Back to Journals » International Journal of General Medicine » Volume 19
Predictive Value of the Combination of Lactate and qSOFA Score for Clinical Outcomes in Cirrhotic Patients with Esophagogastric Variceal Bleeding
Authors Li M, Geng N ![]() , Liu Z, Pan W, Lai C, Cui Y, Miao Y, Zhu Y, Yan B, Li H, Wang J, Liu B
, Liu Z, Pan W, Lai C, Cui Y, Miao Y, Zhu Y, Yan B, Li H, Wang J, Liu B ![]()
Received 24 October 2025
Accepted for publication 17 March 2026
Published 29 March 2026 Volume 2026:19 572229
DOI https://doi.org/10.2147/IJGM.S572229
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Hyam Leffert
Mengyun Li, Nan Geng, Zhao Liu, Wen Pan, Chunlian Lai, Yingying Cui, Yixin Miao, Yueke Zhu, Benyong Yan, Haoqi Li, JingJing Wang, Bo Liu
Emergency Department, Beijing You’an Hospital of the Capital Medical University, Beijing, People’s Republic of China
Correspondence: Bo Liu, Emergency Department, Beijing You’an Hospital, Capital Medical University, No. 8, Xitoutiao, You’anmenwai, Fengtai District, Beijing, 100069, People’s Republic of China, Email [email protected]
Purpose: The objective of our research was to examine the predictive power of the combination of lactate and the quick Sepsis-Related Organ Failure Assessment (qSOFA) score on clinical outcomes in cirrhotic patients with EGVB.
Patients and Methods: This single-center retrospective study consecutively enrolled 547 eligible cirrhotic patients with EGVB admitted to the Emergency Department of Beijing You’an Hospital between July 2022 and November 2022. Data collected included Lactate levels, qSOFA, pre-endoscopic Rockall score (pRS), Glasgow-Blatchford score (GBS), albumin, international normalized ratio (INR), altered mental status, systolic blood pressure, age older than 65 years score (AIMS65), and age, blood tests, comorbidities scores (ABC). These variables were used to predict rebleeding, ICU-admission, and 6-week mortality. Receiver operating characteristic (ROC) curves and logistic regression analysis were used to assess the prognostic value of the scoring systems.
Results: Lactate and qSOFA independently predicted ICU admission and 6-week mortality (P< 0.05). qSOFA alone was an independent predictor of rebleeding, but lactate was not. For rebleeding prediction, the AUC values were: pRS 0.540, GBS 0.582, AIMS65 0.519, ABC 0.510, and Lac+qSOFA 0.564. For ICU-admission, the AUC values were: pRS 0.723, GBS 0.623, AIMS65 0.787, ABC 0.760, and Lac+qSOFA 0.808. For 6-week mortality, the AUC values were: pRS 0.759, GBS 0.715, AIMS65 0.817, ABC 0.834, and Lac+qSOFA 0.818. The combination of lactate and qSOFA showed better predictive performance for ICU admission and 6-week mortality than for rebleeding.
Conclusion: Although the combination of lactate and qSOFA offers limited utility for predicting rebleeding, it is a robust predictor of ICU admission and 6-week mortality in cirrhotic patients with EGVB. Its simplicity and rapid availability make it a highly practical tool for emergency triage in this high-risk population.
Keywords: cirrhosis, esophagogastric variceal bleeding, lactate, qSOFA score, mortality
Introduction
Cirrhosis, resulting from chronic liver injury, progresses to hepatic dysfunction and portal hypertension, often culminating in decompensation. Among its most lethal complications is esophagogastric variceal bleeding (EGVB),1 which accounts for a significant proportion of acute upper gastrointestinal bleeding (AUGIB) cases, with an annual incidence of 10%–15%.2 EGVB is a critical clinical emergency characterized by massive hemorrhage and rapid hemodynamic collapse. Although management strategies for acute variceal bleeding (AVB) have evolved, mortality rates remain stubbornly between 15% and 20%.3,4 Notably, a UK cohort study found that AVB patients have significantly worse survival outcomes compared to those with non-variceal UGIB, underscoring their status as a distinct high-risk group.5 Consequently, the ability to rapidly stratify disease severity and predict prognosis is critical for optimizing therapeutic interventions.
