Back to Journals » International Journal of Women's Health » Volume 18
Predictive Value of Inflammatory Indices for Preeclampsia and Adverse Perinatal Outcomes: A Retrospective Case-Control Study
Received 16 February 2026
Accepted for publication 1 May 2026
Published 13 May 2026 Volume 2026:18 603944
DOI https://doi.org/10.2147/IJWH.S603944
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Hüseyin Kayaalp,1,* Sertaç Ayçiçek2,*
1Department of Obstetrics and Gynecology, Perinatology Unit, Ankara Bilkent City Hospital, University of Health Sciences, Ankara, Turkey; 2Department of Obstetrics and Gynecology, Gazi Yaşargil Training and Research Hospital, University of Health Sciences, Diyarbakır, Turkey
*These authors contributed equally to this work
Correspondence: Hüseyin Kayaalp, Department of Obstetrics and Gynecology, Perinatology Unit, Ankara Bilkent City Hospital, University of Health Sciences, Ankara, Turkey, Tel +90 507 611 00 66, Email [email protected]
Purpose: The aim of this study was to evaluate the predictive value of the systemic inflammatory index (SII), the systemic inflammatory response index (SIRI), and the aggregate systemic inflammatory index (AISI) in patients diagnosed with preeclampsia (PE) for PE and composite adverse perinatal outcomes (CAPO) in patients with PE.
Patients and Methods: This single-center, retrospective case-control study included pregnant women aged 18– 45 years with PE and healthy controls. First- and third-trimester hematological parameters were recorded, and inflammatory indices were calculated. Neonatal intensive care unit (NICU) admission and CAPO were evaluated as clinical outcomes. Receiver operating characteristic (ROC) analysis assessed predictive performance, and multivariable logistic regression was used to adjust for confounding factors.
Results: A total of 300 patients (150 with PE and 150 controls) were included. The PE group had significantly higher rates of NICU admission and CAPO (p < 0.05). Several first- and third-trimester inflammatory indices, including NLR, PNR, SII, SIRI, and AISI, were significantly higher in the PE group. ROC analysis demonstrated that multiple indices were associated with the prediction of PE, NICU admission, and CAPO. In multivariable analysis, third-trimester PLR remained an independent predictor of NICU admission, while third-trimester PLR and PMR were identified as independent predictors of CAPO (p < 0.05). For the prediction of PE, only first-trimester NLR and PNR remained independent predictors (p < 0.05).
Conclusion: Inflammation-based indices derived from routine blood tests were associated with PE and adverse perinatal outcomes. Inflammation-based indices derived from routine blood tests were associated with PE and adverse perinatal outcomes. Certain indices demonstrated independent predictive value, particularly third-trimester PLR for NICU admission, third-trimester PLR and PMR for CAPO, and first-trimester NLR and PNR for PE. However, these indices should be interpreted in conjunction with clinical variables and considered as supportive markers rather than stand-alone predictors in clinical practice.
Keywords: preeclampsia, neutrophil, lymphocyte, platelet, neonatal intensive care unit, composite adverse perinatal outcomes
Introduction
Preeclampsia (PE) is a common pregnancy complication characterized by hypertension and proteinuria that develops after the 20th week of gestation.1 It affects approximately 2–8% of pregnancies worldwide and poses significant risks for both maternal and fetal health.2 The pathogenesis of PE is believed to involve placental ischemia and a subsequent systemic inflammatory response index (SIRI), which triggers endothelial dysfunction and leads to the clinical manifestations of the disease.3 Insufficient remodeling of the spiral arteries results in hypoxia, oxidative stress, and increased levels of inflammatory mediators, forming the core mechanisms of the disease.4 Recent studies have emphasized the central role of immune-inflammatory markers in predicting PE. In particular, the neutrophil-to-lymphocyte ratio (NLR), platelet (PLT)-to-lymphocyte ratio (PLR), and lymphocyte-to-monocyte ratio (LMR) have been proposed as potential indicators of inflammation.5,6 Additionally, hematological inflammation indices such as the Systemic Immune-Inflammation Index (SII), SIRI and Aggregate Index of Systemic Inflammation (AISI) have drawn attention as accessible and cost-effective biomarkers for predicting preeclampsia.7,8 Since the pathophysiological processes of PE begin in the early stages of pregnancy and become more evident in the later stages, laboratory parameters obtained from both the first and third trimesters may provide valuable insights for identifying preeclamptic pregnancies and predicting adverse outcomes. Recent evidence suggests that systemic inflammatory markers may also be associated with adverse perinatal outcomes, including neonatal intensive care unit (NICU) admission and composite adverse perinatal outcomes (CAPO). However, the predictive value of these indices for adverse perinatal outcomes in patients with PE has not been sufficiently established. While several studies have investigated the prediction of PE, research focusing on the prediction of adverse pregnancy outcomes remains limited.9,10 The aim of this study is to evaluate whether hematological inflammatory markers measured in the first and third trimesters of pregnancy can predict the development of PE and adverse outcomes such as NICU admission and CAPO.
Materials and Methods
Study Population
This study was designed as a single-center, retrospective case-control study. Pregnant women aged 18–45 years who were diagnosed with preeclampsia and followed up or treated at the Department of Obstetrics and Gynecology, Gazi Yaşargil Training and Research Hospital, Diyarbakır, Turkey, between January 2023 and January 2025 were included in the study. All procedures were conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval for this study was obtained from the Gazi Yaşargil Training and Research Hospital Ethics Committee on July 25, 2025 (Decision No: 576). Due to the retrospective design of the study, patient consent for review of medical records was not required by the ethics committee. All patient data were anonymized and handled confidentially in accordance with institutional and ethical standards. Patients were categorized into two groups: the PE group (Group 1) and the control group (Group 2). The preeclampsia group was further subdivided into PE without severe features (PE-WSF) and PE with severe features (PE-SF), as well as early-onset and late-onset preeclampsia. In this study, the diagnosis of PE was made according to the criteria of the American College of Obstetricians and Gynecologists (ACOG), based on new-onset hypertension of ≥140/90 mmHg after 20 weeks of gestation accompanied by evidence of proteinuria.2
PE with severe features was defined as the presence of a systolic blood pressure ≥160 mmHg or a diastolic blood pressure ≥110 mmHg, or—regardless of blood pressure levels—the occurrence of at least one of the following: platelet count <100,000/mm3; elevated liver transaminases (more than twice the normal values) or persistent right upper quadrant or epigastric pain; serum creatinine >1.1 mg/dL or doubling of the baseline value; pulmonary edema; new-onset and treatment-resistant headache; or visual disturbances. Preeclamptic patients were further categorized as early-onset (<34 weeks of gestation) or late-onset (≥34 weeks of gestation) according to ACOG guidelines.2 The exclusion criteria were the presence of major fetal anomalies, known chromosomal or genetic abnormalities, multiple pregnancies, pregnancies complicated by additional chronic diseases, premature rupture of membranes (PPROM), and a history of smoking or alcohol use. Homogeneity was ensured between the study and control groups with respect to blood parameters obtained during the first trimester, defined as 10 to 14 weeks of gestation, and the third trimester, defined as 28 to 38 weeks of gestation. The control group consisted of low-risk pregnant women with no medical or obstetric complications. In the study group, patients diagnosed with PE were included, whereas the control group consisted of low-risk pregnant women without any systemic diseases (such as neurological, cardiac, thoracic, gastrointestinal, genitourinary, endocrine, etc.) or obstetric complications (such as PE, gestational diabetes mellitus (GDM), or PPROM).
