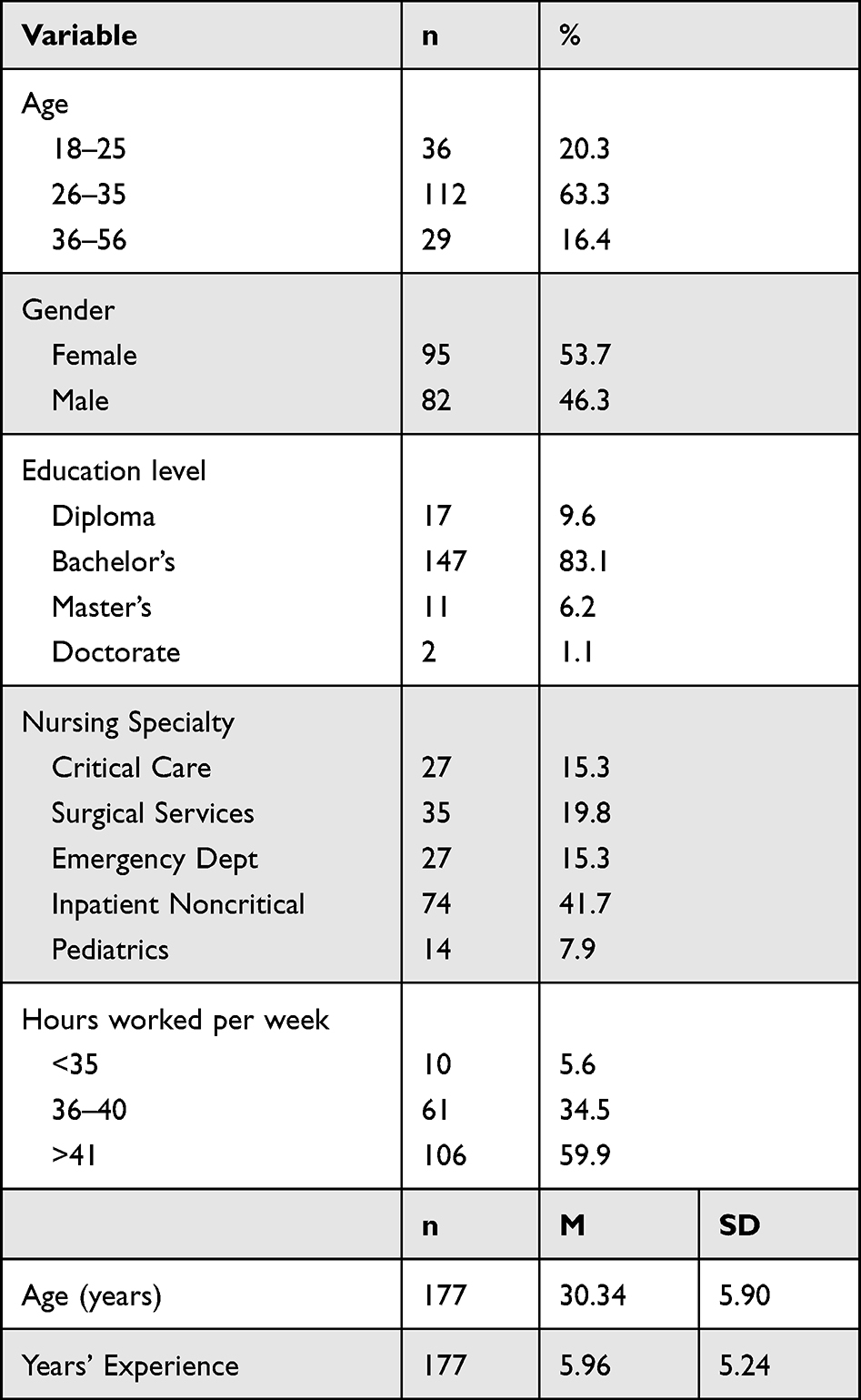 |
Table 1 Descriptive Analysis of Demographic Variables of Study |
Incidence Rates of CS, CF, and Burnout
The ProQOL 5 subscales, CS, CF, and Burnout, demonstrated relatively an average mean values in this study of nurses. The dependent variables underwent a skewness test, revealing distinct patterns in their data distribution. Burnout exhibited the most even distribution (skewness=0.194, SE=0.173), while CF showed moderate skewness (skewness=0.382, SE=0.13), and CS was extremely skewed (skewness=−0.640, SE=0.13). Table 2 provides a summary of the mean data for the subscales, showcasing that respondents scored highly or average on the CS scale, low/average on the CF scale, and low to average on the Burnout scale.