Validated scoring systems enable early risk stratification to guide the clinical management of UGIB. Currently, key risk stratification tools used in UGIB research include the Rockall Score (RS),6 the Glasgow-Blatchford Score (GBS),7 the AIMS65 score (comprising albumin, International Normalized Ratio, altered mental status, systolic blood pressure, and age > 65 years),8 and the ABC score (based on age, blood tests, and comorbidities).9 The RS accurately predicts rebleeding and mortality10–13 but is limited by its complex calculation and reliance on endoscopic findings.14 The pre-endoscopic RS (pRS) avoids this limitation by excluding endoscopic results.6 The GBS performs well in predicting clinical interventions and mortality in UGIB;10,15 however, its calculation remains complex even without endoscopic data. The AIMS65 score was initially designed to evaluate mortality, hospital stay, and healthcare costs in patients with UGIB. Its ease of use makes it suitable for routine clinical practice.8 The ABC score, launched in 2020, is a novel system for assessing 30-day mortality in UGIB patients,9 incorporating six variables (age, blood tests, comorbidities) with a range of 0–18. Multiple studies support its good predictive value for mortality and rebleeding.16–20
Cirrhotic patients with UGIB are susceptible to infection, which elevates the risks of failed bleeding control, rebleeding, and mortality.21 The quick Sequential Organ Failure Assessment (qSOFA) score, introduced in 2016, is primarily used to assess the risk of rapid clinical deterioration in patients with sepsis and organ failure and is widely applied in emergency and critical care settings.22 Notably, recent guidelines from the European Association for the Study of the Liver (EASL) stress the value of the qSOFA score in the early identification of patients at high mortality risk.23 The qSOFA includes three indicators: respiratory rate, altered mental status, and systolic blood pressure.24 It can be calculated on admission without laboratory tests, is easy to memorize and compute, and applies to all emergency department patients.
Lactate is a glucose metabolite reflecting global tissue perfusion; insufficient perfusion elevates blood lactate levels, an indirect marker of hypoxia, hypoperfusion, and hemorrhagic shock severity, as well as a prognostic biomarker.25,26 Several studies have confirmed blood lactate levels as an important predictor of mortality in UGIB.14,27,28 In patients with severe liver cirrhosis, lactate is often used as an indicator of disease severity and organ failure, as well as an independent predictor of short-term mortality in patients with UGIB and liver failure.29 The combination of these two indicators appears effective for assessing the prognosis of patients with EGVB. Therefore, this study aimed to examine the predictive value of lactate level combined with the qSOFA score for rebleeding, ICU admission, and short-term mortality in patients with EGVB.
Materials and Methods
Patients
This single-center retrospective observational study consecutively enrolled 547 eligible cirrhotic patients with EGVB admitted to the Emergency Department of Beijing You’an Hospital between July 2022 and November 2022. The study protocol was approved by the Institutional Ethics Committee (Approval No. LL-2023-021-K).
The inclusion criteria were: (1) age ≥ 18 years; (2) diagnosis of cirrhosis and AUGIB;30 (3) EGVB verified as the bleeding source by clinical assessment or gastroscopy. The exclusion criteria were: (1) concurrent AUGIB caused by other etiologies; (2) cirrhosis complicated by lower gastrointestinal bleeding; (3) underlying hematological disorders; (4) incomplete clinical or laboratory data at admission, particularly missing blood lactate levels; and (5) treatment discontinuation or loss to follow-up.
Data Gathering
Information regarding patient characteristics was documented, including age, sex, bleeding symptoms, vital signs, comorbidities, results of endoscopic examinations, the need for ICU admission, occurrences of rebleeding, survival outcomes, and prior medical history. On the first day of hospitalization, blood gas analysis, whole blood leukocyte counts, and blood biochemistry were assessed. The qSOFA, pRS, GBS, AIMS65, and ABC scores were computed based on vital signs and laboratory data.
Outcome Variables
Rebleeding: Recurrent active hemorrhage occurring ≥72 hours after successful initial hemostasis, excluding persistent melena from the index event. The diagnosis required new-onset overt bleeding (hematemesis, melena, or hematochezia) accompanied by at least one of the following criteria: (1) a decrease in systolic blood pressure of >20 mmHg or an increase in heart rate of >20 beats/min; or (2) a decline in hemoglobin of ≥30 g/L without prior blood transfusion.
Follow-up: All 547 enrolled patients were followed for 6 weeks. Clinical outcomes, including ICU admission, rebleeding, and 6-week mortality, were retrospectively extracted from electronic medical records and documented telephone follow-up records.
Statistical Analysis
Continuous variables that follow a normal distribution are represented as mean ± standard deviation and analyzed using t-tests. In contrast, data that do not conform to a normal distribution are reported as median and compared using U-test. Categorical variables underwent chi-square testing for frequency comparisons. To identify independent predictors of clinical outcomes, logistic regression analysis is employed. Receiver operating characteristic (ROC) curves are generated to evaluate the predictive accuracy of the study scores. Survival probabilities over six weeks were visualized using Kaplan-Meier methodology. A two-sided significance threshold of p < 0.05 was applied throughout all statistical analyses.
Results
Characteristics of the Study Population
As illustrated in Figure 1, a total of 561 patients diagnosed with AUGIB were identified during the period from July 2022 to November 2022. Of these, 14 patients were excluded (11 due to incomplete data and 3 due to other causes of upper gastrointestinal bleeding), leaving 547 patients included in the study.