Data Collection
Clinical and demographic data of the participants were recorded, including maternal age, gravidity, parity, body mass index (BMI), Systolic and Diastolic blood pressure, spot urine protein 24-hour urinary protein, gestational age at delivery, birth weight, mode of delivery, cord pH and base excess (BE), 1-minute and 5-minute APGAR scores, Preterm delivery (PTD), NICU admission, and CAPO; defined as pH <7.1, 5-minute APGAR <7, NICU admission). The indications for NICU admission were defined as respiratory distress, hypoglycemia, hyperbilirubinemia, and prematurity. Blood pressure measurements were taken after at least 5 minutes of rest, with the patient in a seated position, using an appropriately sized cuff placed on the bare upper arm, with the arm supported at heart level. To confirm the diagnosis, two separate readings were required at least four hours apart. Proteinuria was defined as ≥1+ on a dipstick test, ≥300 mg of protein in a 24-hour urine collection, or a protein-to-creatinine ratio ≥0.3 in a spot urine sample. For 24-hour collection, patients discarded the first morning urine and collected all urine over the next 24 hours. Spot urine samples were obtained using the clean midstream technique. Hemoglobin (Hgb), white blood cell count (WBC), neutrophil, lymphocyte, monocyte, platelet (PLT) levels were measured using the Mindray BC-6000 device (China); All tests were performed in our clinical laboratory in accordance with ISO 15189 standards. NLR was defined as the neutrophil-to-lymphocyte ratio, PLR as the platelet-to-lymphocyte ratio, PNR as the PLT-to neutrophil ratio, PMR as the PLT-to- monocyte ratio, MLR as the monocyte-to-lymphocyte Sİİ as the NLR x platelet, SIRI as the NLR x monosit, AISI as the NLR x PLT x monosit, as previously described in the literature.7 These calculations were performed using the SPSS 25.0 statistical software program (SPSS Inc., Chicago, IL, USA).
Statistical Analysis
Statistical analyses were performed using SPSS version 25.0 software (SPSS Inc., Chicago, IL, USA). The Kolmogorov–Smirnov and Shapiro–Wilk tests were used to assess the normality of data distribution. The Mann–Whitney U-test was used for non-normally distributed variables. Descriptive data for non-normally distributed variables were expressed as medians and interquartile ranges (IQR). The chi-square test was used to compare categorical variables. Receiver operating characteristic (ROC) curve analysis was performed to evaluate the predictive value of hematological indices for PE, NICU and CAPO. A p < 0.05 was considered statistically significant. Multiple logistic regression analysis was performed to evaluate the effect of confounding factors. Variables included in the multivariable models were selected based on clinical relevance and prior literature. To avoid multicollinearity, each inflammatory index was entered into separate models adjusted for maternal age, gravidity, and BMI.
Results
A total of 300 patients were included in this study, divided into two groups: 150 patients in the PE group and 150 patients in the control group.
There were significant differences between the study and control groups in terms of maternal age, BMI, fetal weight, gestational week at delivery, 1-minute APGAR, 5-minute APGAR, cord pH (p < 0.001), and base excess (BE) (p = 0.013). However, no statistically significant differences were found regarding gravidity, parity, or mode of delivery (p > 0.05) (Table 1). Significant differences were also observed between the groups with respect to CAPO, NICU admission, and PTD (p < 0.05) (Table 1). The gestational week at diagnosis, the number of patients using antihypertensive medications, the systolic and diastolic blood pressure values, 24 hour urine test results, and spot urine protein analysis results in the study group are presented in Table 1.
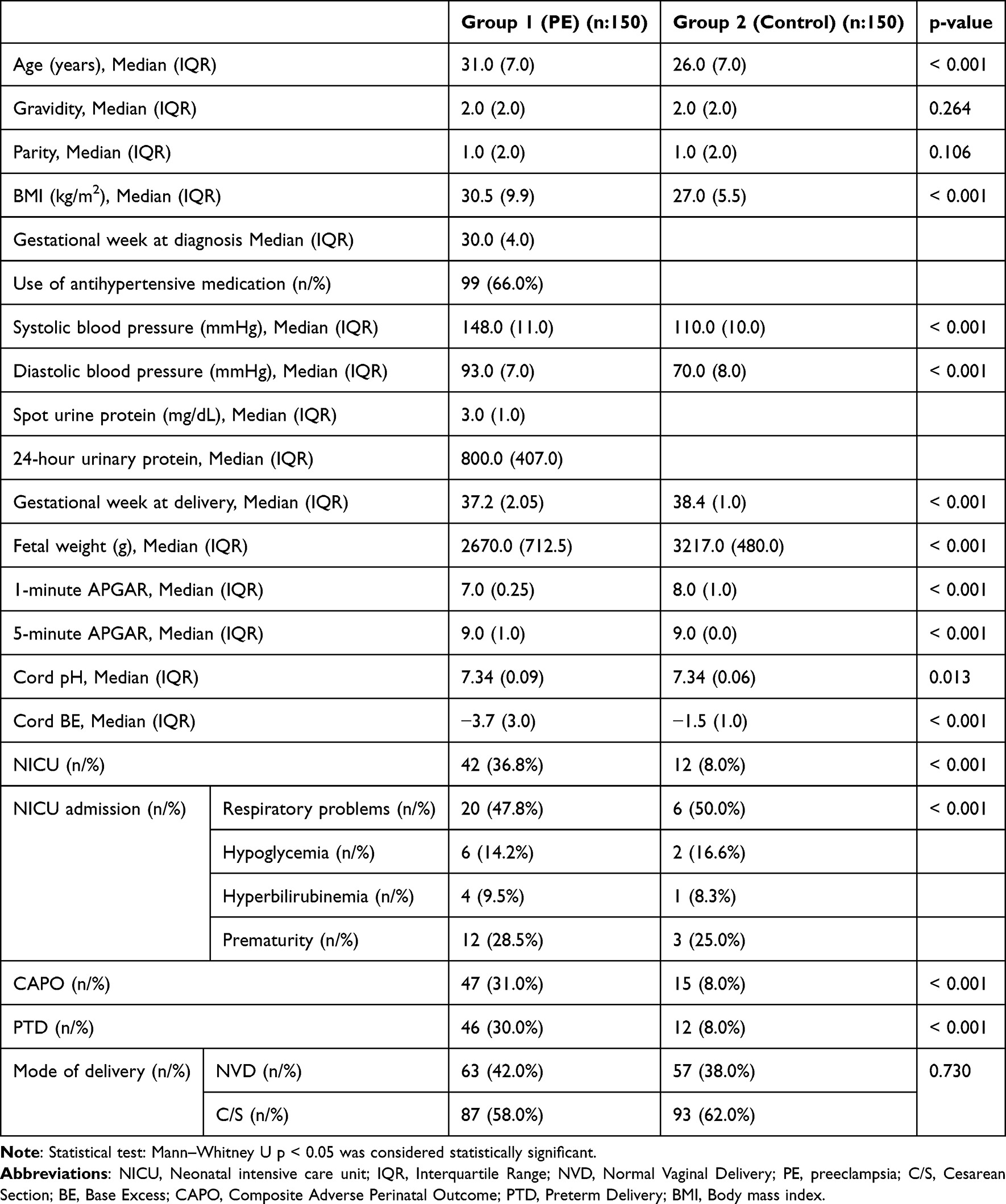 |
Table 1 Evaluation of the Clinical and Demographic Characteristics of the Preeclampsia and Control Groups |
In the first trimester, there were no significant differences between the groups in monocyte, PLT, or lymphocyte (p > 0.05), whereas Hgb (p = 0.002) and neutrophil (p < 0.001) differed significantly (Table 2). In the third trimester, there were no significant differences in platelet or lymphocyte (p > 0.05), while significant differences were observed in hgb (p = 0.002), neutrophil (p < 0.001), and monocyte (p = 0.029) levels (Table 2).
