Back to Journals » Cancer Management and Research » Volume 11
Predictive Role Of Body Composition Parameters In Operable Breast Cancer Patients Treated With Neoadjuvant Chemotherapy
Authors Omarini C ![]() , Palumbo P
, Palumbo P ![]() , Pecchi A, Draisci S, Balduzzi S
, Pecchi A, Draisci S, Balduzzi S ![]() , Nasso C, Barbolini M, Isca C, Bocconi A, Moscetti L
, Nasso C, Barbolini M, Isca C, Bocconi A, Moscetti L ![]() , Galetti S
, Galetti S ![]() , Tazzioli G
, Tazzioli G ![]() , Torricelli P, Cascinu S, Piacentini F
, Torricelli P, Cascinu S, Piacentini F ![]()
Received 20 May 2019
Accepted for publication 4 September 2019
Published 12 November 2019 Volume 2019:11 Pages 9563—9569
DOI https://doi.org/10.2147/CMAR.S216034
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Claudia Omarini,1 Patrizia Palumbo,2 Annarita Pecchi,3 Stefano Draisci,3 Sara Balduzzi,4 Cecilia Nasso,1 Monica Barbolini,1 Chrystel Isca,1 Alessandro Bocconi,1 Luca Moscetti,1 Silvia Galetti,5 Giovanni Tazzioli,6 Pietro Torricelli,3 Stefano Cascinu,1 Federico Piacentini1
1Division of Medical Oncology, Department of Medical and Surgical Sciences for Children & Adults, University Hospital of Modena, Modena, Italy; 2Division of Clinical Nutrition and Metabolism, Department of Specialist Medicines, University Hospital of Modena, Modena, Italy; 3Department of Radiology, University Hospital of Modena, Modena, Italy; 4Statistics Unit, Department of Medical and Surgical Sciences for Children & Adults, University Hospital of Modena, Modena, Italy; 5Division of Clinical Nutrition and Metabolism, Department of Medical and Surgical Sciences for Children & Adults, University Hospital of Modena, Modena, Italy; 6Department of General Surgery and Surgical Specialities, University Hospital of Modena, Modena, Italy
Correspondence: Claudia Omarini
Division of Medical Oncology, Department of Medical and Surgical Sciences for Children & Adults, University Hospital of Modena, Via Del Pozzo 71, Modena 41122, Italy
Tel +39 059 4222845
Email [email protected]
Background: Fat tissue is strongly involved in BC tumorigenesis inducing insulin resistance, chronic inflammation and hormonal changes. Computed tomography (CT) imaging instead of body mass index (BMI) gives a reliable measure of skeletal muscle mass and body fat distribution. The impact of body composition parameters (BCPs) on chemosensitivity is still debated. We examined the associations between BCPs and tumor response to neoadjuvant chemotherapy (NC) in patients treated for operable breast cancer (BC).
Methods: A retrospective review of BC patients treated with NC in Modena Cancer Center between 2005 and 2017 was performed. BCPs, such as subcutaneous fat area (SFA), visceral fat area (VFA), lumbar skeletal muscle index (LSMI) and liver-to-spleen (L/S) ratio were calculated by Advance workstation (General Electric), software ADW server 3.2 or 4.7. BMI and BCPs were correlated with pathological complete response (pCR) and survival outcomes.
Results: 407 patients were included in the study: 55% with BMI < 25 and 45% with BMI ≥ 25. 137 of them had pre-treatment CT scan imagines. Overweight was significantly associated with postmenopausal status and older age. Hormonal receptor positive BC was more frequent in overweight patients (p<0.05). Postmenopausal women had higher VFA, fatty liver disease and obesity compared to premenopausal patients. No association between BMI classes and tumor response was detected. High VFA and liver steatosis were negative predictive factors for pCR (pCR rate: 36% normal VFA vs 20% high VFA, p= 0.048; no steatosis 32% vs steatosis 13%, p=0.056). Neither BMI classes nor BCPs significantly influenced overall survival and relapse-free survival.
Conclusion: Visceral adiposity as well as steatosis were closely involved in chemosensitivity in BC patients treated with NC. Their measures from clinically acquired CT scans provide significant predictive information that outperform BMI value. More research is required to evaluate the relationship among adiposity site and survival outcomes.