 |
Figure 1 Flowchart of the study population. |
The 547 patients with EGVB were categorized into two groups: those in the ICU (n=103) and those in non-ICU settings (n=444). Comparative analysis revealed statistically significant differences in all parameters across three main categories: vital signs (systolic blood pressure [SBP], shock index [SI]); laboratory indices, including white blood cell count (WBC), neutrophil percentage (NEUT%), hemoglobin (Hb), platelet count (PLT), aspartate aminotransferase (AST), total bilirubin (TBil), blood urea nitrogen (BUN), creatinine (Cr), estimated glomerular filtration rate (eGFR), serum sodium (Na+), prothrombin time (PT), prothrombin activity (PTA), and international normalized ratio (INR); and prognostic scores (qSOFA, pRS, GBS, AIMS65, ABC) (Table 1). Furthermore, participants were stratified by rebleeding status into rebleeding (n=103) and no-rebleeding (n=444) groups. Significant differences were observed between the two groups in heart rate (HR), SBP, Hb, lactate, pRS, AIMS65, and ABC score (Table 1). After a 6-week follow-up, statistically significant differences were observed between the survivor (n=464) and non-survivor groups (n=83) in male, age, SBP, WBC, NEUT%, Hb, PLT, alanine aminotransferase (ALT), AST, TBil, BUN, Cr, eGFR, Na+, PT, PTA, INR, Lac, qSOFA, SI, pRS, GBS, AIMS65, and ABC score (Table 1).
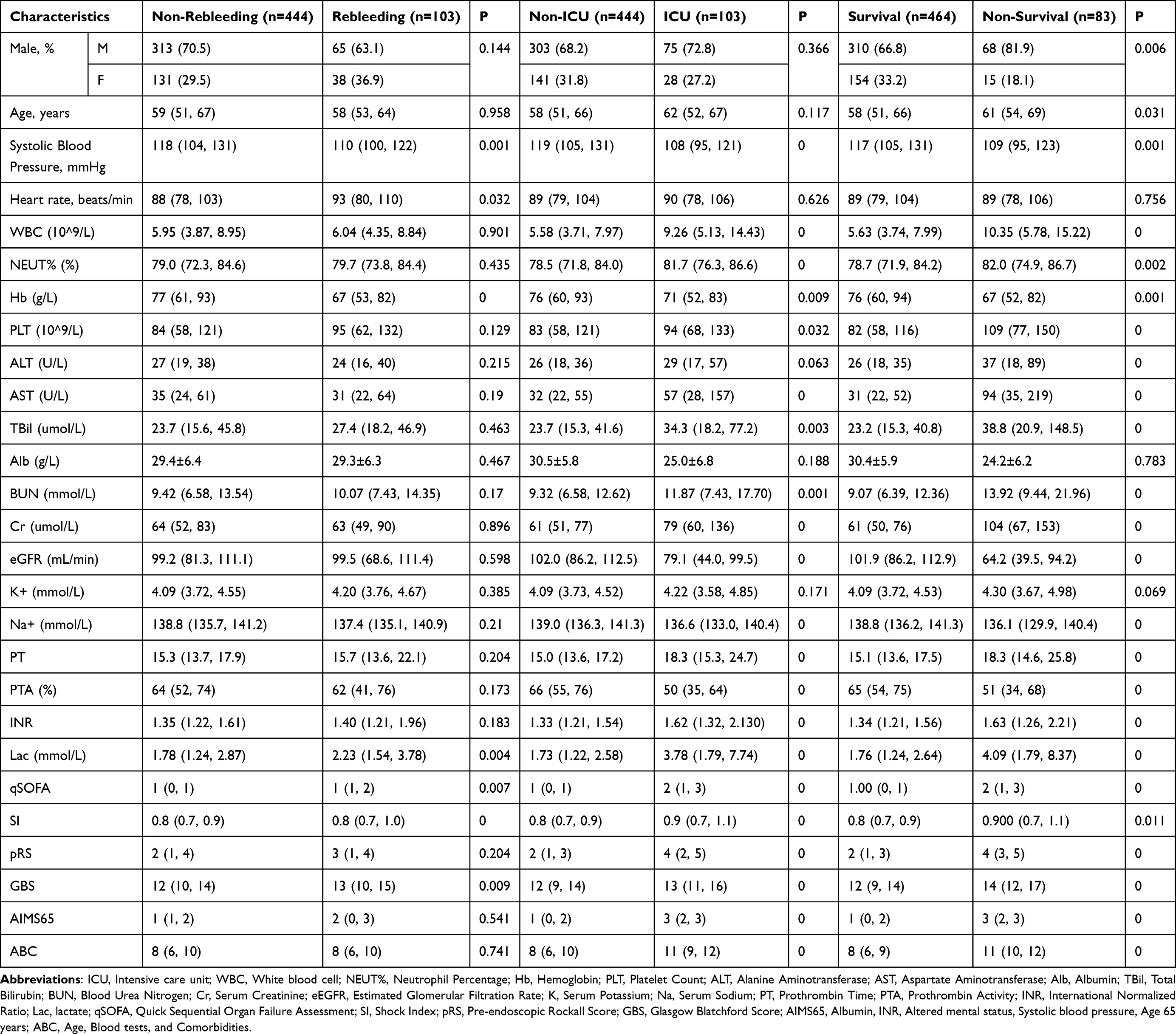 |
Table 1 Characteristics of the Study Population |
Logistic Regression Analysis of Clinical Outcomes in Patients with EGVB
Binary logistic regression was employed to identify independent predictors within our study cohort. For ICU admission, lactate (OR=1.180, 95% CI: 1.072–1.299, P=0.001), qSOFA (OR=1.788, 95% CI: 1.227–2.603, P=0.002), GBS (OR=0.911, 95% CI: 0.834–0.996, P=0.040), AIMS65 (OR=1.518, 95% CI: 1.125–2.048, P=0.006), and ABC score (OR=1.160, 95% CI: 1.001–1.345, P=0.048) were independent predictors (Table 2). Regarding the incidence of rebleeding, qSOFA (OR=1.400, 95% CI: 1.010–1.942, P=0.044) and GBS (OR=1.085, 95% CI: 1.003–1.174, P=0.042) emerged as significant predictors, whereas lactate did not reach statistical significance (OR=0.987, 95% CI: 0.904–1.078, P=0.773) (Table 2). Finally, for 6-week mortality, lactate (OR=1.154, 95% CI: 1.044–1.276, P=0.005), qSOFA (OR=1.722, 95% CI: 1.131–2.620, P=0.011), and ABC score (OR=1.418, 95% CI: 1.199–1.678, P<0.001) were identified as independent risk factors (Table 2).