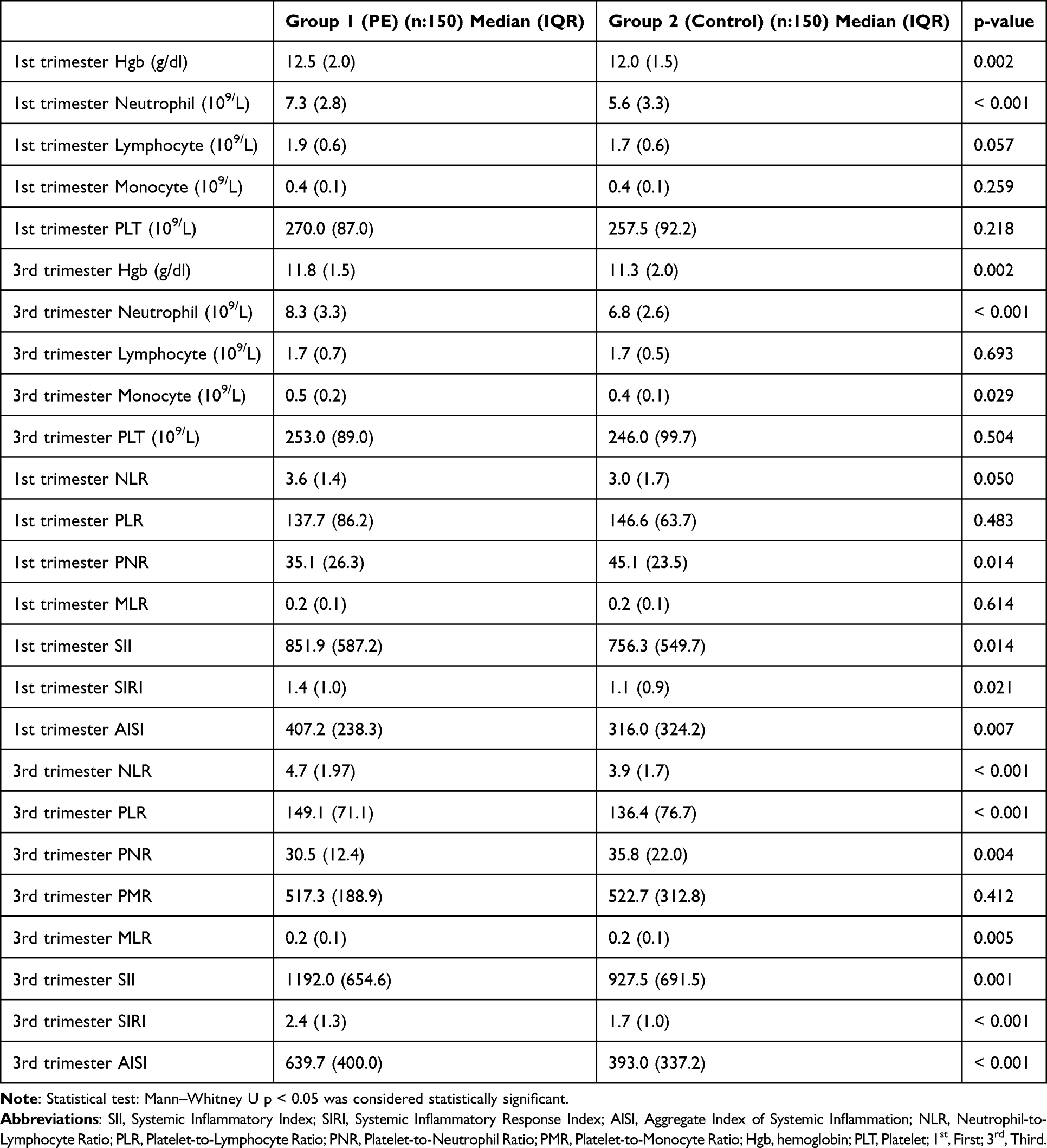 |
Table 2 Evaluation of Maternal Laboratory Findings, SII, SIRI and AISI Results in the Preeclampsia and Control Groups |
Regarding inflammatory indices, there were no significant differences in first-trimester PLR (p = 0.483) or MLR (p = 0.614) between the groups. However, significant differences were found in first-trimester NLR (p = 0.050), PNR (p = 0.014), SII (p = 0.031), SIRI (p = 0.021), and AISI (p = 0.007) (Table 1). In the third trimester, PMR (p > 0.05) showed no significant difference between groups, while significant differences were detected for NLR (p < 0.001), PLR (p = 0.046), PNR (p = 0.004), MLR (p = 0.005), SII (p = 0.005), SIRI (p < 0.001), and AISI (p < 0.001) (Table 2).
In the comparison of patients with PE with severe features and those without severe features, clinicodemographic characteristics, maternal laboratory parameters, and inflammatory indices were found to be similar (Table 3 and Table 4).
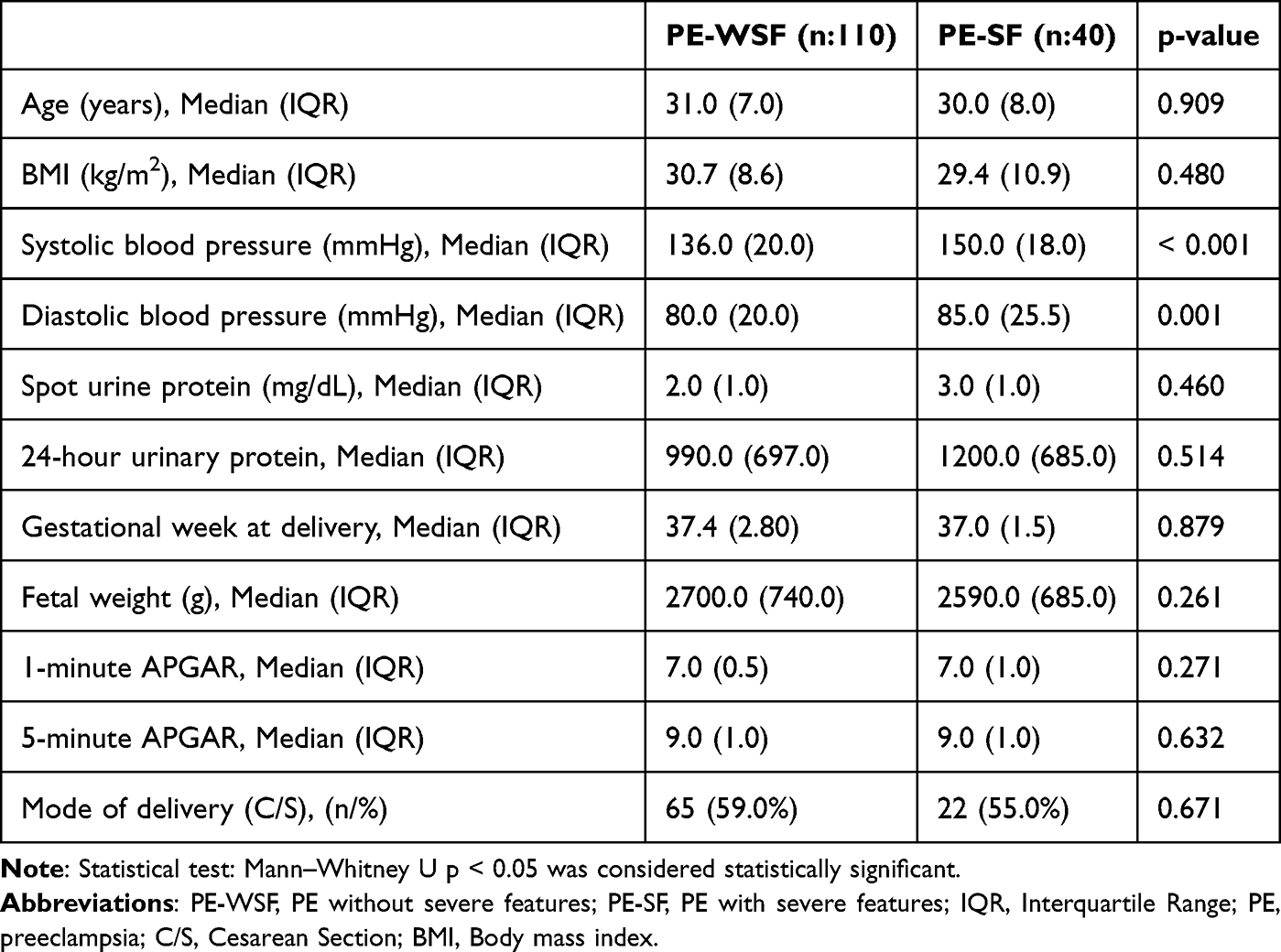 |
