Back to Journals » International Journal of General Medicine » Volume 14
Predictive Value of Laboratory Indexes on Renal Involvement in Children with Henoch-Schönlein Purpura
Authors Xi L, Xu S, Jiang Y ![]() , Su H, Sun Y, Wen Y, Wu J, Ren X
, Su H, Sun Y, Wen Y, Wu J, Ren X ![]()
Received 4 September 2021
Accepted for publication 19 October 2021
Published 9 November 2021 Volume 2021:14 Pages 7951—7959
DOI https://doi.org/10.2147/IJGM.S337437
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Leying Xi,1 Shuang Xu,2 Yingying Jiang,2 Hang Su,2 Yuying Sun,2 Yingying Wen,2 Jingjing Wu,2 Xianqing Ren2
1Department of Pediatrics, Nanjing Hospital of Chinese Medicine Affiliated to Nanjing University of Chinese Medicine, Nanjing, Jiangsu, People’s Republic of China; 2Department of Pediatrics, The First Affiliated Hospital of Henan University of Chinese Medicine, Zhengzhou, Henan, People’s Republic of China
Correspondence: Xianqing Ren
Department of Pediatrics, The First Affiliated Hospital of Henan University of Chinese Medicine, No. 9 Renmin Road, Jinshui District, Zhengzhou, Henan Province, 450000, People’s Republic of China
Tel +86 13673712698
Email [email protected]
Objective: Henoch–Schönlein purpura (HSP) is the most common vasculitis in children. Renal involvement is the main long-term complication of HSP, and presently there is no way to predict which children may have irreversible renal damage from the outset. This study aimed to explore the prediction value of laboratory indexes on renal involvement in children with HSP, which could help the early identification and intervention.
Methods: Children with HSP hospitalized at the First Affiliated Hospital of Henan University of Chinese Medicine from June 2019 to December 2020 were included. The demographic findings, clinical features, laboratory findings including blood routine examination, serum immunoglobulin, complement, T cell subsets levels, liver and kidney function, coagulation function were recorded. Laboratory indexes were analyzed, logistic regression analysis was performed to identify the independent predictors in HSP patients with renal involvement, and receiver operating characteristic (ROC) curves were further used to assess the value of prediction indexes, as well as the efficacy of combined diagnosis.
Results: The study included 146 HSP patients, among them, 50 patients (34.2%) had renal involvement. Age, platelet distribution width (PDW), CD3+ and fibrinogen (FIB) were positively correlated with renal involvement, while the levels of Immunoglobulin G (IgG), C-reactive protein (CRP), and neutrophil/lymphocyte ratio (NLR) were negatively correlated with renal involvement. The area under the ROC Curve (AUC) of these biomarkers ranged from 0.6284 to 0.7009, and among the combinations, a combination of NLR, CRP, CD3+, FIB, PDW, IgG and age had the best AUC value (0.9774).
Conclusion: Age, PDW, CD3+, FIB, CRP, NLR and IgG were prediction indexes for renal involvement in HSP patients, and these indexes can be combined appropriately to improve the diagnostic efficacy.
Keywords: Henoch–Schönlein purpura, laboratory indexes, renal involvement, diagnosis
Introduction
Henoch–Schönlein purpura (HSP) is the most common vasculitis in children. The typical manifestations of HSP are palpable purpura (without thrombocytopenia), abdominal pain, gastrointestinal bleeding, arthritis and renal disease, with the deposition of circulatory IgA immune complexes in the affected tissue.1 Based on the characteristics of abnormal deposition of IgA in affected vessel walls, HSP is also known as IgA vasculitis (IgAV).2 The incidence of children with HSP is about 3–26.7/1,000,000; however, the incidence may be underestimated due to underreporting.3 Although the pathogenesis of HSP remains unknown, infection, food/drug allergy, immune disorders, inflammatory mechanisms, and coagulation disturbances are believed to take part in the HSP pathogenesis.