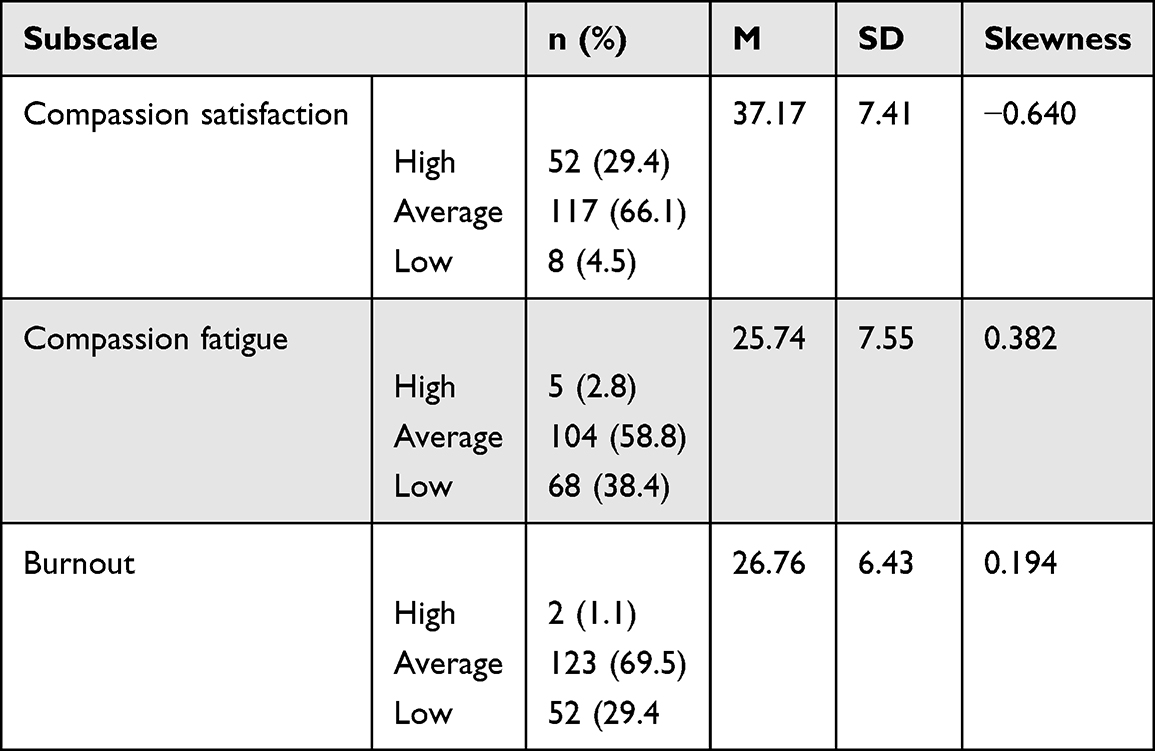 |
Table 2 Summary of Levels of Compassion Satisfaction, Compassion Fatigue, and Burnout Among Nurses (N=177) |
Examination of Job-Related Factors and Their Impact on CS, CF, and Burnout
The study aimed to explore the potential associations between work-related factors, including hours worked, nursing specialty, age group, and nursing qualification, and levels of CS, CF, and Burnout within a population of nurses. To investigate these relationships, one-way ANOVAs were conducted for hours worked, age, and nursing specialty, while an independent samples t-test was employed for nursing qualification.
Hours of Work, Specialty, Certification, and Age
The one-way ANOVAs outcomes reveal that there is no statistically significant correlation between the number of hours worked and the levels of CS, CF, or Burnout (p=0.643, p=0.287, and p=0.655, respectively). Similarly, the analysis using one-way ANOVAs to compare nursing specialties with CS, CF, and Burnout revealed no statistically significant differences among the groups (p=0.114, p=0.082, and p=0.057, respectively). Regarding nursing qualification, an independent samples t-test was conducted to explore its association with CS, CF, and Burnout. The findings indicate that there is no statistically significant correlation between nurses’ professional certification status and their experiences with CS, CF, or Burnout (p=0.186, p=0.486, and p=0.056, respectively). The t-test analysis of professional certification by CS, CF, and Burnout is presented in Table 3.
