Back to Journals » Journal of Inflammation Research » Volume 18
Predictive Significance of the Monocyte-to-High-Density Lipoprotein Cholesterol Ratio in Post-Percutaneous Coronary Intervention Contrast-Induced Nephropathy Among Patients with Coronary Artery Disease
Authors Lin A, Peng Y, Shao J, Chen L, Lin Y ![]()
Received 27 February 2025
Accepted for publication 25 June 2025
Published 26 July 2025 Volume 2025:18 Pages 10015—10028
DOI https://doi.org/10.2147/JIR.S525296
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Wenjian Li
Aijie Lin,1,* Yanchun Peng,2,* Jiayi Shao,1 Liangwan Chen,3 Yanjuan Lin2,4
1School of Nursing, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China; 2Department of Nursing, Fujian Medical University Union Hospital, Fuzhou, Fujian, People’s Republic of China; 3Department of Cardiac Surgery, Fujian Medical University Union Hospital, Fuzhou, Fujian, People’s Republic of China; 4Department of Cardiac Surgery Nursing, Fujian Medical University Union Hospital, Fuzhou, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liangwan Chen, Department of Cardiac Surgery, Fujian Medical University Union Hospital, No. 29 Xinquan Road, Fuzhou, Fujian, 350001, People’s Republic of China, Email [email protected] Yanjuan Lin, Department of Nursing, Fujian Medical University Union Hospital, No. 29 Xinquan Road, Fuzhou, Fujian, 350001, People’s Republic of China, Email [email protected]
Purpose: This study aimed to examine the connection between monocyte-to-high-density lipoprotein cholesterol ratio (MHR) and contrast-induced nephropathy (CIN) and to introduce a novel perspective to early clinical diagnosis of CIN.
Patients and Methods: This single-center bidirectional cohort study included 1771 patients with coronary artery disease (CAD) who underwent elective percutaneous coronary intervention (PCI) from January 2017 to July 2022 at the Fujian Medical University Union Hospital. The study collected data retrospectively through an electronic medical record system with postoperative follow-up. The primary endpoint was CIN, and secondary endpoints were mortality and readmission within two years after PCI, along with total days of hospitalization. Patients were divided into three groups based on preoperative MHR (Group 1: MHR < 0.42; Group 2: MHR ≥ 0.42 and < 0.64; Group 3: MHR ≥ 0.64). The study used regression analyses to investigate the relationship between MHR and CIN rate and postoperative mortality, and demonstrated the cumulative incidence of postoperative fatal events in the three groups of patients by Kaplan-Meier curves, and also analyzed the predictive value of MHR and other inflammatory indicators on the risk of CIN by using receiver operating characteristic (ROC) curves.
Results: Compared to Group 1, Groups 2 and 3 had a higher incidence of CIN, higher mortality, and longer hospital stays (P < 0.001). Survival analysis showed significant differences in long-term mortality among the three groups (Log rank test, P = 0.032). Multivariate regression analysis showed that for every 1-unit increase in MHR, the risk of CIN increased 8.567-fold (95% CI: 4.291– 17.102, P < 0.001) and the risk of death increased 3.080-fold (95% CI: 1.423– 6.666, P = 0.004). ROC analysis showed that MHR had a good predictive ability for CIN (AUC: 0.713, 95% CI: 0.666– 0.759, P < 0.001).
Conclusion: MHR is significantly linked to CIN and 2-year mortality following PCI in CAD patients, serving as a CIN risk assessment tool to assist clinics in early identification of high-risk patients and optimization of treatment strategies.
Keywords: monocyte-to-high-density lipoprotein cholesterol ratio, inflammation, contrast-induced nephropathy, coronary artery disease, cardiovascular diseases, percutaneous coronary intervention
Introduction
From 1990 to 2019, the global incidence of cardiovascular diseases increased from 270 million to 520 million, with coronary artery disease (CAD) ranking as the second most prevalent condition.1 Percutaneous coronary intervention (PCI) is the predominant therapeutic approach for CAD. In 2022, 1.376 million PCI procedures were conducted in China, markedly enhancing the quality of life of those with CAD.2,3 The PCI treatment process necessitates the administration of contrast agent to visualize the lesion area. Contrast-induced nephropathy (CIN), a prevalent complication following PCI, has an incidence rate ranging from 3.3% to 13.3%,4–6 can raise the risk of major adverse cardiovascular events (MACE) by 1.8 times, augment mortality by over 10 times,7 and result in more healthcare expenditures.8 The prompt identification of risk factors linked to CIN and the prevention of its onset are essential for improving patient outcomes post-PCI.
The pathogenesis of CIN remains incompletely understood; however, research indicates that it is primarily associated with oxidative stress and inflammatory responses.9 Recent research findings have established a significant correlation between inflammatory indicators derived from clinical laboratory parameters, including the neutrophil-to-lymphocyte ratio (NLR), neutrophil-to-high-density lipoprotein cholesterol ratio (NHR), and platelet-to-lymphocyte ratio (PLR), with CIN and other inflammation-related diseases.10–12 From the levels of monocytes and high-density lipoprotein cholesterol (HDL-C) in routine blood tests, a new inflammatory indicator called the monocyte-to-high-density lipoprotein cholesterol ratio (MHR) is created. This ratio indicates the body’s pro-inflammatory and anti-inflammatory equilibrium.13 MHR has been used to forecast adverse outcomes, including all-cause mortality and MACE, and is associated with arterial plaque formation and the severity of atherosclerosis due to the accessibility and cost-effectiveness of the data.10,14–16 Recent findings suggest MHR may be an important predictor of CIN after PCI. A study involving 647 patients with acute coronary syndromes (ACS) identified preoperative MHR level as an independent risk factor for CIN, elevating the risk of CIN by a factor of 1.09.13 Similar results were noted in the study of Sağ.17 However, the above articles focused on myocardial infarction (MI) patients. They had relatively small sample sizes, and the studies’ follow-up period was limited to the hospitalization period to 6 months post-procedure, which did not adequately reflect the potential of MHR to forecast CIN and other long-term prognostic outcomes after PCI. Most current research focuses solely on a single sign and does not directly compare the prognostic usefulness of MHR with other inflammation indicators. Consequently, augmenting the sample size and incorporating non-MI CAD patients is imperative to examine the relationship between MHR and post-PCI CIN comprehensively. Furthermore, comparing MHR with other inflammatory indicators will elucidate whether it possesses more excellent predictive capability for CIN.
In conclusion, this study sought to expand the inclusion of sample size to assess the predictive capacity of MHR for CIN following PCI in patients with CAD. By comparing the diagnostic efficacy of MHR with inflammatory markers such as NLR, NHR and PLR, it was determined to explore whether MHR has significant advantages in the prediction of CIN, providing new insights and methods for the early clinical diagnosis and prevention of CIN.
