")
Back to Journals » Patient Preference and Adherence » Volume 17
Predictors of Cardiovascular Morbidity Among Adult Hypertensive Patients: A Cross-Sectional Study from the Kingdom of Saudi Arabia
Authors Al-Ghamdi S, Aldosari KH, Hussain ABO
Received 2 March 2023
Accepted for publication 23 May 2023
Published 6 June 2023 Volume 2023:17 Pages 1361—1369
DOI https://doi.org/10.2147/PPA.S407546
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Sameer Al-Ghamdi,1 Khalid Hadi Aldosari,2 Abo Baker Omar Hussain3
1Department of Family and Community Medicine, College of Medicine, Prince Sattam bin Abdulaziz University, Al Kharj, Saudi Arabia; 2Adult Critical Care Medicine Department, Security Forces Hospital Program, Riyadh, Saudi Arabia; 3Department of Internal Medicine, College of Medicine, Prince Sattam bin Abdulaziz University, Al Kharj, Saudi Arabia
Correspondence: Sameer Al-Ghamdi, Department of Family and Community Medicine, College of Medicine, Prince Sattam bin Abdulaziz University, Al Kharj, 11942, Saudi Arabia, Email [email protected]
Background: Hypertension is a public health issue affecting over a billion people globally. 15% of the adults in the Kingdom of Saudi Arabia (KSA) are thought to have hypertension. A large proportion of them remain undiagnosed or are sub-optimally treated. Those with inadequately treated hypertension have a high risk of life-threatening cardiovascular complications such as ischemic heart disease, left ventricular hypertrophy and heart failure. This study was undertaken to elucidate the cardiovascular morbidity seen in a sample of adult hypertensive patients in Saudi Arabia and identify key demographic and clinical factors associated with cardiovascular morbidity.
Methods: A multicentric cross-sectional study was conducted from November 2019 to November 2021 at three hospitals in Al-Kharj KSA. Totally, 105 adult patients with a documented history of primary hypertension for at least 5 years irrespective of treatment status presenting themselves to the study sites were included. Patients with secondary hypertension, and those without confirmed cause and duration of hypertension were excluded. Logistic regression analysis was performed to determine the factors associated with cardiovascular morbidity.
Results: The study included 105 participants aged 47.75± 13.46 years. 50 (47.6%) were males and 62 (59%) were not Saudis. Left Ventricular Hypertrophy, 64 (61%), diastolic dysfunction, 44 (41.9%), and retinopathy, 33 (31.4%) were the most frequently observed morbidities. Participants aged over 45, those with diabetes, or those with dyslipidemia were more likely to have cardiovascular morbidities (adjusted odds ratio (AOR)): 4.01 (1.29– 12.46), p = 0.016, AOR: 6.4 (1.62– 25.28), p = 0.008, and AOR: 6.71 (1.46– 30.83), p = 0.014, respectively.
Conclusion: Older age, the presence of comorbid diabetes mellitus, and dyslipidemia are associated with a higher likelihood of cardiovascular morbidity in hypertensive patients of Saudi Arabia.
Keywords: mortality, morbidity, hypertension, case–control study, Saudi Arabia
Background
Hypertension, characterized by persistently high blood pressure, is an important public health issue that affects 1.13 billion people globally and is responsible for seven million deaths every year.1 Hypertension is regarded as a “silent killer” as hypertensive patients have a higher risk of life-threatening cardiovascular diseases (CVD) such as ischemic heart disease, stroke, peripheral vascular disease, heart arrhythmias and heart failure.2 Essential hypertension, responsible for 90–95% of all cases of hypertension, is defined as persistently elevated blood pressure, ≥140/90 mmHg, with no secondary cause identified.2 The remaining 5–10% of cases of hypertension are secondary to other diseases such as renal diseases, hyperaldosteronism, Cushing syndrome, thyroid disease, coarctation of aorta, obstructive sleep apnea, pheochromocytoma, pregnancy, and certain drugs such as nonsteroidal anti-inflammatory drugs (NSAIDs) and sodium containing antacids.3
Globally, the prevalence of hypertension in adults is 30–35% with a higher prevalence in men than in women.4 In a 2013 national survey of hypertension conducted in the Kingdom of Saudi Arabia, the prevalence of hypertension among those >15 years was 15.2% and the prevalence of borderline hypertension (defined as systolic blood pressure >120 and <139mmHg and a diastolic blood pressure >80 and <90mmHg) was 40.6%.5 Among those with hypertension, 61.2% of the men and 52.9% of the women not been previously diagnosed with hypertension and 25.6% of those with hypertension were receiving no treatment or sub-optimal treatment.5–7 The high and rising prevalence of hypertension among the Saudi population along with the high prevalence of undiagnosed and undertreated hypertension in Saudi Arabia has contributed towards the high and rising rates of cardiovascular disease, the most common cause of death in Saudi Arabia.8
Studies have shown a continuous relationship between blood pressure measurements and cardiovascular morbidity in all ages and ethnic groups.9,10 Above the age of 50 years, high systolic blood pressure, and high pulse pressure has an additional prognostic role in determining cardiovascular risk.11,12 Patients with other risk factors such as smoking, dyslipidemia, kidney disease and diabetes in addition to carrying a higher cardiovascular risk, are more likely to have severe and treatment resistant hypertension.13 Individuals with increased fibrinogen, apolipoprotein B, lipoprotein(a) levels, high sensitivity C-reactive protein, sedentary lifestyles, central obesity, and those with a family history of premature cardiovascular disease are also more likely to have higher cardiovascular morbidity.14 Lastly, socio-economic deprivation and certain ethnic minorities also carry a higher cardiovascular risk.15 While clinical and socio-demographic predictors of cardiovascular morbidity among hypertensive patients have received a lot of scientific attention worldwide, the predictors of cardiovascular morbidity specific to the Saudi population have not been previously studied.