Keywords: BMI, fat tissue, sarcopenia, pathological complete response, breast cancer
Introduction
Obesity is a known risk factor for various health disorders, including breast cancer (BC).1 Obesity is generally evaluated using body mass index (BMI), that is an indirect measurement of adipose tissue, calculated as weight in kilograms divided height in meters squared. BMI cannot account for differences in fat distribution and cannot distinguish between adipose tissue and muscles. In fact, low BMI can mask excess of adiposity such as high BMI can mask low muscularity. Computed tomography (CT) imaging can be a useful tool for a direct measure of body fat distribution distinguishing among visceral, subcutaneous, internal fat tissue (mostly in the liver) and skeletal muscle mass.2
Several studies highlighted the association between obesity and poor prognosis in BC patients.3 It is well known that women with BC, who are overweight or gain weight after diagnosis, have a greater risk for recurrence and death.3 Moreover, not only the excess of adiposity, but also sarcopenia (low skeletal muscle mass) seems to be a negative prognostic factor for death and recurrence in patients with non-metastatic BC.4 Biologically, fat cells can produce inflammatory cytokines (Il-6 and TNF-α), growth factors (insulin growth factor receptor), aromatase and adiponectin.5 These molecules increase the level of leptin and endogenous sex steroids determining chronic inflammation and insulin resistance.5 Given these facts, adipose tissue may influence treatment sensitivity. Only two studies, with a small sample size, have examined the relationship between body composition and neoadjuvant treatment sensitivity in BC women, providing controversial results.6,7 Our goal was to examine associations between measure of body composition parameters (BCPs), considering adiposity and sarcopenia, and response to neoadjuvant chemotherapy (NC) in patients treated for operable BC.
Patients And Methods
Patient Population
We performed a retrospective review of the electronic medical records of all patients treated with NC for early BC in Modena Cancer Center between 2005 and 2017. All the patients with a histologically proven diagnosis of BC (stage I–III) treated with primary chemotherapy either within clinical trials or on the basis of standard guidelines were included. Patients needed weight and height available and/or pre-treatment CT scan imagines. No other eligibility/exclusion criteria were applied. Tumor-specific characteristics, including cancer stage, grade and tumor subtypes, were collected. Tumor subtypes were defined as follows: human epidermal growth factor receptor 2 (HER2) positive BC (HER2 status was reported as positive or negative according to IHC 3+ or HIS amplification), hormone receptor positive BC (estrogen and/or progesterone receptors expression >1% and HER2 negative) and triple negative (TN) BC (hormone receptor and HER2 negative). NC was given according to the standard recommendation, dose reduction or drug discontinuation were applied in case of toxicity according to clinician’s choice. Data about patient characteristics’ such as age, menopausal status, weight and height at the beginning of NC were collected. Responses to NC were collected too. Pathological complete response (pCR) was defined as complete disappearance of invasive tumor in the breast and axillary lymph nodes.
Body Mass Index (BMI)
According to the international classification of body mass index (BMI), patients were categorized into two main classes: normal weight (BMI < 25) and overweight (BMI ≥ 25). Moreover, in the subgroup of normal weight patients, women with BMI <18.5 were classified as underweight (BMI < 25) while overweight patients with BMI ≥ 30 were considered obese.
Body Composition Parameters (BCPs)
For patients with available CT scan imagines taken at the time of the initial treatment, BCPs were calculated by Advance workstation (General Electric), software ADW server 3.2 or 4.7. The cutoff points used for classifying BCPs were based on data in the literature.6,8 Radiologists, who performed the BCPs measures, were blinded for clinical data. We evaluated subcutaneous fat area (SFA, cm2), visceral fat area (VFA, cm2), lumbar muscle cross-sectional area (LMCA, m2) and liver steatosis (L/S ratio). In particular, the cut-off for high SFA and VFA was 100: VFA and SFA < 100 meaning normal visceral or subcutaneous adiposity while VFA or SFA ≥ 100 meaning high visceral or subcutaneous adiposity, respectively. Using BMI and VFA value, the presence of Obesity Disease, defined as BMI ≥ 25 and VFA ≥ 100 was evaluated too. The lumbar muscle cross-sectional area (LMCA, m2) was used as a measure of total body skeletal muscle mass including psoas, paraspinal and abdominal wall muscles. In order to adjust the LMCA according to patient stature, we calculated the lumbar skeletal muscle index (LSMI, cm2/m2): total L3 skeletal muscle mass/body surface area. The cut-off value for LSMI was 38.5: patients with LSMI < 38.5 were sarcopenic while those with LSMI ≥ 38.5 were normal. Finally, the presence of liver steatosis was considered as a measure of internal fat distribution. The CT liver-to-spleen ratio (L/S ratio) was used for fatty liver analysis. Fatty liver was defined as L/S ratio <1.