 |
Table 2 Binary Logistic Regression Analysis of Clinical Outcomes in Patients with EGVB |
Prediction of Prognostic Outcomes for EGVB Patients
For predicting rebleeding, the AUC values for pRS, GBS, AIMS65, ABC, and Lac+qSOFA were 0.540, 0.582, 0.519, 0.510 and 0.564, respectively. Pairwise comparisons revealed no statistically significant differences between the Lac+qSOFA score and any of the other four scoring systems (Figure 2 and Table 3). Furthermore, the AUC values of pRS, GBS, AIMS65, ABC, and Lac+qSOFA scores for ICU admission were 0.723, 0.623, 0.787, 0.760 and 0.808, respectively. The Lac+qSOFA score demonstrated the highest discriminatory ability; however, pairwise comparisons revealed that this superiority was statistically significant only when compared to pRS and GBS (both P < 0.05). No significant differences were observed between Lac+qSOFA and the other high-performing scores (AIMS65 and ABC). At the optimal cut-off value of >0.211, the Lac+qSOFA score yielded a sensitivity of 66.99%, specificity of 82.88%, positive predictive value (PPV) of 47.6%, and negative predictive value (NPV) of 91.5% (Figure 2 and Table 3). Regarding 6-week mortality, the AUC values of the pRS, GBS, AIMS65, ABC, and Lac+qSOFA scores were 0.759, 0.715, 0.817, 0.834 and 0.818, respectively. Notably, the Lac+qSOFA score demonstrated outstanding predictive accuracy, performing comparably to the numerically highest score, ABC (0.834), as well as AIMS65 (0.817). In contrast, traditional scores such as pRS and GBS exhibited significantly lower discrimination. Crucially, pairwise comparisons confirmed that Lac+qSOFA was statistically superior to GBS (P < 0.05) while showing no significant difference from the top-performing ABC and AIMS65 scores. The cut-off values for Lac+qSOFA was >0.210 (sensitivity 65.06%, specificity 87.07%, PPV 47.4%, and NPV 93.3%) (Figure 2 and Table 3).
 |
Table 3 The ROC Curve in Predicting Rebleeding, ICU-Admission, and 6-Week Mortality in Patients with EGVB |
 |
Figure 2 The ROC curves for various scoring systems used to predict outcomes in cirrhosis patients with EGVB. (A) The ROC curves for different scoring systems predicting rebleeding; (B) The ROC curves for different scoring systems predicting ICU admission; (C) The ROC curves for different scoring systems predicting 6-week mortality. |
Patients’ 6-Week Survival
To demonstrate the capacity of the Lac+qSOFA score for risk stratification in EGVB patients, a comparison of survival using Kaplan–Meier curves was performed. EGVB patients with Lac+qSOFA score above the cutoff (0.21) had significantly lower survival compared to those with scores below this cutoff (P < 0.001) (Figure 3).
 |
Figure 3 Kaplan-Meier curves for Lac+qSOFA in cirrhosis patients with EGVB at the 6-Week follow-up. |
Discussion
EGVB represents a critical decompensation event in cirrhotic patients, accounting for 25–35% of cirrhosis-related mortality.3,4,31,32 Although standardized hemostatic protocols and endoscopic advances have reduced 30-day mortality rates from 30% to 14–20% over the past decade, therapeutic failure persists in 10–15% of cases, with associated mortality exceeding 80%.33–35 Alarmingly, more than 60% of survivors experience rebleeding within 12–24 months due to inadequate secondary prophylaxis. The 6-week mortality rate remains approximately 20%, predominantly due to hepatorenal syndrome and sepsis.36 Current consensus guidelines emphasize 6-week rebleeding and mortality rates as pivotal endpoints for assessing AUGIB outcomes.2,36 Endoscopy and related interventions are crucial for patients with UGIB. However, timely endoscopic access is often delayed globally. In the United Kingdom, only 52% of hospitals provide endoscopy services outside regular hours, and only 50% of patients can access endoscopy within 24 hours.37 Patients with liver cirrhosis often have multiple complications and poor overall health, sometimes rendering them unable to tolerate endoscopy. Additionally, in most healthcare facilities, critical decisions regarding patient management are made in the emergency department.38 Therefore, non-endoscopic scoring systems are clinically valuable, especially in emergency settings.