Understanding the of predictors of cardiovascular morbidity among hypertensive patients will help Saudi clinicians to better establish the cardiovascular risk status of their patients and take early and effective preventative steps to prevent cardiovascular morbidity. Our work will also enable policy makers to identify populations at high risk of cardiovascular disease and make changes in clinical and public health policy to address this risk.
Our study aims to identify the prevalence and key predictors of cardiovascular morbidity among hypertensive patients in the Kingdom of Saudi Arabia.
Our objectives are
- To estimate the prevalence of cardiovascular morbidity among hypertensive patients visiting 3 major hospitals in Riyadh, Kingdom of Saudi Arabia.
- To identify key socio-demographic and clinical predictors of cardiovascular morbidity among hypertensive patients.
Methods
Design of the Study
This cross-sectional study was carried out from November 2019 to November 2021 wherein demographic parameters with clinical parameters and lab test results of the patients were studied to identify the key factors associated with cardiovascular morbidity observed in the study population.
Study Population
Based on past literature, assuming 61.9% of the study population to have cardiovascular morbidity, a sample size was calculated to achieve 95% confidence and 80% power with a 10% margin of error.16 105 participants were recruited from the general family medicine and cardiovascular medicine departments of the King Khalid Hospital and the Prince Sultan Center for Health Services, Prince Sattam Bin Abdulaziz University hospital in Al Kharj, and the Al Kharj Military Industries Corporation hospitals - three major hospitals in the Kingdom of Saudi Arabia. Enrolment of participants in the study was subject to strict predetermined inclusion and exclusion criteria. The inclusion criteria were adult patients of any age and either gender who were residents of the Kingdom of Saudi Arabia capable and willing to give their informed consent with clinically diagnosed histories of primary hypertension for at least 5 years irrespective of treatment status who presented themselves to the study sites during the study. Excluded from the study were those unable or unwilling to provide consent to participate in the study, patients with secondary hypertension, and those in whom the duration and cause of hypertension could not be confirmed due lack of access to older medical records. Duration of hypertension and cause of were confirmed by perusal of older medical records.
Once the participants gave their informed consent and were enrolled in the study, their demographic details were collected by the physician. Medical, laboratory, and other data of the participants were obtained manually from the electronic health records. Clinical examination (general physical examination and fundus examination), blood pressure measurements, laboratory tests (uric acid, lipid profile, and sugar levels), and other radiological tests (echocardiography) were recorded. Blood pressure was measured using calibrated sphygmomanometer, and the averages of three separated measurements of systolic blood pressure (SBP) and diastolic blood pressure (DBP) calculated and recorded as SBP and DBP of each patient.17 Hypertension severity was defined as American College of Cardiology (ACC) and American Heart Association (AHA) criteria; which 130 ≤ SBP < 140 or 80 ≤ DBP < 90 considered as stage 1 (mild), 140 ≤ SBP ≤ 180 or 90 ≤ DBP ≤ 120 considered as stage 2 (moderate), and 180 < SBP and/or 120 < DBP considered as stage 3 (severe).17 Obesity was defined as per the World Health Organization criteria as having a body mass index (BMI) greater than or equal to 30 kg/m2.18 Those with glucose levels >200 mg/dL or HbA1c ≥6.5% or a documented history of type 2 diabetes mellitus were classified as diabetic. Similarly, those with total cholesterol >200 mg/dL, LDL-C ≥130 mg/dL or HDL <40 mg/dL or those with a documented history of dyslipidemia were regarded as having dyslipidemia.19 High uric acid defined as level greater than 5.5 milligram per deciliter in serum.20 We noted details about patient morbidities specifically hypertensive complications, namely ischemic heart disease (IHD), transient ischemic attack (TIA), stroke, heart failure, retinopathy, and renal impairment which were identified by checking the history of patients through their electronic health records. Left ventricular hypertrophy, diastolic dysfunction, and abnormal wall motion retrieved from echocardiography records. The study was granted ethical approval by the institutional review boards of Prince Sattam bin Abdulaziz university prior to data collection with ethics clearance no - IF-PSAU-2021/03/18253.