Approximately 20–60% of pediatric patients develop nephritis in conjunction with hematuria/proteinuria, which is defined as Henoch–Schönlein purpura nephritis (HSPN). It usually occurs within 30–60 days after the initial symptom of HSP and is the most serious long-term complication of HSP, and the severity of renal damage is the principal determinant of the prognosis of HSP.4,5 Impaired renal function, hypoproteinemia, hypertension and long-term renal residual sequelae may occur in the late stage of HSPN.6 Therefore, identifying those who are at great risk of renal injury at an early stage is considered to be the key to reducing the incidence of renal injury, and would be very helpful in allowing a personalized approach to monitoring. Although HSP/HSPN is still diagnosed with symptoms and signs, together with some histopathological findings, the gold standard for diagnosis depends on renal biopsy which is invasive, the development of less invasive and disease-specific laboratory indexes with diagnostic value in the early stage of HSP is needed.
The clinical features and laboratory examination indexes (routine blood examination, serum immunoglobulin, complement, T cell subset levels, liver and kidney function, coagulation function) in HSP and HSPN patients were compared in our study. We aim to explore laboratory and clinical indexes that can predict the renal involvement in HSP, in order to achieve early diagnosis and prompt treatment.
Materials and Methods
Patients Selection
This retrospective observational study was conducted at the First Affiliated Hospital of Henan University of Chinese Medicine from June 2019 to December 2020, 146 HSP inpatients (including 50 HSPN patients) were included. HSP patients were diagnosed based on the European League Against Rheumatism/Paediatric Rheumatology International Trials Organisation/Paediatric Rheumatology European Society (EULAR/PRINTO/PRES) criteria:7 non-thrombocytopenia palpable purpura combined with any of the following characterizations: 1. Diffuse abdominal pain; 2. Typical predominant IgA deposits; 3. Arthritis or arthralgias; 4. Renal involvement. Renal involvement was defined as proteinuria (protein concentration >0.3g/24h) and/or hematuria (>5 red blood cells/high power field or ≥2+ on dipstick). Inclusion criteria were age≤18 years old, a clinical diagnosis of HSP based on EULAR/PRINTO/PRES criteria, and no medication before the blood examination. Patients with other autoimmune diseases, anemia, nephrotic syndrome, idiopathic thrombocytopenic purpura and missing laboratory data were excluded. All participants and their parents/guardians were informed about the purpose of the study and provided informed consent. The study was approved by the local ethics committee (2021HL-103-02) and followed the principles of the Declaration of Helsinki.
Clinical Data Collection
Medical records of the HSP patients were reviewed. Laboratory parameters including blood routine examination: white blood cell (WBC), lymphocyte and neutrophil count/percentage (#/%LYMPH, #/%NEUT), red blood cell count (RBC), platelet (PLT), eosinophilic granulocyte count/percentage (#/%EOS), neutrophil/lymphocyte ratio (NLR), hemoglobin (HGB), platelet/lymphocyte ratio (PLR), Platelet Distribution Width (PDW), mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), mean platelet volume (MPV), procalcitonin (PCT), red blood cell distribution width (RDW), and C-reactive protein (CRP), serum immunoglobulin: IgE, IgA, IgM, and IgG, complement: C3 and C4, and T cell subset levels: the percentage of CD3+ cells, CD3+CD4+ cells, CD3+CD8+, and CD4/CD8, liver and kidney function: total protein (TP), alanine aminotransferase (ALT), albumin (ALB), aspartate aminotransferase (AST), urine creatinine (Cr), blood urea nitrogen (BUN), and uric acid (UA), coagulation function: prothrombin time (PT), fibrinogen (FIB), activated partial thromboplastin (APTT), thrombin time (TT), and d-dimer (DD). Laboratory examination analyses were performed in the laboratory of our hospital.
Statistical Analysis
Statistical analyses were performed using GraphPad Prism version 8.4.2 (GraphPad Software corporation, California, USA). Quantitative data were shown as means ± SD or median (minimum-maximum). Mann–Whitney U-test or Student’s t-test was used to detect differences of continuous variables between the two groups. Categorical variables were shown as percentages and compared by the Chi-square test or Fisher’s exact test. The independent predictors of HSP patients with renal involvement were identified by logistic regression analysis, and the odds ratios (ORs) with 95% confidence intervals (95% CI) were also calculated. In addition, ROC curves were performed to further assess the value of prediction indexes, as well as the efficacy of combined diagnosis. Results were considered statistically significant when P<0.05 (two-tailed).
