Back to Journals » Infection and Drug Resistance » Volume 15
Predictive Value of Combination of Procalcitonin and Predisposition, Infection, Response, and Organ Dysfunction (PIRO) System in Septic Patients with Positive Blood Cultures in the Emergency Department
Authors Yang L ![]() , Lin Y, Zhang X
, Lin Y, Zhang X ![]() , Wei B, Wang J, Liu B
, Wei B, Wang J, Liu B
Received 10 August 2022
Accepted for publication 13 October 2022
Published 26 October 2022 Volume 2022:15 Pages 6189—6202
DOI https://doi.org/10.2147/IDR.S384689
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Long Yang,1,* Yue Lin,2,* Xiangqun Zhang,1 Bing Wei,1 Junyu Wang,1 Bo Liu1
1Emergency Medicine Clinical Research Center, Beijing Chao-Yang Hospital, Capital Medical University, & Beijing Key Laboratory of Cardiopulmonary Cerebral Resuscitation, Beijing, 100020, People’s Republic of China; 2Department of Radiology, China-Japan Friendship Hospital, Beijing, 100029, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bo Liu; Junyu Wang, Emergency Medicine Clinical Research Center, Beijing Chao-Yang Hospital, Capital Medical University, & Beijing Key Laboratory of Cardiopulmonary Cerebral Resuscitation, Beijing, 100020, People’s Republic of China, Tel/Fax +86 10-51718171, Email [email protected]; [email protected]
Purpose: Procalcitonin and predisposition, infection, response, and organ dysfunction (PIRO) system have high predictive value for the prognosis of critically ill patients. There are few studies on the predictive value of patients with positive blood cultures. The aim of the study was to evaluate risk stratification and sepsis-related mortality in patients with positive blood cultures via procalcitonin (PCT) combined with the PIRO system in emergency departments (ED).
Methods: A total of 1074 patients with positive blood cultures were admitted to Beijing Chao-Yang Hospital ED from December 2017 to October 2020. Their serum PCT was recorded, along with a Sequential Organ Failure Assessment (SOFA) score, Mortality in Emergency Department Sepsis (MEDS) score, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, and PIRO score to predict the prognosis of septic patients with positive blood culture in terms of ICU (intensive care unit) admission, multiple organ dysfunction syndrome (MODS) development, and 28-day mortality. Receiver operating characteristic (ROC) curves and logistic regression analysis were used to assess the prognostic value of the scoring systems.
Results: A total of 978 patients met the inclusion criteria. PCT, MEDS, APACHE II, and PIRO scores were found to independently predict ICU-admission, MODS development, and 28-day mortality (P< 0.05), whereas SOFA did not. The AUC values of the PCT, MEDS, APACHE II, and PIRO scores for ICU-admission were 0.620, 0.740, 0.780, and 0.751, respectively. In the prediction of 28-day mortality, the AUC values of PCT, MEDS, APACHE II, and PIRO were 0.782, 0.745, 0.805, and 0.831, respectively. The AUC values combined PCT and PIRO system in predicting MODS and 28-day mortality were better than when predicting ICU-admission.
Conclusion: This study indicates that PCT combined with the PIRO scoring system has a higher predictive value and is superior in predicting MODS and 28-day mortality in septic patients with positive blood cultures.
Keywords: procalcitonin, PIRO scoring system, positive blood culture, 28-day mortality
Introduction
Bacteremia and sepsis are common problems in clinical practice. The term bacteremia denotes the presence of bacteria in the blood.1 Approximately 200,000 patients are affected by bacteremia each year, with 10 cases per 1000 hospital admissions.2,3 Bacteremia has high mortality, and due to the obvious dangers of undertreatment, many physicians liberally order cultures.4 Unlike bacteremia, sepsis is more severe, often involving organ function. Sepsis is a syndrome of systemic inflammation in response to infection, traditionally be defined as life-threatening organ failure by a dysregulated host response to infection, which is usually a leading cause of high morbidity and mortality in hospitalized patients.5 Septic shock remains the dominant cause of death in the United States.6 Blood cultures are generally considered to be the most sensitive method of detecting bacteremia and are useful in certain diagnoses and critically ill patients.7,8 The blood culture results can be used to guide the adjustment of antibiotics regimes.9 Positive blood culture usually indicates a serious infection with fever, chills, leukocytosis, focal infection, sepsis, or suspected endocarditis, and has poor outcome.4
The concept of the predisposition, infection, response, and organ dysfunction (PIRO) scoring system was presented at the 2001 International Sepsis Definitions Conference, to improve on traditional sepsis classification.10 The PIRO system is an ideal staging system that incorporates assessment of premorbid baseline susceptibility, specific disorders responsible for illness, host response to infection, and the resulting degree of organ dysfunction. The four components of the PIRO system cover multiple independent factors that may influence the onset, development, and outcome of sepsis.11 Since the first PIRO system appeared in 2008, many different PIRO systems have been developed. The PIRO system mainly used to study ICU populations with ICU specific features is not suitable for the ED. A new PIRO system developed by Howell is designed for bedside use and is superior to other PIRO systems.12 Our study applied the Howell-PIRO scoring system to predict the risk stratification and prognosis of septic patients with positive blood cultures in the ED. PCT, a prohormone of calcitonin, encoded by the calcitonin-I (CALC-1) gene on chromosome 11, has successfully detected infection, as well as providing antibiotic management guidance.13 It is able to predict infectious origin of a shock occurring in an acutely ill patient with reasonable accuracy. The increase of PCT is related to the appearance and severity of bacterial infection in ICU patients.14 It has been used extensively as a biomarker in sepsis diagnosis, risk stratification, prognosis evaluation, and therapy monitoring in recent years.
However, we found that a large percentage of positive blood culture patients were not admitted to the ICU, and did not develop MODS in clinical practice, instead, following timely, systematic, and effective treatment, they were successfully discharged. Therefore, finding suitable methods for the prognosis of patients with positive blood culture is highly important. Consequently, in view of the strong predictive value of PIRO scoring system and PCT in infectious diseases, we attempted to use PIRO scoring system combined with PCT to evaluate the risk stratification and sepsis-related mortality in patients with positive blood cultures in the ED.
Methods
Patients
The study was conducted in Beijing Chao-Yang Hospital ED, a tertiary teaching hospital of Capital Medical University, and was approved by the human research ethics committee of Beijing Chao-Yang Hospital. A total of 1074 septic patients with positive blood cultures were enrolled in our cohort from 2017 to 2020, and written informed consent upon ED admission was acquired.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) Patients signed informed consent forms; (2) Age >18 years; (3) Patients with sepsis according to Sepsis-3 (suspected or definite infection with an increase in SOFA score ≥2).15 (4) Positive blood culture results. The exclusion criteria were as follows: (1) Age < 18 years; (2) Terminal stage of disease (malignant cancer with metastases, AIDS, end-stage renal or hepatic disease, chronic heart failure); (3) Viral or fungal infection with positive blood cultures. (4) Refusal to participate in the study by patients or their relatives or transferred to other hospitals.
Data Collection
Patient characteristics were recorded including age, gender, vital signs, and past medical history. Whole blood leukocyte counts, blood gas indexes, and blood biochemistry were identified within 24h. The SOFA, MEDS, APACHE II, and PIRO scores were calculated according to vital signs, and laboratory test results. PCT, CRP (C-reactive protein), Lac (Lactate) and ALB (albumin) were detected by separating blood samples in the laboratory. For PCT, blood samples were collected in serum separating gel tubes and blood culture samples in Bactec bottles. They were centrifuged at 2000 g for 15 min and serum was separated and stored at −20 °C until assayed. Serum PCT was analyzed by Roche Elecsys BRAHMS PCT reagent, on electrochemiluminescence automated immunoassay analyser. NLR (Neutrophil-to-Lymphocyte Ratio) was calculated based on existing data. The Howell-PIRO scoring system16 was applied in this study, and the criteria (not included malignant cancer with metastases) are shown in Table 1.