Table 3 Evaluation of the Clinical and Demographic Characteristics of the PE-WSF and PE-SF Groups |
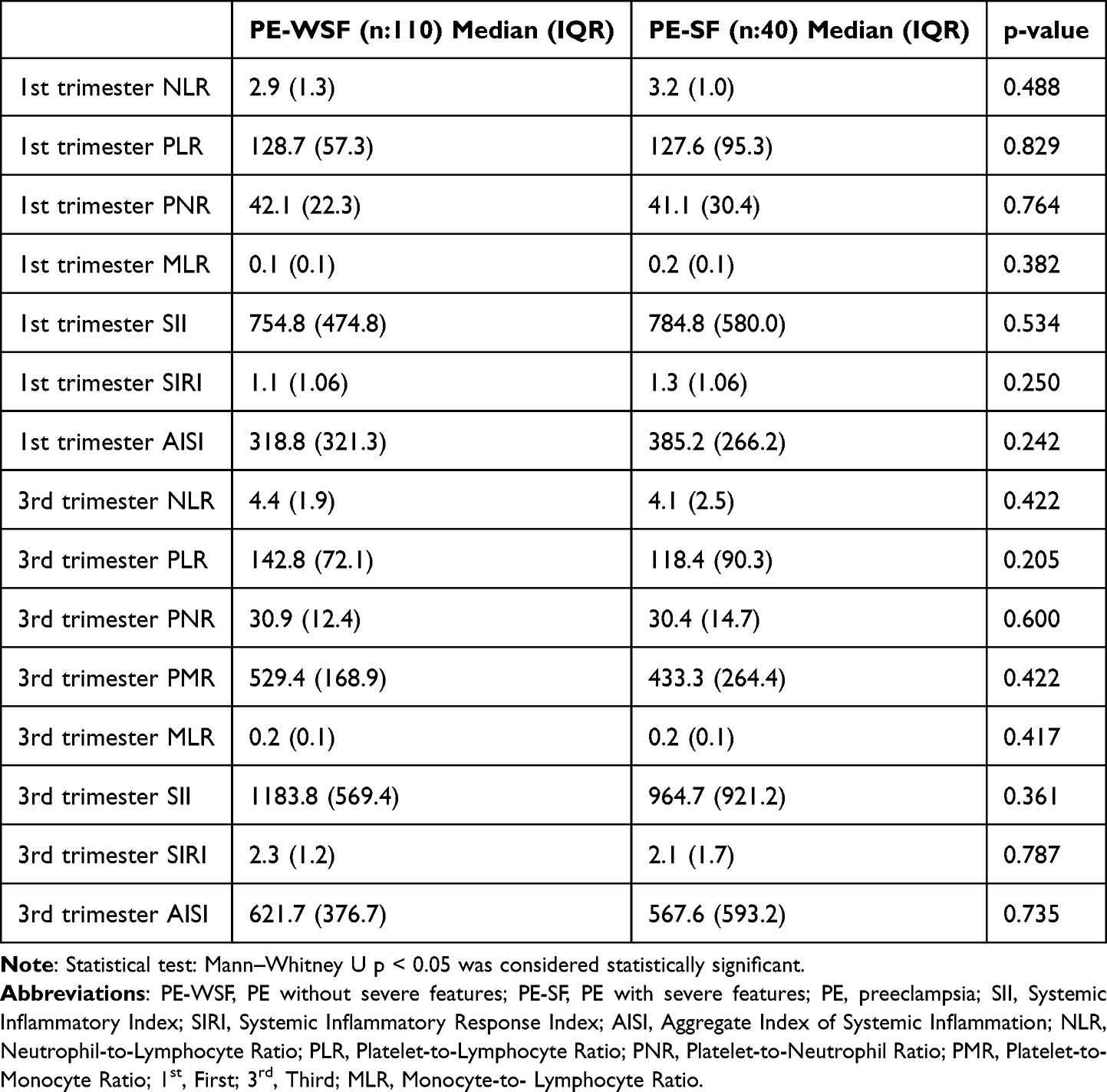 |
Table 4 Evaluation of Maternal Laboratory Findings, SII, SIRI and AISI Results in the PE-WSF and PE-SF Groups |
Similarly, in the comparison between early-onset and late-onset preeclampsia groups, clinicodemographic characteristics, maternal laboratory parameters, and inflammatory indices were comparable (Table 5 and Table 6).
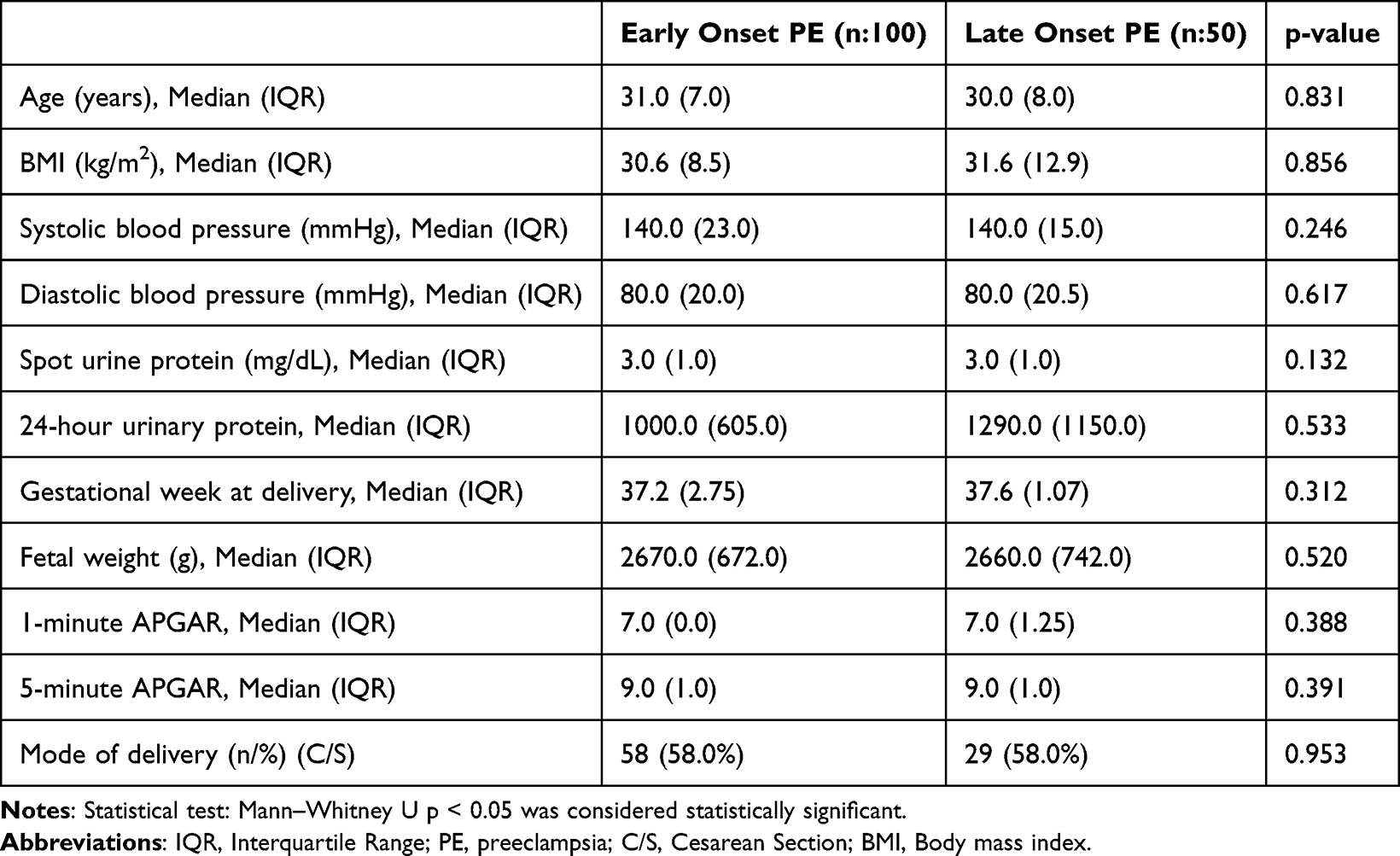 |
Table 5 Evaluation of the Clinical and Demographic Characteristics of the Early Onset and Late Onset Preeclampsia Groups |
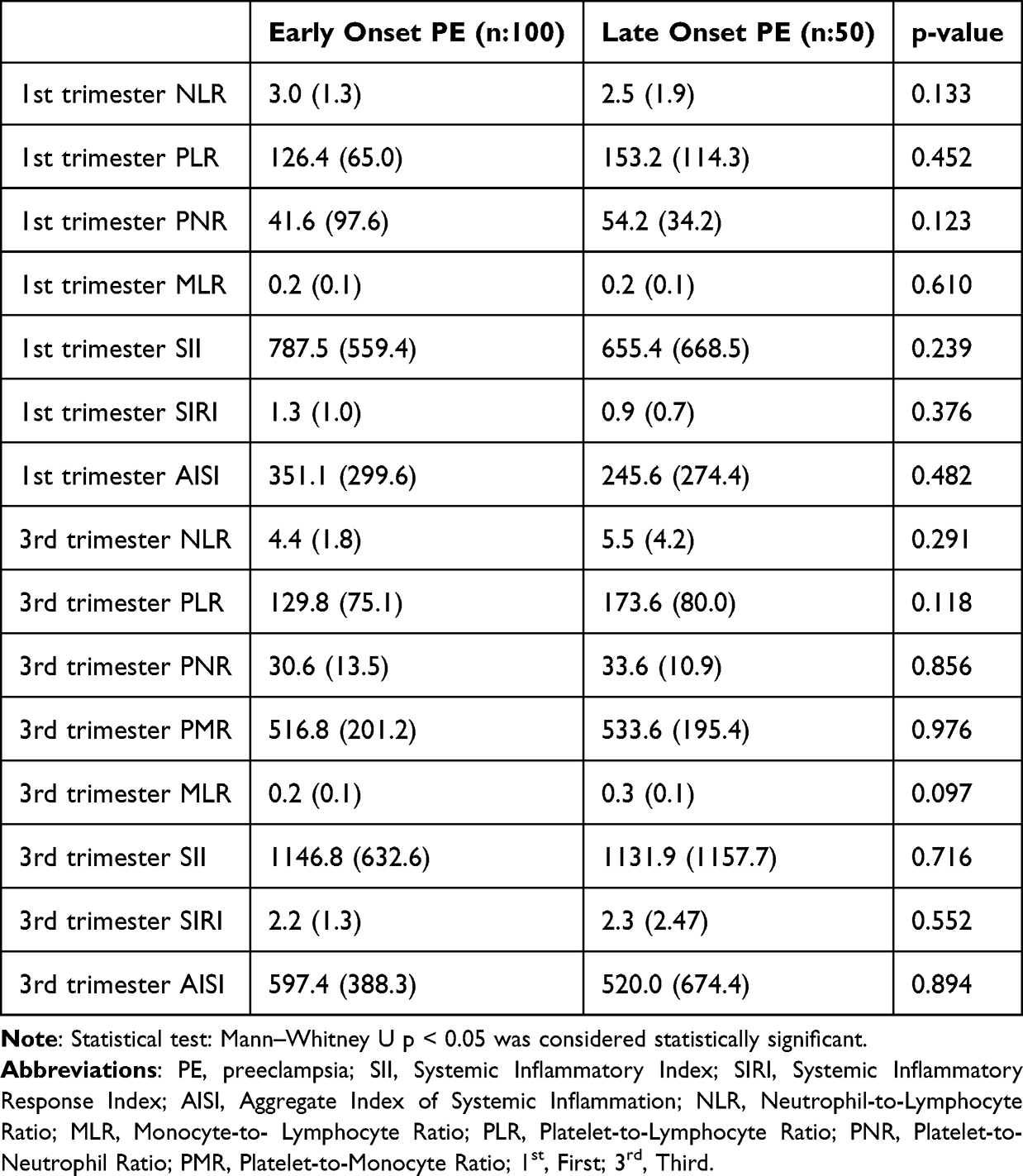 |
Table 6 Evaluation of Maternal Laboratory Findings, SII, SIRI and AISI Results in the Early Onset and Late Onset Preeclampsia Groups |
ROC analysis In the PE group, the ROC analysis for predicting NICU admission demonstrated the following results: third-trimester NLR (AUC: 0.689, p = 0.029, cutoff: 4.89, sensitivity: 75.0%, specificity: 69.2%), PLR (AUC: 0.750, p = 0.004, cutoff: 162.1, sensitivity: 62.5%, specificity: 61.5%), PMR (AUC: 0.679, p = 0.038, cutoff: 527.5, sensitivity: 62.5%, specificity: 61.5%), SII (AUC: 0.756, p = 0.003, cutoff: 1329.0, sensitivity: 68.8%, specificity: 66.7%), AISI (AUC: 0.678, p = 0.040, cutoff: 695.0, sensitivity: 62.5%, specificity: 60.8%) (Table 7).
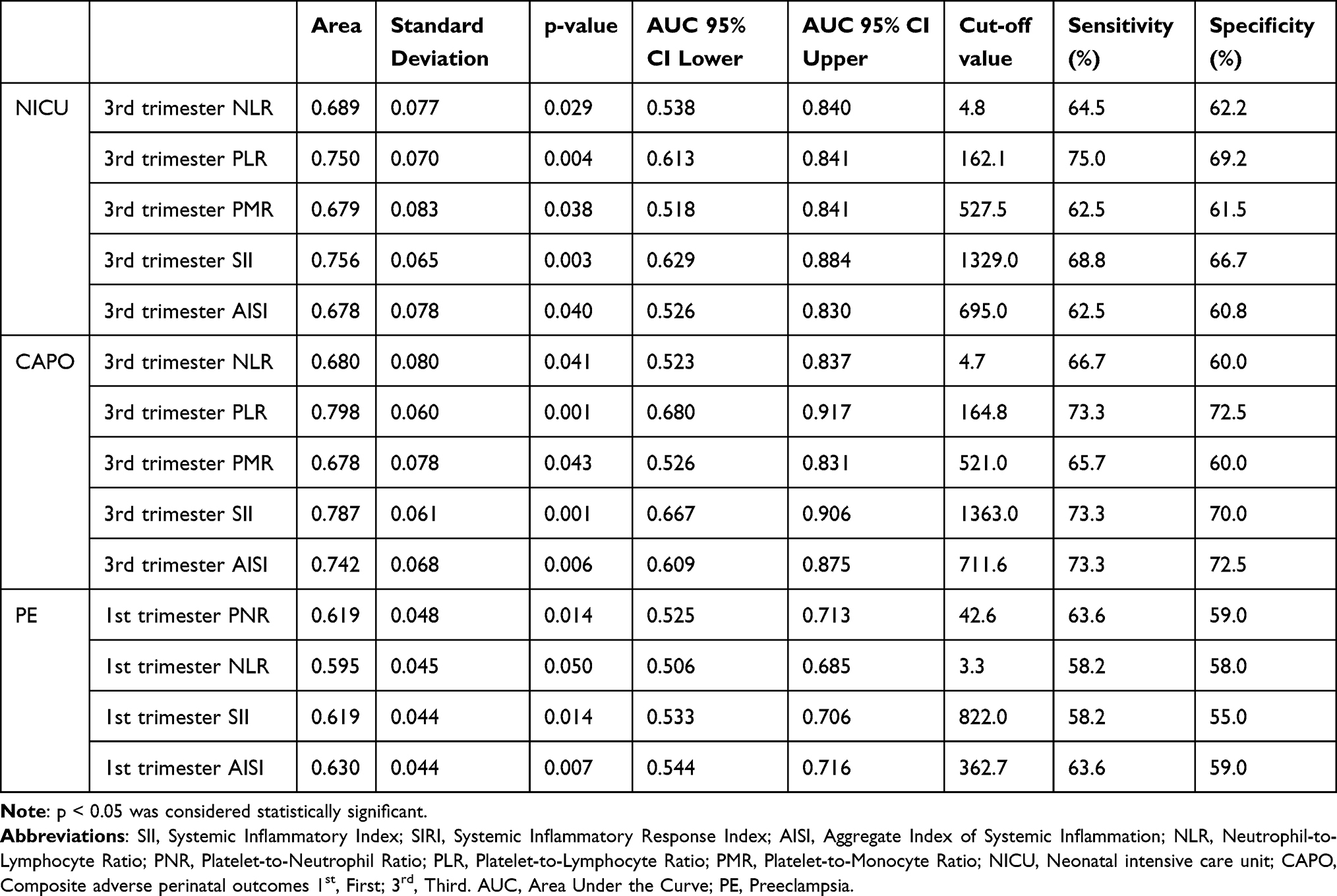 |
Table 7 ROC Curve Analysis Results of Laboratory Parameters and Inflammatory Indices for Predicting Preeclampsia, CAPO, and NICU Admission |
For CAPO prediction, ROC analysis revealed: Third-trimester NLR (AUC: 0.680, p = 0.041, cutoff: 4.7, sensitivity: 66.7%, specificity: 60.0%), PLR (AUC: 0.798, p = 0.001, cutoff: 164.8, sensitivity: 73.3%, specificity: 72.5%), PMR (AUC: 0.678, p = 0.043, cutoff: 521.0, sensitivity: 65.7%, specificity: 60.0%), SII (AUC: 0.787, p = 0.001, cutoff: 1363.0, sensitivity: 73.3%, specificity: 70.0%), AISI (AUC: 0.742, p = 0.006, cutoff: 711.6, sensitivity: 73.3%, specificity: 72.5%) (Table 7).