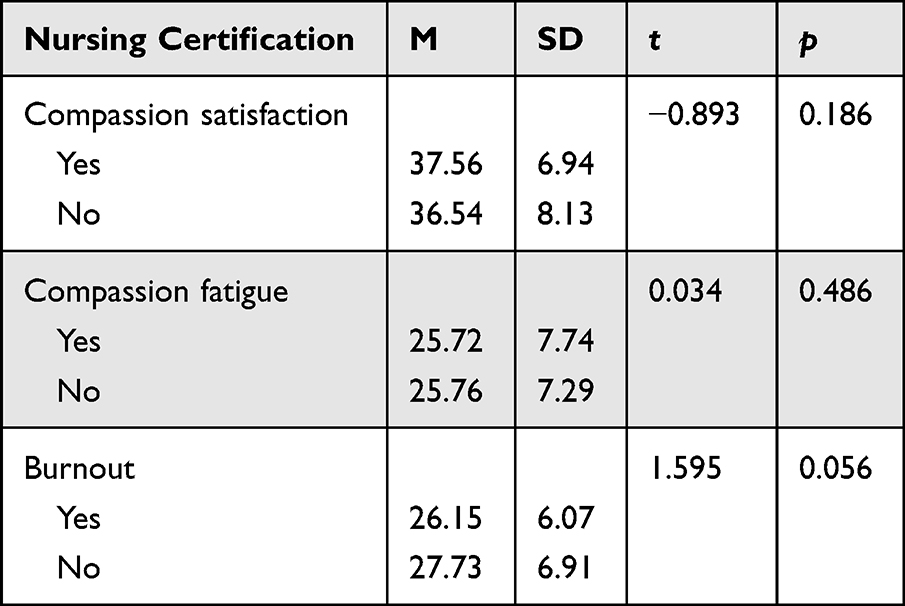 |
Table 3 Independent t-Test of Professional Certification and Compassion Satisfaction, Compassion Fatigue, and Burnout |
Nonetheless, the outcomes from the ANOVA assessing age group’s influence on CS, CF, and Burnout reveal a statistically significant disparity among the age groups concerning Burnout (p=0.016). To pinpoint the specific significant differences within age group categories and Burnout, the Tukey HSD test was employed. The Tukey HSD analysis highlights that nurses aged between 18–25 experienced significantly higher levels of Burnout compared to those aged between 26–35 (p=0.041) and those between 36–56 (p=0.020). Tables 4, which present the ANOVA results pertaining to age group and Burnout.
 |
Table 4 One-Way Analysis of Variance of Age Group by Burnout |
Discussion
Incidence Rates of CS, CF, and Burnout
In the current study, a total of 177 participating nurses reported experiencing low to average levels of CF and burnout, while their CS ranged from average to high. These findings align with a similar small-scale study conducted by Fleming, Mazzatta,26 involving 49 nurses, which also found high CS and low CF and burnout levels. The latter study suggested that providing nurses with training, resources, and support for self-care can enhance job satisfaction and reduce CF.26
Interestingly, in the current study, factors such as hours worked and nursing specialty did not appear to significantly influence nurses’ experiences of CF or CS. These findings contrast with a study conducted by Hunsaker, Chen2 but are consistent with other research indicating that nurses often struggle with high rates of CF and burnout.1,17 Furthermore, it is noteworthy that in the present study, nurses who held professional certification reported higher levels of CS compared to their counterparts without such certification.
Work-Related Attributes and CF, CS, and Burnout
Age
The findings from our study align with previous research concerning the correlation among age group and CF, CS, and burnout between nurses.3,8,16 Notably, nurses between the ages of 18 and 25 exhibited higher levels of burnout compared to those aged between 26 and 35 and those between 36 and 56. This observation is crucial, as nurses are often relied on to work extra shifts to fill schedule gaps and increase pay. However, our data suggests that doing so may have adverse effects on nurses’ mental health, job satisfaction, and overall well-being.
Years of Experience and Certification
Our research revealed a positive relationship between CS and lower CF with years of experience, although this relationship was not of statistical significance. This finding diverges from earlier research, which found that nurses with more than ten years of experience tended to have higher CS and lower CF levels than those with less than ten years of experience.17,19 Kolthoff and Hickman6 proposed that less-experienced professionals could lack a robust peer support system, which could impact their ability to cope with CF and maintain a healthy work-life balance, a crucial component of CS.