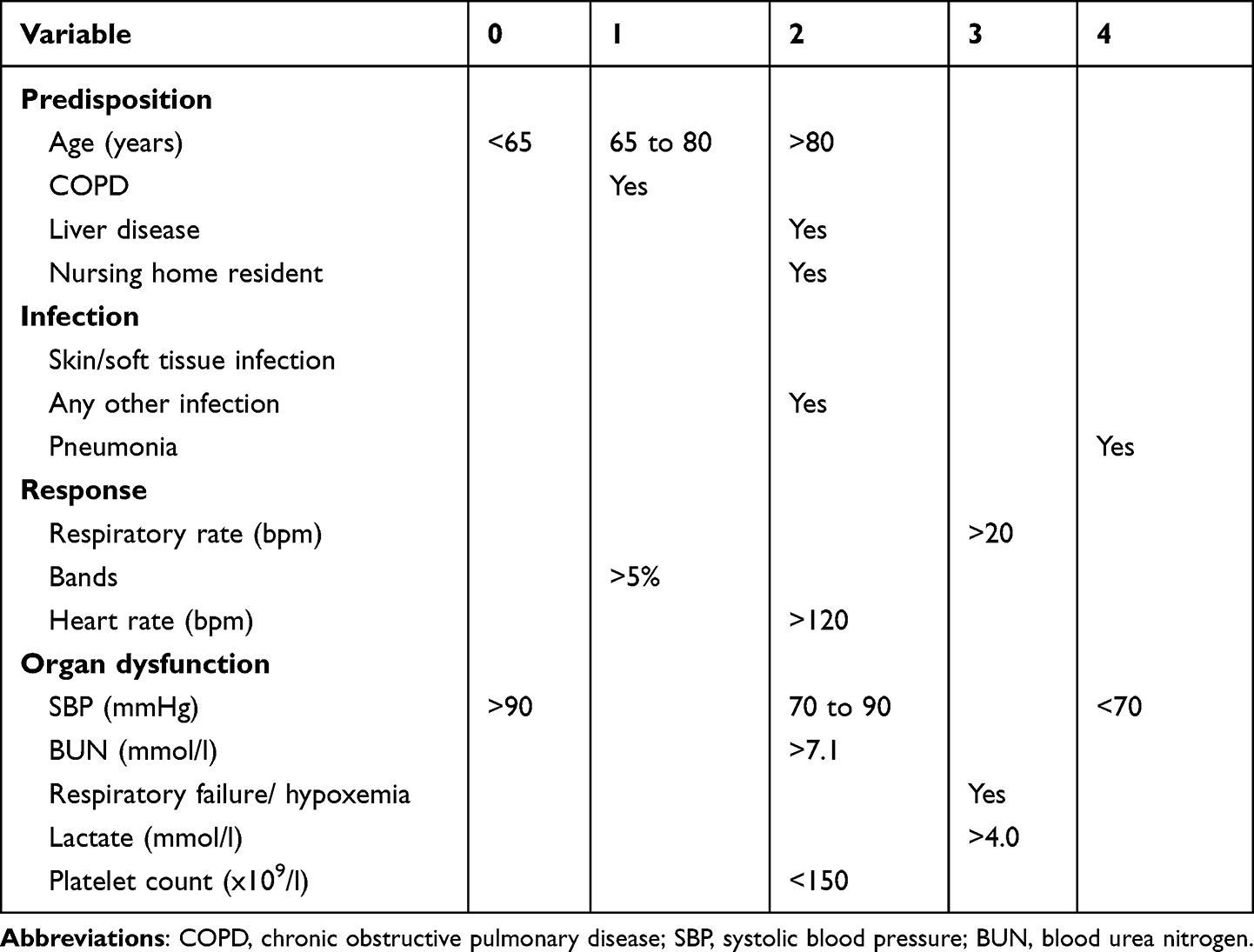 |
Table 1 Criteria of the Howell-PIRO System (Not Included Malignancy) |
Outcome Variables
MODS was defined as the fulfillment of two or more of the severe sepsis criteria at any time within 3 days of enrollment, excluding organ dysfunction, induced by pre-existing disease.11 Organ function was assessed at enrollment and reassessed when deterioration occurred. All patients were followed up for 28 days through medical records or by telephone. ICU admission during follow-up, development of MODS within 3 days, and 28-day mortality were considered as the outcome criteria.
Statistical Analysis
All data were analyzed by SPSS 25.0 (SPSS Inc., Chicago, IL, USA). Normally distributed data, expressed as the mean ± standard (mean±SD) deviation, was compared using an independent-samples t-test. Data with skewed distribution was expressed as the median and quartiles, and was analyzed via a Mann–Whitney U-test, and a chi-square test was used to compare frequencies. Logistic regression analysis was used to determine the independent outcome predictors. Receiver operating characteristic (ROC) curves were constructed and the area under the curves (AUC) was determined to assess predictive value. Kaplan-Meier 28-day survival curves were constructed, and Log rank tests were used to compare the curves. All statistical tests were two-tailed, and P < 0.05 was considered statistically significant.
Results
Characteristics of the Study Cohort
As Figure 1 shows, a total of 1074 septic patients with positive blood cultures in the ED between 2017 and 2020 were enrolled in this study. 71 patients had a viral or fungal infection, 10 patients refused to participate, and 15 patients were transferred to other hospitals. Finally, 978 participants completed the 28 follow-up days.
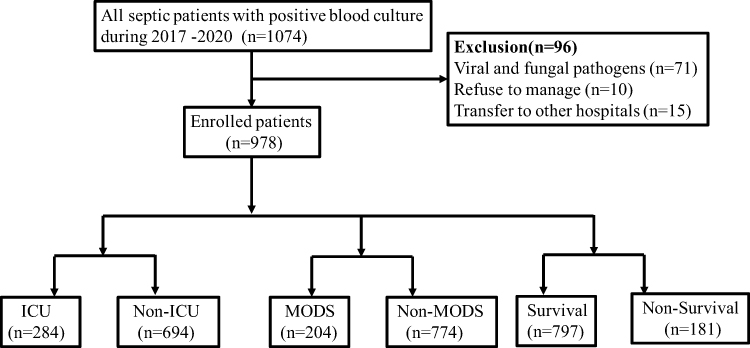 |
Figure 1 Flowchart of the study population. |
In our study, 978 septic patients with positive blood cultures were divided into ICU (n=284) and non-ICU (n=694) admission groups. When comparing the characteristics of these patients, we found that there were significant differences in age (P=0.040), chronic obstructive pulmonary disease (COPD) (P<0.001), hypertension (P=0.001), chronic heart failure (CHF) (P=0.007), mean arterial pressure (MAP) (P<0.001), heart rate (HR) (P<0.001), white blood cells (WBC) (P<0.001), Lac (P<0.001), PCT (P<0.001), CRP (P<0.001), ALB (P<0.001), SOFA (P<0.001), MEDS (P<0.001), APACHE II (P<0.001), and PIRO (P<0.001) between ICU and non-ICU admission groups (Table 2, Figure 1).