Data Analysis
The data obtained in the study were anonymized, tabulated, and analyzed by using the Statistical Package for Social Services version 20. Less than 1% of the data was missing, which was considered negligible. Descriptive statistics were computed for all study variables. Quantitative variables were summarized with mean and standard deviation. Qualitative variables are presented as frequency and percentages. Regarding analysis, Independent variables were considered as demographic attributes (age and gender), obesity, high uric acid, diabetes mellitus, dyslipidemia, smoking, severity of hypertension, renal impairment, and retinopathy, while cardiac morbidity was the outcome of interest defined as patients with history of one or more of the following - left ventricular hypertrophy, diastolic dysfunction, heart failure, abnormal wall motion, stroke, transient ischemic attack and ischemic heart disease. Univariable and multivariable binary logistic regression were carried out to assess the association between cardiac morbidity and associated factors. The significant variables in univariate analysis were included for multivariate analysis. Odd ratios were calculated with a 95% confidence interval. The significance level was set at <0.25 for univariate analysis and <0.05 for multivariate analysis.
Results
We included 105 participants aged 47.75±13.46 years. 57.6% were males and 59% were not Saudis. The majority, 79%, were obese with a BMI of 33.89±7.31kg/m2 and had stage 1 or 2 hypertension, 97.1%. The demographic characteristics of the study participants are in Table 1.
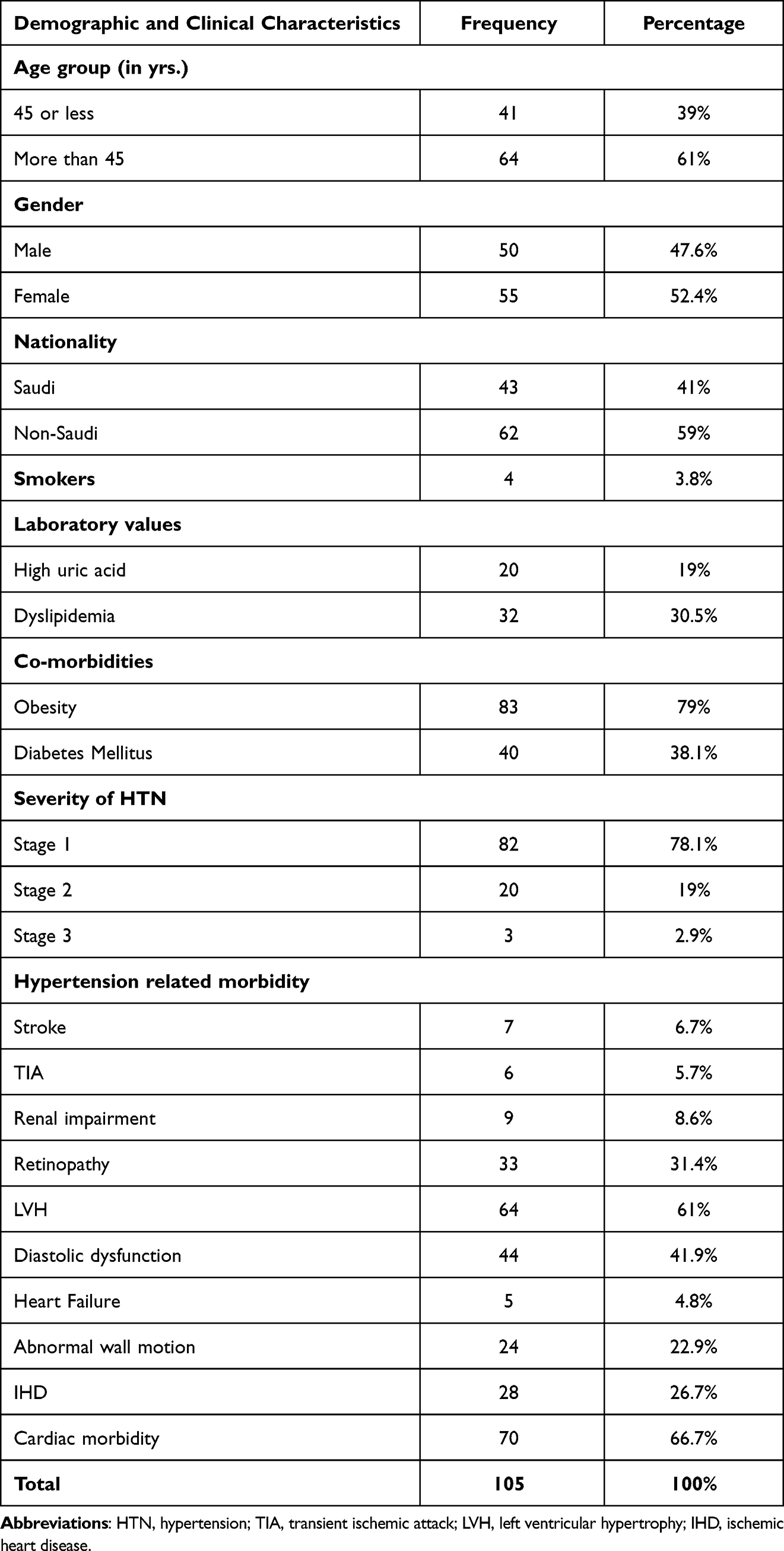 |
Table 1 Demographic and Clinical Characteristics of Hypertensive Patients |
66.7% of participants had a history of cardiovascular morbidity. The morbidity observed in the study population is summarized in Table 1. Left Ventricular Hypertrophy (LVH), 61%, diastolic dysfunction, 41.9%, and retinopathy, 31.4% were the most frequently observed morbidities.