Results
Baseline Characteristics of Patients
A total of 146 patients were enrolled and evaluated in this study, including 96 HSP patients (51 female, 45 male, mean age 9.563±3.254 years) and 50 HSPN patients (25 female, 25 male, mean age 10.96±3.084 years). No differences between the groups in sex (P>0.05). Among the 146 patients, 146 (100.0%) had palpable purpura, 61 (41.8%) had gastrointestinal involvement, 68 (46.6%) had arthralgia, and 50 (34.2%) had renal involvement (Table 1). The median age of HSPN patients was 10 (9 to 14) years, the female/male ratio was 1:1, the median age of HSP patients without renal involvement was 9 (7 to 12) years and the female/male ratio was 1.13:1.
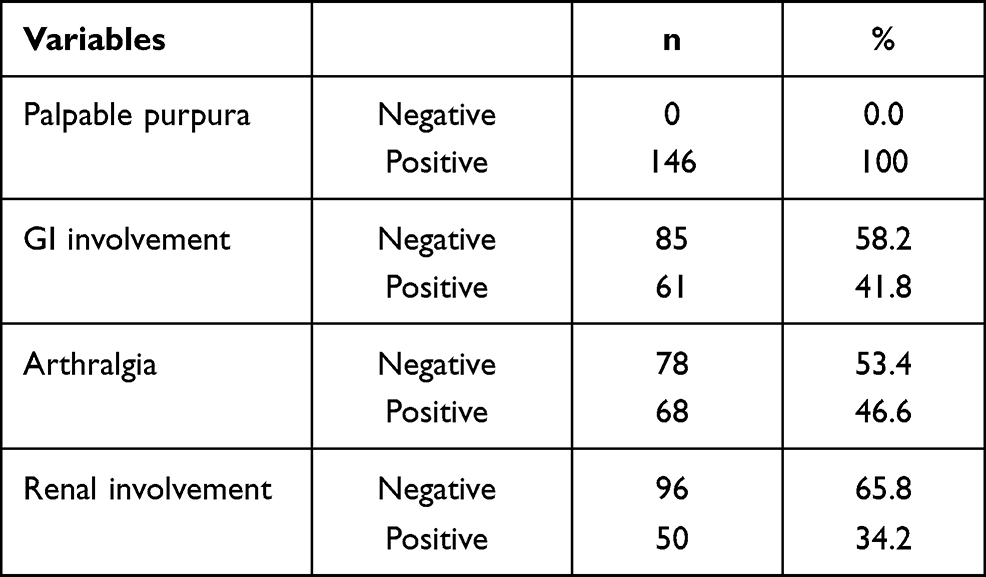 |
Table 1 Clinical Manifestation of 146 HSP Patients |
Among the 50 patients with renal injury, 1 had nephrotic range proteinuria, 34 had non-nephrotic proteinuria, and 15 had only hematuria. In the present study, 8 patients (16%) had renal involvement when diagnosed, 30 (60%) patients had renal involvement in the first month, 6 patients (12%) between the first and the second month, 5 patients (10%) between the second and the sixth month, 1 patient (2%) developed renal injury after 6 months. The mean time for the development of renal involvement was 33.02 days. Renal biopsy was performed on 14 patients (1 had nephrotic range proteinuria, 13 had non-nephrotic proteinuria). Biopsy samples showed: 1 case of normal light microscopy (stage 1), 2 cases of mesangial proliferation only without crescents (stage 2), 11 cases of focal or diffuse proliferation with <50% crescentic glomeruli (stage 3). No renal function damage or renal failure was observed.
Blood Routine Tests in HSP and HSPN Patients
The levels of WBC (8.275±4.632 vs 6.525±2.330), NLR (2.932±3.428 vs 1.384±0.847), MCHC (334.9±9.629 vs 330.5±13.84), and CRP (4.111±4.547 vs 1.704±2.951) in HSP patients without renal involvement were higher than those patients with renal involvement (P=0.03, 0.039, 0.014, and 0.01, respectively). EO% (1.723±1.673 vs 2.042±1.306), MPV (8.744±1.579 vs 9.097±1.043), PDW (13.95±2.110 vs 15.28±1.745) levels in HSP patients were significantly lower than in HSPN patients (P=0.046, 0.008, and 0.002, respectively). There were no significant differences in terms of lymphocyte count (3.387±6.203 vs 2.570±1.037), neutrophil count (6.485±9.733 vs 3.569±2.320), PLT (286.8±86.16 vs 282.2±88.41), RBC (4.597±0.5208 vs 4.668±0.5031), HGB (133.8±12.78 vs 133.0±15.23), and PLR (126.2±69.30 vs 114.9±44.07) between the groups (P>0.05). The leukocyte, neutrophil, monocyte, lymphocyte, MCV, MPV, PDW, MCHC, NLR, HGB, PLT, CRP, RBC and PLR values of HSP and HSPN patients are shown in Table 2.