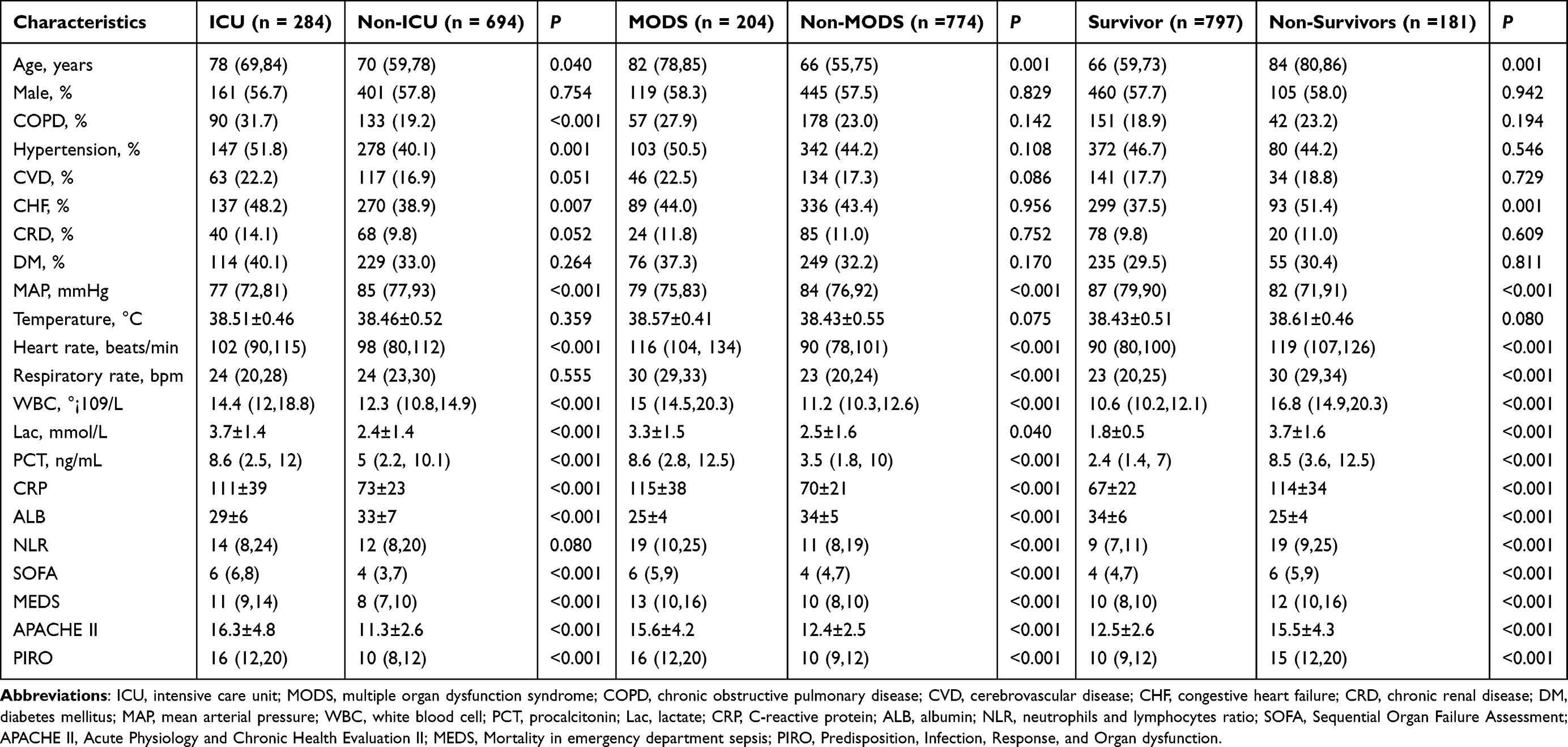 |
Table 2 Characteristics of the Study Cohort |
In addition, we also divided the participants into two other categories, MODS (n=204) and non-MODS (n=774) according to the development of MODS within 3 days. There were obvious differences in age (P=0.001), MAP (P<0.001), HR (P<0.001), respiratory rate (RR) (P<0.001), WBC (P=0.001), Lac (P=0.040), PCT (P<0.001), CRP (P<0.001), ALB (P<0.001), NLR (P<0.001), SOFA (P<0.001), MEDS (P<0.001), APACHE II (P<0.001), and PIRO (P<0.001) between these two groups (Table 2, Figure 1).
After 28 days follow-up, statistical differences were evident in age (P=0.001), chronic heart failure (CHF) (P=0.001), MAP (P<0.001), HR (P<0.001), RR (P<0.001), WBC (P<0.001), Lac (P=0.040), PCT (P<0.001), CRP (P<0.001), ALB (P<0.001), NLR (P<0.001), SOFA (P<0.001), MEDS (P<0.001), APACHE II (P<0.001), and PIRO (P<0.001) between survivor (n=797) and non-survivor (n=181) groups (Table 2, Figure 1).
The median of the SOFA, MEDS, and PIRO scores, and mean of the APACHE II score in ICU-admission, MODS development, and 28-day mortality groups are shown in Table 2, Figure 2. The average SOFA, MEDS, APACHE II, and PIRO scores differed significantly between patients who did, and did not, meet the outcome criteria (P<0.001).
 |
Figure 2 The median levels of SOFA, MEDS and PIRO scores, and mean level of APACHE II score in ICU-admission, developing of MODS and 28-day mortality groups. (A) The median level of SOFA score in ICU-admission, developing of MODS and 28-day mortality groups. (B) The median level of MEDS score in ICU-admission, developing of MODS and 28-day mortality groups. (C) The mean level of APACHE II score in ICU-admission, developing of MODS and 28-day mortality groups. (D) The median level of PIRO score in ICU-admission, developing of MODS and 28-day mortality groups. |
Spearman Correlations Between 28-Day Mortality and SOFA, MEDS, APACHE II or PIRO Score
To investigate the correlations between 28-day mortality and SOFA, MEDS, APACHE II or PIRO score, Spearman correlation analysis was performed. Significant negative linear correlations of 28-day mortality with SOFA, MEDS, APACHE II or PIRO score were presented in Figure 3A–D (r values were −0.62, −0.75, −0.64, −0.49 respectively, and all P<0.001).
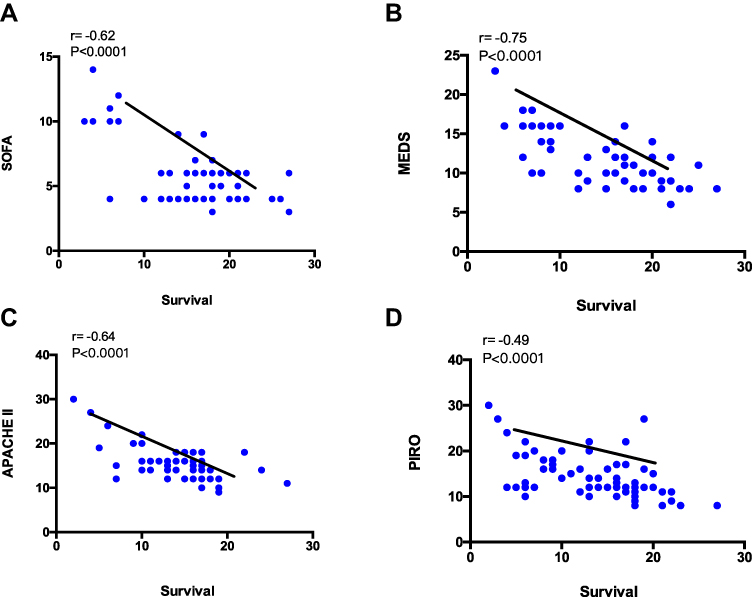 |
Figure 3 Spearman correlations between 28-day mortality and SOFA score (A); MEDS score (B); APACHE II score (C); PIRO score (D) in patients with positive blood cultures. |
Binary Logistic Regression Analysis of the Prognostic Outcome of Septic Patients with Positive Blood Cultures in the ED
Binary logistic regression was used to analyze the independent predictors in our study cohort. The results showed that WBC (β=0.176, odds ratio (OR) (95% CI) =1.192 (1.031–1.379), P=0.018), PCT (β=0.241, OR (95% CI) =1.273 (1.037–1.563), P=0.021), Lac (β=1.261, OR (95% CI) =3.530 (1.867–6.676), P<0.001), ALB (β=−0.142, OR (95% CI) =0.867 (0.792–0.949), P=0.002), NLR (β=0.077, OR (95% CI) =1.080 (1.011–1.155), P=0.023), MEDS score (β=0.895, OR (95% CI) =2.447 (1.607–3.728), P<0.001), APACHE II score (β=0.623, OR (95% CI) =1.864 (1.405–2.474), P<0.001) and PIRO score (β=0.328, OR (95% CI) =1.388 (1.118–1.723), P=0.003) were the independent predictors of ICU-admission, but the SOFA score (β=0.220, OR (95% CI) =2.701 (1.548–4.713), P=0.120) was not (Table 3).
