")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Predictors of an Active Lifestyle in Middle-Aged and Older Adults with HIV in the United States Deep South
Authors Li W, Fazeli PL, Wang G, Maqbool M, Del Bene VA, Triebel K, Martin KM, Vance D
Received 16 December 2022
Accepted for publication 24 February 2023
Published 2 March 2023 Volume 2023:15 Pages 63—70
DOI https://doi.org/10.2147/HIV.S399842
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Wei Li,1 Pariya L Fazeli,2 Ge Wang,3 Muhammad Maqbool,1 Victor A Del Bene,4 Kristen Triebel,4 Karli M Martin,4 David Vance2
1School of Health Professions, University of Alabama at Birmingham, Birmingham, AL, USA; 2School of Nursing, University of Alabama at Birmingham, Birmingham, AL, USA; 3Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 4Department of Neurology, School of Medicine, University of Alabama at Birmingham, Birmingham, AL, USA
Correspondence: Wei Li, Biomedical Sciences, Department of Clinical and Diagnostic Sciences, School of Health Professions, University of Alabama at Birmingham, SHPB 424B, 1720 2nd Avenue South, Birmingham, AL, 35294, USA, Tel +1 205-996-2656, Fax +1 205-975-7302, Email [email protected]
Background and Purpose: An active lifestyle is important for health maintenance and disease prevention. This study was to examine what factors predict an active lifestyle in HIV+ and HIV- adults from the United States Deep South.
Methods: The sample included 279 participants (174 HIV+ and 105 HIV-) who completed a comprehensive assessment. An active lifestyle composite was created using variables of employment status, level of social support, level of physical activity, and diet. Correlations and regression analyses were conducted between the active lifestyle composite and possible predictors for all (HIV+ and HIV-), HIV+, and HIV- participants, respectively.
Results: Lower levels of depression, higher socioeconomic status (SES), and younger age were significant predictors of a more active lifestyle for the full sample, HIV+, and HIV- participants, respectively.
Conclusion: SES and depression represent important factors influencing engagement in an active lifestyle in PLWH. Such factors should be considered when developing and implementing lifestyle interventions.
Keywords: AIDS, health behaviors, HIV-associated neurocognitive disorders, HAND mental health, personality
Introduction
According to HIV Surveillance Report 2018 (updated), there are over 1 million people living with HIV (PLWH) in the United States (US) and the total number of PLWH is increasing as there are nearly 40,000 newly diagnosed cases each year.1 At the same time, combination antiretroviral therapy has substantially extended the lifespan of PLWH, which is comparable to that seen in HIV seronegative individuals.2 Not surprisingly, the percentage of PLWH who are 50 years older is expected to approach 70% by 2030.3 Success in cART has substantially extended the lifespan of PLWH and shifted the focus of care from extending lifespan to improving their quality of life. Unfortunately, advanced age,4 incomplete virologic suppression,5 food insecurity,6 and allostatic load7 represent some known risk factors for poor health outcomes of PLWH. Up to 28% of elderly PLWH could be identified as frail, which puts them at risk for many morbidities and increased mortality.8,9 Furthermore, HIV-related stigma contributes to a high prevalence of mental disorders in PLWH.10
Emerging studies suggest that engaging in an active lifestyle may allow PLWH to maintain health as they age, or in contrast, that an inactive lifestyle may be associated with poorer health outcomes. Factors comprised of an active lifestyle such as employment, physical activity, and social activity are associated with better global cognitive performance as well as a lower prevalence of HIV-associated neurocognitive disorders (HAND).11 By contrast, lower rates of physical activity are associated with an increased cardiometabolic disease risk12 as well as poorer cognitive functioning13–15 among PLWH. Further, specific dietary approaches have demonstrated positive effects on cognitive functioning in PLWH.16 Among PLWH with poor health literacy, a composite of a more healthy diet and exercise positively predicted higher HIV medication adherence.17 Further, the health of HIV+ adults could be improved with interventions for addressing financial, nutritional (related to diet), and social (related to social support) barriers to care engagement.18 Moreover, employment status negatively predicted the number and intensity of clinical symptoms (pain, depression, etc.) being experienced by PLWH.19 In other words, PLWH who work showed fewer and less intense clinical symptoms than their unemployed counterparts.