 |
Table 2 Blood Routine Tests in HSP and HSPN Patients |
Serum Immunoglobulin, Complement Levels and Blood Coagulation Test results in HSP and HSPN Patients
In HSP patients, levels of serum IgG (10.76±2.651 vs 9.67±3.166) (P=0.003) were significantly higher than HSPN patients (Table 3).While there were no differences in IgA (2.083±0.882 vs 2.185±0.786), IgM (1.214±0.483 vs 1.311±0.690), IgE (124.0±230.8 vs 190.1±676.8), C3 (0.961±0.204 vs 0.947±0.220) and C4 (0.294±0.923 vs 0.186±0.054) (P>0.05). FIB levels (3.168±0.760 vs 3.560±0.828) were significantly lower in HSP patients than in HSPN patients (P=0.002). No obvious differences between the HSP patients and the HSPN patients in PT (11.00±0.867 vs 10.97±1.032), APTT (30.95±3.676 vs 32.19±4.804), TT (15.49±0.941 vs 15.46±0.917) and DD (0.541±1.418 vs 0.323±0.485) (P>0.05).
 |
Table 3 Serum Immunoglobulin, Complement Levels and Blood Coagulation Levels in HSP and HSPN Patients |
Liver/Kidney Function and Peripheral Blood T Lymphocyte Subsets Levels in HSP and HSPN Patients
Liver/kidney function test results and peripheral blood T lymphocyte subset levels in patients are shown in Table 4. The TP (67.76±5.694 vs 65.48±6.837), ALB (41.72±3.246 vs 40.48±4.215) levels were significantly lower (P = 0013, 0.029), and the Cr (40.40±34.30 vs 41.05±15.13), CD3+% (62.08±8.716 vs 67.15±6.991), CD4+% (30.58±6.981 vs 33.66±6.819) levels were found to be significantly higher in patients with renal injury than in patients without renal injury (P = 0.016, 0.002, and 0.02, respectively). ALT (18.62±14.26 vs 17.53±12.95), AST (23.73±7.746 vs 22.72±6.351), BUN (3.830±1.153 vs 3.899±1.255), UA (278.6±100.0 vs 284.3±87.93), CD8+% (27.05±5.835 vs 28.25±4.351) levels were not found to be correlated with renal involvement in HSP.
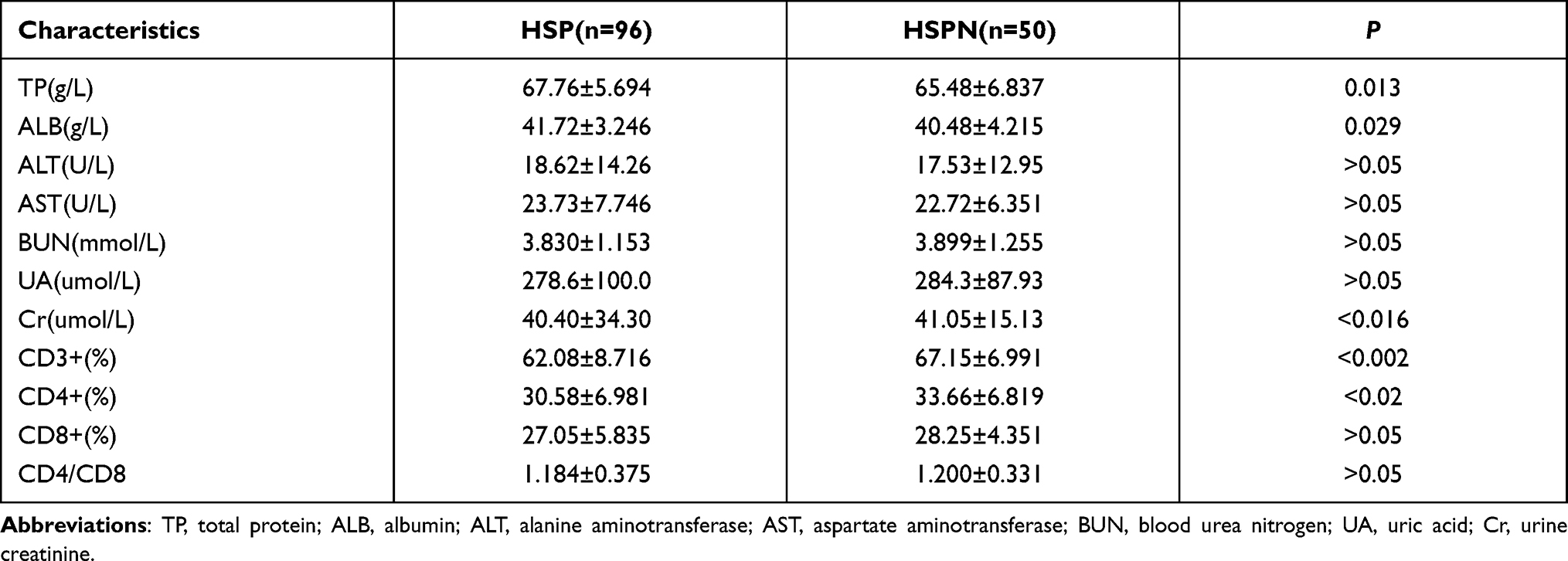 |
Table 4 Liver/Kidney Function Test Results in HSP and HSPN Patients |
Evaluation of Laboratory Indexes to Identifying HSP with Renal Involvement