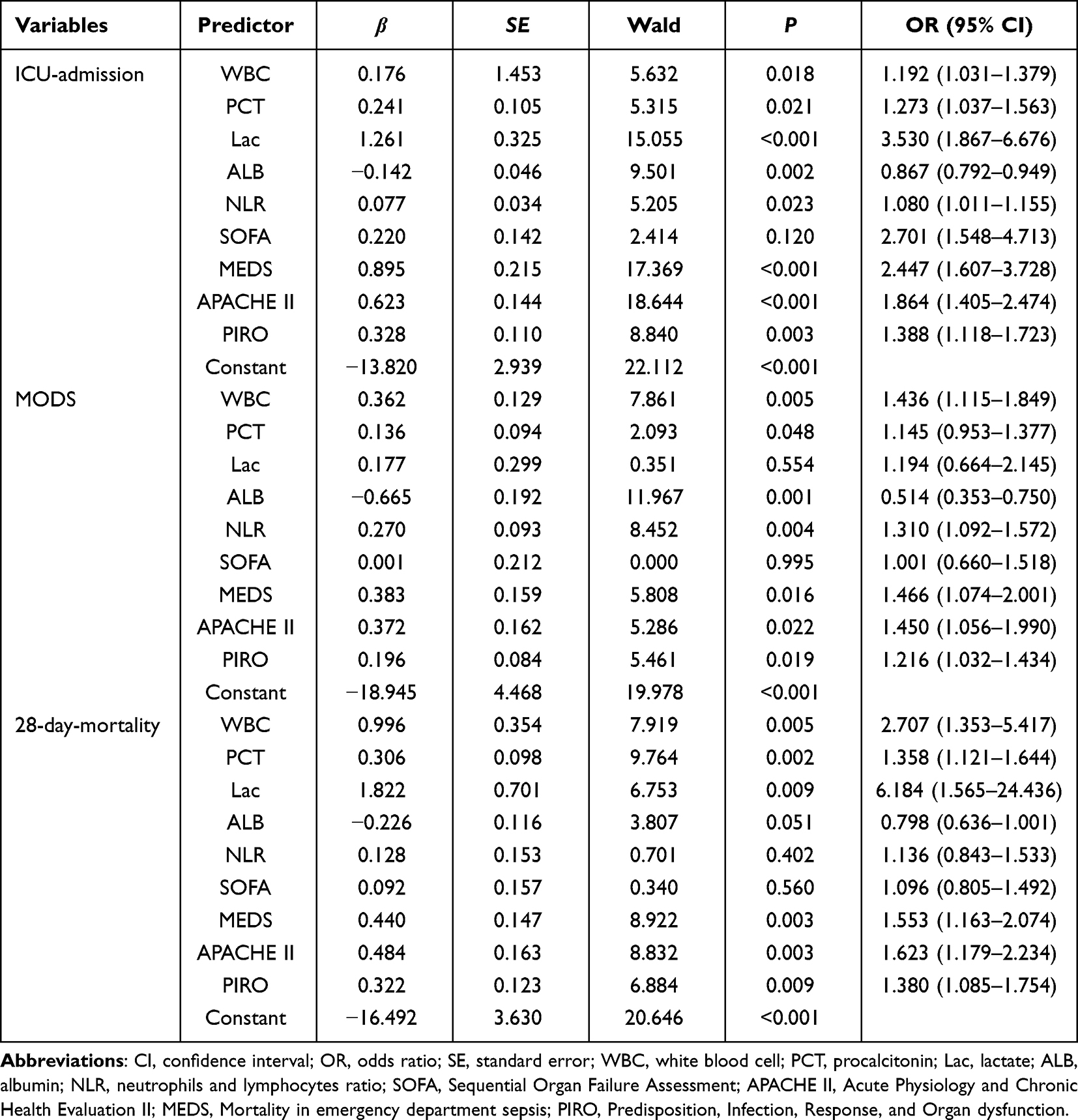 |
Table 3 Binary Logistic Regression Analysis of Clinical Outcome for Septic Patients with Positive Blood Culture |
In MODS development, WBC (β=0.362, OR (95% CI) =1.436 (1.115–1.849), P=0.005), PCT (β=0.136, OR (95% CI) =1.145 (0.953–1.377), P=0.048), ALB (β=−0.665, OR (95% CI) =0.514 (0.353–0.750), P=0.001), NLR (β=0.270, OR (95% CI) =1.310 (1.092–1.572), P=0.004), MEDS score (β=0.383, OR (95% CI) =1.466 (1.074–2.001), P=0.016), APACHE II score (β=0.372, OR (95% CI)=1.450 (1.056–1.990), P=0.022), and PIRO score (β=0.196, OR (95% CI) =1.216 (1.032–1.434), P=0.019) were the independent predictors of developing MODS, but the SOFA scores (β=0.001, OR (95% CI) =1.001 (0.660–1.518), P=0.995) and Lac (β=0.177, OR (95% CI) =1.194 (0.664–2.145), P=0.554) determined it was not a predictor (Table 3).
In addition, with 28-day mortality, the results showed that WBC (β=0.996, OR (95% CI) =2.707 (1.353–5.417), P=0.005), PCT (β=0.306, OR (95% CI) =1.358 (1.121–1.644), P=0.002), Lac (β=1.822, OR (95% CI) =6.184 (1.565–24.436), P=0.009), MEDS score (β=0.440, OR (95% CI) =1.553 (1.163–2.074), P=0.003), APACHE II score (β=0.484, OR (95% CI) =1.623 (1.179–2.234), P=0.003), and PIRO score (β=0.322, OR (95% CI) =1.380 (1.085–1.754), P=0.009) were the independent predictors of 28-day mortality, but SOFA (β=0.092, OR (95% CI) =1.096 (0.805–1.492), P=0.560), NLR (β=0.128, OR (95% CI) =1.136 (0.843–1.533), P=0.402), and ALB (β=−0.226, OR (95% CI) =0.798 (0.636–1.001), P=0.051) were not (Table 3).
Prediction of the Prognostic Outcomes of Septic Patients with Positive Blood Cultures
The ROC curves of the PCT, combined with the severe scores for predicting outcomes in septic patients with positive blood cultures, for ICU-admission, MODS development, and 28-day mortality are shown in Figure 4, and the AUCs are presented in Tables 4–6. The AUC values of the PCT, MEDS, APACHE II, and PIRO scores for ICU-admission were 0.620 (95% CI: 0.533–0.706, P=0.009), 0.740 (95% CI: 0.663–0.817, P<0.001), 0.780 (95% CI: 0.709–0.850, P<0.001), 0.751 (95% CI: 0.674–0.828, P<0.001), respectively. The AUC values of a combination of PCT and severe scores for ICU-admission were as follows: PCT+MEDS: 0.772 (95% CI: 0.698–0.846, P<0.001); PCT+APACHE II: 0.821 (95% CI: 0.757–0.885, P<0.001); PCT+PIRO: 0.795 (95% CI: 0.723–0.867, P<0.001). The predictive ability of APACHE II (AUC:0.780) for ICU-admission was slightly better than that of MEDS (AUC: 0.740) and PIRO (AUC:0.751). Consequently, PCT+APACHE II (AUC:0.821) is much better at predicting ICU admission than PCT+MEDS (AUC:0.772) and PCT+PIRO (AUC:0.795) (Figure 4A, Table 4).