For PE prediction, the ROC analysis yielded: First-trimester PNR (AUC: 0.619, p = 0.014, cutoff: 42.6, sensitivity: 63.6%, specificity: 59.0%), NLR (AUC: 0.595, p = 0.050, cutoff: 3.36, sensitivity: 58.2%, specificity: 58.0%), SII (AUC: 0.619, p = 0.014, cutoff: 822.0, sensitivity: 58.2%, specificity: 55.0%), AISI (AUC: 0.630, p = 0.007, cutoff: 362.7, sensitivity: 63.6%, specificity: 59.0%) (Table 7).
All ROC curve plots corresponding to these findings are presented in Figures 1–4.
 |
Figure 1 ROC curve analysis of third-trimester NLR, PLR, PMR, SII, and AISI for predicting NICU admission in the preeclampsia group. |
 |
Figure 2 ROC curve analysis of third-trimester NLR, PLR, PMR, SII, and AISI for predicting CAPO in the preeclampsia group. |
 |
Figure 3 ROC curve of first-trimester PNR for predicting preeclampsia. |
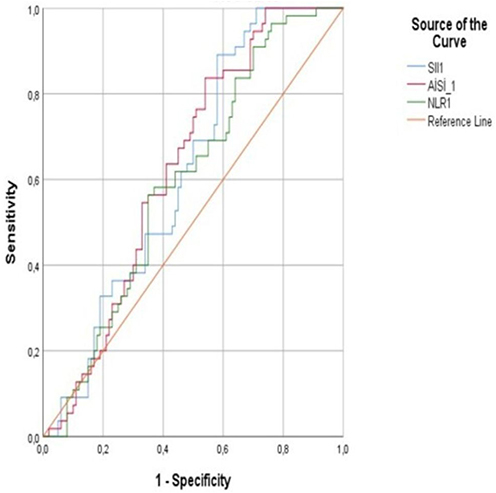 |
Figure 4 ROC curve analysis of first-trimester NLR, SII, and AISI for predicting preeclampsia. |
Multivariable logistic regression analysis was performed for the biochemical indices that were found to be significant in ROC analysis for the prediction of preeclampsia, NICU admission, and CAPO. As a result of the analysis, third-trimester PLR was identified as an independent predictor of NICU admission, while third-trimester PLR and PMR were identified as independent predictors of CAPO (p < 0.05) (Tables 8 and 9).
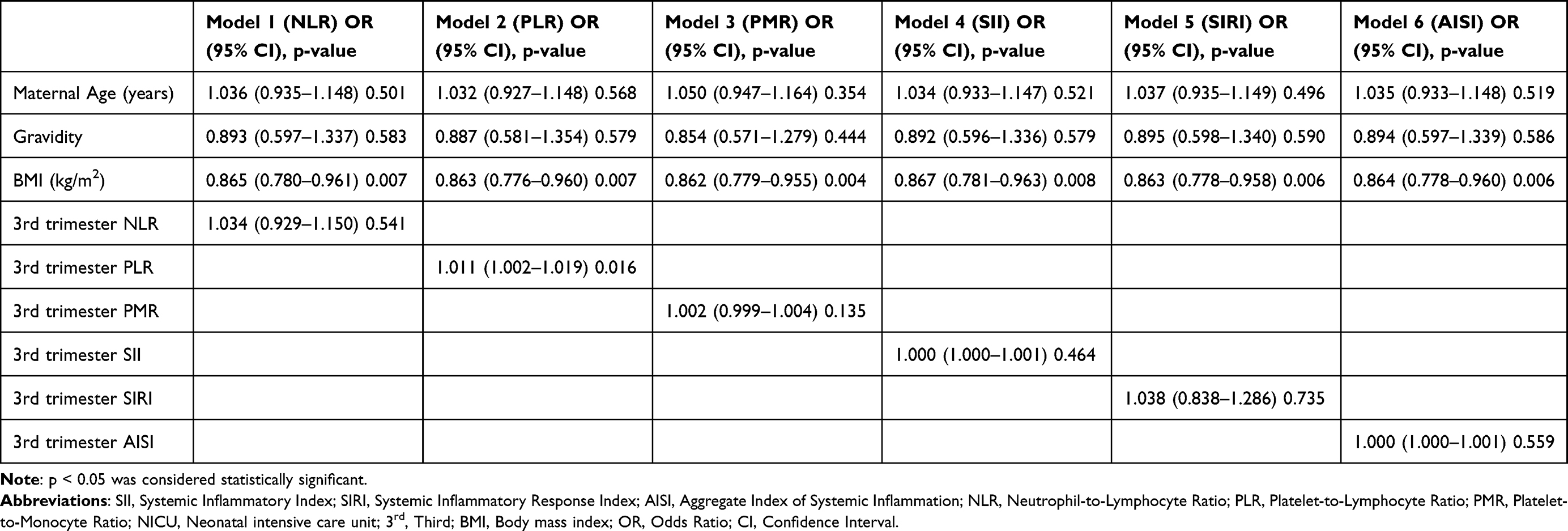 |
Table 8 Multivariate Regression Analysis to Investigate Independent Predictors of NICU Admission |
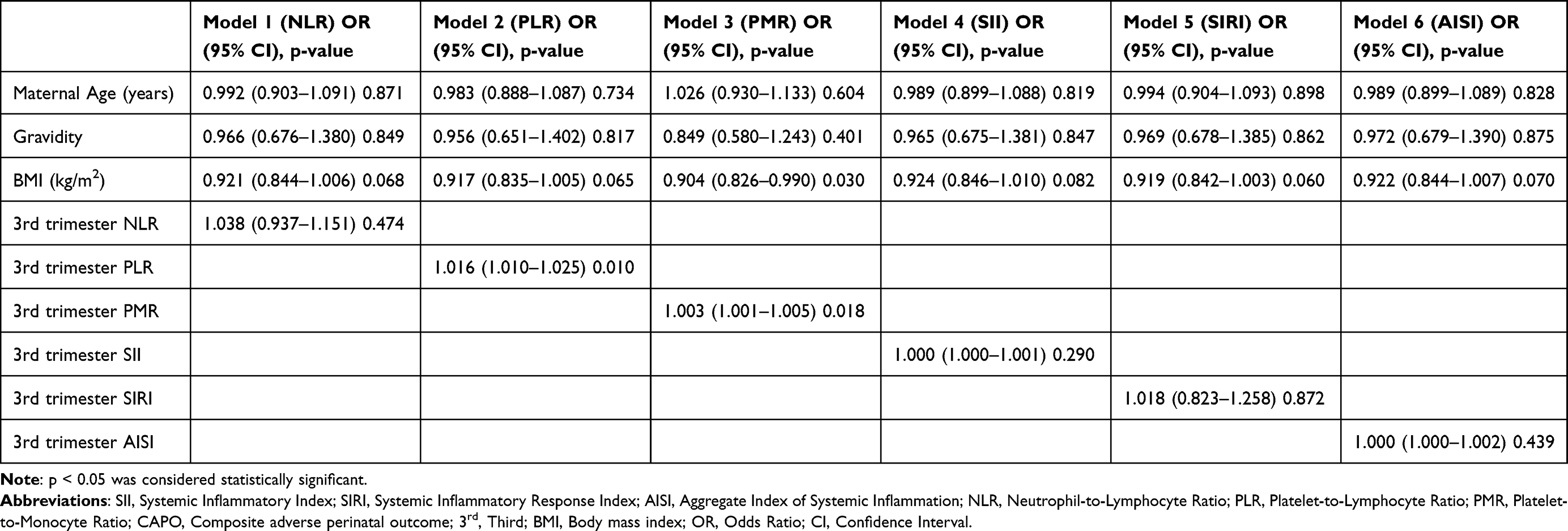 |
Table 9 Multivariate Regression Analysis to Investigate Independent Predictors of CAPO |
While first-trimester SII and AISI (p > 0.005) lost their significance for the prediction of PE, NLR and PNR (p < 0.05) remained strong independent predictors (Table 10).