The association of experiencing cardiac morbidity with various patient demographic and clinical parameters was modelled using univariable and multivariable binary logistic regression models (Refer Table 2 and Table 3). The final model included 7 covariates of which 3 were significant. Participants aged over 45 were 4-times more likely to have cardiac morbidity (adjusted odds ratio (AOR): 4.01 (1.29–12.46)), p = 0.016, with 84.4% of those over 45 experiencing cardiac morbidity compared to the 39% among those aged 45 or less. Participants with diabetes mellitus were 6.4-times more likely to have cardiac morbidity (AOR: 6.4 (1.62–25.28)), p = 0.008, with 90% of patients with diabetes experiencing 1 cardiac event compared to the 52.3% of the participants without diabetes. Participants with dyslipidemia were 6.71-times more likely to have cardiac morbidity, (AOR: 6.71 (1.46–30.83)), p = 0.014, with 90.6% of patients with dyslipidemia experiencing cardiac morbidity compared to the 56.2% of participants without dyslipidemia.
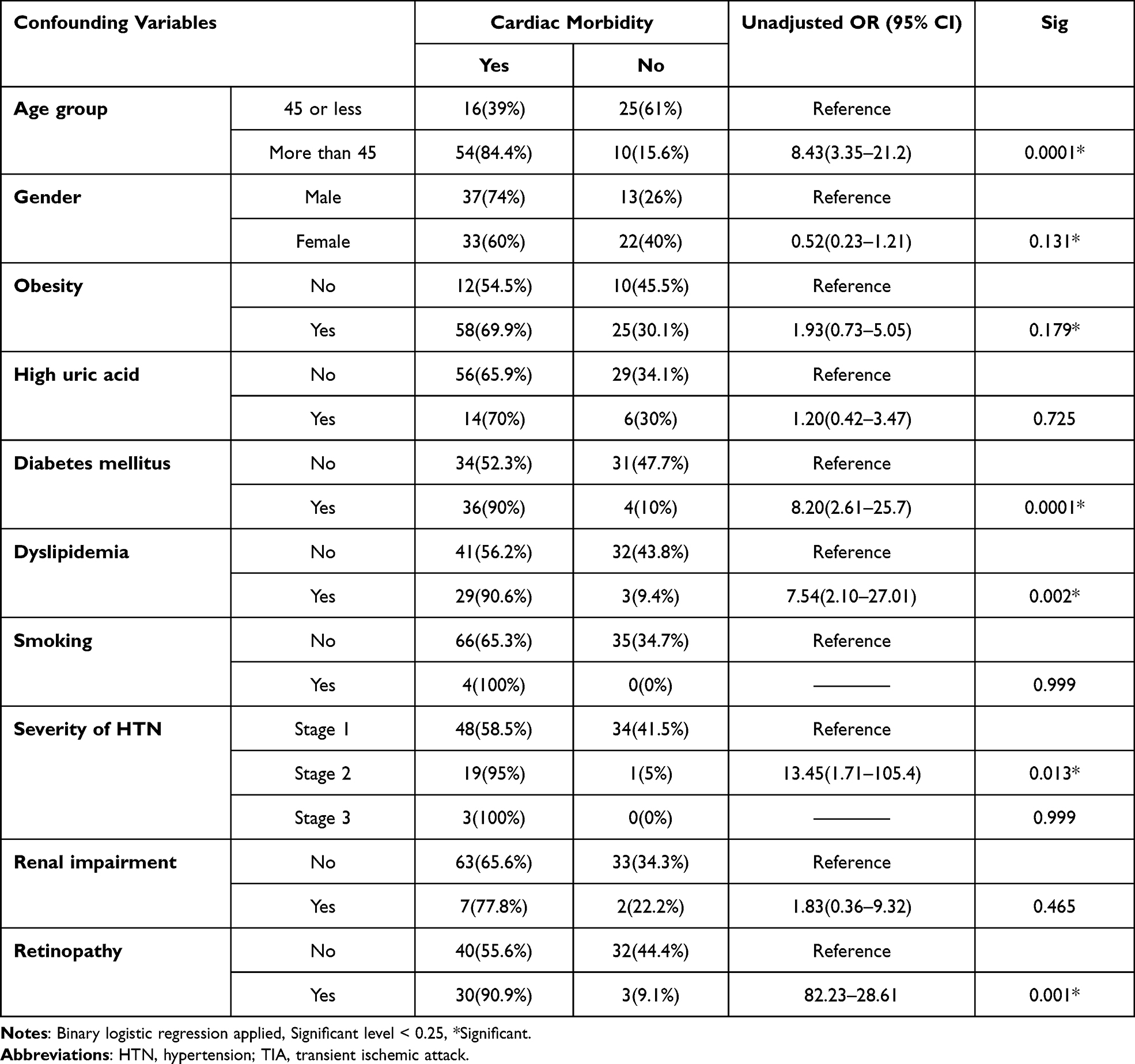 |
Table 2 Association of Cardiac Morbidity with Clinical and Demographic Factors in Hypertensive Patients |