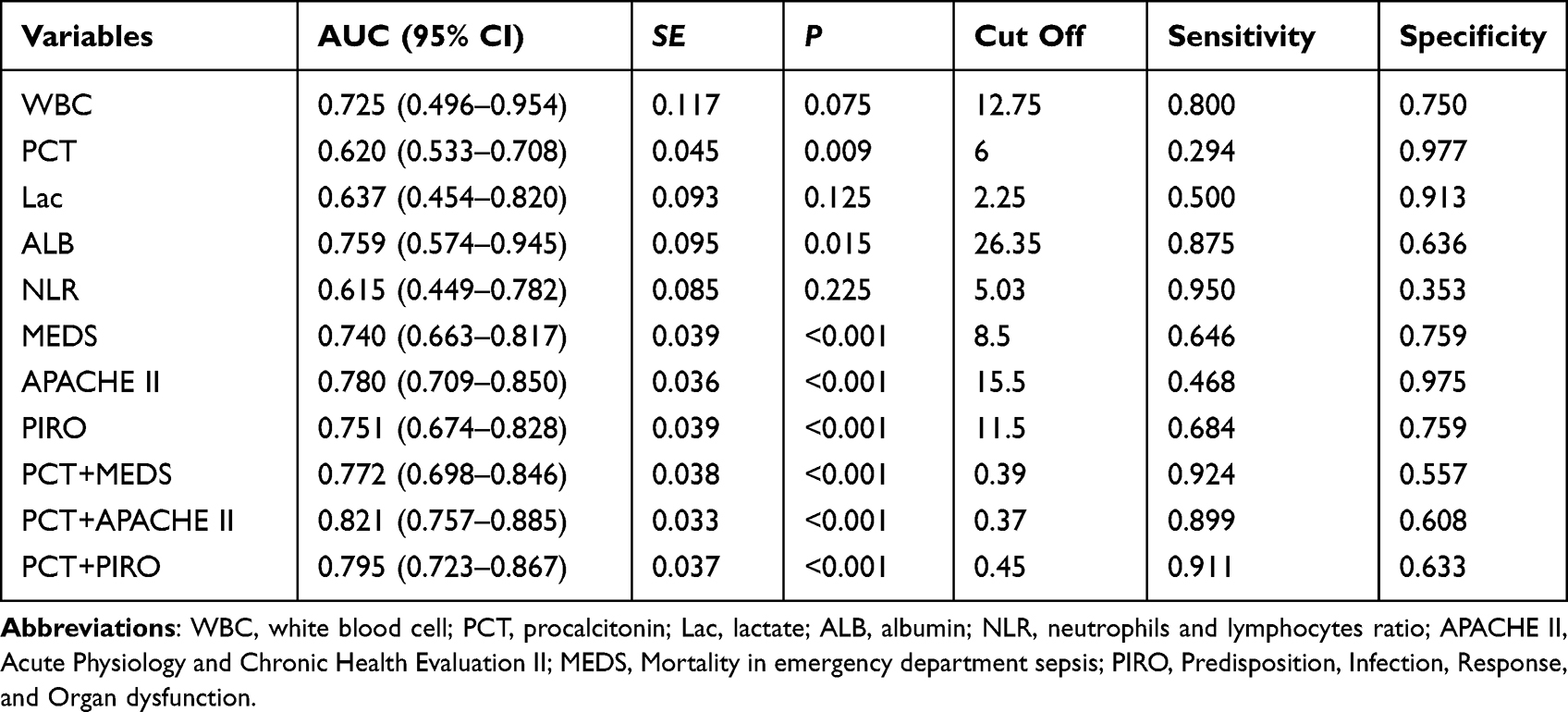 |
Table 4 Statistical Data of ROC Curve in Predicting ICU-Admission in Patients with Positive Blood Cultures |
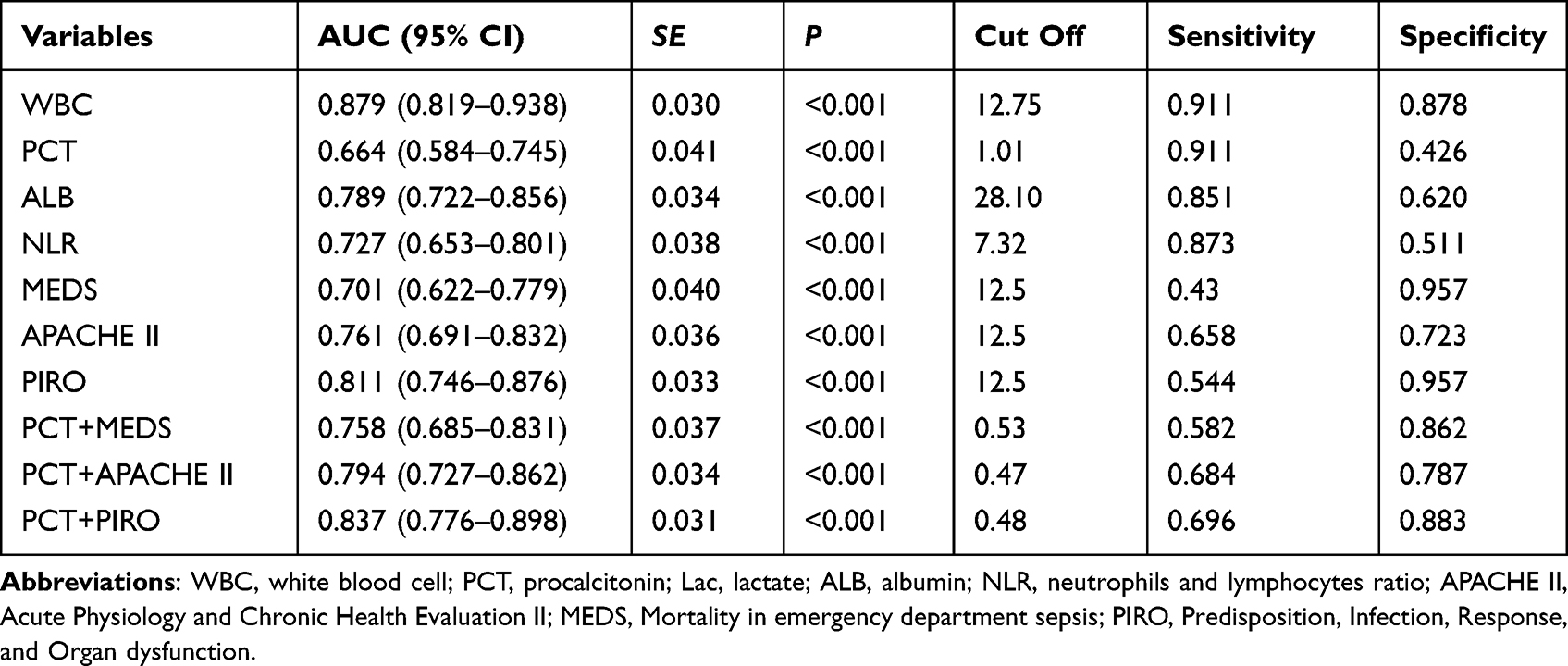 |
Table 5 Statistical Data of ROC Curve in Predicting MODS in Patients with Positive Blood Cultures |
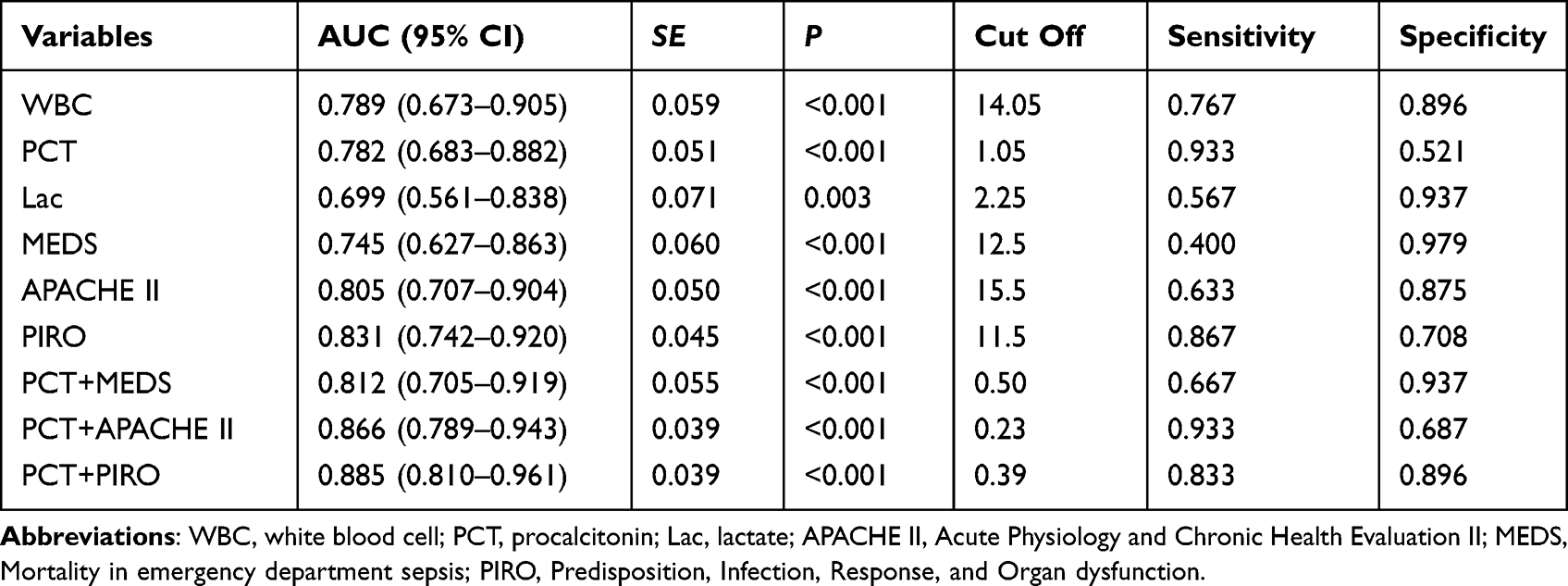 |
Table 6 Statistical Data of ROC Curve in Predicting 28-Day-Mortality in Patients with Positive Blood Cultures |
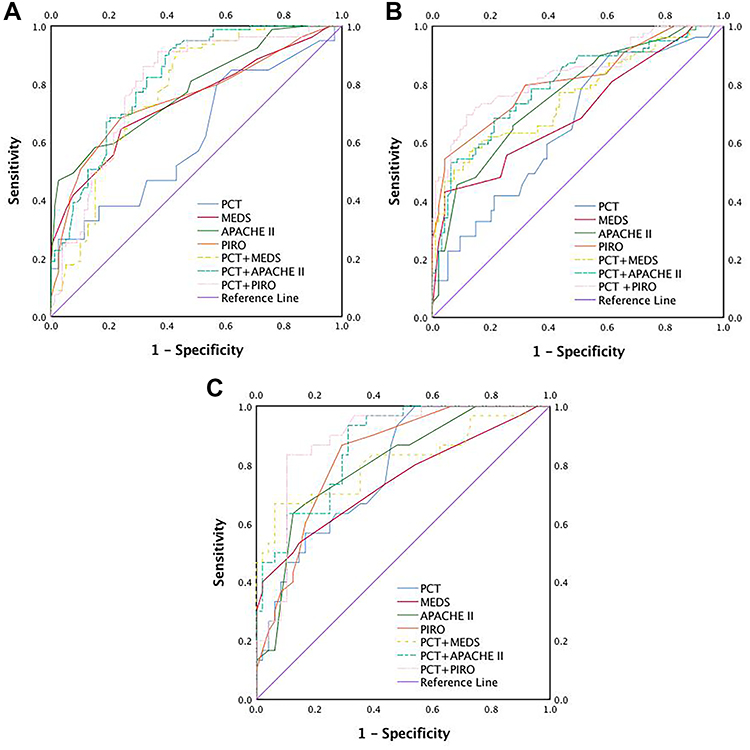 |
Figure 4 The ROC curves of PCT combined with severe scores for predicting outcomes in septic patients with positive blood cultures for ICU-admission, developing of MODS and 28-day mortality. (A) The ROC curves of PCT combined with severe scores in septic patients with positive blood cultures for ICU-admission; (B) the ROC curves of PCT combined with severe scores in septic patients with positive blood cultures for developing of MODS; (C) the ROC curves of PCT combined with severe scores in septic patients with positive blood cultures for 28-day mortality. |
Furthermore, for MODS incidence, the AUC values of the PCT, MEDS, APACHE II, and PIRO scores were 0.664 (95% CI: 0.584–0.745, P<0.001), 0.701 (95% CI: 0.622–0.779, P<0.001), 0.761 (95% CI: 0.691–0.832, P<0.001), 0.811 (95% CI: 0.746–0.876, P<0.001), respectively. The AUC values of the combination of PCT and severity scores were as follows: PCT+MEDS: 0.758 (95% CI: 0.685–0.831, P<0.001); PCT+APACHE II: 0.794 (95% CI: 0.727–0.862, P<0.001); PCT+PIRO: 0.837 (95% CI: 0.776–0.898, P<0.001). The ability of PIRO (AUC:0.811) to predict the onset of MODS was much better than that of MEDS (AUC: 0.701) and APACHE II (AUC: 0.761). Therefore, PCT+PIRO (AUC: 0.837) would be better used in predicting the development of MODS than PCT+MEDS (AUC: 0.758) and PCT+APACHE II (AUC: 0.794) (Figure 4B, Table 5).
In addition, after 28-days follow-up, the AUC values of the PCT, MEDS, APACHE II, and PIRO scores for 28-day mortality were 0.782 (95% CI: 0.683–0.882, P<0.001), 0.745 (95% CI: 0.627–0.863, P<0.001), 0.805 (95% CI: 0.707–0.904, P<0.001), 0.831 (95% CI: 0.742–0.920, P<0.001), respectively. The AUC values of the combination of PCT and severity scores were as follows: PCT+MEDS: 0.812 (95% CI: 0.705–0.919, P<0.001); PCT+APACHE II: 0.866 (95% CI: 0.789–0.943, P<0.001); PCT+PIRO: 0.885 (95% CI: 0.810–0.961, P<0.001). The ability of the PIRO score (AUC: 0.831) to predict 28-day mortality was better than that of MEDS (AUC: 0.745) and APACHE II (AUC: 0.805). Thus, PCT+PIRO (AUC: 0.885) are slightly better at predicting 28-day mortality than PCT+MEDS (AUC: 0.812) and PCT+APACHE II (AUC: 0.866) (Figure 4C, Table 6).