Statistical Analysis
Baseline clinical characteristics were compared between BMI subgroups (<25 vs ≥25) by chi-square test for categorical variables (i.e. menopausal status, BC subtypes, grade, neoadjuvant chemotherapy, type of surgery, stage) and by Wilcoxon Mann–Whitney test for continuous variables (i.e. age at diagnosis). The association between BCPs and menopausal status and the association between BCPs and pathological complete response were evaluated through the chi-square test. The association between BCPs and pCR was assessed by calculating odds ratio and their 95% confidence intervals through univariate logistic regression.
Overall survival (OS: defined as the time from diagnosis of BC to death/last follow-up), and relapse-free survival (RFS: defined as the time from the date of the diagnosis to the date of the first documented relapse or death) were assessed. Hazard ratios (HRs) and their 95% confidence intervals (CIs) were obtained through univariate and multivariate Cox models considering BMI subgroups, BCPs and pathological complete response.
All analyses were performed using STATA 14 (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP).
Results
A total of 407 patients were included in the study, 137 of them had pre-treatment CT scan imagine available for BCPs analysis (Figure 1). Overall, 225 were normal weight with a BMI score under 25 compared to 182 (45%) overweight. Specifically, in the subgroup of overweight women 37% (68) were obese. Only 8 patients were underweight. Patient, tumor and treatment characteristics stratified by BMI subgroups are listed in Table 1. The two cohorts of patients were well balanced according to treatment administered, type of surgery, grade and stage of disease. There was no association between clinical stage, nuclear grade, neoadjuvant chemotherapy regimen, type of surgery and BMI subgroups (p=not significant). Overall, 75% of patients received anthracycline-taxane-based regimen, 5% taxane-based chemotherapy, 9% anthracycline-based regimen and 8% platinum-based regimen. Of note, 7% of overweight patients received a chemotherapy dose reduction due to their high body surface area. Considering patients’ characteristics, overweight was significantly associated with postmenopausal status and older (≥65 years) age. Particularly, 37% of premenopausal women were overweight vs 53% of postmenopausal women (Table 1). Considering tumour subtypes and BMI, hormonal receptor positive (HR+) tumors were more frequent in overweight women (p<0.05). Regarding BCPs, most of the patients (94%) had high SFA while VFA was normal in most than half of them. Overall, 34% of women had criteria for