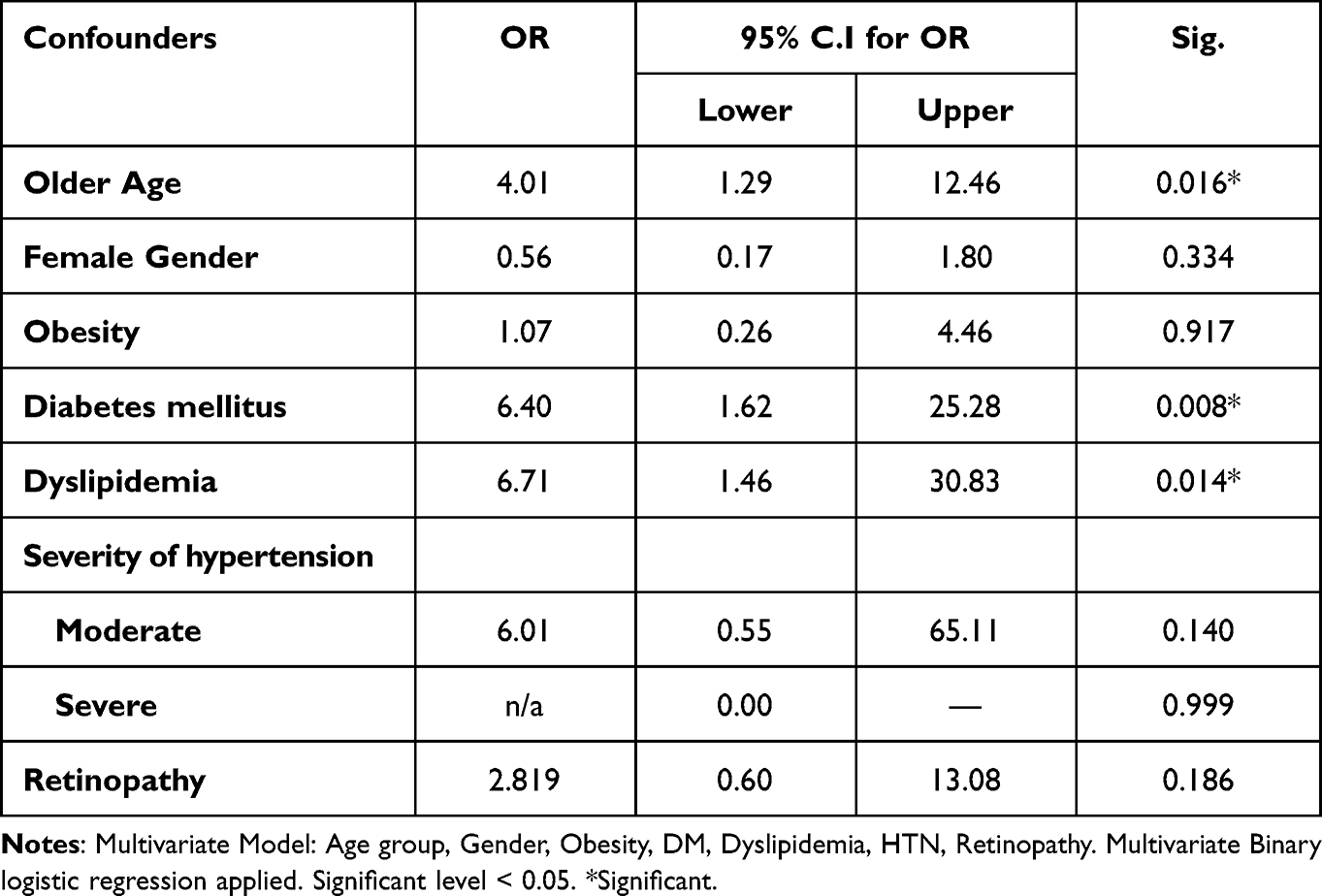 |
Table 3 Multivariate Logistic Regression |
Discussion
Our study showed 66.7% of hypertensive patients suffer from cardiac morbidity. Cardiovascular morbidity was the leading cause of disability and mortality during 2010–2017 In Saudi Arabia.21 Furthermore, The Kingdom of Saudi Arabia has a very high occurrence of hypertension, and this has been increasing over the last 3 decades, from about 10% in 2010 to nearly 26% in 2016.22–24 Despite high occurrence of hypertension, a large proportion of the population has undiagnosed (37.3%) or uncontrolled (27.0%) hypertension with high intra-country variation.21 Undiagnosed and inadequately treated hypertension can lead to severe cardiovascular and other morbidity, which can worsen patient outcomes and increase costs to the healthcare system.25 Thus, regarding high prevalence of hypertension and its cardiac morbidity, effective screening and surveillance systems are required for early detection of patients in order to control their hypertension to decrease the burden on health system care.