Materials and Methods
Study Participants
This was a single-center bidirectional cohort study, encompassing patients with CAD aged 18 years or older who attended the Fujian Medical University Union Hospital for elective PCI between January 2017 and July 2022 to construct a dynamic cohort. MHR was calculated using monocyte versus HDL-C levels measured at admission. Based on the tertiles of MHR, patients were divided into three groups (Group 1: MHR <0.42; Group 2: MHR ≥0.42, <0.64; Group 3: ≥0.64). Exclusion criteria include: (1) severe hepatic and renal insufficiency, with severe hepatic insufficiency defined as serum alanine aminotransferase >2 times the upper limit of the reference value, and severe renal insufficiency defined as an estimated glomerular filtration rate (eGFR) of <15 mL/min/1.73 m2 or the need to undergo prolonged dialysis; (2) hyperthyroidism, severe infection, concurrent malignancy, immune system diseases, or hematological disorders (combined with moderate-to-severe anemia with hemoglobin [Hb] <90 g/L, leucocytosis or leukopenia [peripheral blood leucocyte count consistently above 10.0 × 109/L or consistently below 4.0 × 109/L], thrombocytosis or thrombocytopenia [platelet count consistently above 300 × 109/L or consistently below 100 × 109/L]); (3) exposure to or allergy to contrast agent within 7 days prior to PCI; (4) administration of nephrotoxic drugs within 48 hours before the procedure; (5) absence of any data from a complete blood count or preoperative or postoperative serum creatinine (SCr) within 48 hours following the procedure; and (6) patients receiving specific preoperative prophylactic interventions (e.g., hydration therapy or the need to take non-steroidal mineralocorticoid receptor antagonists [ns-MRAs]). An entire group of 1,771 patients were ultimately incorporated into the study. The approval was obtained from the Medical Ethics Committee of Fujian Medical University Union Hospital (2023KY032). All enrolled patients volunteered and provided informed consent.
Data Collection
Patients’ demographics, interventions, lab results, and length of stay in the hospital were retrieved from their electronic medical records. The blood collection method for determining biochemical indicators in this study involved instructing patients to fast after 8 PM on the night of admission. Each patient was required to fast for at least 10 hours before blood samples were taken, which were taken the following morning between 6 and 8 AM. At least two seasoned interventional cardiologists oversaw each patient’s care while they were in the hospital, and they followed all applicable protocols for PCI and perioperative management.
Endpoints and Follow-Up
The primary endpoint of the study was CIN, which was defined as a rise of SCr of 0.3 mg/dL or more or 50% within 48 hours after PCI, according to the Acute Kidney Injury Network.18 Secondary endpoints were mortality and readmission within two years after PCI, along with total days of hospitalization. The study constructed a retrospective cohort upfront to collect the occurrence of CIN through an electronic medical record system. Postoperative deaths and readmissions were collected by nurses with a license to practice and master’s degree nursing students through outpatient and telephone follow-up visits every four months after PCI. Follow-up time was calculated from the starting point of observation to death, loss of visit, or the termination of two years postoperatively.
Definitions
Smoking was defined as the daily intake of more than one cigarette, sustained for a period surpassing six months.19 Drinking was described as the consumption of at least one alcoholic beverage per week, with a total intake of 50 mL or more, maintained for a duration surpassing six months.20 Repeated in-hospital blood pressure readings of 140 mmHg or higher for systolic and 90 mmHg or higher for diastolic, or the use of anti-hypertensive medication in conjunction with self-reported hypertension, were considered to be hypertension.21 Diabetes mellitus (DM) was characterized by asymptomatic individuals exhibiting fasting blood glucose (FBG) levels of ≥7.0 mmol/L on multiple occasions or postprandial blood glucose levels of ≥11.1 mmol/L two hours after an oral glucose tolerance test; alternatively, glycated hemoglobin levels of ≥6.5%; or the presence of typical hyperglycemic symptoms or a hyperglycemic crisis with a random blood glucose ≥11.1 mmol/L; or a prior diagnosis of DM necessitating the use of oral antidiabetic medications or insulin.22 Hyperlipidemia is identified when cholesterol levels meet the following criteria: total cholesterol (TC) ≥6.21 mmol/L, triglycerides (TG) ≥2.26 mmol/L, low-density lipoprotein cholesterol (LDL-C) ≥4.14 mmol/L, or HDL-C <1.04 mmol/L.23 The definition of anemia was a Hb level below 130 g/L in adult males and 120 g/L in adult females.24 ICD-10 criteria were used to define CAD, chronic kidney disease (CKD), acute myocardial infarction (AMI), heart failure (HF), atrial fibrillation (AF), and stroke.25
The formulas for calculating the various inflammatory indicators involved in this study are as follows:
- MHR = monocyte count (109/L) / HDL-C (mmol/L).
- NLR = neutrophil count (109/L) / lymphocyte count (109/L).
- NHR = neutrophil count (109/L) / HDL-C (mmol/L).
- PLR = platelet count (109/L) / lymphocyte count (109/L).
Statistical Analysis
Continuous variables in patients’ baseline data were presented as mean ± standard deviation (for normal distribution) or median and interquartile range (for skewed distribution). In contrast, categorical variables were represented as counts and percentages. For normally distributed data, we used the ANOVA test; for skewed data, we used the Mann–Whitney U-test; and for categorical variables, we used either the chi-square test or Fisher’s exact test. These statistical methods were applied to identify differences among the three groups. The factors associated with CIN risk were investigated using logistic regression analysis. Age, white blood cell (WBC), left ventricular ejection fraction (LVEF), platelet (PLT), and SCr were corrected in Model I to remove potential confounding variables. Model II corrected for Model I with the number of stents placed, contrast dose, and infarcted vessel status. Model III adjusts for CKD, DM, and AMI based on Model II. We evaluated the diagnostic efficacy of four inflammatory indicators, including MHR, using receiver operating characteristic (ROC) curves and subsequently analyzed the predictive power of MHR for CIN compared to other inflammatory indicators. The study also used Cox proportional hazards regression analysis and expressed the association between preoperative MHR and death within two years after PCI by hazard ratio (HR) and 95% confidence interval (CI). Model I was adjusted for age, LVEF, and SCr. Model II was corrected for the number of stents placed and infarcted vessels. Model III adjusted CKD and DM based on Model II. The Kaplan-Meier and Log rank tests were used for survival analysis on three groups. The study used SPSS 27.0 (SPSS Inc., Chicago, IL, USA) for data analysis and GraphPad Prism 8.3 (GraphPad Software, CA, USA) to visualize the results. A significance level of P <0.05 was considered to be different.
Results
Baseline Characteristics of the Study Population
The inclusion of the study population is shown in Figure 1. The medical records of 1,950 patients with CAD who underwent elective PCI from January 2017 to July 2022 were reviewed. Based on the excluded criteria, 153 patients were omitted from the study. Additionally, 90 patients were lost to follow-up throughout the two years, leaving a final analysis of 1,771 patients (93.9%).