Obesity Disease. Moreover, liver steatosis was detected in 18% of women. Finally, 48 patients were sarcopenic, 8 of them with sarcopenic overweight. We found no detectable difference between body fat distribution parameters and tumor subtype. On the contrary, postmenopausal status was significantly associated with high VFA, fatty liver disease and obesity (Table 2).
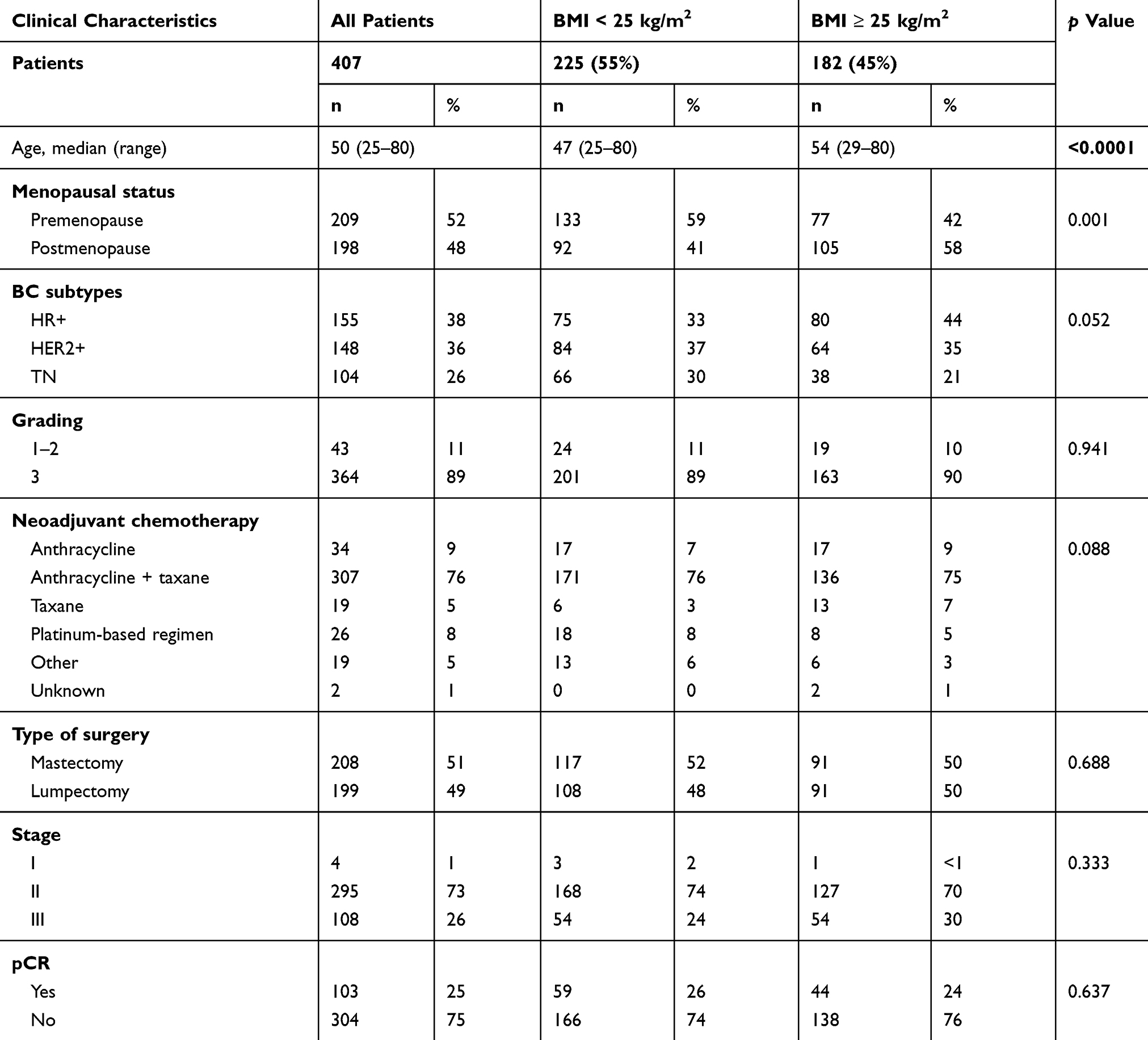 |
Table 1 Patient And Clinical Characteristics By BMI Value Among Women Treated With Neoadjuvant Chemotherapy |
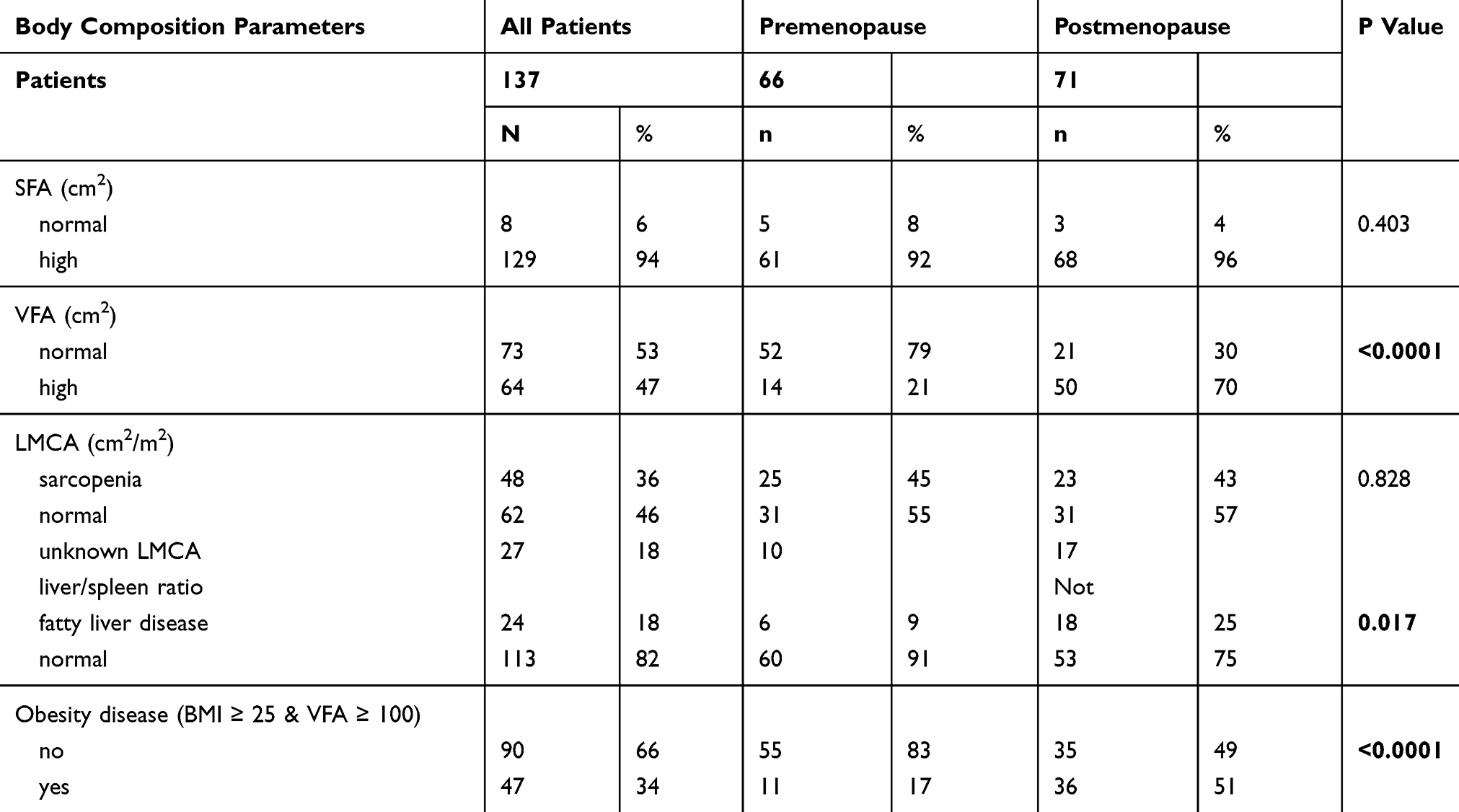 |
Table 2 Body Composition Parameters In Overall Population And According To Menopausal Status |
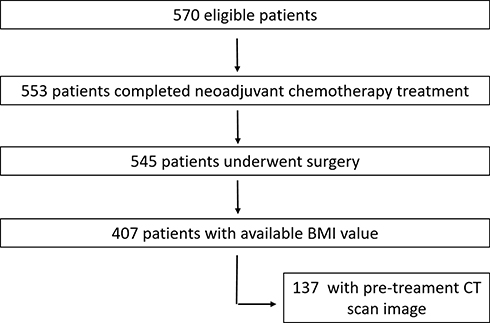 |
Figure 1 Flowchart of the study population. |
Overall, 25% of patients achieved pCR. In particular, 57% of them (59 patients) were normal/underweight vs 43% (44) overweight according to BMI classification (p=not significant) (Table 1). On the contrary, high visceral fat and liver steatosis were negative predictive factors for tumor response to neoadjuvant chemotherapy (p≤0.05) (Table 3 – Figure 2). In particular, in the subgroup of patients with pCR, 67% had normal visceral fat and 92% absence of fatty liver disease, respectively. No statistical significant correlation between BCPs and pCR according to BC phenotype was detected.