Therefore, for PLWH, beyond adhering to medication regimens,20 engaging in an active lifestyle including maintaining a healthy diet, exercising regularly, working, and maintaining a satisfying social support system may promote better health outcomes. An active lifestyle comprised of healthy behaviors may prevent and/or reduce the incidence and prevalence of many diseases. On the other hand, evidence across populations demonstrates that many health problems develop from either a passive lifestyle (eg, being sedentary), poor health behaviors (eg, poor diet), or failing to take proper preventive measures (eg, maintaining a healthy body mass index).21,22
Given the impact of engagement in an active lifestyle on health outcomes, it is important to understand what factors can effectively predict such behaviors in PLWH. Thus, the purpose of this study was to examine if and how an active lifestyle is associated with possible prediction factors with a sample of HIV+ and HIV- adults (40+ years) from the US Deep South. Compared to other places, the US Deep South (Alabama, Georgia, Louisiana, Mississippi, and South Carolina),23 is characterized by a: 1) higher rate of poverty; 2) lower level of education; 3) high percentage of the Black population; and 4) higher percentage of people living in the rural counties.24 According to the 2018 Behavioral Risk Factor Surveillance System, people in the Deep South States have an unhealthier lifestyle than other States (https://www.cdc.gov). In 2013, 40% of PLWH lived in the Deep South, which is only 28% of the US population.25 More alarmingly, the Deep South has the highest death rates from AIDS in the US.25
Methods
Overview
This study was conducted according to the ethical guideline of the Declaration of Helsinki. We received ethical approval from the University of Alabama at Birmingham Institute Review Board.
In this cross-sectional, secondary data analysis, data were collected from a combined cohort of participants from an R01 cognitive training clinical trial with PLWH and an R00 study examining successful aging with HIV. HIV+ participants were recruited for the R01 clinical trial, and a subset participated in the R00 observational study. HIV- participants were also recruited for the R00 study and they completed identical study measures.
Participants and Procedure
The current study included a total of 279 participants (174 were HIV+ and 105 were HIV-). HIV+ participants were recruited from an HIV/AIDS clinic affiliated with the University of Alabama at Birmingham, whereas HIV- participants were recruited via flyers and an online advertisement. Eligibility was assessed over the phone before the assessment visit. Participants were excluded if they had a major comorbid condition that affects cognition or participation in the study (ie, dementia, head injury, current radiation or chemotherapy, blindness, deafness); this was determined via a telephone screening. The age cutoff for HIV+ participants was 40+ as compared to that of 50+ for HIV- participants. Participants were mailed the IRB-approved consent form several days before their assessment appointment. On