Obesity and diabetes mellitus were two highly prevalent comorbidities, 79% and 38.1% respectively in our population. These proportions are comparable to other studies of hypertensive patients in Saudi Arabia.26 We found LVH to be the most common hypertensive complication, 61%, in our study population. Other studies have been revealed LVH shows a varied range from 20% in patients with mild hypertension to near 100% in those suffer from severe hypertension.27 Other complications included diastolic dysfunction, retinopathy, abnormal ventricular wall motion, and ischemic heart disease. These observed hypertensive complications are in line with what has been established in multiple large-scale studies on hypertension.28,29
Our regression analysis revealed increasing age, presence of comorbid diabetes mellitus, and dyslipidemia to be significantly associated with higher likelihoods of having cardiac morbidity such as left ventricular hypertrophy, coronary heart disease, abnormal wall motion, diastolic dysfunction, or heart failure, which is consistent with previous studies. Based on updated risk-assessment guidelines for atherosclerotic CVD published by ACC and AHA; age, sex, race, diabetes, current smoking status, total cholesterol, HDL-C, blood pressure, and blood-pressure treatment status are the strongest predictors of 10-year risk.30 It has been shown in patients with mild to moderate hypertension, coexisting of diabetes, dyslipidemia, and LVH is related to a tremendous risk of developing CVD.31 The risk of death from heart disease in patients with diabetes is two to four times more than patients without diabetes,29 The literature has established that increases in age and comorbid diabetes mellitus are important risk factors for both coronary heart disease and heart failure.32,33 Dyslipidemia has also been proven to worsen cardiovascular morbidity and mortality in hypertension,33 which is also related to age of patient; a 10% decrease in serum cholesterol causes a reduction in coronary heart disease risk of 50%, 40%, 30%, and 20% in the age of 40, 50, 60, and 70, respectively.34 In addition to sufficient antihypertensive treatment, adequate control of blood lipid profiles and glycaemia by means of lifestyle modification and pharmacological agents are pertinent to aid reduction of cardiovascular morbidity in patients with hypertension.29
Previous research has identified several mechanisms linking age, dyslipidemia, and diabetes to cardiovascular disease (CVD). As we age, oxidative stress increases and triggers persistent inflammation, leading to functional and electrical abnormalities of the heart that can eventually result in CVD.35–37 Dyslipidemia, characterized by elevated levels of circulating free fatty acids and triglycerides, can lead to reduced vascular compliance and aggressive atherosclerosis. Additionally, dyslipidemia is associated with heightened stimulation of apolipoprotein B and very low density lipoprotein (VLDL) cholesterol coupled with decreased high density lipoprotein (HDL) levels, which can further contribute to the development of atherosclerosis.38,39 Diabetes can alter triglyceride synthesis and coagulation state, ultimately contributing to the onset of CVD.40
The present study has identified the primary risk factors associated with cardiac morbidity. Given the potential health and financial implications of these diseases on the healthcare system, it is recommended that policymakers develop public health policies aimed at preventing hypertension through education. Early detection of hypertension in its initial stages and educating the population on the symptoms and causes of complications could help mitigate the risk of cardiac morbidities. These measures could ultimately help reduce the burden of CVD on individuals and society as a whole.
Strengths and Limitations of the Study
To the best of the authors’ knowledge no study has previously established clinical morbidities, blood laboratory testing, and abnormal echocardiography findings in patients with chronic hypertension in the Kingdom of Saudi Arabia. Owing to the cross-sectional study design, we were unable to clearly establish a temporal or causal relationship between the risk factors and cardiovascular morbidity. Given that we included only patients from hospital settings, patients with hypertension who might not have had severe comorbid disease that warranted tertiary care hospital visits may have been inadvertently precluded owing to the sampling bias. Thus, the frequencies of morbidities elucidated here may be higher than what is expected in the general Saudi population with hypertension. Furthermore, owing to the relatively small sample and 10% margin of error, additional longitudinal study in the Saudi population is warranted to confirm the results of this study.
Conclusions
Older age, the presence of comorbid diabetes mellitus, and abnormal blood lipid profile are associated with higher likelihoods of having left ventricular hypertrophy, coronary heart disease, abnormal wall motion, diastolic dysfunction, or heart failure in hypertensive patients. Our results suggest that those with diabetes or dyslipidemia are at greatest risk for cardiovascular morbidity and require more aggressive preventative measures to reduce cardiovascular morbidity.