In addition to experience, we investigated nurses with certifications in their specific fields of expertise. Interestingly, our study found no statistically significant difference in CS, CF, and Burnout ratings between nurses with professional qualifications and those without. The lack of research on this topic in the literature makes this result intriguing, warranting further investigation. Additionally, we explored whether certified nurses worked longer hours than non-certified nurses, but our data did not support such a relationship. Overall, our research further informs existing understanding and underscores the importance of understanding how age, experience, and certifications influence nurses’ experiences of CF, CS, and burnout. These insights could facilitate the development of specific mediations and support mechanisms to improve nurses’ well-being and job satisfaction in the healthcare setting.
Study Limitations, Recommendations, and Future Research Directions
Limitations exist in this study that necessitate caution in interpreting the results. One notable limitation is that the measurement of CS, CF, and burnout was conducted during a specific time period, which may not fully capture the dynamic nature of these constructs. Nurses’ perceptions can be influenced by various work-related variables that were excluded from the current study.
Additionally, the low rate of response for the ProQOL 5 administration (59% of invited nurses) raises concerns about the sample’s representativeness and generalizability. Furthermore, some respondents did not fully complete the questionnaire, leading to missing data and difficulty in establishing a complete profile of the participating nurses.
Another constraint is the timing of the investigation, which occurred after the COVID-19 epidemic. The healthcare industry has undergone significant transformation during this period, and early studies suggest an increase in CF and burnout among nursing staff. This evolving context underscores the importance of addressing CF, CS, and burnout in nurses, necessitating attention and preventive measures. Promoting self-care, awareness, and education are essential components in CF prevention, given the hectic healthcare environment where medical professionals often neglect their well-being. Integrating these aspects into the organizational structure can be beneficial for the healthcare context.
Hospital settings may foster a “tough” environment, leading staff to hesitate in acknowledging the impact of patient trauma on their mental well-being. Addressing organizational structures and implementing changes are common strategies for preventing burnout. In pursuit of greater job contentment and higher-quality patient care, nurse managers propose further strategies such as diversifying caseloads, providing mentorship to maintain professional distance in patient care, offering end-to-end self-care activities in the professional setting, and supporting human development through the organizational structure. Future research could explore the relationship between certification and CF and investigate how the number of hours worked relates to CF, CS, and burnout. Topics such as floor staff’s ability to effect change within their units, staffing ratios, and management warrant further investigation to deepen our understanding of nurses’ experiences. Qualitative approaches like focus groups and interviews may provide a more comprehensive understanding.
Conclusion
The study suggests that nursing staff in the medical city tended towards higher/average CS and lower/average CF/burnout. Younger nurses (ages 18–25) experienced higher levels of CF/burnout compared to older counterparts. Multiple variables, including length of experience, age, and professional qualifications, appear to influence nurses’ CF and CS experience. Interestingly, nurses in certain age groups and with less experience are more likely to experience burnout, while professional qualification appear to protect against negative outcomes to some extent.
Notably, the study was conducted in the middle of 2023, and the COVID-19 pandemic subsequently impacted the healthcare system, potentially affecting current CF, CS, and burnout levels. Repeating this analysis after the pandemic could provide valuable insights to the medical community.
Acknowledgments
All authors of this study extend their appreciation to the Researchers Supporting Project Number (RSPD2023R880), King Saud University, Riyadh, Saudi Arabia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hooper C, Craig J, Janvrin DR, et al. Compassion satisfaction, burnout, and compassion fatigue among emergency nurses compared with nurses in other selected inpatient specialties. J Emerg Nurs. 2010;36:420–427. doi:10.1016/j.jen.2009.11.027
2. Hunsaker S, Chen HC, Maughan D, et al. Factors that influence the development of compassion fatigue, burnout, and compassion satisfaction in emergency department nurses. J Nurs Scholarsh. 2015;47(2):186–194. doi:10.1111/jnu.12122
3. Sinclair S, Raffin-Bouchal S, Venturato L, et al. Compassion fatigue: a meta-narrative review of the healthcare literature. Int J Nurs Stud. 2017;69:9–24. doi:10.1016/j.ijnurstu.2017.01.003
4. Todaro-Franceschi V. Compassion Fatigue and Burnout in Nursing: Enhancing Professional Quality of Life. Springer Publishing Company; 2019.
5. Stamm BH. The proqol manual: the professional quality of life scale: compassion satisfaction, burnout & compassion fatigue/secondary trauma scales; 2005. Available from:https://proqol.org/proqol-manual.