the day of the assessment, the consent form was explained to the participants with an opportunity to ask questions; then the participant and the research assistant signed the consent form. After obtaining verbal and written consent from each participant, a comprehensive research battery was performed and information was collected on demographic, HIV serostatus (+ versus -), depressive symptomatology, personality, health literacy, and active lifestyle factors. The descriptive statistics for relevant study variables for all participants are shown in Table 1.
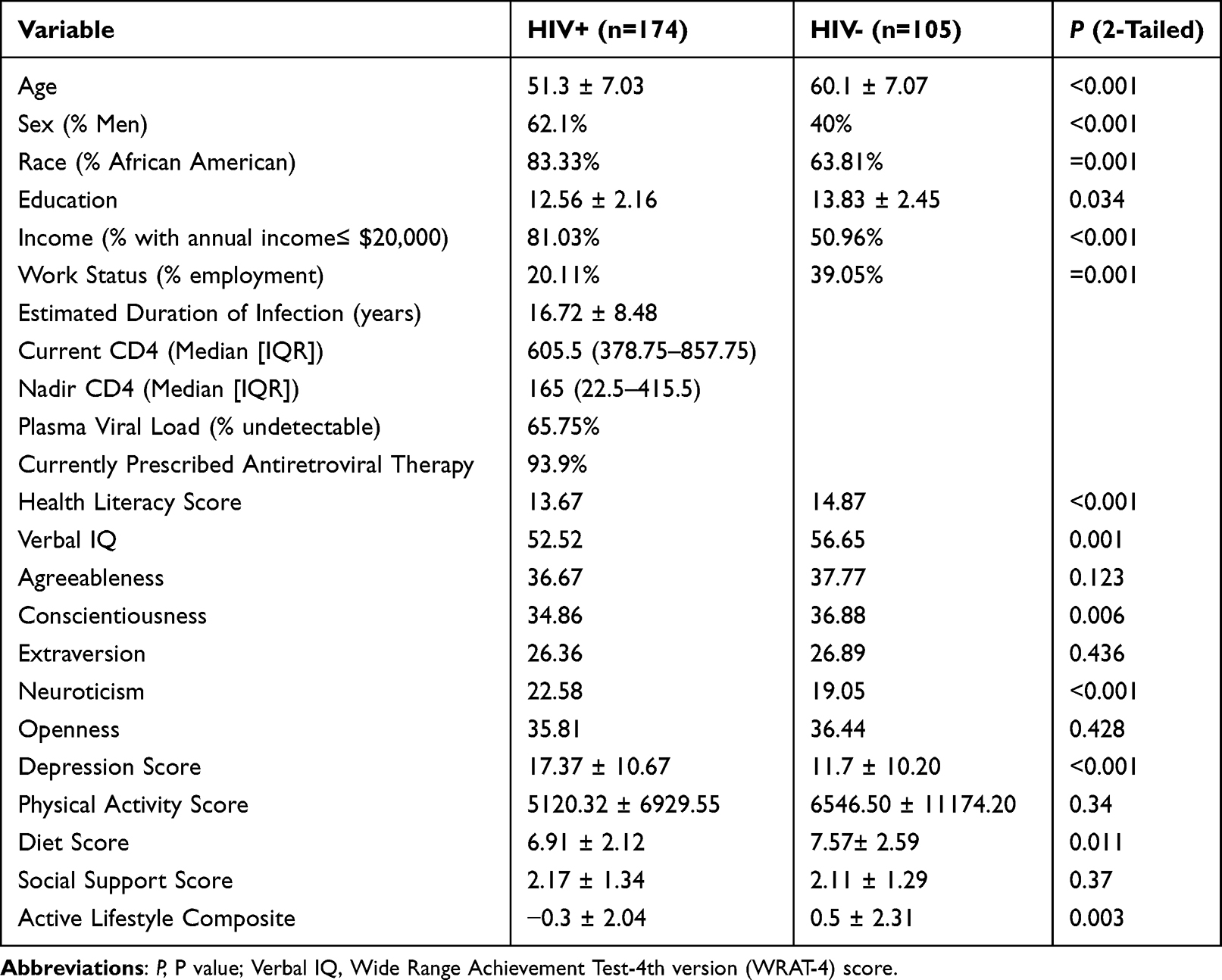 |
Table 1 Sample Characteristics for HIV+ and HIV- Participants |
Demographic and Clinical Information
Basic demographic information was gathered from all participants: age (in years), sex (0 = female; 1 = male), race (0 = non-white/non-Caucasian; 1=White/Caucasian), education (1 = 1st grade; 12 = higher school/high school equivalency diploma; 16 = bachelor’s degree; 18 = master’s degree; 20 = doctoral degree), and income (low = $0–$20,000; other = $20,001–$100,001 and above). A socioeconomic status (SES) variable was created using a sum of z scores of the level of attained education, income as well as the Wide Range Achievement Test (WRAT-4). The WRAT-4 measures an individual’s ability to read, comprehend, spell, and compute. Health literacy was captured with the Test of Functional Health Literacy in Adults (TOFHLA)26 Reading Subtest, which consists of a 50-item reading comprehension. For HIV+ participants only, medical records (at the baseline) were used for verifying their HIV status, duration of infection (in years), current and nadir CD4+ lymphocyte count {median [interquartile range (IQR)]}, current viral load (RNA copies), and if they were on an antiretroviral therapy.
Center for Epidemiological Studies – Depression Scale
The Centers for Epidemiological Studies Depression scale (CES-D) was used for assessing the level of depression.27 Participants completed the full 20-item CES-D. Items focused on how often a participant had specific thoughts, feelings, and behaviors in the last 7 days. Responses were 0 = 0 days, 1 = 1–2 days, 2 = 3–4 days, and 3 = 5–7 days. For this scale, scores range from 0 to 60, with a score of 16 or higher indicating possible depression.
Personality
The Big Five Inventory is a 44-item self-report measure that assesses the five traits of personality: extraversion (eg, gregariousness, assertiveness), agreeableness (eg, trust, empathy), conscientiousness (eg, orderliness, self-discipline), neuroticism (eg, anxiety, depression), and openness.28,29 Forty-four brief descriptive phrases (eg, “(I see myself as someone who) is generally trusting”; “(I see myself as someone who) worries a lot”) are rated by the participant on a 5-point Likert response scale ranging from 1 (“strongly disagree”) to 5 (“strongly agree”) with the mid-point representing “neither agree nor disagree.” Scores for each of the five traits are obtained by calculating the mean of the items associated with each of the five personality traits. Higher scores indicate higher levels of that personality trait.