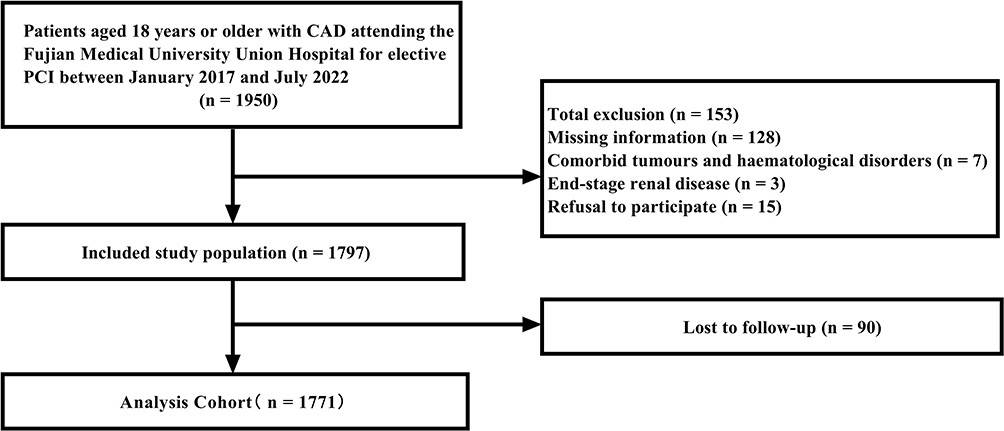 |
Figure 1 Patients included in the study. Abbreviations: CAD, coronary artery disease; PCI, percutaneous coronary intervention. |
The median MHR for all participants was 0.51 (0.36, 0.69). Table 1 delineates the baseline features of patients in each group, categorized by their MHR levels. The average age was 63.7 ± 0.2 years, with 357 (20.2%) female participants. Compared to Group 1, which exhibited lower MHR levels, Groups 2 and 3 comprised older patients, a higher proportion of males, elevated BMI, a more significant number of individuals who smoked and drank, and lower LVEF (P <0.05). In addition, the combination of CKD, hyperlipidemia, AMI, and HF was more significant in Group 2 and Group 3 (P <0.05). Regarding inflammatory indicators, Group 2 and Group 3, with higher MHR, had higher NLR and NHR and lower PLR. The three groups were more evenly matched in terms of drug use and contrast dose (P >0.05).
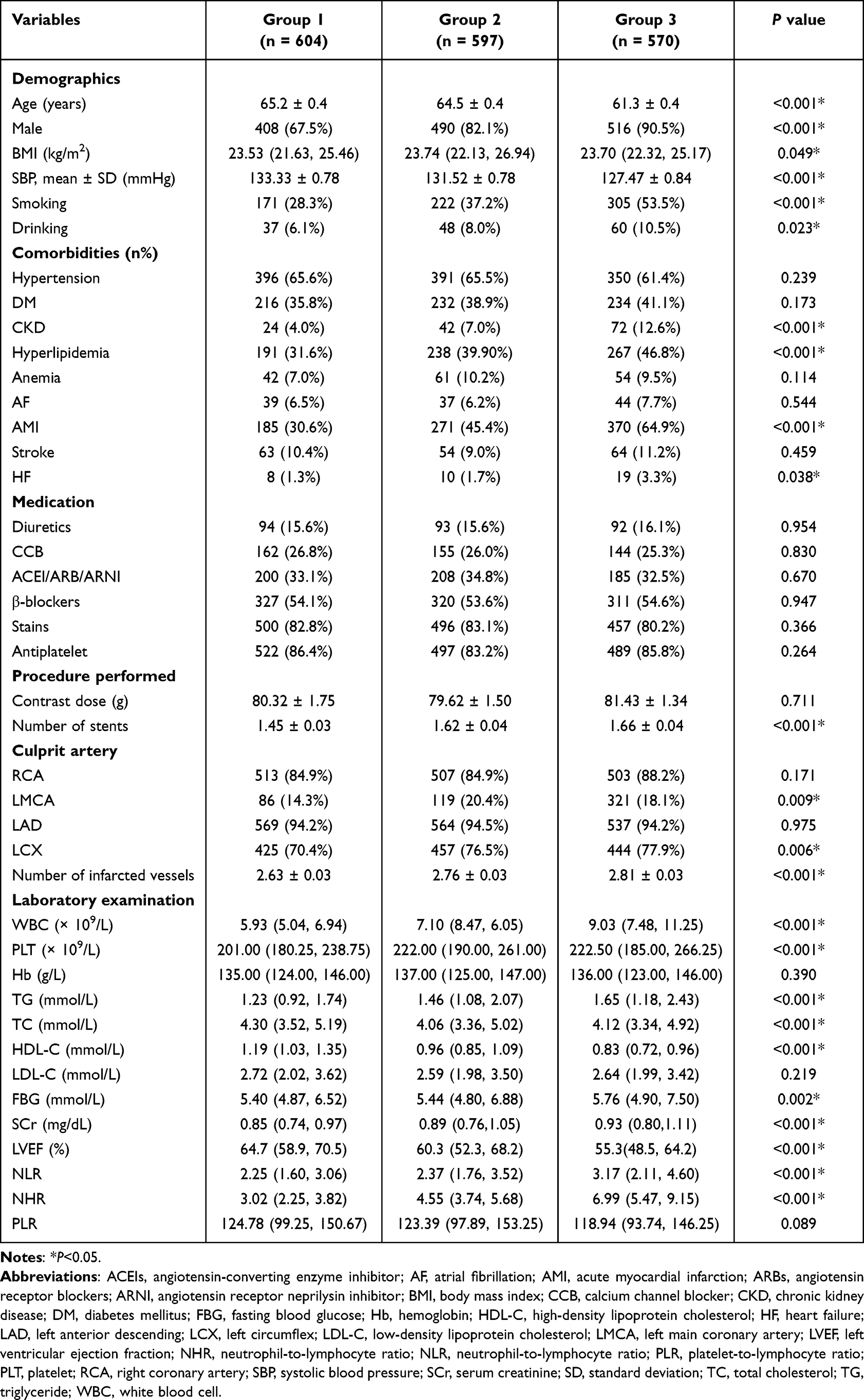 |
Table 1 Baseline Characteristics of Patients |
Differences in Clinical Outcomes of Patients in Different MHR Level Groups
In this study, 113 patients developed CIN in the postoperative period (6.4%), and 69 patients died during the two-year follow-up (3.9%), with a mean length of hospitalization of 8.0 ± 0.1 days and 818 readmissions (46.2%) (Table 2). Median MHR levels were elevated in patients who experienced CIN or mortality following PCI, showing a significant difference from those who did not (0.49 vs 0.67, P <0.001; 0.50 vs 0.62, P = 0.024) (Figure 2). Group 2 and Group 3 exhibited higher rates of CIN incidence, mortality, and extended hospital stays than Group 1 (P <0.001). All three groups had similar readmission rates (P = 0.563) (Table 2). The long-term mortality rates varied significantly among the groups, as seen by the Kaplan-Meier survival analysis curves (Log rank test, P = 0.032) (Figure 3).