6. Kolthoff KL, Hickman SE. Compassion fatigue among nurses working with older adults. Geriatr Nurs. 2017;38(2):106–109. doi:10.1016/j.gerinurse.2016.08.003
7. Joinson C. Coping with compassion fatigue. Nursing. 1992;22(5):118–119.
8. Yoder EA. Compassion fatigue in nurses. Appl Nurs Res. 2010;23(4):191–197. doi:10.1016/j.apnr.2008.09.003
9. Alsadaan N, Jones LK, Kimpton A, et al. Challenges facing the nursing profession in Saudi Arabia: an integrative review. Nurs Rep. 2021;11(2):395–403. doi:10.3390/nursrep11020038
10. Alharbi J, Wilson R, Woods C, et al. The factors influencing burnout and job satisfaction among critical care nurses: a study of Saudi critical care nurses. J Nurs Manag. 2016;24(6):708–717. doi:10.1111/jonm.12386
11. Saati H. Compassion fatigue, satisfaction and burnout among oncology nurses working in pediatric oncology setting. Biosc Biotech Res Comm. 2020;13(3):1314–1320. doi:10.21786/bbrc/13.3/50
12. Qedair JT, Balubaid R, Almadani R, et al. Prevalence and factors associated with burnout among nurses in Jeddah: a single-institution cross-sectional study. BMC Nurs. 2022;21(1):287. doi:10.1186/s12912-022-01070-2
13. Alqahtani R, Al-Otaibi S, Zafar M. Burnout syndrome among nurses in a psychiatric hospital in Dammam, Saudi Arabia. Nurs Midwifery Stud. 2020;9(2):110. (). doi:10.4103/nms.nms_126_19
14. Shahin MA, Al-Dubai SAR, Abdoh DS, et al. Burnout among nurses working in the primary health care centers in Saudi Arabia, a multicenter study. AIMS Public Health. 2020;7(4):844–853. doi:10.3934/publichealth.2020065
15. Stamm B. Secondary Traumatic Stress: Self-Care Issues for Clinicians, Researchers, and Educators. The Sidran Press; 1995.
16. Shah MK, Gandrakota N, Cimiotti JP, et al. Prevalence of and Factors associated with nurse burnout in the US. JAMA Network Open. 2021;4(2):e2036469–e2036469. doi:10.1001/jamanetworkopen.2020.36469
17. Al-Majid S, Carlson N, Kiyohara M, et al. Assessing the degree of compassion satisfaction and compassion fatigue among critical care, oncology, and charge nurses. J Nurs Adm. 2018;48(6):310–315. doi:10.1097/nna.0000000000000620
18. Sun T, Huang X-H, Zhang S-E, et al. Fatigue as a cause of professional dissatisfaction among Chinese nurses in intensive care unit during COVID-19 pandemic. Risk Manag Healthc Policy. 2023;16:817–831. doi:10.2147/RMHP.S391336
19. Berger J, Polivka B, Smoot EA, et al. Compassion fatigue in pediatric nurses. J Pediatric Nurs. 2015;30(6):e11–17. doi:10.1016/j.pedn.2015.02.005
20. Mooney C, Fetter K, Gross BW, et al. A preliminary analysis of compassion satisfaction and compassion fatigue with considerations for nursing unit specialization and demographic factors. J Trauma Nurs. 2017;24(3):158–163. doi:10.1097/jtn.0000000000000284
21. Wu J, Zhang C, He F, et al. Factors affecting intention to leave among ICU healthcare professionals in China: insights from a cross-sectional survey and xgboost analysis. Risk Manag Health Policy. 2023;16:2543–2553. doi:10.2147/rmhp.S432847
22. Burtson PL, Stichler JF. Nursing work environment and nurse caring: relationship among motivational factors. J adv Nurs. 2010;66(8):1819–1831. doi:10.1111/j.1365-2648.2010.05336.x
23. Figley CR. Compassion fatigue: psychotherapists’ chronic lack of self care. J Clin Psychol. 2002;58(11):1433–1441. doi:10.1002/jclp.10090
24. Stamm B The concise manual for the professional quality of life scale; 2010. Available from: https://proqol.org/proqol-manual.
25. Center for Victims of Torture. ProQOL measure. Available from: www.ProQOL.org.
26. Fleming K, Mazzatta GR, Matarese K, et al. Compassion fatigue and the ART model. Nursing. 2020;50(3):58–61. doi:10.1097/01.NURSE.0000654168.38494.dd
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.