Active Lifestyle Composite
In order to operationalize an active lifestyle, we created a composite including multiple variables across domains: cognitive activity, physical activity, social activity, and diet, using an approach similar to that in a prior study.11 Specifically, for cognitive activity, we used work status (working full time was coded as “1”, part time as “0.5” and unemployment as “0”) as a proxy. Physical activity level was determined using the standard scoring for the total metabolic equivalent tasks (MET) minutes per week from the International Physical Activity Questionnaire (IPAQ).30 For social activity, the average score of the Duke Social Support Index was used.31 For diet, the Mediterranean-DASH Diet Intervention for Neurodegenerative Delay (MIND) questionnaire score was used.32 We then calculated the lifestyle composite by summing the Z scores of the above four variables (work status, physical activity level, social support, and diet). Compared to the lifestyle composite variable used in a previous study,11 the variable of diet was added to the formula of calculation since diet choice is also an essential component of an active lifestyle. For the lifestyle composite variable, a higher score indicates a more active lifestyle.
Statistical Analysis
SPSS (version 27) was used to run all the data analyses. Differences between HIV+ and HIV- groups were examined using t-tests or Chi-square tests. A Spearman’s Rho correlation analysis was performed between the lifestyle composite variable and demographic, personality, and health variables listed in Table 2, for the total sample, and for HIV+ participants, HIV- participants individually. Then a multivariate linear regression was performed by incorporating all significant predictors from the bivariate correlation analyses for all participants, HIV+ participants, and HIV- participants, respectively. An alpha level of p < 0.05 was considered statistically significant for all analyses.
 |
Table 2 Spearman’s Rho Correlations Between Active Lifestyle and Study Variables |
Results
The HIV+ group was significantly younger than the HIV- group. Compared with the HIV- group, the HIV+ group was composed primarily of men and Black/African American participants (Table 1). The HIV+ group had a lower level of education, lower employment rate, and a higher percentage with annual income ≤ $20,000 than the HIV- group (Table 1). The HIV+ group had a higher average depression score and a lower diet score (ie, less healthy diet) than the HIV- group. The HIV+ and HIV- groups had comparable average level of physical activity and social support. Of note, the HIV+ group had an average active lifestyle composite (z-score) of −0.3 ± 2.04, which was significantly lower than the HIV- group of 0.5 ± 2.31 (p=0.003) (Table 1).
As seen in Table 2, for the total sample (HIV+ and HIV- combined), the active lifestyle composite variable was significantly correlated with SES (r=0.26, p<0.001), depression (r=−0.312, p<0.001), healthy literacy (r=0.175, p=0.004), as well as five personality traits: agreeableness (r = 0.208, p=0.001), conscientiousness (r=0.237, p<0.001), extraversion (r=0.183, p=0.002), neuroticism (r=−0.235, p<0.001), and openness (r=0.157, p=0.009) (Table 2). Then a multivariate linear regression model was conducted by incorporating HIV status along with all significant possible predictors (SES, depression, healthy literacy score, five personality traits) for the active lifestyle composite variable (Table 3). The multivariate linear regression analysis showed a significant omnibus model (F=4.44, p<0.001, R2= 0.142). For all participants (HIV+ and HIV-), only the depression score was significantly associated with an active lifestyle (p=0.011).
 |
Table 3 Multiple Linear Regression Between Active Lifestyle Composite and Significant Correlates |
For the HIV+ participants, the active lifestyle composite was significantly correlated with SES (r=0.264, p<0.001), depression (r=−0.293, p<0.001) as well as three personality traits: agreeableness (r=0.161, p=0.038), conscientiousness (r=0.214, p=0.005), and neuroticism (r=−0.245, p=0.001) (Table 2). From these possible predictors (SES, depression, agreeableness, conscientiousness, and neuroticism), a multivariate linear regression analysis showed a significant omnibus model predicting the active lifestyle composite (F=4.841, p<0.001, R2= 0.136). For HIV+ participants, SES was the only significant predictor of an active lifestyle (p=0.017).