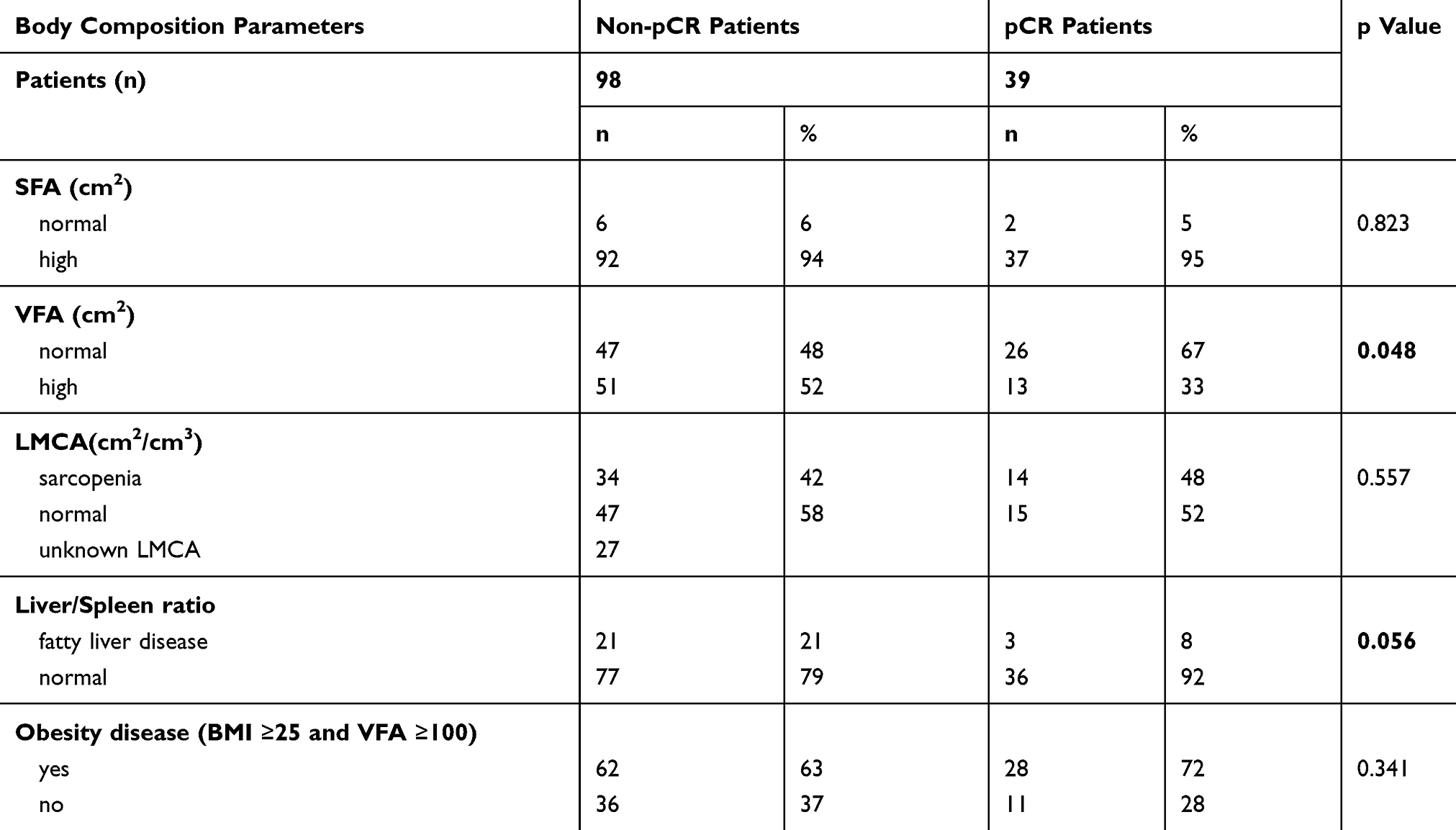 |
Table 3 Results Of The Correlation Analyses For Body Composition Parameters And pCR Rate |
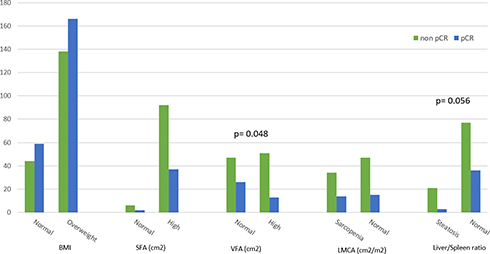 |
Figure 2 pCR rate according to body distribution parameters and BMI. |
At the time of the analysis, 25 patients (6%) had died and 33 (8%) had experienced a recurrence: 7 (3.8%) and 12 (6.5%) in overweight subgroup vs 18 (8%) and 21 (9%) in normal weight cohort, respectively. Neither BMI classes nor BCPs distribution significantly influenced overall survival and relapse-free survival. Only pCR was significantly associated with better survival outcomes in univariate analysis. As expected, patients with pCR have better OS (HR 0.37; 95% CI, 0.18 to 0.77, p= 0.008) and RFS (HR, 0.34; 95% CI, 0.16 to 0.74, p= 0.007) compared to patients with residual cancer disease after systemic therapy.