Patients’ 28-Day Survival
As Figure 5 shows, the cumulative survival probability within 28 days was lower in septic patients with a MEDS score>12.5 (P<0.001 by the Log rank test), an APACHE II score>15.5 (P<0.001 by the Log rank test), a PIRO score>11.5 (P<0.001 by the Log rank test), and a combination of PCT+MEDS>0.5 (P<0.001 by the Log rank test), PCT+APACHE II>0.23 (P<0.001 by the Log rank test), PCT+PIRO>0.39 (P<0.001 by the Log rank test), respectively.
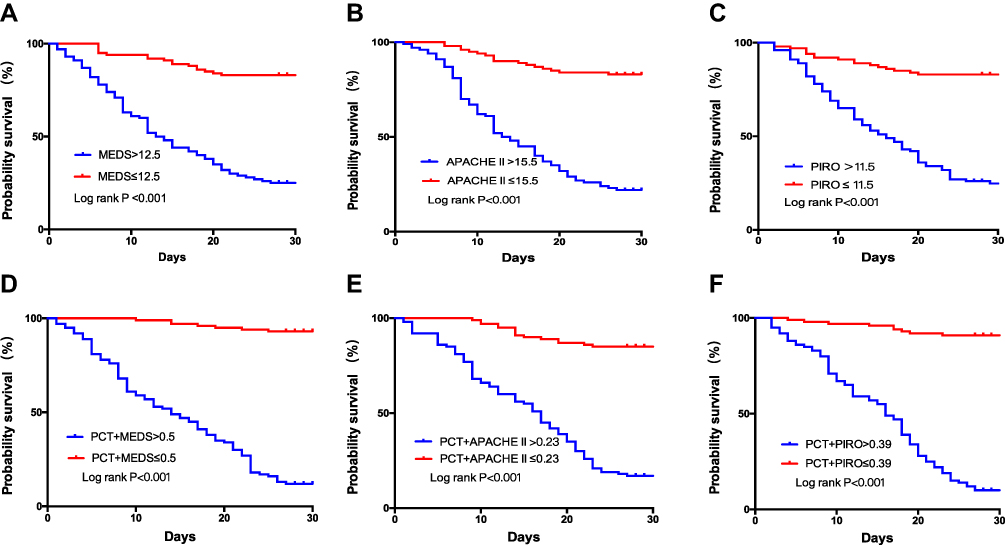 |
Figure 5 Kaplan-Meier curves for 28-day survival categorized by the MEDS score (A), APACHE II score (B), PIRO score (C), and combination value of PCT+MEDS (D), PCT+APACHE II (E), and PCT+PIRO (F) in septic patients with positive blood cultures. |
Discussion
Bloodstream infections (BSIs) are commonly considered as being caused by the presence of viable microorganisms in blood,17 and are often associated with severe infectious diseases with excessively high morbidity and mortality rates.18–20 Blood cultures are considered to be the reference standard for diagnosing BSIs and are still indispensable in BSI diagnosis.17 The Surviving Sepsis Campaign guidelines recommend that blood cultures are taken before starting antimicrobial therapy.21 Blood cultures are straightforward to perform and exhibit high sensitivity to cultivable pathogens.22 The worldwide increases in incidence have emerged as one of the leading causes of death,19 particularly in critically ill patients,20 and the global burden of morbidity and mortality from sepsis is significant.21 However, improvements in the clinical outcomes of patients with sepsis and septic shock have been made within the last decade, when short-term mortality rates had routinely approached 20%.22 Delayed, insufficient, or inappropriate anti-infection treatment leads to increased mortality from BSIs.14,16,23 Prompt initiation of antimicrobial therapies is a critical survival determinant.24 Currently, the cornerstone of BSI sepsis management continues to be early antimicrobial administration, source control, and supportive care.25–28 Therefore, early recognition of sepsis criticality, and immediate intervention is significant.