For the HIV- participants, the active lifestyle composite variable was significantly correlated with age at baseline (r=−0.22, p=0.024), depression (r=0.261, p=0.008), healthy literacy (r=0.209, p=0.035) as well as four personality traits: agreeableness (r=0.249, p=0.012), conscientiousness (r=0.213, p=0.032), extraversion (r=0.288, p=0.003), and openness (r=0.246, p=0.012) (Table 2). For all the possible predictors (age at baseline, SES, healthy literacy, agreeableness, conscientiousness, extraversion, and openness), the multivariate linear regression showed a significant omnibus model (F=2.53, p=0.046, R2= 0.204). For HIV- participants, age at baseline was the only significant predictor for an active lifestyle (p=0.021).
Discussion
This study examined predictors of an active lifestyle with a sample of HIV+ and HIV- adults (40+ years) from the US Deep South. First, we found that HIV+ participants had lower scores on the active lifestyle composite. Next, we found among both HIV+ and HIV- participants, a greater level of depression was associated with a less active lifestyle, which is consistent with prior research findings. From a study with 1300 adult participants (aged 20 to 80 years old) of the National Health and Nutrition Examination Survey (2007–2014), the level of physical activity was found to be strongly and inversely associated with depression.33 Moreover, major depression was found to be associated with a more than 3-fold increase in the odds of smoking and 37% decrease in the odds of staying physically active.34 Therefore, depression may lead to a passive lifestyle, which may exacerbate the existing depression which perpetuates itself (ie, depression ➔ passive lifestyle ➔ more depression). The depression symptoms such as lack of motivation, negative self-view, and learned helplessness are commonly seen in PLWH, which would prevent them from engaging in an active lifestyle.35 By contrast, exercise has been shown as an effective approach for improving depression and quality of life in PLWH.36
Our data supported that a higher SES is positively associated with an active lifestyle in HIV+ participants. Specifically, within the HIV+ sample, SES was associated with active lifestyle engagement. Low SES often comes with practical limitations of time and financial support for engaging in a healthy active lifestyle. In addition, low SES has been found to be associated with a high prevalence of depression in different geographic areas.37–39 Therefore, interventions targeting active lifestyle engagement among PLWH may need to consider both SES and depression as well as their interaction when designing the programs. Within our HIV- sample, we found age was the only significant predictor for an active lifestyle such that the older the age, the less likely it is for a person to have an active lifestyle. Prior work has shown that older adults may be less likely to engage in an active lifestyle than their younger counterparts.40 These findings may also reflect the fact that our HIV- group was older than the HIV+ group.
Although personality and health literacy were significantly correlated with the active lifestyle composite in unadjusted analyses, neither significantly predicted an active lifestyle in our multivariable models. Our SES variable, in contrast, significantly predicted an active lifestyle for HIV+ participants, which suggests that the broader construct of SES may be more influential to activity engagement than health literacy. Indeed, healthy literacy is closely related to the quality of education, which was part of the SES composite. Similarly, our personality variables no longer emerged as predictors in the context of SES, suggesting the dominant role of SES in determining active or inactive lifestyle behaviors. Unfortunately, our cross-sectional data did not allow for understanding the nuanced temporal associations between these factors and engagement in an active lifestyle.
Several limitations are associated with our current study. First, internalized and externalized HIV stigma as well as other types of stigma (homophobia and sexual discrimination, racial discrimination) are a threat to the quality of life and possibly to an active lifestyle.41 Those who experience HIV-related stigma are more vulnerable to psychological distress and may have less social support.42 Unfortunately, our study did not include measures of HIV-related stigma. Second, our data analysis was cross-sectional, limiting our ability to establish causal relationships. Third, our operationalization of an active lifestyle was based upon self-report measures at one time point. Future work would benefit from using objective measurement (eg, actigraphy, diet logs) and contextual data collection methods such as the experience sampling method (ESM) to understand factors that promote or hinder PLWH from engaging in an active lifestyle. Last, substance abuse and trauma experiences may also play important roles in one’s lifestyle choice. Future studies can look at the possible correlations between them. On the other hand, several study strengths are also noted. First, our data were collected from both HIV+ and HIV- participants, so direct comparisons were made between these two independent populations. The findings could potentially be used to optimize care to individuals based on their clinical HIV infection status, SES, and other comorbidities. For example, it is important to know the status of depression in order to improve health-related quality of life.43 Second, all questionnaires for the current study had been used and validated by previous studies. Therefore, the data generated from these questionnaires were reliable. Third, our sample represents people in the US Deep South, the epicenter of the AIDS epidemic. Our findings are meaningful for both HIV+ infected persons living in the US Deep South and the general care of PLWH.