The findings of univariate logistic regression analysis revealed that age (, P=0.0154), WBC (OR=0.8686, P=0.0191), PDW (OR=1.457, P=0.0021), MCHC (OR=0.9656, P=0.0496), CRP (OR=0.8351, P=0.044), NLR (OR=0.5841, P=0.0105), IgG (OR=0.8598, P=0.0381), CD3% (OR=1.087, P=0.003), CD4% (OR=1.068, P=0.0257), TP (OR=0.9394, P=0.0367),and FIB (OR=1.852, P=0.0067) were significant independent predictors for renal involvement in HSP patients (Table 5). The findings of multivariate logistic regression analysis identified age (OR=1.414, P=0.015), PDW (OR=1.498, P=0.0157), CRP (OR=0.748, P=0.0448), NLR (OR=0.537, P=0.006), IgG (OR=0.853, P=0.0445), CD3+% (OR=1.077, P=0.0197), and FIB (OR=1.945, P=0.0056) were significant factors.
 |
Table 5 Logistic Regression Analysis of Predictors for in HSP Patients with Renal Involvement |
ROC curve of these predictors was further performed, and the AUC ranged from 0.6284 to 0.7009 (Table 6). The combinatorial of these indexes were also investigated; the results found that the combined diagnosis can improve the diagnostic efficacy, with the AUC ranging from 0.7157 to 0.9774. Among all the combinations, a combination of NLR, CRP, PDW, IgG, FIB, CD3+ and age had the best AUC value (0.9774). The top sixteen diagnostic capacities of the different combinations are shown in Figure 1 (AUC>0.85). These results indicated that a combination of potential biomarkers could distinguish whether HSP children progress to renal injury.
 |
Table 6 ROC Curve Analysis of Prediction Indexes Involved in HSPN |
 |
Figure 1 ROC curve of the differential combination of laboratory indexes (The top sixteen AUC (>0.85) of the different combinations were shown). |
Discussion
Renal injury is the most serious and persistent complication of HSP and nowadays there is no way to predict which children may progress to renal impairment from the outset. Prediction markers can help diagnose early and guide therapy efficiently. So, we reviewed the medical records of HSP patients and explored the prediction indexes for renal injury in patients with HSP. The relationship between laboratory indexes and the occurrence of renal injury in HSP has been extensively studied. In the present study, we observed that age, PDW, NLR, CRP, IgG, CD3+% and FIB values are useful in predicting renal involvement. Some of our findings confirmed previous reports, while some results shed new insights into the predictors in HSP children with renal involvement.