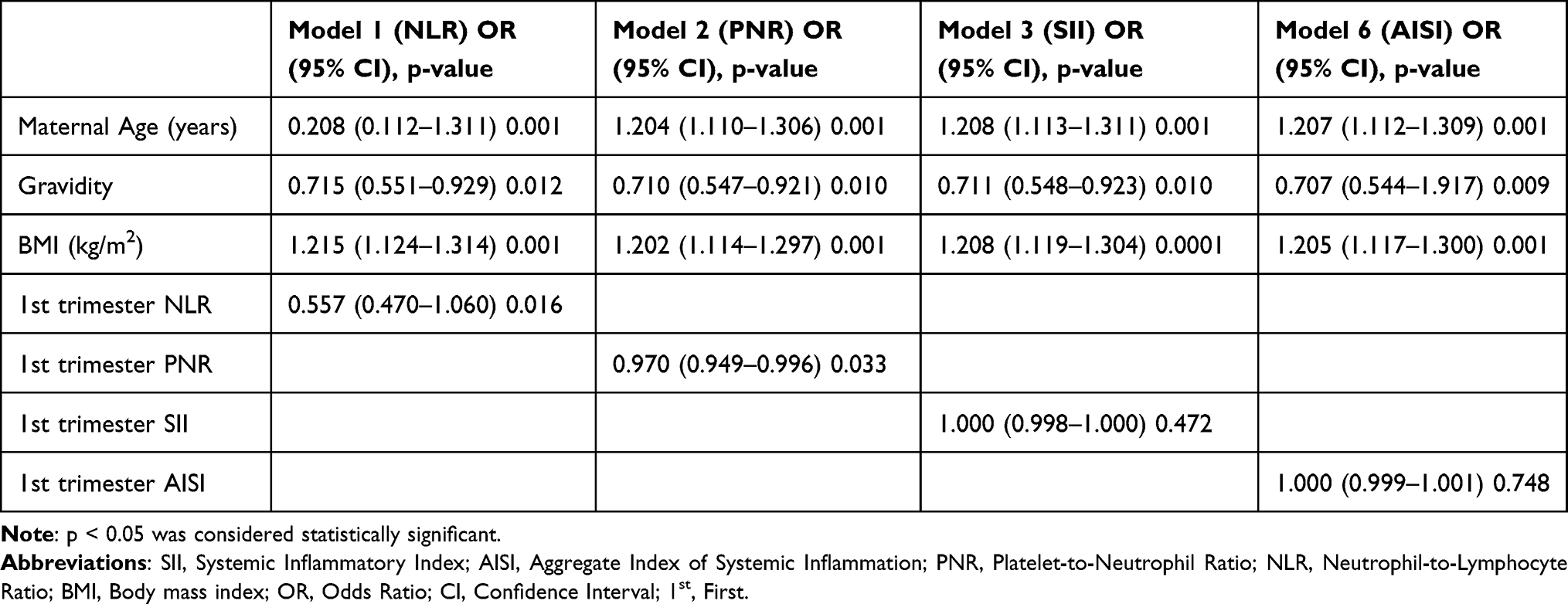 |
Table 10 Multivariate Regression Analysis to Investigate Independent Predictors of Preeclampsia |
Discussion
The aim of this study was to compare the SII, SIRI, and AISI values of patients diagnosed with PE with those of healthy controls and to investigate their role in predicting adverse pregnancy outcomes.
In our study, patients in the PE group had significantly higher BMI, C/S, CAPO, NICU admissions, PTD, while gestational age at delivery, 1-minute APGAR, 5-minute APGAR, and cord pH were significantly lower. Significant differences were observed between the study and control groups in first-trimester neutrophil, and lymphocyte counts; third-trimester Hgb, and neutrophil levels; as well as first- trimester NLR, PNR, SII, SIRI, and AISI, and third- trimester NLR, PLR, PNR, MLR, SII, SIRI, and AISI values. In the PE group, ROC analysis for predicting CAPO and NICU admission revealed significant results for NLR, PLR, PMR, SII, and AISI, whereas ROC analysis for PE prediction demonstrated significance for NLR, PNR, SII, and AISI. Following ROC analysis, multivariable logistic regression revealed that PLR independently predicted NICU admission, PLR and PMR independently predicted CAPO, and NLR and PNR independently predicted PE.
SII is increasingly recognized as a critical component in the pathogenesis of PE. The inflammatory response is associated not only with PE itself but also with adverse perinatal outcomes (APO). Previous studies have shown that pregnant women with poor fetal outcomes exhibit elevated levels of inflammatory factors in both maternal blood and amniotic fluid.11–13 Recently, inflammatory markers derived from complete blood count (CBC) have attracted increasing interest due to their low cost, simplicity, and accessibility in predicting various diseases.14
A substantial number of studies in the literature have examined inflammatory indices in relation to PE. In the meta-analysis by Kang et al, which included 15 studies investigating NLR, it was reported that NLR values were significantly higher in both severe and non-severe PE groups compared with healthy controls.15 In the study by Yavuzcan et al, a significant difference in NLR was found between the severe PE group and non-healthy pregnant women, while PLR did not show a significant difference.16 Similarly, Akdulum et al reported that first-trimester SII values were significantly higher in the PE group compared with controls and that SII was a significant predictor of PE, although its sensitivity was low, suggesting that its predictive performance could be improved when combined with other parameters.17
In our study, consistent with the findings of Yavuzcan et al, NLR values were significantly higher in the PE group compared to controls. In addition, PLR values were also found to be significantly higher in the third trimester in the preeclampsia group. We believe that the lack of a significant difference in PLR reported by Yavuzcan et al may be related to their smaller sample size and the inclusion of only patients with severe PE. Furthermore, in line with the study by Akdulum et al, first-trimester SII values were also significantly higher in our study. Similarly, ROC analysis for predicting PE showed that NLR and SII were significant predictors; however, their sensitivity remained low, consistent with previous studies.
In the study by Altuntaş et al, which evaluated NLR, SII, and SIRI values in 311 patients with preterm delivery, it was found that NLR, SII, and SIRI levels were significantly higher in the preterm birth group. After adjustment for confounding factors using multivariate regression analysis, higher NLR and SII values remained significantly associated with an increased risk of preterm birth.18 Similarly, in our study, consistent with these findings, NLR and SII values were significantly higher in the PE group, while gestational age at delivery and fetal birth weight were significantly lower. It is possible that the heightened inflammatory state may trigger biological mechanisms involved in the onset of labor, leading to earlier delivery.
In the study conducted by Seyhanlı et al, six inflammatory indices, NLR, PLR, MLR, SII, SIRI, and PIV, were evaluated in the first trimester for their predictive value in PE. Among these, SIRI and PIV were found to be significant predictors of PE, although their sensitivity (56.2% and 55.2%, respectively) and specificity (55.6% and 55%) were relatively low.7 In our study, a total of 12 hematologic parameters and 7 inflammatory indices were analyzed. For PE prediction, First-trimester NLR, SII, and AISI were found to be significant, with AISI showing the highest level of significance. Although our findings are generally consistent with the literature, some discrepancies exist among studies regarding which indices demonstrate significance. We believe these inconsistencies may result from differences in sample size, disease severity, and the inclusion of comorbid systemic conditions, while also contributing valuable insight to the existing literature.
Özkan et al divided their participants into three groups: severe PE, mild PE, and a control group. They then compared SII, PIV, and SIRI values among these groups. At the end of the study, they observed that SII, PIV, and SIRI levels were significantly higher in both the severe and mild PE groups compared to the control group. In analyses predicting PE severity, AISI emerged as a strong predictor overall, while SII was particularly strong for mild PE, and SIRI for severe PE.19 Unlike the study by Özkan et al, our study focused on the predictive value of first-trimester inflammatory indices for the development of PE rather than disease severity. In our ROC analysis for PE prediction, first-trimester NLR, PNR, SII, and AISI were found to be significant, with AISI showing the highest level of significance among these indices. However, in the multivariable regression analysis, these indices were not identified as independent predictors. This finding suggests that although these indices may have potential diagnostic value, their predictive performance may be influenced by other clinical factors and should therefore be interpreted with caution.
There are very few studies in the literature investigating the relationship between PE and NICU or CAPO. In a case-control study by Zhuang et al including 749 women with preeclampsia, designed to explore the predictive role of inflammatory markers for adverse outcomes, the PE group showed significantly higher maternal age and BMI, but lower gestational age and birth weight, as well as higher NICU admission rates, placental abruption, and cesarean section rates.20 Our findings are consistent with those of Zhuang et al, demonstrating similar trends.