Rebleeding is an important prognostic outcome in patients with cirrhosis. In a study of 154 ICU patients, lactate clearance was found to be useful for detecting active bleeding.39 A study of 442 cirrhotic patients with UGIB found that qSOFA had value in predicting rebleeding.21 In our study, qSOFA and GBS were independent predictors of 6-week rebleeding in EGVB patients, but lactate was not. The AUC of Lac+qSOFA was 0.564, which was higher than that of pRS (0.540), AIMS65 (0.519), and ABC (0.510), but slightly lower than that of GBS (0.582). Only the AUC difference between Lac+qSOFA and GBS was statistically significant (P < 0.05). Therefore, both Lac+qSOFA and GBS have limited predictive value for 6-week rebleeding, with GBS showing slightly superior performance. Multiple recent studies have also suggested that pRS, GBS, and AIMS65 scores are unable to effectively predict 30-day rebleeding risk in AUGIB patients,10,36,40,41 which aligns with our findings. However, Motola-Kuba et al42 found that GBS could effectively predict AVB rebleeding risk, with an AUC of 0.756, significantly higher than RS (0.691) and AIMS65 (0.664). Ky et al16 demonstrated that the ABC score exhibited good predictive value for early rebleeding in patients with EGVB, with an AUC of 0.744. This limited predictive value may be attributed to several factors. First, rebleeding after EGVB is primarily determined by variceal-specific features (eg, variceal size, red wale marks) and portal pressure, which are not reflected in either lactate or qSOFA. Second, lactate primarily indicates tissue hypoperfusion and shock severity, which correlate more closely with mortality than with rebleeding risk. Third, impaired hepatic lactate clearance in cirrhotic patients may lead to elevated baseline levels, reducing its discriminatory value for rebleeding. In conclusion, Lac+qSOFA did not fully capture variceal-specific risk factors, which explains its limited predictive value for rebleeding in patients with EGVB.2,23
For predicting ICU admission, Shrestha et al26 found that patients with elevated lactate levels were more likely to require ICU admission than those with normal lactate levels. Consequently, lactate measurement may serve as a valuable supplementary tool in the triage process for patients with AUGIB. Kim et al14 demonstrated that lactate levels remain an important predictor of ICU admission in cirrhotic patients with AUGIB. Similarly, studies have shown that the qSOFA score is an effective tool for predicting the need for intensive care and mortality risk in various medical conditions, including sepsis and pneumonia.43,44 In our study, lactate, qSOFA, GBS, AIMS65, and ABC all independently predicted ICU admission. However, the AUC of Lac+qSOFA for predicting ICU admission was significantly higher than that of the other four scoring systems (P < 0.05), suggesting that Lac+qSOFA has superior predictive ability for ICU admission. Taslidere et al45 found that qSOFA outperformed GBS (0.856), RS (0.828), and pRS (0.796) for predicting the need for intensive care, achieving an AUC of 0.92. Lai et al21 found that qSOFA was comparable to AIMS65 for predicting ICU admission and better than GBS, but no combined score was evaluated in that study. The superior predictive ability of Lac+qSOFA for ICU admission may be attributed to its comprehensive capture of hemodynamic and metabolic dysfunction. Rapid hemodynamic evaluation is crucial in UGIB management, particularly in massive bleeding scenarios. When approximately 30% of intravascular volume is lost, patients develop hypovolemic shock, a critical prognostic indicator associated with multi-organ failure and increased mortality.46 The qSOFA score incorporates three key parameters used in staging hypovolemic shock: respiratory rate (reflecting compensatory mechanisms), blood pressure (indicating circulatory compromise), and mental status (signifying cerebral perfusion).45 Lactate complements these clinical variables by providing an objective biochemical marker of tissue hypoxia and hypoperfusion that precedes overt hemodynamic collapse. This explains why Lac+qSOFA demonstrated superior predictive ability for ICU admission compared to some individual scoring systems. Lac+qSOFA offers clear advantages in emergency triage: rapid, straightforward assessment without endoscopy or complex laboratory tests, facilitating early risk stratification. This is especially valuable in resource-limited settings with scarce ICU beds.
For predicting 6-week mortality, research has indicated a correlation between elevated lactate levels and increased mortality in patients with AUGIB.27,28,47 Gulen et al25 confirmed that lactate is helpful in predicting mortality in patients with UGIB. Bagin et al48 demonstrated that qSOFA was strongly associated with mortality in patients with UGIB. Our study showed that lactate, qSOFA, and ABC score were independent predictors of 6-week mortality. The AUC of Lac+qSOFA was 0.818, higher than that of pRS (0.759), GBS (0.715), and AIMS65 (0.817), but slightly lower than ABC score (0.834). The difference between Lac+qSOFA and ABC score was not statistically significant (P > 0.05). The AUC values of these five scores were between 0.7–0.9, which indicated that the five scoring systems had a certain degree of accuracy in the prediction of death within 6 weeks. Laursen et al9 found that compared to previous scoring systems, ABC score demonstrated good performance in predicting mortality from UGIB. In our study, although Lac+qSOFA showed a slightly lower AUC than the ABC score, the difference was not statistically significant. Given that the ABC score requires comorbidity data that may not be immediately available in emergency settings, Lac+qSOFA can serve as a practical alternative for mortality prediction in patients with UGIB.