HSP occurs worldwide and affects children in up to 90% of cases under the age of 10.8 Studies have also shown that there is a slight disease predominance in males, the ratio between males and females is about 1.2–1.8:1. Our results were similar to the previous studies, the mean age of the 146 patients was 10.04±3.254 years (range 3–18 years), the males-to-females ratio was 1.09. Some studies have reported that older age can predict renal injury in children HSP. Sano et al reported that age over 4 years was a significant independent risk indicator for renal injury in HSP.9 Demircioglu et al also reported that children higher than 10 years increased 1.4-fold risk in renal involvement.10 Our results showed that HSP patients with renal involvement were significantly older as well. Demircioglu et al also found females had a 2.7-fold risk for renal involvement in HSP compared to males.10 However, sex was not found to be an indicator associated with renal involvement in the present study.
In recent years, NLR has become a novel potential inflammatory biomarker and proved to be related to autoimmune diseases such as Psoriasis,11 primary Sjögren’s syndrome (pSS),12 dermatomyositis and polymyositis.13 Gayret et al reported that NLR and PLR were significantly increased in HSP patients than in healthy children, and high PLR was a significant predictive indicator for gastrointestinal bleeding in HSP.14 Kim et al reported that NLR was an indicator of renal injury in HSP.15 Other studies also reported that NLR was increased in HSP patients with organ involvement compared to patients without organ involvement.16,17 In the present study, NLR was found to be a predictive index for renal involvement in HSP, while PLR was not found to be statistically different between HSP and HSPN.
CRP is an acute-phase protein that significantly increases during acute infections and stress. Elmas et al reported that CRP values were positively correlated with renal injury in HSP patients.18 Another study also found that patients with higher CRP levels had a 6.57-fold increased risk of kidney involvement.10 While in our study, patients without renal injury had higher CRP levels than those with renal injury. The reason for the difference in CRP levels might be: 1) The small number of HSP and HSPN patients included in the previous studies; 2) Majority of hospitalized HSP patients without renal involvement were in acute inflammation period, while most inpatients with renal involvement were in the late stage of disease, not in acute inflammation period.
IgG, CD3, FIB and PDW were less frequently reported, but they may have potential utility in predicting the occurrence of HSPN and provide significant insights into the underlying pathophysiology of HSPN. Serum IgG levels in HSP patients are not entirely consistent with previous data. Studies have shown that IgG levels may increase, decrease, or remain unchanged.18–20 In our study, compared to the HSP patients without renal injury, IgG levels were significantly increased, while CD3 levels were decreased in those patients with renal involvement. The results reflected that both cellular and humoral immunity disorder participated in the pathogenesis of HSP and HSPN. Although IgA circulating immune complexes deposition plays a key role in HSP, and previous studies suggested HSP is linked with increased serum IgA levels,21,22 in our patients, IgA levels showed no relationship with renal involvement. Recent studies have shown that abnormal coagulation and fibrinolysis participate in the occurrence and development of HSP and HSPN. Yilmaz et al found that D-D levels in children with acute stage HSP were higher than in children with convalescent stage HSP and healthy controls.23 Tian et al reported that D-D and FIB levels were significantly decreased in severe HSPN patients after being treated with low-molecular-weight heparin calcium.24 PDW is a measure of PLT size heterogeneity and represents the activation degree of PLT. FIB can reflect the state of the coagulation function. However, PDW has not yet been investigated as a predictive biomarker for HSP patients with renal injury. In our study, HSP patients with renal injury had higher PDW and FIB levels than patients with no renal injury. There is no obvious difference in PT, APTT and D-D.
In this paper, the AUC of independent PDW, NLR, CRP, IgG, CD3, age and FIB ranged from 0.6284 to 0.7009. In addition, we found that the combination of these biomarkers showed great diagnostic capacity and the AUC of several combination indexes had already exceeded 0.9, which was rarely seen in previous studies.25–27 Among these combinations, the AUC of four combinations could also be higher than 0.85, and most of these indicators came from routine blood tests. These combinations all possess a better diagnostic efficacy, some are easily accessible and inexpensive, and hospitals may select some of them to predict renal involvement in children with HSP.