Data Sharing Statement
Data are available upon request from the corresponding author.
Ethics Approval and Consent to Participate
The study was reviewed and approved by the Deanship of Scientific Research at Prince Sattam bin Abdulaziz University with the ethical no- (IF-PSAU-2021/03/18253) and written informed consent was obtained from participants. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The authors extended their appreciation to the deputyship for research and innovation, ministry of education in Saudi Arabia for funding this research work through the project number (IF-PSAU-2021/03/18253).
Funding
The deputyship for research and innovation, ministry of education in Saudi Arabia for funding this research work through the project number (IF-PSAU-2021/03/18253).
Disclosure
The authors do not have any competing interests to declare.
References
1. Alshammari SA, Alajmi AN, Albarrak RA, et al. Quality of life and awareness of hypertension among hypertensive patients in Saudi Arabia. Cureus. 2021;13(5):125.
2. Oparil S, Acelajado MC, Bakris GL, et al. Hypertension (Primer). Nature Rev. 2018;4(1):18014.
3. Charles L, Triscott J, Dobbs B. Secondary hypertension: discovering the underlying cause. Am Fam Physician. 2017;96(7):453–461.
4. Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020;16(4):223–237. doi:10.1038/s41581-019-0244-2
5. El Bcheraoui C, Memish ZA, Tuffaha M, et al. Hypertension and its associated risk factors in the Kingdom of Saudi Arabia, 2013: a national survey. Int J Hypertens. 2014;2014. doi:10.1155/2014/564679
6. Aljuraiban GS, Al Slail FY, Aldhwailea SK, et al. May measurement month 2019: an analysis of blood pressure screening results from Saudi Arabia. Eur Heart J Supplements. 2021;23(Supplement_B):B128–B130. doi:10.1093/eurheartj/suab029
7. Aldiab A, Shubair MM, Al-Zahrani JM, et al. Prevalence of hypertension and prehypertension and its associated cardioembolic risk factors; a population based cross-sectional study in Alkharj, Saudi Arabia. BMC Public Health. 2018;18(1):1–9. doi:10.1186/s12889-018-6216-9
8. Ahmed AM, Hersi A, Mashhoud W, et al. Cardiovascular risk factors burden in Saudi Arabia: the Africa Middle East cardiovascular epidemiological (ACE) study. J Saudi Heart Assoc. 2017;29(4):235–243. doi:10.1016/j.jsha.2017.03.004
9. Collaboration APCS. Blood pressure and cardiovascular disease in the Asia Pacific region. J Hypertens. 2003;21(4):707–716. doi:10.1097/00004872-200304000-00013
10. Brown DW, Giles WH, Greenlund KJ. Blood pressure parameters and risk of fatal stroke, NHANES II mortality study. Am J Hypertens. 2007;20(3):338–341. doi:10.1016/j.amjhyper.2006.08.004
11. Vishram JK, Borglykke A, Andreasen AH, et al. Impact of age on the importance of systolic and diastolic blood pressures for stroke risk: the MOnica, Risk, Genetics, Archiving, and Monograph (MORGAM) project. Hypertension. 2012;60(5):1117–1123. doi:10.1161/HYPERTENSIONAHA.112.201400
12. Benetos A, Safar M, Rudnichi A, et al. Pulse pressure: a predictor of long-term cardiovascular mortality in a French male population. Hypertension. 1997;30(6):1410–1415. doi:10.1161/01.HYP.30.6.1410
13. Kjeldsen SE. Hypertension and cardiovascular risk: general aspects. Pharmacol Res. 2018;129:95–99. doi:10.1016/j.phrs.2017.11.003
14. Ridker PM, Buring JE, Rifai N, Cook NR. Development and validation of improved algorithms for the assessment of global cardiovascular risk in women: the Reynolds Risk Score. JAMA. 2007;297(6):611–619. doi:10.1001/jama.297.6.611
15. Woodward M, Brindle P, Tunstall-Pedoe H. Adding social deprivation and family history to cardiovascular risk assessment: the ASSIGN score from the Scottish Heart Health Extended Cohort (SHHEC). Heart. 2007;93(2):172–176. doi:10.1136/hrt.2006.108167
16. Park H, Cho M, Lim N. Cardiovascular mortality and morbidities by systolic blood pressure levels in hypertensive patients: results from sample cohort of national health insurance service. J Hypertens. 2018;36:e140–e141. doi:10.1097/01.hjh.0000539368.16023.25
17. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J Am Coll Cardiol. 2018;71(19):e127–e248. doi:10.1016/j.jacc.2017.11.006
18. Cole TJ, Lobstein T. Extended international (IOTF) body mass index cut‐offs for thinness, overweight and obesity. Pediatr Obes. 2012;7(4):284–294. doi:10.1111/j.2047-6310.2012.00064.x
19. Orozco-Beltran D, Gil-Guillen VF, Redon J, et al. Lipid profile, cardiovascular disease and mortality in a Mediterranean high-risk population: the ESCARVAL-RISK study. PLoS One. 2017;12(10):e0186196. doi:10.1371/journal.pone.0186196
20. Feig DI, Kang D-H, Johnson RJ. Uric acid and cardiovascular risk. N Engl J Med. 2008;359(17):1811–1821. doi:10.1056/NEJMra0800885
21. Huguet N, Larson A, Angier H, et al. Rates of undiagnosed hypertension and diagnosed hypertension without anti-hypertensive medication following the affordable care act. Am J Hypertens. 2021;34(9):989–998. doi:10.1093/ajh/hpab069