Limitations
First, the single-center retrospective design limits the generalizability of our findings. Second, variceal-specific risk factors (eg, variceal size, red wale marks) were not collected, which may have affected rebleeding prediction accuracy. Third, dynamic lactate changes were not assessed; assessment of these changes may have improved prognostic accuracy. Finally, the 6-week follow-up period did not capture long-term outcomes such as 1-year rebleeding or mortality.
Conclusion
Our study shows that while the combination of lactate and qSOFA has limited value in predicting rebleeding in cirrhotic patients with EGVB, it performs significantly better for estimating 6-week mortality and ICU admission. The key advantage of this combined metric lies in its practicality: it relies exclusively on rapidly available bedside data, without the need for endoscopy, which makes it an ideal tool for early risk stratification in emergency settings. Given its simplicity and reliable prognostic performance, we support broader use of this score in routine clinical practice and encourage future multicenter prospective studies to validate the optimal lactate cutoff value and explore the role of serial lactate measurements in clinical decision-making.
Data Sharing Statement
The data employed in this study can be obtained from the corresponding author upon request.
Statement of Ethics
This retrospective study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Beijing You’an Hospital (LL-2023-021-K). Given the retrospective nature of the investigation and complete anonymization of participant data, the ethics panel determined written patient consent wasn’t mandatory for this analysis.
Acknowledgments
We express our sincere appreciation to Beijing You’an Hospital for their support in enabling the conduct of this study. Additionally, we wish to recognize the contributions of all data collectors, supervisors, and participants involved in the research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Wang Z, Hu HS, Zhao LM, et al. Effectiveness of prophylactic antibacterial drugs for patients with liver cirrhosis and upper gastrointestinal bleeding: a systematic review and meta-analysis. Front Pharmacol. 2024;15:1324848. doi:10.3389/fphar.2024.1324848
2. Garcia-Tsao G, Abraldes JG, Berzigotti A, et al. Portal hypertensive bleeding in cirrhosis: risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology. 2017;65(1):310–13. doi:10.1002/hep.28906
3. Zhou YF, Xu Y, Ding YF, et al. Novel nomogram model for predicting 6-week mortality in liver cirrhosis patients with acute upper gastrointestinal bleeding. J Dig Dis. 2022;23(8–9):516–526. doi:10.1111/1751-2980.13137
4. Diaz-Soto MP, Garcia-Tsao G. Management of varices and variceal hemorrhage in liver cirrhosis: a recent update. Therap Adv Gastroenterol. 2022;15:1098284688. doi:10.1177/17562848221101712
5. Hearnshaw SA, Logan RF, Lowe D, et al. Acute upper gastrointestinal bleeding in the UK: patient characteristics, diagnoses and outcomes in the 2007 UK audit. Gut. 2011;60(10):1327–1335. doi:10.1136/gut.2010.228437
6. Rockall TA, Logan RF, Devlin HB, et al. Risk assessment after acute upper gastrointestinal haemorrhage. Gut. 1996;38(3):316–321. doi:10.1136/gut.38.3.316
7. Blatchford O, Murray WR, Blatchford M. A risk score to predict need for treatment for upper-gastrointestinal haemorrhage. Lancet. 2000;356(9238):1318–1321. doi:10.1016/S0140-6736(00)02816-6
8. Saltzman JR, Tabak YP, Hyett BH, et al. A simple risk score accurately predicts in-hospital mortality, length of stay, and cost in acute upper GI bleeding. Gastrointest Endosc. 2011;74(6):1215–1224. doi:10.1016/j.gie.2011.06.024
9. Laursen SB, Oakland K, Laine L, et al. ABC score: a new risk score that accurately predicts mortality in acute upper and lower gastrointestinal bleeding: an international multicentre study. Gut. 2021;70(4):707–716. doi:10.1136/gutjnl-2019-320002
10. Stanley AJ, Laine L, Dalton HR, et al. Comparison of risk scoring systems for patients presenting with upper gastrointestinal bleeding: international multicentre prospective study. BMJ. 2017;356:i6432. doi:10.1136/bmj.i6432
11. Kim MS, Choi J, Shin WC. AIMS65 scoring system is comparable to Glasgow-Blatchford score or Rockall score for prediction of clinical outcomes for non-variceal upper gastrointestinal bleeding. BMC Gastroenterol. 2019;19(1):136. doi:10.1186/s12876-019-1051-8