The major limitations of the current study were its single-center and retrospective design. The ethnic differences of these blood biomarkers are currently unknown. Multicenter and prospective studies with a large number of HSP patients and laboratory values are required to confirm and expand the present study. However, abundant laboratory indexes were the strengths of our study.
In conclusion, our study demonstrated that age, PDW, CD3, FIB, CRP, NLR and IgG were prediction indexes for renal injury in patients with HSP. Age, the levels of PDW, CD3 and FIB were positively correlated with renal involvement, while the levels of CRP, NLR and IgG were negatively correlated with renal involvement. These parameters can be combined appropriately to improve the diagnosis efficacy, and a close follow-up visit is needed in HSP patients with these factors. These data may offer support for diagnosis and prognosis and also provide valuable insight into the pathogenesis of HSP and HSPN.
Data Sharing Statement
The raw data cannot currently be shared as the data are also part of an ongoing study.
Ethics Approval and Consent to Participate
The human study was conducted under protocols approved by the Ethics Committee of the First Affiliated Hospital of Henan University of Chinese Medicine. Written consent was obtained from all participants and their parents/guardians.
Acknowledgments
We thank all the participants in this study.
Author Contributions
All listed authors participated in the study design, or analysis and interpretation of the data, all drafted or revised the article, have agreed on the journal currently submitted and given approval for the version to be published.
Funding
This work was supported by the Chinese Medicine Prominent Talent Development Project of Henan Province (Yu CM Science and Education [2018] No.5).
Disclosure
The authors declare no competing interests.
References
1. Piram M, Mahr A. Epidemiology of immunoglobulin A vasculitis (Henoch-Schonlein): current state of knowledge. Curr Opin Rheumatol. 2013;25(2):171–178. doi:10.1097/BOR.0b013e32835d8e2a
2. Jennette JC, Falk RJ, Bacon PA, et al. 2012 revised international chapel hill consensus conference nomenclature of vasculitides. Arthritis Rheum. 2013;65(1):1–11. doi:10.1002/art.37715
3. Roberts PF, Waller TA, Brinker TM, et al. Henoch-Schönlein purpura: a review article. South Med J. 2007;100:821–824. doi:10.1097/SMJ.0b013e3180f62d0f
4. Karadağ ŞG, Tanatar A, Sönmez HE, et al. The clinical spectrum of Henoch-Schönlein purpura in children: a single-center study. Clin Rheumatol. 2019;38(6):1707–1714. doi:10.1007/s10067-019-04460-1
5. Wang K, Sun X, Cao Y, et al. Risk factors for renal involvement and severe kidney disease in 2731 Chinese children with Henoch- Schönlein purpura: a retrospective study. Medicine. 2018;97(38):e12520. doi:10.1097/MD.0000000000012520
6. Davin JC, Coppo R. Henoch-Schonlein purpura nephritis in children. Nat Rev Nephrol. 2014;10(10):563–573. doi:10.1038/nrneph.2014.126
7. Ozen S, Pistorio A, Iusan SM, et al. EULAR/PRINTO/PRES criteria for Henoch–Schönlein purpura, childhood polyarteritis nodosa, childhood Wegener granulomatosis and childhood Takayasu arteritis: ankara 2008. Part II: final classification criteria. Ann Rheum Dis. 2010;69:798–806. doi:10.1136/ard.2009.116657
8. Oni L, Sampath S. Childhood IgA vasculitis (Henoch Schonlein Purpura)-advances and knowledge gaps. Front Pediatr. 2019;7:257. doi:10.3389/fped.2019.00257
9. Sano H, Izumida M, Shimizu H, et al. Risk factors of renal involvement and significant proteinuria in Henoch-Schonlein purpura. Eur J Pediatr. 2002;161(4):196–201. doi:10.1007/s00431-002-0922-z
10. Kilic BD, Demir Bk. Determination of risk factors in children diagnosed with Henoch-Schonlein purpura. Arch Rheumatol. 2018;33(4):395–401. doi:10.5606/ArchRheumatol.2018.6562
11. Paliogiannis P, Satta R, Deligia G, et al. Associations between the neutrophil-to-lymphocyte and the platelet-to-lymphocyte ratios and the presence and severity of psoriasis: a systematic review and meta-analysis. Clin Exp Med. 2019;19(1):37–45. doi:10.1007/s10238-018-0538-x
12. Hu ZD, Sun Y, Guo J, et al. Red blood cell distribution width and neutrophil/lymphocyte ratio are positively correlated with disease activity in primary Sjögren’s syndrome. Clin Biochem. 2014;47(18):287–290. doi:10.1016/j.clinbiochem.2014.08.022
13. Gao MZ, Huang YL, Wu XD, et al. Red blood cell distribution width and neutrophil to lymphocyte ratio are correlated with disease activity of dermatomyositis and polymyositis. J Clin Lab Anal. 2018;32(1):e22209. doi:10.1002/jcla.22209
14. Gayret OB, Erol M, Tekin Nacaroglu H. The relationship of neutrophil-lymphocyte ratio and platelet-lymphocyte ratio with gastrointestinal bleeding in Henoch-Schonlein purpura. Iran J Pediatr. 2016;26(5):e8191.