 |
Table 2 Clinical Outcomes Among the Three Groups |
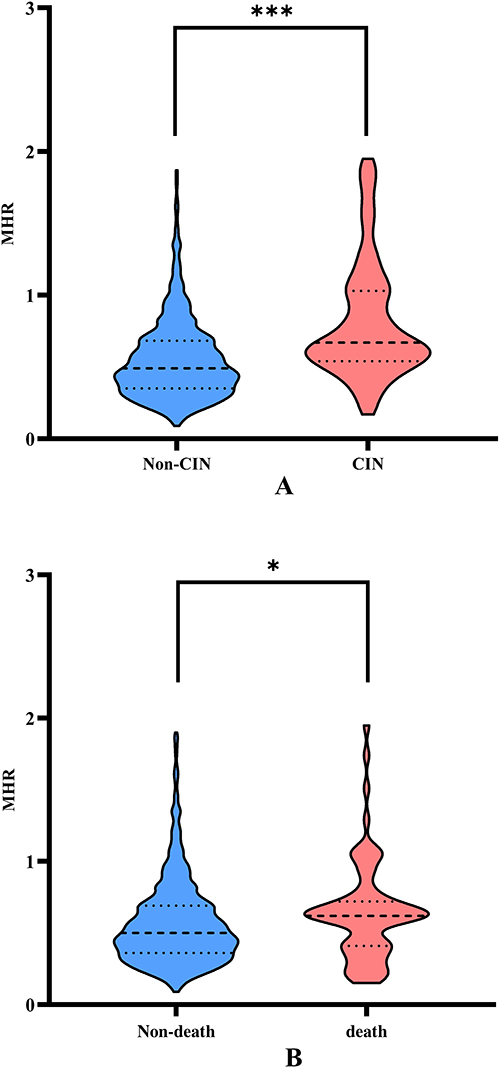 |
Figure 2 Relationship between clinical outcomes and MHR. Abbreviations: MHR, monocyte-to-high-density lipoprotein cholesterol ratio. Notes: (A) Comparison of preoperative MHR levels in patients who developed CIN versus those who did not develop CIN. (B) Comparison of preoperative MHR levels in dead and non-dead patients. *P <0.05, ***P <0.001. |
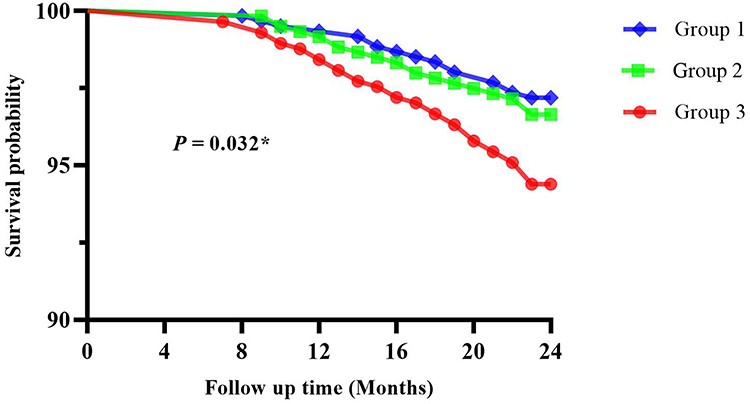 |
Figure 3 Mortality between patients in three groups. Notes: *P <0.05. |
The Predictive Capacity of MHR for Post-PCI CIN and Death Within Two Years of Follow-Up in CAD Patients
To identify potential causes of CIN following PCI, the research employed univariate logistic regression analysis (Table 3). We constructed three logistic regression models to investigate MHR’s predictive power further. In Model I, following adjustments for demographic variables and laboratory markers, the risk of CIN dramatically escalated with each 1-unit rise in MHR, exhibiting an approximate 7.97-fold increase (OR: 7.966, 95% CI: 4.070–15.591, P <0.001). After controlling for confounding variables and certain co-morbidities in Model II, Model III found similar results (OR: 8.567, 95% CI: 4.291–17.102, P <0.001). In all three models, the risk of CIN in Groups 2 and 3 patients exceeded that of Group 1 by more than two times. The study examined the association between MHR and mortality within two years post-PCI through Cox proportional hazards regression analysis. After correction, all three models revealed a significant trend of increased mortality risk associated with higher MHR levels. Patients in Group 3 had more than a two-fold risk of death two years after surgery compared with Group 1. However, no disparity in mortality risk was observed in Group 2 (Table 4).
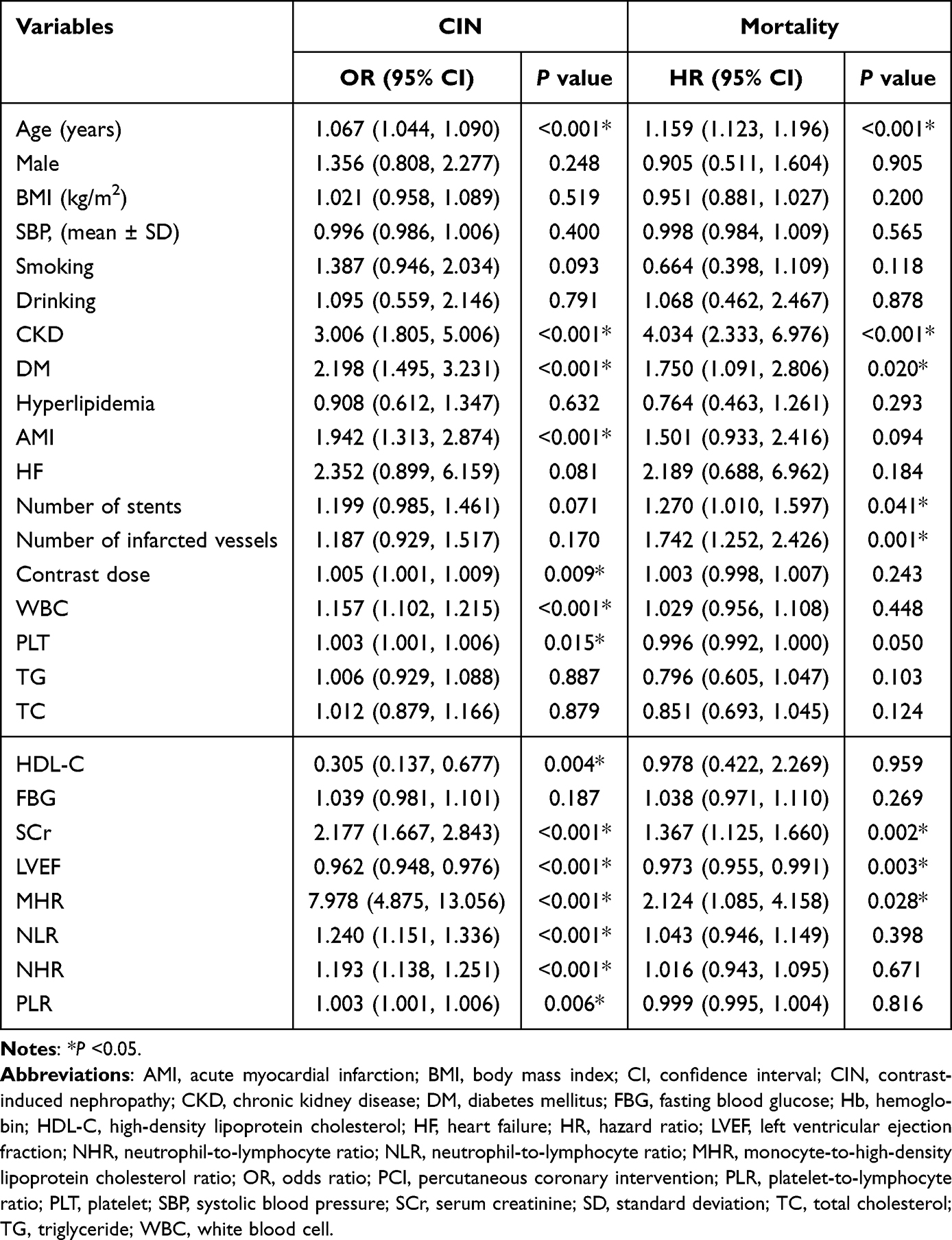 |
Table 3 Univariate Analysis of Predictors of CIN and Death Within Two years of PCI in Patients |