22. Al-Nozha MM, Abdullah M, Arafah MR, et al. Hypertension in Saudi Arabia. Saudi Med J. 2007;28(1):77.
23. Tyrovolas S, El Bcheraoui C, Alghnam SA, et al. The burden of disease in Saudi Arabia 1990–2017: results from the Global Burden of Disease Study 2017. Lancet Planetary Health. 2020;4(5):e195–e208. doi:10.1016/S2542-5196(20)30075-9
24. Herzallah HK, Antonisamy BR, Shafee MH, Al-Otaibi ST. Temporal trends in the incidence and demographics of cancers, communicable diseases, and non-communicable diseases in Saudi Arabia over the last decade. Saudi Med J. 2019;40(3):277. doi:10.15537/smj.2019.3.23585
25. Alsaghah HYA, Alkhabbaz MJM, AlAithan NAM, et al. Hypertension and associated morbidity in Saudi Arabia: a cross-sectional study. Atherosclerosis. 2019;4:4–12.
26. Collaboration PS. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–1913. doi:10.1016/S0140-6736(02)11911-8
27. Ruilope LM, Schmieder RE. Left ventricular hypertrophy and clinical outcomes in hypertensive patients. Am J Hypertens. 2008;21(5):500–508. doi:10.1038/ajh.2008.16
28. Rapsomaniki E, Timmis A, George J, et al. Blood pressure and incidence of twelve cardiovascular diseases: lifetime risks, healthy life-years lost, and age-specific associations in 1.25 million people. Lancet. 2014;383(9932):1899–1911. doi:10.1016/S0140-6736(14)60685-1
29. Hajar R. Risk factors for coronary artery disease: historical perspectives. Heart Views. 2017;18(3):109. doi:10.4103/HEARTVIEWS.HEARTVIEWS_106_17
30. Goff JDC, Lloyd-Jones DM, Bennett G, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. Circulation. 2014;129(25_suppl_2):S49–S73. doi:10.1161/01.cir.0000437741.48606.98
31. Kannel WB. Hypertension: reflections on risks and prognostication. Med Clinics North Am. 2009;93(3):541–558. doi:10.1016/j.mcna.2009.02.006
32. Tromp J, Paniagua SM, Lau ES, et al. Age dependent associations of risk factors with heart failure: pooled population based cohort study. BMJ. 2021;2021:372.
33. Katholi RE, Couri DM. Left ventricular hypertrophy: major risk factor in patients with hypertension: update and practical clinical applications. Int J Hypertens. 2011;2011:1–10. doi:10.4061/2011/495349
34. Law MR, Wald NJ, Thompson S. By how much and how quickly does reduction in serum cholesterol concentration lower risk of ischaemic heart disease? BMJ. 1994;308(6925):367–372. doi:10.1136/bmj.308.6925.367
35. Curtis AB, Karki R, Hattoum A, Sharma UC. Arrhythmias in patients≥ 80 years of age: pathophysiology, management, and outcomes. J Am Coll Cardiol. 2018;71(18):2041–2057. doi:10.1016/j.jacc.2018.03.019
36. Steenman M, Lande G. Cardiac aging and heart disease in humans. Biophys Rev. 2017;9(2):131–137. doi:10.1007/s12551-017-0255-9
37. Rodgers JL, Jones J, Bolleddu SI, et al. Cardiovascular risks associated with gender and aging. J Cardiovascular Dev Dis. 2019;6(2):19. doi:10.3390/jcdd6020019
38. Hamilton SJ, Watts GF. Endothelial dysfunction in diabetes: pathogenesis, significance, and treatment. Rev Diabetic Stud. 2013;10(2–3):133. doi:10.1900/RDS.2013.10.133
39. Hedayatnia M, Asadi Z, Zare-Feyzabadi R, et al. Dyslipidemia and cardiovascular disease risk among the MASHAD study population. Lipids Health Dis. 2020;19:1–11. doi:10.1186/s12944-020-01204-y
40. Leon BM, Maddox TM. Diabetes and cardiovascular disease: epidemiology, biological mechanisms, treatment recommendations and future research. World J Diabetes. 2015;6(13):1246. doi:10.4239/wjd.v6.i13.1246
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.