12. Lu M, Sun G, Huang H, et al. Comparison of the Glasgow-Blatchford and Rockall Scores for prediction of nonvariceal upper gastrointestinal bleeding outcomes in Chinese patients. Medicine. 2019;98(21):e15716. doi:10.1097/MD.0000000000015716
13. Brullet E, Garcia-Iglesias P, Calvet X, et al. Endoscopist’s judgment is as useful as risk scores for predicting outcome in peptic ulcer bleeding: a multicenter study. J Clin Med. 2020;9(2):408. doi:10.3390/jcm9020408
14. Kim D, Jo S, Lee JB, et al. Comparison of the National Early Warning Score+Lactate score with the pre-endoscopic Rockall, Glasgow-Blatchford, and AIMS65 scores in patients with upper gastrointestinal bleeding. Clin Exp Emerg Med. 2018;5(4):219–229. doi:10.15441/ceem.17.268
15. Ak R, Hokenek NM. Comparison of AIMS65 and Glasgow Blatchford scores in predicting mortality in patients with upper gastrointestinal bleeding. Rev Assoc Med Bras. 2021;67(5):766–770. doi:10.1590/1806-9282.20210580
16. Ky TD, Trang NTH, Binh MT. Predictive significance of the ABC score for early re-hemorrhage and in-hospital mortality in high-risk variceal bleeding among cirrhotic patients. Diagnostics. 2023;13(23):3570. doi:10.3390/diagnostics13233570
17. Kherad O, Restellini S, Almadi M, et al. Comparative evaluation of the ABC score to other risk stratification scales in managing high-risk patients presenting with acute upper gastrointestinal bleeding. J Clin Gastroenterol. 2023;57(5):479–485. doi:10.1097/MCG.0000000000001720
18. Saade MC, Kerbage A, Jabak S, et al. Validation of the new ABC score for predicting 30-day mortality in gastrointestinal bleeding. BMC Gastroenterol. 2022;22(1):301. doi:10.1186/s12876-022-02374-y
19. Marmo R, Soncini M, Bucci C, et al. Comparison of assessment tools in acute upper gastrointestinal bleeding: which one for which decision. Scand J Gastroenterol. 2022;57(1):1–7. doi:10.1080/00365521.2021.1976268
20. Liu S, Zhang X, Walline JH, et al. Comparing the performance of the ABC, AIMS65, GBS, and pRS scores in predicting 90-day mortality or rebleeding among emergency department patients with acute upper gastrointestinal bleeding: a prospective multicenter study. J Transl Int Med. 2021;9(2):114–122. doi:10.2478/jtim-2021-0026
21. Lai YC, Hung MS, Chen YH, et al. Comparing AIMS65 score with MEWS, qSOFA score, glasgow-blatchford score, and rockall score for predicting clinical outcomes in cirrhotic patients with upper gastrointestinal bleeding. J Acute Med. 2018;8(4):154–167. doi:10.6705/j.jacme.201812_8(4).0003
22. Seymour CW, Liu VX, Iwashyna TJ. Assessment of clinical criteria for sepsis: for the third international consensus definitions for Sepsis and Septic Shock (Sepsis-3) (vol 315, pg 762, 2016). JAMA. 2016;20:315.
23. Angeli P, Bernardi M, Villanueva C, et al; Liver E A F T. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018;69(2):406–460.
24. Koch C, Edinger F, Fischer T, et al. Comparison of qSOFA score, SOFA score, and SIRS criteria for the prediction of infection and mortality among surgical intermediate and intensive care patients. World J Emerg Surg. 2020;15(1):63. doi:10.1186/s13017-020-00343-y
25. Gulen M, Satar S, Tas A, et al. Lactate level predicts mortality in patients with upper gastrointestinal bleeding. Gastroenterol Res Pract. 2019;2019:5048078. doi:10.1155/2019/5048078
26. Shrestha MP, Borgstrom M, Trowers EA. Elevated lactate level predicts intensive care unit admissions, endoscopies and transfusions in patients with acute gastrointestinal bleeding. Clin Exp Gastroenterol. 2018;11:185–192. doi:10.2147/CEG.S162703
27. El-Kersh K, Chaddha U, Sinha RS, et al. Predictive role of admission lactate level in critically ill patients with acute upper gastrointestinal bleeding. J Emerg Med. 2015;49(3):318–325. doi:10.1016/j.jemermed.2015.04.008
28. Koch A, Buendgens L, Duckers H, et al. [Bleeding origin, patient-related risk factors, and prognostic indicators in patients with acute gastrointestinal hemorrhages requiring intensive care treatment. A retrospective analysis from 1999 to 2010]. Med Klin Intensivmed Notfmed. 2013;108(3):214–222. Swedish. doi:10.1007/s00063-013-0226-2
29. Laursen SB, Dalton HR, Murray IA, et al. Performance of new thresholds of the Glasgow Blatchford score in managing patients with upper gastrointestinal bleeding. Clin Gastroenterol Hepatol. 2015;13(1):115–121. doi:10.1016/j.cgh.2014.07.023