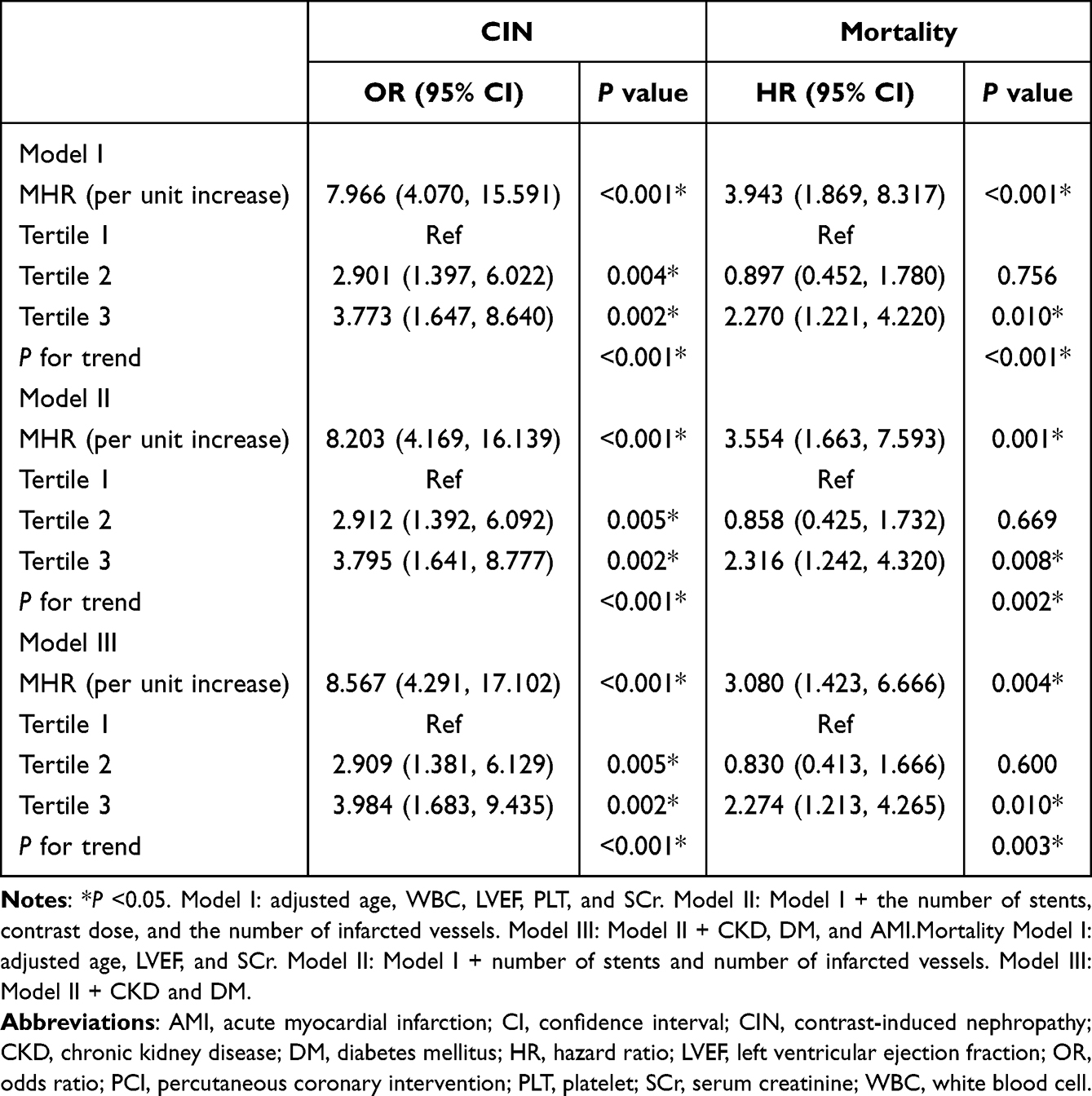 |
Table 4 Multivariate Analysis for Predictors of CIN and Death Within Two years of PCI in Patients |
Comparison with Inflammatory Indicators
Figure 4 shows the ROC curve analysis for predicting CIN. Among the four inflammatory indicators, the AUCs of MHR, NLR, and NHR were above 0.7 (0.713, 0.705, and 0.727, respectively), suggesting a good predictive value for CIN. We found no statistically significant differences between the three AUCs (P >0.05). MHR had a higher sensitivity (83.2%) but lower specificity (51.7%) for predicting CIN compared to the others (Table 5).
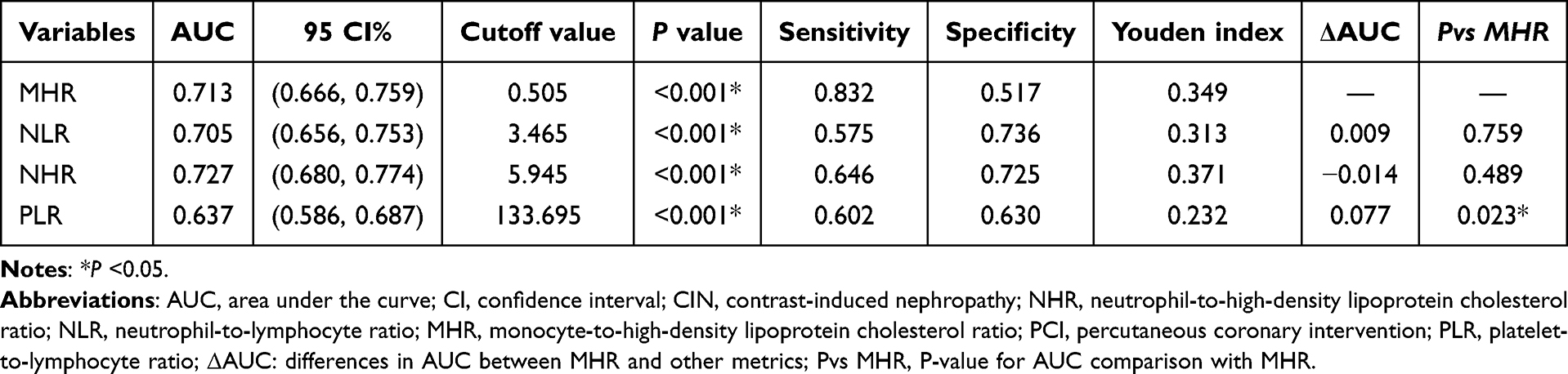 |
Table 5 Predictive Value of MHR, NLR, NHR, and PLR for Developing CIN After PCI in Patients |
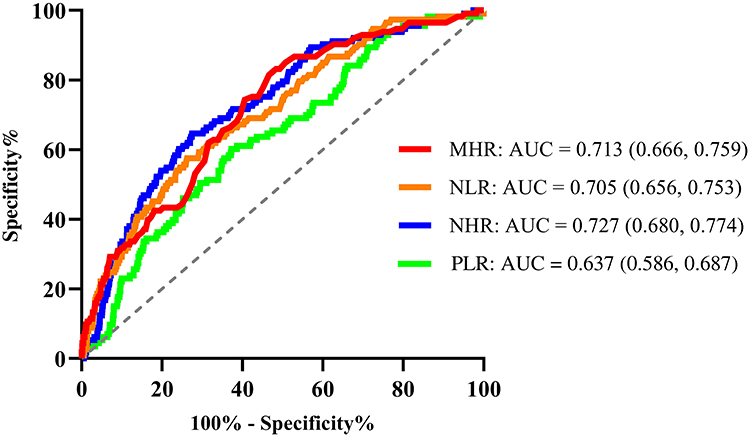 |
Figure 4 Receiver operating characteristic curves of MHR, NLR, NHR, and PLR for CIN. Abbreviations: AUC, area under the curve; CIN, contrast-induced nephropathy; NHR, neutrophil-to-high-density lipoprotein cholesterol ratio; NLR, neutrophil-to-lymphocyte ratio; MHR, monocyte-to-high-density lipoprotein cholesterol ratio; PLR, platelet-to-lymphocyte ratio. |
Discussion
This study evaluated the ability to predict MHR for CIN and mortality within two years post-PCI in CAD patients. It also compared its value for prediction against other inflammatory indicators. This area has not been extensively researched before. The findings suggested that patients presenting elevated MHR levels were at an increased risk of developing CIN following PCI. This association remains even after adjusting for potential confounders. Significantly higher mortality within two years after interventional treatment was also observed in the study in both groups of patients with higher MHR levels. In ROC curves analysis, MHR displayed a moderate predictive ability for CIN relative to other inflammatory indicators. This indicates the significance of MHR in the prognostic evaluation of CAD patients receiving elective PCI.