Implications for Practice and Research
Our findings have the potential to inform and be integrated into clinical practice and public health intervention. While improving SES may be an effective way for one to adopt a more active lifestyle, this is often associated with factors that are not easily or quickly modifiable. For example, low SES most commonly relates to unemployment or underemployment status, which can often be a significant barrier to overcome. Community-based interventions may be helpful although the strength of such findings in economically disadvantaged adults is currently tenuous at best,44 but continued research is warranted.
Depression is a risk factor for an inactive lifestyle. Psychotherapy is an effective treatment for depression.45 Additionally, there is evidence that exercise, when paired with either psychopharmaceutical or psychotherapeutic approaches to treating depression, can further reduce depression.46 However, further research investigating this in PLWH is needed to support this hypothesis. In fact, HIV infection status is an important factor to consider for its potential additive or synergistic effects with age, SES, and depression on a healthy lifestyle choice. In conclusion, our findings have potential clinical implications for delivering individualized care for the PLWH in the US Deep South and beyond.
Data Sharing Statement
- We will share deidentified individual participant data as well as data dictionaries.
- All of the individual participant data collected during the trial will be shared after de-identification.
- Other documents available for being shared: study protocol, statistical analysis procedure, informed consent form, clinical study report, and analytic code.
- The data will be shared directly with the researcher(s) who requested by following the data sharing policy from the University of Alabama at Birmingham.
- The data will be available immediately after publication with no ending date.
Consent for Publication
All participants have given informed consent for their data being analyzed and published.
Acknowledgments
This study was funded by an NIH/National Institute of Mental Health R01-award (1R01MH106366-01A1; ClinicalTrials.gov; NCT02758093; PI: Vance) titled “An RCT of Speed of Processing Training in Middle-aged and Older Adults with HIV”; by an NIH/National Institute on Aging (NIA) R00-award (R00 AG048762; PI: Fazeli); and by an NIH/NIA P30-award (Edward R. Roybal Center for Translational Research in Aging and Mobility; P30 AG022838; PI: Ball).
Disclosure
The authors have no conflicts of interest to disclose in this work.
References
1. Centers for Disease Control and Prevention. HIV Surveillance Report, 2018 (Updated); vol.31. Available from: https://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-report-2018-updated-vol-31.pdf.
2. High KP, Brennan-Ing M, Clifford DB, et al. HIV and aging: state of knowledge and areas of critical need for research. A report to the NIH office of AIDS research by the HIV and Aging Working Group. J Acquir Immune Defic Syndr. 2012;60(Suppl1):S1–18. doi:10.1097/QAI.0b013e31825a3668
3. Wing EJ. The aging population with HIV infection. Trans Am Clin Climatol Assoc. 2017;128:131–144.
4. Kinai E, Komatsu K, Sakamoto M, et al. Association of age and time of disease with HIV associated neurocognitive disorders: a Japanese nationwide multicenter study. J Neurovirol. 2017;23(6):864–874. doi:10.1007/s13365-017-0580-6
5. Chen MF, Gill AJ, Kolson DL. Neuropathogenesis of HIV-associated neurocognitive disorders: roles for immune activation, HIV blipping and viral tropism. Curr Opin HIV AIDS. 2014;9(6):559–564. doi:10.1097/COH.0000000000000105
6. Hobkirk AL, Towe SL, Patel P, Meade CS. Food insecurity is associated with cognitive deficits among HIV-positive, but not HIV-negative, individuals in a United States sample. IDS Behav. 2017;21(3):783–791.