Discussion
The achievement of pCR is a known prognostic factor in BC patients treated with NC. Several biological and clinical parameters influence tumor response to chemotherapy.9–11 Body fat tissue seems to be one of these factors. Fat tissue promotes cancer progression by increasing cell proliferation, cell survival and metastatic processes.5 Adipose tissue determines a dysregulation of several metabolic pathways by a continuous crosstalk between fat tissue and cancer cells.12 Adipocytes modify tumor microenvironment inducing insulin resistance and inflammation by the production of leptin, adiponectin, plasminogen activator inhibitor-1 and vascular endothelial growth factor.13 In particular, finding from a recent clinical studies review, suggested how the influence of adipose tissue on cancer development depends on the type of fat too. Visceral adipose tissue seems to be more bio-energetically active and with more pro-cancer activity than subcutaneous adipose tissue.14 CT scan imagines are a useful tool to assess information on body fat distribution and muscle mass. In literature, limited data exist regarding body composition and chemosensitivity. Our results suggest a negative predictive role of visceral fat in tumor response to NC. In particular, the presence of visceral fat and internal fat tissue assessed from CT scan imagines is significantly associated with lower rate of pCR. In the subgroup of patients with pCR, 67% had normal visceral fat and 92% absence of fatty liver disease, respectively. No association between subcutaneous fat and tumor response was found confirming that visceral fat tissue plays a more central role in chemo-resistance than other type of body fat. These evidences justify the absence of correlation between BMI measure and pCR rate found in our study, too. In fact, BMI value does not account for differences in body composition. It is known how patients with high BMI can be sarcopenic and how patients with normal BMI can have visceral and intra-visceral fat deposits. In literature, data on the predictive role of BMI are extremely controversy. In a large study conducted by MD Anderson Cancer Center, the pCR rate was significantly lower in overweight patients compare to normal/underweight ones.15 Although, a metanalysis based on eight major trials found no association between BMI measure and tumor sensitivity.16
Postmenopausal status is a known cause of changes in body fat distribution, mainly increasing visceral fat tissue.17,18 In our study population, postmenopausal status was significantly associated with overweight, high VFA and fatty liver compared to premenopausal women. Fat tissue is rich in aromatases, enzyme able to convert androgens to estrogens. It is well demonstrated that overweight women have a higher level of estrogens compared to normal weight patients.18 These clinical data can explain the increased number of HR+ BC in overweight women compared to normal weight ones founded in our analysis.
Regarding sarcopenia and pCR rate, no relationship was found in our study. That result must be interpreted with caution considering the small number of patients found to be sarcopenic in our study population. Data from a retrospective study suggested a positive predictive and prognostic value of sarcopenia in the subgroup of normal weight women.7 The reason for this benefit was explained by the relatively higher chemotherapy dose used in that subgroup of patients. On the contrary, evidence on sarcopenia and tumor other than BC identified a strong association between sarcopenia, cachexia syndrome and worse survival outcomes.19
This analysis has some limitations particularly because it is a retrospective cohort study. Other limitation was that patients staging with CT scan included a subgroup of women with more aggressive tumor with a higher risk of metastatic spread compared to women staged with liver-ultrasound and chest x-ray. This selection could justify the absence of association between BCPs and survival outcomes. Finally, 7% of overweight patients received a chemotherapy dose reduction due to their high body surface area that could be a bias in the evaluation of tumor response to chemotherapy.
Conclusion
Fat tissue is strongly involved in BC tumorigenesis inducing insulin resistance, chronic inflammation and hormonal changes.5 In particular, visceral adipose tissue seems to have more pro-cancer activity than other adipose tissue.14 The evaluation of BCPs is the best way to assess the real body composition. BMI alone cannot account for neither differences in fat distribution nor type of body fat. Our finding confirms the evidence that visceral fat is more involved in cancer cells homeostasis than other adipose tissue. High levels of visceral and intra-visceral fat significantly influence chemosensitivity. The rate of pCR is significantly lower in patients with visceral adiposity and steatosis. To improve efficacy of treatment is essential to clarify the relationship among adiposity, treatment sensitivity and survival outcomes.