In interventional cardiology, the prevalence of contrast agent has rendered CIN a clinically important issue. It is the third leading cause of acute kidney injury (AKI) that occurs in hospitals26 and is strongly associated with negative short- and long-term clinical outcomes.13,17 Active prevention and risk prediction are still the mainstays since there are no suitable clinical treatments to lower the occurrence of CIN. While many factors contribute to CIN’s complicated pathophysiology, mounting evidence points to the inflammatory response as one of the critical culprits. Pro-inflammatory cytokines and inflammation are closely related. Research conducted by Kwasa et al indicated that patients exhibiting elevated CRP levels (indicative of an inflammatory state) faced an increased relative risk of developing CIN, implying a possible association between inflammation and CIN.27 The observed situation may result from elevated reactive oxygen species caused by osmotic stress and nephrotoxicity from the contrast agent, alongside endogenous molecules released by injured renal tubular epithelial cells that activate the kidney’s resident phagocytic receptor, initiating an inflammatory cascade that ultimately leads to renal injury.28–30 Current research trends emphasize the identification of potential biomarkers for predicting and diagnosing the onset of CIN, with specific markers linked to the inflammatory response; for instance, baseline levels of interleukin-18 and tumor necrosis factor-α serve as the most reliable predictors of CIN progression.31 Nonetheless, identifying these markers is both time-intensive and expensive, indicating a continued necessity to investigate more efficient and dependable predictive instruments to inform clinical practice.
MHR represents the ratio of monocytes to HDL-C and serves as a novel biomarker of the interplay between inflammation and lipid metabolism in the body. This metric robustly predicts all types of adverse outcomes post PCI.10,16 The findings of this study indicate that MHR levels in patients with CAD are positively correlated with the risk of developing CIN post-PCI and mortality within two years, with preoperative MHR typically elevated in patients exhibiting poorer prognoses. This is consistent with the outcomes of prior research. A Turkish study identified elevated preoperative MHR as an independent risk factor for the onset of CIN following PCI in patients with ACS. However, no correlation with mortality within six months post-surgery was noted.13 The correlation of MHR with CIN, cardiovascular disease, and other poor prognoses can be explained by the biological function of monocytes and HDL-C. Firstly, monocytes are a significant source of pro-inflammatory substances that bind to adhesion molecules on the damaged vascular endothelium, initiating atherosclerosis and releasing pro-inflammatory and pro-oxidant cytokines.32 In addition, monocytes have extensive phenotypic diversity, which are divided into functionally distinct subpopulations. Nonclassical and interferon-responsive monocytes may be more closely associated with increased inflammation in the atherosclerotic process than other subtypes.33 Julla et al investigated the relationship between circulating monocytes and the severity of CAD in patients with T2DM using transcriptomics and metabolomics. Their findings demonstrated a positive correlation between coronary artery calcification scores and monocyte counts and proportions, suggesting that monocytes may act as a predictive indicator for assessing the risk of cardiovascular events in T2DM patients.34 HDL-C represents the ability of high-density lipoprotein (HDL) to transport cholesterol, and HDL has anti-atherosclerotic properties. It inhibits the process of atherosclerosis by promoting cholesterol efflux, reducing the increase in myeloid cells and leukopoiesis, and thereby inhibiting the process of atherosclerosis.35 Disruptions in lipid metabolism, characterized by increased triglyceride, heightened trim, oxidized low-density lipoprotein, and diminished HDL-C, are commonly observed in the initial phases of renal illness.36 A cohort study involving 2,168 patients indicates that low levels of HDL-C are significantly linked to the progression of CKD and represent a key factor affecting its advancement.37 Chen et al conducted a stratified Mendelian randomization analysis using data from the UK Biobank, demonstrating that HDL-C levels below 50 mg/dL significantly and negatively correlated with the risk of cardiovascular diseases.38 Guo et al discovered that HDL-C-related indicators had strong predictive power for the occurrence of MACE during hospitalization following PCI.10 It is noteworthy that high MHR levels were significantly associated with the risk of death within two years after PCI compared with low levels of MHR in this study. However, similar results were not observed in the comparison of the medium and low-level MHR groups. This may be due to the fact that inflammation and metabolic disturbances in the medium-level MHR group had not yet reached the threshold to significantly affect the risk of death. Further exploration is required regarding the MHR threshold that elevates the mortality risk.
Current studies have demonstrated that NHR and NLR are important for CIN prognosis.10,12 Therefore, we further compared the predictive efficacy of MHR with other inflammatory indicators such as NLR, NHR, and PLR for the occurrence of CIN after PCI using ROC curve analysis. The data showed that the predictive efficacy of MHR was similar to that of NHR and NLR. These results may be attributable to the fact that neutrophils are also associated with the key pathophysiological basis of CAD, namely atherosclerosis, and their mediated inflammatory response accelerates the formation and rupture of atherosclerotic plaques.32,39 Indicators derived by combining various laboratory parameters can effectively assess the likelihood of poor prognosis in patients after PCI, providing new ideas for clinical risk stratification. There are many risk-scoring tools available for predicting the occurrence of CIN.40 However, these risk-scoring tools are less likely to incorporate biomarkers other than SCr. The study found that scoring tools incorporating routine blood and basic metabolic parameters are more potent in predicting adverse outcomes in CAD patients than the widely utilized Mehran score.41 Therefore, combining novel indices of biomarkers such as MHR with traditional risk scoring tools is expected to significantly improve the predictive efficacy of existing tools.