7. Fazeli PL, Waldrop-Valverde D, Yigit I, et al. An exploratory study of correlates of allostatic load in older people living with HIV. J Acquir Immune Defic Syndr. 2020;83(5):441–449. doi:10.1097/QAI.0000000000002293
8. Bloch M. Frailty in people living with HIV. AIDS Res Ther. 2018;15(1):19. doi:10.1186/s12981-018-0210-2
9. Deeks SG, Overbaugh J, Phillips A, Buchbinder S. HIV infection. Nat Rev Dis Primers. 2015;1:15035. doi:10.1038/nrdp.2015.35
10. Algarin AB, Sheehan DM, Varas-Diaz N, et al. Enacted HIV-Related stigma’s association with anxiety & depression among people living with HIV (PLWH) in Florida. AIDS Behav. 2021;25:93–103. doi:10.1007/s10461-020-02948-5
11. Fazeli PL, Woods SP, Heaton RK, et al. An active lifestyle is associated with better neurocognitive functioning in adults living with HIV-infection. J Neurovirol. 2014;20(3):233–242. doi:10.1007/s13365-014-0240-z
12. Willig AL, Webel AR, Westfall AO, et al. Physical activity trends and metabolic health outcomes in people living with HIV in the US, 2008–2015. Prog Cardiovasc Dis. 2020;63(2):170–177. doi:10.1016/j.pcad.2020.02.005
13. Fazeli PL, Marquine MJ, Dufour C, et al. Physical activity is associated with better neurocognitive and everyday functioning among older adults with HIV disease. AIDS Behav. 2015;19:1470–1477. doi:10.1007/s10461-015-1024-z
14. Dufour CA, Marquine MJ, Fazeli PL, et al. A longitudinal analysis of the impact of physical activity on neurocognitive functioning among HIV-infected adults. AIDS Behav. 2018;22:1562–1572. doi:10.1007/s10461-016-1643-z
15. Dufour CA, Marquine MJ, Fazeli PL, et al. Physical exercise is associated with less neurocognitive impairment among HIV-infected adults. J Neurovirol. 2013;19(5):410–417. doi:10.1007/s13365-013-0184-8
16. Morrison SA, Fazeli PL, Gower B, et al. Cognitive effects of a ketogenic diet on neurocognitive impairment in adults aging with HIV: a pilot study. J Assoc Nurses AIDS Care. 2020;31(3):312–324. doi:10.1097/JNC.0000000000000110
17. Pellowski JA, Kalichman SC. Health behavior predictors of medication adherence among low health literacy people living with HIV/AIDS. J Health Psychol. 2016;21(9):1981–1991. doi:10.1177/1359105315569617
18. Weiser SD, Hatcher AM, Hufstedler LL, et al. Changes in health and antiretroviral adherence among HIV-infected adults in Kenya: qualitative longitudinal findings from a livelihood intervention. AIDS Behav. 2017;21(2):415–427. doi:10.1007/s10461-016-1551-2
19. Webel A, Wantland D, Rose CD, et al. A cross-sectional relationship between social capital, self-compassion and perceived HIV symptoms. J Pain Symptom Manage. 2015;50(1):59–68. doi:10.1016/j.jpainsymman.2014.12.013
20. Bangsberg DR. Less than 95% adherence to nonnucleoside reverse-transcriptase inhibitor therapy can lead to viral suppression. Clin Infect Dis. 2006;43(7):939–941. doi:10.1086/507526
21. Park JH, Moon JH, Kim HJ, Kong MH, Oh YH. Sedentary lifestyle: overview of updated evidence of potential health risks. Korean J Fam Med. 2020;41(6):365–373. doi:10.4082/kjfm.20.0165
22. Schweren LJS, Larsson H, Vinke PC, et al. Diet quality, stress and common mental health problems: a cohort study of 121,008 adults. Clin Nutr. 2021;40(3):901–906. doi:10.1016/j.clnu.2020.06.016
23. Aly S, Daniel CL, Bae S, et al. Cancer-related beliefs and preventive health practices among residents of rural vs. urban counties in Alabama. Cancer Prev Res. 2021;14:593–602. doi:10.1158/1940-6207.CAPR-20-0458
24. Talaei M, Rabiei K, Talaei Z, et al. Physical activity, sex, and socioeconomic status: a population based study. ARYA Atheroscler. 2013;9(1):51–60.
25. Reif S, Safley D, McAllaster C, Wilson E, Whetten K. State of HIV in the US Deep South. J Community Health. 2017;42(5):844–853. doi:10.1007/s10900-017-0325-8
26. Parker RM, Baker DW, Williams MV, Nurss JR. The test of functional health literacy in adults: a new instrument for measuring patients’ literacy skills. J Gen Intern Med. 1995;10(10):537–541. doi:10.1007/BF02640361
27. Radloff LS. CES-D scale: a self report depression scale for research in the general populations. Appl Psychol Meas. 1977;1:385–401. doi:10.1177/014662167700100306
28. John O, Donahue E, Kentle R. The Big Five Inventory: Versions 4a and 54, Institute of Personality and Social Research. Berkeley, CA: University of California; 1991.