30. Tandon P, Bishay K, Fisher S, et al. Comparison of clinical outcomes between variceal and non-variceal gastrointestinal bleeding in patients with cirrhosis. J Gastroenterol Hepatol. 2018;33(10):1773–1779. doi:10.1111/jgh.14147
31. Magaz M, Baiges A, Hernandez-Gea V. Precision medicine in variceal bleeding: are we there yet? J Hepatol. 2020;72(4):774–784. doi:10.1016/j.jhep.2020.01.008
32. Qi X, Li Y, Li B, et al. Timing of endoscopy in cirrhotic patients with acute variceal bleeding: protocol of a multicenter randomized controlled trial. Therap Adv Gastroenterol. 2024;17:1118478428. doi:10.1177/17562848241295452
33. Carbonell N, Pauwels A, Serfaty L, et al. Improved survival after variceal bleeding in patients with cirrhosis over the past two decades. Hepatology. 2004;40(3):652–659. doi:10.1002/hep.20339
34. Zhao H, Zhao R, Hu J, et al. Upper gastrointestinal hemorrhage in acute-on-chronic liver failure: prevalence, characteristics, and impact on prognosis. Expert Rev Gastroenterol Hepatol. 2019;13(3):263–269. doi:10.1080/17474124.2019.1567329
35. D’Amico G, Garcia-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol. 2006;44(1):217–231. doi:10.1016/j.jhep.2005.10.013
36. Xu X, Tang C, Linghu E, et al. Guidelines for the management of esophagogastric variceal bleeding in cirrhotic portal hypertension. J Clin Transl Hepatol. 2023;11(7):1565–1579. doi:10.14218/JCTH.2023.00061
37. Hearnshaw SA, Logan RF, Lowe D, et al. Use of endoscopy for management of acute upper gastrointestinal bleeding in the UK: results of a nationwide audit. Gut. 2010;59(8):1022–1029. doi:10.1136/gut.2008.174599
38. Redondo-Cerezo E, Vadillo-Calles F, Stanley AJ, et al. MAP(ASH): a new scoring system for the prediction of intervention and mortality in upper gastrointestinal bleeding. J Gastroenterol Hepatol. 2020;35(1):82–89. doi:10.1111/jgh.14811
39. Wada T, Hagiwara A, Uemura T, et al. Early lactate clearance for predicting active bleeding in critically ill patients with acute upper gastrointestinal bleeding: a retrospective study. Intern Emerg Med. 2016;11(5):737–743. doi:10.1007/s11739-016-1392-z
40. Curdia GT, Barbosa M, Xavier S, et al. Optimizing the risk assessment in upper gastrointestinal bleeding: comparison of 5 scores predicting 7 outcomes. GE Port J Gastroenterol. 2018;25(6):299–307. doi:10.1159/000486802
41. Chang A, Ouejiaraphant C, Akarapatima K, et al. Prospective comparison of the AIMS65 score, glasgow-blatchford score, and rockall score for predicting clinical outcomes in patients with variceal and nonvariceal upper gastrointestinal bleeding. Clin Endosc. 2021;54(2):211–221. doi:10.5946/ce.2020.068
42. Motola-Kuba M, Escobedo-Arzate A, Tellez-Avila F, et al. Validation of prognostic scores for clinical outcomes in cirrhotic patients with acute variceal bleeding. Ann Hepatol. 2016;15(6):895–901. doi:10.5604/16652681.1222107
43. Goulden R, Hoyle MC, Monis J, et al. qSOFA, SIRS and NEWS for predicting inhospital mortality and ICU admission in emergency admissions treated as sepsis. Emerg Med J. 2018;35(6):345–349. doi:10.1136/emermed-2017-207120
44. Tokioka F, Okamoto H, Yamazaki A, et al. The prognostic performance of qSOFA for community-acquired pneumonia. J Intensive Care. 2018;6(1):46. doi:10.1186/s40560-018-0307-7
45. Taslidere B, Sonmez E, Ozcan AB, et al. Comparison of the quick SOFA score with Glasgow-Blatchford and Rockall scores in predicting severity in patients with upper gastrointestinal bleeding. Am J Emerg Med. 2021;45:29–36. doi:10.1016/j.ajem.2021.02.016
46. Cannon JW, Longo DL. Hemorrhagic Shock. N Engl J Med. 2018;378(4):370–379. doi:10.1056/NEJMra1705649
47. Shah A, Chisolm-Straker M, Alexander A, et al. Prognostic use of lactate to predict inpatient mortality in acute gastrointestinal hemorrhage. Am J Emerg Med. 2014;32(7):752–755. doi:10.1016/j.ajem.2014.02.010
48. Bagin V, Tarasov E, Astafyeva M, et al. Quick SOFA vs Rockall preendoscopy scores for risk assessment in patients with nonvariceal upper gastrointestinal bleeding: a retrospective cohort study. Int J Emerg Med. 2019;12(1):10. doi:10.1186/s12245-019-0229-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparing the Prognostic Value of Lactate to the Neutrophil to Lymphocyte Ratio Among Sepsis Patients: A Prospective Cohort Study
Bou Chebl R, Haidar S, Kattouf N, Assaf M, Alwan JS, Khamis MM, Abdeldaem K, Makki M, Tamim H, Abou Dagher G
Open Access Emergency Medicine 2025, 17:3-13
Published Date: 20 January 2025