However, in the present study we found that although the accuracy of MHR in predicting CIN was high, the specificity was lower than other similar studies.13 The composition of the research population might account for this discrepancy. Unlike prior studies that have only included patients with MI, ours has a broader cohort of CAD patients that includes both MI and non-MI individuals. Patients with MI usually have a more severe inflammatory response and oxidative stress state, with more significant changes in MHR, thus showing higher specificity in predicting CIN. Conversely, non-MI patients may exhibit less pronounced alterations in MHR compared to MI patients owing to a less inflammatory response. Mixing the two categories of patients for analysis may dilute the specificity of MHR for CIN prediction. Consequently, subsequent subgroup studies may be conducted to investigate the disparities in the predictive capacity of MHR for CIN between infarcted and non-infarcted patients.
Despite advancements in vascular interventional techniques, CIN continues to pose a significant issue for patients with CAD. Its potential impact on patient prognosis warrants careful attention in clinical practice. There is a lack of research on the correlation between MHR and CIN after PCI. The results of this study support the idea that MHR levels are positively associated with the risk of developing CIN and that the potential of MHR in predicting CIN may be greater compared to predicting death after PCI. In addition, MHR is a simple, cost-effective, and easy-to-measure indicator for clinical staff compared to traditional CIN risk factors such as glomerular filtration rate. This study has certain limitations in several aspects. First, this is an observational single-center study with Chinese subjects. Whether there are differences in the predictive ability of MHR for CIN in different ethnic groups and the causal relationship between MHR and CIN needs to be further explored. Second, inflammation indicators fluctuate over time, and a solitary measurement may not accurately represent trends. Future high-quality longitudinal studies are essential to dynamically assess changes in MHR during the perioperative period of PCI and further analyze its association with adverse outcomes, such as CIN. In addition, some inflammatory markers (e.g., erythrocyte sedimentation rate [ESR] and high-sensitivity c-reactive protein [hs-CRP]) were lacking in the patients of this study, and future studies should include more inflammatory markers to assess their relevance and prognostic value in CAD. This study failed to include recent cases due to the limitation of the follow-up time requirement, which may affect the timeliness of the results. Follow-up studies will further update the data to improve the representativeness and reference value of the results.
Conclusions
This study shows that MHR independently forecasts the occurrence of CIN and mortality within two years in patients with CAD undergoing elective PCI, demonstrating strong predictive efficacy. This result suggests that clinical staff may consider the impact of MHR levels on outcomes when performing preoperative risk assessment for patients with CAD. In the future, we can develop more prediction models in conjunction with MHR to improve the application potential of prediction tools and provide more comprehensive support for clinical decision-making.
Abbreviations
ACEIs, angiotensin-converting enzyme inhibitor; ACS, acute coronary syndromes; AF, atrial fibrillation; AKI, acute kidney injury; AMI, acute myocardial infarction; ARBs, angiotensin receptor blockers; ARNI, angiotensin receptor neprilysin inhibitor; AUC, area under the curve; BMI, body mass index; CAD, coronary artery disease; CCB, calcium channel blocker; CI, confidence interval; CKD, chronic kidney disease; DM, diabetes mellitus; eGFR, estimated glomerular filtration rate; ESR, erythrocyte sedimentation rate; FBG, fasting blood glucose; Hb, hemoglobin; HDL, high-density lipoprotein; HDL-C, high-density lipoprotein cholesterol; HF, heart failure; HR, hazard ratio; hs-CRP, high-sensitivity c-reactive protein; LAD, left anterior descending; LCX, left circumflex; LDL-C, low-density lipoprotein cholesterol; LMCA, left main coronary artery; LVEF, left ventricular ejection fraction; MACE, major adverse cardiovascular events; MI, myocardial infarction; NHR, neutrophil-to-lymphocyte ratio; NLR, neutrophil-to-lymphocyte ratio; ns-MRAs, non-steroidal mineralocorticoid receptor antagonists; OR, odds ratio; PCI, percutaneous coronary intervention; PLR, platelet-to-lymphocyte ratio; PLT, platelet; RCA, right coronary artery; SBP, systolic blood pressure; SCr, serum creatinine; SD, standard deviation; TC, total cholesterol; TG, triglyceride; WBC, white blood cell.
Data Sharing Statement
Data supporting the results of this study are available from Fujian Medical University Union Hospital, but the availability of these data is limited and they are used under license for the current study and therefore not publicly available. However, data are available to the authors upon reasonable request and with permission from Fujian Medical University Union Hospital.
Ethics Approval and Informed Consent
The Ethics Committee of Fujian Medical University Union Hospital accepted the study protocol and informed consent procedure. All procedures adhered to the Declaration of Helsinki. All participants provided informed written consent for publication without revealing personally identifiable information.
Acknowledgments
The authors would like to respectfully appreciate Fujian Medical University Union Hospital for providing support and the patients for their active co-operation during the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Fifth Batch of Hospital Key Discipline Construction Projects (2022YYZDXK01).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update From the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
2. National Center for Cardiovascular Quality Improvement. Executive summary of the 2023 national report on the medical care quality of cardiovascular diseasein China. Chin Circulation J. 2024;39(09):833–852.
3. Rajkumar CA, Foley MJ, Ahmed-Jushuf F, et al. A placebo-controlled trial of percutaneous coronary intervention for stable Angina. N Engl J Med. 2023;389(25):2319–2330. doi:10.1056/NEJMoa2310610
4. Mohebi R, Karimi Galougahi K, Garcia JJ, et al. Long-term clinical impact of contrast-associated acute kidney injury following PCI: an ADAPT-DES substudy. JACC. 2022;15(7):753–766. doi:10.1016/j.jcin.2021.11.026
5. Rihal CS, Textor SC, Grill DE, et al. Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation. 2002;105(19):2259–2264. doi:10.1161/01.CIR.0000016043.87291.33
6. He H, Chen XR, Chen YQ, et al. Prevalence and Predictors of Contrast-Induced Nephropathy (CIN) in Patients with ST-Segment Elevation Myocardial Infarction (STEMI) Undergoing Percutaneous Coronary Intervention (PCI): a meta-analysis. J Interv Cardiol. 2019;2019:2750173. doi:10.1155/2019/2750173
7. McCullough PA, Choi JP, Feghali GA, et al. Contrast-induced acute kidney injury. J Am Coll Cardiol. 2016;68(13):1465–1473. doi:10.1016/j.jacc.2016.05.099
8. Subramanian S, Tumlin J, Bapat B, et al. Economic burden of contrast-induced nephropathy: implications for prevention strategies. J Med Econ. 2007;10:119–134. doi:10.3111/200710119134
9. Zhang F, Lu Z, Wang F. Advances in the pathogenesis and prevention of contrast-induced nephropathy. Life Sci. 2020;259:118379. doi:10.1016/j.lfs.2020.118379
10. Guo J, Chen M, Hong Y, et al. Comparison of the predicting value of neutrophil to high-density lipoprotein cholesterol ratio and monocyte to high-density lipoprotein cholesterol ratio for in-hospital prognosis and severe coronary artery stenosis in patients with st-segment elevation acute myocardial infarction following percutaneous coronary intervention: a retrospective study. J Inflamm Res. 2023;16:4541–4557. doi:10.2147/JIR.S425663
11. Velibey Y, Oz A, Tanik O, et al. Platelet-to-lymphocyte ratio predicts contrast-induced acute kidney injury in patients with st-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Angiology. 2017;68(5):419–427. doi:10.1177/0003319716660244
12. He T, Mohammadpour B, Willman M, et al. Prognostic role of neutrophil to lymphocyte ratio in contrast-induced nephropathy: a systematic review and meta-analysis. Angiology;2024. 33197241238512. doi:10.1177/00033197241238512
13. Ulus T, Isgandarov K, Yilmaz AS, et al. Monocyte to high-density lipoprotein ratio predicts contrast-induced nephropathy in patients with acute coronary syndrome. Angiology. 2018;69(10):909–916. doi:10.1177/0003319718760916
14. Zhang DP, Baituola G, Wu TT, et al. An elevated monocyte-to-high-density lipoprotein-cholesterol ratio is associated with mortality in patients with coronary artery disease who have undergone PCI. Biosci Rep. 2020;40(8). doi:10.1042/BSR20201108.