In the same study by Zhuang et al, while PLR did not differ significantly between groups, NLR, SII, and SIRI were significantly higher among patients with adverse pregnancy outcomes. The AUC values for predicting adverse outcomes were 0.632 for NLR, 0.627 for SII, and 0.669 for SIRI, with optimal cutoff values of 4.959, 1070.408, and 3.346, respectively.20 In our study, we similarly observed significantly higher NLR, SII, and SIRI values in the PE group. Furthermore, NLR, SII, and AISI were found to be significant predictors of both NICU and CAPO, reinforcing the association between systemic inflammation and adverse pregnancy outcomes. However, after adjustment for confounding factors including maternal age, gravidity, and BMI, multivariable logistic regression analysis showed that third-trimester PLR was an independent predictor of NICU admission, third-trimester PLR and PMR were independent predictors of CAPO, and first-trimester NLR and PNR were independent predictors of PE. These findings suggest that certain inflammatory indices may have independent predictive value not only for PE but also for specific APO. Nevertheless, these associations should be interpreted in conjunction with clinical variables and disease severity.
The strengths of this study include its case-control design in a tertiary referral center, allowing for the comprehensive assessment of a broad range of hematologic and inflammatory indices in both the first and third-trimesters. Moreover, evaluating these indices in relation to both preeclampsia prediction and adverse perinatal outcomes provides a more integrated and clinically meaningful perspective.
The limitations of this study include its single-center and retrospective design, the relatively small sample size, the lack of evaluation of severe PE prediction, and the limited availability of detailed obstetric history data. These factors may have affected the adjustment for potential confounding variables and the generalizability of the findings.
Conclusion
In this study, NLR, PLR, SII, and AISI were found to be significant predictors for NICU and CAPO, while NLR, PNR, SII, and AISI were significant for the prediction of PE. However, after adjustment for confounding factors including maternal age, gravidity, and BMI, multivariable logistic regression analysis showed that third-trimester PLR was an independent predictor of NICU admission, third-trimester PLR and PMR were independent predictors of CAPO, and first-trimester NLR and PNR were independent predictors of PE. These findings suggest that certain inflammatory indices may have independent predictive value for PE, NICU, and CAPO. However, they should be interpreted in conjunction with clinical variables and considered as supportive adjuncts rather than stand-alone decision-making tools in clinical practice.
Ethics Committee Approval
This study was approved by the Clinical Research Ethics Committee of the University of Health Sciences, Gazi Yaşargil Training and Research Hospital (Decision No: 567, Date: 25.07.2025).
Informed Consent
The authors declared that it was not considered necessary to get consent from the patients because the study was a retrospective data analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no financial support from any private or public institution.
Disclosure
The authors declare that there is no conflict of interest for this work.
References
1. Dimitriadis E, Rolnik DL, Zhou W, et al. Preeclampsia. Nat Rev Dis Prim. 2023;9(1):35. doi:10.1038/s41572-023-00451-4
2. American College of Obstetricians and Gynecologists. Gestational hypertension and preeclampsia: ACOG practice bulletin no. 222. Obstet Gynecol. 2020;135(6):e237–16. doi:10.1097/AOG.0000000000003891
3. Gathiram P, Moodley J. Pre-eclampsia: its pathogenesis and pathophysiology. Cardiovasc J Afr. 2016;27(2):71–78. doi:10.5830/CVJA-2016-009
4. Wang Y, Li B, Zhao Y. Inflammation in preeclampsia: genetic biomarkers, mechanisms, and therapeutic strategies. Front Immunol. 2022;13:883404. doi:10.3389/fimmu.2022.883404
5. Mannaerts D, Heyvaert S, De Cordt C, Macken C, Loos C, Jacquemyn Y. Are the neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), and/or mean platelet volume (MPV) clinically useful as predictive parameters for preeclampsia? J Matern Fetal Neonatal Med. 2019;32(9):1412–1419. doi:10.1080/14767058.2017.1410701
6. Mohamed RA, Ali IA. The role of neutrophil/lymphocyte ratio, uric acid/albumin ratio, and uric acid/creatinine ratio in predicting the severity of preeclampsia. BMC Pregnancy Childbirth. 2023;23(1):763. doi:10.1186/s12884-023-06083-6
7. Seyhanli Z, Bayraktar B, Baysoz OB, et al. The role of first-trimester serum inflammatory indices (NLR, PLR, MLR, SII, SIRI, and PIV) and the β-hCG/PAPP-A ratio in predicting preeclampsia. J Reprod Immunol. 2024;162:104190. doi:10.1016/j.jri.2023.104190
8. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
9. Maziashvili G, Juliana K, Kanimozhi VSSP, et al. Use of systemic inflammatory markers derived from routine blood tests in predicting preeclampsia and the effect of age on marker levels. Cureus. 2023;15(3):e35836. doi:10.7759/cureus.35836
10. Wang J, Zhu QW, Cheng XY, et al. Assessment efficacy of neutrophil-lymphocyte ratio and monocyte-lymphocyte ratio in preeclampsia. J Reprod Immunol. 2019;132:29–34. doi:10.1016/j.jri.2019.02.001
11. Pala Ş, Atilgan R, Ilhan N. High amniotic fluid fractalkine and MIP-1β levels are associated with intrauterine growth restriction: a prospective cohort study. Turk J Med Sci. 2023;54(1):280–290. doi:10.55730/1300-0144.5789
12. Pala Ş, Atılgan R, Çim B, et al. Investigation of fractalkine and MIP-1β levels as biomarkers in premature rupture of membranes: a prospective cohort study. Clin Exp Obstet Gynecol. 2023;50(7):155. doi:10.31083/j.ceog5007155
13. Kağan Açıkgözoğlu M, Pala Ş, Atılgan R, Ilhan N, Ilhan N. High serum angiopoietin-like protein-4 levels are associated with gestational hypertension and preeclampsia: a case-control study. Turk JBiochem. 2024;49(3):344–348. doi:10.1515/tjb-2023-0087
14. Xiao S, Wang Z, Zuo R, et al. Association of systemic immune-inflammation index with all-cause, cardiovascular, and cancer-related mortality in patients with cardiovascular disease: a cross-sectional study. J Inflamm Res. 2023;16:941–961. doi:10.2147/JIR.S402227
15. Kang Q, Li W, Yu N, et al. Predictive role of neutrophil-to-lymphocyte ratio in preeclampsia: a meta-analysis of 3982 patients. Pregnancy Hypertens. 2020;20:111–118. doi:10.1016/j.preghy.2020.03.009
16. Yavuzcan A, Çağlar M, Üstün Y, et al. Mean platelet volume, neutrophil-to-lymphocyte ratio, and platelet-to-lymphocyte ratio in severe preeclampsia. Ginekologia Polska. 2014;85(3):197–203. [PMID:24783431]. doi:10.17772/gp/1713
17. Cevher Akdulum MF, Demirdağ E, Arık Sİ, et al. Is first-trimester systemic immune-inflammation index associated with preeclampsia? Cureus. 2023;15(8):e44063. doi:10.7759/cureus.44063
18. Bezirganoğlu Altuntaş N, Baki Yıldırım S, Bayoğlu Tekin Y. Can inflammatory markers predict the risk of early and preterm birth in women with threatened preterm labor? J Matern Fetal Neonatal Med. 2025;38(1):2566235. doi:10.1080/14767058.2025.2566235
19. Özkan S, Dereli ML, Fıratlıgil FB, et al. The role of systemic immune-inflammation index, systemic inflammation response index, and pan-immune inflammation value in predicting preeclampsia: a retrospective cohort study. Am J Reprod Immunol. 2024;92(6):e70029. doi:10.1111/aji.70029
20. Zhuang Y, Xiao Y, Bai R, et al. Association between peripheral blood immuno-inflammatory biomarkers, preeclampsia, and adverse outcomes: a retrospective study. J Inflamm Res. 2025;18:4359–4366. doi:10.2147/JIR.S504552
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Platelet, Neutrophil and Lymphocyte Quantitative Abnormalities in Patients with Heart Failure: A Retrospective Study
Getawa S, Bayleyegn B
Vascular Health and Risk Management 2023, 19:69-78
Published Date: 5 February 2023
Low HALP (Hemoglobin, Albumin, Lymphocyte, and Platelet) Score Increases the Risk of Post-Stroke Cognitive Impairment: A Multicenter Cohort Study
Zuo L, Dong Y, Liao X, Hu Y, Pan Y, Yan H, Wang X, Zhao X, Wang Y, Seet RCS, Wang Y, Li Z
Clinical Interventions in Aging 2024, 19:81-92
Published Date: 10 January 2024