15. Kim WK, Kim CJ, Yang EM. Risk factors for renal involvement in Henoch-Schonlein purpura. J Pediatr. 2021. doi:10.1016/j.jped.2021.01.008
16. Yakut HI, Kurt T, Uncu N, et al. Predictive role of neutrophil to lymphocyte ratio and mean platelet volume in Henoch-Schonlein purpura related gastrointestinal and renal involvement. Arch Argent Pediatr. 2020;118(2):139–142.
17. Ozdemir ZC, Cetin N, Kar YD, et al. Hemotologic indices for predicting internal organ involvement in Henoch-Schonlein purpura (IgA vasculitis). J Pediat Hematol Onc. 2020;42(1):E46–E49. doi:10.1097/MPH.0000000000001571
18. Elmas AT, Tabel Y. Platelet counts in children with Henoch-Schonlein purpura–relationship to renal involvement. J Clin Lab Anal. 2016;30(1):71–74. doi:10.1002/jcla.21817
19. Ding Y, Zhou Y, Li HR, et al. Characteristics of immune function in the acute phase of Henoch-Schonlein purpura. Clin Rheumatol. 2021;40(9):3711–3716. doi:10.1007/s10067-021-05707-6
20. Zhu X, Zhang M, Lan F, et al. The relationship between red cell distribution width and the risk of Henoch-Schonlein purpura nephritis. Br J Biomed Sci. 2018;75(1):30–35. doi:10.1080/09674845.2017.1368184
21. Hastings MC, Rizk DV, Kiryluk K, et al. IgA vasculitis with nephritis: update of pathogenesis with clinical implications. Pediatr Nephrol. 2021. doi:10.1007/s00467-021-04950-y
22. Wada Y, Matsumoto K, Suzuki T, et al. Clinical significance of serum and mesangial galactose-deficient IgA1 in patients with IgA nephropathy. PLoS One. 2018;13(11):e0206865. doi:10.1371/journal.pone.0206865
23. Yilmaz D, Kavakli K, Ozkayin N. The elevated markers of hypercoagulability in children with Henoch-Schonlein purpura. Pediatr Hematol Oncol. 2005;22(1):41–48. doi:10.1080/08880010590896251
24. Tian M, Liu C. Heparin calcium treated Henoch-Schonlein purpura nephritis in children through inhibiting hyperfibrinolysis. Ren Fail. 2015;37(7):1100–1104. doi:10.3109/0886022X.2015.1061668
25. Liu H, Cui W, Liu H, et al. Predicative value of urinary protein biomarkers on delayed renal involvement in children with Henoch-Schonlein purpura. Sci China Life Sci. 2019;62(12):1594–1596. doi:10.1007/s11427-018-9544-0
26. Kim J, Choi SE, Lee KH, et al. Tubulointerstitial infiltration of M2 macrophages in Henoch-Schonlein purpura nephritis indicates the presence of glomerular crescents and bad clinical parameters. Biomed Res Int. 2019;2019:8579619. doi:10.1155/2019/8579619
27. Pillebout E, Jamin A, Ayari H, et al. Biomarkers of IgA vasculitis nephritis in children. PLoS One. 2017;12(11):e0188718. doi:10.1371/journal.pone.0188718
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.