However, there have been very few studies on the criticality and risk structure of septic patients with BSIs. We did find that not all patients with positive blood cultures have a poor prognosis. After timely and effective treatment, many of them were successfully discharged. Therefore, it is necessary to find suitable predictors for the outcomes and prognosis of positive blood culture sepsis. Previous studies showed that SOFA, MEDS, APACHE II and PIRO scores increased with sepsis progression, reaching a maximum limit in septic shock. The PIRO system is an ideal staging system that incorporates assessment of premorbid baseline susceptibility, specific disorders responsible for illness, host response to infection, and the resulting degree of organ dysfunction. Our study applied the Howell-PIRO scoring system to predict the risk stratification and prognosis of septic patients with positive BSIs in an ED. The study by Narani et al demonstrated the significant value of PIRO scoring system in assessing risk stratification in emergency department patients with suspected sepsis.29 The latest study by Vebri et al showed that the modified PIRO severity score could be used as a predictor of mortality in children with pneumonia, as well as be used to select candidates for intensive care.30 The recent research by Professor T. Cardoso’s team had systematically verified the diagnostic and predictive value of the PIRO clinical staging system in ICU and general ward patients, and provided a basis for the decision-making about specific therapeutic interventions and enrollment in clinical trials.31
As for PCT, the study of Rao et al showed that PCT was significantly elevated in neonatal sepsis, which was of great significance for the diagnosis of sepsis.32 PCT was used as predictor of sepsis in obstructive acute pyelonephritis.33 Zhai et al demonstrated the good diagnostic value of PCT in sepsis closed abdominal injury infection.34 Thus, PCT was of great significance in sepsis diagnosis and mortality prediction.
In our study, as for ICU-admission, binary logistic regression analysis showed that WBC, PCT, Lac, ALB, NLR, along with the MEDS, APACHE II, and PIRO scores were independent predictors, but the SOFA score was not. The AUC of the APACHE II score was 0.780, which was a little higher than that of PCT (0.620), MEDS (0.740), or PIRO (0.751). In addition, the AUC of PCT in combination with the APACHE II score was significantly higher than that of PCT+MEDS. The AUC of PCT in combination with the APACHE II score was slightly higher than that of PCT+PIRO. The APACHE II score is regularly used to evaluate sepsis severity. For patients admitted to the ICU, their condition is usually critical and they are therefore more likely to develop sepsis or sepsis shock. Our results indicate that the APACHE II score has the highest predictive value for septic patients with positive BSIs. Previous studies have shown that the PIRO scoring system is suitable in assessing ICU patient criticality.35 This is consistent with our results. The AUC of the PIRO score was comparable with the APACHE II score, and similarly had a high predictive value of ICUadmission. No single biomarker predictions were particularly high, but when combined with other predictors the prediction value increases significantly.
MODS often indicates disease aggravation and deterioration, and is often associated with short-term mortality.36 In our study, WBC, PCT, NLR, ALB, and the MEDS, APACHE II, and PIRO scores independently predicted MODS development within three days of ED arrival. However, those of Lac and SOFA did not. The AUC of the PIRO score (0.811) was higher than that of the PCT (0.664), MEDS (0.701), or APACHE II (0.761) scores. Meanwhile, the AUC of PCT combined with the PIRO score was significantly higher than that of any single predictor. The AUC of PCT in combination with the PIRO score was slightly higher than that of PCT+MEDS or PCT+APACHE II score. The PIRO scoring system incorporates the high-risk factors of MODS and variable reflected established organ dysfunction.11 Therefore, its predictive value was found to be better than both the APACHE II and MEDS scores. These results correspond with the conclusions of previous studies.
In addition, we analyzed the 28-day mortality of positive BSIs. PIRO had a higher predictive value and showed better predictive ability than MEDS or APACHE II scores. In terms of combined prediction, PCT combined with the PIRO score had the highest predictive value for septic patients with positive BSIs. This was consistent with the characteristics of the PIRO scoring system used to assess the severity of critically ill patients. For 28-day mortality, the PIRO scoring system was superior and therefore could be widely used in sepsis prognosis assessment.
The predictive value of the PIRO scoring system and PCT for sepsis is significant. The perfect combination of their advantages has a significant effect on predicting risk stratification and prognosis in septic patients with positive blood cultures. PCT is often used to indicate the severity of bacterial infection. Through the analysis of previous clinical data, it is found that PCT has a high predictive value for ICUadmission, MODS development and 28-day mortality in septic patients with positive blood cultures. After combining it with PIRO scoring system, its predictive value is significantly improved, which has guiding significance for clinical treatment and prognosis. Consulting the literature, there are few studies on blood culture in sepsis, and there is no study on risk stratification and prognosis of patients with positive blood cultures. Our study is the first and of great significance. In future studies, we will further investigate the risk stratification and predictive value of septic patients with negative blood cultures. This will also be a very meaningful study.
Our study had several limitations: It was limited by being a single-center study with a relatively small sample size, and more centers and samples needed to be added to the cohort; some biomarkers had limitations and could not represent all the characteristics of sepsis, and more evaluation biomarkers were needed in the study. Our study also had some positives, in that this was the first time, to our knowledge, that a combination of the PIRO scoring system and PCT has successfully been used to assess the criticality and prognosis of septic patients with positive BSIs.
Conclusions
This study indicates that PCT combined with the PIRO scoring system is superior to that of PCT+MEDS or PCT+APACHE II score in predicting MODS and 28-day mortality in patients with positive blood cultures. The higher predictive value of the PIRO score is therefore essential in assessing the prognosis of sepsis patients with positive BSIs.
Abbreviations
ICU, Intensive care unit; MODS, multiple organ dysfunction syndrome; COPD, chronic obstructive pulmonary disease; CVD, cerebrovascular disease; CHF, congestive heart failure; CRD, chronic renal disease; DM, diabetes mellitus; MAP, mean arterial pressure; WBC, white blood cell; PCT, procalcitonin; Lac, lactate; CRP, C-reactive protein; ALB, albumin; NLR, neutrophils and lymphocytes ratio; SOFA, Sequential Organ Failure Assessment; APACHE II, Acute Physiology and Chronic Health Evaluation II; MEDS, Mortality in emergency department sepsis; PIRO, Predisposition, Infection, Response, and Organ dysfunction.
Data Sharing Statement
The dataset that was used to support the finding of this study will be made available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participant
All procedures performed in studies involving human participant were in accordance with the ethical standards of the institutional and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by Beijing Chao-Yang Hospital Ethics Committee. Written informed consent was obtained from all participants.
Acknowledgments
We would like to thank Beijing Chao-Yang Hospital for facilitating the study and covering the data collection costs. We would also like to acknowledge all data collectors, supervisors, and respondents without whom this research would not have been realized.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for- profit sectors.
Disclosure
The authors declare that there are no conflicts of interest regarding this work.