Ethics Approval And Informed Consent
The institutional review board of AOU Policlinico of Modena approved this retrospective study and waived the need to obtain informed consent from the patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sun L, Zhu Y, Qian Q, et al. Body mass index and prognosis of breast cancer: an analysis by menstruation status when breast cancer diagnosis. Medicine (Baltimore). 2018;97(26):e11220. doi:10.1097/MD.0000000000011220
2. Caan BJ, Cespedes Feliciano EM, Prado CM, et al. Association of muscle and adiposity measured by computed tomography with survival in patients with nonmetastatic breast cancer. JAMA Oncol. 2018;4(6):798–804. doi:10.1001/jamaoncol.2018.0137
3. Chlebowski RT, Aiello E, McTiernan A. Weight loss in breast cancer patient management. J Clin Oncol. 2002;20(4):1128–1143. doi:10.1200/JCO.2002.20.4.1128
4. Gourd E. Sarcopenia and adiposity linked to overall survival. Lancet Oncol. 2018;19(5):
5. van Kruijsdijk RC, van der Wall E, Visseren FL. Obesity and cancer: the role of dysfunctional adipose tissue. Cancer Epidemiol Biomarkers Prev. 2009;18(10):2569–2578. doi:10.1158/1055-9965.EPI-09-0372
6. Iwase T, Sangai T, Nagashima T, et al. Impact of body fat distribution on neoadjuvant chemotherapy outcomes in advanced breast cancer patients. Cancer Med. 2016;5(1):41–48. doi:10.1002/cam4.571
7. Del Fabbro E, Parsons H, Warneke CL, et al. The relationship between body composition and response to neoadjuvant chemotherapy in women with operable breast cancer. Oncologist. 2012;17(10):1240–1245. doi:10.1634/theoncologist.2012-0169
8. Deluche E, Leobon S, Desport JC, et al. Impact of body composition on outcome in patients with early breast cancer. Support Care Cancer. 2018;26(3):861–868. doi:10.1007/s00520-017-3902-6
9. Omarini C, Guaitoli G, Noventa S, et al. Impact of time to surgery after neoadjuvant chemotherapy in operable breast cancer patients. Eur J Surg Oncol. 2017;43(4):613–618. doi:10.1016/j.ejso.2016.09.020
10. Guarneri V, Dieci MV, Barbieri E, et al. Loss of HER2 positivity and prognosis after neoadjuvant therapy in HER2-positive breast cancer patients. Ann Oncol. 2013;24(12):2990–2994. doi:10.1093/annonc/mdt364
11. Pennisi A, Kieber-Emmons T, Makhoul I, et al. Relevance of pathological complete response after neoadjuvant therapy for breast cancer. Breast Cancer (Auckl). 2016;10:103–106. doi:10.4137/BCBCR.S33163
12. Burhans MS, Hagman DK, Kuzma JN, et al. Contribution of adipose tissue inflammation to the development of type 2 diabetes mellitus. Compr Physiol. 2018;9(1):1–58. doi:10.1002/cphy.c170040
13. Rausch LK, Hofer M, Pramsohler S, et al. Adiponectin, leptin and visfatin in hypoxia and its effect for weight loss in obesity. Front Endocrinol (Lausanne). 2018;9:615. doi:10.3389/fendo.2018.00615
14. Himbert C, Delphan M, Scherer D, et al. Signals from the adipose microenvironment and the obesity-cancer link-a systematic review. Cancer Prev Res (Phila). 2017;10(9):494–506. doi:10.1158/1940-6207.CAPR-16-0322
15. Litton JK, Gonzalez-Angulo AM, Warneke CL, et al. Relationship between obesity and pathologic response to neoadjuvant chemotherapy among women with operable breast cancer. J Clin Oncol. 2008;26(25):4072–4077. doi:10.1200/JCO.2007.14.4527
16. Erbes T, Stickeler E, Rücker G, et al. BMI and pathologic complete response to neoadjuvant chemotherapy in breast cancer: a study and meta-analysis. Clin Breast Cancer. 2016;16(4):e119–32. doi:10.1016/j.clbc.2016.02.018
17. Amadou A, Hainaut P, Romieu I. Role of obesity in the risk of breast cancer: lessons from anthropometry. J Oncol. 2013;2013:906495. doi:10.1155/2013/906495
18. Neuhouser ML, Aragaki AK, Prentice RL, et al. Overweight, obesity, and postmenopausal invasive breast cancer risk: a secondary analysis of the women’s health initiative randomized clinical trials. JAMA Oncol. 2015;1(5):611–621. doi:10.1001/jamaoncol.2015.1546
19. Shachar SS, Williams GR, Muss HB, et al. Prognostic value of sarcopenia in adults with solid tumours: a meta-analysis and systematic review. Eur J Cancer. 2016;57:58–67. doi:10.1016/j.ejca.2015.12.030
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.