15. Xi J, Men S, Nan J, et al. The blood monocyte to high density lipoprotein cholesterol ratio (MHR) is a possible marker of carotid artery plaque. Lipids Health Dis. 2022;21(1):130. doi:10.1186/s12944-022-01741-8
16. Açıkgöz SK, Açıkgöz E, Şensoy B, et al. Monocyte to high-density lipoprotein cholesterol ratio is predictive of in-hospital and five-year mortality in ST-segment elevation myocardial infarction. Cardiol J. 2016;23(5):505–512. doi:10.5603/CJ.a2016.0026
17. Sağ S, Yıldız A, Aydin KA, et al. Association of monocyte to HDL cholesterol level with contrast induced nephropathy in STEMI patients treated with primary PCI. Clin Chem Lab Med. 2017;55(1):132–138. doi:10.1515/cclm-2016-0005
18. Mehta RL, Kellum JA, Shah SV, et al. Acute kidney injury network: report of an initiative to improve outcomes in acute kidney injury. Crit Care. 2007;11(2):R31. doi:10.1186/cc5713
19. Organization WH. Guidelines for Controlling and Monitoring the Tobacco Epidemic. Geneva: World Health Organization: World Health Organization; 1998.
20. Organization WH. Alcohol. Available from: https://www.who.int/newsroom/factsheets/detail/alcohol.
21. Mancia G, Kreutz R, Brunström M, et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension: endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). J Hypertens. 2023;41(12):1874–2071. doi:10.1097/HJH.0000000000003480
22. ElSayed NA, Aleppo G, Bannuru RR. American Diabetes Association Professional Practice Committee. 2. Diagnosis and Classification of Diabetes: Standards of Care in Diabetes—2024. Diabetes Care. 2024;47(Suppl 1):S20–s42. doi:10.2337/dc24-S002
23. National Cholesterol Education Program (NCEP). Expert panel on detection, evaluation, and treatment of high blood cholesterol in Adults (Adult Treatment Panel III). third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel iii) final report. Circulation. 2002;106(25):3143–3421.
24. WHO Guidelines Approved by the Guidelines Review Committee. Guideline on Haemoglobin Cutoffs to Define Anaemia in Individuals and Populations. World Health Organization, © World Health Organization; 2024.
25. Association AM. The complete ofifcial code-book: ICD-10-CM. Eden Prairie. 2016.
26. Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. Am J Kidney Dis. 2002;39(5):930–936. doi:10.1053/ajkd.2002.32766
27. Kwasa EA, Vinayak S, Armstrong R. The role of inflammation in contrast-induced nephropathy. Br J Radiol. 2014;87(1041):20130738. doi:10.1259/bjr.20130738
28. Lau A, Chung H, Komada T, et al. Renal immune surveillance and dipeptidase-1 contribute to contrast-induced acute kidney injury. J Clin Invest. 2018;128(7):2894–2913. doi:10.1172/JCI96640
29. Yao Y, Chen S, Cao M, et al. Antigen-specific CD8(+) T cell feedback activates NLRP3 inflammasome in antigen-presenting cells through perforin. Nat Commun. 2017;8:15402. doi:10.1038/ncomms15402
30. Furuichi K, Wada T, Iwata Y, et al. Interleukin-1-dependent sequential chemokine expression and inflammatory cell infiltration in ischemia-reperfusion injury. Crit Care Med. 2006;34(9):2447–2455. doi:10.1097/01.CCM.0000233878.36340.10
31. Banda J, Duarte R, Dix-Peek T, et al. Biomarkers for diagnosis and prediction of outcomes in contrast-induced nephropathy. Int J Nephrol. 2020;2020:8568139. doi:10.1155/2020/8568139
32. Ganjali S, Gotto AM Jr, Ruscica M, et al. Monocyte-to-HDL-cholesterol ratio as a prognostic marker in cardiovascular diseases. J Cell Physiol. 2018;233(12):9237–9246.
33. Bashore AC, Xue C, Kim E, et al. Monocyte single-cell multimodal profiling in cardiovascular disease risk states. Circ Res. 2024;135(6):685–700. doi:10.1161/CIRCRESAHA.124.324457
34. Julla JB, Girard D, Diedisheim M, et al. Blood monocyte phenotype is a marker of cardiovascular risk in type 2 diabetes. Circ Res. 2024;134(2):189–202. doi:10.1161/CIRCRESAHA.123.322757
35. Yvan-Charvet L, Pagler T, Gautier EL, et al. ATP-binding cassette transporters and HDL suppress hematopoietic stem cell proliferation. Science. 2010;328(5986):1689–1693. doi:10.1126/science.1189731
36. Mitrofanova A, Merscher S, Fornoni A. Kidney lipid dysmetabolism and lipid droplet accumulation in chronic kidney disease. Nat Rev Nephrol. 2023;19(10):629–645. doi:10.1038/s41581-023-00741-w
37. Nam KH, Chang TI, Joo YS, et al. Association between serum high-density lipoprotein cholesterol levels and progression of chronic kidney disease: results from the KNOW-CKD. J Am Heart Assoc. 2019;8(6):e011162. doi:10.1161/JAHA.118.011162
38. Chen JX, Li Y, Zhang YB, et al. Nonlinear relationship between high-density lipoprotein cholesterol and cardiovascular disease: an observational and Mendelian randomization analysis. Metabolism. 2024;154:155817. doi:10.1016/j.metabol.2024.155817
39. Baetta R, Corsini A. Role of polymorphonuclear neutrophils in atherosclerosis: current state and future perspectives. Atherosclerosis. 2010;210(1):1–13. doi:10.1016/j.atherosclerosis.2009.10.028
40. Liu YH, Liu Y, Zhou YL, et al. Comparison of different risk scores for predicting contrast induced nephropathy and outcomes after primary percutaneous coronary intervention in patients with st elevation myocardial infarction. Am J Cardiol. 2016;117(12):1896–1903. doi:10.1016/j.amjcard.2016.03.033
41. Toprak K, Kaplangoray M, Memioğlu T, et al. comparative evaluation of intermountain risk score with mehran risk score for risk estimation of contrast-induced nephropathy and short-term mortality in st-segment elevation myocardial infarction patients. Angiology. 2025;76(2):154–165. doi:10.1177/00033197231201931
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.