29. John OP, Srivastava S. The Big Five Trait Taxonomy: History, Measurement, and Theoretical Perspectives. Handbook of Personality: Theory and Research.
30. Katz ML, Ferketich AK, Broder-Oldach B, et al. Physical activity among Amish and non-Amish adults living in Ohio Appalachia. J Community Health. 2012;37(2):434–440. doi:10.1007/s10900-011-9460-9
31. Mahmud MA, Hazrin M, Muhammad EN, et al. Social support among older adults in Malaysia. Geriatr Gerontol Int. 2020;20(Suppl 2):63–67. doi:10.1111/ggi.14033
32. Morris MC, Tangney CC, Wang Y, et al. MIND diet slows cognitive decline with aging. Alzheimers Dement. 2015;11(9):1015–1022. doi:10.1016/j.jalz.2015.04.011
33. Liu Y, Ozodiegwu ID, Yu Y, Hess R, Bie R. An association of health behaviors with depression and metabolic risks: data from 2007 to 2014 U.S. National Health and Nutrition Examination Survey. J Affect Disord. 2017;217:190–196. doi:10.1016/j.jad.2017.04.009
34. Xiang X. History of major depression as a barrier to health behavior changes after a chronic disease diagnosis. J Psychosom Res. 2016;85:12–18. doi:10.1016/j.jpsychores.2016.04.001
35. Rosenthal WA, Khalil DD. Exploring the challenges of implementing participatory action research in the context of HIV and poverty. Curationis. 2010;33:69–78. doi:10.4102/curationis.v33i2.1103
36. Oliveira VHF, Rosa FT, Santos JC, et al. Effects of a combined exercise training program on health indicators and quality of life of people living with HIV: a randomized clinical trial. AIDS Behav. 2020;24:1531–1541. doi:10.1007/s10461-019-02678-3
37. Wong SYS, Mercer SW, Woo J, et al. The influence of multi-morbidity and self-reported socio-economic standing on the prevalence of depression in an elderly Hong Kong population. BMC Public Health. 2008;8:119. doi:10.1186/1471-2458-8-119
38. Zhou S, Gao L, Liu F, et al. Socioeconomic status and depressive symptoms in older people with the medication role of social support: a population-based longitudinal study. Int J Methods Psychiatr Res. 2021;30:e1894. doi:10.1002/mpr.1894
39. Freeman A, Tyrovolas S, Koyanagi A, et al. The role of socio-economic status in depression: results from the COURAGE (aging survey in Europe). BMC Public Health. 2016;16:1098. doi:10.1186/s12889-016-3638-0
40. Peters TM, Moore SC, Xiang YB, et al. Accelerometer-measured physical activity in Chinese adults. Am J Prev Med. 2010;38(6):583–591. doi:10.1016/j.amepre.2010.02.012
41. Jang N, Bakken S. Relationships between demographic, clinical, and health care provider social support factors and internalized stigma in People Living With HIV. J Assoc Nurses AIDS Care. 2017;28(1):34–44. doi:10.1016/j.jana.2016.08.009
42. Bauermeister JA, Muessig KE, Flores DD, et al. Stigma diminishes the protective effect of social support on psychological distress among young black men who have sex with men. AIDS Educ Prev. 2018;30(5):406–418. doi:10.1521/aeap.2018.30.5.406
43. Wang XW, Luo HB, Yao EL, et al. The role of personality, social economic and prevention strategy effects on health-related quality of life among people living with HIV/AIDS. Infect Dis Poverty. 2021;10:104. doi:10.1186/s40249-021-00890-9
44. Craike M, Wiesner G, Hilland TA, Bengoechea EG. Interventions to improve physical activity among socioeconomically disadvantaged groups: an umbrella review. Int J Behav Nutr Phys Act. 2018;15(1):43. doi:10.1186/s12966-018-0676-2
45. Munder T, Flückiger C, Leichsenring F, et al. Is psychotherapy effective? A re-analysis of treatments for depression. Epidemiol Psychiatr Sci. 2019;28(3):268–274. doi:10.1017/S2045796018000355
46. Belvederi MM, Ekkekakis P, Magagnoli M, et al. Physical exercise in major depression: reducing the mortality gap while improving clinical outcomes. Front Psychiatry. 2019;10:762. doi:10.3389/fpsyt.2018.00762
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.