References
1. Hagel S, Pletz MW, Brunkhorst FM, Seifert H, Kern WV. Bakteriämie und Sepsis. Internist. 2013;54:399–407. doi:10.1007/s00108-012-3185-4
2. Lee -C-C, Chen S-Y, Chang I-J, Chen S-C, S-C W. Comparison of clinical manifestations and outcome of community-acquired bloodstream infections among the oldest old, elderly, and adult patients. Medicine. 2007;86:138–144. doi:10.1097/SHK.0b013e318067da56
3. Weinstein MP, Towns ML, Quartey SM, et al. The clinical significance of positive blood cultures in the 1990s: a prospective comprehensive evaluation of the microbiology, epidemiology, and outcome of bacteremia and fungemia in adults. Clin Infect Dis. 1997;24:584–602. doi:10.1093/clind/24.4.584
4. Long B, Koyfman A. Best clinical practice: blood culture utility in the emergency department. J Emerg Med. 2016;51:529–539. doi:10.1016/j.jemermed.2016.07.003
5. Girard TD, Ely EW. Bacteremia and sepsis in older adults. Clin Geriatr Med. 2007;23:633–647. doi:10.1016/j.cger.2007.05.003
6. Kethireddy S, Bilgili B, Sees A, et al. Culture-negative septic shock compared with culture-positive septic shock: a retrospective cohort study. Crit Care Med. 2018;46:506–512. doi:10.1097/CCM.0000000000002924
7. Coburn B, Morris AM, Tomlinson G, Detsky AS. Does this adult patient with suspected bacteremia require blood cultures? JAMA. 2012;308:502–511. doi:10.1001/jama.2012.8262.
8. Weinstein MP, Reller LB, Murphy JR, Lichtenstein KA. The clinical significance of positive blood cultures: a comprehensive analysis of 500 episodes of bacteremia and fungemia in adults. I. Laboratory and epidemiologic observations. Rev Infect Dis. 1983;5:35–53. doi:10.1093/clinids/5.1.35
9. Berild D, Mohseni A, Diep LM, Jensenius M, Ringertz SH. Adjustment of antibiotic treatment according to the results of blood cultures leads to decreased antibiotic use and costs. J Antimicrob Chemother. 2006;57:326–330. doi:10.1093/jac/dki463
10. Levy MM, Fink MP, Marshall JC, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS international sepsis definitions conference. Crit Care Med. 2003;31:1250–1256. doi:10.1097/01.CCM.0000050454.01978.3B
11. Chen Y-X, C-S L. Risk stratification and prognostic performance of the predisposition, infection, response, and organ dysfunction (PIRO) scoring system in septic patients in the emergency department: a cohort study. Crit Care. 2014;18:R74. doi:10.1186/cc13832
12. Howell MD, Talmor D, Schuetz P, Hunziker S, Jones AE, Shapiro NI. Proof of principle: the predisposition, infection, response, organ failure sepsis staging system. Crit Care Med. 2011;39:322–327. doi:10.1097/CCM.0b013e3182037a8e
13. Gai L, Tong Y, Yan B-Q. Research on the diagnostic effect of PCT level in serum on patients with sepsis due to different pathogenic causes. Eur Rev Med Pharmacol Sci. 2018;22:4238–4242. doi:10.26355/eurrev_201807_15418
14. Shokripour M, Omidifar N, Salami K, Moghadami M, Samizadeh B, Tornesello ML. Diagnostic accuracy of immunologic biomarkers for accurate diagnosis of bloodstream infection in patients with malignancy: procalcitonin in comparison with C-reactive protein. Can J Infect Dis Med Microbiol. 2020;2020:8362109. doi:10.1155/2020/8362109
15. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315:801–810. doi:10.1001/jama.2016.0287
16. Tafelski S, Nachtigall I, Stengel S, Wernecke K, Spies C. Comparison of three models for sepsis patient discrimination according to PIRO: predisposition, infection, response and organ dysfunction. Minerva Anestesiol. 2015;81:264–271.
17. Peker N, Couto N, Sinha B, Rossen JW. Diagnosis of bloodstream infections from positive blood cultures and directly from blood samples: recent developments in molecular approaches. Clin Microbiol Infect. 2018;24:944–955. doi:10.1016/j.cmi.2018.05.007
18. Opota O, Croxatto A, Prod’hom G, Greub G. Blood culture-based diagnosis of bacteraemia: state of the art. Clin Microbiol Infect. 2015;21:313–322. doi:10.1016/j.cmi.2015.01.003
19. Rutanga JP, Nyirahabimana T. Clinical significance of molecular diagnostic tools for bacterial bloodstream infections: a systematic review. Interdiscip Perspect Infect Dis. 2016;2016:6412085. doi:10.1155/2016/6412085
20. Loonen AJM, Wolffs PFG, Bruggeman CA, van den Brule AJC. Developments for improved diagnosis of bacterial bloodstream infections. Eur J Clin Microbiol Infect Dis. 2014;33:1687–1702. doi:10.1007/s10096-014-2153-4
21. Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580–637. doi:10.1097/CCM.0b013e31827e83af
22. Dubourg G, Raoult D. Emerging methodologies for pathogen identification in positive blood culture testing. Expert Rev Mol Diagn. 2016;16:97–111. doi:10.1586/14737159.2016.1112274
23. Heron M. Deaths: leading Causes for 2014. Natl Vital Stat Rep. 2016;65:1–96.
24. GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385:117–171. doi:10.1016/S0140-6736(14)61682-2
25. Reinhart K, Daniels R, Kissoon N, Machado FR, Schachter RD, Finfer S. Recognizing sepsis as a global health priority - a WHO resolution. N Engl J Med. 2017;377:414–417. doi:10.1056/NEJMp1707170
26. Kaukonen K-M, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000–2012. JAMA. 2014;311:1308–1316. doi:10.1001/jama.2014.2637
27. Bearman GML, Wenzel RP. Bacteremias: a leading cause of death. Arch Med Res. 2005;36:646–659. doi:10.1016/j.arcmed.2005.02.005
28. Kumar A, Zarychanski R, Light B, et al. Early combination antibiotic therapy yields improved survival compared with monotherapy in septic shock: a propensity-matched analysis. Crit Care Med. 2010;38:1773–1785. doi:10.1097/CCM.0b013e3181eb3ccd.
29. Sivayoham N, Hussain AN, Shabbo L, Christie D. An observational cohort study of the performance of the REDS score compared to the SIRS criteria, NEWS2, CURB65, SOFA, MEDS and PIRO scores to risk-stratify emergency department suspected sepsis. Ann Med. 2021;53:1863–1874. doi:10.1080/07853890.2021.1992495
30. Valentania V, Somasetia DH, Hilmanto D, Setiabudi D, Nataprawira HMN. Modified PIRO (predisposition, insult, response, organ dysfunction) severity score as a predictor for mortality of children with pneumonia in Hasan Sadikin Hospital, Bandung, Indonesia. Multidiscip Respir Med. 2021;16(1):735. doi:10.4081/mrm.2021.735
31. Cardoso T, Rodrigues PP, Nunes C, et al. Prospective international validation of the predisposition, infection, response and organ dysfunction (PIRO) clinical staging system among intensive care and general ward patients. Ann Intensive Care. 2021;11:180. doi:10.1186/s13613-021-00966-7
32. Rao H, Dutta S, Menon P, Attri S, Sachdeva N, Malik M. Procalcitonin and C-reactive protein for diagnosing post-operative sepsis in neonates. J Paediatr Child Health. 2022;58:593–599. doi:10.1111/jpc.15774
33. Tambo M, Taguchi S, Nakamura Y, Okegawa T, Fukuhara H. Presepsin and procalcitonin as predictors of sepsis based on the new Sepsis-3 definitions in obstructive acute pyelonephritis. BMC Urol. 2020;20:23. doi:10.1186/s12894-020-00596-4
34. Zhai G-H, Zhang W, Xiang Z, et al. Diagnostic value of sIL-2R, TNF-α and PCT for sepsis infection in patients with closed abdominal injury complicated with severe multiple abdominal injuries. Front Immunol. 2021;12:741268. doi:10.3389/fimmu.2021.741268
35. Moreno RP, Metnitz B, Adler L, et al. Sepsis mortality prediction based on predisposition, infection and response. Intensive Care Med. 2008;34:496–504. doi:10.1007/s00134-007-0943-1
36. Padkin A, Goldfrad C, Brady AR, Young D, Black N, Rowan K. Epidemiology of severe sepsis occurring in the first 24 hrs in intensive care units in England, Wales, and Northern Ireland. Crit Care Med. 2003;31:2332–2338. doi:10.1097/01.CCM.0000085141.75513.2B
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.